







Languages
Pages
Legal


Full Terms & Conditions of access and use can be found athttp://www.tandfonline.com/action/journalInformation?journalCode=ierj20
Download by: [University of California, San Diego] Date: 23 October 2015, At: 02:50
Expert Review of Clinical Pharmacology
ISSN: 1751-2433 (Print) 1751-2441 (Online) Journal homepage: http://www.tandfonline.com/loi/ierj20
Ceftazidime–avibactam for the treatmentof complicated urinary tract infections andcomplicated intra-abdominal infections
Yogesh Mawal, Ian A Critchley, Todd A Riccobene & Angela K Talley
To cite this article: Yogesh Mawal, Ian A Critchley, Todd A Riccobene & Angela K Talley(2015): Ceftazidime–avibactam for the treatment of complicated urinary tract infectionsand complicated intra-abdominal infections, Expert Review of Clinical Pharmacology, DOI:10.1586/17512433.2015.1090874
To link to this article: http://dx.doi.org/10.1586/17512433.2015.1090874
Published online: 30 Sep 2015.
Submit your article to this journal
Article views: 38
View related articles
View Crossmark data
Ceftazidime–avibactam forthe treatment of complicatedurinary tract infections andcomplicated intra-abdominalinfectionsExpert Rev. Clin. Pharmacol.
Yogesh Mawal*1,Ian A Critchley2,Todd A Riccobene3
and Angela K Talley4
1Forest Laboratories, Inc., a subsidiary
of Allergan plc (formerly Actavis plc),
New Jersey, USA2Allergan plc, California, USA3Allergan plc (formerly Actavis plc),
Jersey City, NJ, USA4Allergan plc (formerly Actavis plc),
California, USA
*Author for correspondence:
Tel.: +1 201 245 1874
Treatment of complicated urinary tract infections and complicated intra-abdominal infectionsis increasingly difficult due to the rising prevalence of multidrug-resistant Gram-negativebacteria. Ceftazidime–avibactam is a combination of the established third-generationcephalosporin ceftazidime with avibactam, a novel non–b-lactam b-lactamase inhibitor,which restores the activity of ceftazidime against many b-lactamase–producing Gram-negative bacteria, including extended-spectrum b-lactamases and Klebsiella pneumoniaecarbapenemases. Clinical and nonclinical studies supporting the safety and efficacy ofceftazidime–avibactam include microbiological surveillance studies of clinically relevantpathogens, in vivo animal models of infection, pharmacokinetic/pharmacodynamic targetattainment analyses, Phase I clinical pharmacology studies, and Phase II/III studies in thetreatment of complicated intra-abdominal infections and complicated urinary tract infections,including patients with ceftazidime-nonsusceptible Gram-negative infections.
KEYWORDS: avibactam . ceftazidime . complicated intra-abdominal infections . complicated urinary tract infections. multidrug resistance
Both complicated intra-abdominal infections(cIAIs) and complicated urinary tract infec-tions (cUTIs) are common serious bacterialinfections in hospitalized patients and theycarry a considerable risk of morbidity andmortality [1,2]. The definition of a cIAI isusually an abscess formation or peritonitisbeyond the origin of the perforation into theperitoneal cavity, requiring an invasive proce-dure for source control [2]. Infections areoften polymicrobial and may include Gram-negative and Gram-positive organisms, inaddition to various anaerobes. Among theGram-negative pathogens associated withcIAIs, the most common are the Enterobac-teriaceae, especially Escherichia coli andKlebsiella spp. [2]. Urinary tract infections(UTIs) associated with structural or functionalurinary tract abnormalities, or pyelonephritis,are classified as cUTIs [1,3]. E. coli isthe predominant Gram-negative uropathogen,
although other Enterobacteriaceae includingKlebsiella spp. and Gram-negative bacteriasuch as Pseudomonas aeruginosa are frequentlyencountered [4].
Over the last 30 years, b-lactam antibioticsincluding second- and third-generation cepha-losporins, b-lactam/b-lactamase inhibitor com-binations and carbapenems have been widelyused in clinical practice for the treatment ofcIAIs and cUTIs because of their broad cov-erage of clinically important Gram-negativebacteria. For many of these organisms, resis-tance is mediated by the production ofb-lactamases such as CTX-M-like enzymes,AmpC, and more recently, carbapenemasessuch as OXA-48 and K. pneumoniae carbape-nemases (KPCs) [4,5]. The US Center forDisease Control has identified both extended-spectrum b-lactamases (ESBLs) andmultidrug-resistant (MDR) P. aeruginosa asserious public health threats in USA, and
10.1586/17512433.2015.1090874 ISSN 1751-2433 1
Drug Profile
Early online, 1–17 (2015)
www.tandfonline.com © 2015 Actavis/Allergen
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
02:
50 2
3 O
ctob
er 2
015

carbapenemase-resistant Enterobacteriaceae (CRE) as an urgentthreat [6].
Since their emergence in 2001, CRE have proliferated asproblematic pathogens in hospitals in USA and worldwide [7].Carbapenemase-mediated resistance among these pathogens,including KPC-producing strains, leaves clinicians with fewoptions for safe and effective treatment [8–11]. Last-resort ther-apy such as colistin, either as monotherapy or in combinationwith a carbapenem, is not supported by solid clinical evidenceand carries a risk of adverse events (AEs) that may harm theindividual patient [12].
Infections caused by KPC-producing Enterobacteriaceae arecurrently limited to inpatient facilities; however, their high pro-pensity for transmission presents an urgent public health threat,necessitating aggressive infection control measures [6]. An out-break of KPC infections at the US National Institutes ofHealth in 2011 that was traced to a single patient resulted in18 patients being infected, of whom 11 died [13]. This outbreakand a more recent series of cases of CRE infections associatedwith endoscopic retrograde cholangiopancreatography at theUniversity of California, Los Angeles [14] outline the challengesfaced by healthcare centers in minimizing the risk of transmis-sion and highlight the necessity for developing effective antibi-otics to manage infections caused by MDR isolates.
Combining a b-lactam antibiotic with a b-lactamase inhibi-tor has been a well-proven and effective strategy for combatingresistance [5]. Ceftazidime–avibactam is the combination of cef-tazidime, an established, third-generation broad-spectrum ceph-alosporin, with avibactam, a novel non–b-lactam b-lactamaseinhibitor (formerly known as NXL104 and AV1330A). Ceftazi-dime, which has a well-established safety profile, was approvedin USA in 1985 and is currently indicated for the treatment ofmany types of bacterial infections including uncomplicated andcomplicated UTI and intra-abdominal infection (IAI) (FOR-TAZ; GlaxoSmithKline, Research Triangle Park, NC, USA)[15]. However, the efficacy of ceftazidime is increasingly com-promised by the spread of b-lactamase–producing pathogens.Avibactam exerts inhibitory activity against multiple serine-based b-lactamases including Ambler class A ESBLs, class A
KPCs, class C (AmpC) enzymes andsome class D (OXA) enzymes, which is abroader spectrum of b-lactamase inhibi-tory activity than other currently availableb-lactamase inhibitors, but is not activeagainst class B (the metallo-b-lactamases).As a single agent, avibactam has nomeaningful antimicrobial activity at ther-apeutic concentrations, but restores theactivity of a b-lactam such as ceftazidimeagainst a broad range of b-lactamase–producing bacteria [5].
New regulatory pathway options,described recently by the US FDA [3],were intended to address urgent unmetmedical needs for antibiotics in the treat-
ment of MDR Gram-negative bacterial infections. Theseallowed for a revised ceftazidime–avibactam development strat-egy that permitted its approval prior to the availability ofPhase III data for the treatment of adult patients with cUTI,including pyelonephritis, or cIAI, when used in combinationwith metronidazole (AVYCAZ�; Forest Pharmaceuticals, Inc.,a subsidiary of Forest Laboratories, LLC, Cincinnati, OH,USA) [16]. The ceftazidime–avibactam prescribing informationrecommends reserving ceftazidime–avibactam for use in patientswho have limited or no alternative treatment options, based onthe limited clinical safety and efficacy data that are available.
This review summarizes the in vitro and in vivo antibacterialactivity, pharmacodynamic (PD) and pharmacokinetic (PK)properties of ceftazidime–avibactam, and its safety, tolerabilityand efficacy observed in cIAI and cUTI clinical studies.
ChemistryCeftazidime is a semi-synthetic, b-lactam antibacterial drug; itis a pentahydrate of (6R,7R,Z)-7-(2-(2-aminothiazol-4-yl)-2-(2-carboxypropan-2-yloxyimino)acetamido)-8-oxo-3-(pyridinium-1-ylmethyl)-5-thia-1-aza-bicyclo[4.2.0]oct-2-ene-2-carboxylate.Its molecular weight is 636.6. The empirical formula isC22H32N6O12S2 [16].
The chemical structure of avibactam is sodium [(2S,5R)-2-carbamoyl-7-oxo-1,6-diazabicyclo[3.2.1]octan-6-yl] sulfate. Itsmolecular weight is 287.23. The empirical formula isC7H10N3O6SNa [16].
Mode of actionCeftazidime, like other b-lactams, inhibits bacterial cell wallsynthesis by binding to the active sites of penicillin-bindingproteins, ultimately resulting in cell death [15].
Avibactam is a potent member of a novel class of non–b-lactam inhibitors called diazabicyclooctanes [17]. The avibactamcarbonyl carbon residue at position 7 forms a covalent bondwith the active site serine residue of b-lactamases, which isresponsible for binding to b-lactams and rendering them inac-tive [18]. Subsequently, avibactam detaches and its five-membered urea ring is recyclized, regenerating intact avibactam
A B
N
N
O
O
O
OOH
H2N
•5H2O
H2NS
N N+
N
HN
N
SO
O
O O–
OSO3Na
Figure 1. Chemical structures of ceftazidime and avibactam. (A) Ceftazidime pen-tahydrate, molecular weight, 636.6 g/mol. (B) Avibactam sodium, molecular weight,287.23 g/mol.Reproduced from the US Package [16].
Drug Profile Mawal, Critchley, Riccobene & Talley
2 Expert Rev. Clin. Pharmacol.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
02:
50 2
3 O
ctob
er 2
015

