







Languages
Pages
Legal

Haute Autorité de santé, 2 avenue du Stade-de-France – 93218 Saint-Denis-la-Plaine Cedex – Tél. : 01 55 93 70 00 – www.has-sante.fr
CCEERRTTIIFFIICCAATTIIOONN MMAANNUUAALL
FFOORR HHEEAALLTTHHCCAARREE OORRGGAANNIISSAATTIIOONNSS
VV22001100
NNoovveemmbbeerr 22000088
DDeeppaarrttmmeenntt ffoorr tthhee IImmpprroovveemmeenntt ooff QQuuaalliittyy aanndd SSaaffeettyy ooff HHeeaalltthhccaarree
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 2/120 Manuel de certification – Édition novembre 2008
Avant-propos
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 3/120 Manuel de certification – Édition novembre 2008
PREFACE The procedure for the certification of healthcare organisations, which was introduced into the French healthcare system by order No. 96-346 of 24 April 1996 on hospital reform, aims to provide an independent assessment of the quality of services in an establishment. The certificate process is now part of the reality of French healthcare: - certification has allowed the approach to quality to be boosted and made sustainable; - the certification visit is a key period in the life of the healthcare establishments. The 2010 version represents a significant change in the certification process. The aim is to offer to the healthcare system a mechanism that provides a relevant and balanced response to the expectations of users, healthcare professionals and the public authorities: - certification must provide accessible and clear information to users; - its own position as an internal management tool for the establishments must be strengthened; - it must create the conditions under which healthcare professionals wish to act; - it must finally play a role in regulating quality in healthcare organisations. Results of the certification must become an essential element for understanding the quality of
the establishments. Certification V1 aimed to start the process, V2 provided for the medicalisation of the process, while the new system has been thought up and developed to implement a certification system that is both ongoing and efficient. Laurent Degos François Romaneix Chairman of the Haute Autorité de Santé Director of the Haute Autorité de Santé
Introduction
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 4/120 Manuel de certification – Édition novembre 2008
INTRODUCTION 1 - The development of a certification system covered by the V2010 The certification procedure, which is now part of the reality of French healthcare, must respond to numerous expectations from its environment. Within the framework of the development of the 3rd version, the Haute Autorité de Santé wishes to carry out an important reorganisation, with three main concerns in mind: - to learn lessons from the critical feedback noted during the actual operation of the second version of the procedure; - to make the approach suitable for an environment that has changed significantly; - to take into account the processes used in accreditation systems in other countries. The new manual has been drafted with a view to concentrating, during the certification process, on the main levers and on those elements that enable quality and safety of care in healthcare establishments, within a context that is characterised by: - legitimate claims expressed by users; - overexposure of professionals to excessively formal external procedures; - demographic difficulties which are encountered by a very large number of professionals; - budgetary constraints in the healthcare system. a) The positioning of V2010 certification The preparatory V2010 work and feedback from experience in the previous versions have demonstrated the need to bear in mind and clarify the positioning of the certification. This positioning is characterised by three main elements:
1. HAS certification is a certification of an establishment as a whole and not a certification for each one of the areas of activity that make up a healthcare establishment:
The system that has been set up (general frame of reference, non-comprehensive visit, generalist surveyors) relates to the overall operation of the establishment and does not aim to analyse the operation of each area of activity in precise detail.
2. Certification has two complementary aims. It evaluates both:
o implementation of a management system for the establishment, including whether or not a process is in place to improve the quality and safety of
healthcare; o whether the establishment has achieved a level of quality which is based on specific criteria that are deemed to be essential. For this reason, HAS has
endeavoured to improve its methods of evaluation to allow for reproducible measurement of quality in critical areas through the definition of "required priority practices" (RPP) (see below).
Introduction
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 5/120 Manuel de certification – Édition novembre 2008
Both of these objectives have been the subject of further developments. They aim to establish a renewed and reinforced set of requirements, which will be expressed through a process of grading and decision-making using a narrow frame of reference. There will undoubtedly be situations in which HAS will be called upon to declare that healthcare establishments have not been certified.
Certification still promotes the "learning process”, but it is not a simple supportive educational measure for healthcare establishments. It provides an assessment of the quality of an establishment, where expectations of users, professionals and public authorities intersect.
3. Certification is a measure that helps to regulate the quality of healthcare establishments. The approach proposed within the framework of V2010 attaches great importance to the idea that the decision to grant certification should be more firmly anchored to mechanisms of regulation of hospitals by reinforcing the requirements for coherence between the efforts required by the Hospitalisation and Healthcare Organisation Department (DHOS), the Regional Hospitalisation Agencies (ARH) and HAS, where the concern is to implement quality criteria and to analyse quality indicators. More fundamentally, and without giving up the principle of independence of the decision-making process for the certification of healthcare establishments, the aim is to integrate the certification procedure into context, before the visit (through the more systematic use of other available evaluation work and results) and after it (by insuring that certification decisions be considered in discussions between the healthcare establishments and the regional hospitalisation agencies leading to the definition of multi-annual contracts concerning objectives and resources).
b) General objectives pursued when developing V2010 Four general objectives have guided the development of V2010:
1. To reinforce the procedure’s efficiency in terms of improving healthcare quality and safety;
2. To simplify the certification process by reducing the workload and formal requirements;
3. To increase the guarantee provided to users;
4. To include certification and the issue of quality of care in the hospital regulation process. 2 – V2010 certification manual This document contains the reference framework, criteria and assessment elements from version 2010 of the certification. This manual, drafted thanks to the work of groups made up of healthcare professionals, experts and users’ representatives, has been re-read by the various stakeholders and institutions involved in the certification of healthcare establishments.
Introduction
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 6/120 Manuel de certification – Édition novembre 2008
a) The structure of the manual The chosen structure of the manual is: - a two-chapter structure
- chapter I: Management of the establishment - chapter II: Patient care
HAS has chosen to focus on the evaluation of management systems and has simplified the structure of the manual by avoiding redundancy between the requirements relating to the definition of policies and those relating to the implementation and evaluation of those policies.
- organisation of the items to be evaluated according to stages in a process of improvement.
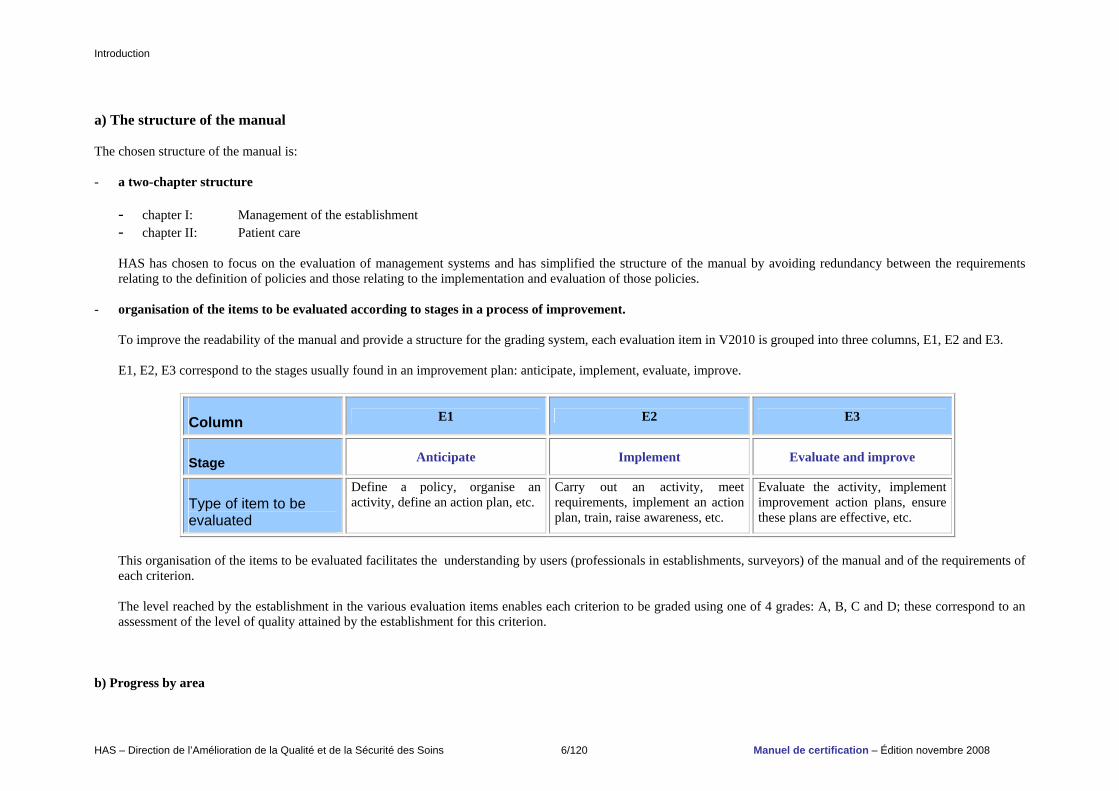
To improve the readability of the manual and provide a structure for the grading system, each evaluation item in V2010 is grouped into three columns, E1, E2 and E3. E1, E2, E3 correspond to the stages usually found in an improvement plan: anticipate, implement, evaluate, improve.
Column E1 E2 E3
Stage Anticipate Implement Evaluate and improve
Type of item to be evaluated
Define a policy, organise an activity, define an action plan, etc.
Carry out an activity, meet requirements, implement an action plan, train, raise awareness, etc.
Evaluate the activity, implement improvement action plans, ensure these plans are effective, etc.
This organisation of the items to be evaluated facilitates the understanding by users (professionals in establishments, surveyors) of the manual and of the requirements of each criterion. The level reached by the establishment in the various evaluation items enables each criterion to be graded using one of 4 grades: A, B, C and D; these correspond to an assessment of the level of quality attained by the establishment for this criterion.
b) Progress by area
Introduction
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 7/120 Manuel de certification – Édition novembre 2008
The subject areas developed in the manual deal with:
- management of establishments
o Strengthening requirements for setting up a system of security management and developing a culture of safety. o Development of requirements for evaluating and improving organisational and professional practices; this involves continuing with measures undertaken as
part of V2 and consolidating these by deploying them at an institutional level, adapting and integrating them in the practice in all areas of activity, widening their scope to include notions of equity, access to care and analysis of the appropriateness of care.
o Raising awareness of management changes within establishments, through: - promotion of decision-making and management procedures by means of scorecards and by monitoring evaluation and improvement activities,
giving a high priority to dialogue; - integration of requirements pertaining to sustainable development.
- patient rights
o New positioning of requirements pertaining to ethical issues. o Raising awareness of the idea of positive treatment. In continuance with a movement that arose within the medical and social work sector, it has appeared
to be necessary, within the framework of V2010, to go beyond requirements for the prevention of abuse, which is limited to criminal and individual behaviour, by encouraging establishments to implement steps to ensure that organisations become more respectful of individuals’ requirements and expectations.
o Reinforcing the requirements concerning the respect of patients’ rights at the end of life and the right to palliative care.
- patient care
o Top-priority objectives for improving the safety of care are displayed. o Reinforcement of evaluation of how operating suites function. o The improvement in the care of chronic illnesses and in therapeutic education for patients educations.
o Reinforcement of the evaluation of high risk activities.
Finally, the manual focuses on the ability of the healthcare establishment to implement a global approach to improvement of healthcare quality and safety and takes into account the work of other inspection and monitoring systems leading to the withdrawal of certain criteria (sterile environment, fire safety, etc.). The corollary of this development is that information about results of regulatory inspections should be disseminated more effectively and should be better integrated in the report and decision-making process.
Complementarity is also sought with various external quality evaluation mechanisms within the establishments. In order to respond to the specific challenges, or in order to fit within the framework of a strategy on quality development, the establishments are often committed to systems that complement HAS certification (certification of the service provided within a specific area, ISO 9001 certification of the sector or establishment, JACIE accreditation for haematopoietic stem cell transplantation activity, audit by the Biomedicines Agency on sample management, professional certification of specialised sectors, etc.). For these systems, HAS is implementing a policy of recognising the various systems in order to establish synergies with HAS certification, in order to enhance the dynamics of quality improvement and to avoid any unnecessary duplication between the various procedures.
Introduction
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 8/120 Manuel de certification – Édition novembre 2008
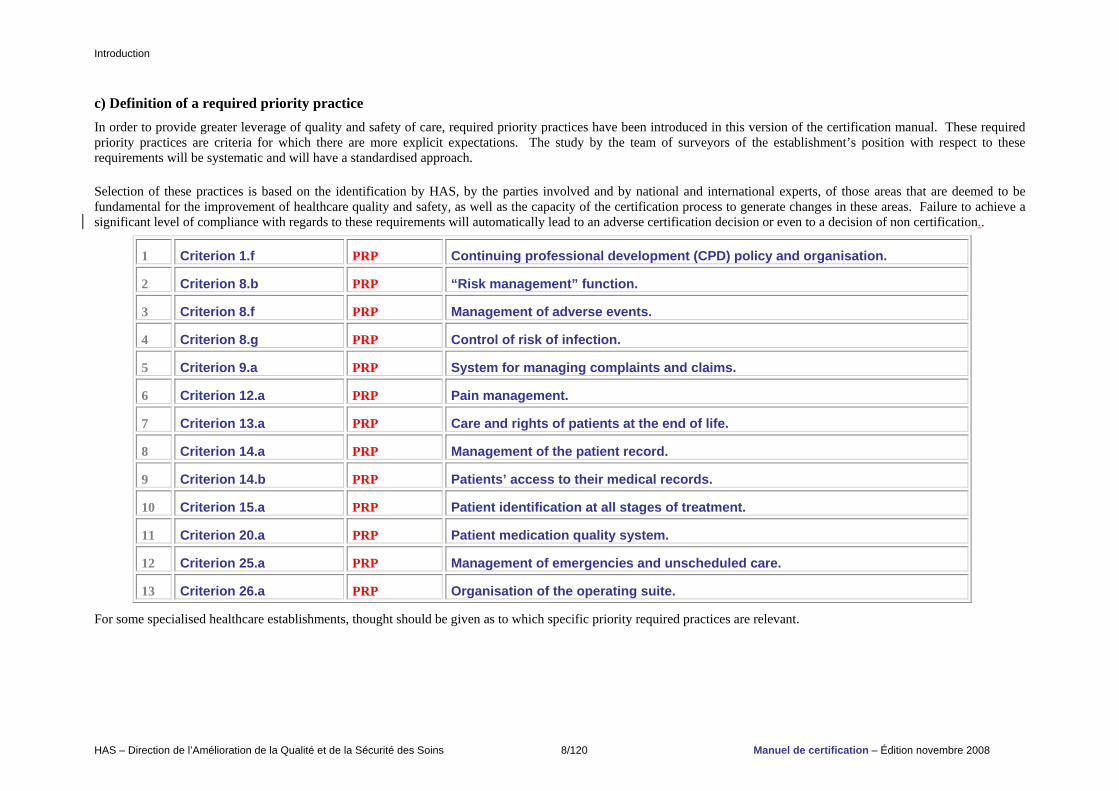
c) Definition of a required priority practice In order to provide greater leverage of quality and safety of care, required priority practices have been introduced in this version of the certification manual. These required priority practices are criteria for which there are more explicit expectations. The study by the team of surveyors of the establishment’s position with respect to these requirements will be systematic and will have a standardised approach. Selection of these practices is based on the identification by HAS, by the parties involved and by national and international experts, of those areas that are deemed to be fundamental for the improvement of healthcare quality and safety, as well as the capacity of the certification process to generate changes in these areas. Failure to achieve a significant level of compliance with regards to these requirements will automatically lead to an adverse certification decision or even to a decision of non certification..
1 Criterion 1.f PRP Continuing professional development (CPD) policy and organisation.
2 Criterion 8.b PRP “Risk management” function.
3 Criterion 8.f PRP Management of adverse events.
4 Criterion 8.g PRP Control of risk of infection.
5 Criterion 9.a PRP System for managing complaints and claims.
6 Criterion 12.a PRP Pain management.
7 Criterion 13.a PRP Care and rights of patients at the end of life.
8 Criterion 14.a PRP Management of the patient record.
9 Criterion 14.b PRP Patients’ access to their medical records.
10 Criterion 15.a PRP Patient identification at all stages of treatment.
11 Criterion 20.a PRP Patient medication quality system.
12 Criterion 25.a PRP Management of emergencies and unscheduled care.
13 Criterion 26.a PRP Organisation of the operating suite.
For some specialised healthcare establishments, thought should be given as to which specific priority required practices are relevant.
Introduction
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 9/120 Manuel de certification – Édition novembre 2008
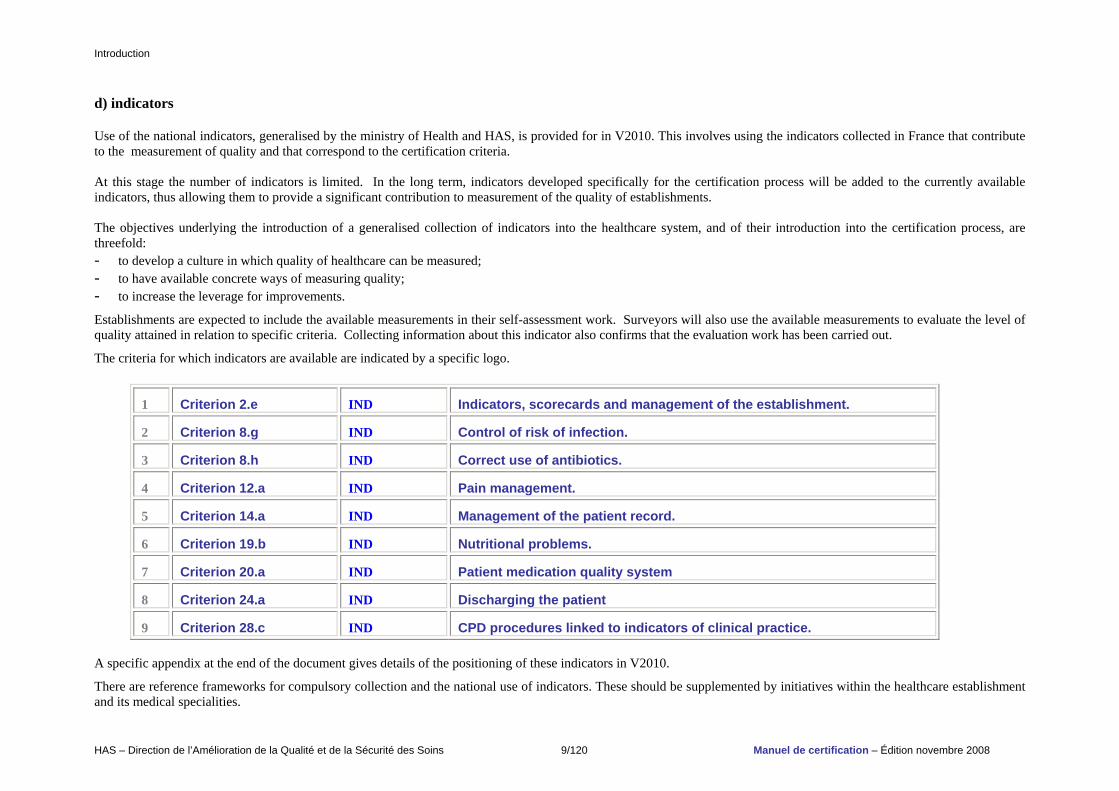
d) indicators Use of the national indicators, generalised by the ministry of Health and HAS, is provided for in V2010. This involves using the indicators collected in France that contribute to the measurement of quality and that correspond to the certification criteria. At this stage the number of indicators is limited. In the long term, indicators developed specifically for the certification process will be added to the currently available indicators, thus allowing them to provide a significant contribution to measurement of the quality of establishments. The objectives underlying the introduction of a generalised collection of indicators into the healthcare system, and of their introduction into the certification process, are threefold: - to develop a culture in which quality of healthcare can be measured; - to have available concrete ways of measuring quality; - to increase the leverage for improvements.
Establishments are expected to include the available measurements in their self-assessment work. Surveyors will also use the available measurements to evaluate the level of quality attained in relation to specific criteria. Collecting information about this indicator also confirms that the evaluation work has been carried out. The criteria for which indicators are available are indicated by a specific logo.
1 Criterion 2.e IND Indicators, scorecards and management of the establishment.
2 Criterion 8.g IND Control of risk of infection.
3 Criterion 8.h IND Correct use of antibiotics.
4 Criterion 12.a IND Pain management.
5 Criterion 14.a IND Management of the patient record.
6 Criterion 19.b IND Nutritional problems.
7 Criterion 20.a IND Patient medication quality system
8 Criterion 24.a IND Discharging the patient
9 Criterion 28.c IND CPD procedures linked to indicators of clinical practice. A specific appendix at the end of the document gives details of the positioning of these indicators in V2010.
There are reference frameworks for compulsory collection and the national use of indicators. These should be supplemented by initiatives within the healthcare establishment and its medical specialities.
Introduction
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 10/120 Manuel de certification – Édition novembre 2008
3 – The V2010 certification procedure The changes in the V2010 certification system are reflected not only in the manual but also in the certification procedure itself. The changes conceern all stages of the procedure and help to improve the efficiency of the certification process and to reduce formal constraints on establishments. Greater freedom is left to the establishment to organise the preparatory work for the self-assessment and the visit. However, the healthcare establishment is requested to continue to work in a multi-professional way and to ensure that all the parties involved participate, particularly users. Drafting of the self-assessment is simplified by using overall criterion-based wording, except for RPPs and the criteria whose field of application were subject to recommendations in the previous certification report. For the latter, self-evaluation for each evaluation element is still required. Self-evaluation of the “patient care process” part continues to be carried out for each type of care (medicine, surgery and obstetrics, mental health, rehabilitation, long-term care, home care). Rules relating to whether or not the criteria in the manual are applied, depending on the category to which the establishment belongs, are also specified. The certification visit itself focuses on the essential points: RPPs, the follow-up on V2 recommendations, the areas for which indicators are available, criteria graded C or D by establishment in its self-assessment and the criteria relative to CPD. The visit also includes some criteria that are randomly selected. Giving up the idea of an exhaustive study of all criteria during the visit enables a focus on the essential subjects. The decision-making process is also reviewed. Items for evaluating the criteria are assessed using a number of points based on their level of compliance. The number of points accumulated for each criterion enables a grade of A, B, C or D to be awarded. The decision-making process concerns the areas graded C or D under the new rules. In order to better respond to situations of clear breaches on essential points, certification may be refused without a prior conditional certification step. A new structure of the report will be drawn up. This will aim to provide a more readable report. One single report will enable a better response to the requirements of various target groups. It will, in particular, include descriptions and diagrams created with a view to having the certification results widely distributed and made accessible to the public.
Introduction
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 11/120 Manuel de certification – Édition novembre 2008
4 – Prospects for changes to the certification process In addition to the setting up of V2010 and following the example of accreditation systems in other countries, the certification process must continue to change, with the aim of increasing efficiency and suitability to the requirements of establishments and of the healthcare system. To this end, HAS has issued three recommendations: - implementation of an ongoing development system for the certification process. This will include planned development of reference frameworks and criteria, sustained by
monitoring of the various areas, feedback from use of the manual and results of the measurements of the impact of the certification process. It also covers adaptation of the system to various types of establishment and management.
- the ongoing progressive increase in the use of indicators in the certification process, based on identifying priority fields requiring development and a progressive
introduction of indicators. The number of indicators must remain limited, for reasons of feasibility and efficiency. - the setting-up of impact measurements: the aim of the certification process is to lead to positive changes in the operation of establishments and in the quality and safety of
the healthcare they provide. In order to manage the certification process and to ensure that its action is visible to and understandable by the parties involved, HAS has developed a system to measure its impact. Its implementation involves identifying and selecting relevant items for measuring the process, organising of the measurement process and monitoring it in a timely manner.
The HAS provides an e-mail address for readers and users of the manual who would like to make comments or suggestions about the certification manual.
Sommaire
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 12/120 Manuel de certification – Édition novembre 2008
TABLE OF CONTENTS Preface 3 Introduction 4 Table of contents 12
CCHHAAPPTTEERR 11 MMAANNAAGGEEMMEENNTT OOFF TTHHEE EESSTTAABBLLIISSHHMMEENNTT.. 1177
PART 1. STRATEGIC MANAGEMENT. 18 STANDARD 1 THE STRATEGY OF THE ESTABLISHMENT. 18 Criterion 1.a Values, missions and strategy of the establishment. 18 Criterion 1.b Commitment to sustainable development. 19 Criterion 1.c Ethical approach. 20 Criterion 1.d Patient rights policy. 21 Criterion 1.e Policy for improving healthcare quality and safety. 21 Criterion 1.f Continuing professional development (CPD) policy and organisation. RRPPPP 22 Criterion 1.g Developing a culture of quality and safety. 23 STANDARD 2 ORGANISATION AND PROCEDURES FOR INTERNAL MANAGEMENT. 23 Criterion 2.a Management and supervision of areas of activity. 23 Criterion 2.b Involvement of users, their representatives and associations. 24 Criterion 2.c How the authorities operate. 24 Criterion 2.d Dialogue between employers and trade unions and staff involvement. 24 Criterion 2.e Indicators, scorecards and management of the establishment. IINNDD 26
PART 2. RESOURCE MANAGEMENT. 28 STANDARD 3 HUMAN RESOURCES MANAGEMENT. 28 Criterion 3.a Management of jobs and skills. 28 Criterion 3.b Integrating new arrivals. 28 Criterion 3.c Occupational health and safety. 29 Criterion 3.d Quality of life at work. 29
Sommaire
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 13/120 Manuel de certification – Édition novembre 2008
STANDARD 4 FINANCIAL RESOURCE MANAGEMENT. 30 Criterion 4.a Budget management. 30 Criterion 4.b Improving efficiency. 30 STANDARD 5 INFORMATION SYSTEM. 31 Criterion 5.a Information system. 31 Criterion 5.b Security of the information system. 31 Criterion 5.c Document management. 31 STANDARD 6 MANAGEMENT OF LOGISTICS AND INFRASTRUCTURE. 33 Criterion 6.a Safety of belongings and individuals. 33 Criterion 6.b Management of infrastructure and equipment (excluding medical devices). 33 Criterion 6.c Quality of catering. 34 Criterion 6.d Laundry management. 34 Criterion 6.e Patient transportation. 35 Criterion 6.f Eco-friendly purchasing and supplies. 35 STANDARD 7 QUALITY AND SECURITY OF THE ENVIRONMENT. 36 Criterion 7.a Water management. 36 Criterion 7.b Air management. 36 Criterion 7.c Energy management. 38 Criterion 7.d Hygiene of premises. 38 Criterion 7.e Waste Management. 39
PART 3 MANAGEMENT OF QUALITY AND SAFETY OF HEALTHCARE. 40 STANDARD 8 GLOBAL AND COORDINATED QUALITY AND RISK MANAGEMENT PROGRAMME. 40 Criterion 8.a Programme for improving healthcare quality and safety. 40 Criterion 8.b “Risk management” function. RRPPPP 40 Criterion 8.c Legal and regulatory obligations. 41 Criterion 8.d A priori risk evaluation. 41 Criterion 8.e Crisis management. 43 Criterion 8.f Management of adverse events. RRPPPP 43 Criterion 8.g Control of risk of infection. RRPPPP IINNDD 45 Criterion 8.h Correct use of antibiotics. IINNDD 46 Criterion 8.i Health alerts and monitoring. 47 Criterion 8.j Control of transfusion risks. 47 Criterion 8.k Management of biomedical equipment. 48
Sommaire
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 14/120 Manuel de certification – Édition novembre 2008
STANDARD 9 MANAGING COMPLAINTS AND THE EVALUATION OF USER SATISFACTION. 49 Criterion 9.a System for managing complaints and claims. RRPPPP 49 Criterion 9.b Evaluation of user satisfaction. 49
CCHHAAPPTTEERR 22 PPAATTIIEENNTT MMAANNAAGGEEMMEENNTT.. 5500
PART 1 RIGHTS AND POSITION OF PATIENTS. 51 STANDARD 10 POSITIVE TREATMENT AND RIGHTS. 51 Criterion 10.a Preventing abuse and promoting positive treatment. 51 Criterion 10.b Respect for patient dignity and privacy. 51 Criterion 10.c Respect for the confidentiality of patient information. 53 Criterion 10.d Reception and support for the patient’s entourage. 53 Criterion 10.e Management of measures for restricting freedom. 54 STANDARD 11 PATIENT INFORMATION, PARTICIPATION AND CONSENT. 55 Criterion 11.a Patient information about state of health and proposed care plan. 55 Criterion 11.b Patient consent and participation. 57 Criterion 11.c Patient information in the case of physical injury related to treatment. 57 STANDARD 12 PAIN MANAGEMENT 59 Criterion 12.a Pain management. RRPPPP IINNDD 59 STANDARD 13 END OF LIFE. 60 Criterion 13.a Care for and rights of patients at the end of life. RRPPPP 60
PART 2. MANAGEMENT OF PATIENT DATA. 62 STANDARD 14 THE PATIENT RECORD 62 Criterion 14.a Management of the patient record. RRPPPP IINNDD 62 Criterion 14.b Patients’ access to their medical record. RPPPP 62 STANDARD 15 PATIENT IDENTIFICATION. 64 Criterion 15.a Patient identification at all stages of treatment. RRPPPP 64
Sommaire
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 15/120 Manuel de certification – Édition novembre 2008
PART 3 PATIENT CARE PATHWAY. 65 STANDARD 16 PATIENT ADMISSION. 65 Criterion 16.a Patient admission system. 65 STANDARD 17 EVALUATION OF THE PATIENT’S STATE OF HEALTH AND THE PERSONALISED CARE PLAN. 65 Criterion 17.a Initial and ongoing evaluation of the patient’s state of health and personalised care plan. 65 STANDARD 18 CONTINUITY AND CO-ORDINATION OF CARE. 67 Criterion 18.a Continuity and coordination of patient care. 67 Criterion 18.b Management of life-threatening emergencies occurring within the establishment. 67 STANDARD 19 SPECIAL CARE. 69 Criterion 19.a Population groups requiring special care. 69 Criterion 19.b Nutritional problems. IINNDD 70 Criterion 19.c Suicide risk. 70 Criterion 19.d Enforced hospitalisation. 71 STANDARD 20 TREATMENT USING MEDICATION. 72 Criterion 20.a Patient medication quality system. RRPPPP IINNDD 72 Criterion 20.b Prescribing drugs for the elderly. 74 STANDARD 21 MANAGEMENT OF LABORATORY TESTS. 74 Criterion 21.a Requesting tests, sample mangement and transmission of results. 74 Criterion 21.b Quality procedures in the laboratory. 75 STANDARD 22 MANAGEMENT OF IMAGING INVESTIGATIONS. 75 Criterion 22.a Requesting tests and transmitting results. 75 Criterion 22.b Approach to quality in the imaging department. 77 STANDARD 23 THERAPEUTIC EDUCATION FOR PATIENTS AND THEIR FAMILIES. 77 Criterion 23.a Therapeutic patient education. 77 STANDARD 24 DISCHARGING THE PATIENT. 78 Criterion 24.a Discharging the patient. IINNDD 78
Sommaire
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 16/120 Manuel de certification – Édition novembre 2008
PART 4 SPECIFIC TYPES OF MANAGEMENT 79 STANDARD 25 PATIENT MANAGEMENT IN THE EMERGENCY DEPARTMENT 79 Criterion 25a Management of emergencies and unscheduled care RRPPPP 79 STANDARD 26 THE FUNCTIONING OF INTERVENTIONAL SECTORS 79 Criterion 26.a Organisation of the operating suite RRPPPP 79 Criterion 26.b Organisation of other high-risk sectors 81 Criterion 26.c Organ and tissue donation for therapeutic purposes 82 STANDARD 27 FOLLOW-UP AND REHABILITATION CARE ACTIVITIES 82 Criterion 27.a Follow-up and rehabilitation care activities 82
PART 5 CONTINUING PROFESSIONAL DEVELOPMENT 84 STANDARD 28 CONTINUING PROFESSIONAL DEVELOPMENT 84 Criterion 28.a Implementation of continuing professional development (CPD) initiatives 84 Criterion 28.b Appropriateness of care 85 Criterion 28.c CPD initiatives associated with clinical practice indicators IINNDD 86 Abbreviations and acronyms used 87 Glossary 88 APPENDIX: Generalised indicators and V2010 certification 95 Acknowledgements 99
Chapitre 1 Management de l’établissement.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 17/120 Manuel de certification – Édition novembre 2008
CCHHAAPPTTEERR 11 MMaannaaggeemmeenntt ooff tthhee eessttaabblliisshhmmeenntt..
Chapitre 1 Management de l’établissement. Partie 1 Management stratégique.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 18/120 Manuel de certification – Édition novembre 2008
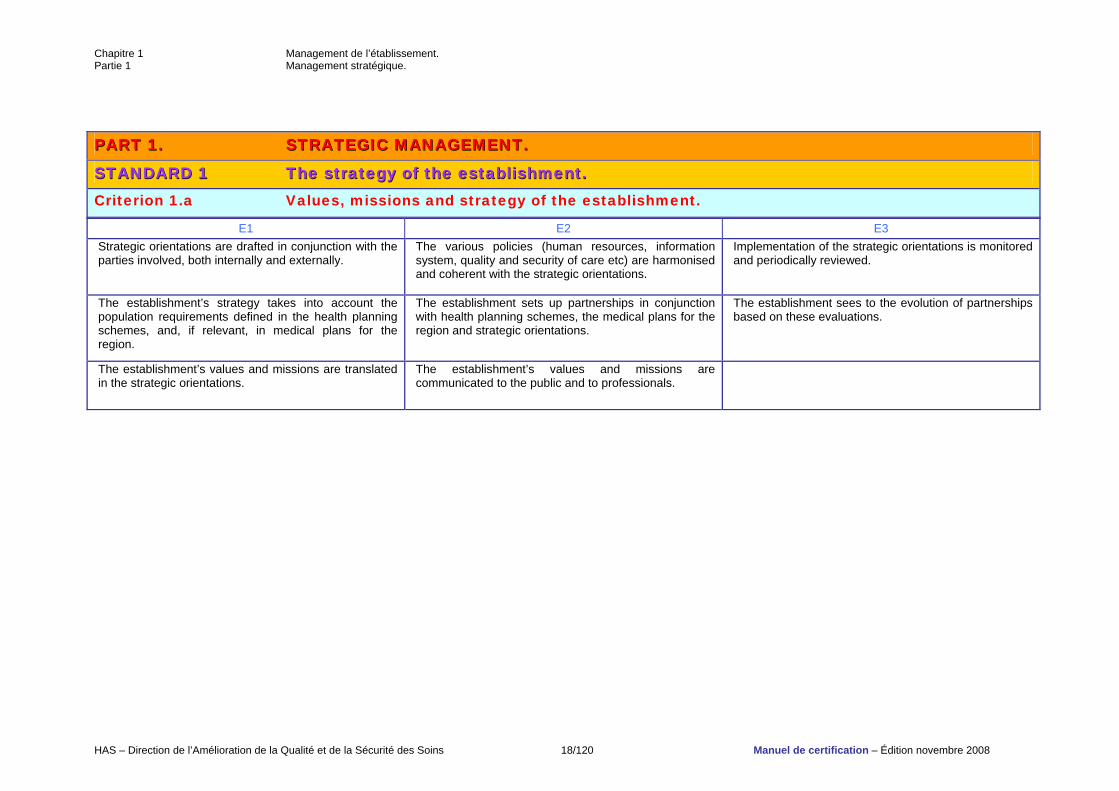
PPAARRTT 11.. SSTTRRAATTEEGGIICC MMAANNAAGGEEMMEENNTT..
SSTTAANNDDAARRDD 11 TThhee ssttrraatteeggyy ooff tthhee eessttaabblliisshhmmeenntt.. Criterion 1.a Values, missions and strategy of the establishment.
E1 E2 E3 Strategic orientations are drafted in conjunction with the parties involved, both internally and externally.
The various policies (human resources, information system, quality and security of care etc) are harmonised and coherent with the strategic orientations.
Implementation of the strategic orientations is monitored and periodically reviewed.
The establishment’s strategy takes into account the population requirements defined in the health planning schemes, and, if relevant, in medical plans for the region.
The establishment sets up partnerships in conjunction with health planning schemes, the medical plans for the region and strategic orientations.
The establishment sees to the evolution of partnerships based on these evaluations.
The establishment’s values and missions are translated in the strategic orientations.
The establishment’s values and missions are communicated to the public and to professionals.

Chapitre 1 Management de l’établissement. Partie 1 Management stratégique.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 19/120 Manuel de certification – Édition novembre 2008
Criterion 1.b Commitment to sustainable development. Sustainable development is generally defined as “meeting the needs of present generations without compromising the ability of future generations to meet their own needs” (Brundtland commission report). Sustainable development is a global and long-term goal and brings together 3 areas: - reliable economic management; - a socially integrated establishment; - an ecologically respectful healthcare establishment. In short: - the values, missions and activities of a healthcare establishment must incorporate the challenges of sustainable development and in particular the notions of
social and environmental responsibility; - initiatives for continuous quality improvement must take into account the perspective of continuity and sustainability; risk management must be broadened to include environmental risks. Several principles of management focused on sustainable development are included in the certification process (taking into account the parties involved, a participative approach, consideration of the quality, security, environmental and human resource management dimensions). The aim of V2010 is to encourage establishments to promote sustainable development in their strategic planning and in their management.
E1 E2 E3 A sustainable development plan has been established by the establishment.
The sustainable development strategy is broken down into a multi-annual programme.
The multi-annual programme is regularly monitored and readjusted.
A sustainable development section is included in the strategic orientations.
The staff’s awareness of sustainable development is raised and they are informed of the establishment’s aims.
The establishment communicates its sustainable development objectives to local social, cultural and economic players.
Sustainable development is taken into account in the case of construction or refurbishment projects.
Chapitre 1 Management de l’établissement. Partie 1 Management stratégique.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 20/120 Manuel de certification – Édition novembre 2008
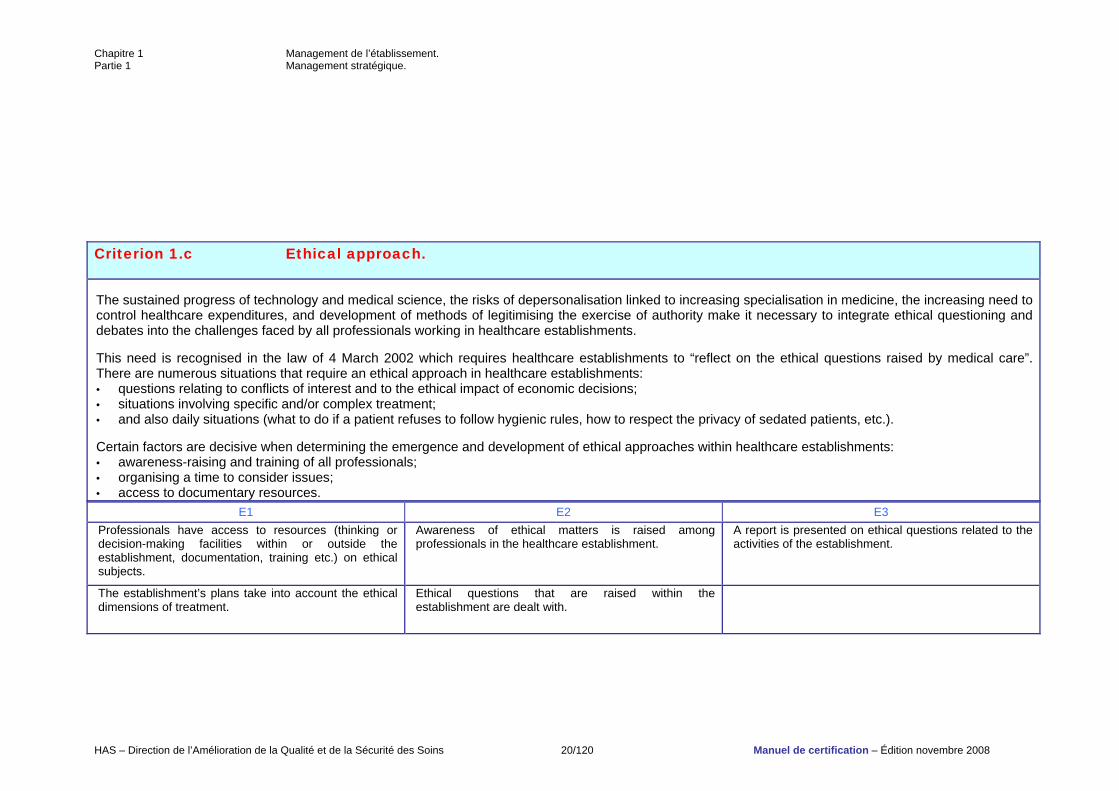
Criterion 1.c Ethical approach. The sustained progress of technology and medical science, the risks of depersonalisation linked to increasing specialisation in medicine, the increasing need to control healthcare expenditures, and development of methods of legitimising the exercise of authority make it necessary to integrate ethical questioning and debates into the challenges faced by all professionals working in healthcare establishments. This need is recognised in the law of 4 March 2002 which requires healthcare establishments to “reflect on the ethical questions raised by medical care”. There are numerous situations that require an ethical approach in healthcare establishments: • questions relating to conflicts of interest and to the ethical impact of economic decisions; • situations involving specific and/or complex treatment; • and also daily situations (what to do if a patient refuses to follow hygienic rules, how to respect the privacy of sedated patients, etc.). Certain factors are decisive when determining the emergence and development of ethical approaches within healthcare establishments: • awareness-raising and training of all professionals; • organising a time to consider issues; • access to documentary resources.
E1 E2 E3 Professionals have access to resources (thinking or decision-making facilities within or outside the establishment, documentation, training etc.) on ethical subjects.
Awareness of ethical matters is raised among professionals in the healthcare establishment.
A report is presented on ethical questions related to the activities of the establishment.
The establishment’s plans take into account the ethical dimensions of treatment.
Ethical questions that are raised within the establishment are dealt with.
Chapitre 1 Management de l’établissement. Partie 1 Management stratégique.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 21/120 Manuel de certification – Édition novembre 2008
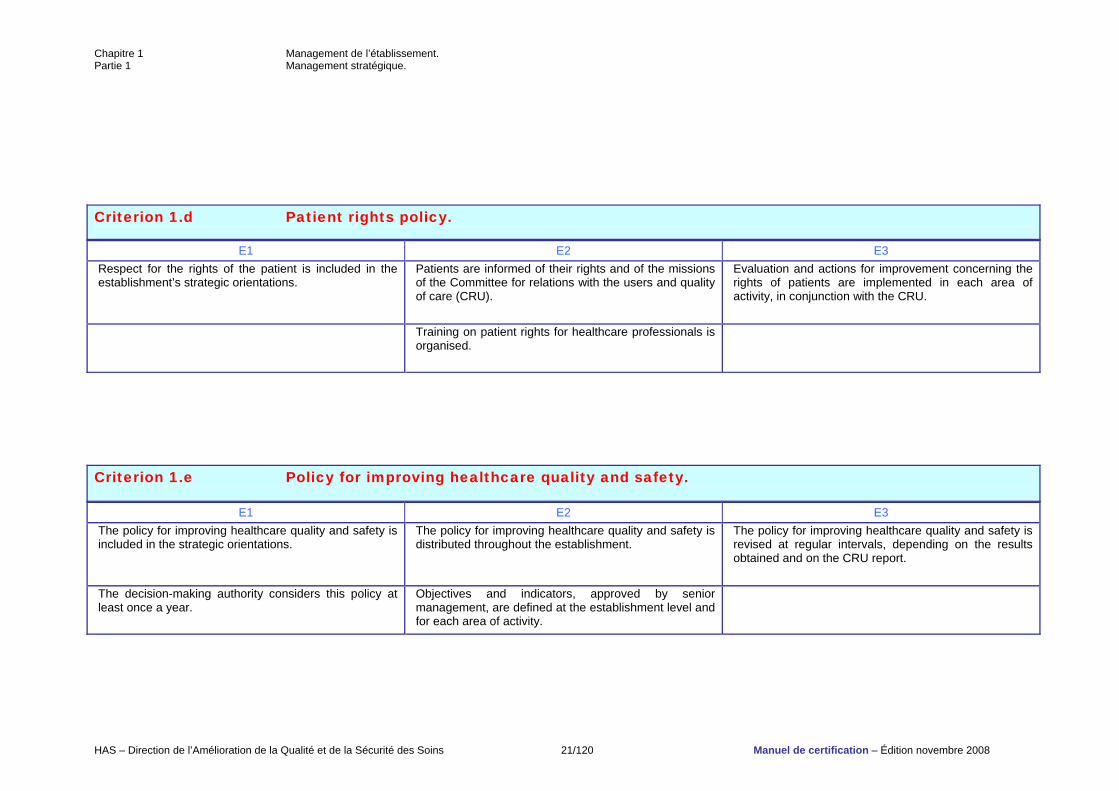
Criterion 1.d Patient rights policy.
E1 E2 E3 Respect for the rights of the patient is included in the establishment’s strategic orientations.
Patients are informed of their rights and of the missions of the Committee for relations with the users and quality of care (CRU).
Evaluation and actions for improvement concerning the rights of patients are implemented in each area of activity, in conjunction with the CRU.
Training on patient rights for healthcare professionals is organised.
Criterion 1.e Policy for improving healthcare quality and safety.
E1 E2 E3 The policy for improving healthcare quality and safety is included in the strategic orientations.
The policy for improving healthcare quality and safety is distributed throughout the establishment.
The policy for improving healthcare quality and safety is revised at regular intervals, depending on the results obtained and on the CRU report.
The decision-making authority considers this policy at least once a year.
Objectives and indicators, approved by senior management, are defined at the establishment level and for each area of activity.
