







Languages
Pages
Legal

Using HTA to Inform Policy and Practice in Newfoundland and Labrador 2015 CADTH Symposium Sheila Tucker, M.L.I.S., B.Ed., B.A. (Hon), CPAD. – CADTH
Disclosure – Sheila Tucker
Relationship with Commercial Interest:
• Grant/Research Support: None
• Speaker Bureau/Honoraria: None
• Consulting fees: None
• Memberships on advisory committees, boards: None
Other Affiliations:
• I am a CADTH employee independently located in Newfoundland.
Objectives
• Describe the local context and approach to outreach and knowledge exchange.
• Share the information and evidence used to inform policy and practice change.
• Discuss early experiences and impact.

Partners
Blood Glucose Monitoring in Long Term Care
• Project leaders:
– Kelli O’Brien, Vice-President of Long Term Care and Rural Health, Western Health
– Heather Brown, Vice-President of Rural Health, Long Term Care, and Community Supports, Central Health
• Project teams at Western Health and Central Health, Newfoundland

Strengthened Customer-facing
Support
Committee/Association Relationships
National Network
Integrated KT
Identification of Knowledge/ Practice Gaps
Pan-Canadian KM Planning
National Partnerships
Key Message +Tool Development
Jurisdictional Network
Individual Customer/ Stakeholder Relationships
Direct Customer Interface
Identification of Context Specific Needs
Local Partnerships/ Opportunities
Topic Identification
Implementation Support
responsive, nimble, customized
A
Awareness & Relationship Management
Knowledge Mobilization & Strategic
Linkages
B
Capacity Building C
Outreach Event Management D
Impact / Value for Money E
CADTH’s Outreach Program: KMLO
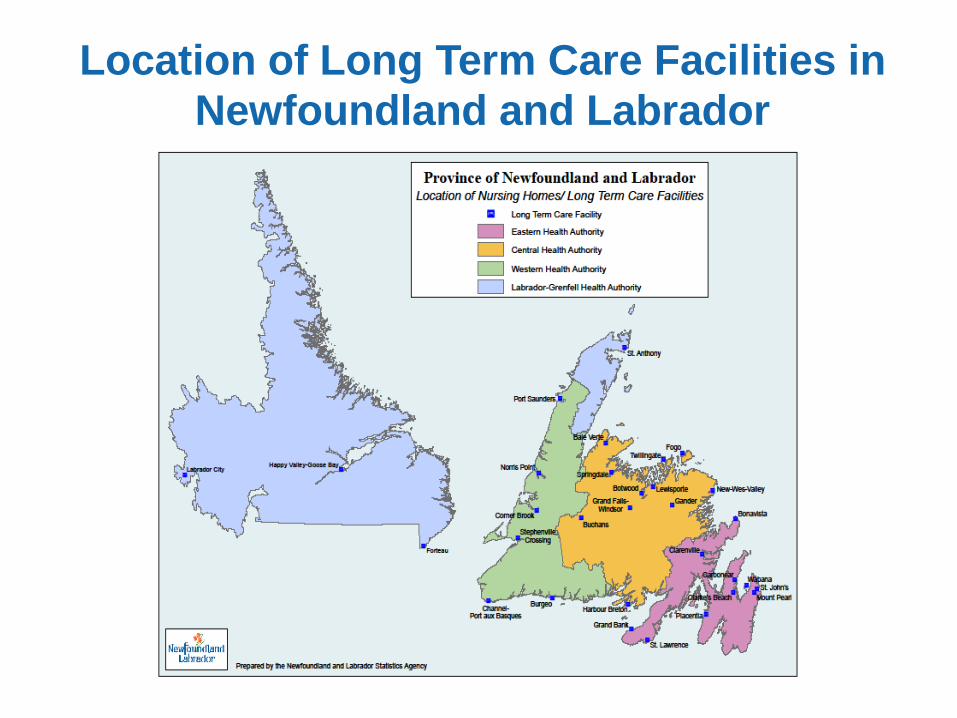
Location of Long Term Care Facilities in
Newfoundland and Labrador
CADTH Evidence on Blood Glucose Monitoring
Outreach in Newfoundland and Labrador
• Self-monitoring of blood glucose in diabetes management.
CADTH (2009)
• Outreach and knowledge exchange activities in
Newfoundland and Labrador (general population)
• Questions raised about sub-groups of patients with type 2
diabetes
• Long term care?
• CADTH Rapid Response report (2010)
Rationale for this Initiative
• Aging Population ↑, Diabetes Prevalence ↑
• Evidence of sub-optimal use of test strips in diabetes
management
• New guidelines
• Role of blood glucose testing in diabetes management
being reconsidered
Releasing Time to Care
Goal:
• Implement best practice in the care of residents with type 2 diabetes.
Anticipated Benefits:
• Supports resident and family-centred care
• Improved assessment skills for care providers
• Less stress and pain for residents
• Improved utilization of resources
• More time and resources for improving the resident experience
• Monitoring foot, dental, and vision health, and A1C.
• Individualized care.
• Well-being, quality of life
Western Health and Central Health
Roles
• Leadership
• Project planning and management
• Stakeholder engagement
• Identification of knowledge gaps
• Adoption of new policy and practice
• Evaluation
• Dissemination
Project Advisory Committees
• Comprised of long term care and diabetes stakeholders
• Front line clinicians
• Critical in providing local, clinical perspective, review and
feedback on evidence, information, and clinical practice
tools.
• Facilitated ownership and adoption of the practice change.
CADTH’s Role
• Liaising with project stakeholders
• Working in collaboration and consultation with the project
leads to:
• Develop presentations to profile the existing evidence
• Outreach to CADTH networks across Canada / informal
scan to identify existing relevant policies and practice
guidelines
• Addressing knowledge gaps
Evidence and Information
Used in the Projects
• Baseline utilization data
• Informal cross-country scans
• Canadian Diabetes Association – 2013 Guidelines for
Diabetes in the Elderly
• Clinical experts
• Accredited webinar
CADTH Rapid Response Report: Management of Diabetes
in the Long-Term Care Population: A Review of Guidelines
(2013) – Summary with Critical Appraisal
What are the evidence-based guidelines for the monitoring of blood glucose for patients with diabetes in the long-term care population?
• Two evidence-based clinical practice guidelines retrieved;
• Suggested laboratory tests be performed when diabetes is suspected.
• Levels of glucose (fasting blood glucose or HbA1c) are recommended to be tested every 3 to 6 months, however the frequency of the blood glucose monitoring should be individualized.
CADTH Rapid Response Report: Glucose Replacement
Agents in Frail Elderly Patients with Type II Diabetes in
Long-Term Care: Clinical and Cost-Effectiveness, Harms,
and Guidelines (2015)
Summary of Abstracts
Q1. What is the clinical effectiveness of glucose replacement
agents in frail elderly patients with type II diabetes who reside
in long-term care (LTC) facilities?
Q2. What are the harms associated with glucose replacement
agents in frail elderly patients with type II diabetes who reside
in LTC facilities?
Glucose Replacement Agents in Frail Elderly Patients with
Type II Diabetes in Long-Term Care: Clinical and Cost-
Effectiveness, Harms, and Guidelines (2015) - Continued
3. What is the cost-effectiveness of using glucose replacement
agents in frail elderly patients with type II diabetes who reside
in LTC facilities?
4. What are the evidence-based guidelines regarding the use
of glucose replacement agents in frail elderly patients with
type II diabetes who reside in LTC facilities?
Results:
• No evidence, however…

