






Languages
Pages
Legal


Aphasia TreatmentEvidence-based Practice – The State
of the EvidenceJanet Patterson, Ph.D., CCC-SLP
VA Northern California Healthcare SystemMartinez CA
andCalifornia State University East Bay
Hayward CA

Session Two
Activity/Participation-based Treatment
Treatment Delivery
Emerging Treatment Techniques

Objectives
–Identify evidence for activity/participation-based treatment techniques
–Identify evidence for emerging treatment techniques
–Identify considerations for successful treatment outcome

ACTIVITY/PARTICIPATION BASED TREATMENT TECHNIQUES

Outcome Measures• Test results• Connected speech– CIUs (Brookshire & Nicholas, 1993)
– Content units (Yorkston & Beukelman, 1980)
• Perceptual data– Interview with PWA, family, friends or associates
(Lomas et al., 1989)
• Activity reports and surveys– ADLs, social occasions, conversation, job success
• Quality of life (Hilary, Byng, Lamping & Smith, 2004)


Blackstone & Hunt Berg, 2006
Life Participation Approach to Aphasia
Core Components
• The explicit goal is enhancement of life participation. • All those affected by aphasia are entitled to service. • Both personal and environmental factors are targets of
assessment and intervention.• Success is measured via documented life enhancement
changes. • Emphasis is placed on availability of services as needed at all
stages of life with aphasia.
Chapey, Duchan, Elman, Garcia, Kagan, Lyon & Simmons Mackie (1999)

Activity/Participation-based treatment techniques
• Group treatment• Conversation participation• Treatment for caregivers or conversation
partners• Personal narratives; scripts• AAC

GROUP TREATMENT
Types of Group Treatment• Goal-directed– Conversation participation (Simmons-Mackie, 2000; Vickers, 1998)
– Specific linguistic goal– Cooperative learning (Avent, 1997)
– Reading and writing (Cherney, Merbitz & Grip, 1986; Clausen & Beeson, 2003)
• Life activities (i.e. book group (Bernstein Ellis & Elman, 2006))• Support (www.naa.org)
• Information (Avent, Glista, Wallace, Jackson, Nishioka &Yip, 2004)

Effect Sizes for Group vs. Individual Treatment --- RCTs ---
Kelly, Brady, Enderby, 2010
Evidence, ES and Conclusions
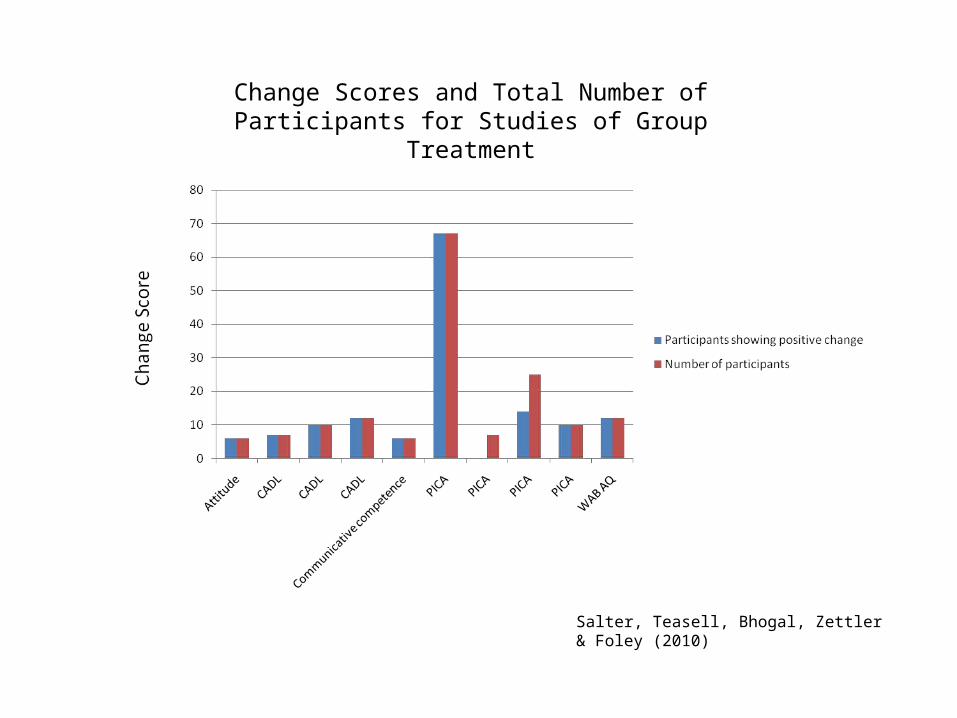
Salter, Teasell, Bhogal, Zettler & Foley (2010)
Change Scores and Total Number of Participants for Studies of Group Treatment