Chapitre 1 Management de l’établissement. Partie 1 Management stratégique.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 22/120 Manuel de certification – Édition novembre 2008
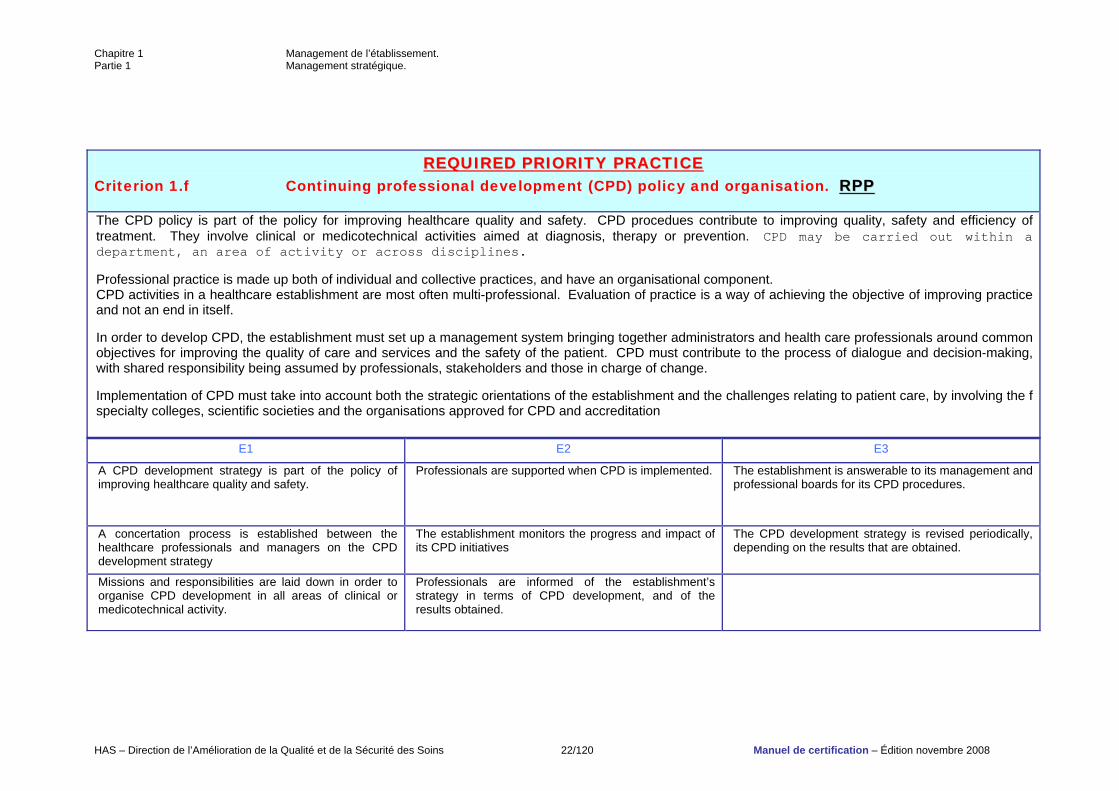
RREEQQUUIIRREEDD PPRRIIOORRIITTYY PPRRAACCTTIICCEE Criterion 1.f Continuing professional development (CPD) policy and organisation. RRPPPP The CPD policy is part of the policy for improving healthcare quality and safety. CPD procedues contribute to improving quality, safety and efficiency of treatment. They involve clinical or medicotechnical activities aimed at diagnosis, therapy or prevention. CPD may be carried out within a department, an area of activity or across disciplines. Professional practice is made up both of individual and collective practices, and have an organisational component. CPD activities in a healthcare establishment are most often multi-professional. Evaluation of practice is a way of achieving the objective of improving practice and not an end in itself. In order to develop CPD, the establishment must set up a management system bringing together administrators and health care professionals around common objectives for improving the quality of care and services and the safety of the patient. CPD must contribute to the process of dialogue and decision-making, with shared responsibility being assumed by professionals, stakeholders and those in charge of change. Implementation of CPD must take into account both the strategic orientations of the establishment and the challenges relating to patient care, by involving the f specialty colleges, scientific societies and the organisations approved for CPD and accreditation
E1 E2 E3
A CPD development strategy is part of the policy of improving healthcare quality and safety.
Professionals are supported when CPD is implemented. The establishment is answerable to its management and professional boards for its CPD procedures.
A concertation process is established between the healthcare professionals and managers on the CPD development strategy
The establishment monitors the progress and impact of its CPD initiatives
The CPD development strategy is revised periodically, depending on the results that are obtained.
Missions and responsibilities are laid down in order to organise CPD development in all areas of clinical or medicotechnical activity.
Professionals are informed of the establishment’s strategy in terms of CPD development, and of the results obtained.
Chapitre 1 Management de l’établissement. Partie 1 Management stratégique.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 23/120 Manuel de certification – Édition novembre 2008
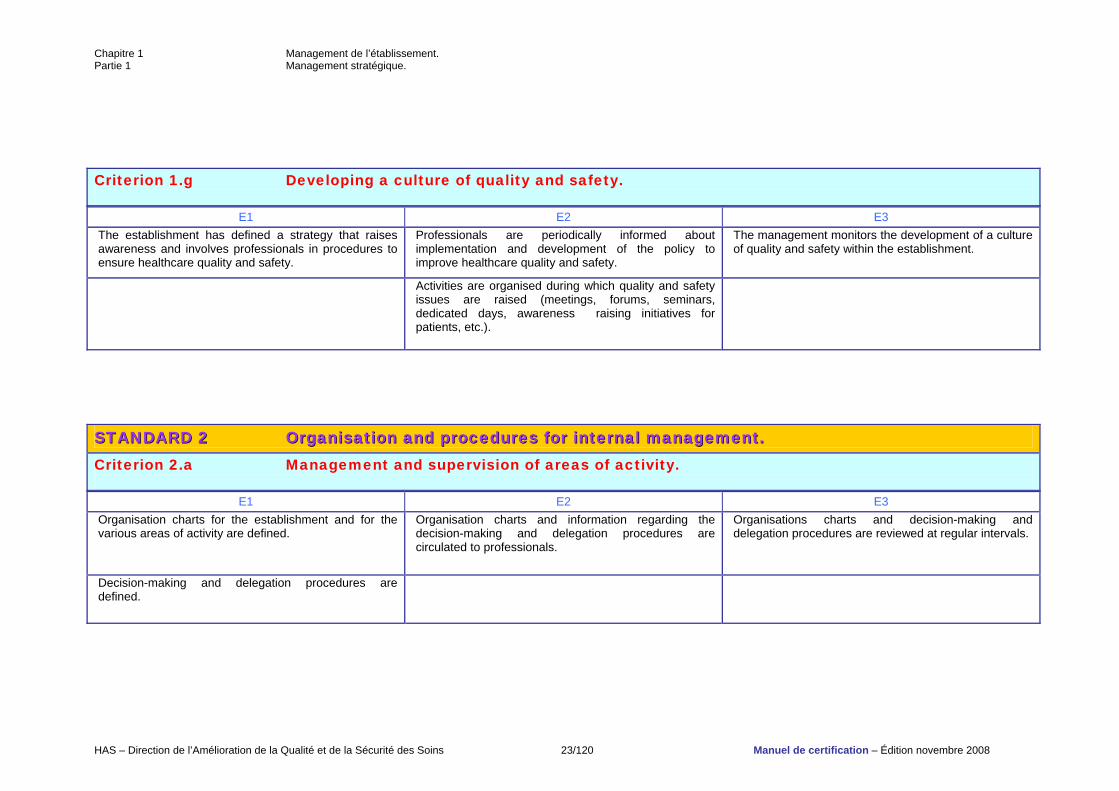
Criterion 1.g Developing a culture of quality and safety.
E1 E2 E3 The establishment has defined a strategy that raises awareness and involves professionals in procedures to ensure healthcare quality and safety.
Professionals are periodically informed about implementation and development of the policy to improve healthcare quality and safety.
The management monitors the development of a culture of quality and safety within the establishment.
Activities are organised during which quality and safety issues are raised (meetings, forums, seminars, dedicated days, awareness raising initiatives for patients, etc.).
SSTTAANNDDAARRDD 22 OOrrggaanniissaattiioonn aanndd pprroocceedduurreess ffoorr iinntteerrnnaall mmaannaaggeemmeenntt.. Criterion 2.a Management and supervision of areas of activity.
E1 E2 E3 Organisation charts for the establishment and for the various areas of activity are defined.
Organisation charts and information regarding the decision-making and delegation procedures are circulated to professionals.
Organisations charts and decision-making and delegation procedures are reviewed at regular intervals.
Decision-making and delegation procedures are defined.
Chapitre 1 Management de l’établissement. Partie 1 Management stratégique.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 24/120 Manuel de certification – Édition novembre 2008
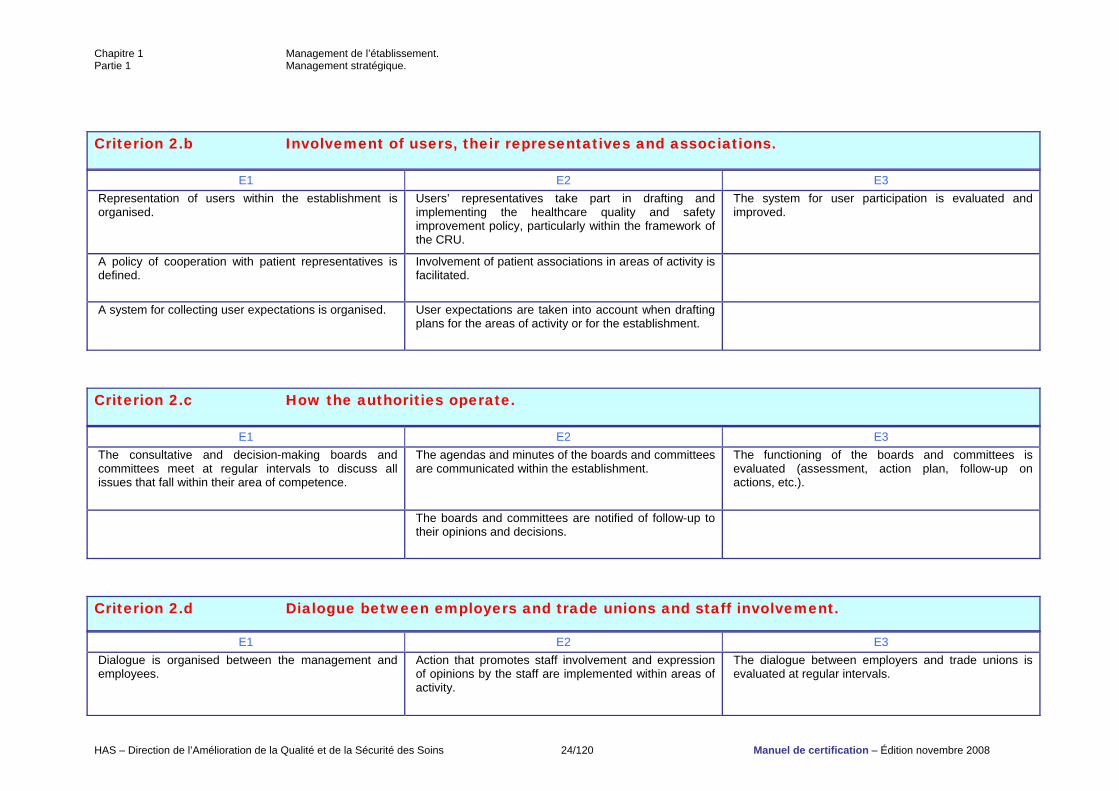
Criterion 2.b Involvement of users, their representatives and associations.
E1 E2 E3 Representation of users within the establishment is organised.
Users’ representatives take part in drafting and implementing the healthcare quality and safety improvement policy, particularly within the framework of the CRU.
The system for user participation is evaluated and improved.
A policy of cooperation with patient representatives is defined.
Involvement of patient associations in areas of activity is facilitated.
A system for collecting user expectations is organised. User expectations are taken into account when drafting plans for the areas of activity or for the establishment.
Criterion 2.c How the authorities operate.
E1 E2 E3 The consultative and decision-making boards and committees meet at regular intervals to discuss all issues that fall within their area of competence.
The agendas and minutes of the boards and committees are communicated within the establishment.
The functioning of the boards and committees is evaluated (assessment, action plan, follow-up on actions, etc.).
The boards and committees are notified of follow-up to their opinions and decisions.
Criterion 2.d Dialogue between employers and trade unions and staff involvement.
E1 E2 E3 Dialogue is organised between the management and employees.
Action that promotes staff involvement and expression of opinions by the staff are implemented within areas of activity.
The dialogue between employers and trade unions is evaluated at regular intervals.
Chapitre 1 Management de l’établissement. Partie 1 Management stratégique.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 25/120 Manuel de certification – Édition novembre 2008
Chapitre 1 Management de l’établissement. Partie 1 Management stratégique.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 26/120 Manuel de certification – Édition novembre 2008
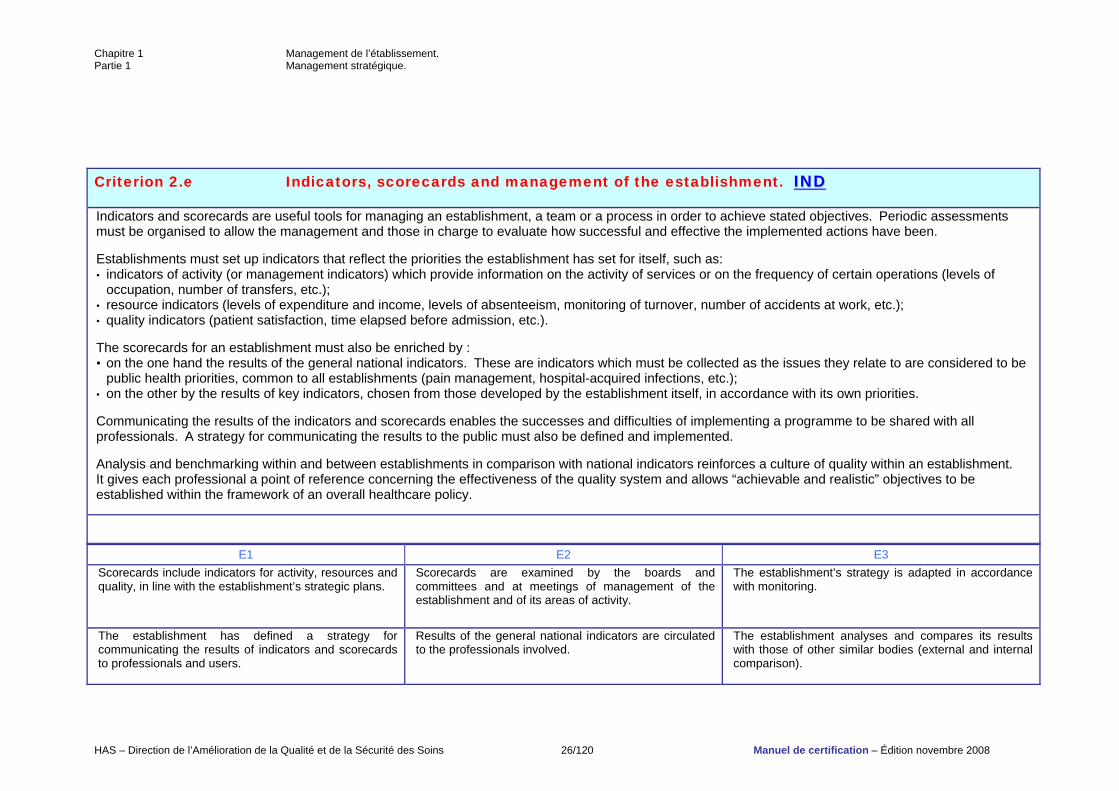
Criterion 2.e Indicators, scorecards and management of the establishment. IINNDD Indicators and scorecards are useful tools for managing an establishment, a team or a process in order to achieve stated objectives. Periodic assessments must be organised to allow the management and those in charge to evaluate how successful and effective the implemented actions have been. Establishments must set up indicators that reflect the priorities the establishment has set for itself, such as: • indicators of activity (or management indicators) which provide information on the activity of services or on the frequency of certain operations (levels of
occupation, number of transfers, etc.); • resource indicators (levels of expenditure and income, levels of absenteeism, monitoring of turnover, number of accidents at work, etc.); • quality indicators (patient satisfaction, time elapsed before admission, etc.). The scorecards for an establishment must also be enriched by : • on the one hand the results of the general national indicators. These are indicators which must be collected as the issues they relate to are considered to be
public health priorities, common to all establishments (pain management, hospital-acquired infections, etc.); • on the other by the results of key indicators, chosen from those developed by the establishment itself, in accordance with its own priorities. Communicating the results of the indicators and scorecards enables the successes and difficulties of implementing a programme to be shared with all professionals. A strategy for communicating the results to the public must also be defined and implemented. Analysis and benchmarking within and between establishments in comparison with national indicators reinforces a culture of quality within an establishment. It gives each professional a point of reference concerning the effectiveness of the quality system and allows “achievable and realistic” objectives to be established within the framework of an overall healthcare policy.
E1 E2 E3 Scorecards include indicators for activity, resources and quality, in line with the establishment’s strategic plans.
Scorecards are examined by the boards and committees and at meetings of management of the establishment and of its areas of activity.
The establishment’s strategy is adapted in accordance with monitoring.
The establishment has defined a strategy for communicating the results of indicators and scorecards to professionals and users.
Results of the general national indicators are circulated to the professionals involved.
The establishment analyses and compares its results with those of other similar bodies (external and internal comparison).
Chapitre 1 Management de l’établissement. Partie 1 Management stratégique.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 27/120 Manuel de certification – Édition novembre 2008
Chapitre 1 Management de l’établissement. Partie 2 Management des ressources.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 28/120 Manuel de certification – Édition novembre 2008
PPAARRTT 22.. RREESSOOUURRCCEE MMAANNAAGGEEMMEENNTT..
SSTTAANNDDAARRDD 33 HHuummaann rreessoouurrcceess mmaannaaggeemmeenntt..
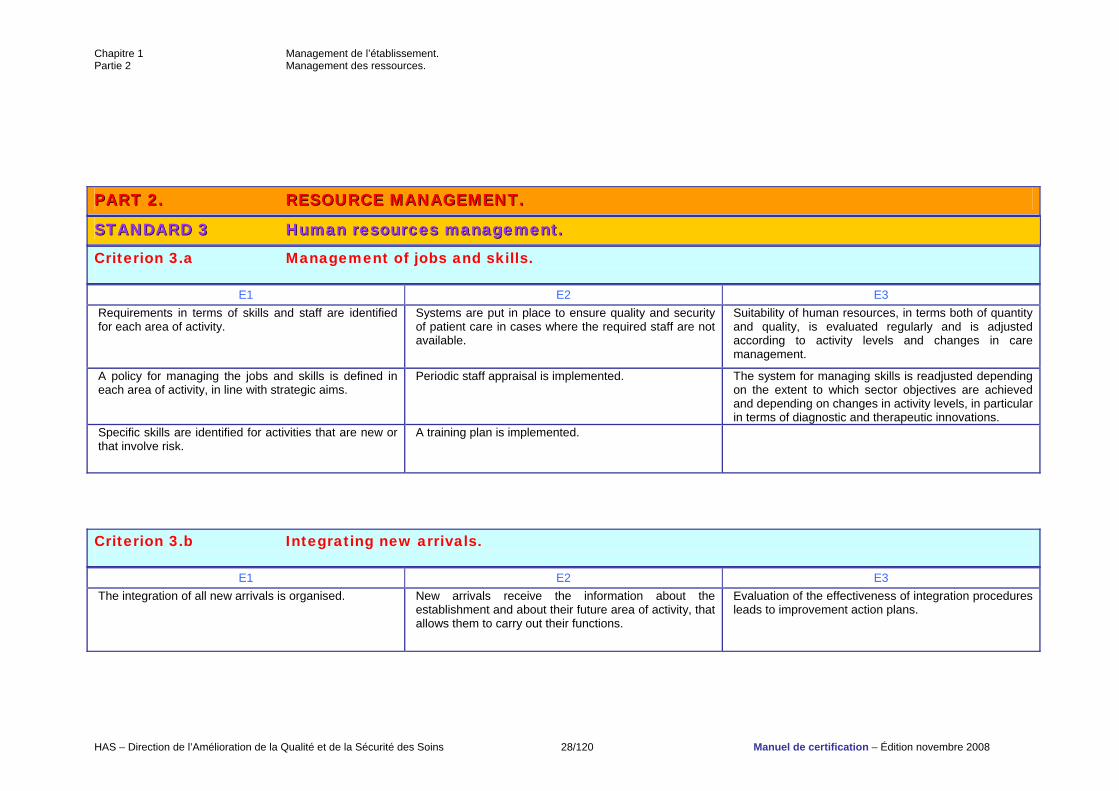
Criterion 3.a Management of jobs and skills.
E1 E2 E3 Requirements in terms of skills and staff are identified for each area of activity.
Systems are put in place to ensure quality and security of patient care in cases where the required staff are not available.
Suitability of human resources, in terms both of quantity and quality, is evaluated regularly and is adjusted according to activity levels and changes in care management.
A policy for managing the jobs and skills is defined in each area of activity, in line with strategic aims.
Periodic staff appraisal is implemented. The system for managing skills is readjusted depending on the extent to which sector objectives are achieved and depending on changes in activity levels, in particular in terms of diagnostic and therapeutic innovations.
Specific skills are identified for activities that are new or that involve risk.
A training plan is implemented.
Criterion 3.b Integrating new arrivals.
E1 E2 E3 The integration of all new arrivals is organised. New arrivals receive the information about the
establishment and about their future area of activity, that allows them to carry out their functions.
Evaluation of the effectiveness of integration procedures leads to improvement action plans.
Chapitre 1 Management de l’établissement. Partie 2 Management des ressources.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 29/120 Manuel de certification – Édition novembre 2008
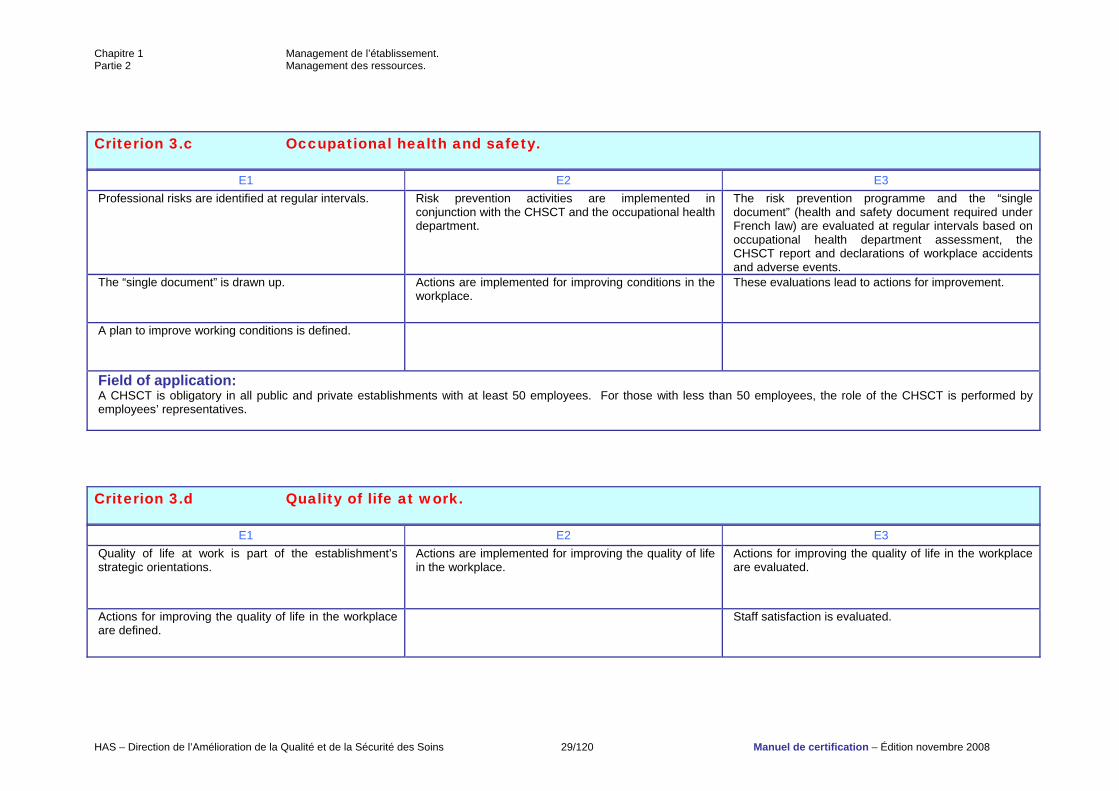
Criterion 3.c Occupational health and safety.
E1 E2 E3 Professional risks are identified at regular intervals. Risk prevention activities are implemented in
conjunction with the CHSCT and the occupational health department.
The risk prevention programme and the “single document” (health and safety document required under French law) are evaluated at regular intervals based on occupational health department assessment, the CHSCT report and declarations of workplace accidents and adverse events.
The “single document” is drawn up. Actions are implemented for improving conditions in the workplace.
These evaluations lead to actions for improvement.
A plan to improve working conditions is defined.
Field of application: A CHSCT is obligatory in all public and private establishments with at least 50 employees. For those with less than 50 employees, the role of the CHSCT is performed by employees’ representatives.
Criterion 3.d Quality of life at work.
E1 E2 E3 Quality of life at work is part of the establishment’s strategic orientations.
Actions are implemented for improving the quality of life in the workplace.
Actions for improving the quality of life in the workplace are evaluated.
Actions for improving the quality of life in the workplace are defined.
Staff satisfaction is evaluated.
Chapitre 1 Management de l’établissement. Partie 2 Management des ressources.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 30/120 Manuel de certification – Édition novembre 2008
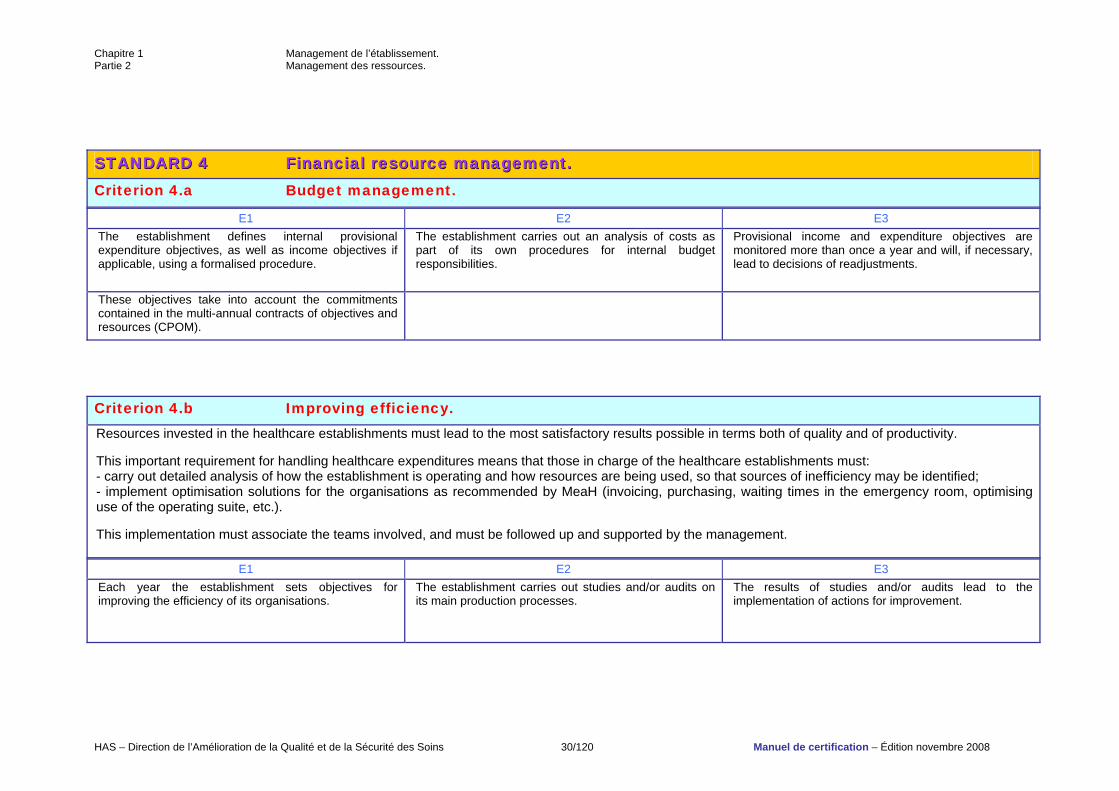
SSTTAANNDDAARRDD 44 FFiinnaanncciiaall rreessoouurrccee mmaannaaggeemmeenntt.. Criterion 4.a Budget management.
E1 E2 E3 The establishment defines internal provisional expenditure objectives, as well as income objectives if applicable, using a formalised procedure.
The establishment carries out an analysis of costs as part of its own procedures for internal budget responsibilities.
Provisional income and expenditure objectives are monitored more than once a year and will, if necessary, lead to decisions of readjustments.
These objectives take into account the commitments contained in the multi-annual contracts of objectives and resources (CPOM).
Criterion 4.b Improving efficiency. Resources invested in the healthcare establishments must lead to the most satisfactory results possible in terms both of quality and of productivity. This important requirement for handling healthcare expenditures means that those in charge of the healthcare establishments must: - carry out detailed analysis of how the establishment is operating and how resources are being used, so that sources of inefficiency may be identified; - implement optimisation solutions for the organisations as recommended by MeaH (invoicing, purchasing, waiting times in the emergency room, optimising use of the operating suite, etc.). This implementation must associate the teams involved, and must be followed up and supported by the management.
E1 E2 E3 Each year the establishment sets objectives for improving the efficiency of its organisations.
The establishment carries out studies and/or audits on its main production processes.
The results of studies and/or audits lead to the implementation of actions for improvement.
Chapitre 1 Management de l’établissement. Partie 2 Management des ressources.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 31/120 Manuel de certification – Édition novembre 2008
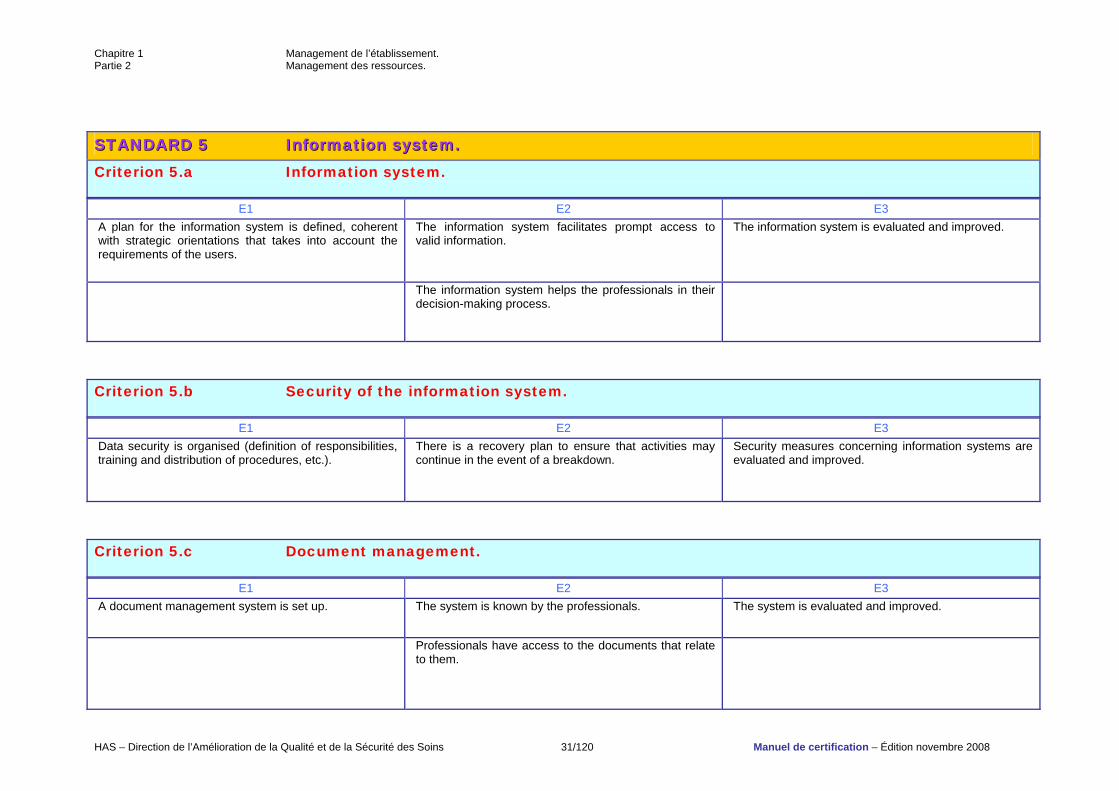
SSTTAANNDDAARRDD 55 IInnffoorrmmaattiioonn ssyysstteemm.. Criterion 5.a Information system.
E1 E2 E3 A plan for the information system is defined, coherent with strategic orientations that takes into account the requirements of the users.
The information system facilitates prompt access to valid information.
The information system is evaluated and improved.
The information system helps the professionals in their decision-making process.
Criterion 5.b Security of the information system.
E1 E2 E3 Data security is organised (definition of responsibilities, training and distribution of procedures, etc.).
There is a recovery plan to ensure that activities may continue in the event of a breakdown.
Security measures concerning information systems are evaluated and improved.
Criterion 5.c Document management.
E1 E2 E3 A document management system is set up. The system is known by the professionals. The system is evaluated and improved.
Professionals have access to the documents that relate to them.
Chapitre 1 Management de l’établissement. Partie 2 Management des ressources.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 32/120 Manuel de certification – Édition novembre 2008
There is a functional system for updating the documents.
Chapitre 1 Management de l’établissement. Partie 2 Management des ressources.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 33/120 Manuel de certification – Édition novembre 2008
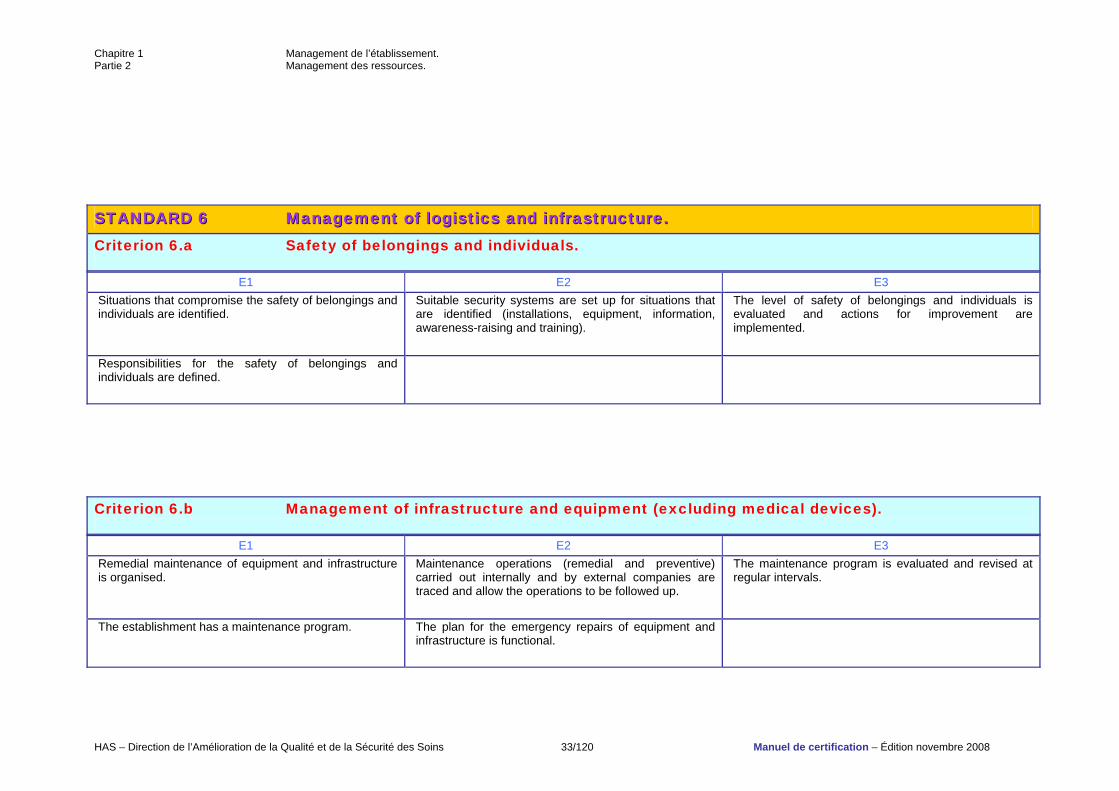
SSTTAANNDDAARRDD 66 MMaannaaggeemmeenntt ooff llooggiissttiiccss aanndd iinnffrraassttrruuccttuurree.. Criterion 6.a Safety of belongings and individuals.
E1 E2 E3 Situations that compromise the safety of belongings and individuals are identified.
Suitable security systems are set up for situations that are identified (installations, equipment, information, awareness-raising and training).
The level of safety of belongings and individuals is evaluated and actions for improvement are implemented.
Responsibilities for the safety of belongings and individuals are defined.
Criterion 6.b Management of infrastructure and equipment (excluding medical devices).
E1 E2 E3 Remedial maintenance of equipment and infrastructure is organised.
Maintenance operations (remedial and preventive) carried out internally and by external companies are traced and allow the operations to be followed up.
The maintenance program is evaluated and revised at regular intervals.
The establishment has a maintenance program. The plan for the emergency repairs of equipment and infrastructure is functional.
Chapitre 1 Management de l’établissement. Partie 2 Management des ressources.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 34/120 Manuel de certification – Édition novembre 2008
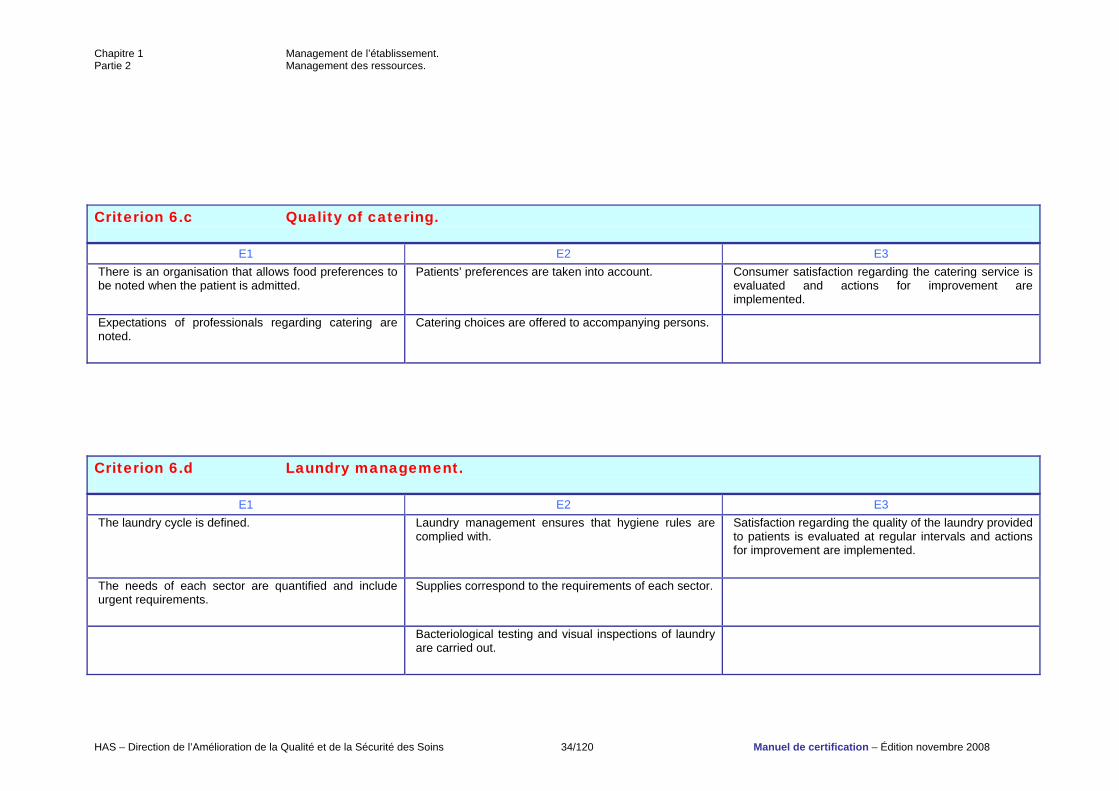
Criterion 6.c Quality of catering.
E1 E2 E3 There is an organisation that allows food preferences to be noted when the patient is admitted.
Patients’ preferences are taken into account. Consumer satisfaction regarding the catering service is evaluated and actions for improvement are implemented.
Expectations of professionals regarding catering are noted.
Catering choices are offered to accompanying persons.
Criterion 6.d Laundry management.
E1 E2 E3 The laundry cycle is defined. Laundry management ensures that hygiene rules are
complied with. Satisfaction regarding the quality of the laundry provided to patients is evaluated at regular intervals and actions for improvement are implemented.
The needs of each sector are quantified and include urgent requirements.
Supplies correspond to the requirements of each sector.
Bacteriological testing and visual inspections of laundry are carried out.
Chapitre 1 Management de l’établissement. Partie 2 Management des ressources.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 35/120 Manuel de certification – Édition novembre 2008
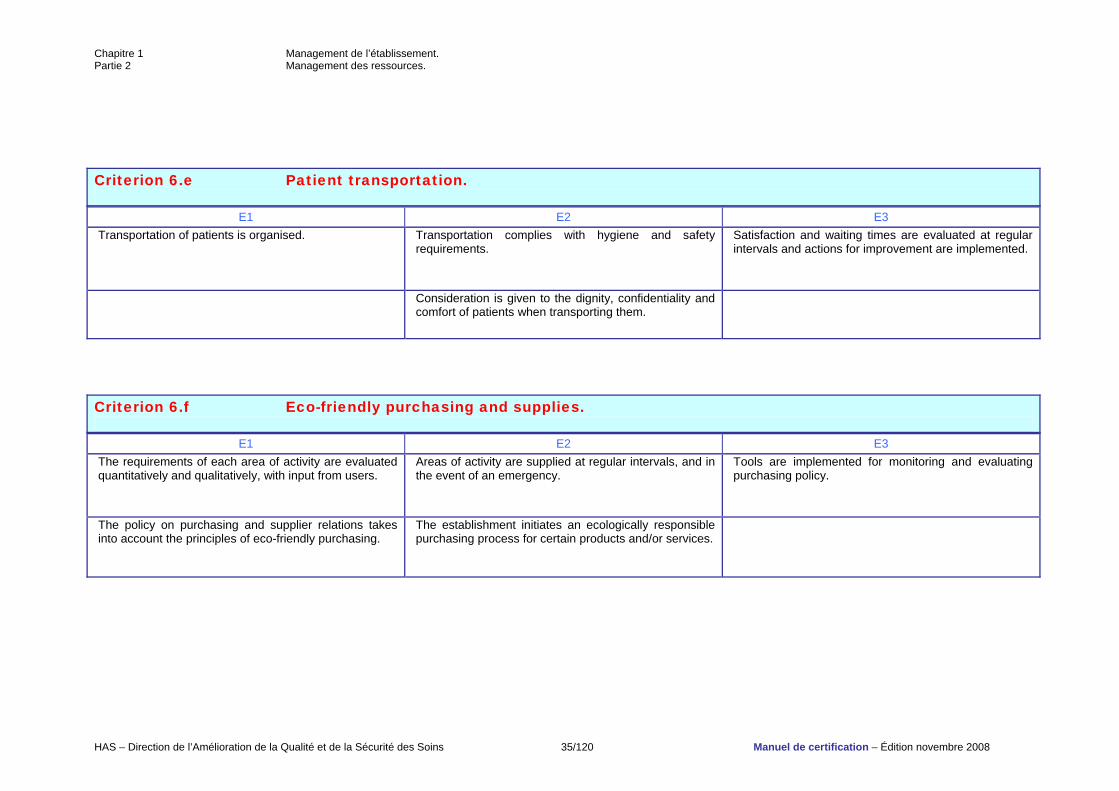
Criterion 6.e Patient transportation.
E1 E2 E3 Transportation of patients is organised. Transportation complies with hygiene and safety
requirements. Satisfaction and waiting times are evaluated at regular intervals and actions for improvement are implemented.
Consideration is given to the dignity, confidentiality and comfort of patients when transporting them.
Criterion 6.f Eco-friendly purchasing and supplies.
E1 E2 E3 The requirements of each area of activity are evaluated quantitatively and qualitatively, with input from users.
Areas of activity are supplied at regular intervals, and in the event of an emergency.
Tools are implemented for monitoring and evaluating purchasing policy.
The policy on purchasing and supplier relations takes into account the principles of eco-friendly purchasing.
The establishment initiates an ecologically responsible purchasing process for certain products and/or services.
Chapitre 1 Management de l’établissement. Partie 2 Management des ressources.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 36/120 Manuel de certification – Édition novembre 2008
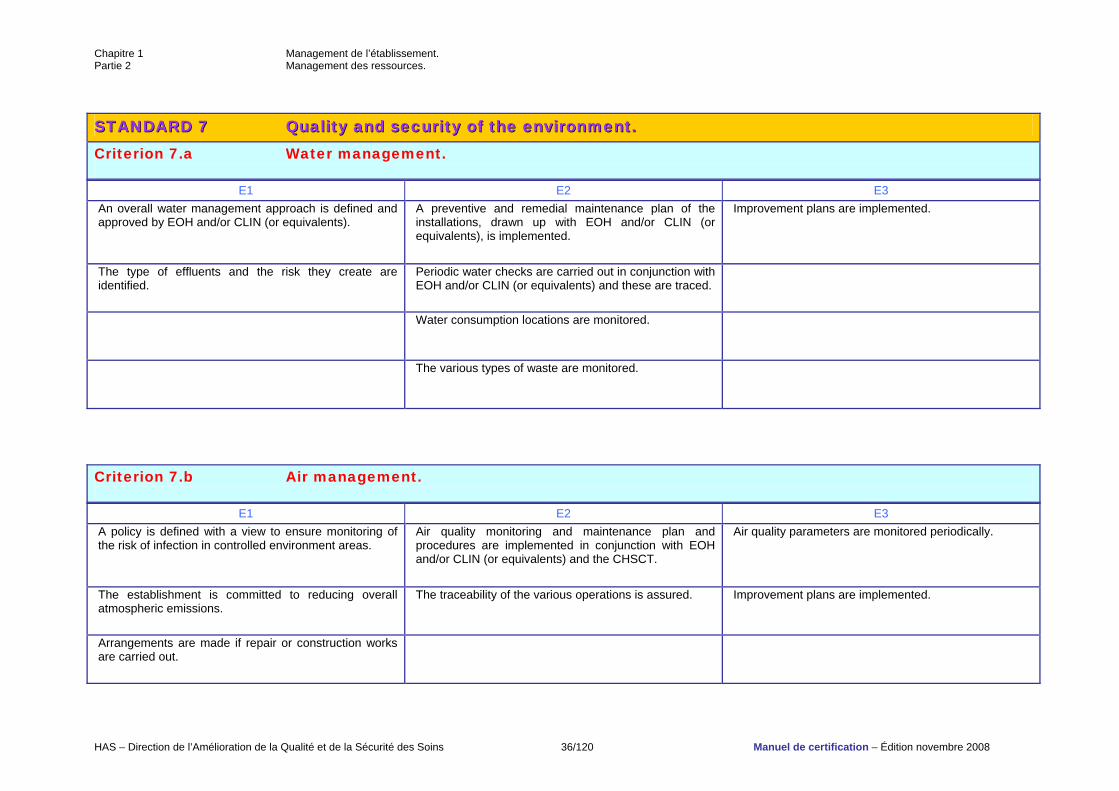
SSTTAANNDDAARRDD 77 QQuuaalliittyy aanndd sseeccuurriittyy ooff tthhee eennvviirroonnmmeenntt.. Criterion 7.a Water management.
