





Languages
Pages
Legal


Applying intersectionality in health and healthcare
Some views from social epidemiology
Davide MalmusiAgència de Salut Pública de Barcelona
ADAPT meeting, Bologna, 22 January 2015

Conceptual framework: determinants of health inequalitiesCommission to Reduce Social Inequalities in Health in Spain

• Some issues on inequality in healthcare by socioeconomic position (SEP) and gender
• Intersectionality in health and in policy evaluation: guide and examples
• Migrant status and intersectionality: an example• Summing up
Outline

• Self-ratings of health capture true inequalities in health by SEP – or they even underestimate them1,2
• GPs disagree more often on low SEP patients’ health ratings – tending to overestimate their health3
Evidence on SEP inequality in quality of care - within public systems (1)
1. Bago d’Uva T, et al. Differential health reporting by education level … Int J Epidemiol. 2008;37:1375-83. 2. Beam Dowd J, Todd M. Does Self-reported Health Bias ... J Gerontol B Psychol Sci Soc Sci. 2011;66:478-89.3. Kelly-Irving M, et al. Do general practitioners overestimate the health ... Soc Sci Med. 2011;73:1416-21.
Patient’s education level GP agrees GP under-rates GP over-rates
High education 75% 11% 14%
Medium education 74% 11% 16%
Low education 50% 12% 37%

• Among the chronically ill, low SEP patients perceive lower quality of doctor-patient relationship4
• Coronary risk scores overestimate mortality risk – much more in higher than lower social classes5
Evidence on SEP inequality in quality of care - within public systems (2)
4. Vonneilich N, et al. [Social inequality and perceived quality...]. Gesundheitswesen. 2011;73:211-6.5. Ramsay SE, et al. Prediction of coronary heart disease... Eur J Cardiovasc Prev Rehabil. 2011;18:186-93.

• Poverty screening – and referral6
• Socioeconomic factors in risk algorithms7
• Consciousness of own bias, positive discrimination8
• Resource allocation and quality incentives in deprived areas9
• Population-wide vs opportunistic programs10
SEP inequality in quality of care: some steps in the good direction
6. Bloch G. Poverty: a clinical tool for primary care in Ontario. Revised Nov 2013. Available at http://ocfp.on.ca 7. Fiscella K, et al. Adding socioeconomic status to Framingham scoring… Am Heart J. 2009;157:988-94.8. Bærøe K, Bringedal B. Just health: On the conditions for acceptable... J Med Ethics. 2011 ;37:526-9.9. Kiran T, et al. The association between quality of primary care... J Epidemiol Community Health. 2010;64:927-34.10. Palència L, et al. Socio-economic inequalities in breast and cervical cancer... Int J Epidemiol. 2010;39:757-65.

• GPs more likely to overestimate women’s health than men’s3
• But are women’s and men’s health self-ratings equally valid?
Gender inequalities in quality of care
3. Kelly-Irving M, et al. Do general practitioners overestimate the health ... Soc Sci Med. 2011;73:1416-21.

Gender inequalities in health: Perception or real illness?

• Women live longer but (in most countries) report poorer health than men
• Is this a matter of perception or illness behaviour?
Gender inequalities in health: Perception or real illness?

Data source: Spanish National Health
Survey 2006
Gender inequalities in health: Perception or real illness?

Data source: Spanish National Health
Survey 2006
Gender inequalities in health: Perception or real illness?

• Women live longer but (in most countries) report poorer health than men
• Is this a matter of perception or illness behaviour?NO -> They really suffer from more (non-life-threathening but limiting and painful) chronic conditions
Gender inequalities in health: Perception or real illness?

• As healthcare systems and professionals, we prioritise action on life-threathening diseases
• Conditions that don’t kill, but cause lot of suffering and disability in large shares of the population, fall behind
• Reorienting healthcare towards these conditions may be also good for gender equity
Gender inequalities in health: What does this matter for healthcare?

• Some issues on inequality in healthcare by SES and gender• Intersectionality in health and in policy evaluation: guide
and examples • Migrant status and intersectionality: an example• Summing up
Outline

Intersectionality: a quick guide

The analysis of health inequalities and health equity impacts of policies is usually centered on social class / socio-economic position.
Other social relations that generate health inequalities are usually more neglected – or treated separately.
Intertwined mechanisms of power relations that interact among them: need for intersectional approaches.
Palència L, Malmusi D, Borrell C. Incorporating intersectionality in policy evaluation analysis. A quick guide.
Intersectionality: a quick guide

Intersections between axes create complex social locations that are more central to the nature of social experiences than any single axe of inequality.
Groups in society are affected by their position in multiple systems of power and oppression, a “matrix of domination” that changes over time and place and in different institutional domains.
Palència L, Malmusi D, Borrell C. Incorporating intersectionality in policy evaluation analysis. A quick guide.
Intersectionality: a quick guide

