







Languages
Pages
Legal


ASTHMA : UNDERGRADUATE STUDENTS
BY
Prof MOHMMAD EL DESOUKY ABOU SHEHATA
Prof .of Thoracic MedicineMansoura University
BY
Prof :MOHMMAD EL DESOUKY ABOU SHEHATA
Prof .of Thoracic MedicineMansoura University

Definition of Asthma
A chronic Inflammatory disorder of the airways Many cells and cellular elements play a role Chronic inflammation leads to an increase in airway
hyper responsiveness with recurrent episodes of wheezing , coughing , and shortness of breath
Wide spread , variable .and often reversible airflow limitation
GINA 2009
Burden of Asthma
300 milion individuals are affected worldwide
Global asthma prevalance 1% --18% Annual world deaths estimated at 250,000 / year
GINA –
2oo7
Asthma Development And Expression
GENETIC FACTORS + ENVIRONMENTAL FACTORS
the mechanisms whereby they influence the development and expression of asthma are
complex and interactive.
Genes likely interact both with other genes and with environmental factors to determine asthma susceptibility
Genetics OF Asthma
Genes Linked To Pathogenesis
Production of allergen- specific igE antibodies Expression of airway hyper responsiveness Generation of inflammatory cytokines Determination of of ratio between Th1 and
Th2 immunoresponse ( relevant to hyageine hypothesis)
Holloway JW, Beghe B, Holgate ST. The genetic basis of atopic asthma. Clin Exp Allergy 1999;29(8):1023-32.
Environmental Factors
Allergens• Indoor: Domestic mites, furred animals (dogs, cats, mice), cockroach allergen, fungi, molds, yeasts• Outdoor: Pollens, fungimolds, yeasts Infections (predominantly viral) Occupational sensitizers Tobacco smoke• Passive smoking• Active smoking Outdoor/Indoor Air Pollution Diet GINA
201o

Th0-cell
IL-12
IL-4
IL-2IFN-TNF-TNF-
IL-4IL-5IL-10IL-13
Predominantantibodyresponse
IgG2a
IgE, IgG1
Biological role
Defence againstintracellularpathogens (e.g.viruses or bacteria)
Defence againstlarge extracellularpathogens and mediators of allergy
Th1-cell
Th2-cell
Pathogenesis : Th-cell cytokine profile determines antibody isotype
Corry DB et al. Nature 1999
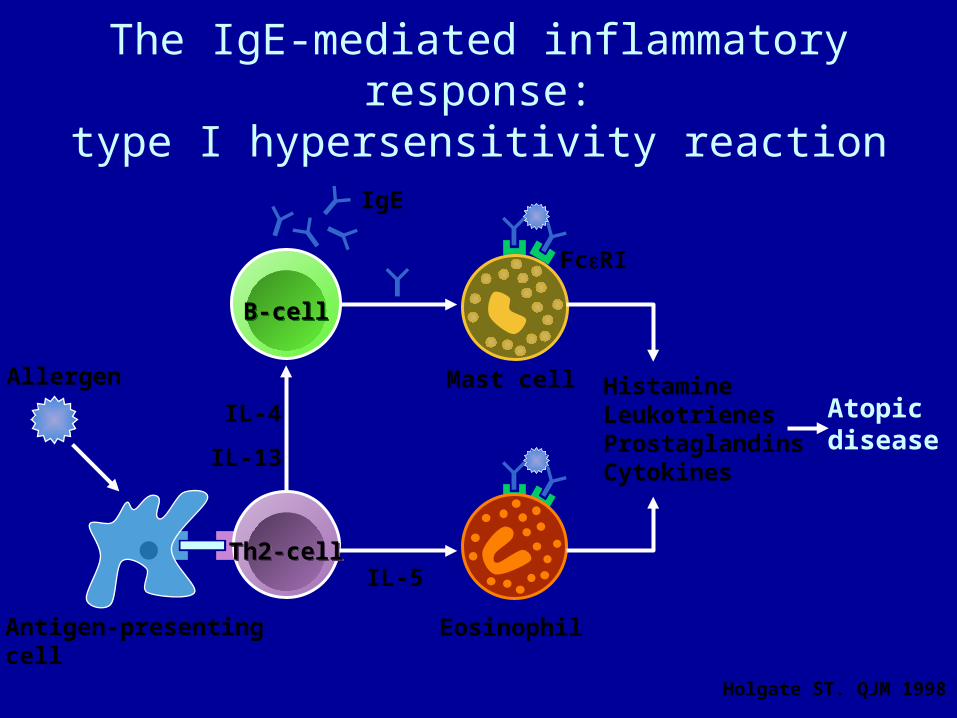
Th2-cellTh2-cell
B-cellB-cell
Eosinophil
IL-4
IL-13
Mast cell
FcRI
IgE
HistamineLeukotrienesProstaglandinsCytokines
Atopicdisease
IL-5
Antigen-presentingcell
Allergen
The IgE-mediated inflammatory response:type I hypersensitivity reaction
Holgate ST. QJM 1998