E1 E2 E3 An overall water management approach is defined and approved by EOH and/or CLIN (or equivalents).
A preventive and remedial maintenance plan of the installations, drawn up with EOH and/or CLIN (or equivalents), is implemented.
Improvement plans are implemented.
The type of effluents and the risk they create are identified.
Periodic water checks are carried out in conjunction with EOH and/or CLIN (or equivalents) and these are traced.
Water consumption locations are monitored.
The various types of waste are monitored.
Criterion 7.b Air management.
E1 E2 E3 A policy is defined with a view to ensure monitoring of the risk of infection in controlled environment areas.
Air quality monitoring and maintenance plan and procedures are implemented in conjunction with EOH and/or CLIN (or equivalents) and the CHSCT.
Air quality parameters are monitored periodically.
The establishment is committed to reducing overall atmospheric emissions.
The traceability of the various operations is assured. Improvement plans are implemented.
Arrangements are made if repair or construction works are carried out.
Chapitre 1 Management de l’établissement. Partie 2 Management des ressources.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 37/120 Manuel de certification – Édition novembre 2008
Chapitre 1 Management de l’établissement. Partie 2 Management des ressources.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 38/120 Manuel de certification – Édition novembre 2008
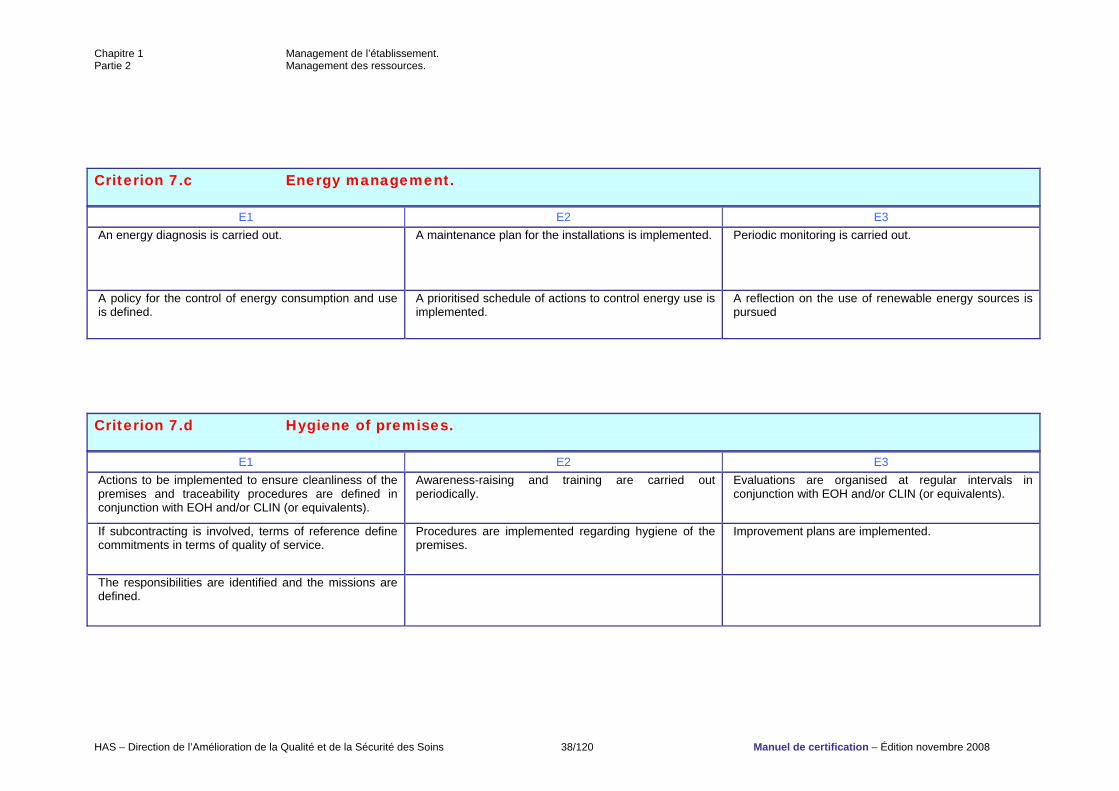
Criterion 7.c Energy management.
E1 E2 E3 An energy diagnosis is carried out. A maintenance plan for the installations is implemented. Periodic monitoring is carried out.
A policy for the control of energy consumption and use is defined.
A prioritised schedule of actions to control energy use is implemented.
A reflection on the use of renewable energy sources is pursued
Criterion 7.d Hygiene of premises.
E1 E2 E3 Actions to be implemented to ensure cleanliness of the premises and traceability procedures are defined in conjunction with EOH and/or CLIN (or equivalents).
Awareness-raising and training are carried out periodically.
Evaluations are organised at regular intervals in conjunction with EOH and/or CLIN (or equivalents).
If subcontracting is involved, terms of reference define commitments in terms of quality of service.
Procedures are implemented regarding hygiene of the premises.
Improvement plans are implemented.
The responsibilities are identified and the missions are defined.
Chapitre 1 Management de l’établissement. Partie 2 Management des ressources.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 39/120 Manuel de certification – Édition novembre 2008
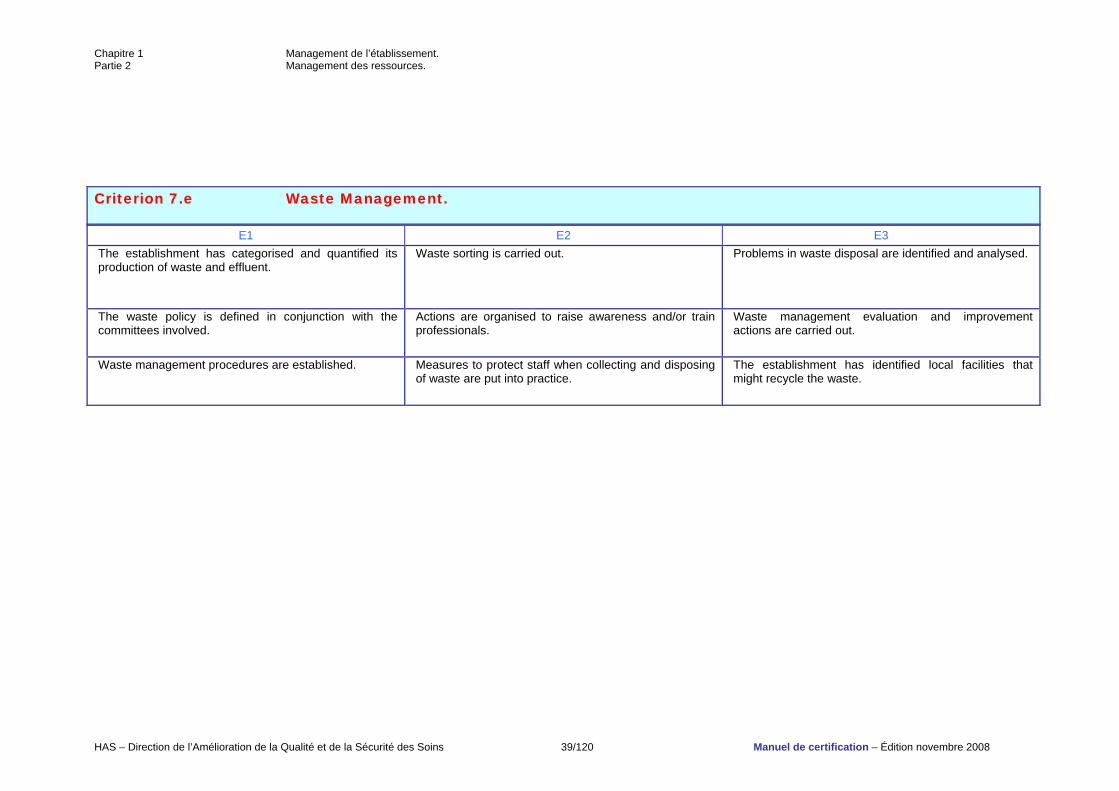
Criterion 7.e Waste Management.
E1 E2 E3 The establishment has categorised and quantified its production of waste and effluent.
Waste sorting is carried out. Problems in waste disposal are identified and analysed.
The waste policy is defined in conjunction with the committees involved.
Actions are organised to raise awareness and/or train professionals.
Waste management evaluation and improvement actions are carried out.
Waste management procedures are established. Measures to protect staff when collecting and disposing of waste are put into practice.
The establishment has identified local facilities that might recycle the waste.
Chapitre 1 Management de l’établissement. Partie 3 Management de la qualité et de la sécurité des soins.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 40/120 Manuel de certification – Édition novembre 2008
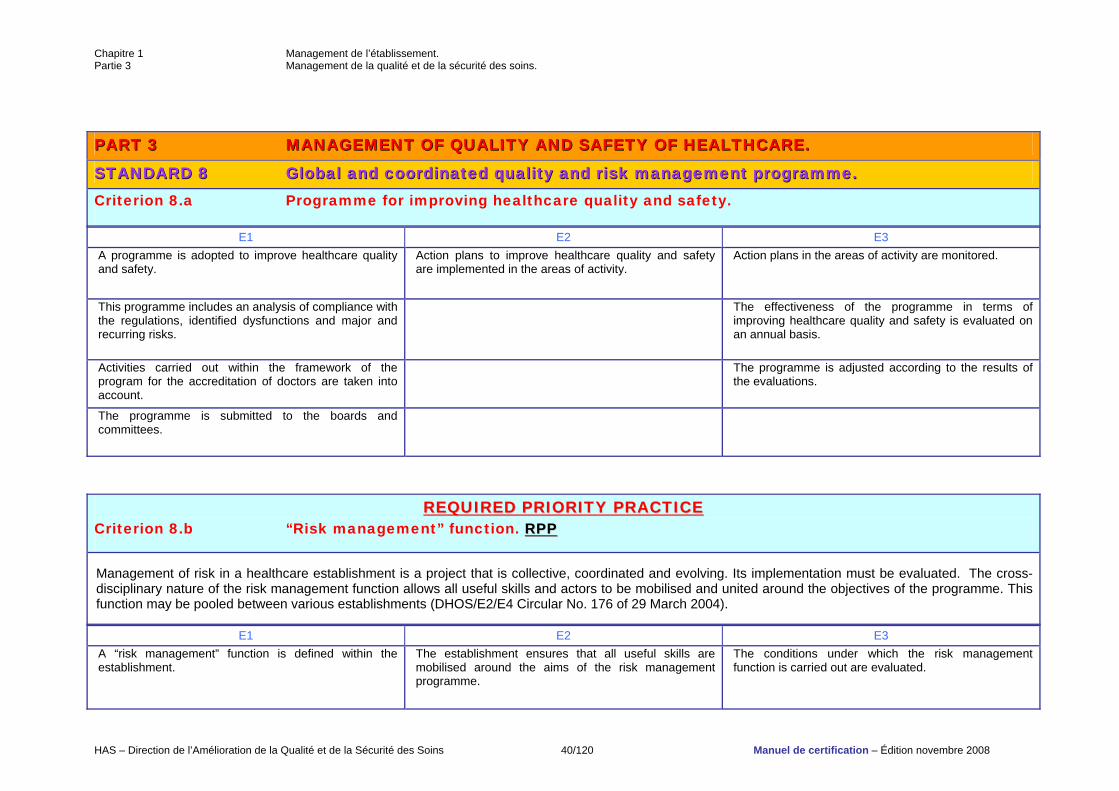
PPAARRTT 33 MMAANNAAGGEEMMEENNTT OOFF QQUUAALLIITTYY AANNDD SSAAFFEETTYY OOFF HHEEAALLTTHHCCAARREE..
SSTTAANNDDAARRDD 88 GGlloobbaall aanndd ccoooorrddiinnaatteedd qquuaalliittyy aanndd rriisskk mmaannaaggeemmeenntt pprrooggrraammmmee.. Criterion 8.a Programme for improving healthcare quality and safety.
E1 E2 E3 A programme is adopted to improve healthcare quality and safety.
Action plans to improve healthcare quality and safety are implemented in the areas of activity.
Action plans in the areas of activity are monitored.
This programme includes an analysis of compliance with the regulations, identified dysfunctions and major and recurring risks.
The effectiveness of the programme in terms of improving healthcare quality and safety is evaluated on an annual basis.
Activities carried out within the framework of the program for the accreditation of doctors are taken into account.
The programme is adjusted according to the results of the evaluations.
The programme is submitted to the boards and committees.
RREEQQUUIIRREEDD PPRRIIOORRIITTYY PPRRAACCTTIICCEE Criterion 8.b “Risk management” function. RRPPPP Management of risk in a healthcare establishment is a project that is collective, coordinated and evolving. Its implementation must be evaluated. The cross-disciplinary nature of the risk management function allows all useful skills and actors to be mobilised and united around the objectives of the programme. This function may be pooled between various establishments (DHOS/E2/E4 Circular No. 176 of 29 March 2004).
E1 E2 E3 A “risk management” function is defined within the establishment.
The establishment ensures that all useful skills are mobilised around the aims of the risk management programme.
The conditions under which the risk management function is carried out are evaluated.
Chapitre 1 Management de l’établissement. Partie 3 Management de la qualité et de la sécurité des soins.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 41/120 Manuel de certification – Édition novembre 2008
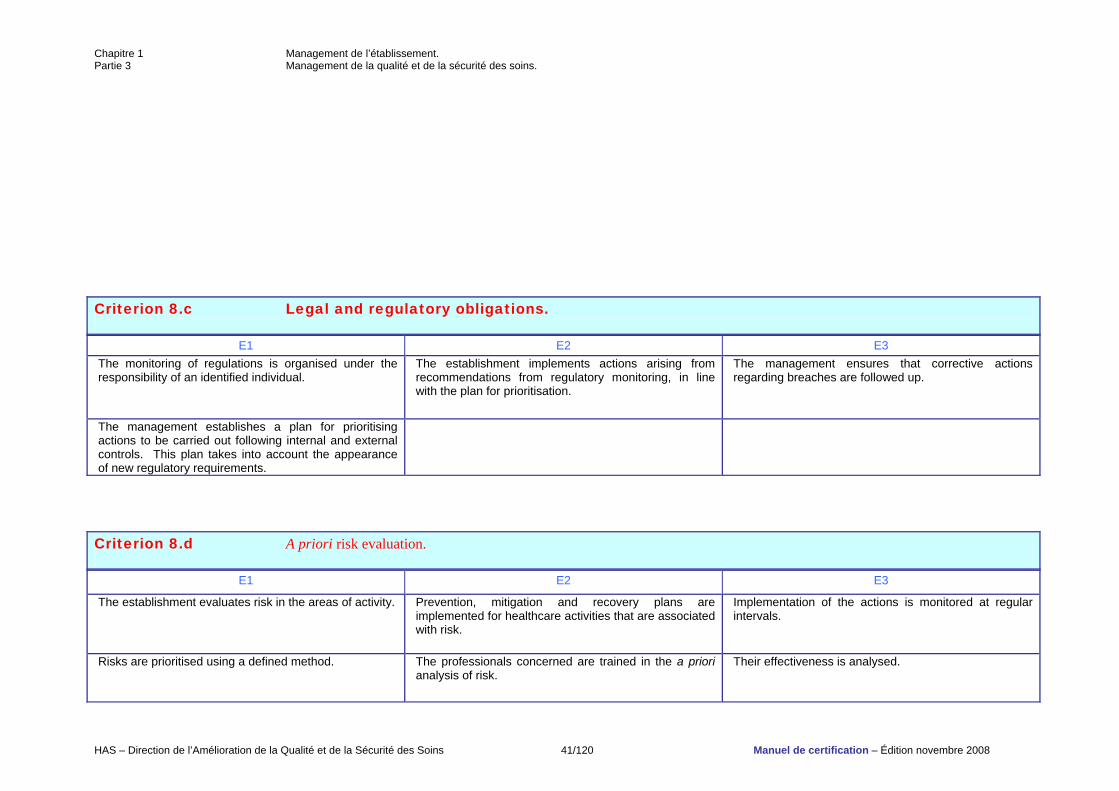
Criterion 8.c Legal and regulatory obligations.
E1 E2 E3 The monitoring of regulations is organised under the responsibility of an identified individual.
The establishment implements actions arising from recommendations from regulatory monitoring, in line with the plan for prioritisation.
The management ensures that corrective actions regarding breaches are followed up.
The management establishes a plan for prioritising actions to be carried out following internal and external controls. This plan takes into account the appearance of new regulatory requirements.
Criterion 8.d A priori risk evaluation.
E1 E2 E3
The establishment evaluates risk in the areas of activity. Prevention, mitigation and recovery plans are implemented for healthcare activities that are associated with risk.
Implementation of the actions is monitored at regular intervals.
Risks are prioritised using a defined method. The professionals concerned are trained in the a priori analysis of risk.
Their effectiveness is analysed.
Chapitre 1 Management de l’établissement. Partie 3 Management de la qualité et de la sécurité des soins.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 42/120 Manuel de certification – Édition novembre 2008
Chapitre 1 Management de l’établissement. Partie 3 Management de la qualité et de la sécurité des soins.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 43/120 Manuel de certification – Édition novembre 2008
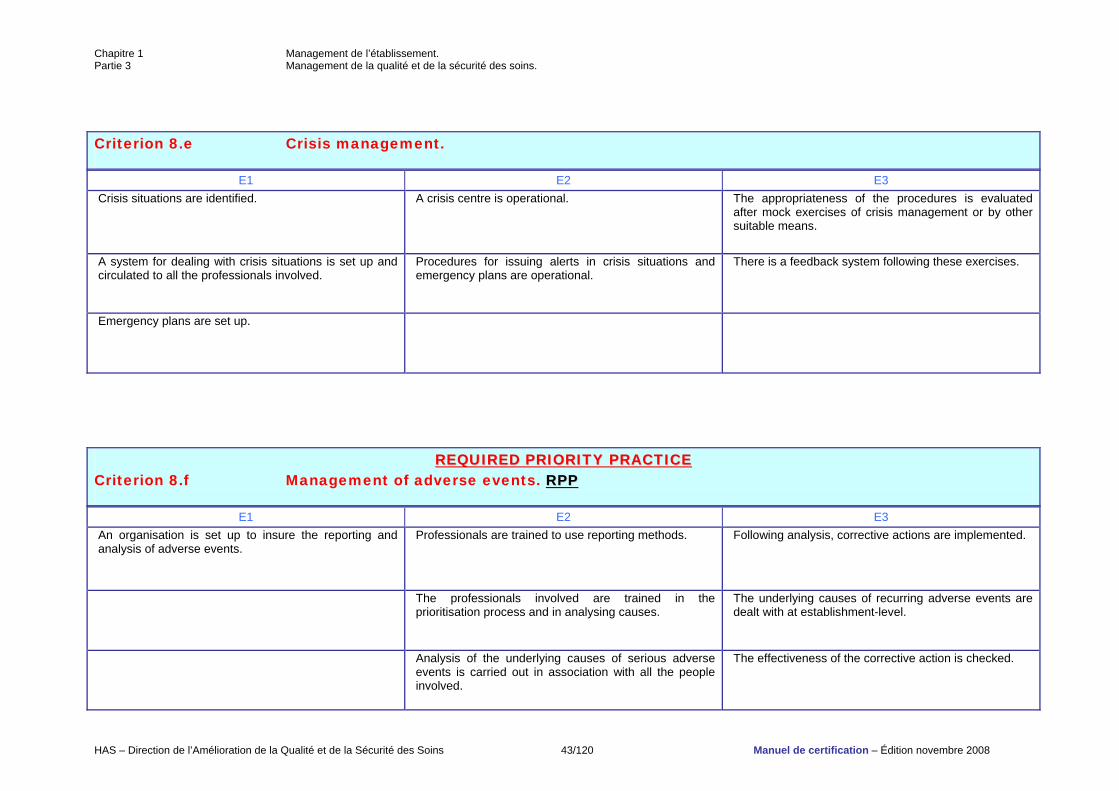
Criterion 8.e Crisis management.
E1 E2 E3 Crisis situations are identified. A crisis centre is operational. The appropriateness of the procedures is evaluated
after mock exercises of crisis management or by other suitable means.
A system for dealing with crisis situations is set up and circulated to all the professionals involved.
Procedures for issuing alerts in crisis situations and emergency plans are operational.
There is a feedback system following these exercises.
Emergency plans are set up.
RREEQQUUIIRREEDD PPRRIIOORRIITTYY PPRRAACCTTIICCEE Criterion 8.f Management of adverse events. RRPPPP
E1 E2 E3 An organisation is set up to insure the reporting and analysis of adverse events.
Professionals are trained to use reporting methods. Following analysis, corrective actions are implemented.
The professionals involved are trained in the prioritisation process and in analysing causes.
The underlying causes of recurring adverse events are dealt with at establishment-level.
Analysis of the underlying causes of serious adverse events is carried out in association with all the people involved.
The effectiveness of the corrective action is checked.
Chapitre 1 Management de l’établissement. Partie 3 Management de la qualité et de la sécurité des soins.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 44/120 Manuel de certification – Édition novembre 2008
Chapitre 1 Management de l’établissement. Partie 3 Management de la qualité et de la sécurité des soins.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 45/120 Manuel de certification – Édition novembre 2008
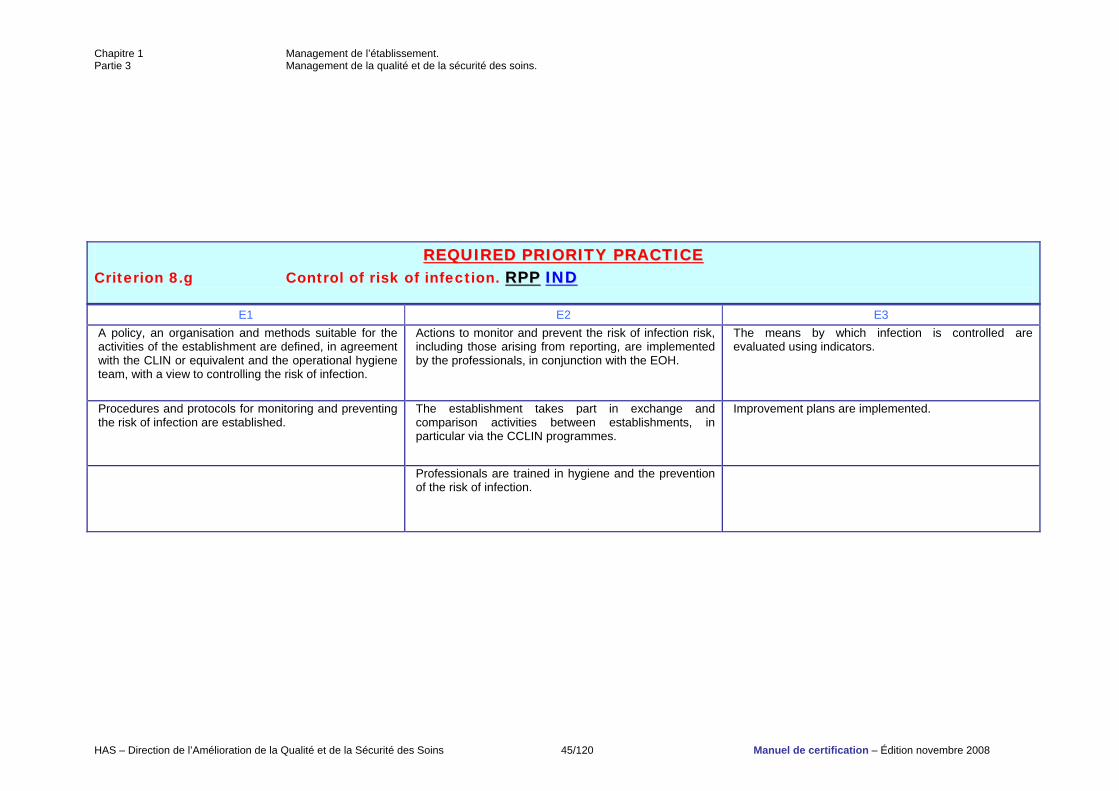
RREEQQUUIIRREEDD PPRRIIOORRIITTYY PPRRAACCTTIICCEE Criterion 8.g Control of risk of infection. RRPPPP IINNDD
E1 E2 E3 A policy, an organisation and methods suitable for the activities of the establishment are defined, in agreement with the CLIN or equivalent and the operational hygiene team, with a view to controlling the risk of infection.
Actions to monitor and prevent the risk of infection risk, including those arising from reporting, are implemented by the professionals, in conjunction with the EOH.
The means by which infection is controlled are evaluated using indicators.
Procedures and protocols for monitoring and preventing the risk of infection are established.
The establishment takes part in exchange and comparison activities between establishments, in particular via the CCLIN programmes.
Improvement plans are implemented.
Professionals are trained in hygiene and the prevention of the risk of infection.
Chapitre 1 Management de l’établissement. Partie 3 Management de la qualité et de la sécurité des soins.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 46/120 Manuel de certification – Édition novembre 2008
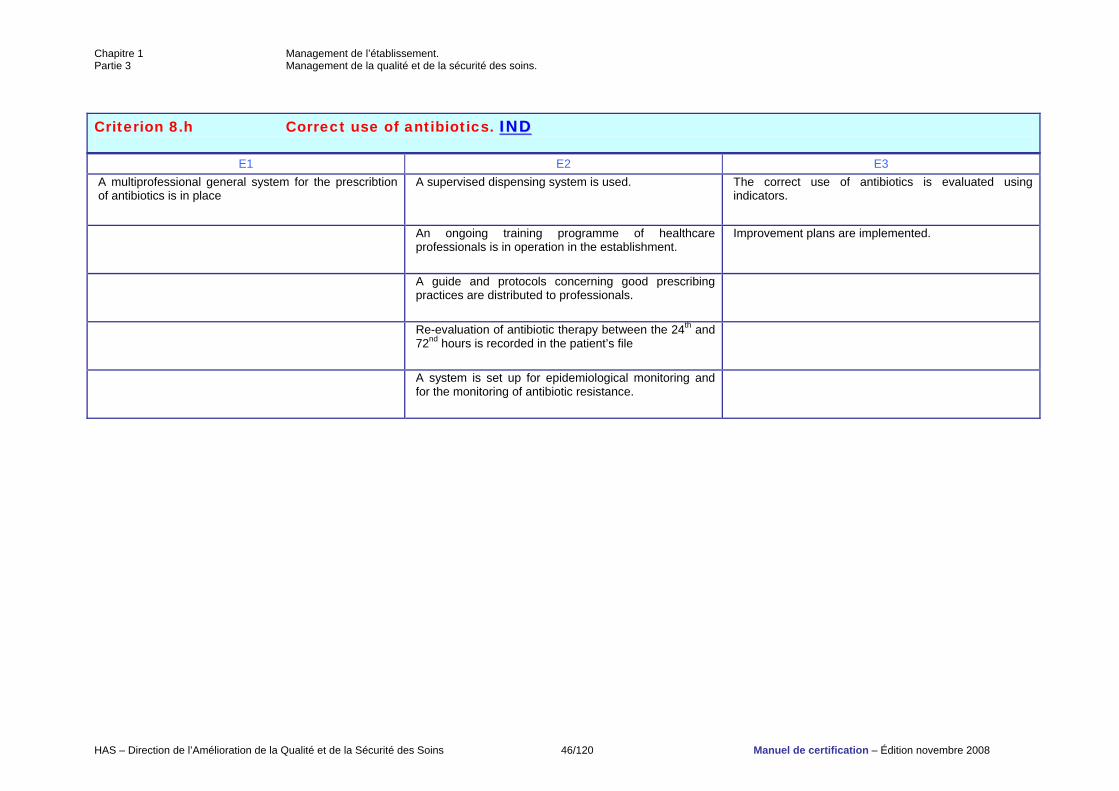
Criterion 8.h Correct use of antibiotics. IINNDD
E1 E2 E3 A multiprofessional general system for the prescribtion of antibiotics is in place
A supervised dispensing system is used. The correct use of antibiotics is evaluated using indicators.
An ongoing training programme of healthcare professionals is in operation in the establishment.
Improvement plans are implemented.
A guide and protocols concerning good prescribing practices are distributed to professionals.
Re-evaluation of antibiotic therapy between the 24th and 72nd hours is recorded in the patient’s file
A system is set up for epidemiological monitoring and for the monitoring of antibiotic resistance.
Chapitre 1 Management de l’établissement. Partie 3 Management de la qualité et de la sécurité des soins.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 47/120 Manuel de certification – Édition novembre 2008
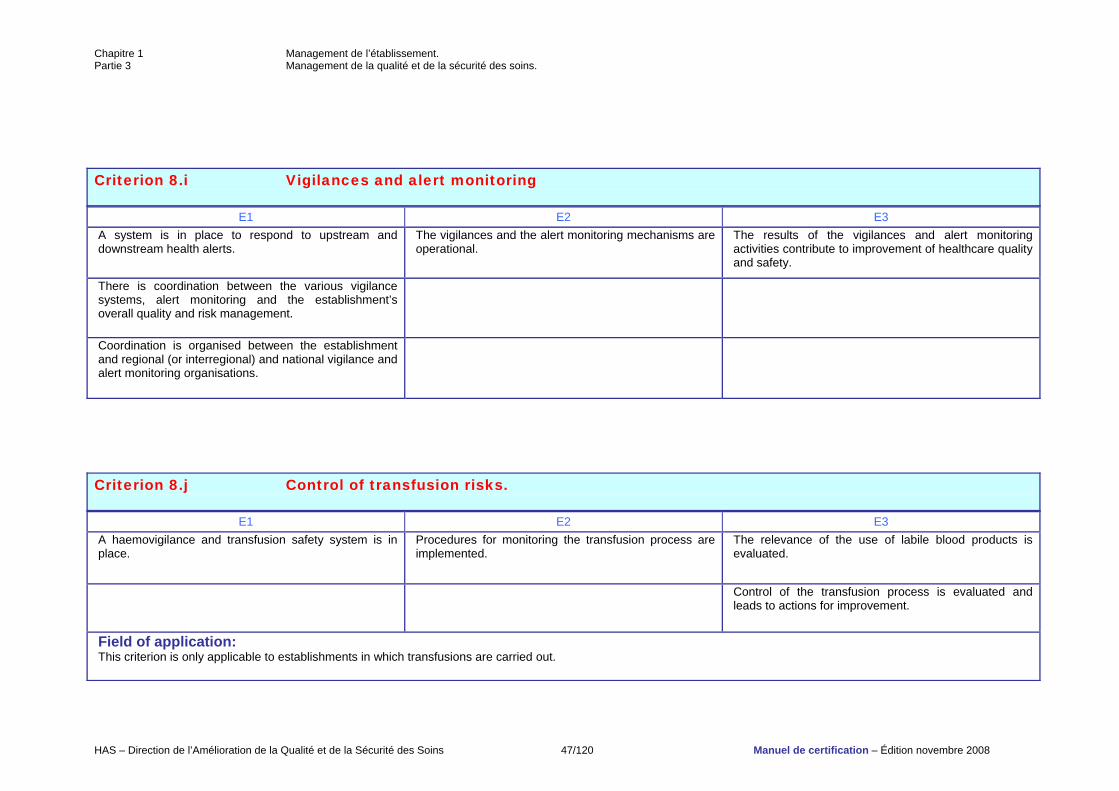
Criterion 8.i Vigilances and alert monitoring
E1 E2 E3 A system is in place to respond to upstream and downstream health alerts.
The vigilances and the alert monitoring mechanisms are operational.
The results of the vigilances and alert monitoring activities contribute to improvement of healthcare quality and safety.
There is coordination between the various vigilance systems, alert monitoring and the establishment’s overall quality and risk management.
Coordination is organised between the establishment and regional (or interregional) and national vigilance and alert monitoring organisations.
Criterion 8.j Control of transfusion risks.
E1 E2 E3 A haemovigilance and transfusion safety system is in place.
Procedures for monitoring the transfusion process are implemented.
The relevance of the use of labile blood products is evaluated.
Control of the transfusion process is evaluated and leads to actions for improvement.
Field of application: This criterion is only applicable to establishments in which transfusions are carried out.
Chapitre 1 Management de l’établissement. Partie 3 Management de la qualité et de la sécurité des soins.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 48/120 Manuel de certification – Édition novembre 2008
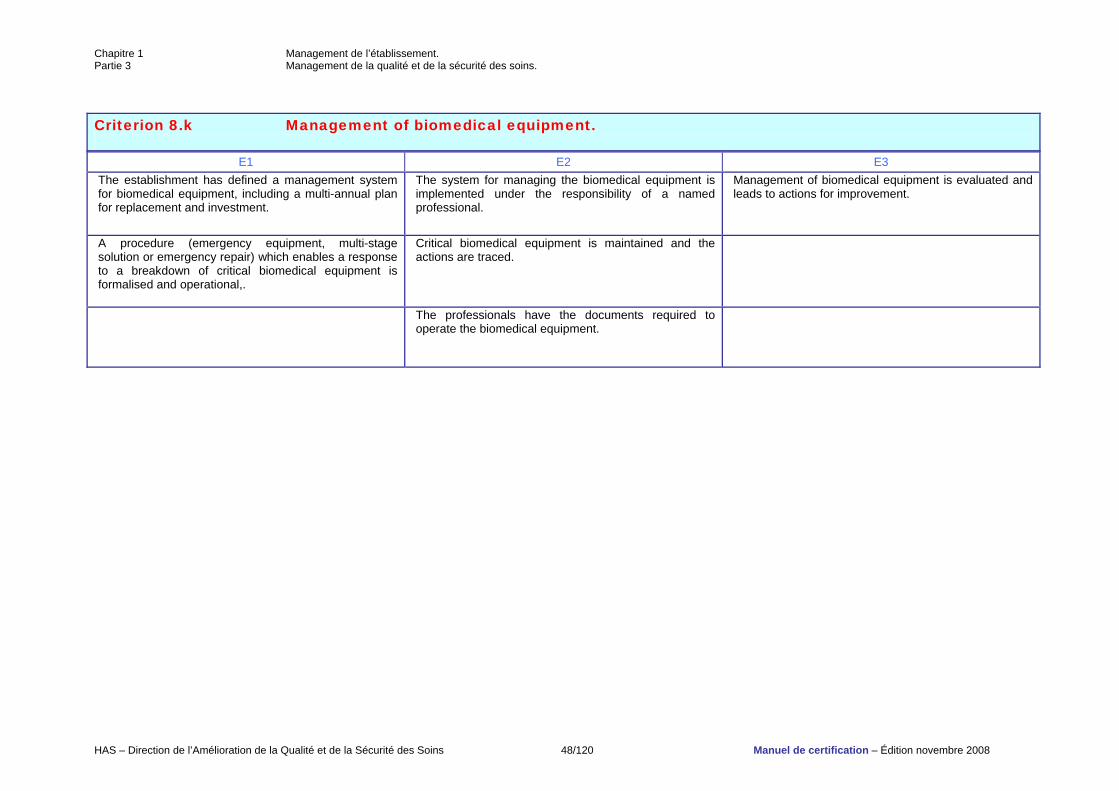
Criterion 8.k Management of biomedical equipment.
E1 E2 E3 The establishment has defined a management system for biomedical equipment, including a multi-annual plan for replacement and investment.
The system for managing the biomedical equipment is implemented under the responsibility of a named professional.
Management of biomedical equipment is evaluated and leads to actions for improvement.
A procedure (emergency equipment, multi-stage solution or emergency repair) which enables a response to a breakdown of critical biomedical equipment is formalised and operational,.
Critical biomedical equipment is maintained and the actions are traced.
The professionals have the documents required to operate the biomedical equipment.
Chapitre 1 Management de l’établissement. Partie 3 Management de la qualité et de la sécurité des soins.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 49/120 Manuel de certification – Édition novembre 2008
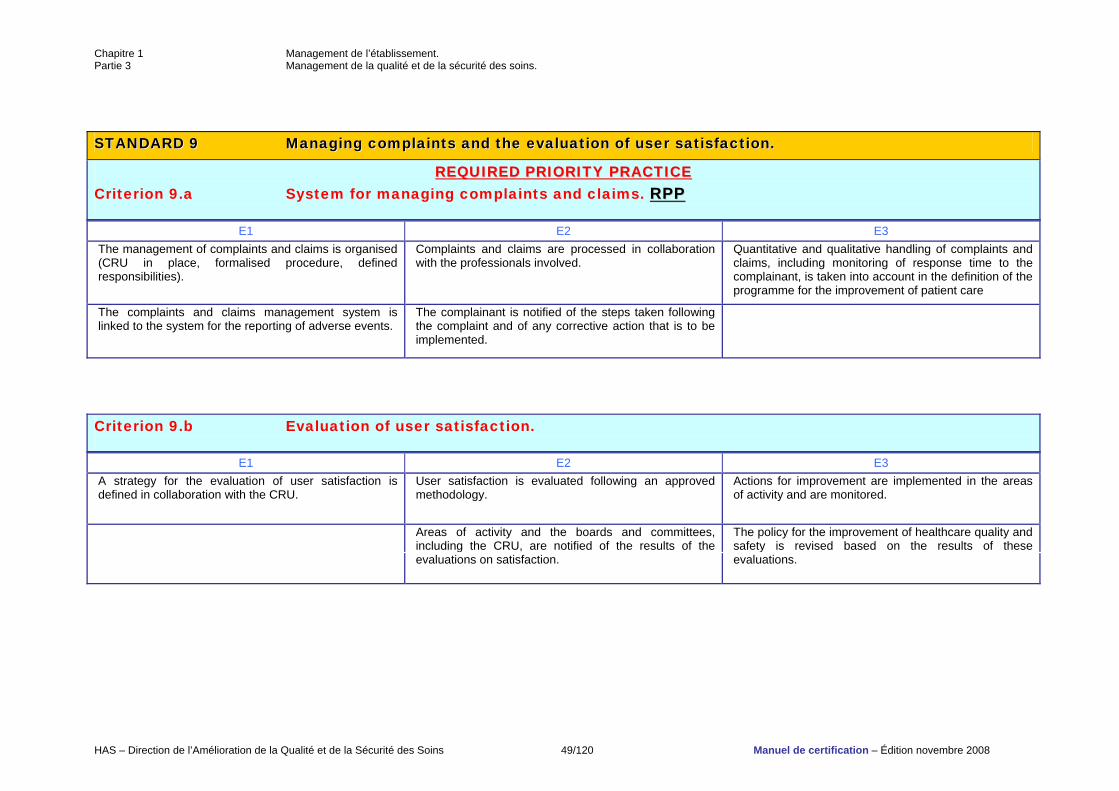
SSTTAANNDDAARRDD 99 MMaannaaggiinngg ccoommppllaaiinnttss aanndd tthhee eevvaalluuaattiioonn ooff uusseerr ssaattiissffaaccttiioonn..
RREEQQUUIIRREEDD PPRRIIOORRIITTYY PPRRAACCTTIICCEE Criterion 9.a System for managing complaints and claims. RRPPPP
E1 E2 E3 The management of complaints and claims is organised (CRU in place, formalised procedure, defined responsibilities).
Complaints and claims are processed in collaboration with the professionals involved.
Quantitative and qualitative handling of complaints and claims, including monitoring of response time to the complainant, is taken into account in the definition of the programme for the improvement of patient care
The complaints and claims management system is linked to the system for the reporting of adverse events.
The complainant is notified of the steps taken following the complaint and of any corrective action that is to be implemented.
Criterion 9.b Evaluation of user satisfaction.
E1 E2 E3 A strategy for the evaluation of user satisfaction is defined in collaboration with the CRU.
User satisfaction is evaluated following an approved methodology.
Actions for improvement are implemented in the areas of activity and are monitored.
Areas of activity and the boards and committees, including the CRU, are notified of the results of the evaluations on satisfaction.
The policy for the improvement of healthcare quality and safety is revised based on the results of these evaluations.
Chapitre 2 Prise en charge du patient.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 50/120 Manuel de certification – Édition novembre 2008
CCHHAAPPTTEERR 22 PPaattiieenntt mmaannaaggeemmeenntt..
Chapitre 2 Prise en charge du patient. Partie 1 Droits et place des patients.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 51/120 Manuel de certification – Édition novembre 2008
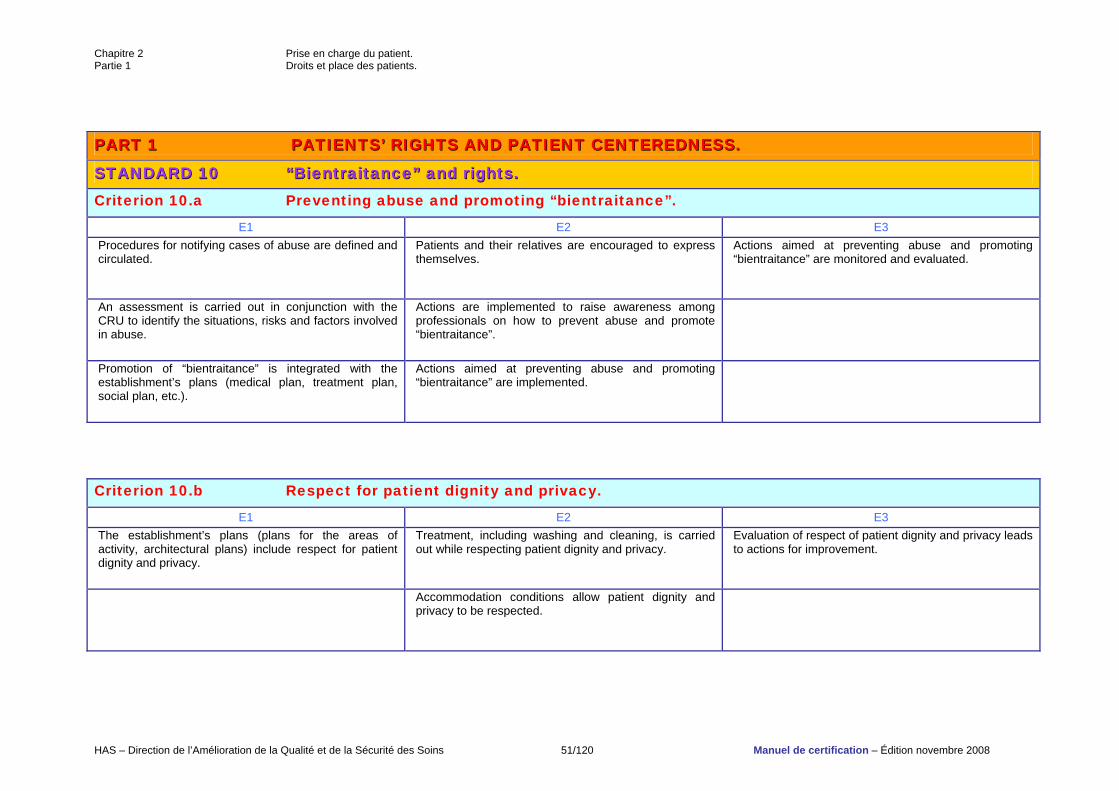
PPAARRTT 11 PPAATTIIEENNTTSS’’ RRIIGGHHTTSS AANNDD PPAATTIIEENNTT CCEENNTTEERREEDDNNEESSSS..
SSTTAANNDDAARRDD 1100 ““BBiieennttrraaiittaannccee”” aanndd rriigghhttss.. Criterion 10.a Preventing abuse and promoting “bientraitance”.
E1 E2 E3 Procedures for notifying cases of abuse are defined and circulated.
Patients and their relatives are encouraged to express themselves.
Actions aimed at preventing abuse and promoting “bientraitance” are monitored and evaluated.
An assessment is carried out in conjunction with the CRU to identify the situations, risks and factors involved in abuse.
Actions are implemented to raise awareness among professionals on how to prevent abuse and promote “bientraitance”.
Promotion of “bientraitance” is integrated with the establishment’s plans (medical plan, treatment plan, social plan, etc.).
Actions aimed at preventing abuse and promoting “bientraitance” are implemented.
Criterion 10.b Respect for patient dignity and privacy.
E1 E2 E3 The establishment’s plans (plans for the areas of activity, architectural plans) include respect for patient dignity and privacy.
Treatment, including washing and cleaning, is carried out while respecting patient dignity and privacy.
Evaluation of respect of patient dignity and privacy leads to actions for improvement.
Accommodation conditions allow patient dignity and privacy to be respected.
Chapitre 2 Prise en charge du patient. Partie 1 Droits et place des patients.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 52/120 Manuel de certification – Édition novembre 2008
Chapitre 2 Prise en charge du patient. Partie 1 Droits et place des patients.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 53/120 Manuel de certification – Édition novembre 2008
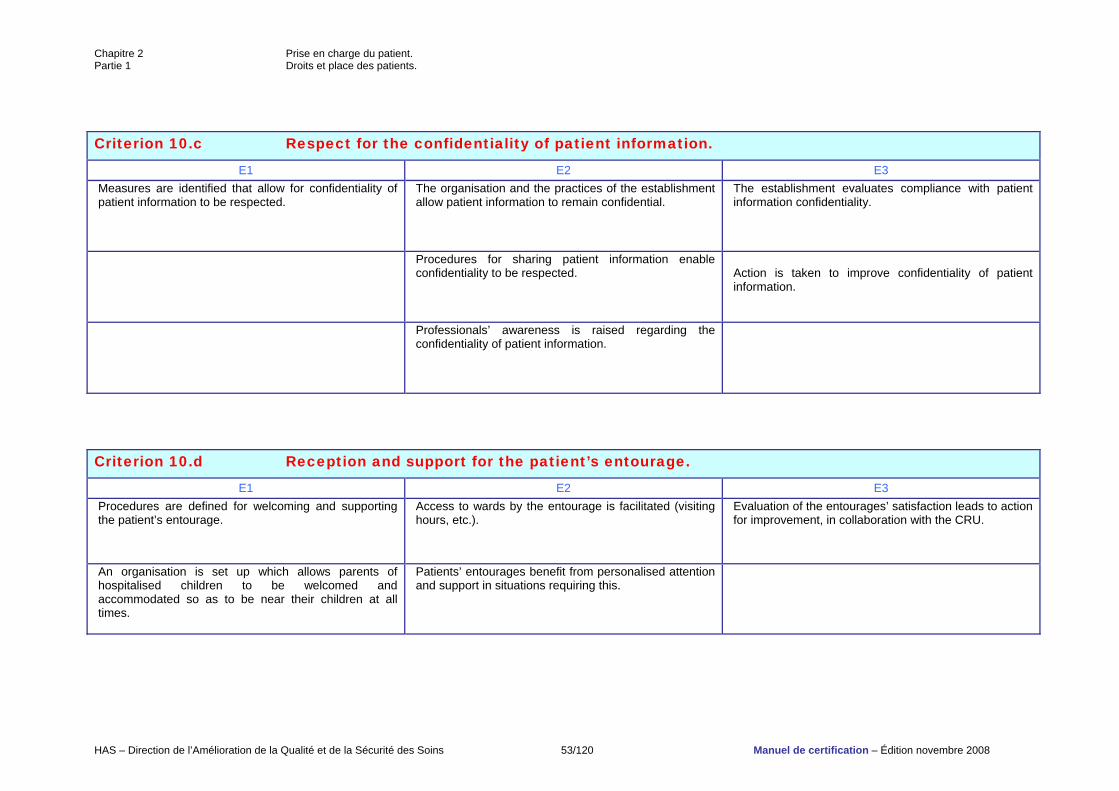
Criterion 10.c Respect for the confidentiality of patient information.
