







Languages
Pages
Legal


DRUGS USED IN THE TREATMENT OF HYPERTENSION
IKE HUSENIKE HUSEN
Depart. Of Pharmacology & TherapyDepart. Of Pharmacology & Therapy
Faculty Of Medicine -Padjadjaran UniversityFaculty Of Medicine -Padjadjaran University
ANTIHYPERTENSIVE DRUGS Principles of blood pressure regulation:Principles of blood pressure regulation:
1.1. Blood pressure is regulated by the Blood pressure is regulated by the following :following :
a. cardiac outputa. cardiac output
b. Peripheral vascular resistanceb. Peripheral vascular resistance
c.Volume of intravascular fluid c.Volume of intravascular fluid (controlled at the kidney)(controlled at the kidney)

2. Baroreflexes adjust moment-to- moment 2. Baroreflexes adjust moment-to- moment
blood pressure:blood pressure: Carotid baroreceptors Carotid baroreceptors
3. Reduction in renal perfusion pressure3. Reduction in renal perfusion pressure

Major Factors Influencing Blood Pressure
ARTERIAL BLOOD PRESSURE
ARTERIAL BLOOD PRESSURE
PERIPHERALRESISTANCE
PERIPHERALRESISTANCE
CARDIAC OUTPUT
Heartrate
Contractility
Filling Pressure
BloodVolume
VenousTone
Arteriolar volume

ANTIHYPERTENSIVE DRUGS
1.1. DIURETICSDIURETICS
2.2. SYMPATHOLYTIC DRUGS SYMPATHOLYTIC DRUGS
3.3. VASODILATORSVASODILATORS
4.4. ACEACE INHIBITORS AND INHIBITORS AND
ANGIOTENSIN II RECEPTOR ANGIOTENSIN II RECEPTOR
ANTAGONISTS ANTAGONISTS
5.5. CALSIUM CHANNEL BLOCKERSCALSIUM CHANNEL BLOCKERS

1. DIURETICS
Mechanisms of ACTION & Mechanisms of ACTION & hemodynamic EFFECT :hemodynamic EFFECT :
- Depleting Na- Depleting Na+ + lead to BV lead to BV & & CO, PR CO, PR
may may . . - 6-8 weeks : CO normal ; PR - 6-8 weeks : CO normal ; PR

Figure 3.Actions of thiazide Diuretics
Decrease inBlood pressure
Thiazidediuretics
Thiazidediuretics
Cardiac OutputCardiac Output
Blood VolumeBlood Volume
Sodium, waterretention
Sodium, waterretention
Peripheralresistance
Peripheralresistance

PHARMACOLOGICAL EFFECT PHARMACOLOGICAL EFFECT DiureticsDiuretics::
Natriuretic (especially loop D.)Natriuretic (especially loop D.) KK+ + excretion (esp. excretion (esp.
acetazolamide; except Kacetazolamide; except K++--Sparing D.)Sparing D.)
CaCa++ ++ excretion (esp. loop D. ; excretion (esp. loop D. ; except Thiazide D.) except Thiazide D.)
Water excretion (esp. loop D.)Water excretion (esp. loop D.)

INDICATION : THIAZIDE DIURETICS : Mild or THIAZIDE DIURETICS : Mild or
moderate essential HT with normal moderate essential HT with normal renal & cardiac function.renal & cardiac function.
LOOP DIURETICS :LOOP DIURETICS :a.a. Severe HT when multiple drugs Severe HT when multiple drugs
with sodium-retaining properties with sodium-retaining properties are used, in combination therapy.are used, in combination therapy.
b.b. Sodium retention : GFR < Sodium retention : GFR < 30ml/mnt, cardiac failure, cirrhosis30ml/mnt, cardiac failure, cirrhosis
POTASSIUM-SPARING DIURETICS : POTASSIUM-SPARING DIURETICS : a.a. >< excessive potassium depletion>< excessive potassium depletionb.b. Natriuretic effects of other Natriuretic effects of other
diuretics diuretics

