







Languages
Pages
Legal


All children should be switched to dolutegravir-based ART
regimens: CONNandita Sugandhi M.D.
ICAP at Columbia University

We need better ARVs for children
Poor virologic suppression in children
Jonnalagadda, et al. Children living with HIV in Malawi: Results from the Malawi Population-based HIV Impact Assessment 2016, IAS 2017, #TUAC0304
Resistance in ART naive children < 18 months2012-2016 (national surveys: Mozambique, Swaziland, Uganda, Zimbabwe, South Africa)
Moz=Mozambique; SWZ=Swaziland UGA=Uganda; ZAF=South Africa; ZIM=Zimbabwe; EFV=efavirenz; NVP=nevirapin; ETR=etravirine; RPV=rilpivirine; AZT=zidovudine; d4t=stavudine; FTC=emtricitabine; TDF=tenofovir
Jordan MR et al. CID 2017
WHO Guidelines
on the public health response
to pretreatment HIVDR
Prevalence of NNRTI pre-
treatment resistance
by calendar year
Countries with national pretreatment
HIV drug resistance to EFV or NVP
greater than or equal to 10% should
consider a rapid transition to DTG
Pre Treatment drug resistance is increasing

Dolutegravir is taking over fast
As of November 2017

What do we need to know before we switch all children to DTG-containing regimens?
Can we dose across all weight bands?
Do we have the right formulations?
Is it safe?
Can we switch existing patients?
What do we know about resistance?
Is this going to solve adherence issues?

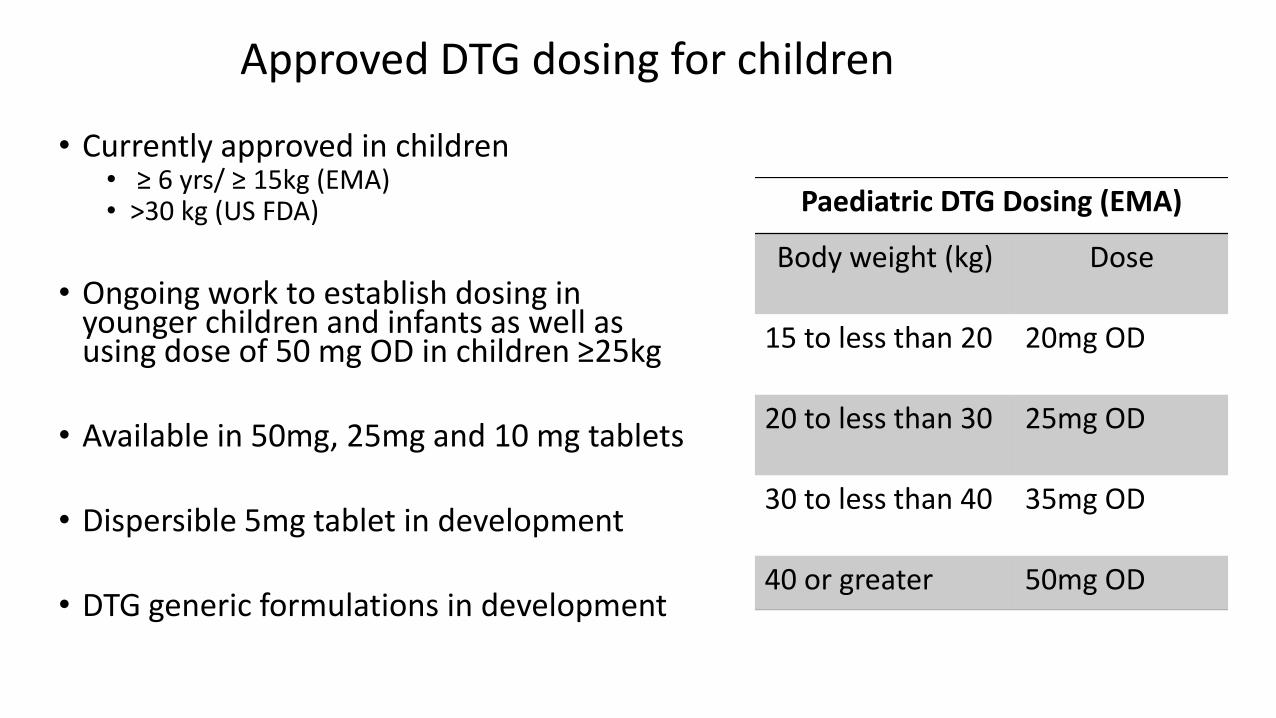
Approved DTG dosing for children
• Currently approved in children• ≥ 6 yrs/ ≥ 15kg (EMA) • >30 kg (US FDA)
• Ongoing work to establish dosing in younger children and infants as well as using dose of 50 mg OD in children ≥25kg
• Available in 50mg, 25mg and 10 mg tablets
• Dispersible 5mg tablet in development
• DTG generic formulations in development
Paediatric DTG Dosing (EMA)
Body weight (kg) Dose
15 to less than 20 20mg OD
20 to less than 30 25mg OD
30 to less than 40 35mg OD
40 or greater 50mg OD