which is available to bind further b-lactamase molecules. Thehalf-life for deacylation and release of intact avibactam fromthe b-lactamase TEM-1 enzyme is around 16 min [18].Avibactam’s inhibition of b-lactamases by reversible acylationdiffers from that of the b-lactam b-lactamase inhibitors clavu-lanic acid, sulbactam and tazobactam, which, after binding tothe active site, are hydrolyzed and rendered inactive.A hydrolytic route has been proposed for the deacylation ofavibactam by the carbapenemase KPC-2, although the slowkinetics of this reaction means that it is unlikely to curtail theclinical effectiveness of ceftazidime–avibactam against Gram-negative bacteria harboring this enzyme [19].
Avibactam has a broader range of activity against clinicallyimportant b-lactamases than clavulanic acid, tazobactam andsulbactam (TABLE 1) [19–27]. Clavulanic acid and tazobactam (but notsulbactam) inhibit common class A b-lactamases, including SHVand the ESBL CTX-M, but the activity of avibactam extends toinhibition of KPCs [21,23], class C enzymes such as AmpC [18,27–29]
and specific class D enzymes (e.g., OXA-48) [18,19]. Thehigher potency of avibactam’s inhibition of b-lactamases com-pared with clavulanate, sulbactam and tazobactam has beenshown by lower IC50 (range 3–170 nM) and reduced reactivationrates for class A and C b-lactamases, including TEM-1,KPC-2 and P99, and AmpC from P. aeruginosa [23,30].
MicrobiologySpectrum of activity against ceftazidime-resistant
pathogens
Many in vitro studies have shown that the addition of avibac-tam to ceftazidime restores activity against b-lactamase–producing strains of Gram-negative bacteria (TABLE 2). Avibactamat a fixed concentration of 4 mg/l in combination withceftazidime has been shown to reduce the MIC90 value of cef-tazidime by >128-fold to £8 mg/l against KPC-producing
Enterobacteriaceae [23,30–32], which is the FDA susceptibilitybreakpoint for ceftazidime–avibactam [16]. The activity of cefta-zidime–avibactam against CTX-M producers among Enterobac-teriaceae increased by 8–32-fold compared with ceftazidimealone, and the MICs reduced to <1 mg/l [21,32]. Against TEMor SHV b-lactamase–producing E. coli and K. pneumoniaestrains, the addition of avibactam reduced the MIC by‡256-fold compared with ceftazidime alone [32].
AmpC-mediated ceftazidime resistance in P. aeruginosastrains was reversed with ceftazidime–avibactam, reducing theMIC values for fully derepressed mutants and isolates to£8/4 mg/l [33], the FDA susceptibility breakpoint for ceftazi-dime–avibactam against P. aeruginosa [16].
Microbiology surveillance studies
Recent microbiological studies have revealed a concerningincrease in b-lactamase–producing strains of Gram-negativebacteria in USA. In 2005, 1.7% of E. coli and 3.2% ofK. pneumoniae isolates were ESBL producing and by 2011,these rates had increased to 7.3 and 13.1%, respectively [34].A study conducted in 24 centers in USA between 2009 and2011 found that 6.8% of E. coli isolates and 10.3% of K. pneu-moniae isolates from patients with UTI were ESBL pro-ducers [35]. Analysis of contemporary US surveillance datacollected in 2012 showed that ESBL prevalence rates for bothE. coli and K. pneumoniae were in excess of 10% in most ofthe nine US Census Bureau regions [4]. The proportion ofCRE strains reported in USA rose from 1.2% in 2001 to 4.2%in 2011, with CREs reported at three-times more centers inthe northeast than in the south, midwest and west. Rates of upto 21% have been recorded in major metropolitan areas [8–11].
The in vitro activity of ceftazidime–avibactam against Gram-negative clinical isolates has been evaluated in two studies inNorth/Latin America and two studies based solely in
Table 1. Summary of b-lactamase spectrum of avibactam activity compared with clavulanic acid andtazobactam.
Amblerclass
Functionalsubgroup
b-Lactamase Avibactam Clavulanicacid
Tazobactam Sulbactam
Class A
(serine)
2be
2f
CTX-M, PER, VEB
TEM, SHV, ESBLs
GES
KPC
Yes
Yes
Yes
Yes
Yes
Yes
Yes
No
Yes
Yes
Yes
No
No
No
No
No
Class B
(metallo)
3a IMP, VIM, NDM No No No No
Class C
(serine)
1e
1
Chromosomal Enterobacteriaceae AmpC
Chromosomal Pseudomonas AmpC
Plasmidic ACC, DHA, FOX, LAT, MIX, MIR,
ACT
Yes
Yes
Yes
No
No
No
No
No
No
Yes
Yes
Yes
Class D
(serine)
2d
2de
2df
Penicillinase-type OXA-1, -10, -13
Penicillinase-type OXA-31
Carbapenemase-type OXA-23, -40, -48, -58
Variable†
Variable
Variable
Variable
Variable
Variable
Variable
Variable
Variable
No
No
No
†Variable activity is due to variable sequence homology among members of Class D family.Data from [19,21–27].
Ceftazidime–avibactam for cUTI & cIAI Drug Profile
3www.tandfonline.com
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
02:
50 2
3 O
ctob
er 2
015

USA [36–40]. The addition of avibactam to ceftazidime resultedin a 128-fold reduction in the MIC90 value against 1132 clini-cally relevant isolates of K. pneumoniae and Enterobacter spp.collected from hospitalized patients in Latin America andUSA [38]. In a study of clinical isolates from patients admittedto Canadian hospital wards (the CANWARD study), avibac-tam at a fixed concentration of 4 mg/l reduced the MIC90
value of ceftazidime by >64-fold against ESBL-producingK. pneumoniae and by >512-fold against ESBL-producing andAmpC-hyperproducing E. coli [39].
The US-based study by Castanheira et al. was conducted aspart of the International Network for Optimal Resistance Mon-itoring (INFORM) program. A total of 20,709 isolates werecollected from patients with bloodstream infection, pneumonia,skin/soft tissue infections, UTIs and IAIs in 79 US hospitalsbetween 2010 and 2013 [37]. The other US-based study, byFlamm et al., collected isolates from 501 patients with IAIsand 2356 patients with UTIs from 73 centers during 2012 [36].
Both US-based studies confirmed the in vitro activity ofceftazidime–avibactam against Enterobacteriaceae (TABLES 3 & 4)
and P. aeruginosa (TABLE 5) [36,37]. The ceftazidime–avibactam
MIC90 values of £0.25 mg/l against Enterobacteriaceae arelower than the FDA susceptibility breakpoint for ceftazidime–avibactam of £8/4 mg/l [16], and compared favorably with cef-tazidime MIC90 values of 2–32 mg/l. MIC90 values of ceftazi-dime–avibactam were £0.5 mg/l against E. coli and Klebsiellaspp. in both studies, and ceftazidime–avibactam was also highlyactive against contemporary clinical isolates of Enterobacterspp., Citrobacter spp., Morganella morganii, Proteus mirabilis,Proteus vulgaris and Serratia marcescens, with MIC90 valuesranging from 0.06 to 0.5 mg/l [36,37].
Potent activity against isolates that produced the commonlydetected b-lactamases in US hospitals was demonstrated by cef-tazidime–avibactam in the INFORM program, with MIC90
values ranging from 0.25–2 mg/l against the isolates producingKPCs, CTX-M-14- and -15–like b-lactamases, SHV and plas-midic AmpCs [37]. Flamm et al. reported that avibactamrestored the activity of ceftazidime against extended-spectrumcephalosporin-resistant strains (ceftazidime MIC90 ‡32 mg/l)with MIC90 values reduced to 0.25 mg/l (UTI) and 0.5 mg/l(IAI) against E. coli, and to 1 mg/l (UTI) and 2 mg/l (IAI)against K. pneumoniae [36].
Table 2. Summary of in vitro studies of ceftazidime–avibactam activity against b-lactamase–producingstrains of Gram-negative bacteria.
Author (year) Enzymes and pathogens Outcome Ref.
Levasseur et al.
(2015)
TEM or SHV among
Escherichia coli and Klebsiellapneumoniae strains
‡256-fold reduction in MIC with ceftazidime–avibactam compared with
ceftazidime alone
[32]
CTX-M producers among
Enterobacteriaceae
8–32-fold reduction in MIC with ceftazidime–avibactam compared with
ceftazidime alone
KPC producers among
Enterobacteriaceae
>128-fold reduction in MIC with ceftazidime–avibactam compared with
ceftazidime alone
Aktas (2012) OXA-48 or CTX-M-15 in
K. pneumoniae; CTX-M-15 in
E. coli
MIC90 against OXA-48 reduced to 0.5 mg/l with ceftazidime–avibactam
compared with 512 mg/l for ceftazidime alone;
MIC90 against CTX-M-15 reduced to 0.25 mg/l from 64 mg/l in
K. pneumoniae and to <0.008 mg/l from 32 mg/l in E. coli
[31]
Livermore et al.
(2011)
CTX-M, KPC, OXA-48 in
E. coli
MIC reduced to 0.25–1 mg/l with ceftazidime–avibactam from ‡64 mg/l with
ceftazidime alone
[22]
Lagace�-Wiens et al.
(2011)
AmpC-hyperproducing E. coli 128-fold reduction in MIC90 to 1 mg/l with ceftazidime–avibactam from
>64 mg/l with ceftazidime alone
[39]
Mushtaq
(2010)
AmpC depressed strains in
Pseudomonas aeruginosa
MICs reduced to £8 mg/l with ceftazidime–avibactam at fixed dose of 4 mg/l
from 64–128 mg/l with ceftazidime alone
[33]
Endimiani
(2009)
KPC isolates in
K. pneumoniaeMIC90 reduced to £8 mg/l with ceftazidime–avibactam from ‡512 mg/l with
ceftazidime
[87]
Stachyra et al.
(2009)
KPC-2-producing
Enterobacteriaceae
Avibactam at a fixed dose of 4 mg/l with ceftazidime reduced MIC 1000-fold
to £1 mg/l (E. coli, K. pneumoniae) and to £8 mg/l (Enterobacter cloacae) from64–1024 mg/l with ceftazidime alone
[23]
Livermore et al.
(2008)
CTX-M-15-like-producing
Enterobacteriaceae
MIC reduced to 0.25–1 mg/l with ceftazidime–avibactam (avibactam at fixed
dose 4 mg/l) from ‡64 mg/l with ceftazidime alone
[21]
Other CTX-M types in
Enterobacteriaceae
MIC reduced to 0.12–1 mg/l with ceftazidime–avibactam from 2–8 mg/l with
ceftazidime alone
Drug Profile Mawal, Critchley, Riccobene & Talley
4 Expert Rev. Clin. Pharmacol.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
02:
50 2
3 O
ctob
er 2
015
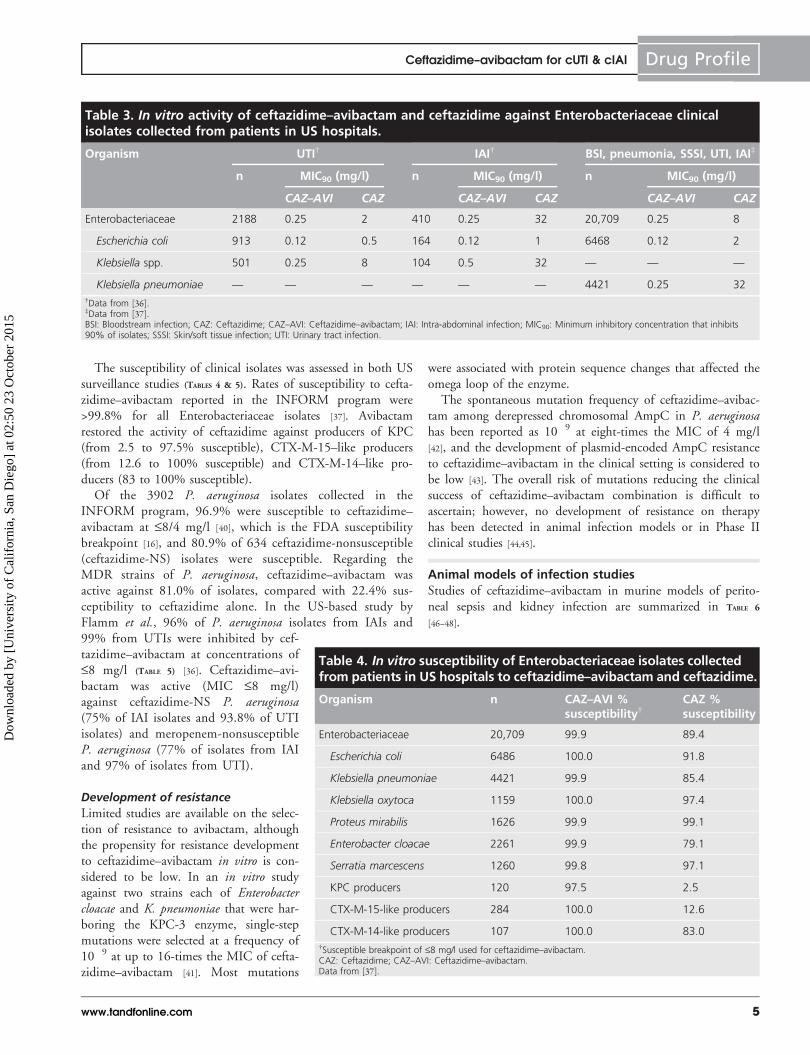
The susceptibility of clinical isolates was assessed in both USsurveillance studies (TABLES 4 & 5). Rates of susceptibility to cefta-zidime–avibactam reported in the INFORM program were>99.8% for all Enterobacteriaceae isolates [37]. Avibactamrestored the activity of ceftazidime against producers of KPC(from 2.5 to 97.5% susceptible), CTX-M-15–like producers(from 12.6 to 100% susceptible) and CTX-M-14–like pro-ducers (83 to 100% susceptible).
Of the 3902 P. aeruginosa isolates collected in theINFORM program, 96.9% were susceptible to ceftazidime–avibactam at £8/4 mg/l [40], which is the FDA susceptibilitybreakpoint [16], and 80.9% of 634 ceftazidime-nonsusceptible(ceftazidime-NS) isolates were susceptible. Regarding theMDR strains of P. aeruginosa, ceftazidime–avibactam wasactive against 81.0% of isolates, compared with 22.4% sus-ceptibility to ceftazidime alone. In the US-based study byFlamm et al., 96% of P. aeruginosa isolates from IAIs and99% from UTIs were inhibited by cef-tazidime–avibactam at concentrations of£8 mg/l (TABLE 5) [36]. Ceftazidime–avi-bactam was active (MIC £8 mg/l)against ceftazidime-NS P. aeruginosa(75% of IAI isolates and 93.8% of UTIisolates) and meropenem-nonsusceptibleP. aeruginosa (77% of isolates from IAIand 97% of isolates from UTI).
Development of resistance
Limited studies are available on the selec-tion of resistance to avibactam, althoughthe propensity for resistance developmentto ceftazidime–avibactam in vitro is con-sidered to be low. In an in vitro studyagainst two strains each of Enterobactercloacae and K. pneumoniae that were har-boring the KPC-3 enzyme, single-stepmutations were selected at a frequency of10�9 at up to 16-times the MIC of cefta-zidime–avibactam [41]. Most mutations
were associated with protein sequence changes that affected theomega loop of the enzyme.
The spontaneous mutation frequency of ceftazidime–avibac-tam among derepressed chromosomal AmpC in P. aeruginosahas been reported as 10�9 at eight-times the MIC of 4 mg/l[42], and the development of plasmid-encoded AmpC resistanceto ceftazidime–avibactam in the clinical setting is considered tobe low [43]. The overall risk of mutations reducing the clinicalsuccess of ceftazidime–avibactam combination is difficult toascertain; however, no development of resistance on therapyhas been detected in animal infection models or in Phase IIclinical studies [44,45].
Animal models of infection studiesStudies of ceftazidime–avibactam in murine models of perito-neal sepsis and kidney infection are summarized in TABLE 6
[46–48].
Table 3. In vitro activity of ceftazidime–avibactam and ceftazidime against Enterobacteriaceae clinicalisolates collected from patients in US hospitals.
Organism UTI† IAI† BSI, pneumonia, SSSI, UTI, IAI‡
n MIC90 (mg/l) n MIC90 (mg/l) n MIC90 (mg/l)
CAZ–AVI CAZ CAZ–AVI CAZ CAZ–AVI CAZ
Enterobacteriaceae 2188 0.25 2 410 0.25 32 20,709 0.25 8
Escherichia coli 913 0.12 0.5 164 0.12 1 6468 0.12 2
Klebsiella spp. 501 0.25 8 104 0.5 32 — — —
Klebsiella pneumoniae — — — — — — 4421 0.25 32
†Data from [36].‡Data from [37].BSI: Bloodstream infection; CAZ: Ceftazidime; CAZ–AVI: Ceftazidime–avibactam; IAI: Intra-abdominal infection; MIC90: Minimum inhibitory concentration that inhibits90% of isolates; SSSI: Skin/soft tissue infection; UTI: Urinary tract infection.
Table 4. In vitro susceptibility of Enterobacteriaceae isolates collectedfrom patients in US hospitals to ceftazidime–avibactam and ceftazidime.
Organism n CAZ–AVI %susceptibility†
CAZ %susceptibility
Enterobacteriaceae 20,709 99.9 89.4
Escherichia coli 6486 100.0 91.8
Klebsiella pneumoniae 4421 99.9 85.4
Klebsiella oxytoca 1159 100.0 97.4
Proteus mirabilis 1626 99.9 99.1
Enterobacter cloacae 2261 99.9 79.1
Serratia marcescens 1260 99.8 97.1
KPC producers 120 97.5 2.5
CTX-M-15-like producers 284 100.0 12.6
CTX-M-14-like producers 107 100.0 83.0
†Susceptible breakpoint of £8 mg/l used for ceftazidime–avibactam.CAZ: Ceftazidime; CAZ–AVI: Ceftazidime–avibactam.Data from [37].
Ceftazidime–avibactam for cUTI & cIAI Drug Profile
5www.tandfonline.com
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
02:
50 2
3 O
ctob
er 2
015

