






Languages
Pages
Legal

04/15/23 DR. M. S. PRASAD 1
Acyanotic Congenital Heart DiseaseAcyanotic Congenital Heart Disease
Dr. M. S. PrasadProfessor & HODDept. of Pediatrics
SGT Medical College
04/15/23 DR. M. S. PRASAD 2
ObjectivesObjectives
• By the end of this class, the students will be able
– to define Congenital Heart Disease (CHD), and
– to describe common types of Acyanotic CHD.
04/15/23 DR. M. S. PRASAD 3
04/15/23 DR. M. S. PRASAD 4
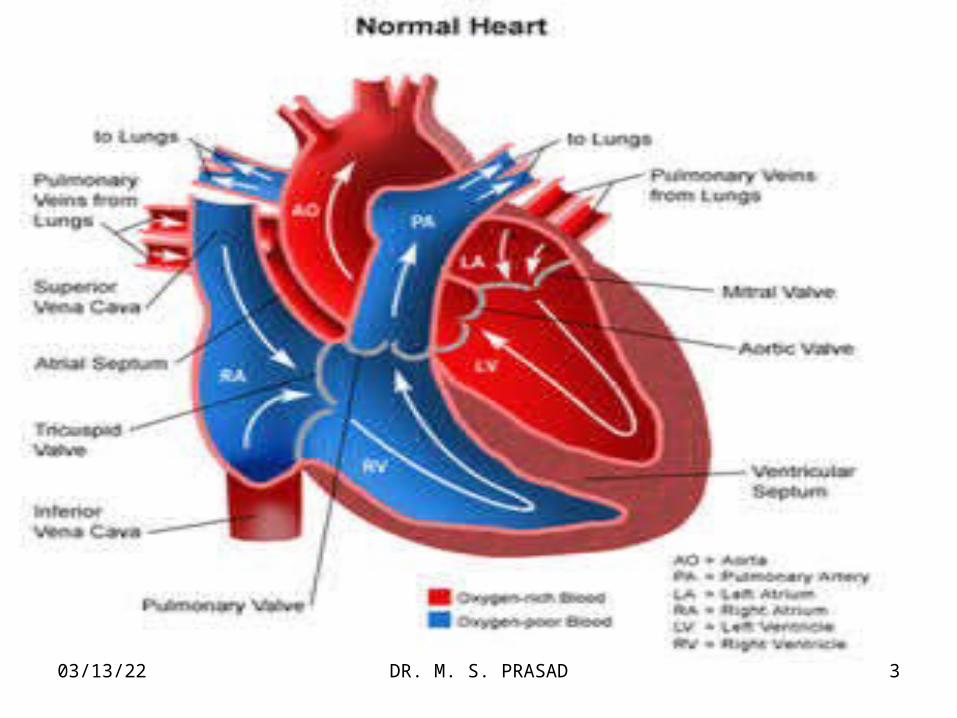
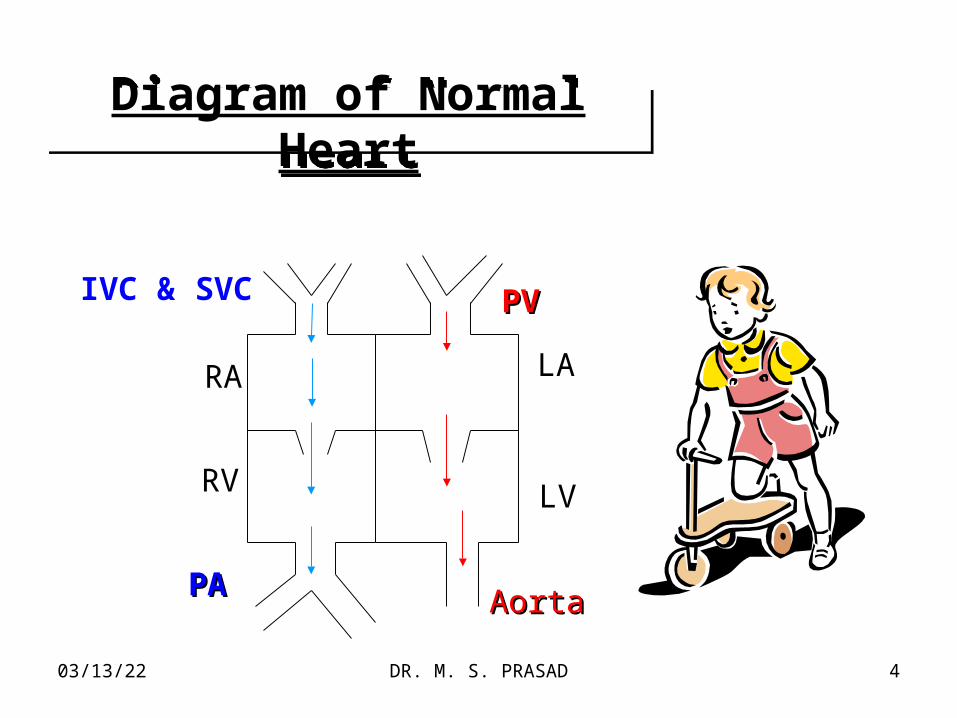
Diagram of Normal HeartDiagram of Normal Heart
PAPAAortaAorta
RA
RV
LA
LV
PVPVIVC & SVC
04/15/23 DR. M. S. PRASAD 5
04/15/23 DR. M. S. PRASAD 6
04/15/23 DR. M. S. PRASAD 7
Cardiovascular DiseasesCardiovascular Diseases
• Congenital Heart Disease– Acyanotic CHD (L R shunt)– Cyanotic CHD (R L shunt).
• Acquired Heart Diseases:– Kawasaki Disease,– Myocarditis,– Rheumatic Heart Disease.
04/15/23 DR. M. S. PRASAD 8
Congenital Heart Disease (CHD)Congenital Heart Disease (CHD)
• Con = Together.
• Genitus = Born.
04/15/23 DR. M. S. PRASAD 9
Definition
• A structural or functional deficiency in heart or its appendages which originates during foetal life is known as ‘Congenital Heart Congenital Heart Disease’Disease’ (CHD).
• It may or may not manifest at birth.
• Congenital Bicuspid Aortic Valve is normal at birth but may take 2, 3, or more decades to stiffen, calcify and present as overt Aortic Stenosis.
04/15/23 DR. M. S. PRASAD 11
CLASSIFICATION
ACYANOTIC
CYANOTIC
Physical Examination, or Pulse Oximetry.
04/15/23 DR. M. S. PRASAD 12
04/15/23 DR. M. S. PRASAD 13
Acyanotic CHDAcyanotic CHD
• Shunt Lesions (Left Right),
• Obstructive Lesions,
• Regurgitant Lesions, and
• Mixed (combination)
04/15/23 DR. M. S. PRASAD 14
L L R Shunt Lesions R Shunt Lesions
• ASD (Atrial Septal Defect),
• AVSD (Atrio-ventricular Septal Defect),
• VSD (Ventricular Septal Defect),
• PDA (Patent Ductus Arteriosus).
04/15/23 DR. M. S. PRASAD 15
Obstructive LesionsObstructive Lesions
• AS (Aortic Stenosis),
• COA (Coarctation of Aorta)
• HLHS (Hypoplastic Left Heart Syndrome),
• PS (Pulmonary Stenosis),
• Mitral Stenosis,
• Tricuspid Stenosis
04/15/23 DR. M. S. PRASAD 16
Regurgitant LesionsRegurgitant Lesions
• AR (Aortic Regurgitation),
• MR (Mitral Regurgitation),
• MVP (Mitral Valve Prolapse),
• TR (Tricuspid Regurgitation),
• PI (Pulmonary Incompetence)

