






Languages
Pages
Legal


AHRQ / QIO
Venous Thromboembolism (VTE) Prevention in the Hospital
Greg Maynard MD, MScClinical Professor of Medicine and Chief,
Division of Hospital MedicineUniversity of California, San Diego

VTE: A Major Source of Mortality and Morbidity
• 350,000 to 650,000 with VTE per year• 100,000 to > 200,000 deaths per year • Most are hospital related. • VTE is primary cause of fatality in half-
– More than HIV, MVAs, Breast CA combined– Equals 1 jumbo jet crash / day
• 10% of hospital deaths– May be the #1 preventable cause
• Huge costs and morbidity (recurrence, post-thrombotic syndrome, chronic PAH)
Surgeon General’s Call to Action to Prevent DVT and PE 2008 DHHS

Risk Factors for VTE
StasisAge > 40ImmobilityCHFStrokeParalysisSpinal Cord injuryHyperviscosityPolycythemiaSevere COPDAnesthesiaObesityVaricose Veins
Hypercoagulability CancerHigh estrogen statesInflammatory BowelNephrotic SyndromeSepsisSmokingPregnancyThrombophilia
Endothelial Endothelial DamageDamageSurgerySurgeryPrior VTEPrior VTECentral linesCentral linesTraumaTrauma
Anderson FA Jr. & Wheeler HB. Anderson FA Jr. & Wheeler HB. Clin Chest MedClin Chest Med 1995;16:235. 1995;16:235.

Risk Factors for VTE
StasisAge > 40ImmobilityCHFStrokeParalysisSpinal Cord injuryHyperviscosityPolycythemiaSevere COPDAnesthesiaObesityVaricose Veins
Hypercoagulability CancerHigh estrogen statesInflammatory BowelNephrotic SyndromeSepsisSmokingPregnancyThrombophilia
Endothelial Endothelial DamageDamageSurgerySurgeryPrior VTEPrior VTECentral linesCentral linesTraumaTrauma
Anderson FA Jr. & Wheeler HB. Anderson FA Jr. & Wheeler HB. Clin Chest MedClin Chest Med 1995;16:235. 1995;16:235. Bick RL & Kaplan H. Bick RL & Kaplan H. Med Clin North AmMed Clin North Am 1998;82:409. 1998;82:409.
Most hospitalized patients have
at least one ris
k factor for V
TE

ENDORSE Results
• Out of ~70,000 patients in 358 hospitals, appropriate prophylaxis was administered in:– 58.5% of surgical patients– 39.5% of medical patients
Cohen, Tapson, Bergmann, et al. Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study): a
multinational cross-sectional study. Lancet 2008; 371: 387–94.

The “Stick” is coming….
NQF endorses measures already
Public reporting and TJC measures coming soon:- Prophylaxis in place within 24 hours of admit or risk
assessment / contraindication justifying it’s absence- Same for critical care unit admit / transfers- Track preventable VTE
CMS – DVT or PE with knee or hip replacement reimbursed as though complication had not occurred.