The health effects of an intervention, context, condition… differ depending on one’s position according to the intersection of several axes / dimensions of inequality / power relations.
When designing/implementing interventions, targeted policies can be as ineffective as general ones in addressing multiple identities and power relations. Tools include multistrand/equality/power mainstreaming and Intersectionality-Based Policy Analysis.
Palència L, Malmusi D, Borrell C. Incorporating intersectionality in policy evaluation analysis. A quick guide.
Intersectionality: a quick guide

The health effects of an intervention, context, condition… differ depending on one’s position according to the intersection of several axes / dimensions of inequality / power relations.
When evaluating interventions (or testing associations) we have to consider that populations are not uniform (nor binary or categorical either), and go beyond the simple “whether” it works, to understand “for whom” (and “why” and “how”)
Palència L, Malmusi D, Borrell C. Incorporating intersectionality in policy evaluation analysis. A quick guide.
Intersectionality: a quick guide

Intersectionality: a quick guideExample 1. Family composition and healthRuiz-Cantero MT et al. A framework to analyse gender bias… JECH 2007
Model adjusted by sex and social class: Larger household size slightly associated with poorer self-rated healthCohabiting with a >65 aged person slightly associated with better health
Palència L, Malmusi D, Borrell C. Incorporating intersectionality in policy evaluation analysis. A quick guide.

Model stratified by sex and adjusted by social class: Household size and cohabiting with elderly strongly associated with poorer self-rated health among women but not among men
Palència L, Malmusi D, Borrell C. Incorporating intersectionality in policy evaluation analysis. A quick guide.
Intersectionality: a quick guideExample 1. Family composition and healthRuiz-Cantero MT et al. A framework to analyse gender bias… JECH 2007

Model stratified by sex and social class: Household size and cohabiting with elderly strongly associated with poorer self-rated health only among manual women
Palència L, Malmusi D, Borrell C. Incorporating intersectionality in policy evaluation analysis. A quick guide.
Intersectionality: a quick guideExample 1. Family composition and healthRuiz-Cantero MT et al. A framework to analyse gender bias… JECH 2007

Intersectionality: a quick guideExample 2. Crisis and mental healthBartoll X et al. The evolution of mental health in Spain… Eur J Public Health 2014
Prevalence (%) of poor mental health (GHQ-12>2)
The “zero change” in the whole population masks a worsening in men and improvement in women.
Palència L, Malmusi D, Borrell C. Incorporating intersectionality in policy evaluation analysis. A quick guide.
2006/07 2011/12 Prevalence Ratio
Total 19,6 19,8 1,01
Men 14,7 16,9 1,15**
Women 24,6 22,7 0,92*
* p<0,05 ** p<0,01 *** p<0,001

Palència L, Malmusi D, Borrell C. Incorporating intersectionality in policy evaluation analysis. A quick guide.
2006/07 2011/12 Prevalence Ratio
Men 14,7 16,9 1,15**
15-24 11,3 11,2 0,98
25-34 15,2 16,1 1,05
35-44 15,0 18,7 1,24*
45-54 14,8 19,1 1,29**
55-64 16,9 17,3 1,02
* p<0,05 ** p<0,01 *** p<0,001
Intersectionality: a quick guideExample 2. Crisis and mental healthBartoll X et al. The evolution of mental health in Spain… Eur J Public Health 2014
Prevalence (%) of poor mental health (GHQ-12>2)

Palència L, Malmusi D, Borrell C. Incorporating intersectionality in policy evaluation analysis. A quick guide.
2006/07 2011/12 Prevalence Ratio
Men 14,7 16,9 1,15**
Social class I 11,8 12,2 1,04
II 14,6 15,4 1,06
III 15,9 15,4 0,97
IV 14,8 18,2 1,23**
V 15,3 18,6 1,21
* p<0,05 ** p<0,01 *** p<0,001
Intersectionality: a quick guideExample 2. Crisis and mental healthBartoll X et al. The evolution of mental health in Spain… Eur J Public Health 2014
Prevalence (%) of poor mental health (GHQ-12>2)

Within men, the worsening is concentrated among the middle-aged and the manual social class, and stronger in immigrants.
Palència L, Malmusi D, Borrell C. Incorporating intersectionality in policy evaluation analysis. A quick guide.
2006/07 2011/12 Prevalence Ratio
Men 14,7 16,9 1,15**
Born in Spain 14,7 16,4 1,11*
Foreign-born 14,5 19,3 1,33*
* p<0,05 ** p<0,01 *** p<0,001
Intersectionality: a quick guideExample 2. Crisis and mental healthBartoll X et al. The evolution of mental health in Spain… Eur J Public Health 2014
Prevalence (%) of poor mental health (GHQ-12>2)

Intersectionality: a quick guideExample 3. Urban renewal and healthMehdipanah R et al. The effects of an urban renewal project… JECH 2014
Palència L, Malmusi D, Borrell C. Incorporating intersectionality in policy evaluation analysis. A quick guide.