E1 E2 E3 Measures are identified that allow for confidentiality of patient information to be respected.
The organisation and the practices of the establishment allow patient information to remain confidential.
The establishment evaluates compliance with patient information confidentiality.
Procedures for sharing patient information enable confidentiality to be respected.
Action is taken to improve confidentiality of patient information.
Professionals’ awareness is raised regarding the confidentiality of patient information.
Criterion 10.d Reception and support for the patient’s entourage.
E1 E2 E3 Procedures are defined for welcoming and supporting the patient’s entourage.
Access to wards by the entourage is facilitated (visiting hours, etc.).
Evaluation of the entourages’ satisfaction leads to action for improvement, in collaboration with the CRU.
An organisation is set up which allows parents of hospitalised children to be welcomed and accommodated so as to be near their children at all times.
Patients’ entourages benefit from personalised attention and support in situations requiring this.
Chapitre 2 Prise en charge du patient. Partie 1 Droits et place des patients.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 54/120 Manuel de certification – Édition novembre 2008
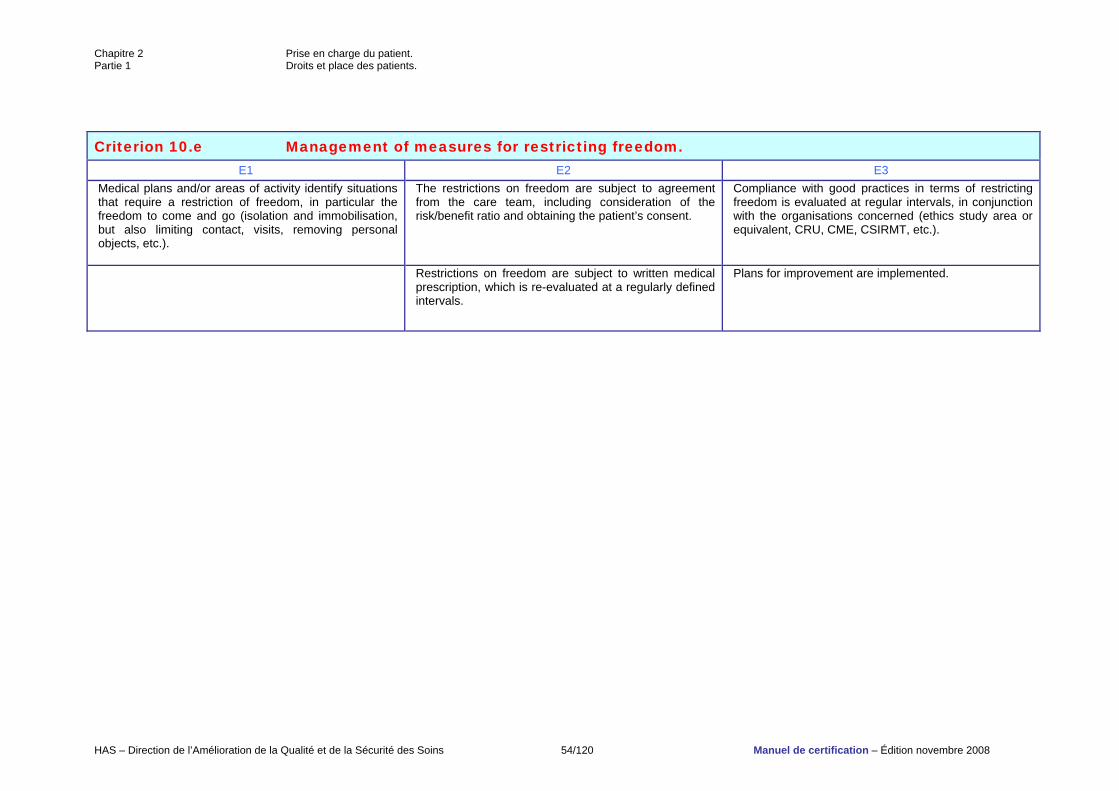
Criterion 10.e Management of measures for restricting freedom. E1 E2 E3
Medical plans and/or areas of activity identify situations that require a restriction of freedom, in particular the freedom to come and go (isolation and immobilisation, but also limiting contact, visits, removing personal objects, etc.).
The restrictions on freedom are subject to agreement from the care team, including consideration of the risk/benefit ratio and obtaining the patient’s consent.
Compliance with good practices in terms of restricting freedom is evaluated at regular intervals, in conjunction with the organisations concerned (ethics study area or equivalent, CRU, CME, CSIRMT, etc.).
Restrictions on freedom are subject to written medical prescription, which is re-evaluated at a regularly defined intervals.
Plans for improvement are implemented.
Chapitre 2 Prise en charge du patient. Partie 1 Droits et place des patients.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 55/120 Manuel de certification – Édition novembre 2008
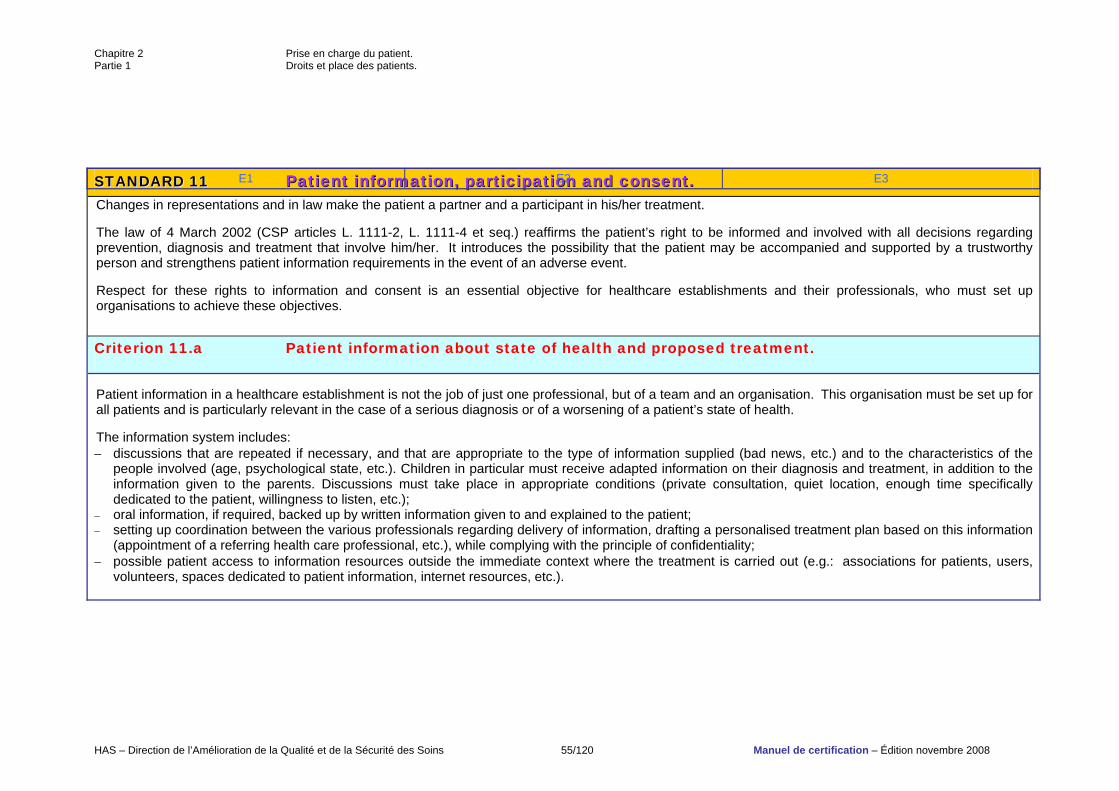
SSTTAANNDDAARRDD 1111 PPaattiieenntt iinnffoorrmmaattiioonn,, ppaarrttiicciippaattiioonn aanndd ccoonnsseenntt.. Changes in representations and in law make the patient a partner and a participant in his/her treatment. The law of 4 March 2002 (CSP articles L. 1111-2, L. 1111-4 et seq.) reaffirms the patient’s right to be informed and involved with all decisions regarding prevention, diagnosis and treatment that involve him/her. It introduces the possibility that the patient may be accompanied and supported by a trustworthy person and strengthens patient information requirements in the event of an adverse event. Respect for these rights to information and consent is an essential objective for healthcare establishments and their professionals, who must set up organisations to achieve these objectives. Criterion 11.a Patient information about state of health and proposed treatment. Patient information in a healthcare establishment is not the job of just one professional, but of a team and an organisation. This organisation must be set up for all patients and is particularly relevant in the case of a serious diagnosis or of a worsening of a patient’s state of health. The information system includes: − discussions that are repeated if necessary, and that are appropriate to the type of information supplied (bad news, etc.) and to the characteristics of the
people involved (age, psychological state, etc.). Children in particular must receive adapted information on their diagnosis and treatment, in addition to the information given to the parents. Discussions must take place in appropriate conditions (private consultation, quiet location, enough time specifically dedicated to the patient, willingness to listen, etc.);
− oral information, if required, backed up by written information given to and explained to the patient; − setting up coordination between the various professionals regarding delivery of information, drafting a personalised treatment plan based on this information
(appointment of a referring health care professional, etc.), while complying with the principle of confidentiality; − possible patient access to information resources outside the immediate context where the treatment is carried out (e.g.: associations for patients, users,
volunteers, spaces dedicated to patient information, internet resources, etc.).
E1 E2 E3
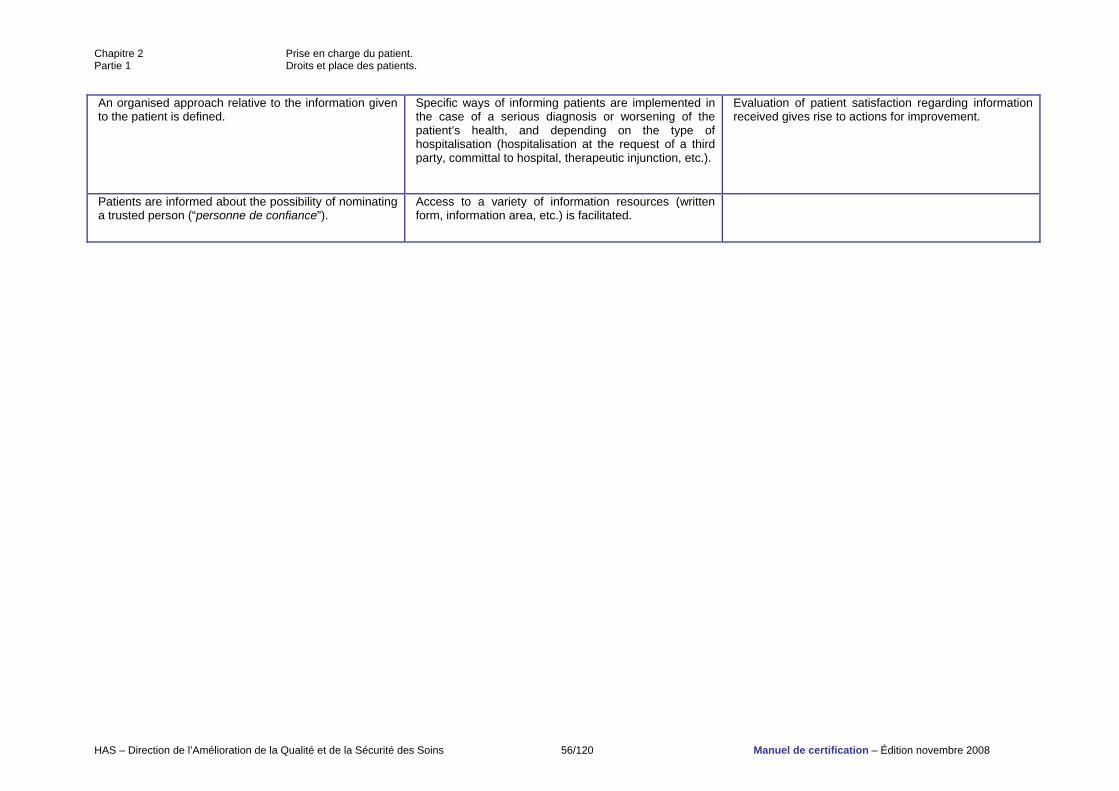
Chapitre 2 Prise en charge du patient. Partie 1 Droits et place des patients.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 56/120 Manuel de certification – Édition novembre 2008
An organised approach relative to the information given to the patient is defined.
Specific ways of informing patients are implemented in the case of a serious diagnosis or worsening of the patient’s health, and depending on the type of hospitalisation (hospitalisation at the request of a third party, committal to hospital, therapeutic injunction, etc.).
Evaluation of patient satisfaction regarding information received gives rise to actions for improvement.
Patients are informed about the possibility of nominating a trusted person (“personne de confiance”).
Access to a variety of information resources (written form, information area, etc.) is facilitated.
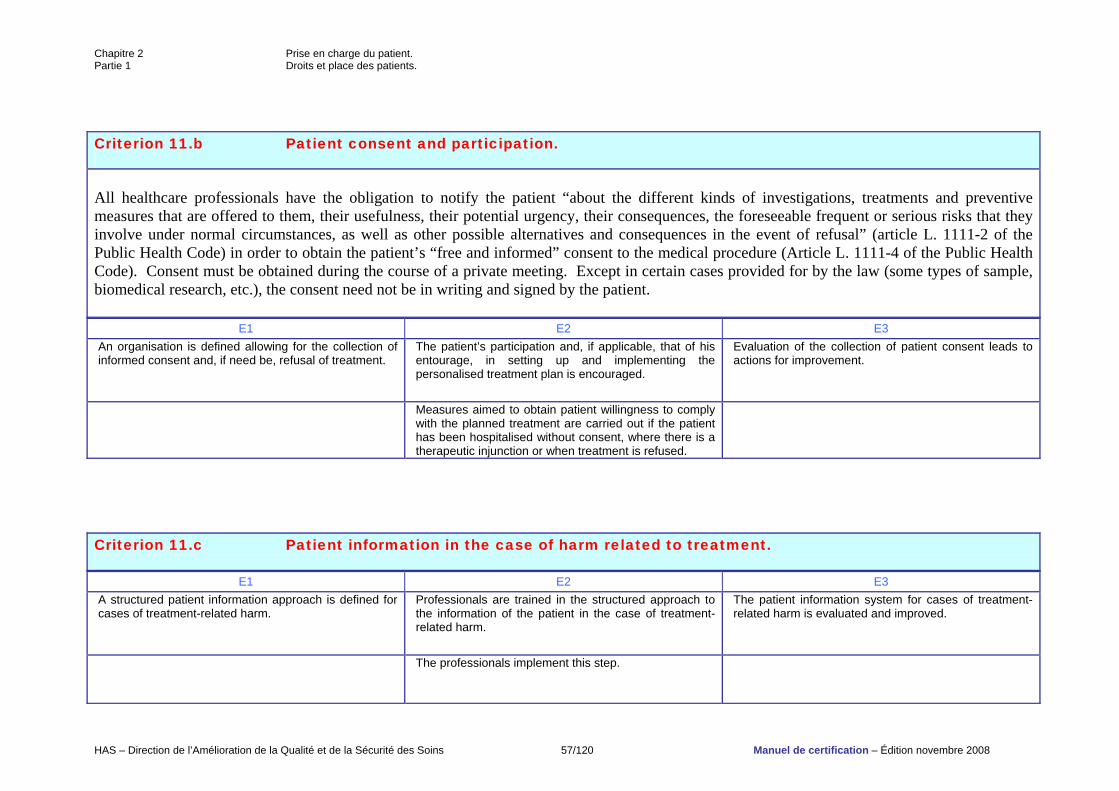
Chapitre 2 Prise en charge du patient. Partie 1 Droits et place des patients.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 57/120 Manuel de certification – Édition novembre 2008
Criterion 11.b Patient consent and participation. All healthcare professionals have the obligation to notify the patient “about the different kinds of investigations, treatments and preventive measures that are offered to them, their usefulness, their potential urgency, their consequences, the foreseeable frequent or serious risks that they involve under normal circumstances, as well as other possible alternatives and consequences in the event of refusal” (article L. 1111-2 of the Public Health Code) in order to obtain the patient’s “free and informed” consent to the medical procedure (Article L. 1111-4 of the Public Health Code). Consent must be obtained during the course of a private meeting. Except in certain cases provided for by the law (some types of sample, biomedical research, etc.), the consent need not be in writing and signed by the patient.
E1 E2 E3 An organisation is defined allowing for the collection of informed consent and, if need be, refusal of treatment.
The patient’s participation and, if applicable, that of his entourage, in setting up and implementing the personalised treatment plan is encouraged.
Evaluation of the collection of patient consent leads to actions for improvement.
Measures aimed to obtain patient willingness to comply with the planned treatment are carried out if the patient has been hospitalised without consent, where there is a therapeutic injunction or when treatment is refused.
Criterion 11.c Patient information in the case of harm related to treatment.
E1 E2 E3 A structured patient information approach is defined for cases of treatment-related harm.
Professionals are trained in the structured approach to the information of the patient in the case of treatment-related harm.
The patient information system for cases of treatment-related harm is evaluated and improved.
The professionals implement this step.
Chapitre 2 Prise en charge du patient. Partie 1 Droits et place des patients.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 58/120 Manuel de certification – Édition novembre 2008
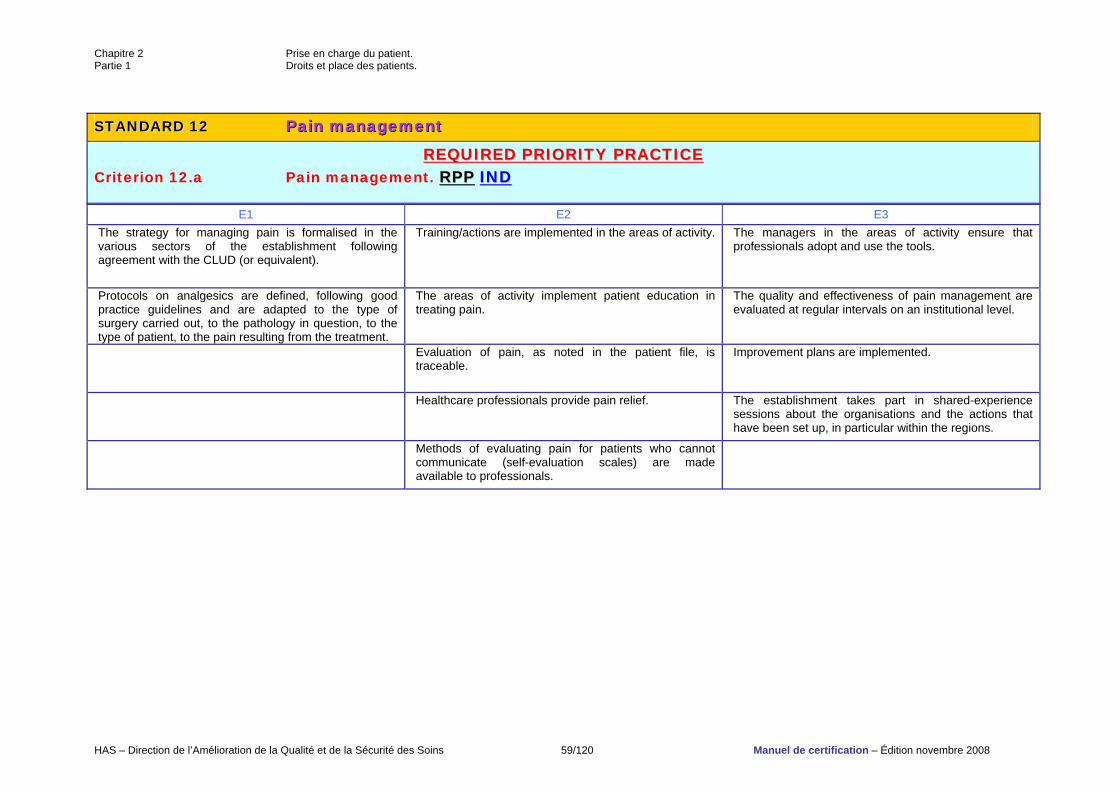
Chapitre 2 Prise en charge du patient. Partie 1 Droits et place des patients.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 59/120 Manuel de certification – Édition novembre 2008
SSTTAANNDDAARRDD 1122 PPaaiinn mmaannaaggeemmeenntt
RREEQQUUIIRREEDD PPRRIIOORRIITTYY PPRRAACCTTIICCEE Criterion 12.a Pain management. RRPPPP IINNDD
E1 E2 E3 The strategy for managing pain is formalised in the various sectors of the establishment following agreement with the CLUD (or equivalent).
Training/actions are implemented in the areas of activity. The managers in the areas of activity ensure that professionals adopt and use the tools.
Protocols on analgesics are defined, following good practice guidelines and are adapted to the type of surgery carried out, to the pathology in question, to the type of patient, to the pain resulting from the treatment.
The areas of activity implement patient education in treating pain.
The quality and effectiveness of pain management are evaluated at regular intervals on an institutional level.
Evaluation of pain, as noted in the patient file, is traceable.
Improvement plans are implemented.
Healthcare professionals provide pain relief. The establishment takes part in shared-experience sessions about the organisations and the actions that have been set up, in particular within the regions.
Methods of evaluating pain for patients who cannot communicate (self-evaluation scales) are made available to professionals.
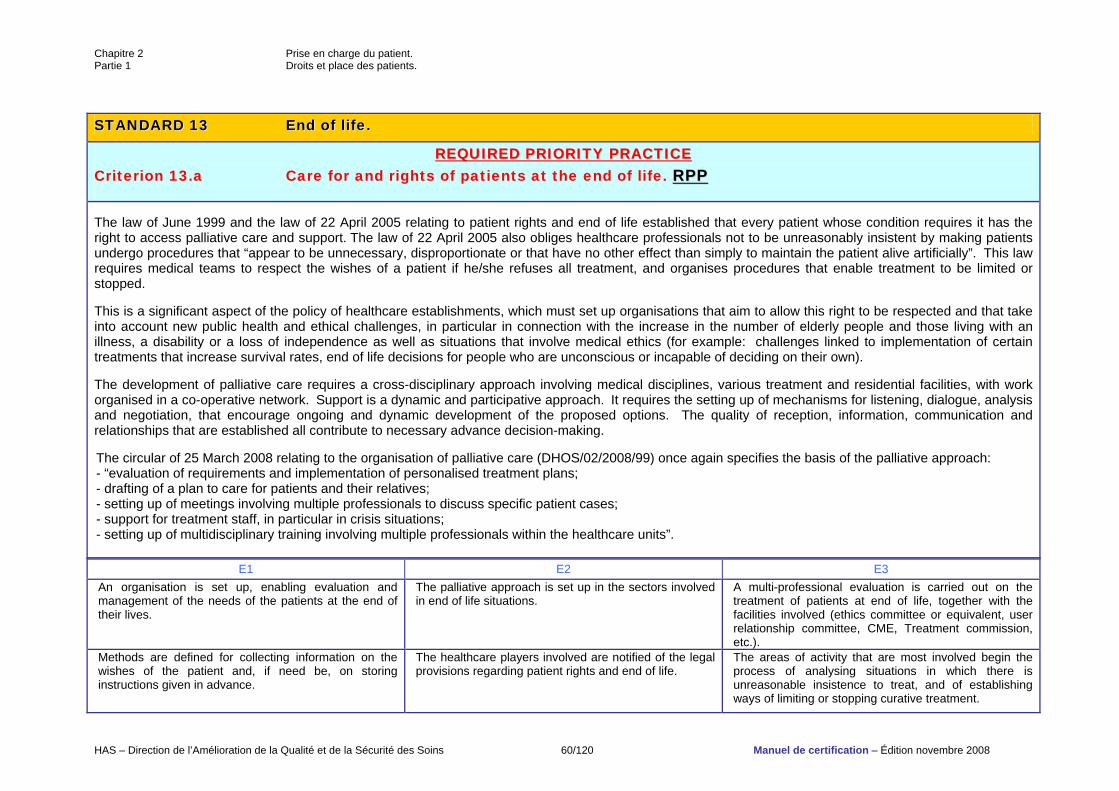
Chapitre 2 Prise en charge du patient. Partie 1 Droits et place des patients.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 60/120 Manuel de certification – Édition novembre 2008
SSTTAANNDDAARRDD 1133 EEnndd ooff lliiffee..
RREEQQUUIIRREEDD PPRRIIOORRIITTYY PPRRAACCTTIICCEE Criterion 13.a Care for and rights of patients at the end of life. RRPPPP The law of June 1999 and the law of 22 April 2005 relating to patient rights and end of life established that every patient whose condition requires it has the right to access palliative care and support. The law of 22 April 2005 also obliges healthcare professionals not to be unreasonably insistent by making patients undergo procedures that “appear to be unnecessary, disproportionate or that have no other effect than simply to maintain the patient alive artificially”. This law requires medical teams to respect the wishes of a patient if he/she refuses all treatment, and organises procedures that enable treatment to be limited or stopped. This is a significant aspect of the policy of healthcare establishments, which must set up organisations that aim to allow this right to be respected and that take into account new public health and ethical challenges, in particular in connection with the increase in the number of elderly people and those living with an illness, a disability or a loss of independence as well as situations that involve medical ethics (for example: challenges linked to implementation of certain treatments that increase survival rates, end of life decisions for people who are unconscious or incapable of deciding on their own). The development of palliative care requires a cross-disciplinary approach involving medical disciplines, various treatment and residential facilities, with work organised in a co-operative network. Support is a dynamic and participative approach. It requires the setting up of mechanisms for listening, dialogue, analysis and negotiation, that encourage ongoing and dynamic development of the proposed options. The quality of reception, information, communication and relationships that are established all contribute to necessary advance decision-making. The circular of 25 March 2008 relating to the organisation of palliative care (DHOS/02/2008/99) once again specifies the basis of the palliative approach: - “evaluation of requirements and implementation of personalised treatment plans; - drafting of a plan to care for patients and their relatives; - setting up of meetings involving multiple professionals to discuss specific patient cases; - support for treatment staff, in particular in crisis situations; - setting up of multidisciplinary training involving multiple professionals within the healthcare units”.
E1 E2 E3 An organisation is set up, enabling evaluation and management of the needs of the patients at the end of their lives.
The palliative approach is set up in the sectors involved in end of life situations.
A multi-professional evaluation is carried out on the treatment of patients at end of life, together with the facilities involved (ethics committee or equivalent, user relationship committee, CME, Treatment commission, etc.).
Methods are defined for collecting information on the wishes of the patient and, if need be, on storing instructions given in advance.
The healthcare players involved are notified of the legal provisions regarding patient rights and end of life.
The areas of activity that are most involved begin the process of analysing situations in which there is unreasonable insistence to treat, and of establishing ways of limiting or stopping curative treatment.
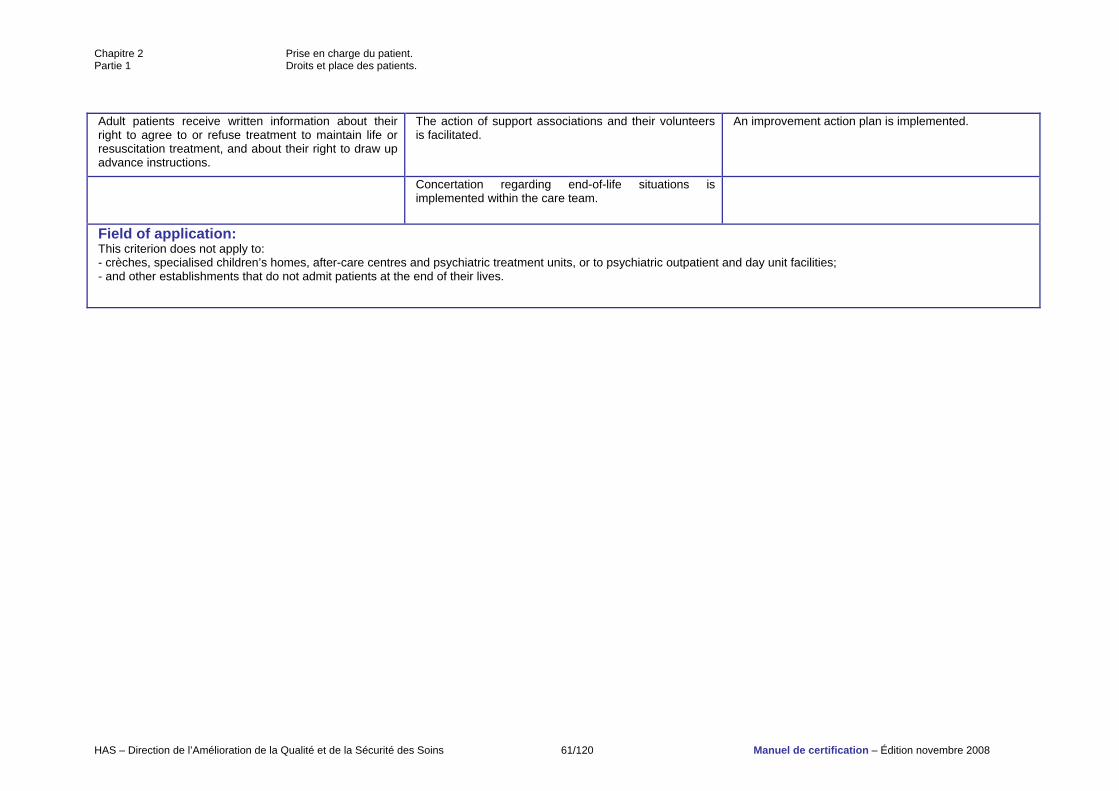
Chapitre 2 Prise en charge du patient. Partie 1 Droits et place des patients.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 61/120 Manuel de certification – Édition novembre 2008
Adult patients receive written information about their right to agree to or refuse treatment to maintain life or resuscitation treatment, and about their right to draw up advance instructions.
The action of support associations and their volunteers is facilitated.
An improvement action plan is implemented.
Concertation regarding end-of-life situations is implemented within the care team.
Field of application: This criterion does not apply to: - crèches, specialised children’s homes, after-care centres and psychiatric treatment units, or to psychiatric outpatient and day unit facilities; - and other establishments that do not admit patients at the end of their lives.
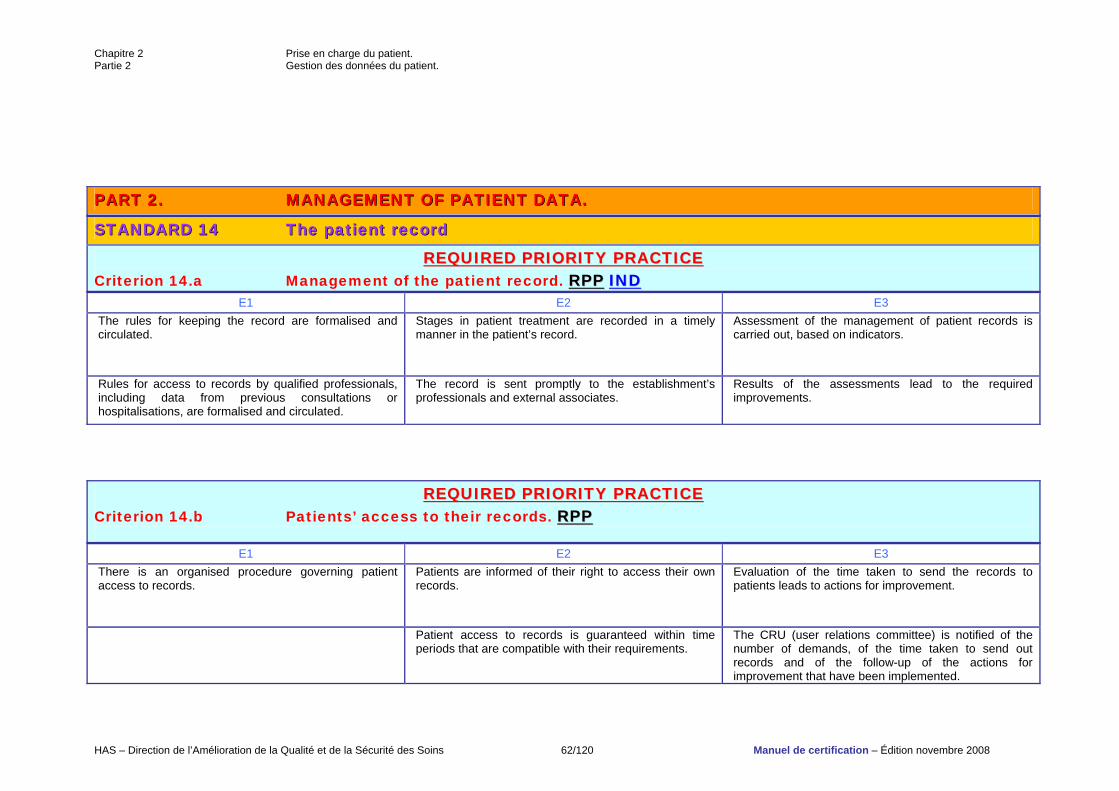
Chapitre 2 Prise en charge du patient. Partie 2 Gestion des données du patient.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 62/120 Manuel de certification – Édition novembre 2008
PPAARRTT 22.. MMAANNAAGGEEMMEENNTT OOFF PPAATTIIEENNTT DDAATTAA..
SSTTAANNDDAARRDD 1144 TThhee ppaattiieenntt rreeccoorrdd
RREEQQUUIIRREEDD PPRRIIOORRIITTYY PPRRAACCTTIICCEE Criterion 14.a Management of the patient record. RRPPPP IINNDD
E1 E2 E3 The rules for keeping the record are formalised and circulated.
Stages in patient treatment are recorded in a timely manner in the patient’s record.
Assessment of the management of patient records is carried out, based on indicators.
Rules for access to records by qualified professionals, including data from previous consultations or hospitalisations, are formalised and circulated.
The record is sent promptly to the establishment’s professionals and external associates.
Results of the assessments lead to the required improvements.
RREEQQUUIIRREEDD PPRRIIOORRIITTYY PPRRAACCTTIICCEE Criterion 14.b Patients’ access to their records. RRPPPP
E1 E2 E3 There is an organised procedure governing patient access to records.
Patients are informed of their right to access their own records.
Evaluation of the time taken to send the records to patients leads to actions for improvement.
Patient access to records is guaranteed within time periods that are compatible with their requirements.
The CRU (user relations committee) is notified of the number of demands, of the time taken to send out records and of the follow-up of the actions for improvement that have been implemented.
Chapitre 2 Prise en charge du patient. Partie 2 Gestion des données du patient.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 63/120 Manuel de certification – Édition novembre 2008
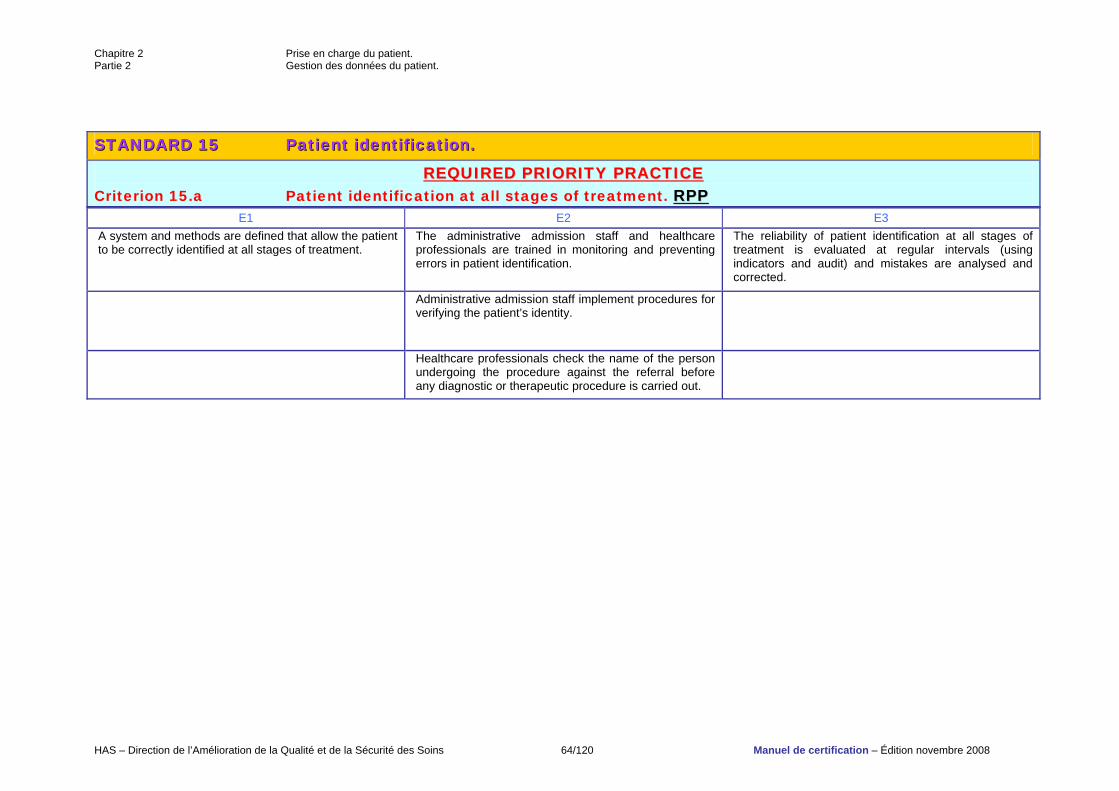
Chapitre 2 Prise en charge du patient. Partie 2 Gestion des données du patient.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 64/120 Manuel de certification – Édition novembre 2008
SSTTAANNDDAARRDD 1155 PPaattiieenntt iiddeennttiiffiiccaattiioonn..
RREEQQUUIIRREEDD PPRRIIOORRIITTYY PPRRAACCTTIICCEE Criterion 15.a Patient identification at all stages of treatment. RRPPPP
E1 E2 E3 A system and methods are defined that allow the patient to be correctly identified at all stages of treatment.
The administrative admission staff and healthcare professionals are trained in monitoring and preventing errors in patient identification.
The reliability of patient identification at all stages of treatment is evaluated at regular intervals (using indicators and audit) and mistakes are analysed and corrected.
Administrative admission staff implement procedures for verifying the patient’s identity.
Healthcare professionals check the name of the person undergoing the procedure against the referral before any diagnostic or therapeutic procedure is carried out.
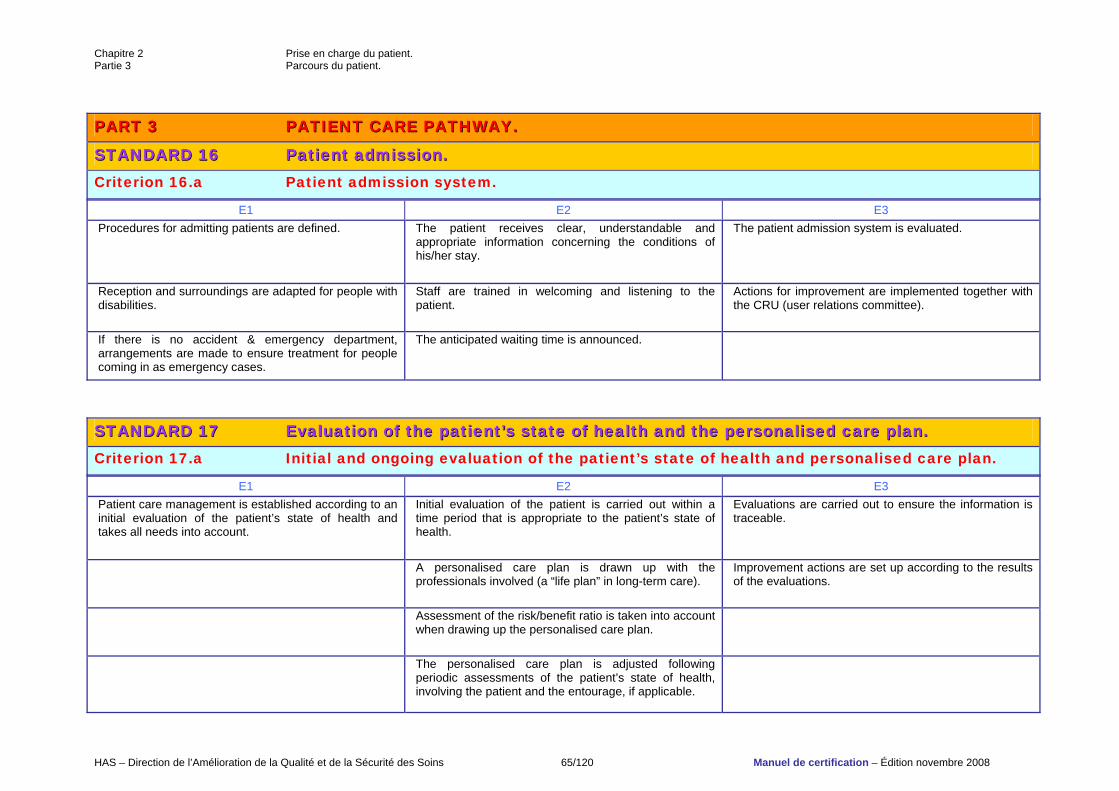
Chapitre 2 Prise en charge du patient. Partie 3 Parcours du patient.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 65/120 Manuel de certification – Édition novembre 2008
PPAARRTT 33 PPAATTIIEENNTT CCAARREE PPAATTHHWWAAYY..
SSTTAANNDDAARRDD 1166 PPaattiieenntt aaddmmiissssiioonn.. Criterion 16.a Patient admission system.
E1 E2 E3 Procedures for admitting patients are defined. The patient receives clear, understandable and
appropriate information concerning the conditions of his/her stay.
The patient admission system is evaluated.
Reception and surroundings are adapted for people with disabilities.
Staff are trained in welcoming and listening to the patient.
Actions for improvement are implemented together with the CRU (user relations committee).
If there is no accident & emergency department, arrangements are made to ensure treatment for people coming in as emergency cases.
The anticipated waiting time is announced.
SSTTAANNDDAARRDD 1177 EEvvaalluuaattiioonn ooff tthhee ppaattiieenntt’’ss ssttaattee ooff hheeaalltthh aanndd tthhee ppeerrssoonnaalliisseedd ccaarree ppllaann.. Criterion 17.a Initial and ongoing evaluation of the patient’s state of health and personalised care plan.
E1 E2 E3 Patient care management is established according to an initial evaluation of the patient’s state of health and takes all needs into account.
Initial evaluation of the patient is carried out within a time period that is appropriate to the patient’s state of health.
Evaluations are carried out to ensure the information is traceable.
A personalised care plan is drawn up with the professionals involved (a “life plan” in long-term care).
Improvement actions are set up according to the results of the evaluations.
Assessment of the risk/benefit ratio is taken into account when drawing up the personalised care plan.
The personalised care plan is adjusted following periodic assessments of the patient’s state of health, involving the patient and the entourage, if applicable.
Chapitre 2 Prise en charge du patient. Partie 3 Parcours du patient.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 66/120 Manuel de certification – Édition novembre 2008
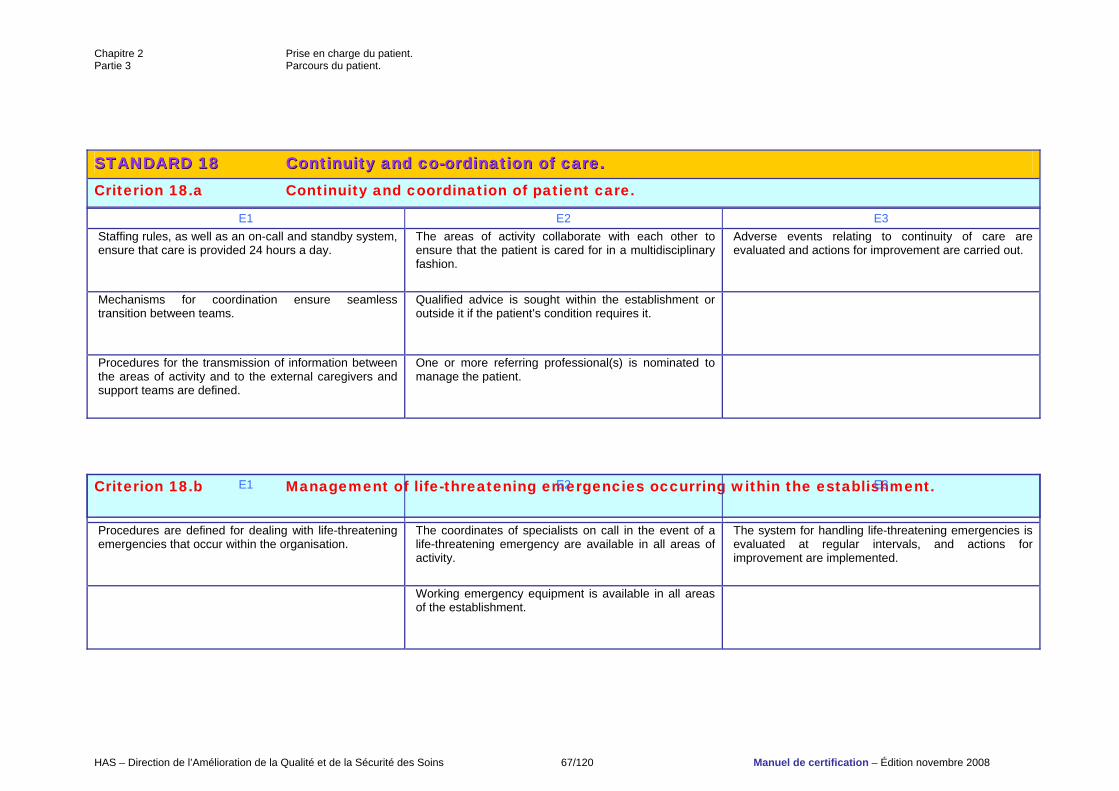
Chapitre 2 Prise en charge du patient. Partie 3 Parcours du patient.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 67/120 Manuel de certification – Édition novembre 2008
SSTTAANNDDAARRDD 1188 CCoonnttiinnuuiittyy aanndd ccoo--oorrddiinnaattiioonn ooff ccaarree.. Criterion 18.a Continuity and coordination of patient care.