Mast cellmediator release
Inflammatory mediators result in early and late-phase asthmatic responses
24
Time (hours)Antigen
% p
red
icte
d F
EV
1
0 1 2 3 4 5 6 7 8
100
80
60
40
20
0
Eosinophil influx and mediator release
Neutrophil influxand mediator release
Histamine, prostaglandins, leukotrienesand thromboxanesmediate bronchospasm
• Inflammation
• Persistent obstruction
• Increased airway responsiveness

AcuteInflammation
AirwayRemodelling
ChronicInflammation
Acute and chronic inflammation
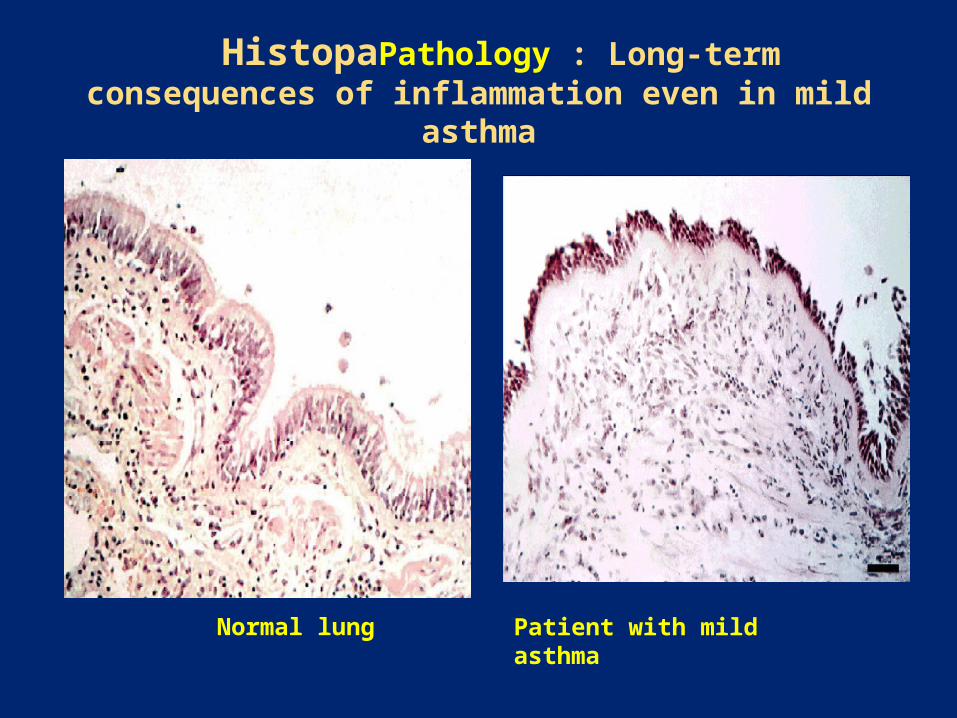
HistopaPathology : Long-term consequences of inflammation even in mild asthma
Normal lung Patient with mild asthma

Asthma Pathology

Bronchoconstriction
Before allergen challenge
10 minutes after allergen challenge
P Howarth
Diagnosis of Asthma
Symptoms and signs Wheeze History of any wheeze cough dyspnea tightnes of chest Symptoms occur or worsen at nights Symptoms occur or worsens in seasons Patient has eczema ; hay fever or family history
of allergy

When We Suspect Asthma?
When symptoms occure or / worsen at night and awaking the patient
When symptoms occur or worsens at season When there is associated eczema ; hay fever and
or family history of asthma

When we suspect Asthma (cont )
Symptoms occur on exposure to Animals with fur Aerosol chemicals Change of temperature Domestic dust mites Drugs Exercise Pollen Infection Smoke Strong emotions Symptoms responds to anti asthma therapy Patient’s cold “ go to the chest” or take more than 10 days

Signs: Athma
In between attacks no signs are detected or minimal signs.
During attacks: - Harsh vesicular breath sounds with prolonged
expiration - Audible wheezes and rhonchi on auscultation. - There may be silent chest in severe cases. The course of asthma is characterized by its
variability, periodicity and unpredictability; exacerbations vary from brief to sever ones.

