




Languages
Pages
Legal


An Analysis of the Demand for a Hemodialysis Facility in the
Kingfisher, Oklahoma, Medical Service Area
Oklahoma Cooperative Extension Service Rural Development
Oklahoma State University
Oklahoma Office of Rural Health Rural Health Policy & Research Center
Oklahoma State University
December 2008

AE-08123
An Analysis of the Demand for a Hemodialysis Facility in the Kingfisher, Oklahoma, Medical Service Area
Lara Brooks- Assistant State Extension Specialist, OSU, Stillwater 405-744-4857; FAX 405-744-9835
Fred C. Eilrich - Assistant State Extension Specialist, OSU, Stillwater
405-744-6083
Brian Whitacre - Extension Economist, OSU, Stillwater 405-744-9825
Stan Ralstin - District Rural Development Specialist, OSU, Enid
580-237-7677
Keith Boevers - Kingfisher County Extension Director, OSU, Kingfisher 405-375-3822
Val Schott - Director, Oklahoma Office of Rural Health, Oklahoma City
405-945-9197
Oklahoma Cooperative Extension Service Rural Development
Oklahoma State University
Oklahoma Office of Rural Health Rural Health Policy & Research Center
Oklahoma State University
December 2008

1
An Analysis of the Demand for a Hemodialysis Facility in the Kingfisher, Oklahoma, Medical Service Area
This report will examine the need for a hemodialysis facility in the Kingfisher, Oklahoma
medical service area. This report briefly describes the process decision makers can utilize to
help determine the demand for a hemodialysis facility. Specifically, the study will:
1. Determine the medical service area and population;
2. Estimate the number of potential patients in the medical service area; and
3. Estimate the number of dialysis stations for a hemodialysis facility in the medical
service area.
No recommendations will be made. The information included in this report is designed to assist
local decision-makers in assessing the need and potential for a hemodialysis facility.
Introduction
The need for hemodialysis (commonly referred to as kidney dialysis) treatment continues
to increase. The latest report by the American Diabetes Association (2008) shows that among
adults, diabetes (one of the leading contributors to kidney failure) increased in both men and
women and in all age groups, but still disproportionately affects the elderly. Over 23 percent of
the population 60 years and older had diabetes in 2007. The aging “Baby Boomer” population
continues to impact the need for hemodialysis treatments. Furthermore, race and ethnicity
remains an influential determinant in diabetes prevalence. After adjusting data from a 2004 -
2006 national survey for population age differences, the rate of diagnosed diabetes was highest
among American Indians and Alaska Natives (16.5 percent). This was followed by African
Americans (11.8 percent) and Hispanics (10.4 percent), which includes rates for Puerto Ricans

2
(12.6 percent), Mexican Americans (11.9 percent), and Cubans (8.2 percent). By comparison,
the rate for Asian Americans was 7.5 percent, with Whites at 6.6 percent.
With this increased need for treatment facilities, hospital administrators could be
considering the option of adding a kidney dialysis treatment unit to their current facilities or
community leaders might be exploring the possibilities of a center in their area. The Center for
Medicare and Medicaid (CMS) identify four types of dialysis facilities or units: 1) Renal
Transplantation Center; 2) Renal Dialysis Center; 3) Renal Dialysis facility (free-standing); and
4) Self Dialysis Unit. In the short term, a kidney dialysis unit will require a significant financial
investment. Over the longer term (3 years or more), a dialysis unit could provide a much needed
service to the residents and a cost effective service for the hospital or the community.
Rural hospitals, in particular, are looking for cost effective or “profit generating” medical
services that will fill the need in the community as well as assist with the financial stability of the
hospital. Rural leaders, including hospital administrators, will need to take a serious look at the
potential market for dialysis patients; the most critical criteria for success of a center being
patient participation.
Hemodialysis units provide medical treatment for end-stage renal disease (ESRD) caused
primarily by the chronic diseases of diabetes and/or hypertension (high blood pressure). The
need for hemodialysis units is increasing as people live longer and more people develop the
diseases that lead to kidney (renal) failure. Also, improvements in dialysis technologies, care,
and related drugs enable dialysis patients to live longer on dialysis. The increased number of
patients requiring hemodialysis has placed an increased demand on urban and rural communities
to provide hemodialysis units that are within a one-hour drive to the patient’s home. According
to the 2008 USRDS Annual Data Report, the number of dialysis units nationwide grew 21.1