E1 E2 E3 Staffing rules, as well as an on-call and standby system, ensure that care is provided 24 hours a day.
The areas of activity collaborate with each other to ensure that the patient is cared for in a multidisciplinary fashion.
Adverse events relating to continuity of care are evaluated and actions for improvement are carried out.
Mechanisms for coordination ensure seamless transition between teams.
Qualified advice is sought within the establishment or outside it if the patient’s condition requires it.
Procedures for the transmission of information between the areas of activity and to the external caregivers and support teams are defined.
One or more referring professional(s) is nominated to manage the patient.
Criterion 18.b Management of life-threatening emergencies occurring within the establishment.
E1 E2 E3
Procedures are defined for dealing with life-threatening emergencies that occur within the organisation.
The coordinates of specialists on call in the event of a life-threatening emergency are available in all areas of activity.
The system for handling life-threatening emergencies is evaluated at regular intervals, and actions for improvement are implemented.
Working emergency equipment is available in all areas of the establishment.
Chapitre 2 Prise en charge du patient. Partie 3 Parcours du patient.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 68/120 Manuel de certification – Édition novembre 2008
Training is provided to professionals in the use of this equipment and first aid procedures.
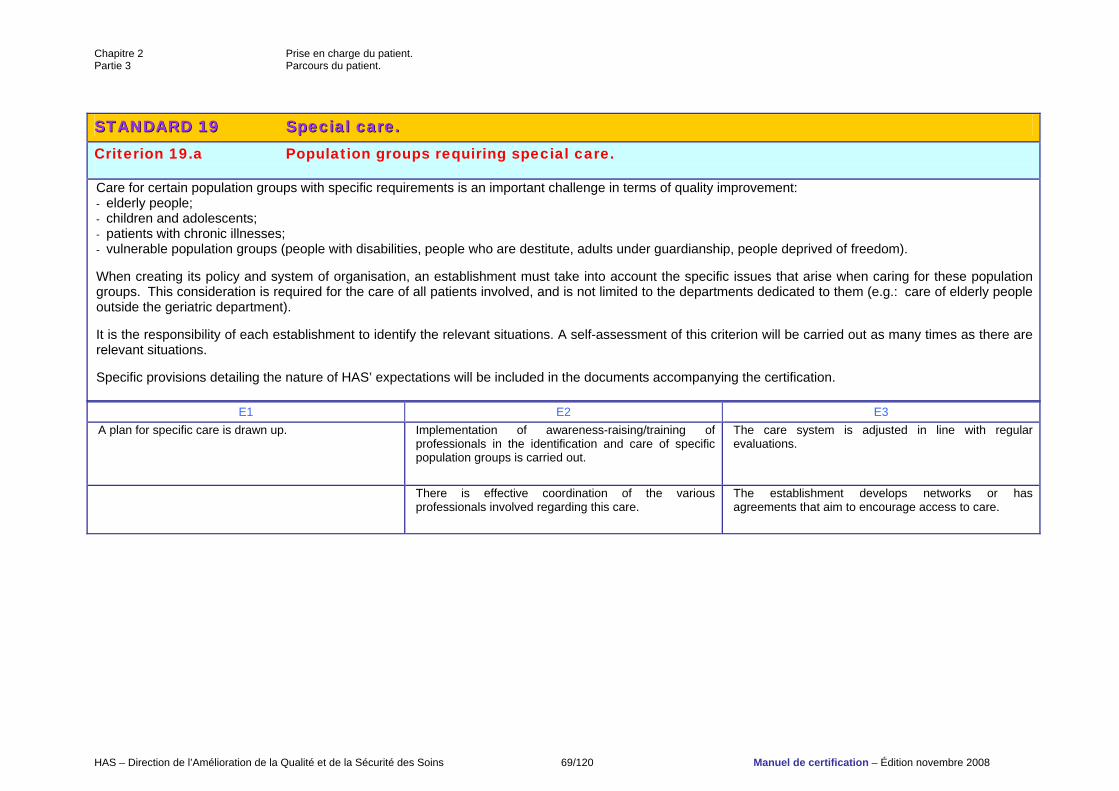
Chapitre 2 Prise en charge du patient. Partie 3 Parcours du patient.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 69/120 Manuel de certification – Édition novembre 2008
SSTTAANNDDAARRDD 1199 SSppeecciiaall ccaarree.. Criterion 19.a Population groups requiring special care. Care for certain population groups with specific requirements is an important challenge in terms of quality improvement: - elderly people; - children and adolescents; - patients with chronic illnesses; - vulnerable population groups (people with disabilities, people who are destitute, adults under guardianship, people deprived of freedom). When creating its policy and system of organisation, an establishment must take into account the specific issues that arise when caring for these population groups. This consideration is required for the care of all patients involved, and is not limited to the departments dedicated to them (e.g.: care of elderly people outside the geriatric department). It is the responsibility of each establishment to identify the relevant situations. A self-assessment of this criterion will be carried out as many times as there are relevant situations. Specific provisions detailing the nature of HAS’ expectations will be included in the documents accompanying the certification.
E1 E2 E3 A plan for specific care is drawn up. Implementation of awareness-raising/training of
professionals in the identification and care of specific population groups is carried out.
The care system is adjusted in line with regular evaluations.
There is effective coordination of the various professionals involved regarding this care.
The establishment develops networks or has agreements that aim to encourage access to care.
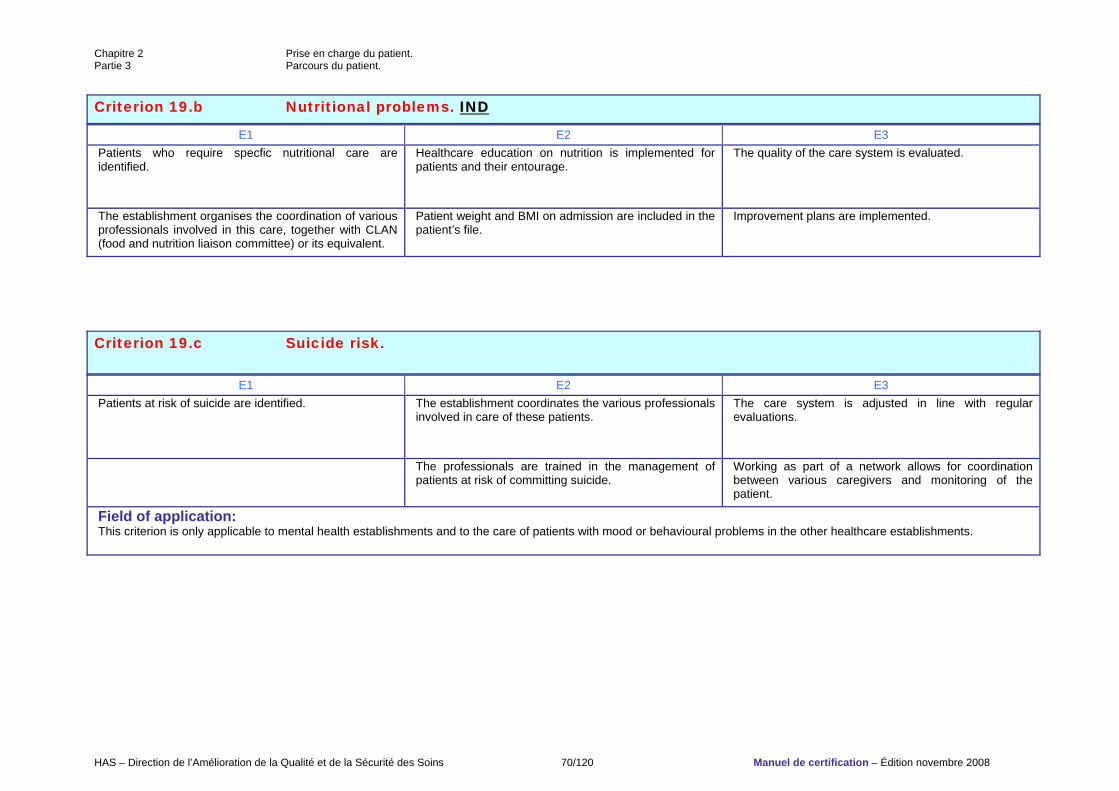
Chapitre 2 Prise en charge du patient. Partie 3 Parcours du patient.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 70/120 Manuel de certification – Édition novembre 2008
Criterion 19.b Nutritional problems. IINNDD
E1 E2 E3 Patients who require specfic nutritional care are identified.
Healthcare education on nutrition is implemented for patients and their entourage.
The quality of the care system is evaluated.
The establishment organises the coordination of various professionals involved in this care, together with CLAN (food and nutrition liaison committee) or its equivalent.
Patient weight and BMI on admission are included in the patient’s file.
Improvement plans are implemented.
Criterion 19.c Suicide risk.
E1 E2 E3 Patients at risk of suicide are identified. The establishment coordinates the various professionals
involved in care of these patients. The care system is adjusted in line with regular evaluations.
The professionals are trained in the management of patients at risk of committing suicide.
Working as part of a network allows for coordination between various caregivers and monitoring of the patient.
Field of application: This criterion is only applicable to mental health establishments and to the care of patients with mood or behavioural problems in the other healthcare establishments.
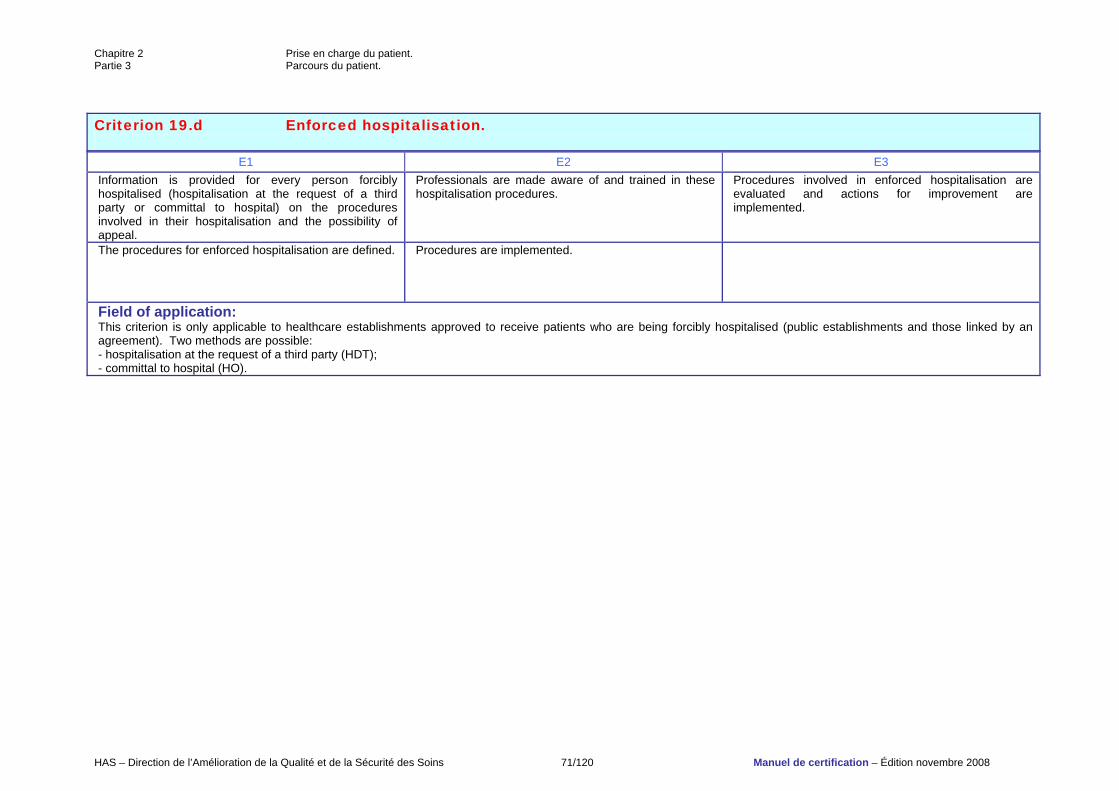
Chapitre 2 Prise en charge du patient. Partie 3 Parcours du patient.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 71/120 Manuel de certification – Édition novembre 2008
Criterion 19.d Enforced hospitalisation.
E1 E2 E3 Information is provided for every person forcibly hospitalised (hospitalisation at the request of a third party or committal to hospital) on the procedures involved in their hospitalisation and the possibility of appeal.
Professionals are made aware of and trained in these hospitalisation procedures.
Procedures involved in enforced hospitalisation are evaluated and actions for improvement are implemented.
The procedures for enforced hospitalisation are defined. Procedures are implemented.
Field of application: This criterion is only applicable to healthcare establishments approved to receive patients who are being forcibly hospitalised (public establishments and those linked by an agreement). Two methods are possible: - hospitalisation at the request of a third party (HDT); - committal to hospital (HO).
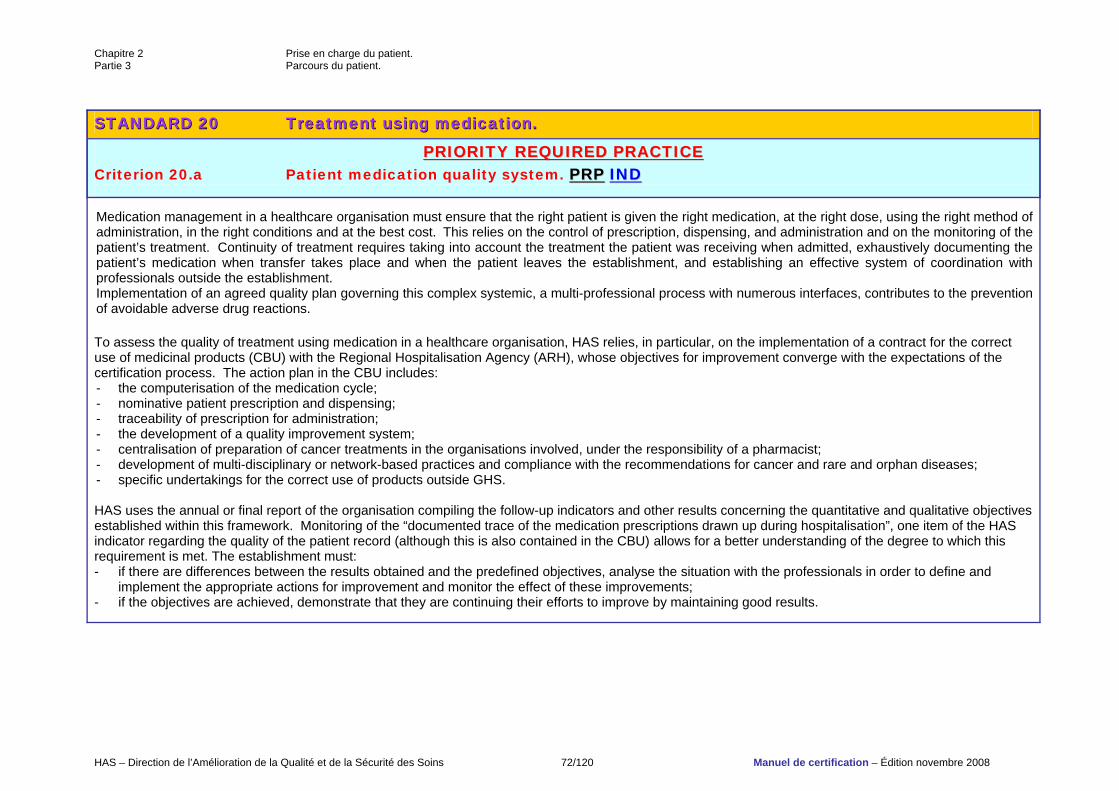
Chapitre 2 Prise en charge du patient. Partie 3 Parcours du patient.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 72/120 Manuel de certification – Édition novembre 2008
SSTTAANNDDAARRDD 2200 TTrreeaattmmeenntt uussiinngg mmeeddiiccaattiioonn..
PPRRIIOORRIITTYY RREEQQUUIIRREEDD PPRRAACCTTIICCEE Criterion 20.a Patient medication quality system. PPRRPP IINNDD
Medication management in a healthcare organisation must ensure that the right patient is given the right medication, at the right dose, using the right method of administration, in the right conditions and at the best cost. This relies on the control of prescription, dispensing, and administration and on the monitoring of the patient’s treatment. Continuity of treatment requires taking into account the treatment the patient was receiving when admitted, exhaustively documenting the patient’s medication when transfer takes place and when the patient leaves the establishment, and establishing an effective system of coordination with professionals outside the establishment. Implementation of an agreed quality plan governing this complex systemic, a multi-professional process with numerous interfaces, contributes to the prevention of avoidable adverse drug reactions. To assess the quality of treatment using medication in a healthcare organisation, HAS relies, in particular, on the implementation of a contract for the correct use of medicinal products (CBU) with the Regional Hospitalisation Agency (ARH), whose objectives for improvement converge with the expectations of the certification process. The action plan in the CBU includes: - the computerisation of the medication cycle; - nominative patient prescription and dispensing; - traceability of prescription for administration; - the development of a quality improvement system; - centralisation of preparation of cancer treatments in the organisations involved, under the responsibility of a pharmacist; - development of multi-disciplinary or network-based practices and compliance with the recommendations for cancer and rare and orphan diseases; - specific undertakings for the correct use of products outside GHS. HAS uses the annual or final report of the organisation compiling the follow-up indicators and other results concerning the quantitative and qualitative objectives established within this framework. Monitoring of the “documented trace of the medication prescriptions drawn up during hospitalisation”, one item of the HAS indicator regarding the quality of the patient record (although this is also contained in the CBU) allows for a better understanding of the degree to which this requirement is met. The establishment must: - if there are differences between the results obtained and the predefined objectives, analyse the situation with the professionals in order to define and
implement the appropriate actions for improvement and monitor the effect of these improvements; - if the objectives are achieved, demonstrate that they are continuing their efforts to improve by maintaining good results.
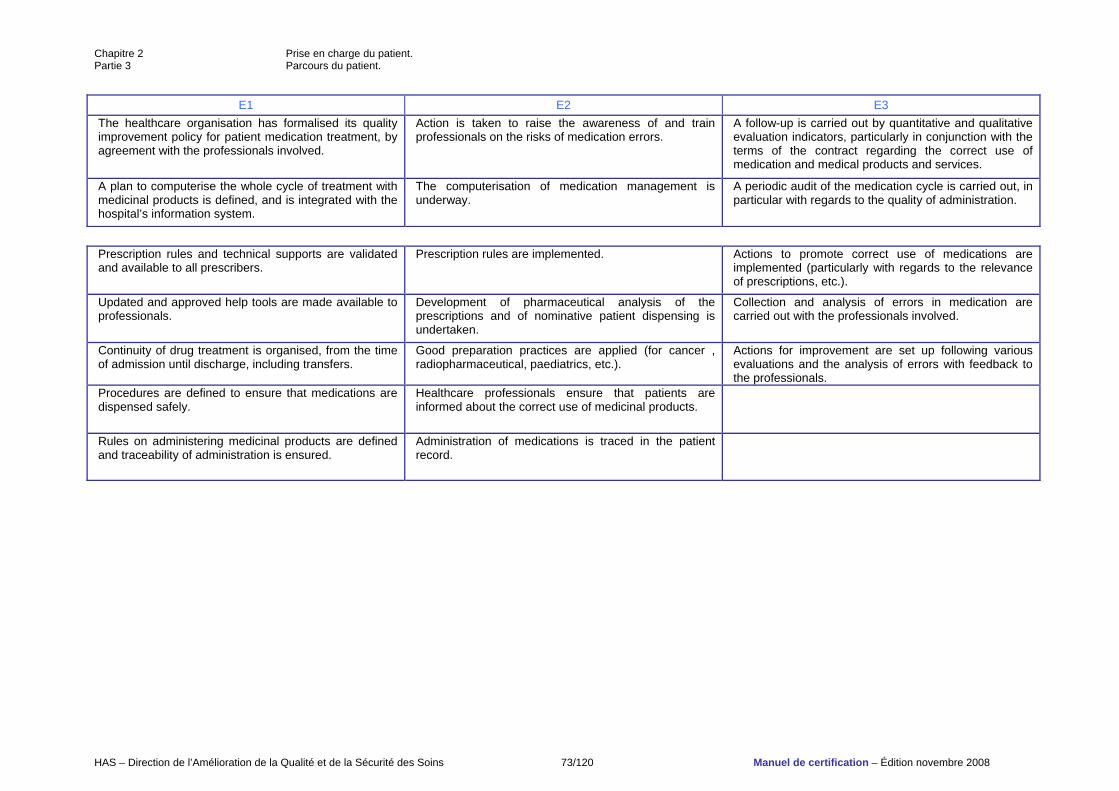
Chapitre 2 Prise en charge du patient. Partie 3 Parcours du patient.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 73/120 Manuel de certification – Édition novembre 2008
E1 E2 E3 The healthcare organisation has formalised its quality improvement policy for patient medication treatment, by agreement with the professionals involved.
Action is taken to raise the awareness of and train professionals on the risks of medication errors.
A follow-up is carried out by quantitative and qualitative evaluation indicators, particularly in conjunction with the terms of the contract regarding the correct use of medication and medical products and services.
A plan to computerise the whole cycle of treatment with medicinal products is defined, and is integrated with the hospital’s information system.
The computerisation of medication management is underway.
A periodic audit of the medication cycle is carried out, in particular with regards to the quality of administration.
Prescription rules and technical supports are validated and available to all prescribers.
Prescription rules are implemented. Actions to promote correct use of medications are implemented (particularly with regards to the relevance of prescriptions, etc.).
Updated and approved help tools are made available to professionals.
Development of pharmaceutical analysis of the prescriptions and of nominative patient dispensing is undertaken.
Collection and analysis of errors in medication are carried out with the professionals involved.
Continuity of drug treatment is organised, from the time of admission until discharge, including transfers.
Good preparation practices are applied (for cancer , radiopharmaceutical, paediatrics, etc.).
Actions for improvement are set up following various evaluations and the analysis of errors with feedback to the professionals.
Procedures are defined to ensure that medications are dispensed safely.
Healthcare professionals ensure that patients are informed about the correct use of medicinal products.
Rules on administering medicinal products are defined and traceability of administration is ensured.
Administration of medications is traced in the patient record.
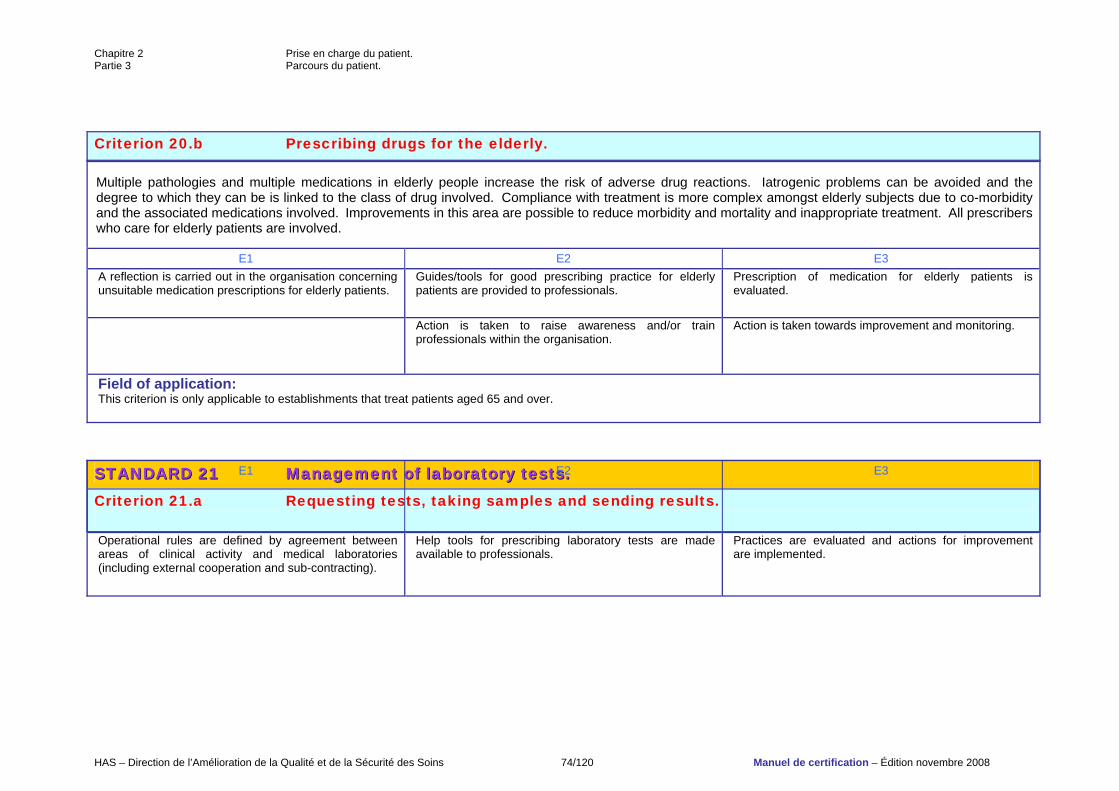
Chapitre 2 Prise en charge du patient. Partie 3 Parcours du patient.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 74/120 Manuel de certification – Édition novembre 2008
Criterion 20.b Prescribing drugs for the elderly. Multiple pathologies and multiple medications in elderly people increase the risk of adverse drug reactions. Iatrogenic problems can be avoided and the degree to which they can be is linked to the class of drug involved. Compliance with treatment is more complex amongst elderly subjects due to co-morbidity and the associated medications involved. Improvements in this area are possible to reduce morbidity and mortality and inappropriate treatment. All prescribers who care for elderly patients are involved.
E1 E2 E3 A reflection is carried out in the organisation concerning unsuitable medication prescriptions for elderly patients.
Guides/tools for good prescribing practice for elderly patients are provided to professionals.
Prescription of medication for elderly patients is evaluated.
Action is taken to raise awareness and/or train professionals within the organisation.
Action is taken towards improvement and monitoring.
Field of application: This criterion is only applicable to establishments that treat patients aged 65 and over.
SSTTAANNDDAARRDD 2211 MMaannaaggeemmeenntt ooff llaabboorraattoorryy tteessttss.. Criterion 21.a Requesting tests, taking samples and sending results.
E1 E2 E3
Operational rules are defined by agreement between areas of clinical activity and medical laboratories (including external cooperation and sub-contracting).
Help tools for prescribing laboratory tests are made available to professionals.
Practices are evaluated and actions for improvement are implemented.
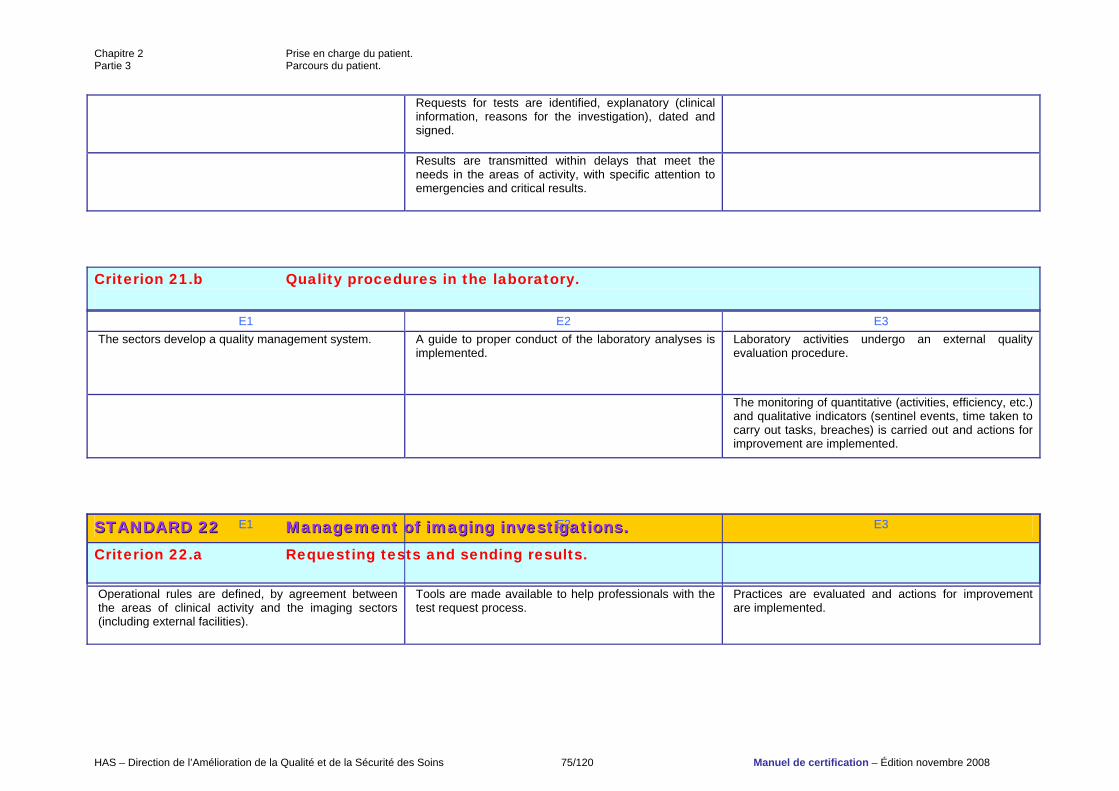
Chapitre 2 Prise en charge du patient. Partie 3 Parcours du patient.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 75/120 Manuel de certification – Édition novembre 2008
Requests for tests are identified, explanatory (clinical information, reasons for the investigation), dated and signed.
Results are transmitted within delays that meet the needs in the areas of activity, with specific attention to emergencies and critical results.
Criterion 21.b Quality procedures in the laboratory.
E1 E2 E3 The sectors develop a quality management system. A guide to proper conduct of the laboratory analyses is
implemented.
Laboratory activities undergo an external quality evaluation procedure.
The monitoring of quantitative (activities, efficiency, etc.) and qualitative indicators (sentinel events, time taken to carry out tasks, breaches) is carried out and actions for improvement are implemented.
SSTTAANNDDAARRDD 2222 MMaannaaggeemmeenntt ooff iimmaaggiinngg iinnvveessttiiggaattiioonnss.. Criterion 22.a Requesting tests and sending results.
E1 E2 E3
Operational rules are defined, by agreement between the areas of clinical activity and the imaging sectors (including external facilities).
Tools are made available to help professionals with the test request process.
Practices are evaluated and actions for improvement are implemented.
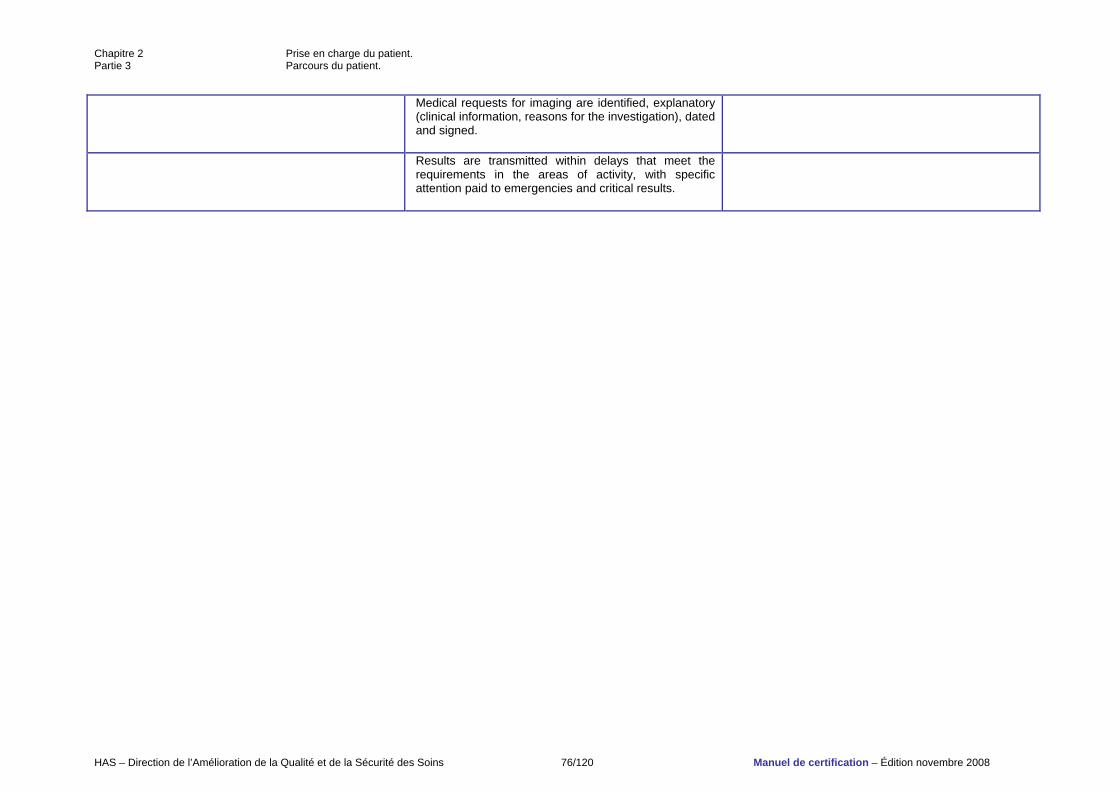
Chapitre 2 Prise en charge du patient. Partie 3 Parcours du patient.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 76/120 Manuel de certification – Édition novembre 2008
Medical requests for imaging are identified, explanatory (clinical information, reasons for the investigation), dated and signed.
Results are transmitted within delays that meet the requirements in the areas of activity, with specific attention paid to emergencies and critical results.
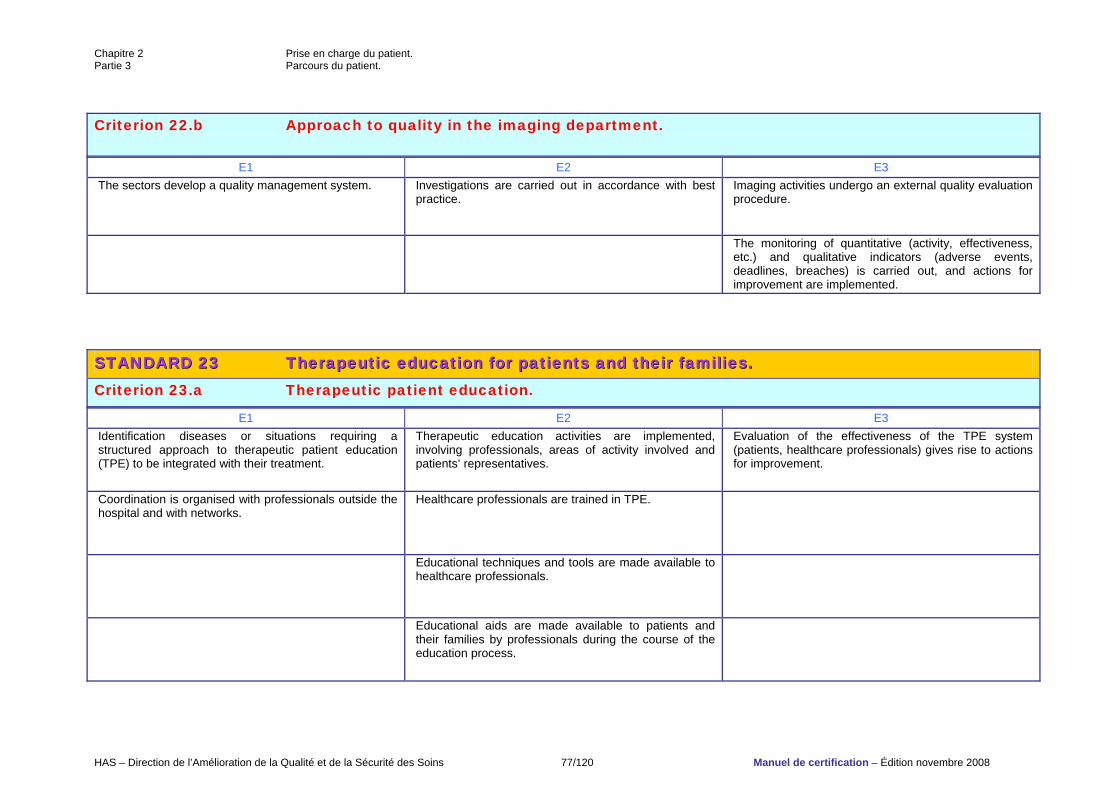
Chapitre 2 Prise en charge du patient. Partie 3 Parcours du patient.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 77/120 Manuel de certification – Édition novembre 2008
Criterion 22.b Approach to quality in the imaging department.
E1 E2 E3 The sectors develop a quality management system. Investigations are carried out in accordance with best
practice. Imaging activities undergo an external quality evaluation procedure.
The monitoring of quantitative (activity, effectiveness, etc.) and qualitative indicators (adverse events, deadlines, breaches) is carried out, and actions for improvement are implemented.
SSTTAANNDDAARRDD 2233 TThheerraappeeuuttiicc eedduuccaattiioonn ffoorr ppaattiieennttss aanndd tthheeiirr ffaammiilliieess.. Criterion 23.a Therapeutic patient education.
E1 E2 E3 Identification diseases or situations requiring a structured approach to therapeutic patient education (TPE) to be integrated with their treatment.
Therapeutic education activities are implemented, involving professionals, areas of activity involved and patients’ representatives.
Evaluation of the effectiveness of the TPE system (patients, healthcare professionals) gives rise to actions for improvement.
Coordination is organised with professionals outside the hospital and with networks.
Healthcare professionals are trained in TPE.
Educational techniques and tools are made available to healthcare professionals.
Educational aids are made available to patients and their families by professionals during the course of the education process.
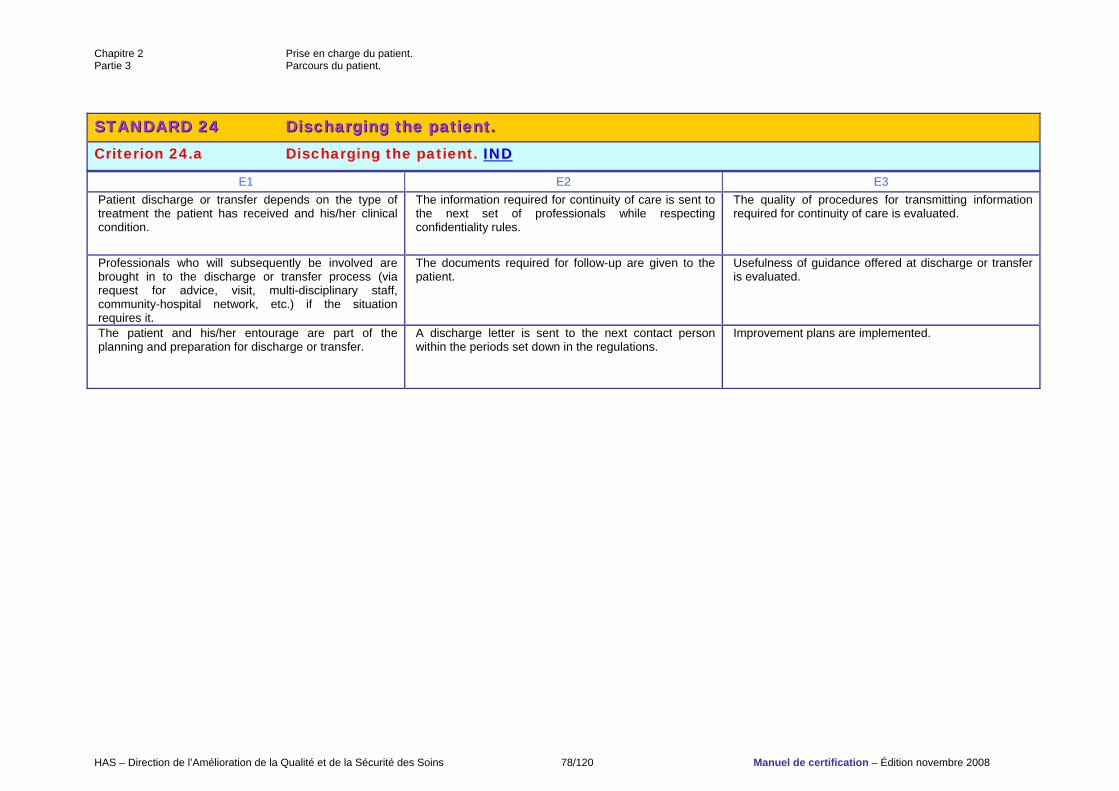
Chapitre 2 Prise en charge du patient. Partie 3 Parcours du patient.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 78/120 Manuel de certification – Édition novembre 2008
SSTTAANNDDAARRDD 2244 DDiisscchhaarrggiinngg tthhee ppaattiieenntt.. Criterion 24.a Discharging the patient. IINNDD
E1 E2 E3 Patient discharge or transfer depends on the type of treatment the patient has received and his/her clinical condition.
The information required for continuity of care is sent to the next set of professionals while respecting confidentiality rules.
The quality of procedures for transmitting information required for continuity of care is evaluated.
Professionals who will subsequently be involved are brought in to the discharge or transfer process (via request for advice, visit, multi-disciplinary staff, community-hospital network, etc.) if the situation requires it.
The documents required for follow-up are given to the patient.
Usefulness of guidance offered at discharge or transfer is evaluated.
The patient and his/her entourage are part of the planning and preparation for discharge or transfer.
A discharge letter is sent to the next contact person within the periods set down in the regulations.
Improvement plans are implemented.
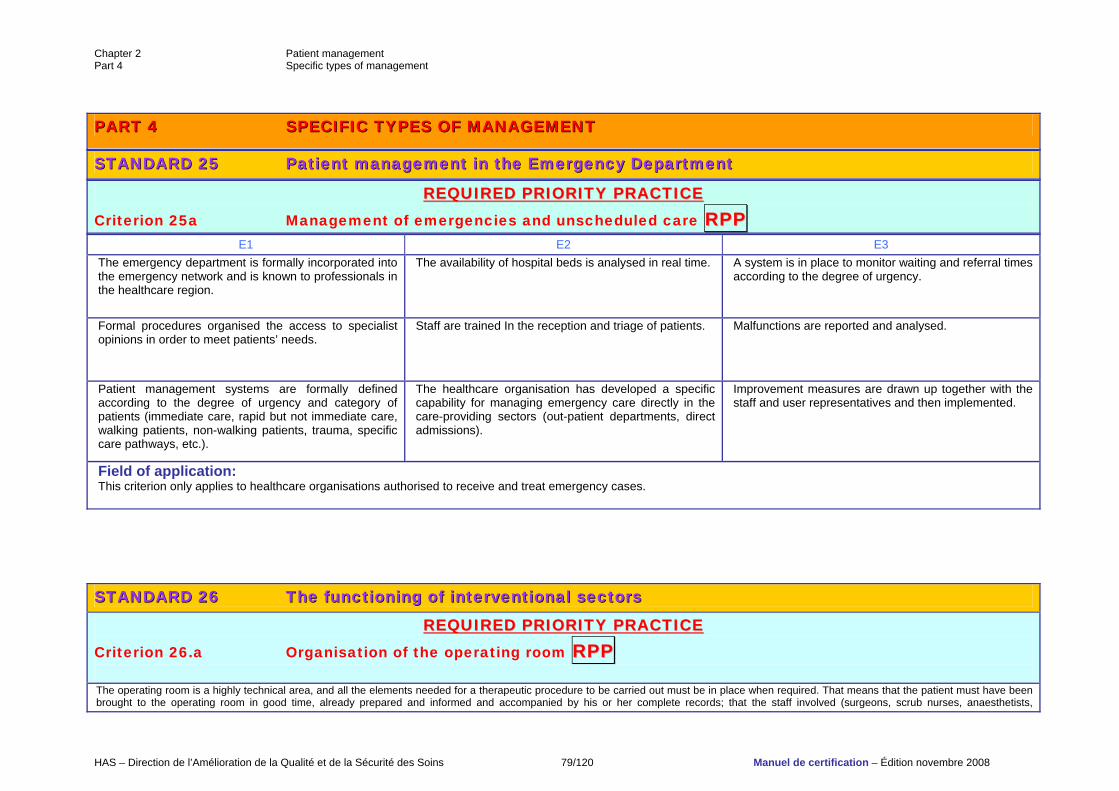
Chapter 2 Patient management Part 4 Specific types of management
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 79/120 Manuel de certification – Édition novembre 2008
RREEQQUUIIRREEDD PPRRIIOORRIITTYY PPRRAACCTTIICCEE Criterion 25a Management of emergencies and unscheduled care RRPPPP
PPAARRTT 44 SSPPEECCIIFFIICC TTYYPPEESS OOFF MMAANNAAGGEEMMEENNTT
SSTTAANNDDAARRDD 2255 PPaattiieenntt mmaannaaggeemmeenntt iinn tthhee EEmmeerrggeennccyy DDeeppaarrttmmeenntt
E1 E2 E3 The emergency department is formally incorporated into the emergency network and is known to professionals in the healthcare region.
The availability of hospital beds is analysed in real time.
A system is in place to monitor waiting and referral times according to the degree of urgency.
Formal procedures organised the access to specialist opinions in order to meet patients’ needs.
Staff are trained In the reception and triage of patients.
Malfunctions are reported and analysed.
Patient management systems are formally defined according to the degree of urgency and category of patients (immediate care, rapid but not immediate care, walking patients, non-walking patients, trauma, specific care pathways, etc.).
The healthcare organisation has developed a specific capability for managing emergency care directly in the care-providing sectors (out-patient departments, direct admissions).
Improvement measures are drawn up together with the staff and user representatives and then implemented.
Field of application: This criterion only applies to healthcare organisations authorised to receive and treat emergency cases.