Factors Influencing the Developmentand Expression of Asthma
Environmental Factors Allergens Indoor: Domestic mites, furred animals (dogs, cats, mice), cockroach allergen, fungi, molds, yeasts Outdoor: Pollens, fungimolds, yeasts Infections (predominantly viral) Occupational sensitizers Tobacco smoke Passive smoking Active smoking Outdoor/Indoor Air Pollution Diet
GINA 201o

Diagnostic Challenge In AsthmaPseudo – Asthma (cont)
When cough is not Asthma
Cystic fibrosis Primary Ciliary Dyskinesia Chronic purulent ( Bacterial ) bronchitis Tracheomalasia Habit – cough syndrome

Diagnostic Challenge In AsthmaPseudo – Asthma (cont)
When wheezing Is not Asthma
Vocal Cord Dysfunction Partial Aiway Obstruction ( COPD ) Foreign body Bronchomalasia

Diagnostic Challenge In AsthmaPseudo – Asthma (cont)
When Dyspnea Is not Asthma
Hyperventilation Anaxiety Exertional Dyspnea

Investigation of Asthma
Lung Function Spirometry
- Increase of FEV1> 12% or 200 ml after administration
- of bronchodilators Peak expiratory flow rate (PEF) - Improvement of 60 L / min or 20% of pre-
bronchodilator administration - Diurnal variation more than 20% suggest a diagnosis
of asthma Aiway hyper responsivenes ( when lung function is normal ) Metaccholine ; histamine and manitol Skin tests and Specific IgE in serum
Differential Diagnosis of Asthma
1. COPD (chronic bronchitis and emphysema). 2. Left sided heart failure (cardiac asthma). 3. Pulmonary embolism. 4. Mechanical obstruction of the airways by
tumors or foreign body. 5. Drug induced cough e.g; angiotensin
converting enzyme (ACE) inhibitors. 6. Vocal cord dysfunction (Factitious asthma).

Complications of Asthma
Respiratory failure may follow acute severe attacks.
Chronic severe asthma with steroid resistance. Spontaneous Pneumothorax. Fractures of ribs and other complications of
repeated cough may occur especially in old age. Segmental collapse due to plugging with mucus. Allergic bronchopulmonary aspergillosis. Psychological troubles.
Asthma Control ( Treatment )
Asthma education ( patient/ doctor relationship
Identify and reduce risk factors Asses , Treat , and Monitor asthma Manage asthma exacerbation
Asthma Management And Prevention
1. Development of Patient/Doctor Partenership
2. Identify and Reduce Risk Factors
3. Assess ; Treat And Monitor Asthma
4. Manage Asthma Exacerbation
5. Special Consideration
GINA 2010
ASTHMA CONTROL
• Assessing Asthma Control
• Treating to Achieve Control
• Monitoring to Maintain Control
GINA 2009

Component 4: Asthma Management and Prevention Program
Controller MedicationsComponent 4: Asthma Management and Prevention Program
Controller Medications
Inhaled glucocorticosteroids Leukotriene modifiers Long-acting inhaled β2-agonists Systemic glucocorticosteroids Theophylline Cromones Long-acting oral β2-agonists Anti-IgE Systemic glucocorticosteroids
Inhaled glucocorticosteroids Leukotriene modifiers Long-acting inhaled β2-agonists Systemic glucocorticosteroids Theophylline Cromones Long-acting oral β2-agonists Anti-IgE Systemic glucocorticosteroids
Component 4: Asthma Management and Prevention Program
Reliever MedicationsComponent 4: Asthma Management and Prevention Program
Reliever Medications
• Rapid-acting inhaled β2-agonists
• Anticholinergics
• Theophylline
• Short-acting oral β2-agonists
• Rapid-acting inhaled β2-agonists
• Anticholinergics
• Theophylline
• Short-acting oral β2-agonists