Weight band dosing for DTG
30- <40kg ≥ 40kg
35 mg 50 mg
3.0-5.9 kg 6.0-9.9 kg 10.0-13.9 kg 14.0-19.9 kg 20.0-24.9 kg 25.0-34.9 kg ≥ 35 kg
- - - - - -TLD
(50mg)
15- <20kg 20- <30kg 30- <40kg ≥ 40kg
20 mg 25 mg 35 mg 50 mg
WHO weight bands
EMA DTG dosing
FDA DTG dosing

Weight band dosing for DTG
30- <40kg ≥ 40kg
35 mg 50 mg
3.0-5.9 kg 6.0-9.9 kg 10.0-13.9 kg 14.0-19.9 kg 20.0-24.9 kg 25.0-34.9 kg ≥ 35 kg
- - - - - -TLD
(50mg)
15- <20kg 20- <30kg 30- <40kg ≥ 40kg
20 mg 25 mg 35 mg 50 mg
WHO weight bands
EMA DTG dosing
FDA DTG dosing
50mg

P1093: Dolutegravir (DTG) in 6-12 Year Olds 48 Week Data
▪ Stage 1: intensive PK in 11 children
‒ Median age (range) was 10 yrs (6, 11)
‒ Median weight (range) was 30.0 kg (18, 54)
▪ Stage 2: safety and efficacy in 21 children
‒ HIV RNA < 50 c/mL was achieved in 74%
▪ The EMA approved DTG dosing for ≥ 6 years and
weighing ≥ 15 kg based on population PK modeling
and simulation analyses
▪ Because the available PK data in these weight bands
were minimal and the observed Ctrough
concentrations were lower than expected, the FDA did
not approve dosing for children weighing <30 kg
Wiznia A et al. CROI 2016 Boston Abs 816
PK Results, 6-12 Year Cohort
(chosen dose ~1 mg/kg)
Virologic Efficacy: % VL <400
VL <50: 74% at 48 wks

• Enrolled 10 HIV+ children age 2-<6 years in PK study of DTG granules for suspension.
Dolutegravir PK in HIV-Infected Children Age 2-<6 YrsRuel T et al. CROI 2017, Seattle, WA. Poster 806
▪ DTG granules-in-suspension at
dose ~0.8 mg/kg once daily
achieved the target AUC24h.
▪ HIV-1 RNA levels were <400
copies/mL in 8 out of 10
participants at 4 weeks of
treatment.
▪ The manufacturer of dolutegravir
does not plan to produce the oral
pediatric granule formulation
LBPEN023
TITLE
Pharmacokinetic and 4-week safety/efficacy of dolutegravir (S/GSK 1349572) dispersible tablets in HIV-infected children aged 4 weeks to < 6 years: Results from IMPAACT P1093
PRESENTERCindy Brothers
AUTHORST Ruel1, E Acosta2, R Singh3, C Alvero4, K George5, S Popson5,E Townley6, R Hazra7, C Brothers3, C Vavro3, A Buchanan3, A Wiznia8, IMPAACT P1093 Team
Coming soon to a conference center near you!

What do we need to know before we switch all children to DTG-containing regimens?
Can we dose across all weight bands?
Do we have the right formulations?
Is it safe?
Can we switch existing patients?
What do we know about resistance?
Is this going to solve adherence issues?
✗
✗
Let’s check back on Tuesday
Not yet
Tsepamo Study: Preliminary Analysis May 2018
• Additional data on birth outcomes in 11,558 HIV positive women starting ART before conception:• 4 neural tube defects amongst 426 women started on DTG
prior to conception (0.9%)• 14 neural tube defects amongst 11,173 women taking other
ARVs (0.1%)
Unless it is established that early exposure to DTG does not significantly increase the risk of birth defects, current guidance is to be cautious when using TLD in women of childbearing age who may
become pregnant

Adolescent birth rate (per 1000 women age 15-19 years), 2009-2016
Uganda: 141 births/1000 in adolescents 15-19 years

Is this where the adolescent girls will go to switch off DTG?