3
percent between 2001 and 2005. Nearly 63 percent of patients were treated in units owned by
one of the four largest dialysis organizations. In 2006, hospital-based and independently owned
units accounted for 11.4 percent and 18.8 percent, respectively.
Rural hemodialysis units provide the patient with needed services that are easily
accessible with minimal travel time. Preferably a family member or a friend drives the
hemodialysis patient to and from the treatment facility, especially if the facility is a significant
distance from the patient’s residence. However it is not uncommon for the patient to transport
him/herself because treatments are so frequent. If the patient is driven, the driver waits at the
facility while the patient receives treatment (which takes approximately 4-5 hours) then drives
the patient home. In instances of bad weather, the travel to and from the treatment unit may take
more time and be more stressful to both the patient and/or the driver. For the patient who needs
hemodialysis yet does not live within easy commuting distance of a treatment unit, the only
option may be to move to a community that has a unit. This means the patient may incur
additional expense in relocating and may no longer have a social support system available to
him/her in the local community. It also adds to current problem of decreasing population
numbers experienced by numerous rural communities.
The information provided in this study is a starting point for the hospital administrator
and board members to use in determining whether their community can support this medical
service. Several national and local providers of dialysis services are available to partner with
local communities, hospitals, physicians, and investors to develop and operate a dialysis facility.
A hemodialysis facility can enter into a management contract or joint venture
arrangement with many of the regional or national corporations involved in the business of
providing hemodialysis services. The management contract could provide the facility with 1)

4
consultation services from a clinical nutritionist and a social worker; 2) in-service training
programs for staff; 3) computer programs for clinical documentation of services, billing and
collections, and laboratory work; 4) purchasing or leasing capacity for equipment; 5) purchasing
capacity for expendable supplies; and 6) quality assurance procedures for documentation to
CMS. Purchasing equipment and supplies as part of a corporate group would enable the center
to obtain these items at less cost. Corporate groups also have the capacity of doing their own
market feasibility study. Under a joint venture arrangement, the corporate partner also shares in
development expenses, capital expenditures, start-up and ongoing working capital requirements,
and operating expenses.
The End Stage Renal Disease (ESRD) Program was established in 1972 by federal
legislation that extended Medicare coverage to almost all individuals with ESRD who require
either dialysis or transplantation to sustain life. There are currently eighteen ESRD Networks
who provide information on the Medicare-approved hemodialysis and transplant centers
functioning in their region (ESRD Networks, 2008). The United States Renal Data System
(USRDS) is a national data system that collects, analyzes, and distributes information about
ESRD from the ESRD Networks. The USRDS defines dialysis patients as either prevalent or
incident. A prevalent patient is a patient currently receiving renal replacement therapy or having
a functioning kidney transplant (regardless of when the transplant was performed), or the number
of people on hemodialysis at a given time. An incident patient is a patient starting renal
replacement therapy for end stage renal disease during the calendar year or the new patients
starting hemodialysis during a calendar year. Both definitions (prevalence or incidence) exclude
persons with acute renal failure, persons with chronic renal failure who die before receiving
treatment for ESRD, and persons whose ESRD treatments are not reported through CMS. Data