TOXICITY/ADVERSE REACTION : Hypokalemia (except for potassium-Hypokalemia (except for potassium-
sparing D.), precaution :sparing D.), precaution : a.a. Persons taking digitalisPersons taking digitalis b.b. Chronic arrhythmiasChronic arrhythmias c.c. AMI AMI
HypomagnesiaHypomagnesia Metabolic effect (especially at Metabolic effect (especially at dose): dose):
a.Glucose intolerancea.Glucose intolerance
b.Serum lipid b.Serum lipid c.Uric acid c.Uric acid , precipitate gout, precipitate gout

2. SYMPATHOLYTIC DRUGS2A. 2A. BLOCKERS BLOCKERS
DRUGS:Prazosin, terazosin, doxazosinDRUGS:Prazosin, terazosin, doxazosin
11 blocking agent: relaxation of arterial blocking agent: relaxation of arterial & &
venous smooth muscle PR and venous smooth muscle PR and arterial BP arterial BP
CO, RBF, GFR CO, RBF, GFR min. (tachycardia and min. (tachycardia and
increased renin release don not occur)increased renin release don not occur)

PHARMACOKINETICS & DOSAGE:
Plasma concentration prazosin Plasma concentration prazosin in in patient CHDpatient CHD
owing primarily to reduced 1owing primarily to reduced 1stst pass pass metabolismmetabolism T T 1/21/2 DOSAGEDOSAGE
PrazosinPrazosin 3-4 h3-4 h Dosis initial 1mg 3X sehari (*)Dosis initial 1mg 3X sehari (*)
Dosis dapat ditingkatkan 20-30mg/hDosis dapat ditingkatkan 20-30mg/h
TerazosinTerazosin 12 h12 h Umumnya: sehari sekali (5-20 mg/h)Umumnya: sehari sekali (5-20 mg/h)
DoxazosinDoxazosin 22 h22 h Sehari sekali, dosis initial 1mg/h (*)Sehari sekali, dosis initial 1mg/h (*)
Dosis dapat ditingkatkan sampai 4mg/h Dosis dapat ditingkatkan sampai 4mg/h atau lebih (prn)atau lebih (prn)
(prn): prorenata = bila perlu(*); untuk mencegah hipotensi postural, sinkop

SIDE EFFECT & TOXICITY
11 blockers causes postural blockers causes postural hypotension, and syncope after hypotension, and syncope after the 1the 1stst dose (1 dose (1stst pass effect) pass effect) the 1the 1stst dose should be small and dose should be small and should be administered at should be administered at bedtimebedtime
Other toxicities (rare): dizziness, Other toxicities (rare): dizziness, headache, palpitations, lethargyheadache, palpitations, lethargy

INDICATION :
Mild to moderate HT.Mild to moderate HT. In combination with In combination with
propranolol or a diuretic for propranolol or a diuretic for additive effect.additive effect.

Figure 4. Actions of -adrenoceptor blocking agents (- BLOCKERS)
Activation of B1 adrenoceptors
on heart
Activation of B1 adrenoceptors
on heart
Cardiacoutput
Cardiacoutput
Peripheral resistance
Peripheral resistance
Angiotensin IIAngiotensin IIReninRenin
Decrease inBlood pressure
AldosteronAldosteron
Sodium, water retention
Sodium, water retention
Blood volumeBlood volume
-Adrenoceptor blockers
-Adrenoceptor blockers
2B. Blockers

DRUGS:
Non selectiveNon selective: propranolol, : propranolol, nadolol, carteololnadolol, carteolol
11 blockers (cardioselective): blockers (cardioselective): atenolol, metoprolol (relative), atenolol, metoprolol (relative), betaxolol, bisoprololbetaxolol, bisoprolol
Partial agonist (Partial agonist (-blockers with -blockers with ISA):ISA): pindolol, acebutolol pindolol, acebutolol (cardioselective), penbutolol.(cardioselective), penbutolol.
-blockers with -blockers with -blocking -blocking effect: labetalol & carvediloleffect: labetalol & carvedilol

PHARMACOKINETICS & DOSAGE: Propranolol: Propranolol: Oral doses >> IV doses (1Oral doses >> IV doses (1stst-pass -pass
hepatic metabolic). T ½ 3-6 h.hepatic metabolic). T ½ 3-6 h. Dose started 80mg/d in divided Dose started 80mg/d in divided
doses. Effective antihypertensive doses. Effective antihypertensive dosage 80-480mg/d, once or twice dosage 80-480mg/d, once or twice daily.daily.
Measures of resting bradycardia and Measures of resting bradycardia and reduction in HR during exercise may reduction in HR during exercise may be used as guides in regulating be used as guides in regulating dosage.dosage.