What do we need to know before we switch all children to DTG-containing regimens?
Can we dose across all weight bands?
Do we have the right formulations?
Is it safe?
Can we switch existing patients?
What do we know about resistance?
Is this going to solve adherence issues?
✗
✗
We’re not really sure✗
Let’s check back on Tuesday
Not yet
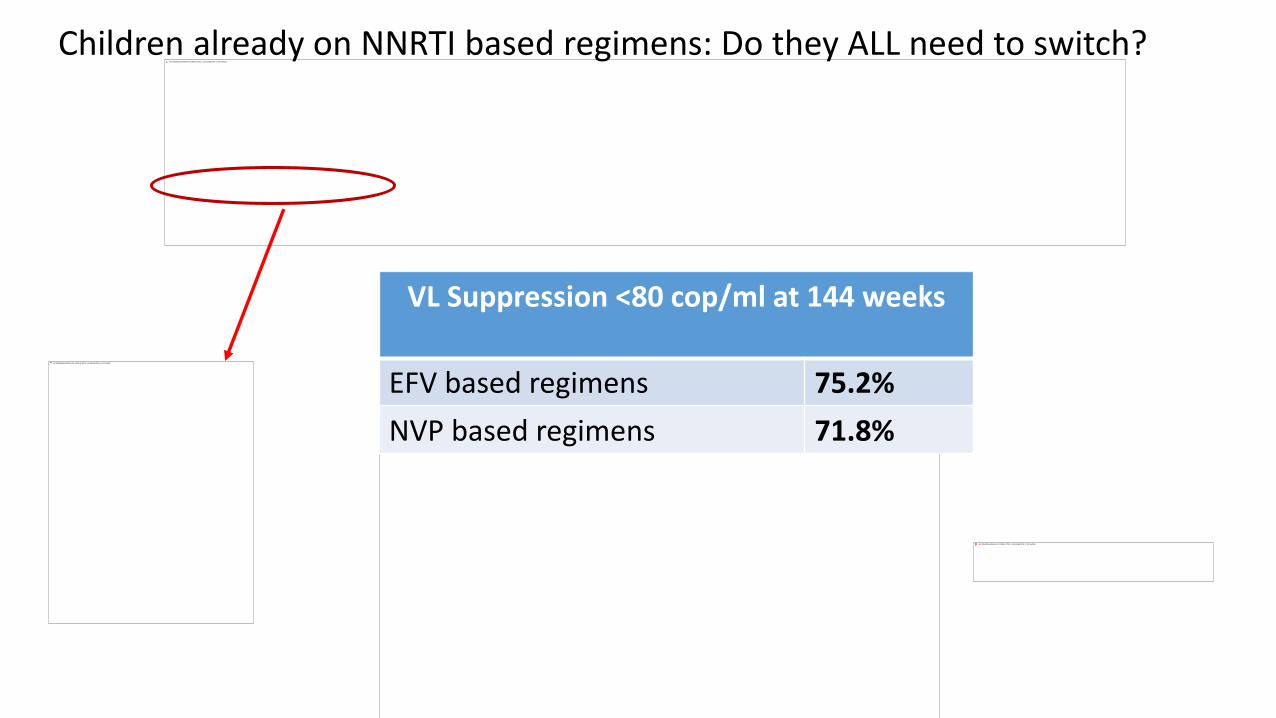
Children already on NNRTI based regimens: Do they ALL need to switch?
VL Suppression <80 cop/ml at 144 weeks
EFV based regimens 75.2%
NVP based regimens 71.8%

• 4 switch studies of patients with viral suppression then switched to a DTG-containing regimen• NEAT 022 • STRIIVING• SWORD 1/2
• 9 non switch studies• Treatment naïve• Treatment experienced
• Risk of Grade 1-4 adverse events were 9% higher (p<.001) in switch studies compared to the 9 non-switch studies
• Risk of discontinuation for adverse events was 3% higher in switch studies compared to the 9 non-switch studies
If patients are already tolerating current ART the risk of switching to DTG could outweigh benefits