A murine model of pyelonephritis caused by injection ofapproximately 104 CFU of AmpC- or ESBL-producing Entero-bacteriaceae into the kidney of immunocompromised miceassessed ceftazidime alone and combined with avibactam andadministered at 4, 8, 24 and 32 h post-infection [46]. The bac-terial burden at 48 h was reduced by 2.6 log10–4.5 log10 CFUwith ceftazidime–avibactam, compared with the group givenceftazidime alone (p < 0.05).
In a murine septicemia model, ceftazidime–avibactam dem-onstrated potent in vitro activity and efficacy againstceftazidime-resistant Enterobacteriaceae producing class A andC b-lactamases [47]. Ceftazidime–avibactam in a 4:1 ratioagainst two KPC-producing strains of K. pneumoniae, bothwith ceftazidime MIC values of ‡256 mg/l, reduced themedian effective doses for 50% (ED50) of mice to 15.1 mg/kg(K. pneumoniae VA-361) and 3.8 mg/kg (K. pneumoniaeVA-406), compared with 1578 and 709 mg/kg, respectively,with ceftazidime alone [47]. In a second murine septicemiastudy of ESBL- and AmpC-producing Enterobacteriaceae iso-lates (ceftazidime MIC ‡64 mg/l), ceftazidime–avibactam in a4:1 ratio reduced the unit dose ED50 to <5–58 mg/kg from>84 mg/kg with ceftazidime alone [48]. Unit dose ED50 valuesagainst two AmpC and six CTX-M producers ranged from 2–27 mg/kg for ceftazidime–avibactam, compared with >90 mg/kg for ceftazidime alone.
Ceftazidime in combination with avibactam has also demon-strated significant bacterial killing and efficacy in a number ofother animal models of infection, including the neutropenicmouse thigh infection model [47,49,50] and lung infectionmodel [51–53], and a rabbit model of meningitis in animalsinoculated with ceftazidime-NS Enterobacteriaceae strains [54].The organisms evaluated in these studies included bacteria thatproduce the clinically important class A and C b-lactamasesincluding the ESBL, KPC and AmpC enzymes.
PharmacodynamicsThe percent of time that unbound concentration of the drugsremains above the MIC over a dosing interval (%f T > MIC)is well-established as the PK/PD index that best defines theefficacy for b-lactam antibiotics such as ceftazidime [55–58],whereas the percent of time that free drug concentrations areabove a ‘threshold’ concentration (CT) over a dose interval (%f T > CT) was determined to be the PK/PD index associatedwith the efficacy of avibactam [52,59–61].
Target for ceftazidime
A PK/PD target of 50% f T > MIC was associated with theefficacy of cephalosporins against both ESBL-producing Entero-bacteriaceae and non-ESBL producers [62,63]. Neutropenicmouse models have shown that bacteriostasis is achieved at
Table 5. In vitro activity of ceftazidime–avibactam and ceftazidime against Pseudomonas aeruginosa clinicalisolates collected from patients in US hospitals.
Organism UTI IAI
Ceftazidime–avibactam Ceftazidime Ceftazidime–avibactam Ceftazidime
n MIC90† %S‡ MIC90
† %S§ n MIC90† %S‡ MIC90
† %S§
Pseudomonas aeruginosa 155 4 98.7 16 89.7 82 4 96.3 32 85.4
Ceftazidime-NS
P. aeruginosa (MIC ‡16 mg/l)
16 8 NA >32 0 12 16 NA >32 0
Meropenem-NS
P. aeruginosa (MIC ‡4 mg/l)
33 8 NA >32 75.8 13 16 NA >32 53.8
† MIC values were measured in mg/L.‡ Based on a proposed susceptibility breakpoint of £ 8 mg/L (FDA susceptibility interpretative criteria for ceftazidime-avibactam is £8/4 mg/L) [16].§ The susceptibility rate for ceftazidime was determined by the Clinical Laboratory Standards Institute (CSLI) breakpoints [71].NA: Not available.
Table 6. Summary of ceftazidime–avibactam in vivo efficacy against extended-spectrum b-lactamase-producing Enterobacteriaceae in animal models of infection.
Author (year) Enzyme and bacterial spp. Findings Ref.
Borgonovi
(2007)
Class A ESBL and/or AmpC in
Enterobacteriaceae spp.
Ceftazidime–avibactam reduced bacterial kidney burden in
immunodepressed male CD1 mice by 2.6 log10 to 4.5, compared with
ceftazidime alone (p < 0.05)
[46]
Endimiani et al.(2011)
KPC-producing Klebsiellapneumoniae
Ceftazidime–avibactam reduced bacterial load in murine infection models
by >2-log CFU, compared with no decrease for ceftazidime alone
[47]
Levasseur et al.
(2014)
SHV-, TEM- or AmpC-producing
Enterobacteriaceae spp.
Ceftazidime–avibactam reduced unit dose ED50 in murine septicemia model
to <5–65 mg/kg from >90 mg/kg with ceftazidime alone
[48]
ESBL: Extended-spectrum b-lactamase.
Drug Profile Mawal, Critchley, Riccobene & Talley
6 Expert Rev. Clin. Pharmacol.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
02:
50 2
3 O
ctob
er 2
015