5
on prevalent and incident patients is available at the national, state, and county level from the
USRDS website (www.usrds.org) from the Renal Data and Extraction Reference (RenDER)
database.
Total Medicare expenditures for end-stage renal disease patients increased almost six
percent from the previous year. Total expenditures reached $22.7 billion in 2006 or 6.7 percent
of the Medicare budget (USRDS 2008 Annual Data Report). Medicare begins to pay for
hemodialysis after the patient has been receiving treatments for 90 days. If the patient has health
care coverage, it will pay for treatments for the period of time identified in the policy, and then
the patient will apply for Medicare. If the patient does not have any other coverage and is unable
to pay for treatment, the hemodialysis facility absorbs the cost for three months until the patient
qualifies for Medicare. Most new patients on hemodialysis do not have any other health care
coverage.
The total number of reported patients receiving ESRD therapy on December 31, 2006
was 506,256; a 2.3 percent increase over the previous year. Among the prevalent patients,
327,754 or nearly 65 percent were undergoing dialysis. There was a 3.4 percent increase in new
patients (110,854) in 2006. The racial and ethnic disparities in ESRD persist, with 2006 rates in
African American and Native American populations being 3.6 and 1.8 times greater than the rate
among Whites; and the rate in the Hispanic population being 1.5 times greater than rates for non-
Hispanics.
Medical Service Area
Estimating potential patient participation in a hemodialysis unit requires defining the
service area for the unit, identifying the population of the service area and calculating the
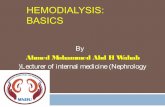
prevalence and incidence rates for different age and racial groups. Figure 1 shows the proposed

6
medical service area with the surrounding hemodialysis facilities according to the latest
Oklahoma Medical Facilities Directory (April, 2008) obtained from the Oklahoma State
Department of Health website (www.health.ok.us). The proposed service area for the Kingfisher
hemodialysis facility is derived by considering the relative travel distances to the alternative
centers. The proposed medical service area includes all of the zip codes shown in Table 1.
Table 1 presents the 2000 census estimates and 2000 estimates from ESRI (a different data
source) for comparison purposes. Zip code delineations are arbitrary and change frequently
resulting in slight differences between the two estimates. Zip Code data is not available from the
U.S. Census for 2007. Therefore, population from the 2007 ESRI estimates will be utilized in
estimating number of patients and stations. The 2007 ESRI estimated population of the medical
service area is 46,724. The largest zip code population in the medical service area is Guthrie’s
zip code 73044 with 20,294 people. Watonga’s zip code 73772 is the second largest zip code
area with 6,698. Kingfisher’s zip code 73750 closely follows with a population of 6,298. The
total population by race and age for the proposed service area is given in Table 2 and Table 3,
respectively.
Table 4 presents the total prevalence data for the state and the three counties included in
the service area (Blaine, Kingfisher, and Logan). Data is also presented by race and age for the
state of Oklahoma. For confidentiality reasons, data is not available by race and age for the three
counties represented.

7
Kingfisher Area Dialysis Center
SOURCE: Oklahoma State Department of Health Location of Existing Hemodialysis Units 1. Morning Star Dialysis Center Northwest Bethany Dialysis Center 2. Edmond Dialysis Center 3. El Reno Regional Dialysis Center 4. Renal Care Group - Enid 5. FMC Dialysis Services Heritage Park Midwest City Dialysis 6. BMA of Oklahoma City at St. Anthony's Hospital Choice One Renal Care of Oklahoma, LLC Cinema Dialysis St. Anthony Hospital - Transplant Unit
6. (Cont.) Fresenius Medical Care North Central - Oklahoma City Fresenius Medical Care of Southwest - Oklahoma City Medical Plaza Dialysis Oklahoma City Dialysis Center Oklahoma City South Dialysis OU Medical Center - ESRD OU Medical Center - Transplant Unit South Oklahoma City Dialysis Center

8
Table 1 Population of Proposed Service Area
Zip Code Area 2000 Census 2000 ESRI 2007 ESRI
73016 Cashion 1,367 588 640
73028 Crescent 3,199 3,209 3,477
73043 Greenfield 165 185 177
73044 Guthrie 18,391 18,538 20,294
73056 Marshall 436 403 417
73063 Mulhall 685 498 501
73734 Dover 981 585 618
73742 Hennessey 3,617 4,138 4,261
73744 Hitchcock 378 242 232
73750 Kingfisher 6,551 6,663 6,928
73756 Loyal 289 136 140
73762 Okarche 1,966 1,950 2,025
73764 Omega 182 45 46
73772 Watonga 5,992 6,139 6,968
TOTAL 44,199 43,319 46,724
SOURCE: U.S. Census Bureau, 2000 Census Data, ESRI 2007 Community Sourcebook of Zip Code Demographics, 21st ed., ESRI Business Solutions