INDICATION:
- HT with SV tachyarrhythmia, - HT with SV tachyarrhythmia, previous MI, A. pectoris, previous MI, A. pectoris, glaucoma, migraine headache.glaucoma, migraine headache.
- It more effective : young - It more effective : young patient > elderly.patient > elderly.

2C. CENTRALLY ACTING ADRENERGIC DRUGS
a.a. Clonidine (Clonidine (2 2 )) : Mild to : Mild to moderate HT (not responded to moderate HT (not responded to diuretic alone). diuretic alone). Half of drugs: eliminated Half of drugs: eliminated
unchanged in the urine patient unchanged in the urine patient with renal insuff. with renal insuff. DO DO
Toxicity: dry mouth and sedation Toxicity: dry mouth and sedation (frequent and may be severe) (frequent and may be severe)
CI: risk of mental depressionCI: risk of mental depression

b. Methyldopab. Methyldopa : PR : PR BP BP Do :1-2 g/d orally in Do :1-2 g/d orally in
divided/single dosesdivided/single doses Renal insuff. : reduced drug Renal insuff. : reduced drug
clearanceclearance Distribution: CNS (+)Distribution: CNS (+) Toxicity: sedation, drowsiness; Toxicity: sedation, drowsiness;
depression, Vertigo, lactation depression, Vertigo, lactation (included in men)(included in men)

3. VASODILATORS
Vasodilator:Vasodilator:
A.A. Hidralazine & minoxidil (p.o): Hidralazine & minoxidil (p.o):
long term outpatient Th/long term outpatient Th/
B.B. P.e : nitroprusside & diazoxide P.e : nitroprusside & diazoxide
Hypertensive Emergencies.Hypertensive Emergencies.
C.C. Calcium channel blockersCalcium channel blockers

Figure 5Figure 5MEKANISME KERJA
Arteriole relax Renin C
Vasc. Resistance & BP Na+ & water retention
blockers
Baroreflex:Ino & chronotropic (+)Oxygen consumption
Risk: A.pectoris, Mi, Cardiac failure (in predisposed individuals
3A1. Hydralazine
Dilates arteries and arteriole (not Dilates arteries and arteriole (not veins) veins)
PR and reflex PR and reflex HR & CO. HR & CO. Pharmacokinetics :Pharmacokinetics :
Bioavailability Bioavailability (25%) (25%) Metabolism : rapid & slow Metabolism : rapid & slow acetylatorsacetylators

Toxicity:Toxicity: headache, anorexia, headache, anorexia, palpitations, Sweating and palpitations, Sweating and flushing flushing
Usage:Usage: Th/ moderately severe Th/ moderately severe HT HT
It is almost always as It is almost always as combination combination
with a with a -blockers and diuretics -blockers and diuretics
((see figuresee figure 5: slide 22) 5: slide 22)

3A2. Minoxidil
Dilates arterioles (not venules)Dilates arterioles (not venules) Indication: severe to malignant Indication: severe to malignant
HT that is HT that is
refractory to other refractory to other drugs (p.o)drugs (p.o)

3B. HYPERTENSI EMERGENCY
Diastolic BP > 150 mmHg Diastolic BP > 150 mmHg (uncomplicated p.) or >130 (uncomplicated p.) or >130 mmHg with complications :mmHg with complications :
- Encephalopathy- Encephalopathy
- Cerebral hemorrhage- Cerebral hemorrhage
- Left ventricular failure- Left ventricular failure
- Aortic stenosis- Aortic stenosis Goal Th/ : rapidly reduce blood Goal Th/ : rapidly reduce blood
pressurepressure