• RCTs– Inconsistent data supporting effectiveness of
group treatment over individual treatment• Limited support for social groups and language change
• Other published studies– Moderate support for group treatment and
language change– Varying methodology and outcome measures

• Anecdotal and qualitative information– Improved quality of life (Avent & Austerman, 2003)
– Feeling of community (Bernstein-Ellis & Elman, 1999)
– Improved sense of self (Elman, 2007)
– Safe environment in which to practice – People “vote with their feet”• Number of aphasia groups increasing• Expanded variety of group types
– Book group, artistic expression, theater group, exercise group, choral group

CONVERSATION PARTICIPATION

Script Training
• Client and clinician create short, relevant scripts
• Repetition until mastery– Personal cues (Freed, Marshall, Nippold, 1995)
– Computer directed (Cherney, Halper, Holland & Cole, 2008)
– Speech-language pathologist as trainer (Youmans, Holland, Muňoz &Bourgeois, 2005)
• Insertion into connected speech situation
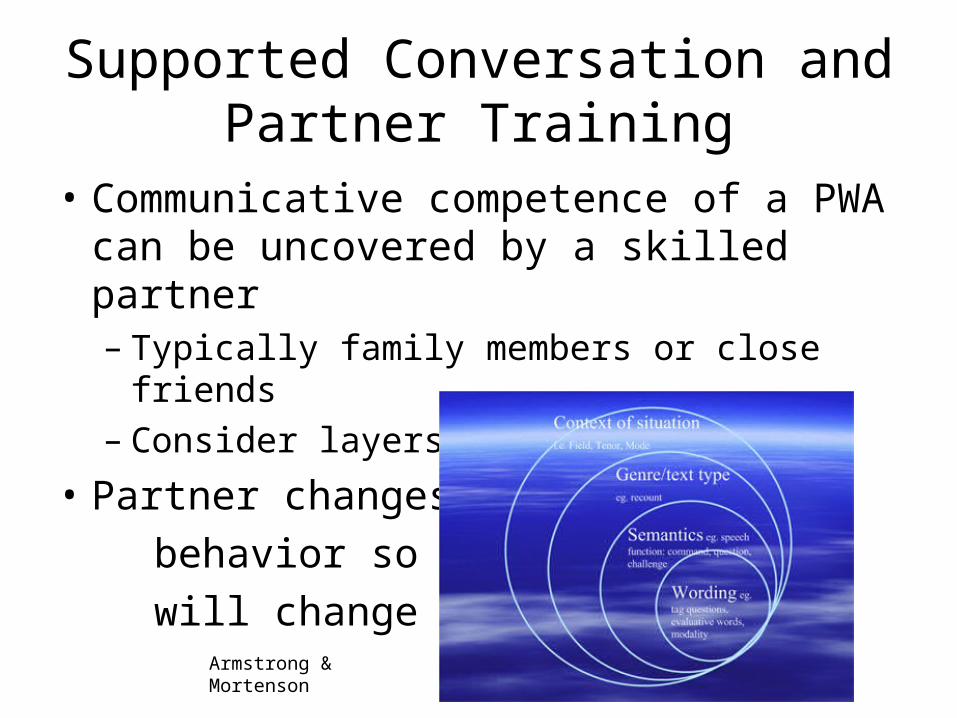
Supported Conversation and Partner Training
• Communicative competence of a PWA can be uncovered by a skilled partner– Typically family members or close friends– Consider layers of training
• Partner changes behavior so PWA will change
Armstrong & Mortenson
Treatment Techniques
• PACE Promoting Aphasics’ Communicative Effectiveness (Davis & Wilcox, 1985)
– Collaborative exchange of information• RET Response Elaboration Training (Kearns, 1985)
– Expand utterance content• Conversational Coach (Hopper, Holland & Rewega, 2002)
– Clinician coaches PWA and partner• Reciprocal Scaffolding(Avent & Austerman, 2003; Avent, Patterson, Lu & Small,
2009)
– Apprenticeship model with communication embedded within meaningful contexts