SSTTAANNDDAARRDD 2266 TThhee ffuunnccttiioonniinngg ooff iinntteerrvveennttiioonnaall sseeccttoorrss
RREEQQUUIIRREEDD PPRRIIOORRIITTYY PPRRAACCTTIICCEE Criterion 26.a Organisation of the operating room RRPPPP The operating room is a highly technical area, and all the elements needed for a therapeutic procedure to be carried out must be in place when required. That means that the patient must have been brought to the operating room in good time, already prepared and informed and accompanied by his or her complete records; that the staff involved (surgeons, scrub nurses, anaesthetists,
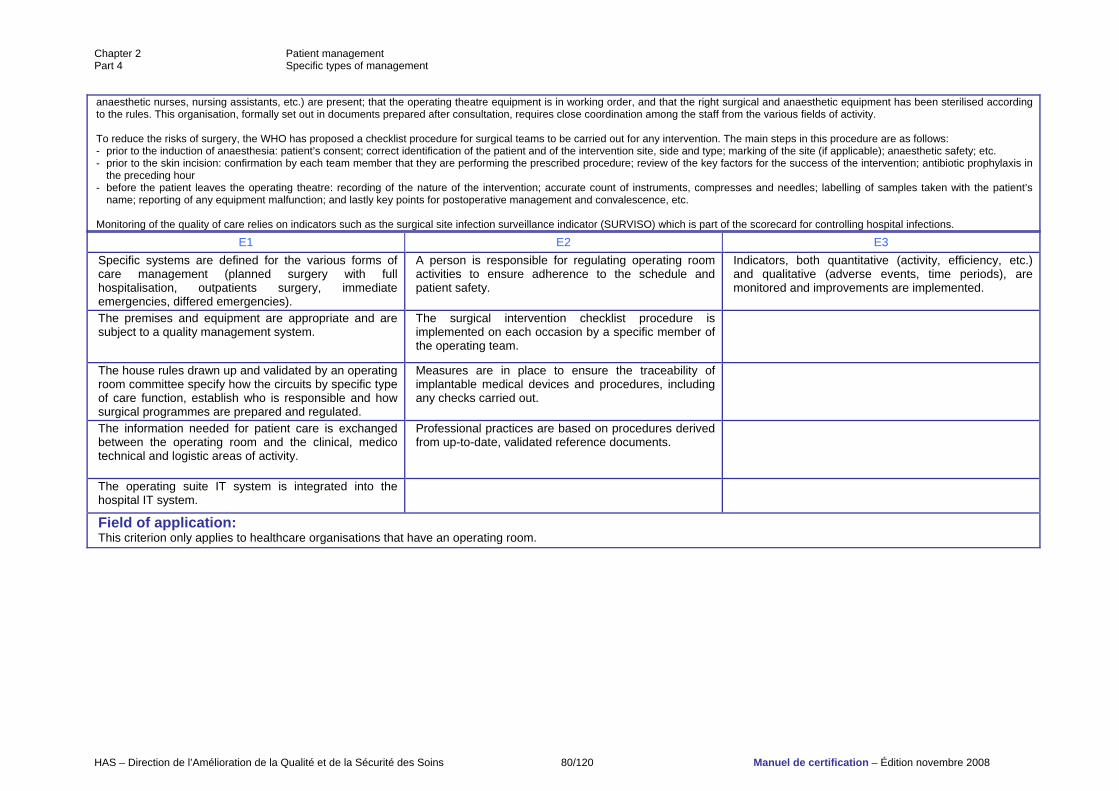
Chapter 2 Patient management Part 4 Specific types of management
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 80/120 Manuel de certification – Édition novembre 2008
anaesthetic nurses, nursing assistants, etc.) are present; that the operating theatre equipment is in working order, and that the right surgical and anaesthetic equipment has been sterilised according to the rules. This organisation, formally set out in documents prepared after consultation, requires close coordination among the staff from the various fields of activity. To reduce the risks of surgery, the WHO has proposed a checklist procedure for surgical teams to be carried out for any intervention. The main steps in this procedure are as follows: - prior to the induction of anaesthesia: patient’s consent; correct identification of the patient and of the intervention site, side and type; marking of the site (if applicable); anaesthetic safety; etc. - prior to the skin incision: confirmation by each team member that they are performing the prescribed procedure; review of the key factors for the success of the intervention; antibiotic prophylaxis in
the preceding hour - before the patient leaves the operating theatre: recording of the nature of the intervention; accurate count of instruments, compresses and needles; labelling of samples taken with the patient’s
name; reporting of any equipment malfunction; and lastly key points for postoperative management and convalescence, etc. Monitoring of the quality of care relies on indicators such as the surgical site infection surveillance indicator (SURVISO) which is part of the scorecard for controlling hospital infections.
E1 E2 E3 Specific systems are defined for the various forms of care management (planned surgery with full hospitalisation, outpatients surgery, immediate emergencies, differed emergencies).
A person is responsible for regulating operating room activities to ensure adherence to the schedule and patient safety.
Indicators, both quantitative (activity, efficiency, etc.) and qualitative (adverse events, time periods), are monitored and improvements are implemented.
The premises and equipment are appropriate and are subject to a quality management system.
The surgical intervention checklist procedure is implemented on each occasion by a specific member of the operating team.
The house rules drawn up and validated by an operating room committee specify how the circuits by specific type of care function, establish who is responsible and how surgical programmes are prepared and regulated.
Measures are in place to ensure the traceability of implantable medical devices and procedures, including any checks carried out.
The information needed for patient care is exchanged between the operating room and the clinical, medico technical and logistic areas of activity.
Professional practices are based on procedures derived from up-to-date, validated reference documents.
The operating suite IT system is integrated into the hospital IT system.
Field of application: This criterion only applies to healthcare organisations that have an operating room.
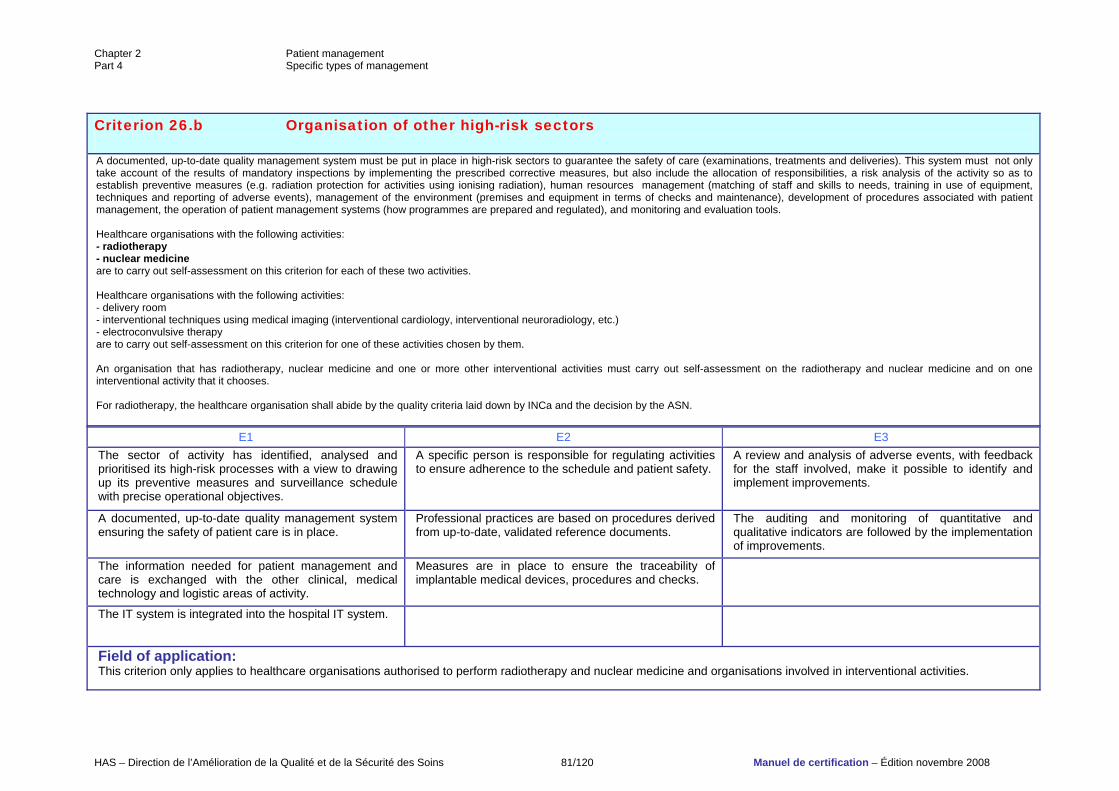
Chapter 2 Patient management Part 4 Specific types of management
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 81/120 Manuel de certification – Édition novembre 2008
Criterion 26.b Organisation of other high-risk sectors A documented, up-to-date quality management system must be put in place in high-risk sectors to guarantee the safety of care (examinations, treatments and deliveries). This system must not only take account of the results of mandatory inspections by implementing the prescribed corrective measures, but also include the allocation of responsibilities, a risk analysis of the activity so as to establish preventive measures (e.g. radiation protection for activities using ionising radiation), human resources management (matching of staff and skills to needs, training in use of equipment, techniques and reporting of adverse events), management of the environment (premises and equipment in terms of checks and maintenance), development of procedures associated with patient management, the operation of patient management systems (how programmes are prepared and regulated), and monitoring and evaluation tools. Healthcare organisations with the following activities: - radiotherapy - nuclear medicine are to carry out self-assessment on this criterion for each of these two activities. Healthcare organisations with the following activities: - delivery room - interventional techniques using medical imaging (interventional cardiology, interventional neuroradiology, etc.) - electroconvulsive therapy are to carry out self-assessment on this criterion for one of these activities chosen by them. An organisation that has radiotherapy, nuclear medicine and one or more other interventional activities must carry out self-assessment on the radiotherapy and nuclear medicine and on one interventional activity that it chooses. For radiotherapy, the healthcare organisation shall abide by the quality criteria laid down by INCa and the decision by the ASN.
E1 E2 E3 The sector of activity has identified, analysed and prioritised its high-risk processes with a view to drawing up its preventive measures and surveillance schedule with precise operational objectives.
A specific person is responsible for regulating activities to ensure adherence to the schedule and patient safety.
A review and analysis of adverse events, with feedback for the staff involved, make it possible to identify and implement improvements.
A documented, up-to-date quality management system ensuring the safety of patient care is in place.
Professional practices are based on procedures derived from up-to-date, validated reference documents.
The auditing and monitoring of quantitative and qualitative indicators are followed by the implementation of improvements.
The information needed for patient management and care is exchanged with the other clinical, medical technology and logistic areas of activity.
Measures are in place to ensure the traceability of implantable medical devices, procedures and checks.
The IT system is integrated into the hospital IT system.
Field of application: This criterion only applies to healthcare organisations authorised to perform radiotherapy and nuclear medicine and organisations involved in interventional activities.
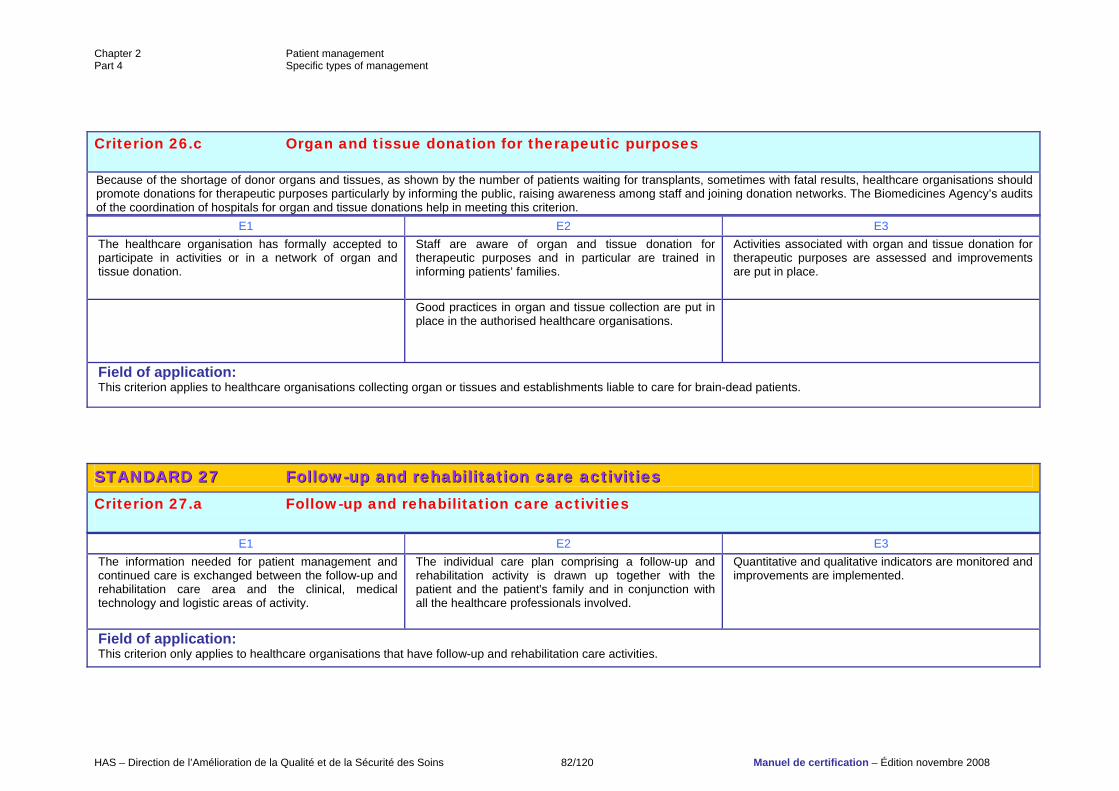
Chapter 2 Patient management Part 4 Specific types of management
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 82/120 Manuel de certification – Édition novembre 2008
Criterion 26.c Organ and tissue donation for therapeutic purposes Because of the shortage of donor organs and tissues, as shown by the number of patients waiting for transplants, sometimes with fatal results, healthcare organisations should promote donations for therapeutic purposes particularly by informing the public, raising awareness among staff and joining donation networks. The Biomedicines Agency’s audits of the coordination of hospitals for organ and tissue donations help in meeting this criterion.
E1 E2 E3 The healthcare organisation has formally accepted to participate in activities or in a network of organ and tissue donation.
Staff are aware of organ and tissue donation for therapeutic purposes and in particular are trained in informing patients’ families.
Activities associated with organ and tissue donation for therapeutic purposes are assessed and improvements are put in place.
Good practices in organ and tissue collection are put in place in the authorised healthcare organisations.
Field of application: This criterion applies to healthcare organisations collecting organ or tissues and establishments liable to care for brain-dead patients.
SSTTAANNDDAARRDD 2277 FFoollllooww--uupp aanndd rreehhaabbiilliittaattiioonn ccaarree aaccttiivviittiieess Criterion 27.a Follow-up and rehabilitation care activities
E1 E2 E3 The information needed for patient management and continued care is exchanged between the follow-up and rehabilitation care area and the clinical, medical technology and logistic areas of activity.
The individual care plan comprising a follow-up and rehabilitation activity is drawn up together with the patient and the patient's family and in conjunction with all the healthcare professionals involved.
Quantitative and qualitative indicators are monitored and improvements are implemented.
Field of application: This criterion only applies to healthcare organisations that have follow-up and rehabilitation care activities.
Chapter 2 Patient management Part 4 Specific types of management
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 83/120 Manuel de certification – Édition novembre 2008
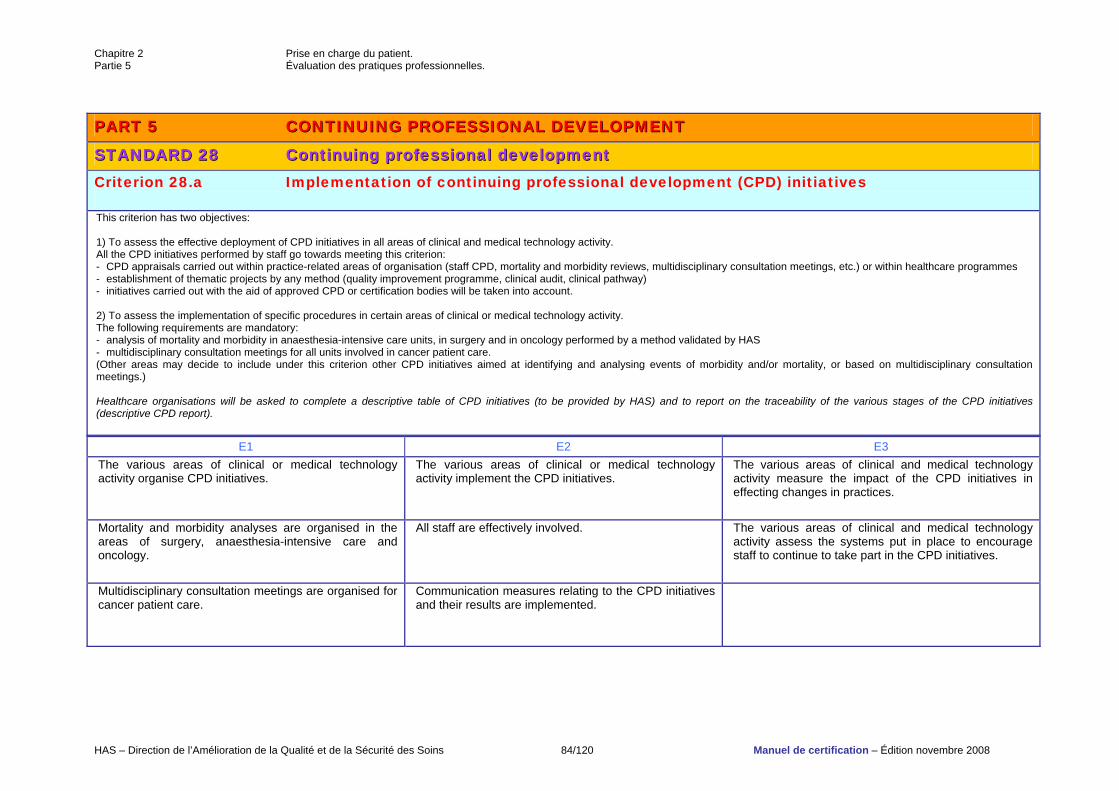
Chapitre 2 Prise en charge du patient. Partie 5 Évaluation des pratiques professionnelles.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 84/120 Manuel de certification – Édition novembre 2008
PPAARRTT 55 CCOONNTTIINNUUIINNGG PPRROOFFEESSSSIIOONNAALL DDEEVVEELLOOPPMMEENNTT
SSTTAANNDDAARRDD 2288 CCoonnttiinnuuiinngg pprrooffeessssiioonnaall ddeevveellooppmmeenntt Criterion 28.a Implementation of continuing professional development (CPD) initiatives This criterion has two objectives: 1) To assess the effective deployment of CPD initiatives in all areas of clinical and medical technology activity. All the CPD initiatives performed by staff go towards meeting this criterion: - CPD appraisals carried out within practice-related areas of organisation (staff CPD, mortality and morbidity reviews, multidisciplinary consultation meetings, etc.) or within healthcare programmes - establishment of thematic projects by any method (quality improvement programme, clinical audit, clinical pathway) - initiatives carried out with the aid of approved CPD or certification bodies will be taken into account. 2) To assess the implementation of specific procedures in certain areas of clinical or medical technology activity. The following requirements are mandatory: - analysis of mortality and morbidity in anaesthesia-intensive care units, in surgery and in oncology performed by a method validated by HAS - multidisciplinary consultation meetings for all units involved in cancer patient care. (Other areas may decide to include under this criterion other CPD initiatives aimed at identifying and analysing events of morbidity and/or mortality, or based on multidisciplinary consultation meetings.) Healthcare organisations will be asked to complete a descriptive table of CPD initiatives (to be provided by HAS) and to report on the traceability of the various stages of the CPD initiatives (descriptive CPD report).
E1 E2 E3 The various areas of clinical or medical technology activity organise CPD initiatives.
The various areas of clinical or medical technology activity implement the CPD initiatives.
The various areas of clinical and medical technology activity measure the impact of the CPD initiatives in effecting changes in practices.
Mortality and morbidity analyses are organised in the areas of surgery, anaesthesia-intensive care and oncology.
All staff are effectively involved.
The various areas of clinical and medical technology activity assess the systems put in place to encourage staff to continue to take part in the CPD initiatives.
Multidisciplinary consultation meetings are organised for cancer patient care.
Communication measures relating to the CPD initiatives and their results are implemented.
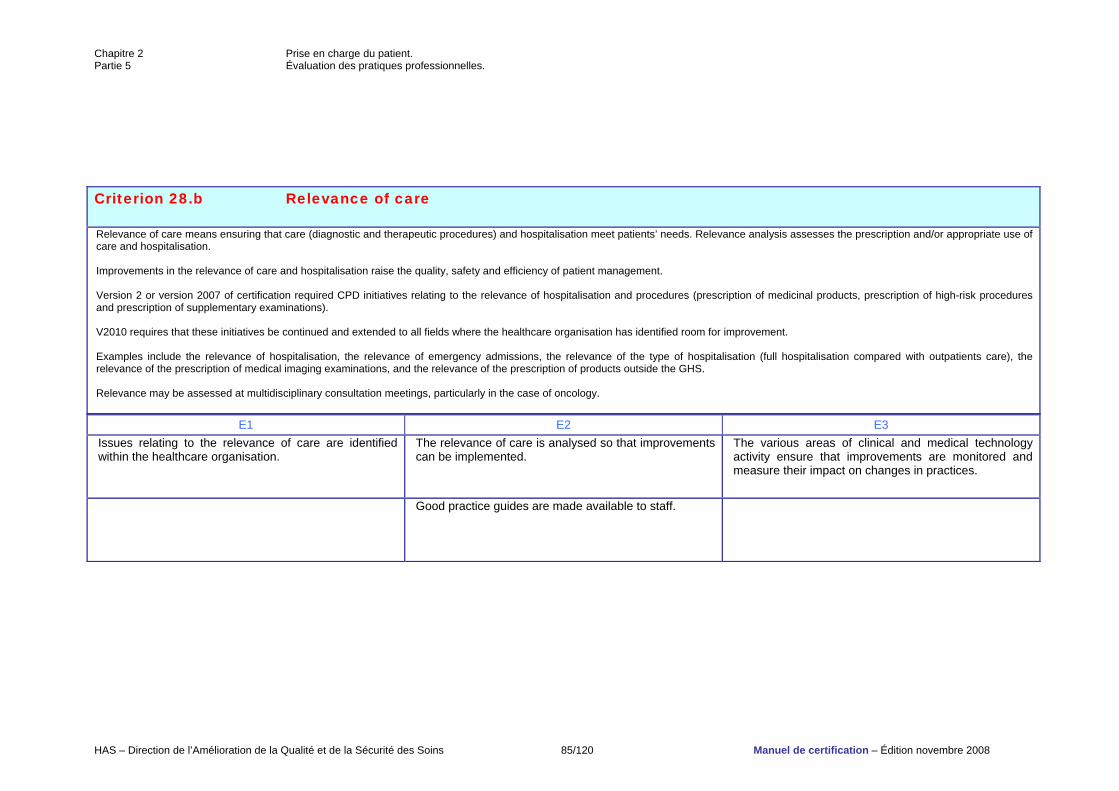
Chapitre 2 Prise en charge du patient. Partie 5 Évaluation des pratiques professionnelles.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 85/120 Manuel de certification – Édition novembre 2008
Criterion 28.b Relevance of care Relevance of care means ensuring that care (diagnostic and therapeutic procedures) and hospitalisation meet patients’ needs. Relevance analysis assesses the prescription and/or appropriate use of care and hospitalisation. Improvements in the relevance of care and hospitalisation raise the quality, safety and efficiency of patient management. Version 2 or version 2007 of certification required CPD initiatives relating to the relevance of hospitalisation and procedures (prescription of medicinal products, prescription of high-risk procedures and prescription of supplementary examinations). V2010 requires that these initiatives be continued and extended to all fields where the healthcare organisation has identified room for improvement. Examples include the relevance of hospitalisation, the relevance of emergency admissions, the relevance of the type of hospitalisation (full hospitalisation compared with outpatients care), the relevance of the prescription of medical imaging examinations, and the relevance of the prescription of products outside the GHS. Relevance may be assessed at multidisciplinary consultation meetings, particularly in the case of oncology.
E1 E2 E3 Issues relating to the relevance of care are identified within the healthcare organisation.
The relevance of care is analysed so that improvements can be implemented.
The various areas of clinical and medical technology activity ensure that improvements are monitored and measure their impact on changes in practices.
Good practice guides are made available to staff.
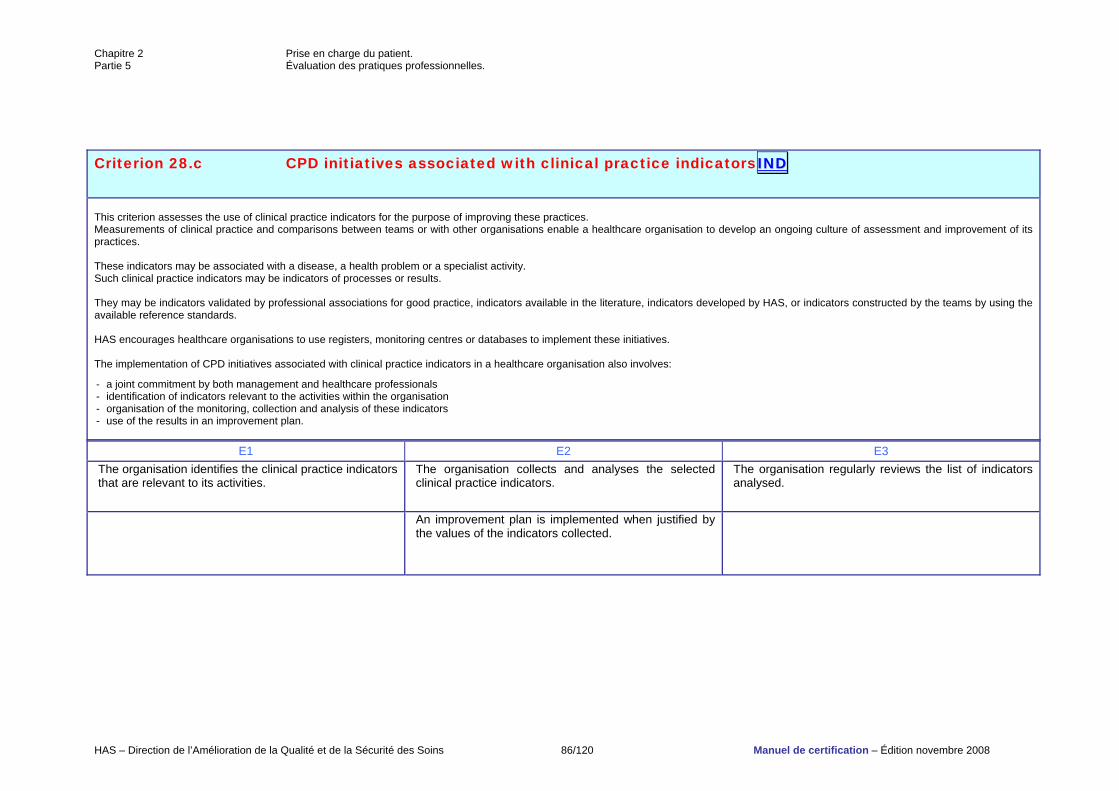
Chapitre 2 Prise en charge du patient. Partie 5 Évaluation des pratiques professionnelles.
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 86/120 Manuel de certification – Édition novembre 2008
Criterion 28.c CPD initiatives associated with clinical practice indicatorsIINNDD
This criterion assesses the use of clinical practice indicators for the purpose of improving these practices. Measurements of clinical practice and comparisons between teams or with other organisations enable a healthcare organisation to develop an ongoing culture of assessment and improvement of its practices. These indicators may be associated with a disease, a health problem or a specialist activity. Such clinical practice indicators may be indicators of processes or results. They may be indicators validated by professional associations for good practice, indicators available in the literature, indicators developed by HAS, or indicators constructed by the teams by using the available reference standards. HAS encourages healthcare organisations to use registers, monitoring centres or databases to implement these initiatives. The implementation of CPD initiatives associated with clinical practice indicators in a healthcare organisation also involves:
- a joint commitment by both management and healthcare professionals - identification of indicators relevant to the activities within the organisation - organisation of the monitoring, collection and analysis of these indicators - use of the results in an improvement plan.
E1 E2 E3 The organisation identifies the clinical practice indicators that are relevant to its activities.
The organisation collects and analyses the selected clinical practice indicators.
The organisation regularly reviews the list of indicators analysed.
An improvement plan is implemented when justified by the values of the indicators collected.
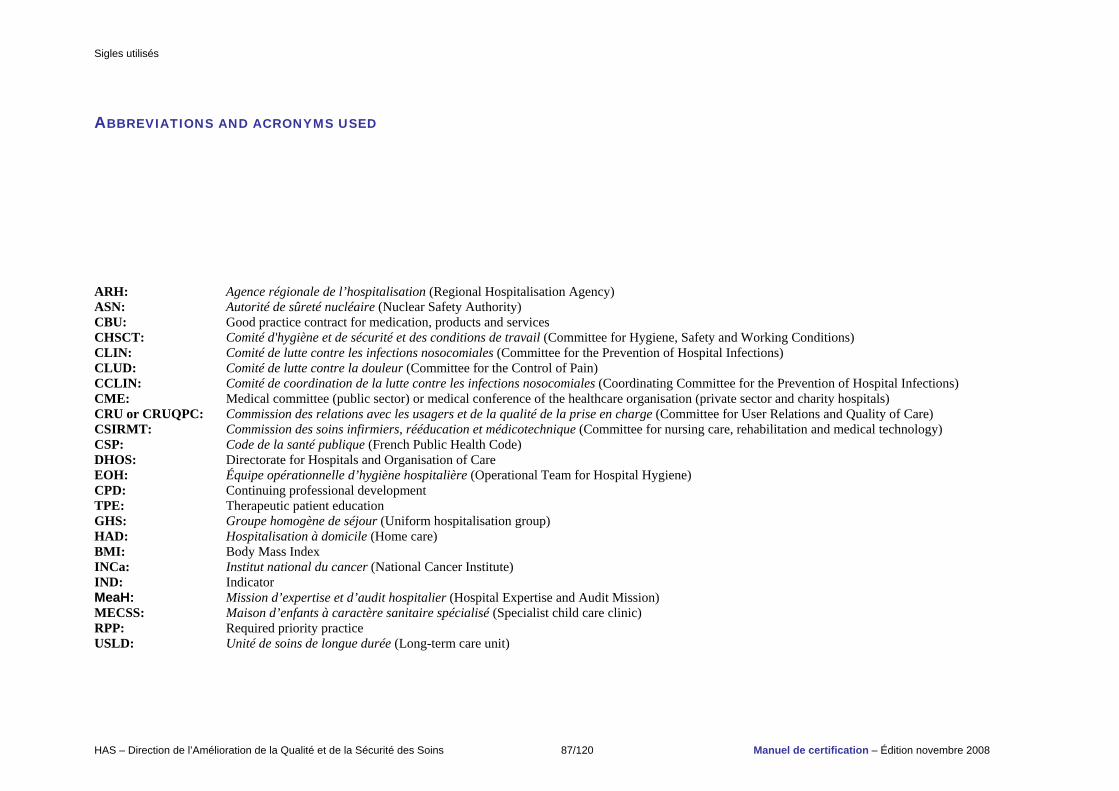
Sigles utilisés
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 87/120 Manuel de certification – Édition novembre 2008
ABBREVIATIONS AND ACRONYMS USED ARH: Agence régionale de l’hospitalisation (Regional Hospitalisation Agency) ASN: Autorité de sûreté nucléaire (Nuclear Safety Authority) CBU: Good practice contract for medication, products and services CHSCT: Comité d'hygiène et de sécurité et des conditions de travail (Committee for Hygiene, Safety and Working Conditions) CLIN: Comité de lutte contre les infections nosocomiales (Committee for the Prevention of Hospital Infections) CLUD: Comité de lutte contre la douleur (Committee for the Control of Pain) CCLIN: Comité de coordination de la lutte contre les infections nosocomiales (Coordinating Committee for the Prevention of Hospital Infections) CME: Medical committee (public sector) or medical conference of the healthcare organisation (private sector and charity hospitals) CRU or CRUQPC: Commission des relations avec les usagers et de la qualité de la prise en charge (Committee for User Relations and Quality of Care) CSIRMT: Commission des soins infirmiers, rééducation et médicotechnique (Committee for nursing care, rehabilitation and medical technology) CSP: Code de la santé publique (French Public Health Code) DHOS: Directorate for Hospitals and Organisation of Care EOH: Équipe opérationnelle d’hygiène hospitalière (Operational Team for Hospital Hygiene) CPD: Continuing professional development TPE: Therapeutic patient education GHS: Groupe homogène de séjour (Uniform hospitalisation group) HAD: Hospitalisation à domicile (Home care) BMI: Body Mass Index INCa: Institut national du cancer (National Cancer Institute) IND: Indicator MeaH: Mission d’expertise et d’audit hospitalier (Hospital Expertise and Audit Mission) MECSS: Maison d’enfants à caractère sanitaire spécialisé (Specialist child care clinic) RPP: Required priority practice USLD: Unité de soins de longue durée (Long-term care unit)
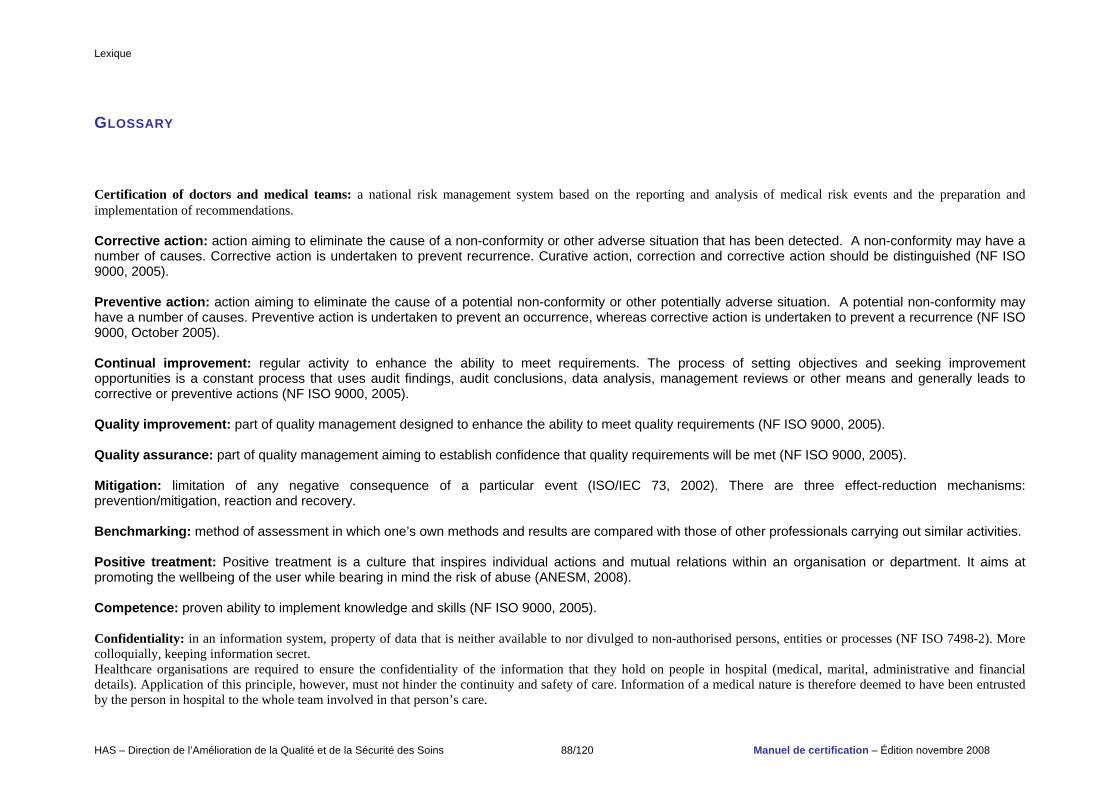
Lexique
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 88/120 Manuel de certification – Édition novembre 2008
GLOSSARY Certification of doctors and medical teams: a national risk management system based on the reporting and analysis of medical risk events and the preparation and implementation of recommendations. Corrective action: action aiming to eliminate the cause of a non-conformity or other adverse situation that has been detected. A non-conformity may have a number of causes. Corrective action is undertaken to prevent recurrence. Curative action, correction and corrective action should be distinguished (NF ISO 9000, 2005). Preventive action: action aiming to eliminate the cause of a potential non-conformity or other potentially adverse situation. A potential non-conformity may have a number of causes. Preventive action is undertaken to prevent an occurrence, whereas corrective action is undertaken to prevent a recurrence (NF ISO 9000, October 2005). Continual improvement: regular activity to enhance the ability to meet requirements. The process of setting objectives and seeking improvement opportunities is a constant process that uses audit findings, audit conclusions, data analysis, management reviews or other means and generally leads to corrective or preventive actions (NF ISO 9000, 2005). Quality improvement: part of quality management designed to enhance the ability to meet quality requirements (NF ISO 9000, 2005). Quality assurance: part of quality management aiming to establish confidence that quality requirements will be met (NF ISO 9000, 2005). Mitigation: limitation of any negative consequence of a particular event (ISO/IEC 73, 2002). There are three effect-reduction mechanisms: prevention/mitigation, reaction and recovery. Benchmarking: method of assessment in which one’s own methods and results are compared with those of other professionals carrying out similar activities. Positive treatment: Positive treatment is a culture that inspires individual actions and mutual relations within an organisation or department. It aims at promoting the wellbeing of the user while bearing in mind the risk of abuse (ANESM, 2008). Competence: proven ability to implement knowledge and skills (NF ISO 9000, 2005). Confidentiality: in an information system, property of data that is neither available to nor divulged to non-authorised persons, entities or processes (NF ISO 7498-2). More colloquially, keeping information secret. Healthcare organisations are required to ensure the confidentiality of the information that they hold on people in hospital (medical, marital, administrative and financial details). Application of this principle, however, must not hinder the continuity and safety of care. Information of a medical nature is therefore deemed to have been entrusted by the person in hospital to the whole team involved in that person’s care.
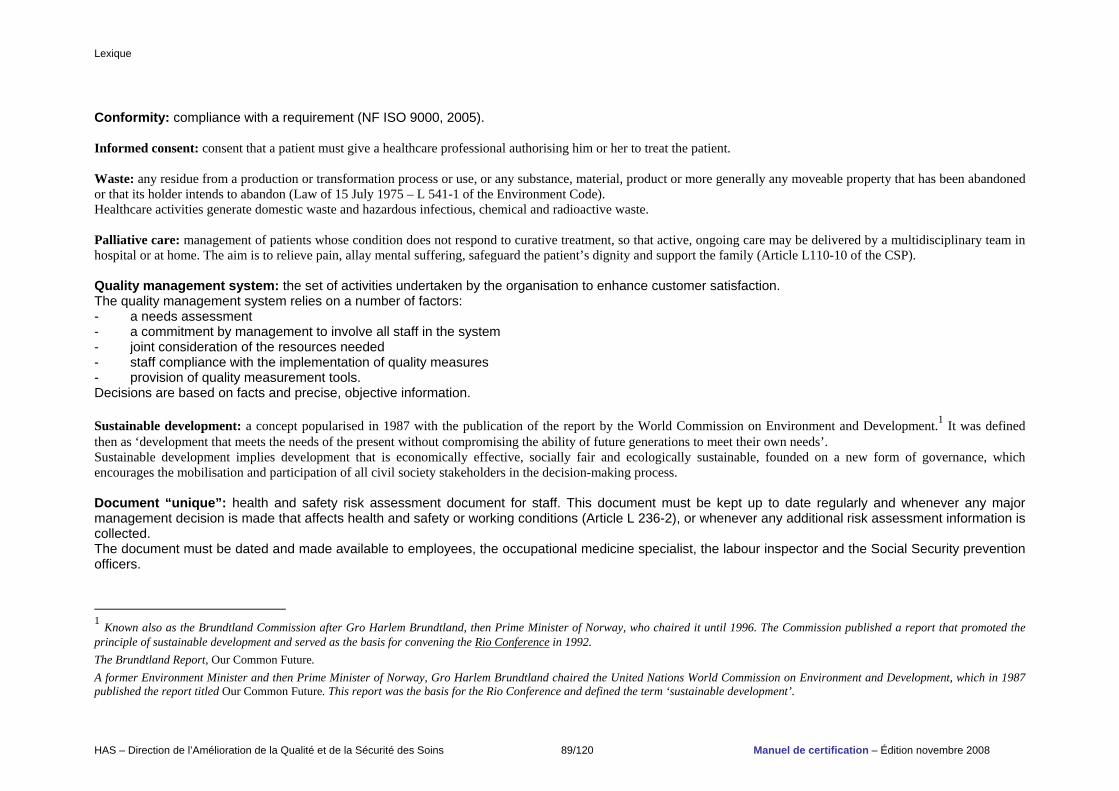
Lexique
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 89/120 Manuel de certification – Édition novembre 2008
Conformity: compliance with a requirement (NF ISO 9000, 2005). Informed consent: consent that a patient must give a healthcare professional authorising him or her to treat the patient. Waste: any residue from a production or transformation process or use, or any substance, material, product or more generally any moveable property that has been abandoned or that its holder intends to abandon (Law of 15 July 1975 – L 541-1 of the Environment Code). Healthcare activities generate domestic waste and hazardous infectious, chemical and radioactive waste. Palliative care: management of patients whose condition does not respond to curative treatment, so that active, ongoing care may be delivered by a multidisciplinary team in hospital or at home. The aim is to relieve pain, allay mental suffering, safeguard the patient’s dignity and support the family (Article L110-10 of the CSP). Quality management system: the set of activities undertaken by the organisation to enhance customer satisfaction. The quality management system relies on a number of factors: - a needs assessment - a commitment by management to involve all staff in the system - joint consideration of the resources needed - staff compliance with the implementation of quality measures - provision of quality measurement tools. Decisions are based on facts and precise, objective information. Sustainable development: a concept popularised in 1987 with the publication of the report by the World Commission on Environment and Development.1 It was defined then as ‘development that meets the needs of the present without compromising the ability of future generations to meet their own needs’. Sustainable development implies development that is economically effective, socially fair and ecologically sustainable, founded on a new form of governance, which encourages the mobilisation and participation of all civil society stakeholders in the decision-making process. Document “unique”: health and safety risk assessment document for staff. This document must be kept up to date regularly and whenever any major management decision is made that affects health and safety or working conditions (Article L 236-2), or whenever any additional risk assessment information is collected. The document must be dated and made available to employees, the occupational medicine specialist, the labour inspector and the Social Security prevention officers.
1 Known also as the Brundtland Commission after Gro Harlem Brundtland, then Prime Minister of Norway, who chaired it until 1996. The Commission published a report that promoted the principle of sustainable development and served as the basis for convening the Rio Conference in 1992. The Brundtland Report, Our Common Future. A former Environment Minister and then Prime Minister of Norway, Gro Harlem Brundtland chaired the United Nations World Commission on Environment and Development, which in 1987 published the report titled Our Common Future. This report was the basis for the Rio Conference and defined the term ‘sustainable development’.
Lexique
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 90/120 Manuel de certification – Édition novembre 2008
Harm: physical injury or damage to the health of people or damage to property or the environment (ISO/IEC 51, 1999). Deviation: difference between an observed fact and the standard. Ecological purchases (eco-friendly purchases): purchases that are less harmful to the environment (products may be termed ‘eco-designed’ and/or ‘eco-labelled’, e.g. NF Environment label). Effectiveness: measure of the degree to which planned activities are realised and planned results are achieved (NF ISO 9000, 2005). Efficiency: the relationship between the results achieved and the resources used (NF ISO 9000, 2005). Effluent: a generic term for urban or industrial wastewater and, more generally, any liquid waste carrying a certain polluting load (whether dissolved, colloidal or particulate). Effluents may also be gaseous. Renewable energy: technologies for producing electricity or heat from renewable sources. An energy source is renewable if its consumption does not limit its consumption in future by exhausting it or harming the environment and society. Customer satisfaction surveys: these may be quantitative or qualitative. They involve listening to customers and taking note of what they say. Taken altogether, their opinions provide an image of the level of customer satisfaction. The organisation can then decide which aspects need improving most. Environment: the surroundings in which an organisation operates, including air, water, land, natural resources, flora, fauna, humans and their interrelation (ISO 14001, 1996). Continuing professional development (CPD): analysis of professional practice with reference to guidelines and by a validated method, including the implementation and follow-up of measures to improve practice (Decree of 14 April 2005). Patient satisfaction assessment: information revealing patients’ opinions on the various human, technical and logistic components of their care. Patient satisfaction must be regularly measured pursuant to the Order of 24 April 1996 reforming public and private hospitalisation. Adverse event: a situation that departs from procedures or results expected in a normal situation and which is or could be a potential source of harm. There are several types of adverse events: malfunctions (non-conformity, anomaly, fault), incidents, sentinel events, precursors, near accidents and accidents. Avoidable adverse event: an event that would not have happened if the care or its environment had conformed to management regarded as being satisfactory. Serious adverse event: an adverse event which results in death, is life-threatening, requires inpatient hospitalisation or prolongation of existing hospitalisation or results in disability or incapacity (Commission Directive 2000/38/EC of 5 June 2000, amending chapter Va – Pharmacovigilance). Sentinel event: adverse event which acts as a warning signal and routinely initiates an investigation and an in-depth analysis.
Lexique
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 91/120 Manuel de certification – Édition novembre 2008
Reliability: likelihood that a device will operate without fault under given conditions and for a given length of time. Document management: a set of general rules specifying in particular: - methods for drawing up and amending documents - management of reference standards (source documentation) - development of identification and classification criteria - drafting of document verification, validation and dissemination procedures - provisions relating to document content security. For document management to be implemented, the types of operations must be specified, a document management plan must be drawn up and the IT system must be specified. Risk identification: process to find, list and characterise elements of risk. Elements can include source or hazard, event, consequence and probability (ISO/IEC 73, 2002). Patient identification: the operation of assigning an identifier or obtaining one or more identifiers on the basis of characteristics (surname, name, gender, date of birth, etc.) of a patient in order to obtain information associated with the patient (GMSIH). Indicator: a measurement tool for characterising an evolving situation, an action or the consequences of an action so as to assess them against given ranges of values. Indicators must be developed in relation to the project objectives. Maintenance: set of actions for keeping an asset in or restoring it to a specific condition or for guaranteeing a particular service (NF X 60-010). Risk control: actions implementing risk management decisions. Risk control may involve monitoring, re-evaluation and compliance with decisions (ISO/IEC 73, 2002). Abuse: ‘any act or omission which undermines the life, the physical and psychological integrity or the freedom, etc., or harms the development of his or her personality and/or undermines or damages his or her financial security’ (Council of Europe, 1987). Recent work by the Ministry of Health, the hospital federations and ANESM has revealed the need not to limit the fight against abuse to the suppression of acts of intentional, individual and criminal abuse. Discussion on the subject of abuse should also address the existence of ordinary (DREES – Ministry of Health) or passive (FHF) abuse, including daily neglect. Management: all the techniques used for coordinating and running an organisation. By extension, management also refers to the people who manage the enterprise (NF ISO 9000, 2005). Quality management: coordinated activities for directing and controlling a body (NF ISO 9000, 2005). Risk management: coordinated activities for directing and steering a body in relation to risk. Risk management generally includes risk estimation, risk treatment, risk acceptance and risk communication (ISO/IEC 73, 2002).
