







Languages
Pages
Legal


Collaboration, Culture and Outcome
11 am- 11: 40 Tuesday 13th November
Todd McEwan
Director Operations Acute Hospital Network
Hunter New Englad Local Health District

Metaphor for Waiting List Management

It’s managements problem!
• Waiting lists are an artificial political construct
• I won’t recategorise
• Just give me more time
• You don’t listen too me I know whats right for
my patients
• It’s your problem because you wont resource
us to the level the community expects

Managements issues
• Medical autonomy is Dead
• There is significant variation in what you and
your colleagues do in managing your waiting
list
• I agree waiting lists are an artificaial political
construct, but surely getting the patient done
on time is in the patients interest
• Don’t use the patient as a pawn
• Excellence Every Patient Every Time

Gynaecology Services around Newcastle
• JHH/ RNC: – 12 OT theatres
– 1208 elective gynae cases
– 439 emergency gynae cases
– 1057 Obstetric Cases
– AAAA Clinic Attendances
• Belmont Hospital – 4 OT theatres
– 600 elective gynae cases
– 13 emergency gynae cases
• Maitland Hospital – 4 OT theatres
– 497 elective gynae cases
– 144 emergency gynae cases
– 684 Obstetric cases
• Peripheral primary and community hospitals – Singleton, Cessnock etc
– 220 elective gynae cases

Strategy

Challenges faced
• Medical staff had fractional appointments
• Consequently their work schedule was inflexible Additional OT sessions and leave relief were difficult to schedule.
• Imbalance between surgeons with OT capacity and surgeons with waiting list challenges
• Although the majority of surgeons were agreeable to the idea of pooling patients it did not work in practice as the bureaucratic and practical barriers were insurmountable.
• Wide division between gynaecology and gynaecology oncology service
• Relationship between the neighbouring facilities

Risk Management
Collaboration
• There were significant internal issues not
readily apparent
• The tangible a intangible issues had to be
dealt with
Clinical and management changes implemented
• Clinical Leadership Model
• Change in surgeon staff profile
• Enhanced flexibility
• Close relationships with “satellite” facilities
• Additional OT time
• Administrative and booking staff support

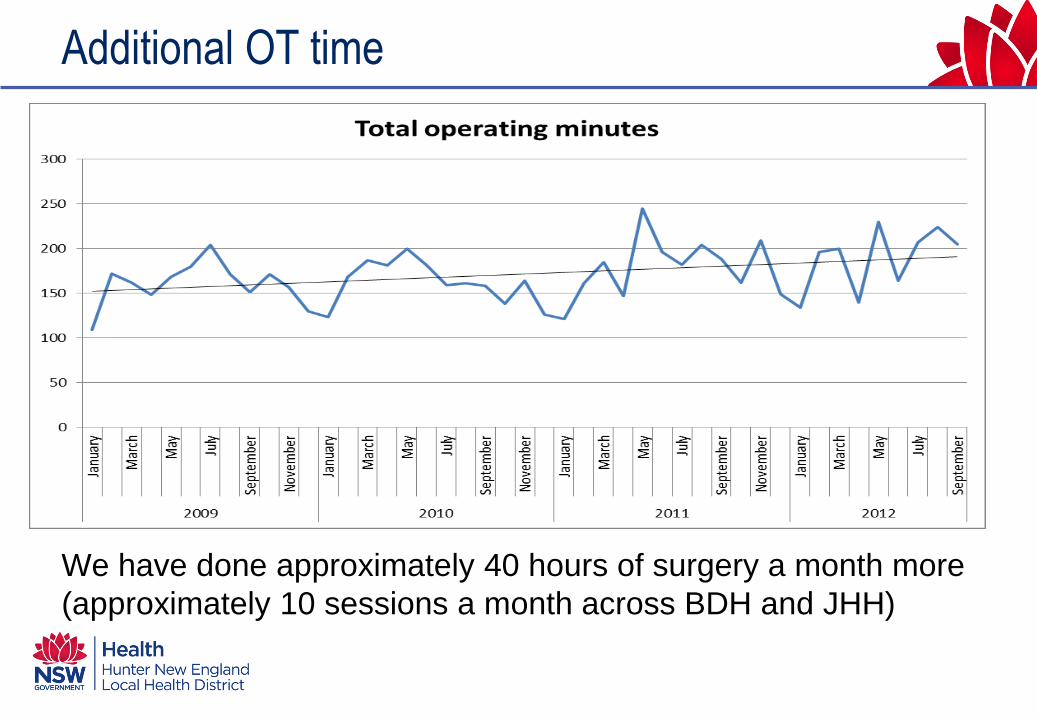
Additional OT time
• 20% increase in OT time since 2009
• Although the Department could not initially see
how the additional OT time could be
accommodated, it was initially absorbed by
utilising VMOs who primarily worked in Obstetrics
but were willing to accept elective patients from
other AMO’s gynae lists.
• As time has gone on and a number of specialists
went part time and more specialists were
employed the new surgeons accepted these lists
Additional OT time
We have done approximately 40 hours of surgery a month more
(approximately 10 sessions a month across BDH and JHH)