Evidence, ES, Conclusions
• Script training– Approximately 15 studies • PWA have variable characteristics
– Mild to moderate aphasia– Typically 6 months or more post onsets
• Outcomes– Improved production of practiced scripts– Some generalization to other communication situations– Slightly increased speaking rate– Error reduction
– Insufficient evidence for systematic review - yet

• Review of partner training studies– PWA – variable characteristics
• Most lived independently• 4-178 MPO• Mild to moderate to severe aphasia• Comprehension and/or expression deficits
– Partners• Primarily family members or usual partners
– Approaches• Partner change was goal• Facilitate desirable behavior or inhibit undesirable behavior
Turner & Whitworth , 2006; http://www.asha.org/members/reviews.aspx?id=7499
• Outcomes– Improved interaction
• More successful conversation turns• Fewer interruptions• Fewer turns devoted to repair
– Successful social validation– More accurate sense of partner’s aphasia– Maintenance and generalization of behavior
Turner & Whitworth, 2006
• Moderate (RCT) to limited (small studies) evidence supporting conversation and partner training
• Considerations– Individual personalities of PWAs and partners– Conversational style
Turner & Whitworth, 2006

Treatment techniques
• PACE and RET– Several studies investigating each treatment– Primarily positive results reported• Trained items• Untrained items• Generalization items
– No systematic review of the techniques• Single subject design studies

• Conversational Coaching and Reciprocal Scaffolding – Few studies investigating each treatment– Primarily positive results reported• Some generalization reported
– No systematic review of the technique• Single subject design studies

Summary
Moderate (small studies) or inconsistent (RCTs) support for group treatment.
Modest support for script training (multiple forms).
Modest support for communication partner training.
Modest support for PACE and RET.

TREATMENT INFLUENCES

Intensity and Dosage
• Theories supporting treatment intensity– Hebbian cell assemblies (Hebb, 1949)
– Education learning theory http://www.emtech.net/learning_theories.htm
– Neuronal plasticity (Kleim & Jones, 2008)
– Dosage (frequency, intensity, duration)
• Early aphasia treatment research (Darley, 1972)

ES for Outcome Measures for studies investigating intensity of treatment
Cherney, Patterson, Raymer, Frymark & Schooling, 2008; Frymark, Cherney, Patterson & Raymer, 2010
Errorless (Reduced Error) Learning• Theoretical foundation– Initially demonstrated in animal learning– Memory rehabilitation – Error behavior can be self-reinforcing > eliminate
• Contrast– Errorless learning• Error elimination• Error reduction
– Errorful learning (cueing hierarchy)• Errors not controlled

• Review of 27 studies• 91 outcome measures at three times– Immediate benefit = 78% yes; 25% no– Follow up benefit = 38% yes; 27% no– Generalization = 30% yes; 67% no
• Variations– Aphasia type and fluency– Therapy type (expressive, receptive, mixed, nonlangugae)– Technique (Errorful, error reducing, error elimination)
Fillingham, Hodgson, Sage & Lambon Ralph (2003)

Neuronal PlasticityPrinciples of experience-dependent neural plasticity
• Use it or lose it
• Use it and improve it
• Specificity
• Repetition matters
• Intensity matters
• Time matters
• Salience matters
• Age matters
• Transference
• Interference
Kleim & Jones, 2008; Raymer et al., 2008; Raymer, Maher, Patterson & Cherney, 2007

• Experience-dependent neuronal plasticity is the basis for learning and influences recovery– In the presence of treatment– Without treatment as one navigates the world
• Research aimed at translation of neuroscience to neurorehabilitation– Neuroimaging studies– Dosage– Application of principles individually and in combination
Summary
Greater intensity may be more effective than lesser intensity.Individual variation for aphasia type, TPO and task.
Errorless, reduced error and errorful treatment techniques are effective.
Individual variation for aphasia type, TPO and task.
Principles of neuronal plasticity positively influence treatment effectiveness.