Levels of Asthma Control
Characteristic ControlledPartly controlled(Any present in any
week)Uncontrolled
Daytime symptomsNone (2 or less /
week)More than
twice / week
3 or more features of
partly controlled
asthma present in any week
Limitations of activities
None Any
Nocturnal symptoms / awakening
None Any
Need for rescue / “reliever” treatment
None (2 or less / week)
More than twice / week
Lung function (PEF or FEV1)
Normal <80% predicted or
personal best (if known) on any day
Exacerbation None One or more / year 1 in any week
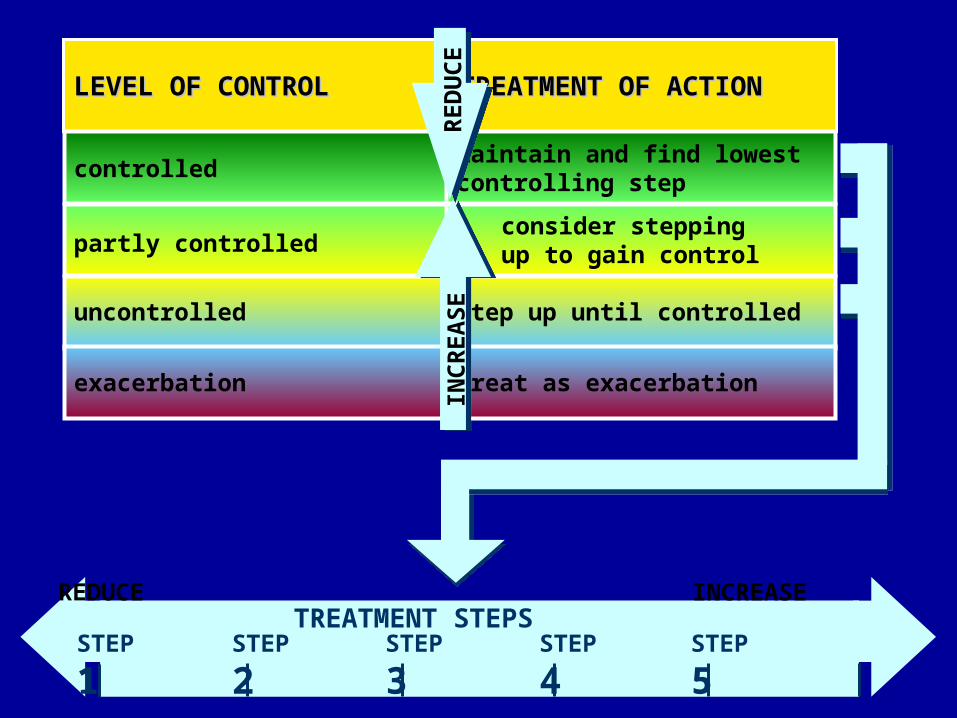
controlled
partly controlled
uncontrolled
exacerbation
LEVEL OF CONTROLLEVEL OF CONTROL
maintain and find lowest controlling step
consider stepping up to gain control
step up until controlled
treat as exacerbation
TREATMENT OF ACTIONTREATMENT OF ACTION
TREATMENT STEPSREDUCE INCREASE
STEP
1STEP
2STEP
3STEP
4STEP
5
RE
DU
CE
INC
RE
AS
E