3B1. Sodium Nitroprusside (IV)
Vasodilator (V&A) Vasodilator (V&A) reflex reflex tachycardia tachycardia
VR VR decomp. (-) decomp. (-)
COCO(slight)(slight)
or or change change
decomp. (+) CO decomp. (+) CO

PHARMACOKINETICS:
T ½ : in minutes continuous infusion.T ½ : in minutes continuous infusion.
(<1 hour)(<1 hour)
Nitroprusside Nitroprusside cyanide (*) cyanide (*) thiocyanatethiocyanate
(toxic) (toxic) (nontoxic)(nontoxic)
thiosulfatethiosulfate
urineurine
(*) : rhodenase (mithoch. Enzyme)(*) : rhodenase (mithoch. Enzyme)

SIDE EFFECT/TOXICITY:
Metabolite: may produce cyanide, but cyani- Metabolite: may produce cyanide, but cyani- de toxicity is rare. Th/: thiosulphat and rho-de toxicity is rare. Th/: thiosulphat and rho- danase to produce thiocyanate (less toxic and danase to produce thiocyanate (less toxic and eliminated by kidneys).eliminated by kidneys). Per oral: hydrolyzed to cyanide (!!!)Per oral: hydrolyzed to cyanide (!!!) Toxicity related to accumulation of cyanide :- Toxicity related to accumulation of cyanide :- - Metabolic acidosis- Metabolic acidosis
- - Arrhythmias Arrhythmias - - Excessive hypotensionExcessive hypotension - - Death.Death.

3B2. Diazoxide
Direct-acting arteriolar vasodilator. Direct-acting arteriolar vasodilator. Vascular effect Vascular effect hydralazine. hydralazine. For coronary insuff. patients : diazoxide IVFor coronary insuff. patients : diazoxide IV + + blocker (>< reflex activation of the heart). blocker (>< reflex activation of the heart). USAGE: USAGE: Th/ HT emergency, especially:Th/ HT emergency, especially:
- Malignant HT- Malignant HT- HT encephalopathy- HT encephalopathy- Eclampsia- Eclampsia
TOXICITY: TOXICITY: Excessive hypotension Excessive hypotension

3C. Calcium Channel Blockers
ACTION :ACTION :
- Inhibit Ca- Inhibit Ca++ ++ influx into vasc. smooth influx into vasc. smooth muscle muscle
cells cells tones & vasc. resistance tones & vasc. resistance BP BP (vasodilators) (vasodilators)
- Intrinsic natriuretic effect- Intrinsic natriuretic effect
-- Useful in HT with asthma, Useful in HT with asthma, diabetes, anginadiabetes, angina
and peripheral vascular diseaseand peripheral vascular disease

DRUGS :
A. Dihydropyridine family:A. Dihydropyridine family: - - NifedipineNifedipine - Isradipine - Isradipine - Nicardipine- Nicardipine - Nisoldipine - Nisoldipine - Amlodipine- Amlodipine - Felodipine - Felodipine - - Nimodipine (esp. cerebral Nimodipine (esp. cerebral
vasodilator)vasodilator)Pharmacological effect :Pharmacological effect : - Selective vasodilators - Selective vasodilators - - Cardiac depressant <<< verap./diltiaz.Cardiac depressant <<< verap./diltiaz. - - Reflex sympathetic activation: slight Reflex sympathetic activation: slight
tachycardia and slight increases COtachycardia and slight increases CO

B. Verapamil It has the greatest effect on the heart:It has the greatest effect on the heart: Slows cardiac cond. Slows cardiac cond. HR HR , balanced by , balanced by
reflex activation, NET EFFECT : reflex activation, NET EFFECT : moderate moderate
cardiac suppression (HR&CO cardiac suppression (HR&CO )) Contraindicated in patient with Contraindicated in patient with
preexisting depressed cardiac function preexisting depressed cardiac function or AV conduct. abnormalities !!!or AV conduct. abnormalities !!!
Weak vasodilatorWeak vasodilator
C. Diltiazem
It reduces HR (lesser than It reduces HR (lesser than verapamil), verapamil),
BP BP ..