EMERGING TREATMENTS

Emerging treatment techniques
• Pharmacotherapy• Computer-aided treatment• Repetitive Transcranial Magnetic Stimulation
(rTMS)• Transcranial Direct Current Stimulation (tDCS)• Epidural cortical stimulation

Pharmacotherapy
• Drugs investigated in RCTs– Piracetam • Weak evidence in support but concern for side effects
– Dextran – insufficient evidence
– Bifemelane - insufficient evidence
– Bromocriptine - insufficient evidence
– Idebenone - insufficient evidence
– Piribedil - insufficient evidence
Greener, Enderby & Whurr, 2010

• Additional studies of drugs therapy in aphasia– Piracetam – strong, positive evidence in favor (n=5)
– Bromocriptine – strong evidence against (n=4)
– Levodopa – moderate evidence in favor (n=1)
– Amphetamines – moderate evidence in favor (n=2)
– Bifemelane – insufficient evidence (n=1)
– Dextran – moderate evidence against (n=1)
– Moclobemide – insufficient evidence (n=1)
– Donepizil – moderate evidence in favor during active treatment (n=2)
– Memantine – moderate evidence in favor with CILT (n=1)
Salter, Teasell, Bhogal, Zettler & Foley, 2010

Computer-based Treatment
• Not so new but re-emerging technique– As primary treatment (Doesborgh, van de Sandt-Koenderman, Dippel, van
Ahrskamp, Koustall & Visch-Brink, 2004; Cherney, Halper, Holladn & Cole, 2008)
– Practice of skills learned in treatment– Telehealth
• Strong evidence in favor of improvement at impairment level
• Limited evidence for generalization functional communication
Salter, Teasell, Bhogal, Zettler & Foley, 2010
Cortical stimulation• Repetitive Transcranial Magnetic Stimulation (rTMS)
– How it works• Noninvasive; Cause depolarization of neurons • Place electrodes on scalp at regions of interest
– R perisylvian area or RH Broca’s area homologue
• Induces weak electric current in rapidly changing magnetic field• Facilitates neuronal activity
– Some evidence in favor • Patients with chronic nonfluent aphasia• Improvement in naming• Some improvement in spontaneous speech
Salter, Teasell, Bhogal, Zettler & Foley, 2010; Martin, Naeser, Ho, Doron, Kurland, Kaplan, Wang, Nicholas, Baker, Alonso, Fregni & Pascual-Leone, 2009
• Transcranial Direct Current Stimulation (tDCS)– How it works• Application of weak electrical currents (1-2 mA) to
modulate the activity of neurons • Polarity determines whether excitability is increased or
decreased
– Limited evidence in favor• Patients with chronic nonfluent aphasia• Improvement in naming
Salter, Teasell, Bhogal, Zettler & Foley, 2010; Baker, Rorden & Fridriksson, 2010

• Epidural Cortical Stimulation– How it works• Impulse generator implanted subclavicularly• Epidural electrode embedded over dura of target
cortical area• Neurons stimulated; perhaps to rewire themselves
– Limited evidence in favor when used with behavioral treatment• Chronic nonfluent aphasia
Cherney, 2009; Cherney & Small, 2007
Summary
Inconsistent evidence supporting pharmacological treatment.Some favorable evidence in conjunction with behavioral treatment.
Computer-based treatment effective at impairment level; inconsistent evidence for generalization.
Some indication that cortical stimulation in conjunction with behavioral treatment may improve naming.
Top Related