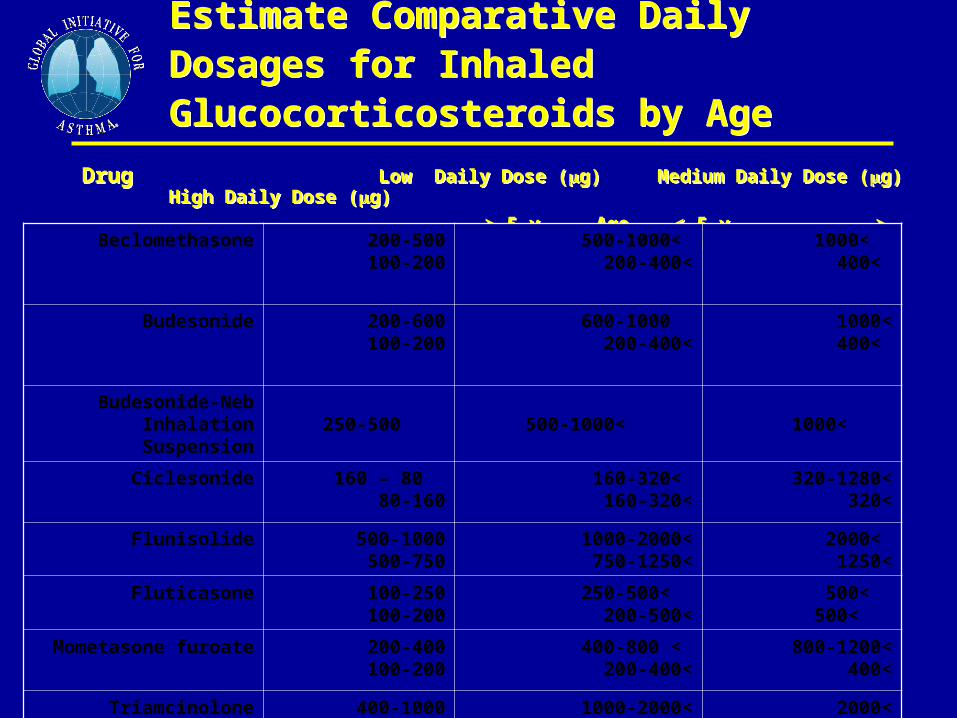
Estimate Comparative Daily Dosages for Inhaled Glucocorticosteroids by AgeEstimate Comparative Daily Dosages for Inhaled Glucocorticosteroids by Age
Drug Low Daily Dose (g) Medium Daily Dose (g) High Daily Dose (g)
> 5 y Age < 5 y > 5 y Age < 5 y > 5 y Age < 5 y
Drug Low Daily Dose (g) Medium Daily Dose (g) High Daily Dose (g)
> 5 y Age < 5 y > 5 y Age < 5 y > 5 y Age < 5 y
Beclomethasone 200-500 100-200 > 500-1000> 200-400 > 1000> 400
Budesonide 200-600 100-200 600-1000> 200-400 >1000> 400
Budesonide-Neb Inhalation Suspension
250-500 > 500-1000 > 1000
Ciclesonide 80 – 160 80-160 > 160-320> 160-320 >320-1280> 320
Flunisolide 500-1000 500-750 >1000-2000> 750-1250 > 2000> 1250
Fluticasone 100-250 100-200 > 250-500> 200-500 > 500> 500
Mometasone furoate 200-400 100-200
< 400-800< 200-400 <800-1200< 400
Triamcinolone acetonide 400-1000 400-800 >1000-2000> 800-1200 >2000> 1200

Immunotherapy
Allergen immunotherapy indicated whena. There is clear evidence of relationship between symptoms and
exposure to allergen.
b. Symptoms occur in major portion of the year.
c. There is difficulty in controlling symptoms with
pharmacological management.
Acute Severe Asthma
Symptom and Signs Severe dyspnea Patient can,t talk few wards or short sentenses Silent Chest Diaphoresis Tachypnea R.R > 30/m Tachycadia pulse > 120/ m Pulsus paradoxus Cyanosis Hypoxemia and increased CO2 level (near fatal
asthma)

Acute Severe Asthma
Investigations: Peak flow meter < 60 liter/min. Decrease of PaO2 with normal PaCO2, Later on, with
progression of the attack PaCO2 may increase Treatment of Acute Severe Asthma:
Oxygen therapy. Oxygen should be administered by nasal cannula or face mask.
Rapid-acting 2-agonistic are generally administered by nebulizer (Salbutamol on tubercului solution).
Ipratropeum bromide: a combination of neublized 2-agonists and anticholenergic ipratropneium bromide may produce better bronchodilator effect than either drug alone.

Acute Severe Asthma
Theophylline: Loading dose: half the patient's body weight in kg
x 10 in I.V. infusion over 30 min (e.g. for a 60 kg patient dose = 10 x 30 = 300 mg aminophylline).
Maintenance dose: 0.5 mg/kg/hour I.V. Corticosteroids:
Parenteral hydrocortisone in a dose up to 4 mg/kg which may be repeated.
Effective within 4-6 hours. Hydration: plenty of oral and I.V fluids

Mechanical ventilation in Asthma
Indication of mechanical ventilation: Patients who are drowsy or comatosed. Patients who are exhausted with respiratory
muscle fatigue. Paradoxical thoracoabdominal movement. Presence of cyanosis and hypercapnia. Previous history of mechanical ventilation in
intensive care.

Top Related