Not surprisingly, providing OT access alone was
not the solution
Discussion of the non-tangable and
cultural aspects

All washed up!

Culture
• Leadership drives change
• Accountability delivers outcomes

The Clinical Leadership Model
• Rather than just one Clinical Director and a
Service Manager there is now a leadership team
representing facility management, foetal
medicine, gynaecology, obstetrics, gynaecology
oncology, registrar training supervisor
• Focused Accountability

Common Messages
• Key messages from the leadership team are
– Enthusiasm for working in the public sector
– Acceptance that there will always be differences
between the public and private sector
– A commitment to finding professional satisfaction
not just hip pocket satisfaction.

Change in staff profile
• Staff specialist v VMO: it is not employment
model but the cultural model that is important.
• Introduction of Post Graduate Fellow: resulted
in significant service provision improvements.
Also able to provide training opportunities
• Enthusiasm for the public sector.

Administrative and booking staff support
• Waiting List Manager
• Manager of Outpatient Clinics
• Admissions staff
• Theatre Manager
• Administration and administrative staff within
the department.

Flexibility
• Incorporate increased flexibility into work
patterns
– Surgeons
– Clinics
– Administrative and waiting list staff
– Patients
• This has also required a realistic assessment of
medico legal risk over such things as
transferring care between clinicians.

Movement between sites
Close relationship between facilities and surgeons allowed patients
to be operated on at the clinically appropriate site which allowed
the most rapid admission

So it’s a game of Chess?

What do the changes feel like on the ground?
• Admission staff no longer fear the routine
auditing of the gynae list as now when there are
enquiries about waiting time, positive
expectations and viable alternatives can be
expressed.
• There is a reported reduction in the number of
patients ringing with enquiries (and greater
reduction in disgruntled enquiries)
• It can look like a headache for the waiting list,
admissions, clinic and operating theatre staff

What do the changes feel like on the ground
• The Surgeon’s perspective
– “Feels like admissions aren’t always on your
back about lists”
– I’m not in McEwan’s Office every week, that’s
better for me and him!

What have we achieved across BDH and JHH.
• July 2009: 732 pts. On
list an average of 142
days,
• Jan 2011, 760 pts. On
list an average of 192
days.
• Sept 2012 702 pts On
list an average of 113
days.

The referrals did not stop
And our number of additions and removals remained reasonably
aligned.

Composition of the Waiting List
During this time, the relative contributions from each urgency
category remained essentially unchanged

Common Goals / Accountability

• Manage the change over of post graduate fellow
• Some surgeons with specific demand problems
exist, but these are increasingly seen as a
departmental problem requiring whole of
department solutions
• Potential introduction of a mechanism of
creating a “free agent” surgeon.
Challenges ahead still?

Top Related