• 2005 – AHRQ grant to:– Design and implement VTE prevention protocol– Monitor impact on VTE prophylaxis and HA VTE– Validate a VTE risk assessment model / protocol
Attempt to use portable methodology, build toolkit to allow others to accomplish the same thing
Percent of randomly sampled inpatients with adequate vte prophylaxis
8
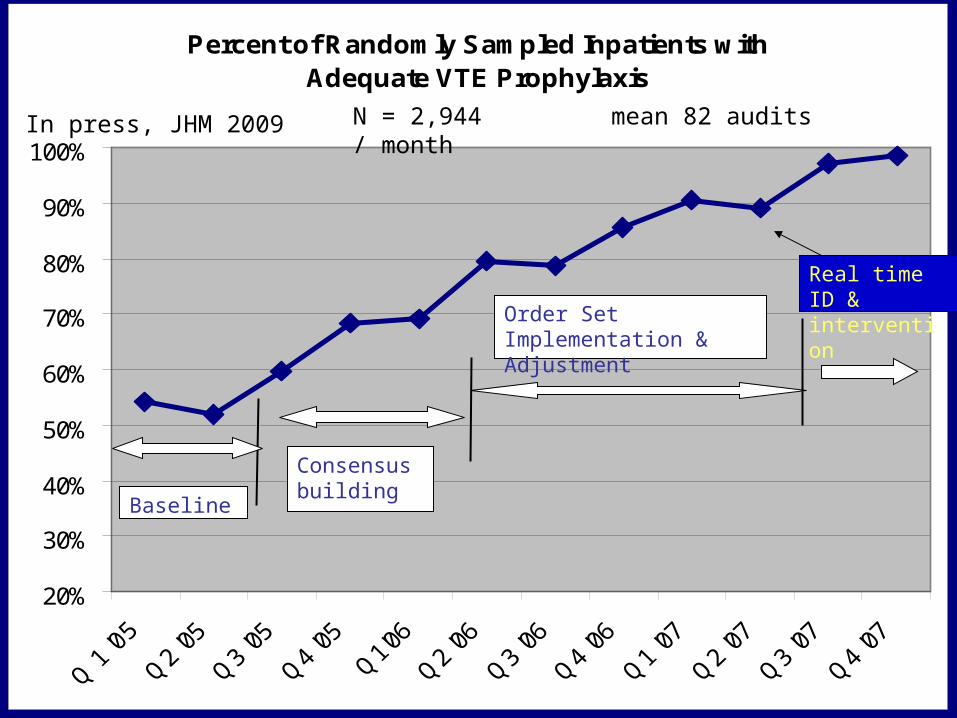
Percent of Randomly Sampled Inpatients with Adequate VTE Prophylaxis
20%
30%
40%
50%
60%
70%
80%
90%
100%
Baseline
Consensus building
Order Set Implementation & Adjustment
Real time ID & intervention
Percent of Randomly Sampled Inpatients with Adequate VTE Prophylaxis
20%
30%
40%
50%
60%
70%
80%
90%
100%
Baseline
Consensus building
Order Set Implementation & Adjustment
Real time ID & intervention
N = 2,944 mean 82 audits / monthIn press, JHM 2009

UCSD – Decrease in patients with preventable ha vteUCSD - Decrease in Patients with Preventable HA
VTE
0
2
4
6
8
10
12
14
Q 1 '0
5
Q2 '05
Q3 '05
Q4 '05
Q1'06
Q2 '06
Q3 '06
Q4 '06
Q1 '07
Quarter
# o
f P
ati
en
ts
Medicine
Surgery
Ortho
Other
Total
9
Level 5 Oversights identified and addressed in real timeOversights identified and addressed in real time 95+%

UCSD VTE Protocol Validated
• Easy to use, on direct observation – a few seconds• Inter-observer agreement –
– 150 patients, 5 observers- Kappa 0.8 and 0.9
• Predictive of VTE • Implementation = high levels of VTE prophylaxis
– From 50% to sustained 98% adequate prophylaxis– Rates determined by over 2,900 random sample audits
• Safe – no discernible increase in HIT or bleeding• Effective – 40% reduction in HA VTE
– 86% reduction in risk of preventable VTE

VTE Prevention Guides
VTE Prevention Guides
http://ahrq.hhs.gov/qual/vtguide/
http://www.hospitalmedicine.org/ResourceRoomRedesign/RR_VTE/VTE_Home.cfm

VTE QI Resource Room www.hospitalmedicine.org
VTE QI Resource Room

Collaborative Efforts and Kudos
• SHM VTE Prevention Collaborative I - 25 sites• SHM / VA Pilot Group - 6 sites• SHM / Cerner Pilot Group – 6 sites
• AHRQ / QIO (NY, IL, IA) - 60 sites• IHI Expedition to Prevent VTE – 60 sites
• SHM Team Improvement Award• NAPH Safety Net Award (Honorable Mention)• Venous Disease Coalition

To Achieve Improvement
• Real institutional support / prioritization
• Will to standardize
• Physician leadership
• Measurement of process / outcomes
• Protocol, integrated into order sets
• Education
• Continued refinement / tweaking- PDSA
SHM and AHRQ Guides on VTE Prevention

The Essential First Intervention
1) a standardized VTE risk assessment, linked to…2) a menu of appropriate prophylaxis options, plus…3) a list of contraindications to pharmacologic VTE
prophylaxis
Challenges: Make it easy to use (“automatic”)
Make sure it captures almost all patientsTrade-off between guidance and ease of use /
efficiency 15
VTE Protocol