about 30% f T > MIC with ceftazidime for Enterobacteriaceaeand at 40% f T > MIC for P. aeruginosa [56,64]. In patientswith nosocomial pneumonia, a %f T > MIC ‡45% was associ-ated with favorable clinical and microbiological outcomes [58]
and a ceftazidime f T > MIC >53% was associated with favor-able microbiological outcomes in patients with ventilator-associated bacterial pneumonia [65]. Taken together, these datasuggested that 40–50% f T > MIC was an appropriate targetfor ceftazidime in analyses of probability of PK/PD targetattainment (PTA).
Avibactam target in combination with ceftazidime for
Enterobacteriaceae
The PK/PD target for avibactam was defined in a series ofexperiments using the hollow fiber infection model with eightceftazidime-resistant Enterobacteriaceae strains producingdifferent b-lactamases (AmpC, CTX-M-15, SHV-5, SHV-1,TEM-1, TEM-10, KPC-3) with high ceftazidime MICs(‡64 mg/l) and a range of ceftazidime–avibactam MICs(£0.125–4 mg/l) [60]. Continuous infusion of ceftazidime (8 or16 mg/l) in combination with avibactam concentrations thatwere varied to simulate single-dose human PK profiles causedrapid killing of ceftazidime-resistant Enterobacteriaceae fol-lowed by regrowth between 12 and 24 h [60]. The concentra-tion of avibactam at 12 h ranged from 0.15 to 0.28 mg/l, andwas therefore considered the CT to suppress bacterial growth.Further experiments showed that continuous infusion of avibac-tam at 0.25–0.5 mg/l over 4.5 h in the presence of ceftazidime2000 mg every 8 h suppressed regrowth for 12–24 h.
These data suggested that an avibactam concentration ofbetween 0.25 and 0.5 mg/l at the mid-point of an 8 h dosinginterval would be required for growth suppression. Hence,a CT of 0.5 mg/l would be appropriate for estimating thePK/PD target attainment for avibactam when combined withceftazidime against Enterobacteriaceae.
A single simulated clinical dose of ceftazidime–avibactam(2000 mg ceftazidime and 500 mg avibactam) tested in thehollow fiber system was rapidly cidal against all eightceftazidime-resistant Enterobacteriaceae strains, and growth ofall organisms was held below the limit of detection (<102
CFU/ml) for the entire 8 h period of the experiment [60].
Avibactam target in combination with ceftazidime for
P. aeruginosa
The ceftazidime–avibactam PK/PD target against P. aeruginosawas established in neutropenic mouse thigh infection and lunginfection models using seven well-characterized P. aeruginosastrains from clinical sources that were ceftazidime resistant(MIC 32–128 mg/l) and exhibited ceftazidime–avibactamMICs ranging from 2 to 16 mg/l [52,59].
Dose fractionation studies with both the thigh and lunginfection models demonstrated that the PK/PD index best asso-ciated with efficacy was %f T > CT for a CT of 1 mg/l. In thelung infection model, the effect of avibactam was decreasedwith a reduction in dose frequency, further substantiating that
the PK/PD target for avibactam is time dependent [52]. Themean %f T > CT value for a CT of 1 mg/l associated with sta-sis was 20%, for 1-log kill was 24% and for 2-log kill was30.3%. In the thigh infection model, the mean %f T > CT fora CT of 1 mg/l avibactam was 40.2% for bacterial stasis and50.3% for 1-log kill.
These data supported an appropriate target of 40–50%f T > CT for a CT of 1 mg/l for estimating avibactam PK/PDtarget attainment against P. aeruginosa. The similar magnitudeof the target %f T > MIC for ceftazidime and %f T > CT foravibactam suggested that concentrations of the inhibitor wouldexceed the CT for about the same period of time that concen-trations of the b-lactam are above the MIC.
Animal models using human-simulated PK
A series of studies have evaluated free drug concentration–timeprofiles in animals which approximated those in humans given2000 mg ceftazidime every 8 h (2-h infusion), with or withoutavibactam at 500 mg every 8 h (2-h infusion) [49,50].
A murine thigh infection model evaluating ceftazidime–avibactam against 27 isolates of P. aeruginosa (ceftazidimeMICs 8–128 mg/l and ceftazidime–avibactam MICs 4–32mg/l) compared ceftazidime–avibactam with ceftazidime aloneadministered 2 h post-infection [49]. The change in bacterialburden in the thigh was determined after 24 h and comparedwith 0 h controls. Bacterial killing (0.7–>3-log reductions inbacterial counts) occurred against 16/17 isolates with ceftazi-dime–avibactam MICs of £8 mg/l and 5/8 isolates with ceftazi-dime–avibactam MICs of 16 mg/l. After the 24-h treatmentperiod, no bacterial colonies were observed from thigh homoge-nates plated on drug-containing plates, suggesting no resistancedevelopment to ceftazidime–avibactam.
In a second study by the same investigators, simulatedhuman exposures of ceftazidime–avibactam resulted in decreasesin CFU against 13/14 Enterobacteriaceae isolates with ceftazi-dime–avibactam MICs >8 mg/l [50]. The remaining isolate, anEn. cloacae strain with a ceftazidime MIC >128 mg/l and cefta-zidime–avibactam MIC of 8 mg/l, showed a static response toceftazidime–avibactam. Variable activity was noted at ceftazi-dime–avibactam MICs of 32 mg/l, and efficacy (which wasunexpected given 0% f T > MIC) was observed against isolateswith ceftazidime–avibactam MIC values ‡128 mg/l.
PK & metabolismThe Cmax and area under the curve of ceftazidime increasedirectly with dose [15], and avibactam demonstrated approxi-mately linear PK across the dose range studied (50–2000 mg)for single intravenous (iv.) administration [66]. The PK parame-ters of ceftazidime and avibactam given in combination as asingle 2-h infusion and as multiple 2-h infusions every 8 h for11 days are shown in TABLE 7 [16,66]. There was no appreciableaccumulation of ceftazidime (2000 mg) or avibactam (500 mg)following multiple iv. infusions every 8 h for up to 11 days inhealthy adults with normal renal function [66,67]. The distribu-tion of both ceftazidime (mean volume of distribution at steady
Ceftazidime–avibactam for cUTI & cIAI Drug Profile
7www.tandfonline.com
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
02:
50 2
3 O
ctob
er 2
015

state [Vss] ranged from 17.0 to 28.2 l in the ceftazidime–avi-bactam Phase I studies) [61] and avibactam (range of mean Vss:15.2–24.4 l) [66] in healthy subjects approximated the extracel-lular fluid volume. The PK properties of ceftazidime and avi-bactam were not affected when the two drugs were co-administered compared with when they were administeredalone, either after single or repeat dosing [66]. Binding of avi-bactam (5.7–8.2%) and ceftazidime (5–23%) to human plasmaproteins was low and independent of the concentration [61]. Noclinically significant differences were seen in the PK of avibac-tam based on age or sex; therefore, no dosage adjustment basedon age or sex is necessary [68].
Avibactam and ceftazidime are both primarily cleared by thekidneys and their clearance is reduced in renally impairedpatients [66,69,70]. Hence, dosage adjustment of ceftazidime–avibactam is required in patients with creatinine clearance<50 ml/min [16].
No drug–drug interactions were observed in healthy subjectsgiven metronidazole as a 1-h infusion every 8 h, followed 1 hlater by a 2-h infusion of ceftazidime–avibactam every 8 h,demonstrating that ceftazidime–avibactam may be administeredwith metronidazole to provide coverage for anaerobic pathogensin cIAI [71].
Population PK & PK/PD target attainment simulations
PK data from Phase I and II studies were used to developpopulation PK models for avibactam and ceftazidime [72]. ThePK of both drugs were well-described by a two-compartmentmodel with first-order elimination from the central compart-ment. The primary predictors of variability in ceftazidime andavibactam PK were identified to be creatinine clearance(CrCL), subject status (cIAI or cUTI patients vs healthy sub-jects) and body weight.
The population PK models for ceftazidime and avibac-tam were used to conduct simulations across six different
levels of renal function [61,73]. The renal function groupsranged from normal (CrCL >80 ml/min) to end-stage renaldisease (CrCL £5 ml/min), and the dose regimens simu-lated were based on the dose adjustments by renal functionfor ceftazidime, with the avibactam dose adjusted to main-tain the ceftazidime–avibactam ratio at 4:1 [61]. A cIAIpopulation was used to simulate exposures and calculatethe PTA, as cIAI patients showed lower ceftazidime–avibac-tam exposures than cUTI patients or healthy individuals.PTA was calculated as the percentage of simulated subjectswho met the PK/PD dose targets for both ceftazidime andavibactam (joint PTA). The most stringent joint target wasdefined as 50% f T > MIC for ceftazidime (using the cef-tazidime–avibactam MIC) and 50% f T >1.0 mg/l for avi-bactam. The percent free fraction used to calculate freedrug concentrations was 85% for ceftazidime and 92% foravibactam [61].
The PK/PD target attainment results supported a breakpointof 8/4 mg/l for the dose regimen of 2000 mg ceftazidime com-bined with 500 mg avibactam given as a 2-h iv. infusion every8 h for subjects with normal renal function or mild renalimpairment.
Clinical studiesPhase II studies
Two Phase II, randomized, comparative clinical studies havebeen conducted with ceftazidime–avibactam, one in patientswith cUTI and the other one in cIAI [44,45]. Both studies wereinitial assessments of the efficacy and safety of ceftazidime–avibactam compared with a carbapenem and were not designedto demonstrate statistical noninferiority.
The cUTI study was a multicenter, randomized, investigator-blinded study that enrolled 137 patients with serious cUTIsincluding acute pyelonephritis. Patients were randomized 1:1 toreceive either ceftazidime–avibactam or imipenem–cilastatin [44].
Table 7. Pharmacokinetic parameters of ceftazidime–avibactam in healthy adult males.
Parameter Ceftazidime geometric mean (%CV) Avibactam geometric mean (%CV)
Ceftazidime–avibactam†
single doseCeftazidime–avibactam†
multiple dose‡Ceftazidime–avibactam†
single doseCeftazidime–avibactam†
multiple dose‡
(n = 16) (n = 16) (n = 16) (n = 16)
Cmax (mg/l) 88.1 (14) 90.4 (16) 15.2 (14) 14.6 (17)
AUC§ (mg.h/l) 289 (15)¶ 291 (15) 42.1 (16)# 38.2 (19)
T½ (h) 3.27 (33)¶ 2.76 (7) 2.22 (31)# 2.71 (25)
CL (l/h) 6.93 (15)¶ 6.86 (15) 11.9 (16)# 13.1 (19)
Vss (l) 18.1 (20)¶ 17 (16) 23.2 (23)# 22.2 (18)
†2000 mg ceftazidime + 500 mg avibactam administered as a 2-h infusion.‡Every 8 h for 11 days.§AUC0–inf reported for single dose infusion, AUC0–tau reported for multiple dose infusions.¶n = 15.#n = 13.AUC0–inf: Area under concentration–time curve from time 0 to infinity; AUC0-tau: Area under concentration–time curve over dosing interval; CL: Plasma clearance;Cmax: Maximum observed concentration; %CV: %Coefficient of variance; T½: Terminal elimination half-life; Vss: Volume of distribution at a steady state.Data from [16].
Drug Profile Mawal, Critchley, Riccobene & Talley
8 Expert Rev. Clin. Pharmacol.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
02:
50 2
3 O
ctob
er 2
015

The primary efficacy endpoint wasmicrobiological outcome at the test-of-cure (TOC) visit, 5–9 days after the endof study therapy, in the microbiologicallyevaluable (ME) population [44]. Themicrobiological response at TOC wasalso assessed in the microbiological modi-fied intent-to-treat population (mMITT).
Dose selections of ceftazidime–avibac-tam and imipenem–cilastatin were basedon the US labeled doses of these antibiot-ics for the treatment of UTI at the timethe study was conducted [15,74]. Ceftazi-dime–avibactam 625 mg (500 mg ceftazi-dime/125 mg avibactam) wasadministered as a 30-min iv. infusionevery 8 h [44]. This was increased in thesubsequent Phase III cUTI clinical trialto 2500 mg (2000 mg ceftazidime/500 mg avibactam) every 8 h, adminis-tered iv. as a 2-h infusion, based on PK/PD target attainment analysis, and is thedose approved by the FDA [16]. Imipe-nem–cilastatin was given at a dose of500 mg iv. over 30 min every 6 h. After4 days of iv. treatment, patients whoshowed clinical improvement could be switched to oral therapy(ciprofloxacin 500 mg twice daily) to receive a total treatmentcourse (iv. plus oral therapy) of 7–14 days [44].
One hundred and thirty-five patients received at least onedose study therapy with either ceftazidime–avibactam (n = 68)or imipenem–cilastatin (n = 67). Patient demographics andbaseline characteristics were generally balanced across the treat-ment groups for all analysis populations [44,61]. A favorablemicrobiological response at TOC was achieved by a similarproportion of patients in the ceftazidime–avibactam and imipe-nem–cilastatin treatment groups in both the ME [44] andmMITT populations (TABLE 8) [61]. In a subgroup analysis of themMITT population by baseline uropathogen, favorable micro-biological response rates in patients infected with the mostcommon pathogen, E. coli, were 72% for ceftazidime–avibac-tam and 62% for imipenem–cilastatin (TABLE 8) [61]. No patientswith a cUTI caused by P. aeruginosa showed a favorable micro-biological response; however, it is notable the dosage regimensin both treatment groups (ceftazidime–avibactam 625 mg iv.every 8 h; imipenem 500 mg iv. every 6 h) were lower thanthe labeled dose for ceftazidime–avibactam (2500 mg every8 h) [16] and for imipenem–cilastatin for moderate to severeinfections due to P. aeruginosa (1000 mg every 6 h or 8 h) [74].Over a third of patients in the mMITT population had infec-tions due to ceftazidime-NS Gram-negative pathogens, definedfor all Phase II and Phase III clinical studies as isolateswhose susceptibility results are classified as ‘intermediate’ or‘resistant’ to ceftazidime using Clinical and Laboratory Stand-ards Institute methodology (Enterobacteriaceae ceftazidime
MIC ‡8 mg/l and P. aeruginosa ceftazidime MIC ‡16 mg/l)[61,75]. Favorable microbiological response rates for this sub-group were 64% with ceftazidime–avibactam and 56% withimipenem–cilastatin.
The cIAI study was a multinational, randomized, double-blind study comparing ceftazidime–avibactam 2500 mg iv.every 8 h as a 30-min infusion (plus metronidazole 500 mg iv.every 8 h for coverage against anaerobic pathogens) with mero-penem 1000 mg iv. every 8 h in adult patients with qualifyingdisease characteristics of cIAI. Treatment was administered fora minimum of 5 days and a maximum of 14 days [45]. The pri-mary efficacy endpoint was clinical response at the TOC visit,2 weeks after the end of study therapy, in the ME population.The clinical response at TOC was also assessed for the mMITTpopulation.
A total of 203 patients received at least one dose of studytherapy with either ceftazidime–avibactam plus metronidazole(n = 101) or meropenem (n = 102). Demographic data andbaseline disease characteristics were generally similar across bothtreatment groups for all study populations [45]. Favorable clini-cal response at TOC was similar between the ceftazidime–avibactam group and the meropenem group in both the MEpopulation [45] and the mMITT population (TABLE 9) [61].
The most predominant pathogen was E. coli, and 82% ofpatients given ceftazidime–avibactam showed a clinical curecompared with 89% of patients given meropenem [61]. Theclinical cure rate of infections caused by P. aeruginosa was100% in both groups. Of note, 30% of patients in themMITT population had cIAI due to a ceftazidime-NS
Table 8. Favorable microbiological outcome (eradication) at test ofcure in patients with complicated urinary tract infection.
Ceftazidime–avibactam,n/N (%)
Imipenem–cilastatin,n/N (%)
Treatmentdifference (CI)†
Overall
ME population‡
mMITT population§
19/27 (70.4)
31/46 (67.4)
25/35 (71.4)
31/49 (63.3)
�1.1 (95%
CI: �27.2, 25.0)
4.1 (95%
CI: �17.1, 25.4)
By baseline pathogen (mMITT population)§,¶
Enterobacteriaceae 31/43 (72.1) 31/47 (66.0)
Escherichia coli 31/43 (72.1) 26/42 (61.9)
Pseudomonas aeruginosa 0/3 (0.0) 0/2 (0.0)
Ceftazidime-NS pathogens§,# 9/14 (64.3) 10/18 (55.6) 8.7 (90% CI:
�20.2, 35.7)
†Ceftazidime–avibactam – imipenem–cilastatin, nonstratified Miettinen–Nurminen method.‡Data from [44].§Data from [61].¶Data presented for pathogens with ‡2 isolates in either treatment group.#Includes ceftazidime-resistant or ceftazidime-intermediate baseline pathogens. Susceptibility designationsdetermined according to CLSI, 2013 [75].ME: Microbiologically evaluable (patients with a clinical and microbiological assessment at test of cure receiv-ing ‡7 days of study treatment or classified as failures after completing at least 48 h of study treatment, withno major protocol violations); mMITT: Microbiological modified intent-to-treat population (patients with‡1 baseline uropathogen, receiving ‡1 one dose of the study drug); NS: Nonsusceptible.
Ceftazidime–avibactam for cUTI & cIAI Drug Profile
9www.tandfonline.com
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
02:
50 2
3 O
ctob
er 2
015