Lexique
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 92/120 Manuel de certification – Édition novembre 2008
Stakeholders (or interested parties): all the groups affected by the organisation. Stakeholders may be internal or external and include the employees, shareholders, banks and public authorities, as well as the consumers, suppliers, trade unions, NGOs, media and all other groups to which the organisation must answer. In a sustainable development approach, it is important to identify them precisely, evaluate their influences on the organisation’s economic life, evaluate the organisation’s influence on each of them, understand and anticipate their expectations, arrange them in a hierarchy and then study their integration. Trusted person: The regulations (Article L 1111-6 of the CSP) give the trusted person two roles: - if the patient so wishes, the trusted person may accompany him or her throughout the process and attend the medical interviews in order to help him or her make decisions - the trusted person will be consulted in cases where the patient is unable to express his or her own wishes. Consulting the trusted person is a requirement for patients unable to express their own wishes: - outside end-of-life situations: for any intervention or investigation - in end-of-life situations: for reducing or stopping treatment. The trusted person’s opinion prevails over any other non-medical opinion, apart from instructions given in advance, when a person is in an advanced or terminal stage of a serious, incurable condition. Relevance of care (review): a method for assessing the extent to which the care and length of hospitalisation meet the patient’s needs. It is applied to an element or programme of care and can relate to the indication for, initiation of or continuation of the care. It aims to strike a balance between the particular needs of a patient and the resources available within the management of a system of care. Recovery plan: a solution to ensure continuity in the event of a breakdown. Prevention: a measure aimed at reducing the frequency of risks. Procedure: a specified way of carrying out an activity or process (NF ISO 9000, 2005). Process: a set of correlated or interacting activities which transform inputs into outputs (NF ISO 9000, 2005). Healthcare products: in the context of this manual, these include medicinal products, labile blood products, narcotic or psychotropic substances, medical devices, medical systems for in vitro diagnosis, organs, tissues, cells and accessory therapeutic products, master preparations, hospital preparations, etc.
Lexique
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 93/120 Manuel de certification – Édition novembre 2008
Personalised care plan: a plan laying down an approach to treatment and care adapted to the individual patient, which ‘must be dynamic, progressive and consensual while taking account of the opinions of the patient and family’. The plan is adjusted to the individual and takes account of the patient’s biological, psychological, social and spiritual needs. NB: The PERSONALISED PROGRAMME OF CARE (PPS) (measure 31 in the cancer plan) is a simple, informative document that explains to the patient the coordinated chain of care that is put in place around him or her. It is drawn up at a specific moment in the patient’s care and is subject to change, in that it may be supplemented, amended or even replaced. It also enables a doctor who does not know the patient to provide optimum treatment (when the regular doctor is unavailable, for example). It takes the form of a paper document which includes at least the following items: - the theoretical treatment plan, i.e. the treatment proposal accepted by the patient and the way it is arranged over time - the various assessments planned - the names and contact details of the doctor in charge of treatment and the specialist healthcare team who may be contacted by the primary care doctor, the patient or the patient’s family - details of patient groups that the patient can contact. Protocol: description of techniques to use and/or instructions to observe. Good practice guidelines (or professional guidelines): proposals developed by a specified method to help the health professional and the patient to find the most appropriate care in particular clinical circumstances. They are produced by HAS, health agencies, learned societies and professional associations, etc. Healthcare networks: ‘The purpose of healthcare networks is to facilitate access to healthcare, and the coordination, continuity or multidisciplinarity of healthcare, particularly care specific to certain population groups, diseases or healthcare activities. They ensure that care meets the person’s needs in terms of health education, prevention, diagnosis and the care itself. They may take part in public health activities. They carry out assessments in order to guarantee the quality of their services and procedures’ (Law of 4 March 2002 on patients’ rights and quality of the healthcare system). Multidisciplinary consultation meetings (MCM): a forum for exchanges among specialists in various disciplines on diagnostic and therapeutic strategies in cancer care. MCMs may be organised by a single organisation, a group of organisations or a cancer care network, in the context of cancer coordination centres (C3). Regular assessment by MCMs should recognise ongoing improvement in the quality of the healthcare and medical services provided to the patient. These meetings may also be held in other specialties.
Lexique
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 94/120 Manuel de certification – Édition novembre 2008
Mortality and morbidity review: analysis of those cases in which care was marked by an unexpected adverse event resulting in complications or even the death of the patient. A mortality and morbidity review consists of examining and studying such events in order to understand the mechanism and identify contributing factors, without seeking to apportion blame to an individual or team. The aim is to put in place preventive and corrective measures in terms of protocols, training, organisation, etc. It is a method of risk management. Risk: a number of definitions may be proposed: - undesirable situation having negative consequences resulting from one or more events whose occurrence is uncertain - any feared event which reduces the hope of gain and/or effectiveness in a human activity. Areas of activity: activity units. The areas of activity are set by the organisation. Safety: the state in which the risk to individuals is reduced to a minimum. This state is achieved by means of a safety initiative to identify and deal with the different sources of risks. Reporting of adverse events: an action whereby any adverse event is brought by a health professional to the attention of the vigilance structure responsible for the compilation, evaluation and validation of cases. Crisis situation: a situation that threatens individuals or an organisation and requires appropriate decisions to be made urgently (crisis scale: minor incident, major incident or serious accident, disaster). Staff CPD: regular staff meetings (roughly every 2 to 3 months), at which files are reviewed in conjunction with a literature review (or vice-versa) and one or more improvements are identified for implementation, based on the best available standards, practitioners’ expertise and patients’ choices. Scorecard: a scorecard gathers a selection of key indicators that periodically provide multidimensional information on a policy or programme. The aim is to be able to monitor the deployment or state of progress of this policy or programme and to assess the relevance of the policy or the effectiveness of the programme. The purpose of scorecards is to gather the indicators in one place and summarise them so as to present them in a form that managers can use to facilitate decision making. Traceability: the possibility of finding, within a system, a list of previously determined information attached to one or more elements in the system to explain its failures. Healthcare vigilance: mandatory types of healthcare vigilance cover the use of healthcare products (vigilance of medicinal products, blood products, medical devices, biological materials, cosmetic products and reagents), medically assisted reproduction, compulsory notification of healthcare-associated serious adverse events, including healthcare-associated infections, and significant radiation protection events. The aim is to monitor adverse events through an ongoing process of collection, recording, identification, treatment, assessment and investigation. Controlled environment area: a delimited area where sources of biological contamination are controlled by specific means.
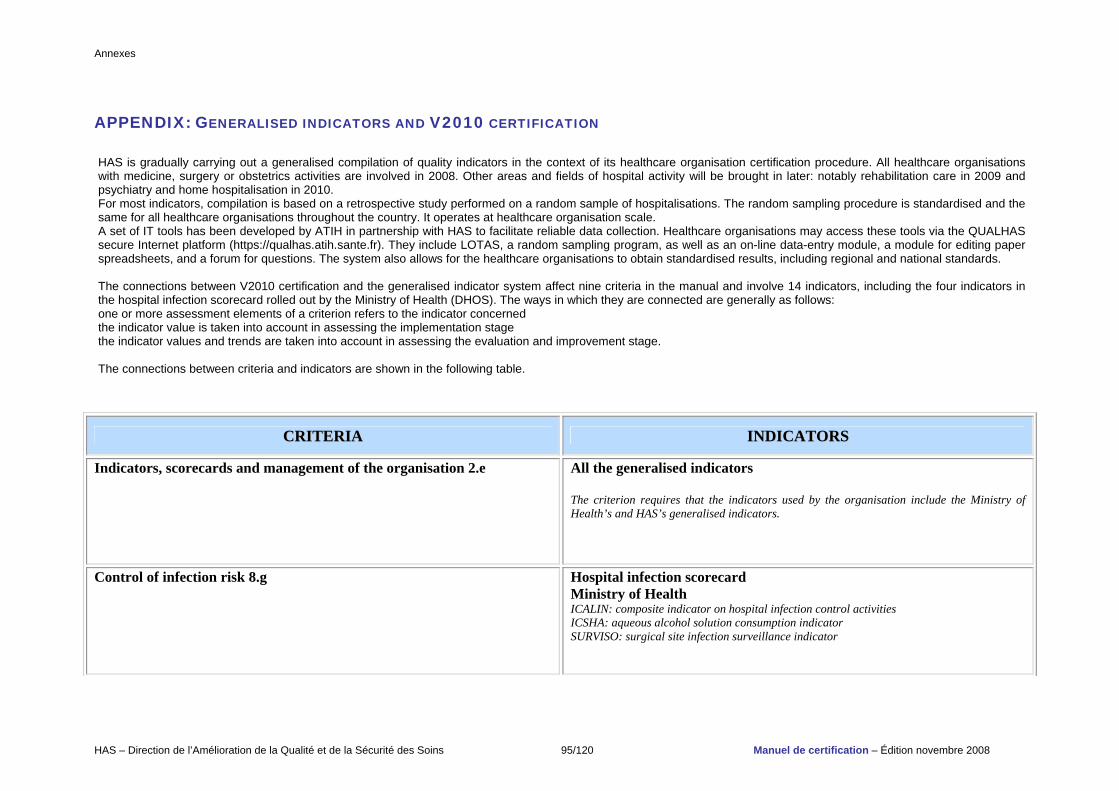
Annexes
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 95/120 Manuel de certification – Édition novembre 2008
APPENDIX: GENERALISED INDICATORS AND V2010 CERTIFICATION
CCRRIITTEERRIIAA IINNDDIICCAATTOORRSS
Indicators, scorecards and management of the organisation 2.e All the generalised indicators The criterion requires that the indicators used by the organisation include the Ministry of Health’s and HAS’s generalised indicators.
Control of infection risk 8.g Hospital infection scorecard Ministry of Health ICALIN: composite indicator on hospital infection control activities ICSHA: aqueous alcohol solution consumption indicator SURVISO: surgical site infection surveillance indicator
HAS is gradually carrying out a generalised compilation of quality indicators in the context of its healthcare organisation certification procedure. All healthcare organisations with medicine, surgery or obstetrics activities are involved in 2008. Other areas and fields of hospital activity will be brought in later: notably rehabilitation care in 2009 and psychiatry and home hospitalisation in 2010. For most indicators, compilation is based on a retrospective study performed on a random sample of hospitalisations. The random sampling procedure is standardised and the same for all healthcare organisations throughout the country. It operates at healthcare organisation scale. A set of IT tools has been developed by ATIH in partnership with HAS to facilitate reliable data collection. Healthcare organisations may access these tools via the QUALHAS secure Internet platform (https://qualhas.atih.sante.fr). They include LOTAS, a random sampling program, as well as an on-line data-entry module, a module for editing paper spreadsheets, and a forum for questions. The system also allows for the healthcare organisations to obtain standardised results, including regional and national standards. The connections between V2010 certification and the generalised indicator system affect nine criteria in the manual and involve 14 indicators, including the four indicators in the hospital infection scorecard rolled out by the Ministry of Health (DHOS). The ways in which they are connected are generally as follows: one or more assessment elements of a criterion refers to the indicator concerned the indicator value is taken into account in assessing the implementation stage the indicator values and trends are taken into account in assessing the evaluation and improvement stage. The connections between criteria and indicators are shown in the following table.
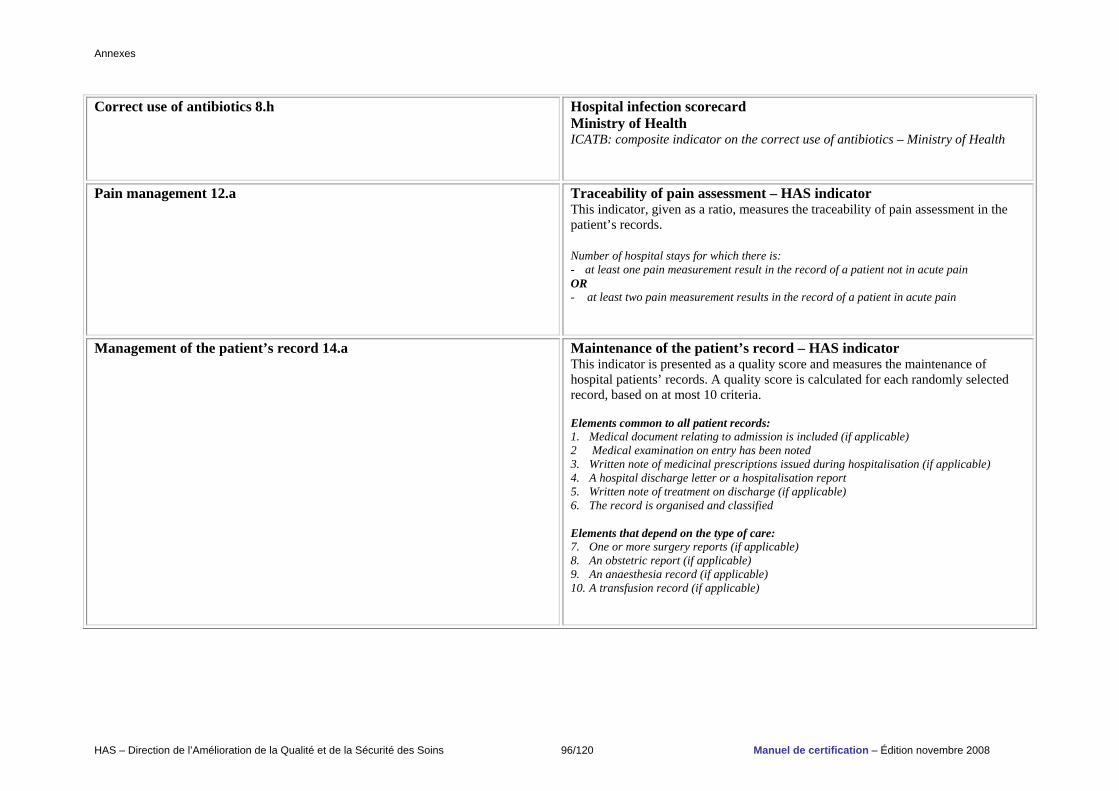
Annexes
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 96/120 Manuel de certification – Édition novembre 2008
Correct use of antibiotics 8.h Hospital infection scorecard Ministry of Health ICATB: composite indicator on the correct use of antibiotics – Ministry of Health
Pain management 12.a Traceability of pain assessment – HAS indicator This indicator, given as a ratio, measures the traceability of pain assessment in the patient’s records. Number of hospital stays for which there is: - at least one pain measurement result in the record of a patient not in acute pain OR - at least two pain measurement results in the record of a patient in acute pain
Management of the patient’s record 14.a Maintenance of the patient’s record – HAS indicator This indicator is presented as a quality score and measures the maintenance of hospital patients’ records. A quality score is calculated for each randomly selected record, based on at most 10 criteria. Elements common to all patient records: 1. Medical document relating to admission is included (if applicable) 2 Medical examination on entry has been noted 3. Written note of medicinal prescriptions issued during hospitalisation (if applicable) 4. A hospital discharge letter or a hospitalisation report 5. Written note of treatment on discharge (if applicable) 6. The record is organised and classified Elements that depend on the type of care: 7. One or more surgery reports (if applicable) 8. An obstetric report (if applicable) 9. An anaesthesia record (if applicable) 10. A transfusion record (if applicable)
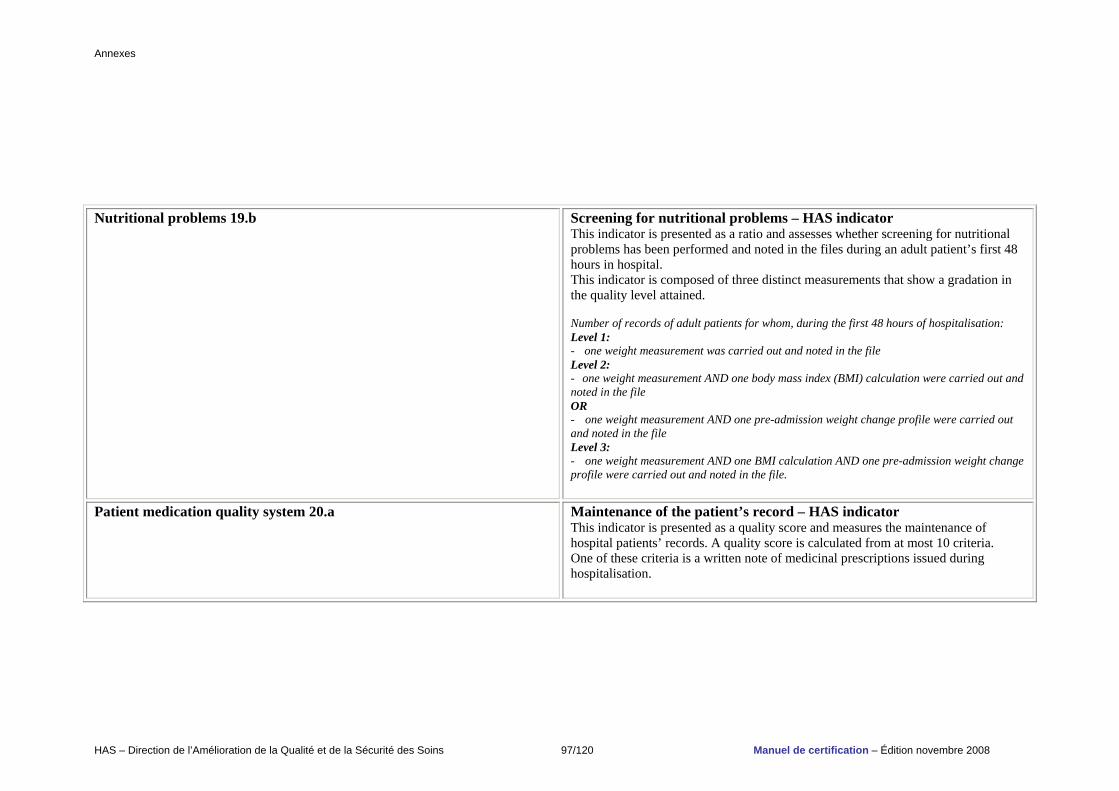
Annexes
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 97/120 Manuel de certification – Édition novembre 2008
Nutritional problems 19.b Screening for nutritional problems – HAS indicator
This indicator is presented as a ratio and assesses whether screening for nutritional problems has been performed and noted in the files during an adult patient’s first 48 hours in hospital. This indicator is composed of three distinct measurements that show a gradation in the quality level attained. Number of records of adult patients for whom, during the first 48 hours of hospitalisation: Level 1: - one weight measurement was carried out and noted in the file Level 2: - one weight measurement AND one body mass index (BMI) calculation were carried out and noted in the file OR - one weight measurement AND one pre-admission weight change profile were carried out and noted in the file Level 3: - one weight measurement AND one BMI calculation AND one pre-admission weight change profile were carried out and noted in the file.
Patient medication quality system 20.a
Maintenance of the patient’s record – HAS indicator This indicator is presented as a quality score and measures the maintenance of hospital patients’ records. A quality score is calculated from at most 10 criteria. One of these criteria is a written note of medicinal prescriptions issued during hospitalisation.
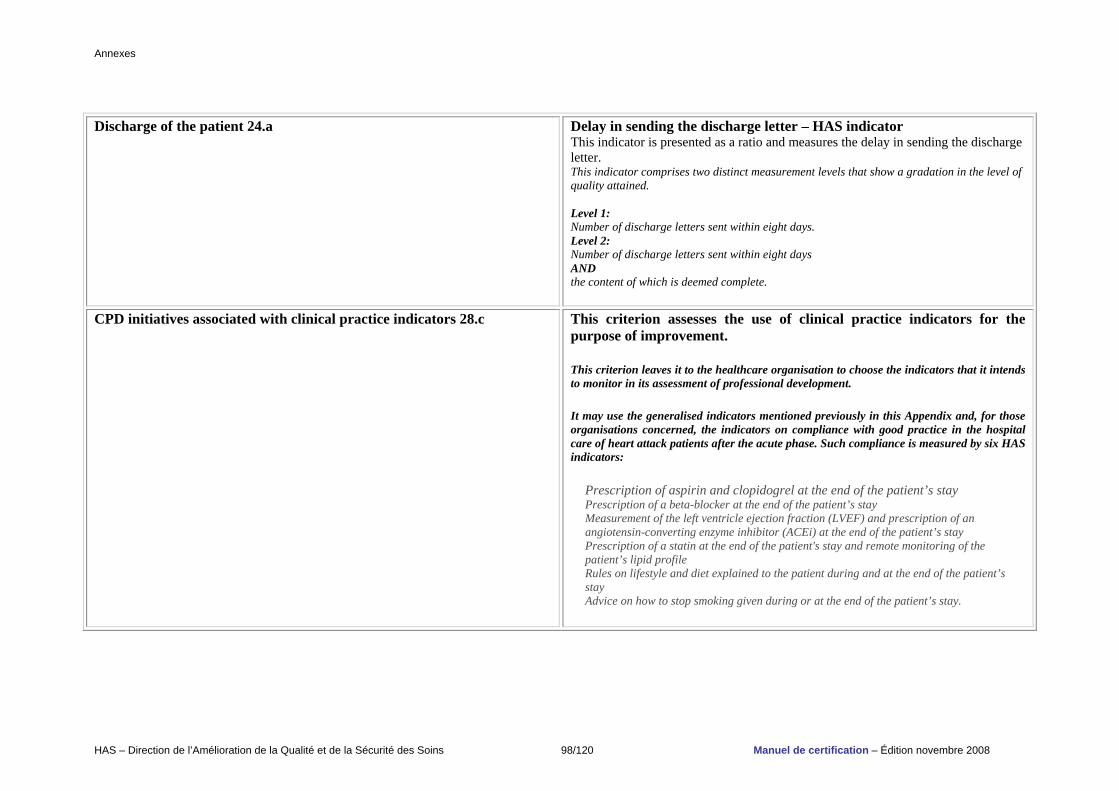
Annexes
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 98/120 Manuel de certification – Édition novembre 2008
Discharge of the patient 24.a Delay in sending the discharge letter – HAS indicator
This indicator is presented as a ratio and measures the delay in sending the discharge letter. This indicator comprises two distinct measurement levels that show a gradation in the level of quality attained. Level 1: Number of discharge letters sent within eight days. Level 2: Number of discharge letters sent within eight days AND the content of which is deemed complete.
CPD initiatives associated with clinical practice indicators 28.c This criterion assesses the use of clinical practice indicators for the purpose of improvement.
This criterion leaves it to the healthcare organisation to choose the indicators that it intends to monitor in its assessment of professional development.
It may use the generalised indicators mentioned previously in this Appendix and, for those organisations concerned, the indicators on compliance with good practice in the hospital care of heart attack patients after the acute phase. Such compliance is measured by six HAS indicators:
Prescription of aspirin and clopidogrel at the end of the patient’s stay
Prescription of a beta-blocker at the end of the patient’s stay
Measurement of the left ventricle ejection fraction (LVEF) and prescription of an angiotensin-converting enzyme inhibitor (ACEi) at the end of the patient’s stay
Prescription of a statin at the end of the patient's stay and remote monitoring of the patient’s lipid profile
Rules on lifestyle and diet explained to the patient during and at the end of the patient’s stay
Advice on how to stop smoking given during or at the end of the patient’s stay.
Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 99/120 Manuel de certification – Édition novembre 2008
ACKNOWLEDGEMENTS
V2010 Steering Committee
Dr Nafissa Abdelmoumène, project manager, Certification Development Department, DAQSS, HAS. Mrs Isabelle Alquier, deputy head of the Healthcare Organisation Certification Department, certification systems section, DAQSS, HAS. Mrs Rose-Marie Andrieux, deputy head of the Healthcare Organisation Certification Department, DAQSS, HAS (until December 2007). Mr Frédéric Bousquet, head of the Department of Performance Indicators for the Improvement of Hospital Quality, DAQSS, HAS (until July 2008). Dr Matthieu Boussarie, deputy head of the Certification Development Department, DAQSS, HAS. Dr Charles Bruneau, technical consultant, Division for the Improvement of Healthcare Quality and Safety (DAQSS), HAS. Mr René Caillet, director, CRF L’Espoir, Hellemmes. Mr Alain-Michel Ceretti, director, Information and Development of Mediation on Nosocomial Infections (IDMIN), HAS. Mr Philippe Chevalier, project manager, Practice Evaluation and Improvement Department (SEVAM), DAQSS, HAS. Mrs Anne Depaigne-Loth, project manager, Certification Development Department, DAQSS, HAS. Mrs Isabelle Dessales, communications officer, Institutional Communications Department, DCIP, HAS. Mrs Christine Devaud, project manager, Documentation Department, Public Information (DCIP), HAS. Mrs Marie Erbault, project manager, Pilot Programme Unit (UPP), DAQSS, HAS. Mrs Dominique Ferréol, project manager, Certification Development Department, DAQSS, HAS. Mr Jean-Paul Guérin, Chairman of the Healthcare Organisations Certification Committee, HAS. Dr Michèle Hebert-Demay, head of the Institutional Communications Department, DCIP, HAS. Mrs Muriel Jakubowski, project manager, Certification Development Department, DAQSS, HAS. Dr Laurent Jouffroy, anaesthetist intensivist , Clinique des Diaconesses, Strasbourg. Mr Raymond Le Moign, director, Division for the Improvement of Healthcare Quality and Safety (DAQSS), HAS. Mrs Michèle Lenoir-Salfati, head of the Healthcare Organisation Certification Department, DAQSS, HAS. Mrs Aline Maserak, retired senior nurse, former member of the Healthcare Organisation Certification Committee, surveyor for the Haute Autorité de Santé, Salomé. Mrs Fabienne Menot, Division for the Improvement of Healthcare Quality and Safety (DAQSS), HAS. Dr François Meyer, director, Division of Medical, Economic and Public Health Assessment (DEMESP), HAS. Dr Philippe Michel, director, Division of Healthcare Strategy Assessment (DESS), HAS (until October 2007). Mr Yvonnick Morice, director general, University Hospital Centre, Angers. Dr Vincent Mounic, head of the Certification Development Department, DAQSS, HAS.
Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 100/120 Manuel de certification – Édition novembre 2008
Mr Jean-Philippe Mousnier, sociologist, Murart Areo, Boulogne-Billancourt. Mr Loïc Ricour, director, National Mission for the Development of Mediation, Information and Dialogue for Healthcare Safety (MIDISS). Dr Nathalie Riolacci, project manager, Pilot Programme Unit (UPP), DAQSS, HAS. Mr François Romaneix, Director of Haute Autorité de Santé. Mrs Christiane Rossatto, director, Division of Communication and Public Information (DCIP), HAS. Dr Isabelle Rullon, project manager, Certification Development Department, DAQSS, HAS. Mrs Yasmine Sami, project manager, Certification Development Department, DAQSS, HAS. Mr Antoine Vigneron, head of the Information Systems Department, DAGRI, HAS.
V2010 Project Group Dr Nafissa Abdelmoumène, project manager, Certification Development Department, DAQSS, HAS. Mrs Isabelle Alquier, deputy head of the Healthcare Organisation Certification Department, certification systems section, DAQSS, HAS. Mrs Rose-Marie Andrieux, deputy head of the Healthcare Organisation Certification Department, DAQSS, HAS (until December 2007). Mrs Évelyne Belliard, head of the Department of Indicators for the Improvement of Hospital Quality, DAQSS, HAS Dr Matthieu Boussarie, deputy head of the Certification Development Department, DAQSS, HAS. Dr Charles Bruneau, technical consultant, DAQSS, HAS. Mrs Sabine Cohen, deputy head of the Healthcare Organisation Certification Department, certification information section, DAQSS, HAS. Mrs Dominique Ferréol, project manager, Certification Development Department, DAQSS, HAS. Mrs Muriel Jakubowski, project manager, Certification Development Department, DAQSS, HAS. Mr Philip Laly, deputy head of the Healthcare Organisation Certification Department, surveyors section, DAQSS, HAS. Mr Raymond Le Moign, director, Division for the Improvement of Healthcare Quality and Safety (DAQSS), HAS. Mrs Michèle Lenoir-Salfati, head of the Healthcare Organisation Certification Department, DAQSS, HAS. Mrs Fabienne Menot, Division for the Improvement of Healthcare Quality and Safety (DAQSS), HAS. Dr Vincent Mounic, head of the Certification Development Department, DAQSS, HAS. Dr Roger Peschaud, policy officer, Certification Development Department, DAQSS, HAS. Mrs Magali Rineau, deputy head of the Healthcare Organisation Certification Department, tools and methods section, DAQSS, HAS (until February 2008). Dr Isabelle Rullon, project manager, Certification Development Department, DAQSS, HAS. Mrs Yasmine Sami, project manager, Certification Development Department, DAQSS, HAS.
Members of the Healthcare Organisations Certification Committee Mr Jean-Paul Guérin, Chairman of the Healthcare Organisations Certification Committee, HAS. Mr Christian Anastasy, director general, Compagnie Stéphanoise de Santé, Saint-Priest-en-Jarez. Mrs Geneviève Baheu, senior health supervisor, Centre Hospitalier, Saumur. Dr Sylvia Benzaken, PH, Central Immunology Laboratory, Hôpital de l’Archet, CHRU, Nice. Prof. Patrice Beutter, face and neck surgeon, Centre Hospitalier Universitaire, Tours. Mrs Marie-Lise Biscay, hospital pharmacist, Centre Hospitalier des Pyrénées, Pau. Mr René Caillet, director, CRF L’Espoir, Hellemmes. Mr Christian Caoduro, director, Clinique Sainte Odile, Strasbourg. Mr Olivier Debay, director general, Clinique du Sud, Carcassonne. Mrs Édith Dufay, pharmacist, head of department, Centre Hospitalier, Lunéville.
Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 101/120 Manuel de certification – Édition novembre 2008
Mrs Marie-Françoise Dumay, quality/risk management policy officer, Agence régionale de l’hospitalisation d’île-de-France, Paris. Prof. Patrice François, specialist in public health, head of the Health Monitoring Department, Centre Hospitalier Universitaire, Grenoble. Dr Jacques Glikman, PH, psychiatrist, Centre Médicopsychologique Tagore, Épinay-sur-Seine. Dr Anne Gruson, pathologist, head of department, Centre Hospitalier, Arras. Mr Denis Frechou, director, Centre Hospitalier Esquirol, St-Maurice. Mr Pierre Huin, PSPH, director of care arrangements and quality, Groupe Hospitalier Privé du Centre-Alsace, Colmar. Dr Laurent Jouffroy, anaesthetist intensivist , Clinique des Diaconesses, Strasbourg. Mrs Anne Laurin-Inizan, deputy director, Fondation Hôpital Saint-Joseph, Paris. Mrs Marie-Claude Lefort, director of healthcare, general coordinator of public healthcare, Centre Hospitalier Universitaire, Angers. Prof. Pierre Lombrail, Public Health and Epidemiology Laboratory, Hôpital Saint-Jacques, CHU, Nantes. Mr Bruno Lucet, director of quality and risk management, AP-HP, Centre Hospitalier Universitaire Henri-Mondor, Créteil. Mrs Monique Mazard, director of care, general coordinator of healthcare services, Centre Hospitalier Universitaire, Nice. Mrs Aline Maserak, retired senior nurse, former member of the Healthcare Organisation Certification Committee (HAS), surveyor for the Haute Autorité de Santé, Salomé. Mr Yvonnick Morice, director general, Centre Hospitalier Universitaire, Angers. Mr Jean-Philippe Mousnier, sociologist, Murart Areo, Boulogne-Billancourt. Dr Jean-Paul Ortiz, nephrologist, Polyclinique Saint-Roch, Cabestany. Mr Emmanuel Rodriguez, confederation secretary, vice-president of CISS users, Confédération Syndicale des Familles, Paris. Mr Jean-Daniel Simon, chairman of the board, Hôpital Keraudren, Brest. Mrs Claude Rambaud, president, Association Le Lien, Courtabœuf.
Members of the HAS Board
Professor Laurent Degos, President of the Haute Autorité de Santé, HAS, Saint-Denis. Prof. Gilles Bouvenot, board member, Haute Autorité de Santé, Saint-Denis. Mr Raoul Briet, board member, Haute Autorité de Santé, Saint-Denis. Mr Étienne Caniard, board member, Haute Autorité de Santé, Saint-Denis. Prof. Jean-Michel Dubernard, board member, Haute Autorité de Santé, Saint-Denis. Mr Jean-Paul Guérin, board member, Haute Autorité de Santé, Saint-Denis. Dr Claude Maffioli, board member, Haute Autorité de Santé, Saint-Denis. Prof. Lise Rochaix, board member, Haute Autorité de Santé, Saint-Denis.
Members of the V2010 working groups
Dr Bernard Abry, anaesthetist intensivist, Institut hospitalier Jacques-Cartier, Massy. Dr Philippe-Emmanuel Adès, anaesthetist intensivist, Clinique de l’Europe, Rouen. Mrs Delphine Aigle, engineer in charge of quality and organisation, Centre Alexis-Vautrin, Vandœuvre-lès-Nancy. Mrs Laure Albertini, director, Department of Patients’ Rights and Associations, Legal Affairs Division, AP-HP, Paris. Prof. René Amalberti, doctor of medicine, policy officer, deputy director, IMASSA, Brétigny-sur-Orge.
Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 102/120 Manuel de certification – Édition novembre 2008
Mrs Michelle Anahory-Zirah, Landwell et associés, Montpellier. Mrs Hélène Antonini-Castera, deputy director, quality director, Hôpital Gériatrique Les Magnolias, Longjumeau. Mr Jérôme Audouin-Zuccoli, sustainable development strategy consultant, Paris. Mrs Marielle Audouin, head of quality assurance, member of the Sustainable Development Committee, Clinique Milan, Paris. Mr Bertrand Bailleul, director, Hôpital Saint-Jean, Gennevilliers. Mr Pierre-Jean Bargnoux, pharmacist, head of the Biology Department, Centre de Lutte contre le Cancer, Clermont-Ferrand. Mrs Christine Belhomme, coordinator of the Sustainable Development Committee, La Plaine-Saint-Denis. Mrs Marie-France Berdat-Dellier, user representative, ORGECO, Montreuil-en-Touraine. Mr Xavier Bernard, AFNOR Skills - DP2i , Saint-Denis. Mrs Patricia Bessy, quality engineer, Centre Hospitalier Neuro-Cardio HCL, Bron. Dr Jean-Louis Blache, medical doctor, head of the Anaesthesia and Resuscitation Department, Institut Paoli-Calmette, Marseille. Dr Catherine Blacker-Scholler, AFNOR Skills - DP2i , Saint-Denis. Mrs Marianne Blanc, midwife, surveyor, in charge of quality and risk management, CH, Annonay. Dr Jean-Marie Bobillo, paediatric psychiatrist, area head, Centre Hospitalier Sainte-Marie, Privas. Dr Henri Bonfait, orthopaedic and trauma surgeon, Hôpital Notre-Dame du Perpétuel Secours, Levallois-Perret. Dr Stéphanie Bordes-Couecou, hospital practitioner in hospital hygiene, CH de la Côte Basque, Bayonne. Mrs Béatrice Borrel, user representative, UNAFAM, Paris. Dr Roland Bouet, psychiatrist, CHS Henri-Laborit, Poitiers. Mr Nicolas Brun, policy officer, UNAF, Paris. Mr Jean-Pierre Burnier, director general, Centre Hospitalier, Gonesse. Dr Véronique Bussy Malgrange, medical doctor, coordinator of the CLIN-Est regional branch office, Clinique de Champagne, CHU, Reims. Mrs Marie-Catherine Camp, LA SHAM, Lyon. Mr Philippe Caralp, management and risk analysis consultant, Étaples. Mrs Aude Caria, psychologist, policy officer, WHO Collaborative Centre, in charge of the users’ resource centre, CH Sainte-Anne, Paris. Mrs Alice Casagrande, project manager, Agence nationale d’évaluation sociale et médicosociale (ANESM), Saint-Denis. Mr Alain Chalochet, director, Geriatrics Hospital Group, Hospices Civils de Lyon. Mr Jean-Robert Chevallier, deputy director general, Centre Hospitalier Régional, Orléans. Mr Philippe Choupin, director general, Nouvelles Cliniques Nantaises, Nantes. Dr Roger Ciais, cardiologist, director general, Clinique des Trois-Luc, Marseille. Mrs Claire Compagnon, Cabinet C. Compagnon Conseil, Paris. Mrs Laura d’Ancezune, director, health quality section, Groupe Korian, Paris. Mrs Marie-José Darmon, senior health supervisor, anaesthetist, Hôpital de Nice.
Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 103/120 Manuel de certification – Édition novembre 2008
Dr Jean-François de Frémont, nephrologist, mediator, Polyclinique Saint-Côme, Compiègne. Mr Gérard Delahaye, Centre Hospitalier Spécialisé Philippe-Pinel, Amiens. Mr Jean Delaunay, healthcare director, Centre Hospitalier Georges-Daumezon, Fleury-les-Aubrais. Mr Jean-Louis Denis, PhD, Université de Montréal, Québec, Canada. Mrs Isabelle Desquerre, biomedical engineer, Division of quality and risk management, AP-HM, Mareille. Dr Bernard Devalois, head of department, palliative care unit, Centre Hospitalier, Puteaux. Dr Daniel d'Hérouville, Maison Médicale Jeanne-Garnier, Paris. Mrs Marie-Christine Duboulet, deputy director, Clinique Turin, Paris. Mrs Édith Dufay, pharmacist, head of department, Centre Hospitalier, Lunéville. Mrs Christine Fabry, director of user relations, Hospices Civils de Lyon. Mrs Nadine Raffy-Pihan, Fédération nationale des médecins radiologues, Paris. Dr Fadila Farsi, coordinating doctor, ONCORA network, CRLCC Léon-Bérard, Lyon. Mr Stéphane Fraisse, deputy director, HAD Soins et Santé Lyon, Caluire. Mr Gilles Gaebel, user representative, AVIAM. Dr Sylvie Garnaud-Touquet, medical doctor, surveyor, CHR, Orléans. M. Hubert Garrigue-Guyonnaud, director general, CHRU, Tours. Dr Claire Gatecel, anaesthetist intensivist, Centre Hospitalier, Béziers. Mrs Véronique Ghadi, public health study provider, Paris. Prof. Martine Gilard, cardiologist, CHU, Brest. Dr Jean-Marie Gomas, hospital practitioner, Groupe Hospitalier Sainte-Perrine, Paris. Dr Catherine Grenier, medical doctor, director of the Indicators and Quality Department, FNCLCC, Paris. Mr Franck Guarnieri, director of the risk analysis section, École nationale des mines Paris, Sophia Antipolis. Dr Marc Guerrier, deputy director, Ethics area, AP-HP, CHU Saint-Louis, Paris. Mr Patrick Guez, quality and risks officer, Centre d’Accueil et de Soins Hospitaliers, Nanterre. Dr Benoît Guimbaud, medical doctor, director, accident management and risk prevention, LA SHAM, Lyon. Mrs Françoise Haffemayer, director and healthcare coordinator, retired, Le Mans. Dr Joseph Hajjar, medical doctor, head of the Hygiene and Epidemiology Department, Centre Hospitalier Général, Valence. Dr Jean Halligon, angiologist – vascular medicine, La Membrolle-sur-Longuenée. Mrs Ismaël Jamin, risk manager, Générale de Santé, Paris. Mrs Geneviève Jean-Louis, social and education officer, head of social service and technical consultant, EPS de Maison-Blanche, Paris. Dr Laurent Jouffroy, anaesthetist intensivist , Clinique des Diaconesses, Strasbourg. Mrs Marie-Jeanne Karle, director of nursing, Centre Cardiologique du Nord, Saint-Denis.
Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 104/120 Manuel de certification – Édition novembre 2008
Mrs Annie Labbé, user representative, president of the Association ARGOS 2001, Paris. Mr Philippe Laly, deputy director in charge of strategic guidance and quality, healthcare director, Association l'Élan Retrouvé, Paris. Mrs Anne Laverny, director, Economics and Logistics Department, Centre Hospitalier, Chartres. Mrs Anne-Marie Lecouturier, senior health supervisor, CHU de Caen. Dr Pierre Lefranc, specialist in emergency medicine, Société Hospitalière d’Assurances Mutuelles (SHAM), Lyon. M. Jean-Michel Lemauff, user representative, Ligue Nationale contre le Cancer, Vineuil. Mr Bruno Lucet, director of quality and risk management, AP-HP, University Hospital Centre Henri-Mondor, Créteil. Mrs Annick Macrez, director of quality and risk management, Groupe Hospitalier Bichat-Claude-Bernard, Paris. Mrs Zohra Malali, quality officer, Hôpital Saint-Camille, Bry sur Marne. Mrs Sophie Malvaux, quality, risk management and evaluation officer, Centre René-Gauducheau, Nantes. Mrs Marie-Paule Masseron, user representative, vice-president, FNAMOC, Paris. Dr Marie-Christine Moll, medical doctor, quality and risk officer, CHU, Angers. Mrs Maud Morardet, quality and risk management engineer, Groupe Public de Santé Perray-Vaucluse, Hôpital Henri-Ey, Paris. Mrs Christel Mouras, director, Hôpital Local, Mauléon. Mr Jean-Philippe Mousnier, sociologist, Murart Areo, Boulogne-Billancourt. Mrs Martine Naud, nursing supervisor, Clinique Psychiatrique MGEN, Rueil-Malmaison. Mrs Cherifa Nimal, deputy healthcare director, Hôpital Ambroise Paré, Marseille. Dr Jean Petit, medical doctor, in charge of quality, CHU de Rouen. Dr Marie-Pascale Pomey, Université de Montréal, Québec, Canada. Dr Christiane Privat, medical doctor, medical director, CMPR LAENNEC, Malakoff. Dr Jean-François Quaranta, medical doctor, chairman of the Health Vigilance and Risk Management Coordinating Committee, Hôpital de Cimiez, Nice. Dr Jean-Luc Quenon, risk management expert, CCECQA, Hôpital Xavier-Arnozan, Pessac. Mr Olivier Renaudeau, director, member of the Sustainable Development Committee, Clinique de la Reine Blanche, Orléans. Dr Gilles Ribeil, medical doctor, director general, Clinique Sainte-Anne, Langon. Mrs Isabelle Robineau, head of quality, Centre Hospitalier de Ville-Évrard, Neuilly-sur-Marne. Mr Emmanuel Rodriguez, confederation secretary, vice-president of CISS users, Confédération Syndicale des Familles, Paris. Mrs Séverine Romain, nursing health supervisor, Hôpital Local, Sully-sur-Loire. Dr Sylvie Rosenberg-Reiner, paediatrician, Hôpital Necker, Paris. Mr Frédéric Rossband, associate in the Quality, Communication and Safety Division, Centre Bouffard-Vercelli, Cerbert. Mrs Martine Sene-Bourgeois, user representative, retired nursing supervisor, surveyor, Paris. Mrs Michèle Sizorn, president, SOS Hépatites Paris-Île-de-France, Paris.

Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 105/120 Manuel de certification – Édition novembre 2008
Mrs Catherine Stamm, pharmacist, Centre Hospitalier Lyon-Sud, Pierre Bénite. Mr Jean-Jacques Stoltz, director of the Nursing Care Department, surveyor, Centre Hospitalier, Lourdes. Mrs Catherine Tardy, healthcare director, Hôpital Pédiatrique Gatien de Clocheville, CHRU, Tours. Mr Daniel Teissonnier, director, Oncology Centre for Région PACA, Générale de Santé, Centre de Radiothérapie de Clairval, Marseille. Mrs Corinne Tiberghien-Metzger, deputy director, CMCR Les Massues, Lyon. Dr Clotilde Watelet, pharmacist, president of CME-CLIN, Clinique Jeanne-d’Arc, Luneville. Dr Marc Weiner, psychiatrist, Réseau Plénitude, L’Arbresle. Mr Jean Wils, users’ rights officer, Hôpital Européen Georges-Pompidou, Paris. French Society of Physical Medicine and Rehabilitation (SOFMER) The working groups were steered by: Dr Nafissa Abdelmoumène, project manager, Certification Development Department, DAQSS. Dr Matthieu Boussarie, deputy head of the Certification Development Department, DAQSS. Dr Charles Bruneau, technical consultant, Division for the Improvement of Healthcare Quality and Safety. Mrs Anne Depaigne-Loth, project manager, Certification Development Department, DAQSS. Mrs Dominique Ferréol, project manager, Certification Development Department, DAQSS. Mrs Muriel Jakubowski, project manager, Certification Development Department, DAQSS. Mr Philip Laly, deputy head of the Healthcare Organisation Certification Department, surveyors section, DAQSS. Mr Raymond Le Moign, director, Division for the Improvement of Healthcare Quality and Safety. Dr Vincent Mounic, head of the Certification Development Department, DAQSS. Dr Isabelle Rullon, project manager, Certification Development Department, DAQSS. Mrs Yasmine Sami, project manager, Certification Development Department, DAQSS. Members of the V2010 working groups within HAS: Mrs Rose-Marie Andrieux, deputy head of the Healthcare Organisation Certification Department, DAQSS, HAS (until December 2007). Mr Bruno Bally, project manager, Practice Evaluation and Improvement Department, DAQSS. Mr Yann Barreau, project manager, Healthcare Organisation Certification Department, DAQSS. Mr Alexandre Biosse-Duplan, Mission for Relations with Patient and User Groups. Mrs Emmanuelle Blondet, project manager, Documentation Department, DCIP. Dr Philippe Cabarrot, technical consultant, Division for the Improvement of Healthcare Quality and Safety (DAQSS). Mrs Renée Cardoso, project manager, Documentation Department, Public Information, DCIP. Mr Thierry De Lambert, project manager, Healthcare Organisation Certification Department, DAQSS. Mrs Anne-Sophie Grossemy, project manager, Healthcare Organisation Certification Department, DAQSS.

Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 106/120 Manuel de certification – Édition novembre 2008
Dr Pierre Liot, project manager, Medical Information Quality Department (SQIM). Mr Bruno Lucet, deputy head of the Healthcare Organisation Certification Department, methods and organisation section, DAQSS. Mrs Fabienne Menot, Division for the Improvement of Healthcare Quality and Safety (DAQSS). Dr Roger Peschaud, policy officer, Certification Development Department, DAQSS. Mrs Émilie Prin-Lombardo, project manager, Healthcare Organisation Certification Department, DAQSS. Mr Stéphane Thibault, project manager, Healthcare Organisation Certification Department, surveyors section, DAQSS, HAS, Saint-Denis. Assistants: Mrs Rébéha Benabou, executive secretary, Certification Development Department, DAQSS. Mrs Sylvia Desnoyers, executive secretary, Certification Development Department, DAQSS.