9
Table 2 Population by Race for Proposed Service Area
Age Census 2000 ESRI 2000 % of Total
ESRI 2007 % of Total
White 36,741 35,828 82.7 38,560 82.5 A. American 3,129 3,142 7.3 3,457 7.4 N. American 2,663 2,644 6.1 2,876 6.2 Other 1,666 1,695 3.9 1,831 3.9 Total 44,199 43,319 46,724
SOURCE: U.S. Census Bureau, 2000 Census Data, ESRI 2007 Community Sourcebook of Zip Code Demographics, 21st ed., ESRI Business Solutions
Table 3 Population by Age for Proposed Service Area
Age Census 2000 ESRI 2000 % of Total
ESRI 2007 % of Total
0-19 12,679 12,395 28.6 13,352 28.6 20-44 14,859 14,604 33.8 15,793 33.8 45-64 10,087 9,871 22.8 10,637 22.8 65-74 3,394 3,325 7.7 3,581 7.7 75+ 3,162 3,123 7.2 3,361 7.2 Total 44,199 43,319 46,724
SOURCE: U.S. Census Bureau, 2000 Census Data, ESRI 2007 Community Sourcebook of Zip Code Demographics, 21st ed., ESRI Business Solutions

10
Table 4 Prevalence1 of Hemodialysis Patients for the State of Oklahoma
and Blaine, Kingfisher, and Logan Counties
2004 2005 2006
Total State of Oklahoma 3,135 3,179 3,291
Blaine County 12 * * Kingfisher County 12 12 10* Logan County 16 18 15
Race (Oklahoma) White 1,733 1,751 1,858 African American 766 773 778 Native American 564 581 583 Other 72 74 66 Age (Oklahoma) 0-19 11 16 16 20-44 493 493 490 45-64 1,272 1,358 1,413 65-74 757 727 759 75+ 602 585 613
SOURCE: The data reported here have been supplied by the United States Renal Data System (USRDS). The interpretation and reporting of these data are the responsibility of the author(s) and in no way should be seen as an official policy or interpretation of the U.S. Government.
1Prevalent patient - A patient receiving renal replacement therapy or having a functioning kidney transplant (regardless of when the transplant was performed.) *If less than 10 patients, data is not reported; number included in total count for all years. The numbers have been supplied based upon secondary data from RenDER.

11
Table 5 Incidence1 of Hemodialysis Patients for the State of Oklahoma
and Blaine, Kingfisher, and Logan Counties
2004 2005 2006
Total State of Oklahoma 1,059 1,040 1,075
Blaine County * * *
Kingfisher County * * *
Logan County * * *
Race (Oklahoma) White 703 692 720 African American 177 171 785 Native American 161 166 158 Other 18* 11* 12* Age 0-19 3* 5* 3 20-44 116 133 116 45-64 415 400 410 65-74 270 257 285 75+ 255 245 261
SOURCE: The data reported here have been supplied by the United States Renal Data System (USRDS). The interpretation and reporting of these data are the responsibility of the author(s) and in no way should be seen as an official policy or interpretation of the U.S. Government.
1Incident patient - A patient starting renal replacement therapy for end-stage renal disease during the calendar year. *If less than 10 patients, data is not reported; number included in total count for all years. The numbers have been supplied based upon secondary data from RenDER.