pathogen (defined above). In this important subgroup, a clini-cal cure rate of 90% was obtained with ceftazidime–avibactamand 83% was obtained with meropenem [61].
In the Phase II cUTI and cIAI studies, ceftazidime–avibac-tam appeared effective in the treatment of cUTI and cIAI, withmicrobiological and clinical response rates comparable with thecarbapenem comparators. Importantly, ceftazidime–avibactamappeared to be effective in the treatment of infections causedby ceftazidime-NS Gram-negative bacteria in both studies.
Phase III studies
Two ceftazidime–avibactam Phase III studies have been com-pleted and results made available. One, the RECLAIM study,was initiated as two separate studies evaluating ceftazidime–avi-bactam plus metronidazole compared with meropenem inpatients with cIAI (RECLAIM-1 and -2) and were combinedto form a single global Phase III study database followingagreement with both US and European regulatory agencies [76].The clinical efficacy of ceftazidime–avibactam compared withbest available therapy (BAT) was also assessed in the Phase IIIREPRISE resistant pathogen study, which enrolled patientswith cIAI or cUTI caused by ceftazidime-resistant patho-gens [77]. Both Phase III studies evaluated the labeled dose regi-men for ceftazidime–avibactam (2500 mg iv. every 8 h over a2-h infusion, with the addition of metronidazole in patientswith cIAI).
The primary endpoint of the RECLAIM study was clinicalcure rate at the TOC visit, 28–35 days after randomization.Noninferiority between treatments was defined as the differ-ence in the clinical cure rates between treatment groups
having a 95% CI lower limit of greater than �10% forthe mMITT population [76]. Recently reported data from theRECLAIM study showed overall clinical cure rates in themMITT population of 82% (337/413) for ceftazidime–avibactam and 85% (349/410) for meropenem (treatmentdifference �3.5%; 95% CI: �8.6 to 1.6%), demonstratingnoninferiority between treatments. Among the patientsincluded in the mMITT population with cIAIs caused byceftazidime-NS pathogens, there were similar clinical curerates in the ceftazidime–avibactam group (83% [39/47]) andthe meropenem group (86% [55/64]) (treatment difference�3.0%; 95% CI: �17.9, 10.6) [76].
In a subgroup of patients with moderate renal impairmentat baseline (CrCL 30–50 ml/min), clinical cure rates werelower compared with patients with normal renal function ormild renal impairment (CrCL >50 ml/min) [61]. The reduc-tion in clinical cure rates in this subgroup was more markedin patients treated with ceftazidime–avibactam (clinical curerate at TOC was 45% [14/31]) compared with meropenem-treated patients (74% [26/35]). This difference may havebeen due to a rapid improvement in CrCL after enrollmentinto the study, without a corresponding rapid correction indosing. Within this subgroup, patients treated with ceftazi-dime–avibactam received a daily dose that was 33% lowerthan is currently recommended in the approved prescribinginformation for patients with CrCL of 30–50 ml/min [16,61].This underlines the importance of daily monitoring of CrCLin patients with changing renal function who are receivingceftazidime–avibactam, and adjusting the dose wherenecessary [16].
Table 9. Favorable clinical response at test of cure in patients with complicated intra-abdominal infectionscaused by Gram-negative aerobes.
Ceftazidime–avibactam plusmetronidazole, n/N (%)
Meropenem,n/N (%)
Treatment difference (CI)†
Overall
ME population‡
mMITT population§62/68 (91.2)
70/85 (82.4)
71/76 (93.4)
79/89 (88.8)
�2.2% (95% CI: �20.4%, 12.2%)
�6.4 (95% CI: �17.3, 4.2)
By baseline pathogen (mMITT population)§,#
Enterobacteriaceae 57/70 (81.4) 64/74 (86.5)
Escherichia coli 49/60 (81.7) 55/62 (88.7)
Klebsiella pneumoniae 6/8 (75.0) 11/13 (84.6)
Enterobacter cloacae 1/1 (100) 4/5 (80.0)
Pseudomonas aeruginosa 6/6 (100) 5/5 (100)
Ceftazidime-NS pathogens§,¶ 27/30 (90.0) 19/23 (82.6) 7.4 (90% CI: �8.5, 25.3)
†Ceftazidime–avibactam – meropenem, nonstratified Miettinen–Nurminen method.‡Data from [45].§Data from [61].#All pathogens with >2 isolates in either treatment group.¶Includes ceftazidime-resistant or ceftazidime-intermediate baseline pathogens. Susceptibility designations determined according to CLSI, 2013 [75].ME: Microbiologically evaluable (patients with qualifying complicated intra-abdominal infection, ‡1 susceptible baseline pathogen who received an adequate course oftherapy and were evaluable at test of cure); mMITT: Microbiological modified intent-to-treat population (patients with qualifying complicated intra-abdominal infectionreceiving ‡1 one dose of the study drug and ‡1 baseline pathogen regardless of susceptibility); NS: Nonsusceptible.
Drug Profile Mawal, Critchley, Riccobene & Talley
10 Expert Rev. Clin. Pharmacol.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
02:
50 2
3 O
ctob
er 2
015

The REPRISE Phase III study was a prospective, open-labelstudy in patients with cIAI or cUTI caused by ceftazidime-resistant Gram-negative pathogens, defined similarly as forceftazidime-NS above [77]. Interim data from 126 patientshave been reported, of whom 64 received ceftazidime–avibac-tam (cUTI, n = 58; cIAI, n = 6) and 62 received acarbapenem-based regimen (BAT) (cUTI, n = 56; cIAI,n = 6). The primary endpoint was clinical cure at TOC inthe mMITT population, which was similar with ceftazidime–avibactam (93% [55/59]) and BAT (90% [47/52]). Inpatients with cUTI, per-patient microbiological response rateswere higher with ceftazidime–avibactam (78% [43/55]) thanwith BAT (50% [24/48]).
The majority of available clinical Phase III data is frompatients with cIAI, and confirms ceftazidime–avibactam to bean effective treatment in infections caused by Enterobacteria-ceae or P. aeruginosa, including those with ceftazidime-resistant phenotypes, which is consistent with the Phase IIcIAI study. Results are awaited from a recently completedPhase III cIAI study in Asia (RECLAIM 3, clinicaltrials.govidentifier NCT01726023), a Phase III cUTI study (RECAP-TURE 1, NCT01595438 and RECAPTURE 2,NCT01599806 combined into a single study database) and aPhase III study in hospital-acquired bacterial pneumonia(including ventilator-associated bacterial pneumonia)(REPROVE, NCT01808092).
Safety & tolerabilityAs a chemical class, the cephalosporins, including ceftazidime,have a well-established safety profile and are generally consid-ered to be well-tolerated during many years of use, with a lowincidence of reported AEs [15]. The safety of avibactam aloneand in combination with ceftazidime has been evaluated inhealthy volunteers in Phase I studies, including one studywhich showed that supratherapeutic doses of ceftazidime–avi-bactam were not associated with QT/QTc prolongation [78].Ceftazidime–avibactam was generally well-tolerated in thePhase II cUTI and cIAI studies [44,45]. The most commonadverse reactions to ceftazidime–avibactam in Phase II studies(incidence of ‡10% in either indication) were vomiting,nausea, constipation and anxiety [16].
In the Phase II cUTI study, 68% (46/68) patients in theceftazidime–avibactam group and 76% (51/67) patients in thecomparator group experienced AEs [44]. The most commonevents in both treatment groups were headache and injection/infusion site reactions. Gastrointestinal events were also com-mon in both treatment groups; constipation and abdominalpain were more common in the ceftazidime–avibactam group(10 and 15%, respectively) than in the comparator group(3 and 6%, respectively). During antibiotic treatment, drug-related treatment-emergent AEs were reported in 35% (24/68)and 51% (34/67) of patients who received ceftazidime–avibactam or imipenem–cilastatin, respectively. Three serioustreatment-emergent AEs that were drug related were reportedin the ceftazidime–avibactam group (renal failure, diarrhea and
an accidental overdose of ceftazidime–avibactam due to misad-ministration of study drug – this serious treatment-emergentAE was not associated with any other AE), and one patient inthe imipenem–cilastatin group experienced a serious AE (SAE)of an increase in serum creatinine, which was considered to beprobably drug related.
In the cIAI Phase II study, AEs were observed in 64%(65/101) patients treated with ceftazidime–avibactam plusmetronidazole and 58% (59/102) patients treated with mero-penem [45]. Overall, the types of events reported were compa-rable between the two treatment groups, although nausea(10%), vomiting (14%) and abdominal pain (8%) were morecommon in the ceftazidime–avibactam plus metronidazolegroup than in the meropenem group (6, 5 and 3%, respec-tively). Elevated liver enzymes were more common among thepatients who received meropenem (increased alanine amino-transferase, 13%; increased aspartate aminotransferase, 15%)than among those who received ceftazidime–avibactam (ala-nine aminotransferase, 8%; aspartate aminotransferase, 9%).In the ceftazidime–avibactam group, SAEs were reported in9% (9/101) of patients (one of these, elevated liver enzymes,was considered to be study drug related), compared with11% (11/102) of patients in the meropenem group, none ofwhich were related to the study drug. There were five deathsin the study (three in the ceftazidime–avibactam group andtwo in the meropenem group), and these were not consideredto be related to study treatment.
Overall AE rates observed in the Phase III RECLAIM studywere 46% in the ceftazidime–avibactam plus metronidazolegroup (n = 532) and 43% in the meropenem group (n = 534)[76]. Rates of SAEs were 8% in both groups, and the mostfrequently reported AEs with ceftazidime–avibactam plus met-ronidazole were diarrhea, nausea, vomiting and fever. Deathoccurred in 2.5% (13/529) of patients who received ceftazi-dime–avibactam and 1.5% (8/529) of patients who receivedmeropenem [16]. These data were made available for regulatoryreview during the ceftazidime–avibactam approval process, inadvance of publication of Phase III safety data [61].
In a subgroup of patients with moderate renal impairment atbaseline (CrCL 30–50 ml/min), death occurred in 26% (8/31)of patients in the ceftazidime–avibactam and 9% (3/35) ofpatients in the meropenem group [16]. None of these deathswere considered to be study drug related. The majority of thesepatients were in the mMITT population, and their outcomeswere classified as clinical failure or indeterminate at the TOCvisit (6/8 in the ceftazidime–avibactam group and 2/3 in themeropenem group) [61]. Death was attributed to various causesincluding progression of underlying infection, delayed surgicalintervention and lack of efficacy of the study drug against base-line pathogens [61]. Among patients with normal renal functionor mild impairment, there was no difference between treat-ments in the number of deaths (1% [n = 5] patients in eachgroup).
Interim data from the Phase III REPRISE study have shownthat 28% (18/64) of patients in the ceftazidime–avibactam
Ceftazidime–avibactam for cUTI & cIAI Drug Profile
11www.tandfonline.com
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
02:
50 2
3 O
ctob
er 2
015