Clinical Practice Tools
Developed/customized in consultation with project
teams:
• Resident / family pamphlets
• “Reducing Blood Glucose Testing for Residents With Type 2
Diabetes in Long Term Care”
• “Stop Hypoglycemia” (new tool)
• Clinical practice guidance card
• Poster
• Pocket card

Education and Change Management
• Two new policies:
• Blood Glucose Monitoring;
• Glycemic Control in the Frail Elderly
• Staff education sessions
• Clinical Order Sets
• Letters to physicians, other stakeholders
Early Experiences
Central Health and Western Health
• Enhanced knowledge, networks - “we are not alone”.
• Skill development - evidence informed decision
making processes.
• Time commitments required for partnerships, practice
and policy change.

Capacity Building
• Two-way • RHA capacity HTA use
• CADTH capacity to engage with front line healthcare practitioners to fully understand needs, perspectives
• Team approach to addressing emerging questions and challenges
• Importance of ongoing service support/continuity
CADTH is helping us to develop the skills and build the confidence of our people to critically appraise, contextualize, and use the evidence. HEATHER BROWN, Central Health, NL
Going Forward
RHA Plans
• Evaluation
• Dissemination
• Future initiatives to improve practice in other settings
• Opportunities to address research gaps

Acknowledgements
• Kelli O’Brien, Western Health
• Heather Brown, Central Health
• Project advisory committees at Western Health and Central
Health
• Rapid Response Team, CADTH
• Knowledge Mobilization, CADTH
Photo provided by Western Health
Releasing Time to Care Stay Tuned for Future Updates – Thank you!
Top Related