12
Estimating Patient Participation
The number of patients receiving hemodialysis changes during the year due to deaths of
existing patients and the addition of new patients. Estimating potential patient participation in a
hemodialysis facility requires calculating the prevalence and incidence rates for different age and
racial groups. Coefficients have been calculated for Oklahoma that indicates the number of
hemodialysis patients per 100,000 population for both prevalence and incidence. The
coefficients are the latest available based on the 2006 data from the RenDER database. The
number of projected hemodialysis patients is estimated by multiplying these coefficients with a
service area’s population.
The coefficients allow for prediction of patients by three methods: (1) population by race;
(2) population by age; and (3) total population. The prevalence coefficients calculate the number
of current hemodialysis patients. Table 6 shows the coefficient for each of the three methods,
along with prevalent predictions by race, age, and total population for the Kingfisher proposed
medical service area.
The incidence coefficients for age, race, or total population are used to calculate the
number of new patients (rounded to the nearest person) that will receive treatment without
Medicare reimbursement for the first three months. Table 7 shows these coefficients the
incidence predictions by race, age, and total population for the Kingfisher proposed medical
service area. Again, these coefficients are based on the latest available information. Populations
are taken from 2007 ESRI zip code data.
For the proposed service area, the number of prevalent patients is estimated to be
between 41.6 and 43.5 and for incidence patients between 13.9 and 14.4. The estimated number
of dialysis stations will be based on 43 prevalent patients and 14 incident patients for an

13
estimated total of 57 hemodialysis patients.
Table 6 Estimated Number of Current (Prevalent) Hemodialysis Patients
for the Proposed Service Area
SOURCE: U.S. Census Bureau, 2006 Census Data, United States Renal System Renal Data Extraction and Reference (RenDER)
1Coefficients based on 2006 Census estimated population and 2006 RenDER data represent number of prevalence hemodialysis patients per 100,000 population. The data reported here have been supplied by the United States Renal Data System (USRDS). The interpretation and reporting of these data are the responsibility of the author(s) and in no way should be seen as an official policy or interpretation of the U.S. Government.
2007 ESRI Population Coefficients1 Estimated Current Patients
Race White 38,560 66.3 25.6 African American 3,457 279.0 9.6 Native American 2,876 202.6 5.8 Other 1,831 31.6 0.6 Total 46,724 41.6 Age 0-19 13,352 1.6 0.2 20-44 15,793 40.0 6.3 45-64 10,637 158.8 16.9 65-74 3,581 308.5 11.0 75+ 3,361 269.5 9.1 Total 46,724 43.5 Total Population Service Area 46,724 91.9 42.9

14
Table 7 Estimated Number of New (Incident) Hemodialysis Patients
for the Proposed Service Area
2007 ESRI Population Coefficients1 Estimated Current Patients
Race White 38,560 25.7 9.9 African American 3,457 66.3 2.3 Native American 2,876 54.9 1.6 Other 1,831 5.7 0.1 Total 46,724 13.9 Age 0-19 13,352 0.3 0.0 20-44 15,793 9.5 1.5 45-64 10,637 46.1 4.9 65-74 3,581 115.8 4.1 75+ 3,361 114.7 3.9 Total 46,724 14.4 Total Population Service Area 46,724 30.0 14.0
SOURCE: U.S. Census Bureau, 2006 Census Data, United States Renal System Renal Data Extraction and Reference (RenDER) 1Coefficients based on 2006 Census estimated population and 2006 RenDER data represent the number of new (incident) hemodialysis patients per 100,000 population. The data reported here have been supplied by the United States Renal Data System (USRDS). The interpretation and reporting of these data are the responsibility of the author(s) and in no way should be seen as an official policy or interpretation of the U.S. Government.

15
Estimating Number of Dialysis Stations
Table 8 estimates the number of stations, annual treatments, and potential maximum
expansion for the proposed service area. Each of the options presents variations in the number of
stations and staffing levels. The total cost per station decreases as the number of stations
increase. However, due to the significant capital investment, decision makers will have to
investigate the best alternative mix of stations and staffing. This report presents several
alternatives that can be considered to provide the necessary treatments for the proposed medical
service area. The alternatives range from a three day per week treatment option with two
treatments per day to six days per week with three daily treatments. The first column presented
allows for 2 daily treatments three days a week. This would require a total of 29 stations to meet
the demand of the 57 estimated patients, resulting in total annual treatments of 8,892. This
scenario would allow for expansion to 58 patients with current staffing for the 15 stations. The
numbers at the bottom of the table represent the maximum capacity for 29 stations if staffing
allowed for three daily treatments, six days a week. The maximum expansion capacity would be
174 patients or 27,144 annual treatments. Three other options for staffing versus number of
stations are provided. To determine the best solution for the number of stations in a
hemodialysis unit, local decision makers will need to consider the capital investment of
equipment and building space for additional stations versus the annual operating cost for the
additional staffing needed to provide services for more patients with fewer stations.