group and 50% (31/62) of patients in the BAT group experi-enced an AE, and the SAE rates were 4.7 and 6.5%, respec-tively [77]. The most frequently reported AEs in both groupswere gastrointestinal disorders. Safety data for patients withmoderate renal impairment at baseline enrolled in this studyare expected to be reported elsewhere.
The AEs observed in the completed and reported ceftazi-dime–avibactam Phase III studies were consistent with the AEprofile seen with ceftazidime–avibactam in Phase II studies.Together, these data show that ceftazidime–avibactam possessesan AE profile that is comparable with ceftazidime alone and/ormetronidazole (cIAI) and, likewise, is consistent with the AEprofile of the cephalosporin class.
Expert commentaryThird-generation cephalosporins have had an important role inthe treatment of cUTI and cIAI; however, the rising prevalenceof b-lactamase–producing strains is limiting their effectiveness.Carbapenems are increasingly favored as the first-line therapyfor these serious infections, but the emergence ofcarbapenemase-producing bacteria also threatens their utility.Therefore, new treatment options for cUTI and cIAI areurgently needed. Ceftazidime–avibactam, a combination of anestablished third-generation cephalosporin and a novelb-lactamase inhibitor, has the potential to meet this need byproviding a new effective treatment option for certain MDRGram-negative bacteria causing these infections.
Data generated by PK/PD studies, animal infection models,Phase I/II clinical studies for ceftazidime–avibactam, and previ-ous findings on the efficacy and safety of ceftazidime alonesupported FDA approval of ceftazidime–avibactam for thetreatment of cIAI and cUTI in advance of completion ofPhase III studies. As the clinical data supporting approval wereprimarily from Phase II studies and interim Phase III data, theuse of ceftazidime–avibactam is currently reserved for patientswith limited or no other treatment options [16].
Ceftazidime and avibactam have complementary PK profilesand no drug–drug interactions, making their co-administrationpracticable. Both agents have predictable PK and are primarilyexcreted unchanged by the renal route; therefore, dosage adjust-ment is necessary in patients with moderately or more severelyimpaired renal function [16]. Avibactam has a broad spectrumof inhibitory activity against b-lactamases, covering Amblerclass A enzymes, including KPCs and CTX-M ESBLs, class Cb-lactamases including AmpC and some class D enzymes (e.g.,OXA-48), which represents a significant advance on currentlyavailable b-lactamase inhibitors. In combination with ceftazi-dime, avibactam restored the in vitro activity of ceftazidimeagainst b-lactamase–producing Enterobacteriaceae and P. aeru-ginosa, common causative pathogens in cUTI and cIAI infec-tions. A PK/PD target attainment analysis based on data fromPhase I and Phase II studies in humans, in vitro studies andin vivo animal models of infection supported an in vitro sus-ceptibility breakpoint MIC value of £8/4 mg/l for ceftazidime–avibactam against Enterobacteriaceae and P. aeruginosa. The
PK/PD analysis supports a dosage regimen of ceftazidime–avi-bactam 2000 mg–500 mg by 2-h iv. infusion every 8 h for usein cUTI and cIAI [16].
In the Phase II studies in cUTI and cIAI, ceftazidime–avibactam demonstrated overall clinical and microbiologicalresponse rates that were similar to the carbapenem compara-tors. It is notable that the dose of ceftazidime–avibactam inthe cUTI study was one-quarter of the approved dose [16,44]
and, similarly, the dose of imipenem was also lower than thelabeled dose for moderate to severe infections due to P. aeru-ginosa or pathogens with decreased susceptibility. It is likelythat this accounts for the lack of clinical response observedfor both treatment groups in the limited number of infectionsdue to P. aeruginosa in the Phase II cUTI study. Based onPK/PD target attainment analyses, the dose of ceftazidime–avibactam was increased in the Phase III cUTI study to thecurrently labeled dose of 2000 mg–500 mg (2-h infusion)every 8 h [16]. The clinical cure rate against P. aeruginosa inthe Phase II cIAI study, which used the currently approveddose of ceftazidime–avibactam (2000 mg–500 mg every 8 h)[16], was 100% [45,61]. Importantly, ceftazidime–avibactam alsodemonstrated high microbiological success rates againstceftazidime-NS pathogens in both Phase II clinical studies.The approved dose of ceftazidime–avibactam was given topatients enrolled in the Phase III studies, and its clinical effec-tiveness has been confirmed by the Phase III studies forwhich the results are available, which included infectionscaused by ceftazidime-NS pathogens.
Ceftazidime–avibactam was well-tolerated in Phase I, II andIII studies, with a safety profile reflective of the cephalosporinclass. Ceftazidime–avibactam provides clinicians with a muchneeded new treatment option for patients with cUTI or cIAI,with limited or no treatment options, particularly in thoseinfections due to ESBL- and KPC-producing bacteria orceftazidime-NS P. aeruginosa.
Five-year viewTreatment guidelines are increasingly taking into account theissues surrounding emerging antibiotic resistance [2,7,79], withrecommendations to reduce the risk of new antibiotic-resistantstrains through measures such as appropriate prescribing. Thisaims to address the association between antibiotic usage,including carbapenems, and the increasing frequency of CREsfound in Enterobacteriaceae [80]. Antimicrobial stewardship andregional intervention strategies can slow the rate of spread ofCREs; however, the marked rise of ESBL- or carbapenemase-expressing Enterobacteriaceae and MDR P. aeruginosa over thelast 5–10 years is expected to continue [81]. Novel antimicro-bials are required to provide additional treatment options notjust in the short term, but also over the medium and longterm, as only a continued focus on developing innovative treat-ment strategies is likely to meet the challenge of controllingMDR pathogens.
Combining a b-lactam with a b-lactamase inhibitor is aproven strategy for responding to the threat posed by the
Drug Profile Mawal, Critchley, Riccobene & Talley
12 Expert Rev. Clin. Pharmacol.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
02:
50 2
3 O
ctob
er 2
015