SIDE EFFECT AND TOXICITY :
Excessive inhibition of CaExcessive inhibition of Ca++ ++ influx influx serious cardiac depression :serious cardiac depression :
- - Cardiac arrestCardiac arrest - - BradycardiaBradycardia
- - AV blockAV block - CHF- CHF
SIDE EFFECT :SIDE EFFECT :
- - FlushingFlushing - Headache - Headache
- - HypotentionHypotention - Peripheral - Peripheral edemaedema
- - ConstipationConstipation - Fatigue- Fatigue
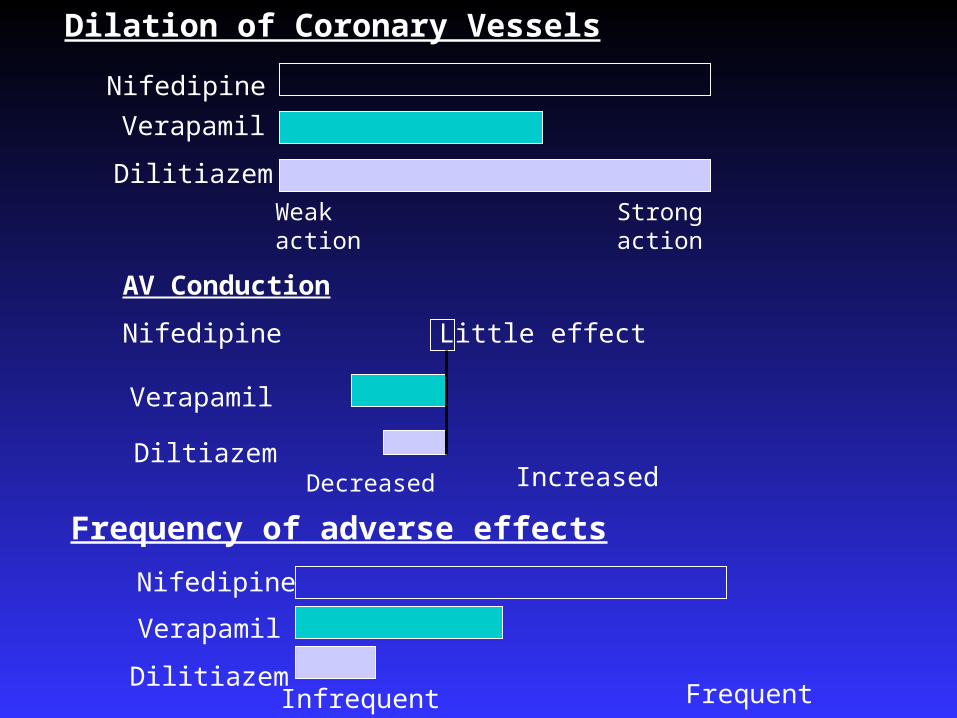
Dilation of Coronary Vessels
Nifedipine
Verapamil
Dilitiazem
Weakaction
Strong action
AV Conduction
Nifedipine
Verapamil
DiltiazemDecreased
Little effect
Increased
Frequency of adverse effects
Verapamil
Dilitiazem
Nifedipine
Infrequent Frequent

4. INHIBITORS OF ANGIOTENSIN
A. ACE-IBHIBITORA. ACE-IBHIBITOR
- - CaptoprilCaptopril - Fesinopril- Fesinopril
- - EnalaprilEnalapril - Moexipril- Moexipril
- - LisinoprilLisinopril - Quinopril- Quinopril
- - BenazeprilBenazepril - Ramipril - Ramipril (long (long
acting)acting)

B. ANGIOTENSIN RECEPTOR- BLOCKING AGENTS
B1. Angiotensin Type 1 (ATB1. Angiotensin Type 1 (AT11) Receptor) Receptor
Blocking AgentsBlocking Agents
- Losartan- Losartan
- Valsartan- Valsartan
B2. Analog and competitive Inhibitor B2. Analog and competitive Inhibitor ofof
Angiotensin II : SaralasinAngiotensin II : Saralasin