16
Table 8 Estimating Number of Stations and Annual Treatments
for the Proposed Service Area
3-day
week
2 x/day
3-day week
3 x/day
6-day week 3&1 x/day
6-day week
3 x/day
Number of Stations
A. Number of new patients estimated from coefficients 43 43 43 43B. Expected number of new patients estimated from coefficients 14 14 14 14C. Total estimated number of patients (A + B) 57 57 57 57
D. Number of daily treatments per M.W.F. rotation per station 2 3 3 3E. Number of daily treatments per T.Th.Sat. rotation per station 0 0 1 3F. Total Number of daily treatments for all rotations (D + E) 2 3 4 6
G. Number of stations required (C/F) 28.5 19.0 14.3 9.5H. Actual number of stations (round up to whole number) 29.0 19.0 15.0 10.0
Number of annual treatments I. Number of annual treatments from prevalent patients (A x 3 x 52) 6,708 6,708 6,708 6,708
J. Number of annual treatments from new patients (B x 3 x 52) 2,184 2,184 2,184 2,184
K. Total number of annual treatments (I + J) 8,892 8,892 8,892 8,892
L. Maximum number of patients based on current staffing (H x F) 58 57 60 60 M. Maximum number of annual treatments based on current staffing (L x 3 x 52) 9,048 8,892 9,360 9,360
Maximum Capacity based on number of Stations w/ 6-day week, 3X/day Actual Number of Stations 29 19 15 10 Total Patients 174 114 90 60 Total Annual Treatments 27,144 17,784 14,040 9,360

17
Estimating Patients Participation and Stations without the 73044, Guthrie, OK, Zip Code
This section utilizes the same methodology that was used in the previous sections to
determine the number of patients and number of stations required to service those patients, but
does not include the 73044 zip code (Guthrie) in the proposed service area. In the previous
sections, Guthrie was included since there is not a kidney dialysis facility available locally. The
nearest facilities would be Kingfisher, Stillwater, or Edmond. It is feasible that some Guthrie
residents will travel to Kingfisher to receive treatment. However, it is just as likely that these
residents will go to Stillwater or Edmond. The purpose of this section is to perform a
“sensitivity analysis” on including Guthrie in the proposed service area. Since the 73044 zip
code encompasses such a large population, it would be beneficial to estimate patient
participation without including Guthrie in the Kingfisher service area. According to Table 1,
ESRI estimates the 73044 zip code to be 20,294 in 2007 effectively giving a lower bound of
expected participants. The total population of the service area according to ESRI’s 2007
estimates would be 26,430. This will also lower the values for the race and age sections.
Table 9 displays the estimated number of prevalent hemodialysis patients. The same
three methods were utilized when determining patient participation, age, race, and total
population. All three methods suggest 22-25 prevalent patients for the Kingfisher service area
without the 73044 zip code.
Table 10 displays the estimated number of incidence hemodialysis patients. Again, the
same methods from the previous sections were utilized. All three methods suggest
approximately 8 incident patients in the new Kingfisher service area.

18
Table 9
Estimated Number of Current (Prevalent) Hemodialysis Patients for the Proposed Service Area
2007 ESRI Population Coefficients1 Estimated Current Patients
Race White 21,891 66.3 14.5 African American 1,337 279.0 3.7 Native American 1,782 202.6 3.6 Other 1,420 31.6 0.4 Total 26,430 22.3 Age 0-19 7,448 1.6 0.1 20-44 9,121 40.0 3.6 45-64 5,812 158.8 9.2 65-74 2,057 308.5 6.3 75+ 1,992 269.5 5.4 Total 26,430 24.7 Total Population Service Area 26,430 91.9 24.3 SOURCE: U.S. Census Bureau, 2006 Census Data, United States Renal System Renal Data Extraction and Reference (RenDER) 1Coefficients based on 2006 Census estimated population and 2006 RenDER data represent number of prevalence hemodialysis patients per 100,000 population. The data reported here have been supplied by the United States Renal Data System (USRDS). The interpretation and reporting of these data are the responsibility of the author(s) and in no way should be seen as an official policy or interpretation of the U.S. Government.