emergence of resistant strains, and combining ceftazidime withavibactam in a 4:1 ratio restores the activity of ceftazidimeagainst ESBL-producing Gram-negative pathogens [15,16].
The novel cephalosporin ceftolozane (CXA-201) in combina-tion with an established b-lactamase inhibitor, tazobactam, hasrecently been approved by the FDA for patients with cIAIs(with metronidazole) and cUTIs that are proven or stronglysuspected to be caused by susceptible bacteria (ZERBAXA�;Cubist Pharmaceuticals U.S., Lexington, MA, USA) [82]. Cefto-lozane–tazobactam has a spectrum of activity against Gram-negative pathogens such as E. coli and K. pneumoniae, includingESBL producers, and P. aeruginosa, including certain MDRand carbapenemase-producing strains. Exceptions to its spec-trum of activity include bacteria that produce serine carbapene-mases (e.g., KPCs) and metallo-b-lactamases [82].
Another b-lactamase inhibitor, MK-7655, of the same dia-zabicyclooctane class as avibactam, is currently in Phase IIclinical development. MK-7655 displays good in vitro activityagainst class A and class C carbapenemases, especially in com-bination with imipenem–cilastatin [83]. The serine b-lactamaseinhibitor RPX7009 combined with meropenem has showngood activity against Enterobacteriaceae, including KPCs, andis currently in Phase III trials in patients with cUTIs [84].Plazomicin is a novel aminoglycoside that is currently in
Phase III clinical development for patients with cUTI [85]. Ithas shown good in vitro activity against Enterobacteriaceae [86],which extends to ESBL and KPC producers. It remains to beseen whether the clinical success of these agents will be suffi-cient to support approval for the treatment of cUTI andcIAI; however, they would be welcome additions to ceftolo-zane–tazobactam and ceftazidime–avibactam in the armamen-tarium against serious infections associated with MDR Gram-negative pathogens.
Financial & competing interests disclosure
Clinical studies were funded by AstraZeneca; Cerexa, Inc., a wholly-owned
subsidiary of Forest Laboratories, LLC and Forest Laboratories, Inc. All
authors were employees of Forest Laboratories LLC. Actavis acquired Forest
Laboratories in July 2014. As a result of the acquisition, all authors are
shareholders of Allergan plc (formerly Actavis plc). AK Talley is a consul-
tant for Allergan plc (formerly Actavis plc). IA Critchley is currently
employed by Allergan plc and TA Riccobene is currently employed by
Allergan plc (formerly Actavis plc). The authors have no other relevant
affiliations or financial involvement with any organization or entity with
a financial interest or financial conflict with the subject matter or materi-
als discussed in the manuscript apart from those disclosed.
Editorial assistance for this manuscript was provided by Micron
research and was funded by Forest Laboratories LLC.
Key issues
. Infections due to drug-resistant Gram-negative pathogens are associated with significant morbidity and mortality, and extended-
spectrum b-lactamase- and carbapenemase-producing Enterobacteriaceae and multidrug-resistant Pseudomonas aeruginosa have been
designated as serious or urgent threats to public health by the US Center for Disease Control.
. Ceftazidime–avibactam is a combination of the established third-generation cephalosporin ceftazidime and the novel non–b-lactamb-lactamase inhibitor avibactam, and was recently approved by the US FDA for the treatment of complicated intra-abdominal infections
(cIAIs) and complicated urinary tract infections (cUTIs) caused by designated susceptible microorganisms. Approval of ceftazidime–avibac-
tam in advance of pivotal Phase III data was based in part on existing data for ceftazidime, along with nonclinical microbiology, pharma-
cokinetic/pharmacodynamic analyses, and clinical data supporting the safety and efficacy of ceftazidime–avibactam in patients with cIAI
and cUTI from Phase II studies. As only limited clinical data are available pending final Phase III trial results, ceftazidime–avibactam is
reserved for use in patients with limited or no other treatment options.
. Avibactam has a broader spectrum of inhibitory action than current b-lactamase inhibitors, which includes certain enzymes for which
there are a limited number of, or an absence of, other effective agents (e.g., CTX-M, KPC, AmpC, OXA-48); hence, ceftazidime–
avibactam addresses a critical unmet need for effective therapy against pathogens producing these enzymes.
. The administration of avibactam with ceftazidime does not significantly alter the pharmacokinetics of ceftazidime. Ceftazidime–
avibactam is cleared primarily via the kidneys and dose adjustment is required in patients with renal impairment (creatinine clearance
<50 ml/min).
. In clinical studies, the safety profile of ceftazidime–avibactam appears to be comparable with ceftazidime alone and is consistent with
the adverse event profile of the cephalosporin class.
. Ceftazidime–avibactam appears efficacious and well-tolerated in clinical studies of adult patients with cUTI and cIAI, including infections
caused by ceftazidime-nonsusceptible pathogens.
Ceftazidime–avibactam for cUTI & cIAI Drug Profile
13www.tandfonline.com
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
02:
50 2
3 O
ctob
er 2
015
References
Papers of special note have been highlighted as:. of interest.. of considerable interest
1. Nicolle LE; AMMI Canada Guidelines
Committee. Complicated urinary tract
infection in adults. Can J Infect Dis Med
Microbiol 2005;16:349-60
2. Solomkin JS, Mazuski JE, Bradley JS, et al.
Diagnosis and management of complicated
intra-abdominal infection in adults and
children: Guidelines by the Surgical
Infection Society and the Infectious Diseases
Society of America. Clin Infect Dis
2010;50:133-64
3. US Food and Drug Administration.
Guidance for industry: complicated urinary
tract infections: developing drugs for
treatment; Revision 1. 2012. Available from:
www.fda.gov/downloads/Drugs/Guidances/
ucm070981.pdf [Last accessed 17 March
2015]
4. Castanheira M, Farrell SE, Krause KM,
et al. Contemporary diversity of
b-lactamases among Enterobacteriaceae in
the nine U.S. census regions and
ceftazidime-avibactam activity tested against
isolates producing the most prevalent
b-lactamase groups. Antimicrob Agents
Chemother 2014a;58:833-8
5. Drawz SM, Papp-Wallace KM,
Bonomo RA. New b-lactamase inhibitors:
a therapeutic renaissance in an MDR world.
Antimicrob Agents Chemother 2014;58:
1835-46
6. Centers for Disease Control and Prevention
(CDC). Antibiotic resistant threats in the
United States. 2013. Available from: www.
cdc.gov/drugresistance/threat-report-2013/
pdf/ar-threats-2013-508.pdf [Last accessed
15 April 2015]
7. Gupta K, Bhadelia N. Management of
urinary tract infections from
multidrug-resistant organisms. Infect Dis
Clin North Am 2014;28:49-59
8. Boucher HW, Talbot GH, Bradley JS, et al.
Bad bugs, no drugs: no ESKAPE! An
update from the Infectious Diseases Society
of America. Clin Infect Dis 2009;48:1-12
9. Kanj SS, Kanafani ZA. Current concepts in
antimicrobial therapy against resistant
gram-negative organisms: extended-spectrum
beta-lactamase-producing Enterobacteriaceae,
carbapenem-resistant Enterobacteriaceae, and
multidrug-resistant Pseudomonas
aeruginosa. Mayo Clin Proc 2011;86:250-9
10. Nordmann P, Naas T, Poirel L. Global
spread of carbapenemase-producing
Enterobacteriaceae. Emerg Infect Dis
2011;17:1791-8
11. Nordmann P. Carbapenemase-producing
Enterobacteriaceae: overview of a major
public health challenge. Med Mal Infect
2014;44:51-6
12. Paul M, Carmeli Y, Durante-Mangoni E,
et al. Combination therapy for
carbapenem-resistant Gram-negative
bacteria. J Antimicrob Chemother 2014;69:
2305-9
13. Snitkin ES, Zelazny AM, Thomas PJ, et al.
Tracking a hospital outbreak of
carbapenem-resistant Klebsiella pneumoniae
with whole-genome sequencing. Sci Transl
Med 2012;4:148
14. Centers for Disease Control and Prevention
(CDC). CDC Statement: Los Angeles
County/UCLA investigation of CRE
transmission and duodenoscopes. Available
from: www.cdc.gov/hai/outbreaks/
cdcstatement-LA-CRE.html [Last accessed
14 April 2015]
15. US FDA. FORTAZ� (ceftazidime
injection) Prescribing Information 2007.
GlaxoSmithKline. Updated January. 2007.
Available from: www.accessdata.fda.gov/
drugsatfda_docs/label/2007/
050578s053,050634s020lbl.pdf [Last
accessed 17 March 2015]
16. US FDA. AVYCAZ� (ceftazidime-
avibactam) for injection. Package insert.
Forest Pharmaceuticals, Inc. Subsidiary of
Forest Laboratories. 2015. Available from:
www.avycaz.com/ [Last accessed 2 April
2014]
. Ceftazidime–avibactam US package insert.
17. Coleman K. Diazabicyclooctanes (DBOs):
a potent new class of non-b-lactamb-lactamase inhibitors. Curr Opin
Microbiol 2011;14:550-5
18. Ehmann DE, Jahic�H, Ross PL, et al.
Avibactam is a covalent, reversible,
non-b-lactam b-lactamase inhibitor. Proc
Natl Acad Sci USA 2012;109:11663-8
19. Ehmann DE, Jahic H, Ross PL, et al.
Kinetics of avibactam inhibition against class
A, C, and D beta-lactamases. J Biol Chem
2013;288:27960-71
20. Li H, Estabrook M, Jacoby GA, et al. In
vitro susceptibility of characterized
b-lactamase-producing strains tested with
avibactam concentrations. Antimicrob
Agents Chemother 2015;59(3):1789-93
21. Livermore DM, Mushtaq S, Warner M,
et al. NXL104 combinations versus
Enterobacteriaceae with CTX-M extended-
spectrum beta-lactamases and
carbapenemases. J Antimicrob Chemother
2008;62:1053-6
22. Livermore DM, Mushtaq S, Warner M,
et al. Activities of NXL104 combinations
with ceftazidime and aztreonam against
carbapenemase-producing
Enterobacteriaceae. Antimicrob Agents
Chemother 2011;55:390-4
23. Stachyra T, Levasseur P, Pe�chereau MC,
et al. In vitro activity of the b-lactamase
inhibitor NXL104 against
KPC-2 carbapenemase and
Enterobacteriaceae expressing KPC
carbapenemases. J Antimicrob Chemother
2009;64:326-9
24. Bush K. Proliferation and significance of
clinically relevant b-lactamases. Ann N Y
Acad Sci 2013;1277:84-90
25. b-lactamase classification and amino acid
sequences for TEM, SHV and
OXA extended-spectrum and inhibitor
resistant enzymes. Lahey Hospital and
Medical Center. Burlington, MA. Available
from: www.lahey.org/Studies/webt.asp#OXA
[Last accessed 12 August 2015]
26. Akova M. Sulbactam-containing b-lactamase
inhibitor combinations. Clin Microbiol
Infect 2008;(Suppl 1):185-8
27. Drawz SM, Bonomo RA. Three decades of
beta-lactamase inhibitors. Clin Microbiol
Rev 2010;23:160-201
28. Lahiri SD, Mangani S, Durand-Reville T,
et al. Structural insight into potent
broad-spectrum inhibition with reversible
recyclization mechanism: avibactam in
complex with CTX-M-15 and Pseudomonas
aeruginosa AmpC b-lactamases. Antimicrob
Agents and Chemother 2013;57:2496-505
29. Porres-Osante N, Dupont H, Torres C,
et al. Avibactam activity against
extended-spectrum AmpC-b-lactamases.
J Antimicrob Chemother 2014;69:1715-16
30. Stachyra T, Pe�chereau MC, Bruneau JM,
et al. Mechanistic studies of the inactivation
of TEM-1 and P99 by NXL104, a novel
non-beta-lactam beta-lactamase inhibitor.
Antimicrob Agents Chemother 2010;54:
5132-8
31. Aktas Z, Kayacan C, Oncul O. In vitro
activity of avibactam (NXL104) in
combination with b-lactams against
Gram-negative bacteria, including OXA-48
b-lactamase-producing Klebsiella
pneumonia. Int J Antimicrob Agents
2012;39:86-9
32. Levasseur P, Girard A, Miossec C, et al. In
vitro antibacterial activity of the
ceftazidime-avibactam combination against
Enterobacteriaceae, including strains with
Drug Profile Mawal, Critchley, Riccobene & Talley
14 Expert Rev. Clin. Pharmacol.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
02:
50 2
3 O
ctob
er 2
015

well-characterized b-lactamases. Antimicrob
Agents Chemother 2015;59:1931-4
33. Mushtaq S, Warner M, Livermore DM. In
vitro activity of ceftazidime + NXL104
against Pseudomonas aeruginosa and other
non-fermenters. J Antimicrob Chemother
2010;65:2376-81
34. Babinchak T, Badal R, Hoban D, et al.
Trends in susceptibility of selected
gram-negative bacilli isolated from intra-
abdominal infections in North America:
SMART 2005-2010. Diagn Microbiol
Infect Dis 2013;76:379-81
35. Bouchillon SK, Badal RE, Hoban DJ, et al.
Antimicrobial susceptibility of inpatient
urinary tract isolates of gram-negative bacilli
in the United States: results from the study
for monitoring antimicrobial resistance
trends (SMART) program: 2009–2011.
Clin Ther 2013;35:872-7
36. Flamm RK, Farrell DJ, Sader HS, et al.
Ceftazidime/avibactam activity tested against
Gram-negative bacteria isolated from
bloodstream, pneumonia, intra-abdominal
and urinary tract infections in US medical
centers (2012). J Antimicrob Chemother
2014;69:1589-98
37. Castanheira M, Mills JC, Costello SE, et al.
Ceftazidime-avibactam tested against
Enterobacteriaceae from United States
hospitals (2011–2013) and characterization
of b-lactamase producing strains.
Antimicrob Agents Chemother 2015;59:
3509-17
.. In vitro activity of ceftazidime–avibactam
and comparator agents against
20,709 clinical isolates of
Enterobacteriaceae, including 743 isolates
containing b-lactamases, collected from
US hospitals.
38. Lob S, Badal R, Hackel M, et al.
Susceptibility to ceftazidime-avibactam and
comparators of the ESKAPE pathogens,
Klebsiella pneumoniae and Enterobacter
spp., in the USA and Latin America in
2013 (Abstract C-767). 54th Annual
Interscience Conference on Antimicrobial
Agents and Chemotherapy (ICAAC), 2014
39. Lagace�-Wiens P, Tailor F, Simner P, et al.
Activity of NXL 104 in combination with
b-lactams against genetically characterized
Escherichia coli and Klebsiella pneumoniae
isolates producing class
A extended-spectrum b-lactamases and class
C b-lactamases. Antimicrob Agents
Chemother 2011;55:2434-7
40. Sader HS, Castanheira M, Mendes RE,
et al. Ceftazidime-avibactam activity tested
against multi-drug resistant Pseudomonas
aeruginosa isolated from United States
Medical Centers (2012–2013). Antimicrob
Agents Chemother 2015;59:3656-9
.. In vitro activity of ceftazidime–avibactam
and comparator agents against
3902 clinical isolates of Pseudomonas
aeruginosa from US hospitals.
41. Livermore DM, Jamrozy D, Warner M,
et al. In-vitro selection of Enterobacteriaceae
mutants with KPC carbapenemases resistant
to ceftazidime-avibactam. (Abstract
C-1191 poster). 54th Interscience
Conference on Antimicrobial Agents and
Chemotherapy (ICAAC), 2014
42. Lahiri SD, Walkup GK, Whiteaker JD,
et al. Selection and molecular
characterization of ceftazidime/avibactam-
resistant mutants in Pseudomonas
aeruginosa strains containing derepressed
AmpC. J Antimicrob Chemother 2015;70:
1650-8
43. Lahiri SD, Johnstone MR, Ross PL, et al.
Avibactam and class C b-lactamases:
mechanism of inhibition, conservation of
the binding pocket, and implications for
resistance. Antimicrob Agents Chemother
2014;58:5704-13
44. Vazquez JA, Gonzalez Patzan LD, et al.
Efficacy and safety of ceftazidime–avibactam
versus imipenem–cilastatin in the treatment
of complicated urinary tract infections,
including acute pyelonephritis, in
hospitalized adults: results of a prospective,
investigator-blinded, randomized study.
Curr Med Res Opin 2012;28:1921-31
.. Phase II study demonstrating the efficacy
and safety of ceftazidime–avibactam in
patients with complicated urinary tract
infections.
45. Lucasti C, Popescu I, Ramesh MK, et al.
Comparative study of the efficacy and safety
of ceftazidime/avibactam plus metronidazole
versus meropenem in the treatment of
complicated intra-abdominal infections in
hospitalized adults: results of a randomized,
double-blind, Phase II trial. J Antimicrob
Chemother 2013;68:1183-92
.. Phase II study demonstrating the efficacy
and safety of ceftazidime–avibactam in
patients with complicated
intra-abdominal infections.
46. Borgonovi M, Miosses C, Lowther J. The
efficacy of ceftazidime combined with
NXL-104, a novel b-lactamase inhibitor, in
a mouse model of kidney infections induced
by b-lactamase producing Enterobacteriaceae
(Abstract P794). 17th European Congress of
Clinical Microbiology and Infectious
Disease (ECCMID), 2007
47. Endimiani A, Hujer KM, Hujer AM, et al.
Evaluation of ceftazidime and NXL104 in
two murine models of infection due to
KPC-producing Klebsiella pneumoniae.
Antimicrob Agents Chemother 2011;55:
82-5
48. Levasseur P, Girard A-M, Lavallade L, et al.
Efficacy of a ceftazidime-avibactam
combination in a murine septicemia model
caused by Enterobacteriaceae species
producing AmpC or extended-spectrum
b-lactamases. Antimicrob Agents Chemother
2014;58:6490-5
49. Crandon JL, Schuck VJ, Banevicius MA,
et al. Comparative in vitro and in vivo
efficacies of human simulated doses of
ceftazidime and ceftazidime-avibactam
against Pseudomonas aeruginosa.
Antimicrobial Agents Chemother 2012;56:
6137-46
50. MacVane SH, Crandon JL, Nichols WW,
et al. In vivo efficacy of humanized
exposures of ceftazidime-avibactam in
comparison with ceftazidime against
contemporary Enterobacteriaceae isolates.
Antimicrob Agents Chemother 2014a;58:
6913-19
51. Merdjan H, Girard AM, Miossec C, et al.
Pharmacokinetics (PK) and efficacy of
ceftazidime (CAZ)/NXL104 combination in
murine pneumonia model caused by a
AmpC-producing Klebsiella pneumoniae
(Abstract A1-006). 49th Annual Interscience
Conference on Antimicrobial Agents and
Chemotherapy (ICAAC), 2009
52. Berkhout MJ, Melchers CH, Van Mill S,
et al. Pharmacodynamics of Ceftazidime
and Avibactam in a Neutropenic Mouse
Lung Model [abstract A-1022]. 53rd
Interscience Conference on Antimicrobial
Agents and Chemotherapy (ICAAC), 2013b
53. Housman ST, Crandin JL, Nichols WW,
et al. Efficacies of Ceftazidime-Avibactam
and Ceftazidime against Pseudomonas
aeruginosa in a murine lung infection
model. Antimicrob Agents Chemother
2014;58:1365-71
54. Cottagnoud P, Merdjan H, Acosta F, et al.
Pharmacokinetics of the new b-lactamase
inhibitor NXL104 in an experimental rabbit
meningitis model: restoration of the
bacteriological efficacy of ceftazidime (CAZ)
against a class C producing K. pneumoniae
[Abstract F1-321]. 47th Interscience
Conference on Antimicrobial Agents and
Chemotherapy (ICAAC), 2007
55. Craig WA. Interrelationship between
pharmacokinetics and pharmacodynamics in
determining dosage regimens for
Ceftazidime–avibactam for cUTI & cIAI Drug Profile
15www.tandfonline.com
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
02:
50 2
3 O
ctob
er 2
015