Fig. Page 16Fig. Page 16
Kininogen
Bradykinin
Vasodilation
VR
BP
inactive
Angiotensin I
Angiotensi II
Vasoconstriction Aldosteron
VR Na+, water retention
BP
* *
**
Hypertrophi &Remodeling cor & vasc.
*Site of ACE blockade (ACE inhibitor)**Site of receptor blockade (angiotensin-Receptor blocking agent

Figure. 6: Effects of ACE inhibitors
Angiotensinogen(2globulin in blood)
Angiotensin I(inactive)
Renin(from kidney)
Decreased angiotensin II
ACE
-
ACE Inhibitors
Output of sympathetic
nervous systemVasodilation of vascular smooth
muscle
Retention of sodium and water
Levels of bradykinin
Decreasedaldosterone production
Decreased blood pressure

4A. ACE INHIBITOR
Pharmacological effect:Pharmacological effect:Captopril:Captopril:
- - VRVR BP BP- - Aldosteron secretion Aldosteron secretion Na Na++ & &
water water retention retention & K & K++ retention retention
- - Bradikinin Bradikinin vasodilation vasodilation- - VasodilatorVasodilator preload preload COCO
EnalaprilEnalapril: bradykinin : bradykinin
Pharmacokinetics & dosage:
Bioavailability captopril p.o: 70% after Bioavailability captopril p.o: 70% after fasting, p.c.:fasting, p.c.: 30-40%, the antihypertensive 30-40%, the antihypertensive action un-affected. Lisinopril is slowly action un-affected. Lisinopril is slowly absorbed.absorbed.
Distribution: captopril: most body tissues, Distribution: captopril: most body tissues, except CNSexcept CNS
Do. : - captopril: 25mg, 2-3 times daily, Do. : - captopril: 25mg, 2-3 times daily, enalapril: 10-20mg once or twice daily, enalapril: 10-20mg once or twice daily, lisinopril: 10-80mg once daily.lisinopril: 10-80mg once daily.
All of ACE inhib. except fosinopril & All of ACE inhib. except fosinopril & moexipril are eliminated primarily by moexipril are eliminated primarily by kidney. kidney.

Toxicity/side effect:
- - Severe hypotension after initial Severe hypotension after initial dose (in dose (in hypovolemic due to hypovolemic due to diuretics, salt restric-diuretics, salt restric- tion, or GI fluid tion, or GI fluid loss)loss)
- - ARF (particularly in renal stenosis)ARF (particularly in renal stenosis) - - HyperkalemiaHyperkalemia - - Dry coughDry cough - - AngioedemaAngioedema - - Altered sense of tasteAltered sense of taste - - Allergic skin rashes, Drug feverAllergic skin rashes, Drug fever

Contraindication: Contraindication: 22ndnd and 3 and 3rdrd trimesters of pregnancytrimesters of pregnancy
Drug interaction:Drug interaction:
- - Potassium supp./pot.-sparing Potassium supp./pot.-sparing diureticsdiuretics
hyperkalemia hyperkalemia
- - NAIDS may impair the hypotensive NAIDS may impair the hypotensive
effect by blocking bradykinineffect by blocking bradykinin

USAGE:
- - Mild-moderate hypertension Mild-moderate hypertension - - Hypertension who were Hypertension who were
refractory to refractory to standard standard multidrug antihypertensive multidrug antihypertensive regimensregimens
- Hypertension with chronic - Hypertension with chronic congestive congestive heart failureheart failure

4B1. Angiotensin Type 1 (AT4B1. Angiotensin Type 1 (AT11) Receptor) Receptor Blocking Agents (Losartan and Blocking Agents (Losartan and
valsartan).valsartan). Effect on bradykinin metabolism Effect on bradykinin metabolism
(selective (selective blockers) blockers) Losartan: uricosuric effectLosartan: uricosuric effect
4B2. Analog and competitive Inhibitor 4B2. Analog and competitive Inhibitor ofof Angiotensin II : SaralasinAngiotensin II : Saralasin Antagonist and also weak agonist Antagonist and also weak agonist
AT IIAT II the effect: unpredictable the effect: unpredictable
Top Related