Palència L, Malmusi D, Borrell C. Incorporating intersectionality in policy evaluation analysis. A quick guide.
Intersectionality: a quick guideExample 3. Urban renewal and healthMehdipanah R et al. The effects of an urban renewal project… JECH 2014

Palència L, Malmusi D, Borrell C. Incorporating intersectionality in policy evaluation analysis. A quick guide.
Intersectionality: a quick guideExample 3. Urban renewal and healthMehdipanah R et al. The effects of an urban renewal project… JECH 2014

Palència L, Malmusi D, Borrell C. Incorporating intersectionality in policy evaluation analysis. A quick guide.
Effects also varied by neighbourhood: clearer health improvement in the periphery (intervention with strong residents’ participation, including subway, elevators, escalators,) but not in the inner city (where the program was one among the many changes going on)
Qualitative studies are also key to study intersectionality: in an inner city neighbourhood, age and immigrant status shaped the perception on changes occurring - a senior group reported mainly discontent with gentrification and immigration, an immigrant-background youth group was satisfied with new public spaces and youth centers(Mehdipanah et al., Health Place 2013; Mehdipanah et al., Soc Sci Med 2015)
Intersectionality: a quick guideExample 3. Urban renewal and healthMehdipanah R et al. The effects of an urban renewal project… JECH 2014

• Some issues on inequality in healthcare by SES and gender• Intersectionality in health and in policy evaluation: guide
and examples • Migrant status and intersectionality: an example• Summing up
Outline

Intersectionality: my first (?) encounter

Intersectionality in health status in Catalonia
Objectives: To propose a health-equity-based classification of migration types. To analyse inequalities in self-rated health in Catalonia in the intersections of migration type, gender and social class. To analyse the contribution of socioeconomic conditions to migration-related health inequalities in Catalonia.Methods: Cross-sectional analysis of two 2005-06 population surveys (Health and Living Conditions). Population aged 25 to 64. “Age-adjusted” prevalences and logistic regressions.

Intersectionality in health status in Catalonia
Migration type internal/international, rich/poor, recent/less recent based on birthplace and year of arrival:• Catalonia (Local-born)• Rest of Spain
– High tertile of regional development in 1981– Medium or low tertile of development
• Foreign countries– Very highly developed countries (UN HDI) in 2006– Rest of the world, divided based on year of arrival:
• Recent immigrants (since 2000)• Less recents (until 1999)

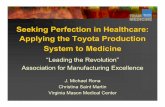
Intersectionality in health status in Catalonia2 dimensions: Migration type and gender
Odds Ratio of fair/poor self-rated health by migration typeAdjusted by age (Model 1) + class (M2) + standards of living (M3)
Women Men

Intersectionality in health status in Catalonia
Social class based on current, last or partner’s occupation:• I: higher-level professionals, managers, directors of large
companies• II: medium-level professionals and directors of small companies• III non-manual: administrative workers, clerks, safety and
security workers• III manual: self-employed and supervisors in manual occupations• IV-a: skilled manual occupations• IV-b: semi-skilled manual occupations• V: unskilled manual occupations

Intersectionality in health status in CataloniaSample by social class and migration type (women)
1192
880
171
108
88
33
102
342
146
33
17
3
60176
139
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
No manual Manual qualificat Manual no qualificat
Estranger-pobre
Estranger-ric
Espanya-pobre
Espanya-rica
Catalunya

Intersectionality in health status in Catalonia3 dimensions: Gender, social class and migration
Age-adjusted prevalence of material deprivation

Intersectionality in health status in Catalonia3 dimensions: Gender, social class and migration
Age-adjusted prevalence of fair/poor self-rated health
The two bars for the same category show results in the two surveys

Summing up
Gender and class also determine inequities in quality of care
People’s positions of power arise from (time- and place-specific) matrices of domination according to multiple axes
In quantitative studies, multi-stratified analysis can reveal the specific groups that are disadvantaged or whose health is affected by a policy, condition… – and give us hints of why, which can be further explored with qualitative studies

sophie-project.eu
@sophieproject
[email protected]@aspb.cat
Thank you! Gràcies!Grazie!
Photos: Roberto Brancolini, Roberto Malaguti, Fredi Roig
Top Related