





Languages
Pages
Legal

Paula M. Jacobs, Ph.D. Associate Director, DCTD. NCI
Cancer Imaging Program
Cancer Imaging Program Update
High Country Nuc Med 4 March 2013
A New Environment
• FDA regulation stepped up – Clinical PET agents need NDA/ANDA or IND – New GMPs for PET
• New FDA guidance documents – PET INDs – Imaging endpoint in therapeutic trials
• Proposal in PF to revise USP <821> • Economic pressures on advanced imaging

History
• In 2005, Cancer Imaging Program in NCI initiated an effort to encourage more systemic and widespread use of “generic” PET agents in therapeutic research
• We concentrated on agents with broad potential but little possibility of proprietary development in the regulatory environment
• FLT is the poster child for this effort and led to the “shared IND” concept

Overall strategy
• File INDs for selected generic imaging agents • Make the IND documents public, including
SOPS • Provide letters of authorization to extramural
community on request • Provide some advice • Push the envelope!

“SHARED” INDS
One strategy to reduce the barriers to investigational use of molecular imaging agents

Letter of Right of Reference
• Also called: cross-file letter, letter of authorization (LOA)
• Incorporates the specified sections from one IND, DMF, or NDA into another by reference
• The information is not repeated in the new IND and the information is not provided to the new applicant
• All the new applicant needs is the letter The holder of the original IND has
no responsibility for the new IND
Example: LOA to NCI FLT IND given to a University or Industry Investigator
• Letter specified that authorization is given for: – Pharmacology & toxicology information – Previous human experience
• Letter noted – That CMC reference is not authorized – Some commercial firms have filed DMF – New applicant may submit their own CMC – New applicant may use commercial firms with LOA to
the commercial DMF • The LOA is filed to the NCI IND and the new IND

Advantages
• Saves the lives of many animals (and $$) by avoiding repetitive toxicology studies
• Saves the work needed to organize and present several sections of an IND
• Reduces uncertainty since the FDA has accepted the information provided in the original IND and/or DMF
• Saves FDA review time – review can focus on clinical trial

Additional Resources from NCI
• Documents on the CIP web site – http://imaging.cancer.gov/programsandresources/Ca
ncer-Tracer-Synthesis-Resources – Full sets of SOPs for the USP<823> environment that
anyone can use to customize for their manufacturing (135+ SOPs)
– Investigators Brochures, summarizing known information, updated yearly for a few IND agents
– For some, full toxicology reports • Some “hand-holding” advice

F-18 FLUOROTHYMIDINE
Example: promise and pitfalls

[18F] fluorothymidine: early 2000’s
• No USP monograph • No multicenter trials • Most human research under RDRC • “Generic” drug – no IP • 2004 IND filed by NCI
– Univ. Wash. first site – Tracer synthesis at 4 contract trial sites – Object: multicenter trials

Did this work?
• Not as well as we wished – Chemistry issues – Public access to regulatory documents limited
• 2006: expanded access and out-reach – Web posting, implicit click-thru MTA – LOA given to qualified entities on request – Regulatory “hand-holding” for PIs – Engaged the major commercial suppliers
Current Status • Commercial firms - drug master files (DMF) • LOA provided to legitimate entities
– 9 companies for drug development – 34 academic sites – 1 Society
• LOA from Medivir for pharm-tox data • Cooperative activities
– Contract trials – Clinical Center Trials – ACRIN multicenter trials

Trials now posted
• Approximately 90 trials, at least 21 multicenter; more than half dependent on LOA from NCI – Variety of tumors – Diagnosis, response to therapy – Correlation with Ki67 – RT planning – Evaluation of new therapies
• US and Europe/Asia- 75% are US • Academic and industrial –20% companies

Lessons learned • Commercial entities best for manufacturing
– Understand the logistics – Strong incentive for national CMC uniformity
• Regulatory ignorance is astonishingly high: “I don’t need an IND/DMF because…” – “I am using the same synthesis that NCI filed” – “I am an academic not a company” – “My IRB approved, why would I need more?” – “I registered for the SNM Trial Network”

Commercial FLT Supply Sites

A LITTLE BIT ABOUT OUR OTHER INDS

Molecular Imaging Probes – NCI IND
• [18F]-FLT – proliferation • [18F]- FMISO - hypoxia • [18F]- FES – estrogen receptor • [18F] – Sodium Fluoride – bone seeking • [111In]-trastuzumab ̶ Her 2 • [89Zr]-panitumumab ̶ EGFR • [one MR agent: ferumoxytol]
Most recent: 89Zr-panitumumab
• EGFR directed antibody – Colon – HNSCC
• PET agent • Made under USP <823> not GMP • All steps performed in radiopharmacy • Primary FDA issue was sterility of isotope
FMISO
• [18F] fluoromisonidazole (FMISO) – Hypoxia - trapped in cells in absence of O2
• Regulatory documents posted on website • One company has DMF • 9 LOA • Trials
– Contract trial at Univ Wash: response to CRT – ACRIN: response to CRT in GBM
– 25 Trials listed (5 multisite