Thirteen healthcare organisations which tested the pilot manual in June 2008
Centre Hospitalier Bichat Claude-Bernard - Paris (75) Centre Hospitalier de Rouffach (68) Centre Hospitalier du Pays d’Apt (84) Centre Hospitalier René Dubos - Pontoise (95) CHU d’Angers (49) Clinique Champeau - Béziers (34) Clinique les Émailleurs - Limoges (87) Clinique Sainte-Odile - Strasbourg (67) CRFF Le Brasset - Meaux (77) Hôpital Local de Bort-les-Orgues (19) Hôpital Saint-Joseph - Paris (75) Institut Paoli Calmette - Marseille (13) Maison de Repos Plein Soleil - Balaruc-les-Bains (34)
Reviewers of the V2010 pilot manual
Dr Bernard Abry, anaesthetist intensivist, Institut Hospitalier Jacques-Cartier, Massy. Dr Philippe-Emmanuel Adès, anaesthetist intensivist, Clinique de l’Europe, Rouen. Mr Richard Agnetti, Diet and Nutrition Mission, vice-president of CLAN Central de l’AP-HP, Department of Logistics and Hospital Ecology, Division of Estates, Logistics and Accommodation, AP-HP, Paris. Mrs Delphine Aigle, engineer in charge of quality and organisation, Centre Alexis-Vautrin, Vandœuvre-lès-Nancy.
Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 107/120 Manuel de certification – Édition novembre 2008
Mrs Isabelle Alquier, deputy head of the Healthcare Organisation Certification Department, certification systems section, DAQSS, HAS. Mr Christian Anastasy, director general, Compagnie Stéphanoise de Santé, Saint-Priest-en-Jarez. Dr Marie-France Angelini-Tibert, regional haemovigilance coordinator, DRASS Réunion Mayotte. Mrs Hélène Antonini-Castera, deputy director, quality director, Hôpital Gériatrique Les Magnolias, Longjumeau. Mrs Sylvia Arena Canault, head of quality, Maternité Catholique de Provence l’Étoile, Puyricard. Dr Charles Arich, PH, medical resuscitation unit, HAS surveyor, CHU, Nîmes. Dr François Aubart, Orthopaedics Department, Centre Hospitalier Simone-Veil, Eaubonne. Mrs Christine Aubeneau, senior health supervisor, Quality and Evaluation Division, CHU de Poitiers. Dr Régis Aubry, head of the Pain and Palliative Care Department and the Autonomy and Disability Centre, president of the Federation of Healthcare Networks of Franche Comté, CHU, Besançon. Mr Bertrand Bailleul, director, member of the Sustainable Development Committee, Hôpital Saint-Jean, Gennevilliers. Dr Christine Bara, director, Department of Healthcare Quality and Innovation, Institut National du cancer (INCa), Boulogne-Billancourt. Mrs Monique Bardet, quality officer, supervisory quality and risk management engineer, CH, Moulins-Yzeure. Mrs Catherine Barette, senior health supervisor, quality officer, HIA Val de Grâce, Paris. Mr Pierre-Jean Bargnoux, pharmacist, head of the Biology Department, Centre de Lutte contre le Cancer, Clermont-Ferrand. Dr Jean-Luc Baron, Montpellier. Mr Yan Barreau, project manager, Healthcare Organisation Certification Department, certification procedures section, DAQSS, HAS, Saint-Denis. Mrs Marie-France Barreau, deputy director, Centre Hospitalier, Niort. Mrs Andrée Barreteau, head of the Centre for Health and Medical-Social Organisation, Fédération Hospitalière de France (FHF), Paris. Mrs Yvette Barrière, health supervisor, Clinique Chénieux, Limoges. Mr Remi Batifoulie, deputy director, Polyclinique de Navarre, Pau. Miss Martine Baume, senior health supervisor, Centre Hospitalier Le Mas Careiron, Uzès. Mrs Élisabeth Beau, director, Mission nationale d’expertise et d’audit hospitalier (MeaH), Paris. Mrs Annick Bechet, healthcare director, Centre Hospitalier de Saint-Jean-de-Dieu, Lyon. Prof. Bertrand Becq-Giraudon, PU-PH, quality officer, Quality Division, CHU, Poitiers. Mrs Évelyne Belliard, head of the Department of Indicators for the Improvement of Hospital Quality, DAQSS, HAS, Saint-Denis. Mrs Béatrice Bellot, quality officer, Centre Hospitalier, Lorquin. Mrs Audrey Benini-Venet, quality engineer, Hôpital de Cimiez, Nice. Dr Sylvia Benzaken, PH, Central Immunology Laboratory, Hôpital de l’Archet, CHRU, Nice. Dr Éric Bérard, medical doctor, quality officer, Centre Médical de l’Argentière, L’Arbresle. Mrs Isabelle Bernardi, quality specialist, Vandœuvre. Dr Lucien Berte, geriatrician, Centre Hospitalier La Meynardie, Saint-Privat-des-Prés. Mrs Helena Beudaert-Izel, assistant manager, Healthcare Organisation Certification Department, certification procedures section, DAQSS, HAS, Saint-Denis. Dr Michèle Billing-Grima, MCU-PH, director, quality officer, CHU, Strasbourg.
Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 108/120 Manuel de certification – Édition novembre 2008
Mrs Véronique Binet-Décamps, head of the Certification Mission, AP-HP, Medical Policy Division, DAM, Paris. Mr Alexandre Biosse-Duplan, Mission for Relations with Patient and User Groups, HAS, Saint-Denis. Mrs Marie-Lise Biscay, hospital pharmacist, Centre Hospitalier des Pyrénées, Pau. Mrs Caroline Bizet, quality officer, CH Lannion-Trestel, Lannion. Mrs Marianne Blanc, midwife, HAS surveyor, quality and risk management officer, Centre Hospitalier, Annonay. Mrs Frédérique Blarel, project manager, Healthcare Organisation Certification Department, certification procedures section, DAQSS, HAS, Saint-Denis. Mr Didier Bled, quality officer, Centre Hospitalier Georges-Mazurelle, EPSM Hôpital-Sud, La Roche-sur-Yon. Dr Patrice Blondel, president, French Association of Health Risk Managers (AFGRIS), Hôpital Delafontaine, Saint-Denis. Dr Jean-Marie Bobillo, paediatric psychiatrist, area head, Centre Hospitalier Sainte-Marie, Privas. Mrs Nathalie Bocquillon, deputy director in charge of quality and performance assessment, Centre Hospitalier Universitaire, Amiens. Dr Henri Bonfait, orthopaedic and trauma surgeon, Hôpital Notre-Dame du Perpétuel Secours, Levallois-Perret. Mrs Corinne Bonnetaud, quality assistant, Hôpital de Jour Baudin, Limoges. Mr Bernard Bonnici, general adviser on healthcare organisations, DHOS, Ministry of Health, Youth, Sports and Collective Organisations, Paris. Dr Éric-Nicolas Bory, dentist, clinical epidemiologist, president of the Rhône-Alpes Buccodental Health and Disability Network, codirector of the Unit for Clinical Epidemiology, Disability, Dependence and Vulnerability of RECIF, HAS surveyor, head of the Dentistry Department, Centre Hospitalier Le Vinettier. Dr Roland Bouet, psychiatrist, CHS Henri-Laborit, Poitiers. Mr Joël Bouffies, director, Centre Hospitalier Sud-Francilien, Corbeil. Mr Frédéric Bousquet, head of the Department of Performance Indicators for the Improvement of Hospital Quality, DAQSS, HAS (until June 2008). Mrs Martine Bouyssié, quality officer, HAS surveyor, Institut Paoli Calmettes, Marseille. Dr Patrick Boyer, psychiatrist, chairman of the quality subcommittee of the CME, Centre Hospitalier Le Mas Careiron, Uzès. Prof. Alain Branchereau, Hôpital de la Timone, Vascular Department, Marseille. Prof. Serge Briancon, Department of Clinical Epidemiology and Evaluation, director of the School of Public Health, Hôpital Marin, Nancy. Dr Frédérique Brudon, general secretary, French Federation of Neurology, Clinique du Tonkin, Villeurbanne. Mr Nicolas Brun, policy officer, UNAF, Paris. Mr Damien Brunel, quality officer, CMRP Orcet, Hauteville-Lompnes. Dr Jean Bruxelle, president, French Society for the Study and Treatment of Pain (SFETD), Paris. Mr Philippe Burnel, general representative, Fédération de l’hospitalisation privée (FHP), Paris. Dr Véronique Bussy-Malgrange, pratitioner in hygiene, coordinator, Resclin Champagne-Ardenne, CLIN-Est regional branch office, CHU, Clinique de Champagne, Reims. Mr René Caillet, director general, president of the Nord-Pas-de-Calais Quality and Health Network, CRF L’Espoir, Hellemmes. Mr Tony-Marc Camus, deputy director, Centre Hospitalier, Saint-Yrieix-la-Perche. Dr Corinne Capponi Guillon, doctor of hygiene, Syndicat Interhospitalier, Brive Tulle Ussel.
Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 109/120 Manuel de certification – Édition novembre 2008
Mr Philippe Caralp, management and risk analysis consultant, Étaples. Mrs Aude Caria, psychologist, policy officer at the WHO Collaborative Centre, in charge of the users’ resource centre, Centre Hospitalier Sainte-Anne, Paris. Mrs Dominique Cartron, president, Soleil AFELT (Friends and Families of Children with Leukaemia or Tumours), Doué-la-Fontaine. Mrs Alice Casagrande, project manager, Agence nationale d’évaluation sociale et médicosociale (ANESM), Saint-Denis. Mrs Marie Castagne, quality officer, Hôpital de Jour Baudin, Limoges. Mr Paul Castel, president of the Conference of Directors General of Regional and University Hospital Centres, Director General, Hospices Civils, Lyon. Dr Anne Castot, public health doctor, head of the Department of Evaluation, Risk Surveillance and Information on Medicinal Products, Division of Evaluation of Medicinal and Biological Products, French Health Products Safety Agency (AFSSAPS), Saint-Denis. Dr Maxime Cauterman, public health doctor, head of pilot sites, Mission nationale d’expertise et d’audit hospitalier (MeaH), Paris. Dr Gilles Cebe, medical doctor, DIM, Centre Hospitalier Le Mas Careiron, Uzès. Mr Gérard Cettour-Baron, director, Division of Users, Quality and Communication, Expertise section, Centre Hospitalier Régional, Orléans. Mr Alain Chalochet, director, Geriatrics Hospital Group, Hospices Civils de Lyon. Mrs Christel Chambet, quality officer, Clinique Saint-Odilon, Moulins. Prof. Alain Chantepie, president, French Society of Paediatrics (SFP), CHU, Tours. Mr Michel Chanteur, director, CMCR des Massues, Lyon. Dr Serge Charmion, Internal Medicine Department, Hôpital Nord, CHU de Saint-Etienne. Mr Jean-Michel Chartier, director, Clinique des Trois Soleil, Boissise-le-Roi. Mrs Christiane Chevillard, senior health supervisor, deputy regional representative, National Association for the Training of Hospital Staff (ANFH Île-de-France), Paris. Dr Roger Ciais, cardiologist, director general, Clinique des Trois-Luc, Marseille. Mrs Sabine Cohen, deputy head of the Healthcare Organisation Certification Department, certification information section, DAQSS, HAS, Saint-Denis. Mrs Geneviève Col, quality coordinator, Centre Hospitalier Universitaire, Limoges. Prof. Cyrille Colin, Medical Information and Research Assessment Centre, Hospices Civils de Lyon, CEPPRAL, Lyon. Prof. Philippe Colombat, president, GRASSPHO, Haematology and Cell Therapy Department, CHRU Hôpital Bretonneau, Tours. Mrs Sylvie Combe, nursing supervisor, quality assurance officer, Clinique La Présentation, Fleury-les-Aubrais. Mr Joël Convert, nursing supervisor, Centre Psychothérapique de l’Ain, Bourg-en-Bresse. Mrs Françoise Cosani, quality officer, Groupe Hospitalier Les Cheminots, Draveil. Dr Hervé Creusvaux, head of the Safety and Quality Centre, Biomedicine Agency, Saint-Denis. Mr Christophe Crouzevialle, quality officer, SSR La Chênaie, Verneuil-sur-Vienne. Mr David Cuzin, deputy director in charge of quality and risk management, Centre Hospitalier, La Rochelle. Mrs Émilie Daimant, project manager, Healthcare Organisation Certification Department, certification procedures section, DAQSS, HAS, Saint-Denis.
Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 110/120 Manuel de certification – Édition novembre 2008
Dr Marie-José d’Alché-Gautier, president of the Lower Normandy Regional Health and Quality Network Association, head of the DIM, CHU, Caen. Mrs Marie-José Darmon, senior health supervisor, anaesthetist, Hôpital de Nice. Mrs Annick Darrieumerlou, quality officer, CMC Ambroise-Paré et Pierre-Cherest, Neuilly-sur-Seine. Dr Valentin Daucourt, public health doctor, member of the RéQUA, Besançon. Dr Jean-François de Frémont, nephrologist, mediator, Polyclinique Saint-Côme, Compiègne. Mr Ludovic de Gaillande, senior hospital technician, quality-certification branch, Hôpital Local, Sartène. Mr Olivier Debay, director general, Clinique du Sud, Carcassonne. Mr Jacques Defer, deputy director, HAS coordinating surveyor, Centre Hospitalier de Rouffach. Mrs Annie Defosse, retired nursing supervisor, Romans-sur-Isère. Mr Gérard Delahaye, director, Centre Hospitalier Philippe-Pinel, Amiens. Mr Thierry De Lambert, project manager, Healthcare Organisation Certification Department, surveyors section, DAQSS, HAS, Saint-Denis. Dr Christian Delaunay, specialist, Clinique de l’Yvette, Longjumeau. Mrs Claire Delon, director, Division of Organisation, Quality and Risk Prevention, Hôpital de l’Institut Curie, Paris. Mr Antoine de Riccardis, director general, Centre Hospitalier Charles-Perrens, Bordeaux. Dr Marie-Ange Desailly-Chanson, general adviser on healthcare organisations, head of coordination for support and advisory missions, DHOS, Ministry of Health, Youth, Sports and Collective Organisations, Paris. Dr Jacques Desbaumes, specialist, quality officer, Centre Léon-Bérard, Lyon. Mrs Chantal Deschamps, health mediator, member of the National Committee for the Accreditation of Healthcare User Groups, member of the CISS (AFVS), member of the National Advisory Committee on Ethics for the Life and Health Sciences, Paris. Prof. Alain Destée, president of the Conference of Presidents of University Hospital Medical Committees, Centre Hospitalier Universitaire, Lille. Dr Armelle Develay, hospital pharmacist, section H adviser to the Order of Pharmacists, honorary president of Synprefh, CHU, Nîmes. Mrs Aude-Emmanuelle Develay, project manager, Department of Indicators for the Improvement of Hospital Quality, DAQSS, HAS, Saint-Denis. Mr Jean-Pierre Deymier, director, Clinique Pasteur, Toulouse. Dr Daniel d'Hérouville, Maison Médicale Jeanne-Garnier, Paris. Mrs Isabelle Dorléans, project manager, Healthcare Organisation Certification Department, surveyors section, DAQSS, HAS, Saint-Denis. Prof. Étienne Dorval, president, Evaluation and accreditation of hepatogastroenterologists (EA-HGE), CHU Trousseau, Tours. Mrs Christiane Dosseh, project manager, Healthcare Organisation Certification Department, certification procedures section, DAQSS, HAS, Saint-Denis. Mrs Claudine Drouin, nursing supervisor, director of quality healthcare, Groupe Médipsy – Générale de Santé, Rennes. Dr Michel Dru, president, National Union of Hospital Anaesthetists and Intensivists (SNPH@R), Hôpital Henri Mondor, Créteil Cedex. Mr Fabrice Dubost, consultant, Rhône-Alpes Technical Division, SOGETI, Villeurbanne. Mr Hugues Dufey, director, Group for the Modernisation of Hospital Information Systems (GMSIH), Paris. Mrs Marie-Françoise Dumay, president, French Society for Risk Management in Healthcare Organisations (SoFGRES), quality and risk management policy officer, Île-de-France Regional Hospitalisation Agency, Paris.
Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 111/120 Manuel de certification – Édition novembre 2008
Mrs Claire Dupont, quality officer, AURA Paris, Paris. Prof. Isabelle Durand-Zaleski, head of the Evaluation Studies Unit, scientific director at the Health Policy Studies Institute, Hôpital Henri-Mondor, Créteil. Prof. Alain Durocher, anaesthetist intensivist, Department of Respiratory Emergencies, Medical Resuscitation and Hyperbaric Medicine, Hôpital Calmette, CHRU, Lille. Mrs Martine Dutoit, user representative, Advocacy, Paris. Dr Mounir El Mhamdi, project manager, Healthcare Organisation Certification Department, DAQSS, HAS, Saint-Denis. Dr Fabienne Empereur, hospital practitioner, head of the Evaluation Unit, Clinical Epidemiology and Evaluation Department, EVALOR, Hôpital Marin, Nancy. Mr Claude Ethuin, user representative, president of the Nord-Mentalités Association, member of the Regional Health Conference of Nord-Pas-de-Calais, Tourcoing. Mrs Christine Fabry, director of user relations, Hospices Civils, Lyon. Prof. Jean-Yves Fagon, director of medical policy, AP-HP, Paris. Dr Fadila Farsi, coordinating doctor, ONCORA network, CRLCC Léon-Bérard, Lyon. Mrs Élodie Faure, quality specialist, Centre Hospitalier Les Genêts d’Or, Évaux-les-Bains. Mrs Christine Feisthammel, healthcare director, Maternité Catholique de Provence l’Étoile, Puyricard. Dr Francis Fellinger, cardiologist, president of the Conference of Presidents of Hospital Medical Committees, Hospital Medical Committee, Centre Hospitalier, Haguenau. Mrs Claude Finkelstein, president, National Federation of Associations of Psychiatric Patients (FNAP Psy), Paris. Mr Pascal Forcioli, director, Picardie Regional Hospitalisation Agency, Amiens. Mrs Gabriele-Hélène Fradin, Group of Retired Educators Without Frontiers (GREF), administrator of Cofrade, Paris. Mr Vincent Franchi, head of studies, Nuclear Safety Authority, Paris. Prof. Patrice François, specialist in public health, head of the Health Monitoring Department, University Hospital Centre, Grenoble. Dr Marie-France Frutoso, president of the Medical Committee, Centre Hospitalier Le Mas Careiron, Uzès. Dr Pierre Gabach, Division for Healthcare Management and Organisation, Hospitalisation Department, Caisse Nationale d’Assurance Maladie des Travailleurs Salariés, Paris. Mr Gilles Gaebel, user representative, AVIAM. Prof. Rémi Gagnayre, professor of education sciences, Health Education Laboratory, UFR SMBH Léonard-de-Vinci, Université Paris-13 XIII, Villetaneuse. Mrs Christine Gardel, technical adviser on indicators and measures of programme impact, DAQSS, HAS, Saint-Denis. Prof. Laurent Gerbaud, Public Health Department, member of GREQUAU (Regional Quality Group in Auvergne), Hôtel-Dieu, CHU, Clermont-Ferrand. Mr Christophe Ghio, director, Centre Hospitalier Henri-Mondor, Aurillac.
Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 112/120 Manuel de certification – Édition novembre 2008
Mrs Monique Gibert, director of healthcare, director of human resources, quality officer, Maison de Santé, Épinay. Mrs Doris Gillig, director of quality and risk management, Centre Hospitalier, Mulhouse. Mr Patrice Giraud, head of quality assurance, ALURAD, Limoges. Dr Alexandra Giraud, GREQUAU Auvergne, CMRE Auvergne, Public Health Department, Hôtel-Dieu, CHU, Clermont-Ferrand. Mrs Bernadette Girol, quality specialist, Centre Hospitalier Esquirol, Limoges. Dr Jacques Glikman, PH, psychiatrist, Centre Médicopsychologique Tagore, Épinay-sur-Seine. Mr Jean-Luc Godet, director, Division of Ionising Radiation and Health, Nuclear Safety Authority, Paris. Mrs Fanny Gonçalves, quality officer, Centre Hospitalier Gériatrique, Cornil. Mrs Laurence Grasmagnac, CSI, Clinique du Colombier, Limoges. Mr Marcel Graziani, president, Collectif Interassociatif sur la Santé (CISS) Limousin, Limoges. Mrs Cécile Grelou, quality technician, Centre Hospitalier, Tulle. Dr Catherine Grenier, director, Department of Quality and Indicators, National Federation of Cancer Centres (FNCLCC), Paris. Dr Anne Gruson, pathologist, head of department, Centre Hospitalier, Arras. Mrs Claude Gueldry, director, Bureau of Quality Assurance and Health Economics Information for Private Hospitals (BAQIMEHP), Paris. Dr Jean-Pierre Guéraud, surgeon, CTRRF and Clinique Saint-Pierre, Perpignan. Mrs Geneviève Guérin, healthcare director, CLCC Nantes Atlantique, Saint-Herblain. Dr Marc Guerrier, deputy director, Ethics area, AP-HP, CHU Saint-Louis, Paris. Mr Patrick Guez, quality and risks officer, Centre d’Accueil et de Soins Hospitaliers, Nanterre. Mrs Gwenn Guichaoua, specialist, quality officer, Centre de Soins de Suite et de Réadaptation Le Bodio, Pontchâteau. Prof. Henri Guidicelli, Montesquieu-des-Albères. Mrs Béatrice Guillou, quality officer, Centre Hospitalier du Pays d’Eygurande, Monestier-Merlines. Mrs Françoise Haffemayer, director and healthcare coordinator, retired, Le Mans. Dr Joseph Hajjar, medical doctor, head of the Hygiene and Epidemiology Department, president, French Society of Hospital Hygiene (SFHH), Centre Hospitalier Général, Valence. Dr Jean Halligon, president, Conference of Presidents of Private Hospital Medical Committees (CNPCMEHP), Polyclinique de l’Espérance, Angers. Mr Joseph Halos, director, EPSM Lille-Métropole, Armentières. Mrs Lallia Hammadi, head of quality and risk management, Centre Médical des Sept Collines, Saint-Étienne. Mrs Frédérique Haniquaut, project manager, Healthcare Organisation Certification Department, certification procedures section, DAQSS, HAS, Saint-Denis. Mrs Catherine Hardy, healthcare director, vice-president of the Healthcare Quality and Safety Committee, CH de Pontoise. Dr Éric Hergon, director of quality and regulatory affairs, Établissement Français du Sang (EFS), La Plaine Saint-Denis. Mr Alain Hergott, director, Hôpital Local Intercommunal, Soultz-Issenheim. Dr Chantal Houlbert, medical pathologist, CHIC Alençon Mamers, Alençon.
Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 113/120 Manuel de certification – Édition novembre 2008
Mr Pierre Huin, PSPH, director of care arrangements and quality, Groupe Hospitalier Privé du Centre-Alsace, Colmar. Mrs Monique Hulin, senior health supervisor, Hôpital Édouard-Herriot, Hospices Civils de Lyon, Lyon. Dr Béatrice Janvoie-Ouillet, lung specialist, Centre Hospitalier, Blois. Mrs Geneviève Jean-Louis, social and education officer, head of social service and technical consultant, EPS de Maison-Blanche, Paris. Mr Philippe Jeanne, director, Clinique MGEN, Specialist Healthcare Organisation, Rueil-Malmaison. Dr Laure Jonca, medical information doctor, doctor in charge of medical affairs, vigilance coordinator, Hôpital Joseph-Ducuing, Toulouse. Mrs Audrey Joncour, project manager, Bureau of Quality Assurance and Health Economics Information for Private Hospitals (BAQIMEHP), Paris. Dr Laurent Jouffroy, anaesthetist intensivist , Clinique des Diaconesses, Strasbourg. Mrs Joëlle Jouneau, pharmacist, head of the Department of Quality, Hygiene and Risk Management, Institut Bergonie, Bordeaux. Dr Patrick Jourdain, president of the Healthcare Quality and Safety Committee, CH de Pontoise, Pontoise. Dr Jacques Jourdan, PU-PH specialist in internal medicine, head of department, head of centre, Groupe Hospitalo-Universitaire Carémeau, Nîmes. Dr Mikhaël Kassab, vascular surgeon, president of the Medical Committee, HAS CPD medical appraiser, Polyclinique de Poitiers. Dr Irène Kahn-Bensaude, president of the Public Health and Medical Demography Section, Ordre National des Médecins, Paris. Mrs Chantal Klein, health supervisor, Polyclinique de l’Atlantique, Saint-Herblain. Mrs Valérie Kozyreff-Vallin, Pompignac. Mr Jean-Pierre Lacroix, president, Collectif Interassociatif sur la Santé Languedoc-Roussillon (CISS Languedoc-Roussillon), Nîmes. Mrs Marie-Alexandrine Lagarde, quality officer, Centre Rééducation Réadaptation Fonctionnelle André-Lalande, Noth. Mrs Corinne Lahorgue Poulot, quality engineer, Association AURA Auvergne (Regional Home Dialysis Association), Chamalières. Mrs Laurence Laine, director of human resources, Clinique du Colombier, Limoges. Mr Philippe Lamoureux, director general, National Institute for Prevention and Health Education (INPES), Saint-Denis. Dr Monique Lathelize, hospital practitioner, member of GIP-REQUASS, CHU, Limoges. Mr Jean-Claude Laurens, policy officer, certification coordinator, Quality Division, Centre Hospitalier de Toulouse, Hôtel-Dieu, Toulouse. Dr Guillaume Laurent, director of the information system, CHR, Orléans. Mrs Virginie Laveaux, quality specialist, Centre Hospitalier, Saint-Yrieix-la-Perche. Prof. Maurice Laville, nephrologist, president, Association of Nephrology Societies and Unions (A2SN), Nephrology Department, Hôpital Édouard-Herriot, Université Claude Bernard, Lyon. Mr Marc Le Chartier, deputy director, Centre Hospitalier Valvert, Marseille. Mrs Béatrice Le Coz, quality assistant, SSR La Chênaie, Verneuil-sur-Vienne. Mr Fabrice Le Floch, quality officer, quality specialist, CH Henri-Mondor, Aurillac. Mrs Gaëlle Le Gallais, quality officer, Centre de Lutte contre le Cancer René-Huguenin, Saint-Cloud.
Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 114/120 Manuel de certification – Édition novembre 2008
Dr Corinne Le Goaster, medical epidemiologist, Alert Coordination Cell, Institut de Veille Sanitaire (InVS), Saint-Maurice. Dr Catherine Le Gouhir, PH, Department of Medical Information, Centre René-Gauducheau, Nantes. Mr Francis Le Jeune, senior health supervisor, quality officer, quality certification mission, Centre Hospitalier Montperrin, Aix-en-Provence. Mr Alain Le Henaff, administrative officer, Centre René-Gauducheau, Nantes. Mr Gilbert Le Pichon, director, CSI Logis des Francs, Cherveux. Dr Hervé Leclet, Professionnal Radiology Council, Institut Calot, Berck. Dr Jean-Alain Lefoll, psychiatrist, head of department, president of PME, Centre Hospitalier Guillaume-Régnier, Rennes. Mrs Marie-Claude Lefort, director of healthcare, general coordinator, Centre Hospitalier Universitaire, Angers. Dr Pierre Lefranc, specialist in emergency medicine, Société Hospitalière d’Assurances Mutuelles (SHAM), Lyon. Dr Michel Legmann, president, Ordre National des Médecins, Paris. Mrs Dominique Leygnac, vice-president, National Association of Legal Representatives for the Protection of Adults (ANGT/ANMJPM), Montpellier. Mr Dominique Libault, director, Social Security Division, Ministry of Health, Youth, Sports and Collective Organisations, Paris. Dr Pierre Liot, project manager, Medical Information Quality Department, HAS, Saint-Denis. Dr Hélène Logerot, medical adviser, Federation of Hospitals and Personal Assistance Organisations (FEHAP), Paris. Dr Jean-François Loriferne, anaesthetist intensivist, HAS surveyor, Hôpital Saint-Camille, Centre Hospitalier, Bry-sur-Marne. Mr André Loth, head of the Health System Computerisation Mission (MISS), Ministry of Employment, Social Relations and Solidarity, Ministry of Health, Youth, Sports and Collective Organisations, Paris. Mr Gérard Machet, hospital pharmacist, AP-HP, Hôpital Villemin Paul-Doumer, Nord University Hospital Group, Liancourt. Mrs Annick Macrez, vice-president of the French Association of Health Risk Managers (AFGRIS), quality director, Hôpital Bichat-Claude-Bernard, Paris. Mrs Isabelle Mahégalisson, quality coordinator, Quality Systems Development Office, DQRD, Quality in Health Network 44, CHU de Nantes-PIMESP, Nantes. Mr Antoine Mahieux, administrative officer, Centre Psychothérapique de Vion, Saint-Clair-de-la-Tour. Mrs Sophie Malvaux, quality, risk management and evaluation officer, Centre René-Gauducheau, Nantes. Mr Robert Marmocchi, HAS surveyor, former healthcare organisation director, retired, Ollières. Mr Bruno Mars, deputy head of Office SD1A, Social Security Division, Ministry of Health, Youth, Sports and Collective Organisations, Paris. Dr Michel Martin, Division for Healthcare Management and Organisation, Hospitalisation Department, Caisse Nationale d’Assurance Maladie des Travailleurs Salariés (CNAMTS), Paris. Mr Yannick Martin, health safety consultant, member of the scientific committee, LIEN, Paris. Dr Michel Marty, director, Division for Healthcare Management and Organisation, Hospitalisation Department, Caisse Nationale d’Assurance Maladie des Travailleurs Salariés, Paris.
Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 115/120 Manuel de certification – Édition novembre 2008
Mrs Aline Maserak, retired senior nurse, former member of the Healthcare Organisation Certification Committee (HAS), surveyor for the Haute Autorité de Santé, Salomé. Mrs Isabelle Mauras, project manager, Healthcare Organisation Certification Department, certification procedures section, DAQSS, HAS, Saint-Denis. Mrs Évelyne Melani, senior supervisor, quality officer, HAS surveyor, Centre Antoine-Lacassagne, Nice. Mrs Aline Mercier, director, HAS surveyor, Hôpital Local, Amplepuis. Dr Philippe Michel, medical director, CCECQA, Hôpital Xavier-Arnozan, Pessac. Dr Jeanne Mihura, oncologist, Institut Claudius-Régaud, Toulouse. Mrs Emmanuelle Minassoff, pharmacist, member of the Quality and Risk Management Cell, MGEN Soins Spécialisés et Court Séjour, Rueil-Malmaison. Prof. Jean-Claude Moisdon, École des Mines, Centre of Management Science, Paris. Mrs Anne Montaron, healthcare director, Centre Médical de Forcilles, Férolles-Attilly. Mrs Maud Morardet, quality and risk management engineer in charge of monitoring the organisation project, Groupe Public de Santé Perray-Vaucluse, Hôpital Henri-Ey, Paris. Mrs Élisabeth Moreau, health supervisor, quality and risk management officer, HAS surveyor, Centre Hospitalier Saint-Cyr, Villeneuve-sur-Lot. Mr Marc Morel, director, Collectif Interassociatif sur la Santé (CISS), Paris. Dr Leila Moret, PIMESP Department, CHU, Nantes. Mrs Annick Moulsma, head of department, Pharmadim section, Centre Hospitalier de Saint-Cyr, Saint-Cyr-au-Mont-d’Or. Mrs Sabine Mouney, quality coordinator, Clinique du Colombier, Limoges. Mr Gilbert Mounier-Shahmoradi, quality officer, Clinique des Diaconesses, Strasbourg. Mr Hervé Nabarette, head of the Medical Information Quality Department, HAS, Saint-Denis. Dr Patrick Nachin, director, RéQua, Besançon. Dr Claude Naudin, specialist, Centre Médical de Bligny, Briis-sous-Forges. Mrs Carmen Navarro, quality officer, Centre Hospitalier de Pontoise. Mr René Nething, director, head of the certification and contract section, Établissement Public de Santé Alsace-nord, Brumath. Mrs Cherifa Nimal, deputy healthcare director, Hôpital Ambroise-Paré, Marseille. Mr François Nocton, president, Association OLIVIER+, Help for sick children and their families, Centre de Rencontre de Brichebay, Senlis. Mrs Sophie Ollivier, project manager, Healthcare Organisation Certification Department, surveyors section, DAQSS, HAS, Saint-Denis. Dr Jacques Orvain, lecturer, École des Hautes Études en Santé Publique (EHESP), Rennes. Mrs Caroline Pansa, project manager, Healthcare Organisation Certification Department, methods and organisation section, DAQSS, HAS, Saint-Denis. Dr Patrice Papin, project manager, Practice Evaluation and Improvement Department, DAQSS, HAS, Saint-Denis. Mrs Françoise Papo, director, Réseau Santé Qualité Nord-Pas-de-Calais, Loos. Mrs Anne-Françoise Pauchet-Traversat, project manager, Department of Long-Term Conditions and Patient Support, DAQSS, HAS, Saint-Denis. Dr Jean Parrot, president, National Council of the Order of Pharmacists, Paris.
Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 116/120 Manuel de certification – Édition novembre 2008
Dr Nicole Perier, Continuing Professional Development policy officer, Quality and Certification Coordinating Committee, Division of Medical Policy, AP-HP, Paris. Mrs Sylvie Peron-Moukalou, psychiatrist, section head, Centre Hospitalier Henri-Laborit Hôpital de Jour, CECAT, Poitiers. Dr Agnès Perrin, Coordinating Committee for Vigilance and Prevention of Healthcare-Related Risks, SGRIVI, Hôpital Calmette, CHRU, Lille. Mrs Nathalie Peyrot, quality assistant, Clinique Chénieux, Limoges. Mrs Annie Podeur, director, Division for Hospitals and Organisation of Care, Ministry of Health, Youth, Sports and Collective Organisations, Paris. Mr Ronald Pontefract, director in charge of quality and safety measures, HAS surveyor, CHU d’Angers, Angers. Mr Pierre Portigliatti, director, Clinique le Méditerranée, La Roque-d’Anthéron. Mrs Frédérique Pothier, head of the Practice Evaluation and Improvement Department, DAQSS, HAS, Saint-Denis. Mrs Nadine Potier, DSI, Clinique du Colombier, Limoges. Mr Pierre-Jean Poulin, quality specialist, Centre Hospitalier Esquirol, Limoges. Mrs Catherine Pouyet, project manager, Healthcare Organisation Certification Department, certification procedures section, DAQSS, HAS, Saint-Denis. Mrs Emmanuelle Prada Bordenave, director general, Biomedicine Agency, Saint-Denis-la-Plaine. Miss Émilie Prin-Lombardo, project manager, Healthcare Organisation Certification Department, certification procedures section, DAQSS, HAS, Saint-Denis. Prof. Jean-Pierre Pruvo, secretary general, French Radiology Society, Paris. Mr Olivier Pujo, president, Association of Parents and Friends of Children Treated at the Institut Curie (APAESIC), Paris. Dr Jean-François Quaranta, medical doctor, chairman of the Health Vigilance and Risk Management Coordinating Committee, Hôpital de Cimiez, Nice. Mrs Claude Rambaud, president, Association Le Lien, Courtabœuf. Dr Pierre Rance, psychiatrist, Clinique Mon Repos, Marseille. Dr Thierry Ravel, lung specialist, coordinating doctor, quality officer, HAS surveyor, Centre Médical Rhône-Azur, Briançon. Mr Jean-Paul Georges Ray, deputy director general, HAS surveyor, Centre Médical de l’Argentière, Aveize. Dr Jean-François Rey, president, National Union of Confederated Specialist Doctors (UMESPE), Paris. Dr Gilles Ribeil, medical doctor, director general, Clinique Sainte-Anne, Langon. Mr Loïc Ricour, director, National Mission for the Development of Mediation, Information and Dialogue for Healthcare Safety (MIDISS), HAS, Saint-Denis. Mrs Annie Rigaut, director, GIP-REQUASS, Limoges. Mrs Isabelle Robineau, deputy director of quality and strategic affairs, L’Élan Retrouvé, Paris. Mr Emmanuel Rodriguez, confederation secretary, vice-president of CISS users, Confédération Syndicale des Familles, Paris. Mrs Séverine Romain, nursing health supervisor, Hôpital Local, Sully-sur-Loire. Dr Sylvie Rosenberg-Reiner, paediatrician, Hôpital Necker, Paris. Mr Frédéric Rossband, associate in the Quality, Communication and Safety Division, Centre Bouffard-Vercelli, Cerbert. Mrs Carole Rousse-Lussac, senior health supervisor, Brens. Mrs Anne Sananikone, quality officer, CH MANHES, Fleury-Mérogis.
Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 117/120 Manuel de certification – Édition novembre 2008
Dr Frédéric Sanguignol, medical director, HAS surveyor, Clinique du Château de Vernhes, Bondigoux. Mr Thomas Sannié, user representative, French Haemophiliac Association, Paris. Mr Christian Saout, president, Collectif Interassociatif sur la Santé (CISS), Paris. Mrs Marie-Claude Saux, president, French Clinical Pharmacy Society, Groupe Hospitalier Sud, Pessac. Mrs Marylène Schimmenti, physiotherapist, quality officer, Clinique Médicale du Mas de Rochet, Castelnau-le-Lez. Mrs Béatrice Schmitt, director of human resources, Clinique Chénieux, Limoges. Dr Christophe Schmitt, PH, paediatric psychiatrist, president of the Medical Committee, head of the Medical Information section, President of the CLIN, Centre Hospitalier de Jury-lès-Metz, Metz. Mr Hervé Segalen, president, Collectif Interassociatif sur la Santé (CISS) Île-de-France, Bobigny. Dr Christophe Segouin, head of the Public Health and Health Economics Department, AP-HP, Groupe Hospitalier Lariboisière – Fernand-Widal, Paris. Mrs Martine Séné-Bourgeois, retired health supervisor, user representative, Collectif Interassociatif sur la Santé (CISS), HAS surveyor, Paris. Mrs Andrée Sfeir, general representative, ÉVEIL Association, Croissy-sur-Seine. Dr Christian Sicot, secretary general, Le Sou Médical, Groupe MACSF, La Défense. Mr Grégory Sieradzki, project manager, Healthcare Organisation Certification Department, certification procedures section, DAQSS, HAS, Saint-Denis. Mrs Michèle Sizorn, president, SOS Hépatites Paris-Île-de-France, Paris. Dr Nicole Smolski, vice-president, National Union of hospital anaesthetists and intensivists (SNPH@R), Hôpital de la Croix-Rousse, Lyon. Prof. Annick Steib, president, French Board of Anaesthetists Internists (CFAR), Paris. Mr Jean-Jacques Stoltz, director of the Nursing Care Department, HAS surveyor, Centre Hospitalier, Lourdes. Mr Jean-Claude Stutz, coordinator of the Haute-Alsace sampling network, CSS, CH de Mulhouse, Mulhouse Cedex. Dr Catherine Tainturier, president of the Medical Committee, head of the Nuclear Medicine Department, Hôpital Foch, Suresnes. Mrs Sophie Tardieu, public health pharmacist, Medical Evaluation Cell, Assistance Publique Hôpitaux de Marseille, Marseille. Mrs Valérie Tarnaud, administrative officer, Clinique du Colombier, Limoges. Mr Stéphane Thibault, project manager, Healthcare Organisation Certification Department, surveyors section, DAQSS, HAS, Saint-Denis. Mr Emmanuel Thomas, quality-risk management engineer, Centre Hospitalier Alphonse-Guérin, Ploërmel. Mrs Corinne Tiberghien-Metzger, deputy director, CMCR Les Massues, Lyon. Mr Olivier Toma, director, president of the Sustainable Development Committee (C2DS), Clinique Champeau, Béziers. Mr Nicolas Touchon, quality officer, CRRF La Châtaigneraie, Menucourt. Dr Bénédicte Toulouse, coordinator of CEPPRAL, Hospices Civils de Lyon, Lyon. Dr Sandrine Touzet, PH in public health, head of the Continuing Professional Development Study Unit, Medical Information, Evaluation and Research Section, Hospices Civils, CEPPRAL, Lyon. Mr Loïc Turbel, head of organisation and methods, Clinique Saint-Yves, Rennes. Prof. Guy Vallancien, Institut Montsouris, Paris.
Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 118/120 Manuel de certification – Édition novembre 2008
Dr Patrice Van Amerongen, UNAFAM (National Union of Friends and Family of Psychiatric Patients), Paris Mr Frédéric Van Roekeghen, director general, Caisse Nationale de l’Assurance-Maladie des Travailleurs Salariés, Paris. Mrs Stéphanie Vazille, quality engineer and risk manager, Centre Hospitalier Pierre-Nouveau, Cannes. Mrs Catherine Vergely, president, Association ISIS, Villejuif Cedex. Mrs Christine Vermel, project manager, Healthcare Organisation Certification Department, methods and organisation section, DAQSS, HAS, Saint-Denis. Mrs Nathalie Vidal, quality officer, Clinique du Colombier, Limoges. Mr Romain Vignoli, director, Association for the Treatment of Kidney Failure (ATIR), Avignon. Dr Jean-Marc Villatte, quality coordinating doctor, Clinique du Grand Pré, Durtol. Mrs Barbara Walter, president, French Council of Children’s Rights Associations (COFRADE), Paris. Dr Clotilde Watelet, pharmacist, president of the CME-CLIN, Clinique Jeanne-d’Arc, Lunéville. Dr Patrick Werner, project manager, Practice Evaluation and Improvement Department, DAQSS, HAS, Saint-Denis. Mr Jean Wils, users’ rights officer, Hôpital Européen Georges-Pompidou, Paris. Mrs Françoise Wolf, healthcare director, Centre Hospitalier Universitaire, Limoges. Dr Sébastien Woynar, medical adviser, Mission Nationale d’Expertise et d’Audit Hospitalier (MeaH), Paris.
Healthcare organisations that reviewed the manual
Clinique de Verdaich – Gaillac-Toulza (31) Clinique de Médecine Physique et de Réadaptation Fonctionnelle Les Grands Chênes -Bordeaux (33) Centre Hospitalier de Béziers (34) Centre Maguelone – Castelnau-le-Lez (34) Centre Psychothérapique Saint-Martin de Vignogoul – Pignan (34) Centre de Soins Spécialisé Lanuéjols – Mende (48) Centre Hospitalier de Saint-Dizier (52) Clinique Notre-Dame-de-Pritz – Changé (53) Centre Psychothérapique de Nancy (54) ALPHA Santé – Hayange (57) Hôpitaux Privés de Metz (57) Centre Hospitalier du Quesnoy (59) Centre Hospitalier de Denain (59) Clinique Saint-Sauveur – Mulhouse (68) Clinique Médicale de Champvert – Lyon (69) Clinique Saint-Vincent de Paul – Lyon (69)
Infirmerie Protestante de Lyon – Caluire (69) Centre Hospitalier de La Savoie – Chambéry (73) ADAPT CMRP Les Baumes – Valence (26) Aude Social and Medical Association for the Elderly - Limoux (11) Centre Cardio Vasculaire Valmante – Marseille (13) Centre de Postcure Mentale ARGIA – Cambo-les-Bains (64) Centre de Rééducation et de Réadaptation Fonctionnelle André-Lalande – Noth (23) Centre Hospitalier Alphonse-Guérin – Ploërmel (56) Centre Hospitalier Bichat Claude-Bernard - Paris (75) Centre Hospitalier Charles-Perrens – Bordeaux (33) Centre Hospitalier de Compiègne (60) Centre Hospitalier de La Rochelle (17) Centre Hospitalier de Niort (79) Centre Hospitalier de Poitiers (86) Centre Hospitalier de Rouffach (68) Centre Hospitalier de Saint-Junien (87)
Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 119/120 Manuel de certification – Édition novembre 2008
Centre Hospitalier de Tulle(19) Centre Hospitalier Départemental Les Oudairies – La Roche-sur-Yon (85) Centre Hospitalier des Pyrénées – Pau (64) Centre Hospitalier du Mans (72) Centre Hospitalier du Pays d’Apt (84) Centre Hospitalier Émile Roux – Le Puy-en-Velay (43) Centre Hospitalier Esquirol – Limoges (87) Centre Hospitalier Intercommunal Châtillon-Montbard – Montbard (21) Centre Hospitalier Intercommunal de Cornouaille – Quimper (29) Centre Hospitalier Régional d’Orléans – Orléans (45) Centre Hospitalier René Dubos – Pontoise (95) Centre Hospitalier Valvert – Marseille (13) Centre Médical MGEN Action Sanitaire et Sociale Pierre-Chevalier – Hyères (83) Centre Psychothérapique de Nancy – Laxou (54) Centre René Gauducheau – Nantes (44) Centre Hospitalier d’Ardèche Méridionale – Aubenas (07) Centre Hospitalier Régional d’Orléans – Orléans (45) Centre Hospitalier Universitaire d’Angers (49) Centre Hospitalier Universitaire de Nice (06) Centre Hospitalier Universitaire de Reims (51) Clinique Champeau – Béziers (34) Clinique de l’Espérance – Rennes (35) Clinique du Docteur Vignoli – Générale de Santé – Salon-de-Provence (13) Clinique du Pré – Théza (66) Clinique du Val de Loire – Beaumont-la-Ronce (37) Clinique Les Émailleurs – Limoges (87) Clinique Mon Repos – Marseille (13) Clinique Pasteur – Toulouse (61)
Clinique Sainte-Odile – Strasbourg (67) CMC Ambroise-Paré et Pierre-Cherest – Neuilly-sur-Seine (92) CRF Léopold-Bellan – Chaumont-en-Vexin (60) CRFF Le Brasset – Meaux (77) CSSRA Marienbronn – Lobsann (67) EPSM Lille-Métropole – Armentières (59) Foyer de la Résidence des Boisseaux – Monéteau (89) Hôpital de l’Institut Curie – Paris (75) Hôpital Georges Clemenceau – Champcueil (91) Hôpital Intercommunal des Monts et Barrages – Saint-Léonard-de-Noblat (87) Hôpital Lenval – Nice (06) Hôpital Local de Bort-les-Orgues (19) Hôpital Saint-Joseph – Paris (75) Hôpital Saint-Louis – Paris (75) Institut Paoli-Calmette – Marseille (13) Maison de Repos Plein Soleil – Balaruc-les-Bains (34) Maison de Santé d’Épinay (93) Maternité Catholique de Provence l’Étoile – Aix-en-Provence (13) Pôle Hospitalier Mutualiste de Saint-Nazaire (44) Polyclinique Le Languedoc – Narbonne (11) Polyclinique Saint-Côme – Compiègne (60)
Remerciements
HAS – Direction de l’Amélioration de la Qualité et de la Sécurité des Soins 120/120 Manuel de c
Internet users
We are grateful to the internet users who have sent their opinions, suggestions and comments on the pilot manual to the V2010 mailbox: [email protected]
Corrections Should you wish to point out an error or omission in the list of reviewers, please e-mail us at: [email protected]
Top Related