19
Table 10 Estimated Number of New (Incident) Hemodialysis Patients
for the Proposed Service Area
2007 ESRI Population Coefficients1 Estimated Current Patients
Race White 21,891 25.7 5.6 African American 1,337 66.3 0.9 Native American 1,782 54.9 1.0 Other 1,420 5.7 0.1Total 26,430 7.6Age 0-19 7,448 0.3 0.0 20-44 9,121 9.5 0.9 45-64 5,812 46.1 2.7 65-74 2,057 115.8 2.4 75+ 1,992 114.7 2.3Total 26,430 8.2Total Population Service Area 26,430 30.0 7.9 SOURCE: U.S. Census Bureau, 2006 Census Data, United States Renal System Renal Data Extraction and Reference (RenDER) 1Coefficients based on 2006 Census estimated population and 2006 RenDER data represent the number of new (incident) hemodialysis patients per 100,000 population. The data reported here have been supplied by the United States Renal Data System (USRDS). The interpretation and reporting of these data are the responsibility of the author(s) and in no way should be seen as an official policy or interpretation of the U.S. Government.

20
Table 11 explores the number of stations needed to service the new number of prevalent
and incidence patients from the new Kingfisher service area. After adding the number of
prevalent and incidence patients, there is a new total of 32 total patients with a total of 4,992
annual treatments. The days and schedules remained the same from the previous section. As
expected, the smaller population of the new service area reduces the amount of stations required.
For example, for a 6-day week operating 3 times per day, 6 stations are now required (as
opposed to 10 under the original population assumptions).
Table 11 Estimating Number of Stations and Annual Treatments
for the Proposed Service Area 3-day
week
2 x/day
3-day week
3 x/day
6-day week 3&1 x/day
6-day week
3 x/day
Number of Stations
A. Number of new patients estimated from coefficients 24 24 24 24B. Expected number of new patients estimated from coefficients 8 8 8 8C. Total estimated number of patients (A + B) 32 32 32 32
D. Number of daily treatments per M.W.F. rotation per station 2 3 3 3E. Number of daily treatments per T.Th.Sat. rotation per station 0 0 1 3F. Total Number of daily treatments for all rotations (D + E) 2 3 4 6
G. Number of stations required (C/F) 16.0 10.7 8.0 5.3 H. Actual number of stations (round up to whole number) 16.0 11.0 8.0 6.0
Number of annual treatments I. Number of annual treatments from prevalent patients (A x 3 x 52) 3,744 3,744 3,744 3,744
J. Number of annual treatments from new patients (B x 3 x 52) 1,248 1,248 1,248 1,248
K. Total number of annual treatments (I + J) 4,992 4,992 4,992 4,992
L. Maximum number of patients based on current staffing (H x F) 32 33 32 36 M. Maximum number of annual treatments based on current staffing (L x 3 x 52) 4,992 5,148 4,992 5,616

21
Summary Many assumptions have been made in the preceding analysis. These include items that may
change such as the population of the service area or service area delineation. For example, the
service area depicted here may change due to the exit or entry of dialysis facilities. Should this
occur, revised estimates of hemodialysis patients and stations should be made.
All assumptions should be closely examined by local decision-makers to verify that they
reflect local conditions. Local data should be included when available. If further analysis is needed,
please contact the authors on the cover page or your county extension office listed on the cover page
of this document.

22
References
American Diabetes Association, Diabetes 4-1-1 Facts, Figures and Statistics at a Glance, www.diabetes.org.
ESRI 2007 Community Sourcebook of Zip Code Demographics, 21st ed., ESRI Business
Solutions.
Lawler, MK, & Doeksen, GA. (2002). Guidebook Estimating the Economic Viability of a Hemodialysis Center. Stillwater, OK: Oklahoma State University.
United States Renal Data System. USRDS 2008 Annual Data Report: Atlas of End Stage Renal Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD. 2008.
United States Renal Data System. www.usrds.org (accessed October 2008).
Top Related