FMISO Imaging to Plan RT
Rajendran EJNMMI: 33;S44, 2006

FES
•16α-[18F]Fluoro-17-β-estradiol (FES) –Binds to estrogen receptor (ERα)
•Regulatory documents posted on website •Manufactured at Univ Wash & NCI •Trials
–Univ Wash & NCI, response to Rx –10 trials (1 multisite)
•No DMF (to my knowledge) • 3 LOA

Confirming Estrogen Receptor Targeting with Therapy
Endometrial Cancer, pre therapy
3 days endoxifen

Sodium Fluoride F-18
• Sodium [18F]-fluoride • The clinical need
– Diagnose bone metastases (breast, prostate) – Other bone diseases – Technetium 99m shortages
• Trials – NCI IND, ACRIN multicenter trial – Multicenter trial by AMI – 10 trials (3 multicenter)
• NCI NDA filed 2009, approved 1/2012
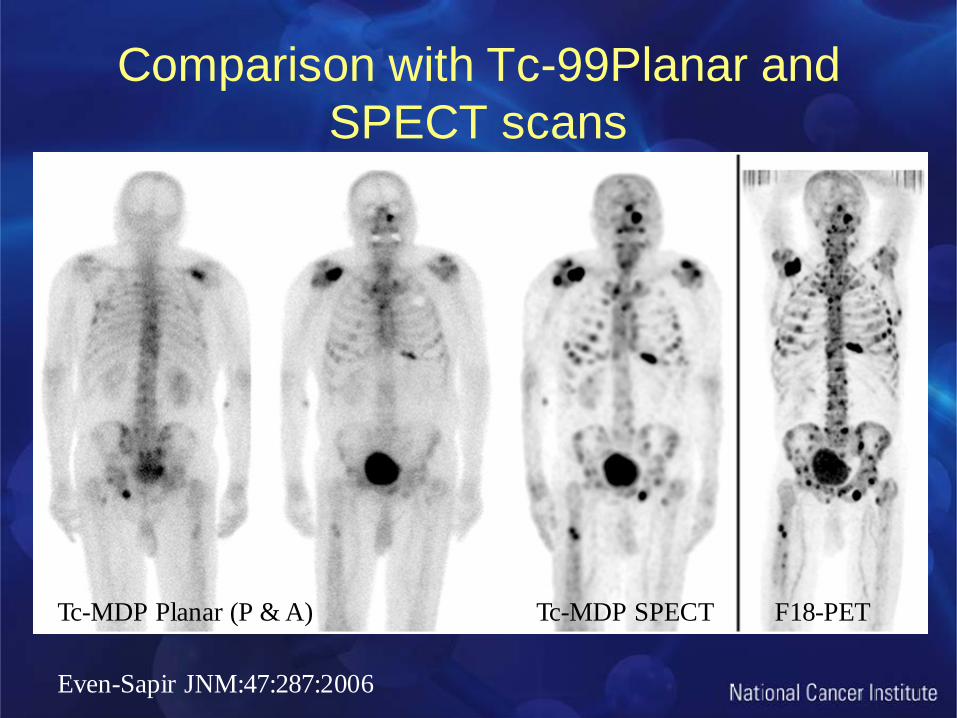
Comparison with Tc-99Planar and SPECT scans
Tc-MDP Planar (P & A) Tc-MDP SPECT F18-PET
Even-Sapir JNM:47:287:2006

NEW REGULATORY ENVIRONMENT

FDA regulation stepped up for PET
• Manufacturing for clinical use requires GMP – PET specific GMPs finalized in 2009 : 21 CFR 212 – Not for other radiopharmaceuticals
• Clinical PET agents need NDA/ANDA – ANDA for 18F-FDG, 13N-NH3, 18F-NaF, 11C-Choline – Others need NDA
• Investigational PET usually need IND • FDA flexible with expanded use INDs

PET INDs Final Guidance Dec. 2012
• Summarizes IND process for unapproved PET drugs
• Makes recommendations on how to submit an IND
• Provides advice on investigational PET drug expanded access options, and
• Describes the process for requesting permission to charge for an investigational PET drug
• http://www.fda.gov/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/default.htm

FDA PET IND Guidance
• No new IND regulations in this guidance – PET drugs must have IND, NDA, or ANDA – FDA has exercised some enforcement discretion
• Recognition that many PET agents are not commercializable – No IP – Tiny markets
• Some regulatory flexibility permitted

Proposal in PF to revise USP <821>
• PF 38 (4) 2012 (http://www.usppf.com/pf/ ) • Remove informational aspects to new chapter
<1821> titled Radioactivity • Retitle <821> ldentification and Assay o f
Radionuclides with extensive update • Draft revisions for public comment fall 2013

Top Related