broad-spectrum cephalosporins. Diagn
Microbiol Infect Dis 1995;22:89-96
56. Craig WA. Basic pharmacodynamics of
antibacterials with clinical applications to
the use of b-lactams, glycopeptides, and
linezolid. Infect Dis Clin North Am
2003;17:479-501
57. Craig WA. Pharmacodynamics of
antimicrobials: general concepts and
applications. In: Nightingale CH,
Ambrose PG, Drusano GL, Murakawa T,
editors. Antimicrobial pharmacodynamics in
theory and clinical practice. 2nd edition.
Informa Healthcare; New York; 2007. p.
129-46
58. Muller AE, Punt N, Mouton JW. Optimal
exposures of ceftazidime predict the
probability of microbiological and clinical
outcome in the treatment of nosocomial
pneumonia. J Antimicrob Chemother
2013;68:900-6
59. Berkhout MJ, Melchers CH, Van Mill S,
et al. Exposure response relationships of
Ceftazidime and Avibactam in a
Neutropenic Thigh Model (Abstract
A-1023 poster). 53rd Interscience
Conference on Antimicrobial Agents and
Chemotherapy (ICAAC), 2013a
60. Coleman K, Levasseur P, Girard AM, et al.
Activities of ceftazidime and avibactam
against b-lactamase-producing
Enterobacteriaceae in a hollow-fiber
pharmacodynamic model. Antimicrob
Agents Chemother 2014;58:3366-72
61. Cerexa Inc., A Subsidiary of Actavis plc.
2014. Briefing Document and Addendum.
NDA 206494. Anti-Infective Drugs
Advisory Committee. 2014. Available from:
www.fda.gov/downloads/
AdvisoryCommittees/
CommitteesMeetingMaterials/Drugs/Anti-
InfectiveDrugsAdvisoryCommittee/
UCM425459.pdf [Last accessed 17 March
2015]
62. DeRyke C, Nicolau D. Is all free time
above the minimum inhibitory
concentration the same: implications
for-lactam in vivo modelling. Int J
Antimicrob Agents 2007;29:341-3
63. Andes D, Craig WA. Treatment of
infections with ESBL-producing organisms:
pharmacokinetic and pharmacodynamic
considerations. Clin Microbiol Infect
2005;11:10-17
64. Andes D, Craig WA. Animal model
pharmacokinetics and pharmacodynamics:
a critical review. Int J Antimicrob Agents
2002;19:261-8
65. MacVane SH, Kuti JL, Nicolau DP.
Clinical pharmacodynamics of
antipseudomonal cephalosporins in patients
with ventilator-associated pneumonia.
Antimicrob Agents Chemother 2014b;58:
1359-64
66. Merdjan H, Rangaraju M, Tarral A. Safety
and pharmacokinetics of single and multiple
ascending doses of avibactam alone and in
combination with ceftazidime in healthy
male volunteers: results of two randomized,
placebo-controlled studies. Clin Drug
Investig 2015;35:307-17
. Phase I studies of ceftazidime–avibactam.
67. Edeki T, Armstrong J, Li J.
Pharmacokinetics of avibactam (AVI) and
ceftazidime (CAZ) following separate or
combined administration in healthy
volunteers. [Abstract A-1019]. 53rd
Interscience Conference on Antimicrobial
Agents and Chemotherapy (ICAAC), 2013
68. Tarral A, Merdjan H. Effect of age and sex
on the pharmacokinetics and safety of
avibactam in healthy volunteers. Clin Ther
2015;37:877-86
69. Merdjan H, Tarral A, Haazen W, et al.
Pharmacokinetics and tolerability of NXL
104 in normal subjects and patients with
varying degrees of renal insufficiency
(Abstract P1598). 20th European Congress
of Clinical Microbiology and Infectious
Diseases (ECCMID), 2010
70. Vishwanathan K, Mair S, Gupta A, et al.
Assessment of the mass balance recovery and
metabolite profile of avibactam in humans
and in vivo drug-drug interaction potential.
Drug Metab Dispos 2014;42:932-42
71. Li J, Armstrong J, Edeki T.
Pharmacokinetic (PK) drug interaction
study of ceftazidime-avibactam (CAZ-AVI)
and metronidazole (MTZ) in healthy
volunteers (Abstract A-1020). 53rd
Interscience Conference on Antimicrobial
Agents and Chemotherapy (ICAAC), 2013
72. Carrothers TJ, Green M, Chiu J, et al.
Population pharmacokinetic modeling of
combination treatment of intravenous
ceftazidime and avibactam (Abstract T-071).
Fifth American Conference on
Pharmacometrics (ACoP5), 2014
73. Li J, Knebel W, Riggs M, et al. Population
pharmacokinetic modelling of ceftazidime
(CAZ) and avibactam (AVI) in healthy
volunteers and patients with complicated
intra-abdominal infection (cIAI) (Abstract
A-634). 52nd Interscience Conference on
Antimicrobial Agents and Chemotherapy
(ICAAC), 2012
74. US FDA. Primaxin� I.V. Imipenem and
cilastatin for injection package insert. Merck
& Co., Inc. Issued August 2009. Available
from: www.accessdata.fda.gov/
drugsatfda_docs/label/2009/
050587s072,050630s035lbl.pdf [Last
accessed 25 June 2015]
75. Clinical and Laboratory Standards Institute.
Performance standards for antimicrobial
susceptibility testing: twenty third
informational supplement. CLSI M100 S23.
Clinical and Laboratory Standards. Wayne;
PA: 2013
76. Mazuski JE, Gasnik L, Armstrong J, et al.
Efficacy and safety of ceftazidime-avibactam
plus metronidazole versus meropenem in
the treatment of complicated
intra-abdominal infection – results from a
Phase III programme (Abstract O191). 25th
European Congress of Clinical Microbiology
and Infectious Disease (ECCMID), 2014
77. Carmeli Y, Armstrong J, Laud P, et al.
Efficacy and safety of ceftazidime-avibactam
and best available therapy in the treatment
of ceftazidime-resistant infections – results
from a Phase III study (Abstract
LBEV0061b). 25th European Congress of
Clinical Microbiology and Infectious
Disease (ECCMID), 2014
78. Das S, Armstrong J, Mathews D, et al.
Randomized, placebo-controlled study to
assess the impact on QT/QTc interval of
supratherapeutic doses of
ceftazidime-avibactam or ceftaroline
fosamil-avibactam. J Clin Pharmacol
2014;54:331-40
79. Sartelli M, Viale P, Catena F, et al.
2013 WSES guidelines for management of
intra-abdominal infections. World J Emerg
Surg 2013;8:3
80. McLaughlin M, Advincula MR,
Malczynski M, et al. Correlations of
antibiotic use and carbapenem resistance in
Enterobacteriaceae. Antimicrob Agents
Chemother 2013;57:5131-3
81. Centers for Disease Control and Prevention.
Vital signs: Carbapenem-resistant
Enterobacteriaceae. MMWR 2013;62:
165-70
82. US FDA. ZERBAXA� (ceftolozane/
tazobactam) for injection. Package insert.
Cubist Pharmaceuticals U.S. 2014. Available
from: www.zerbaxa.com/pdf/
PrescribingInformation.pdf [Last accessed
15 April 2014]
83. Hirsch EB, Ledesma KR, Chang K, et al. In
vitro activity of MK-7655, a novel
b-lactamase inhibitor, in combination with
imipenem against carbapenem-resistant
Drug Profile Mawal, Critchley, Riccobene & Talley
16 Expert Rev. Clin. Pharmacol.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
02:
50 2
3 O
ctob
er 2
015

Gram-negative bacteria. Antimicrob Agents
Chemother 2012;50:3753-7
84. Castanheira M, Rhomberg PR, waters A,
Jones RN. In vitro activity of meropenem/
RPX7009, a carbapenem/b-lactamase
inhibitor combination tested against
contemporary populations of
Enterobacteriaceae and KPC-producing
strains (Abstract 257). ID Week 2014b
85. Achaogen. Plazomicin. Available from:
www.achaogen.com/plazomicin [Last
accessed 12 May 2015]
86. Walkty A, Adam H, Baxter M, et al. In
vitro activity of plazomicin against
5015 gram-negative and gram-positive
clinical isolates obtained from patients in
Canadian hospitals as part of the
CANWARD study, 2011–2012. Antimicrob
Agents Chemother 2014;58:2554-63
87. Endimiani A, Choudhary Y, Bonomo A. In
vitro activity of NXL104 in combination
with b-lactams against Klebsiella
pneumoniae isolates producing KPC
carbapenemases. Antimicrob Agents
Chemother 2009;53:3599-601
Ceftazidime–avibactam for cUTI & cIAI Drug Profile
17www.tandfonline.com
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
02:
50 2
3 O
ctob
er 2
015
Top Related