Hierarchy of Reliability
No protocol* (“State of Nature”)
Decision support exists but not linked to order writing, or prompts within orders but no decision support
Protocol well-integrated
(into orders at point-of-care)
Protocol enhancedProtocol enhanced
(by other QI / high reliability strategies)(by other QI / high reliability strategies)
Oversights identified and addressed in Oversights identified and addressed in real timereal time
Level
4
1
2
3
5
Predicted
Prophylaxis rate
40%
50%
65-85%
90%
95+%
* Protocol = standardized decision support, nested within an order set, i.e. what/when

Map to Reach Level 3Implementing an Effective VTE Prevention
Protocol• Examine existing admit, transfer, periop order
sets with reference to VTE prophylaxis.• Design a protocol-driven DVT prophylaxis order
set (w/ integrated risk assessment model [RAM])• Vette / Pilot – PDSA• Educate / consensus building• Place new standardized DVT order set ‘module’
into all pertinent admit, transfer, periop order sets.
• Monitor, tweak - PDSA

Too Little GuidancePrompt ≠ Protocol
DVT PROPHYLAXIS ORDERS
Anti thromboembolism Stockings Sequential Compression Devices UFH 5000 units SubQ q 12 hours UFH 5000 units SubQ q 8 hours LMWH (Enoxaparin) 40 mg SubQ q day LMWH (Enoxaparin) 30 mg SubQ q 12 hours No Prophylaxis, Ambulate

Most Common Mistakes in VTE Prevention Orders
• Point based risk assessment model• Improper Balance of guidance / ease of use
– Too little guidance - prompt ≠ protocol
– Too much guidance- collects dust, too long
• Failure to revise old order sets• Too many categories of risk• Allowing non-pharm prophy too much• Failure to pilot, revise, monitor• Linkage between risk level and prophy choices are
separated in time or space

20
Is your order set in a competition?

Low Medium HighAmbulatory with no other risk factors. Same day or minor surgery
CHF
COPD / Pneumonia
Most Medical Patients
Most Gen Surg Patients
Everybody Else
Elective LE arthroplasty
Hip/pelvic fx
Acute SCI w/ paresis
Multiple major trauma
Abd / pelvic CA surgery
Early ambulation
UFH 5000 units q 8 h (5000 units q 12 h if > 75 or weight <50 kg)
LMWH Enox 40 mg q day
Other LMWH
CONSIDER add IPC
Enox 30 mg q 12 h or
Enox 40 q day or
Other LMWH or
Fondaparinux 2.5 mg q day or
Warfarin INR 2-3
AND MUST HAVE
IPC 21
IPC needed if contraindication to AC exists
Example from UCSD Keep it Simple – A “3 bucket” model

Hierarchy of Reliability
No protocol* (“State of Nature”)
Decision support exists but not linked to order writing, or prompts within orders but no decision support
Protocol well-integrated
(into orders at point-of-care)
Protocol enhancedProtocol enhanced
(by other QI / high reliability strategies)(by other QI / high reliability strategies)
Oversights identified and addressed in Oversights identified and addressed in real timereal time
Level
4
1
2
3
5
Predicted
Prophylaxis rate
40%
50%
65-85%
90%
95+%
* Protocol = standardized decision support, nested within an order set, i.e. what/when

Map to Reach Level 595+ % prophylaxis
• Use MAR or Automated Reports to Classify all patients on the Unit as being in one of three zones:
GREEN ZONE - on anticoagulationYELLOW ZONE - on mechanical
prophylaxis only RED ZONE – on no prophylaxis
Act to move patients out of the RED!

Situational Awareness and Measure-vention: Getting to
Level 5• Identify patients on no anticoagulation• Empower nurses to place SCDs in
patients on no prophylaxis as standing order (if no contraindications)
• Contact MD if no anticoagulant in place and no obvious contraindication– Templated note, text page, etc
• Need Administration to back up these interventions and make it clear that docs can not “shoot the messenger”

Summary of Key Strategies
• Basic Building Blocks– Institutional support, team, education,
protocol, metrics, PDSA
• Physician performs VTE risk assessment within easy to use order sets, which captures all admits / transfers
• Active monitoring for non-adherents to protocol, intervene in real time
Top Related