What do we need to know before we switch all children to DTG-containing regimens?
Can we dose across all weight bands?
Do we have the right formulations?
Is it safe?
Can we switch existing patients?
What do we know about resistance?
Is this going to solve adherence issues?
✗
✗
We’re not really sure
Should we?
✗
✗
Let’s check back on Tuesday
Not yet

We are just beginning to understand DTG resistance
• Combination of two pathways involved in raltegravir resistance confers dolutegravir resistance1
• 1 patient failing on RAL treated with DTG and developed virus with N155 and Q148
• The combination of N155H, G140S, Q148H led to strong DTG resistance
• G118R and F121Y mutations identified in patients failing raltegravir treatment confer dolutegravir resistance2
• Results obtained with in vitro and ex vivo assays conferred intermediate resistance to DTG
• High frequency of dolutegravir resistance in patients failing a raltegravir-containing salvage regimen3
• 92 patients with viral failure on RAL-containing regimen• 32 (35%) showed resistance to DTG
1Malet et al J Antimicrob Chemother 20152Mounir et al J Antimicrob Chemother 20153de Souza Cavalcantiet al J Antimicrob Chemother 2015

THPEB114
TITLE
Emergence of resistance in HIV-1 integrase (IN) following dolutegravir (DTG) treatment in 6 to 18 year old participants enrolled in the P1093 study
PRESENTERCindy Vavro
AUTHORSC Vavro1 , T Ruel2, A Wiznia3, C Alvero4, S Popson5, T Fenton4, R Hazra6 E Townley7,8, A Buchanan1, P Palumbo9
Coming soon to a conference center near you!

What do we need to know before we switch all children to DTG-containing regimens?
Can we dose across all weight bands?
Do we have the right formulations?
Is it safe?
Can we switch existing patients?
What do we know about resistance?
Is this going to solve adherence issues?
✗
✗
We’re not really sure
Let’s check back on Tuesday
Should we?
✗
✗
✗
Let’s check back on Tuesday
Not yet

No drug can fix all adherence issues
• Reliance on caregiver/multiple caregivers
• Complex regimens
• Pill burden
• Treatment fatigue
• Inconvenient dosing schedule
• Inconvenient life schedule
• Lack of disclosure
• Stigma

What do we need to know before we switch all children to DTG-containing regimens?
Can we dose across all weight bands?
Do we have the right formulations?
Is it safe?
Can we switch existing patients?
What do we know about resistance?
Is this going to solve adherence issues?
✗
✗
We’re not really sure
Let’s check back on Tuesday
Should we?
✗
✗
✗
✗ No.
Let’s check back on Tuesday
Not yet

Is this the right time to suggest switching all children to DTG-containing regimens?
No
• No dosing for younger children
• Formulations needed are not available
• Potential toxicity risk
• Many patients are stable on their current regimen
• Resistance emerging
• Can’t fix all adherence challenges
Yes
• Potent
• Everyone else is doing it

All children should NOT be switched to dolutegravir-based
ART regimens: Rebuttal

What do we need to know before we switch all children to DTG-containing regimens?
Can we dose across all weight bands?
Do we have the right formulations?
Is it safe?
Can we switch existing patients?
What do we know about resistance?
Is this going to solve adherence issues?
✗
✗
We’re not really sure
Let’s check back on Tuesday
Should we?
✗
✗
✗
✗ No.
Let’s check back on Tuesday
Not yet
Is it AVAILABLE?
December 1, 2017:
https://msfaccess.org/msf-urges-viiv-register-its-paediatric-hiv-drug-formulation-dolutegravir-broadly-across-low-and

July 19, 2018:
https://msfaccess.org/request-urgently-step-efforts-ensure-widespread-access-dolutegravir-children
• Despite a commitment made in November 2017 to make pediatric formulations of DTG available in LMIC, limited progress has been made
• Dossiers for pediatric DTG formulations have only been filed in THREE sub-Saharan countries
• Not using waivers in countries where it is not registered

Switch to DTG for all children?
• Unknowns are many
• No dosing for younger children
• Inconvenient formulations
• Can’t fix adherence issues
• Ongoing concerns about toxicity
• Resistance possible (especially after RAL)
• Needs MORE TIME

Thank you!
AcknowledgementsTed RuelMartina PenazzatoElaine AbramsFatima TsourisAddy Kekitiinwa
Top Related