04/15/23 DR. M. S. PRASAD 17
Patent Foramen Ovale Patent Foramen Ovale (PFO)(PFO)
&&Atrial Septal DefectAtrial Septal Defect
(ASD)(ASD)
04/15/23 DR. M. S. PRASAD 18
PFOPFOPFOPFO
• An isolated patent foramen (PFO) is a common finding during infancy and it usually closes.
• It is not considered abnormal, even if it persists throughout life.
• It is usually of no hemodynamic significance and is not considered an ASD.
May play an important role if other structural heart defects are present.
04/15/23 DR. M. S. PRASAD 19
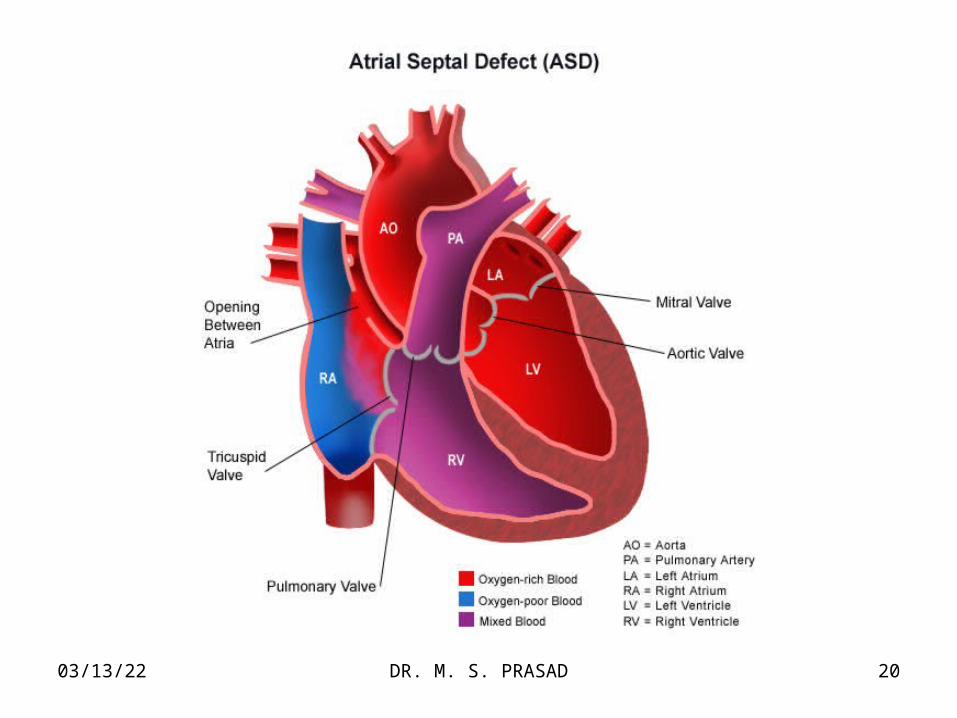
Atrial Septal Defect (ASD)Atrial Septal Defect (ASD)
• A defect in the wall between left and right atrium is known as Atrial Septal Defect (ASD).
• This is one of the Acyanotic CHD with L R shunt.
• More common in females than in males.
[M:F = 1:2].
04/15/23 DR. M. S. PRASAD 20
04/15/23 DR. M. S. PRASAD 21
Types of ASDTypes of ASD
• Ostium Secundum Defect(5-10% of CHD)
• Sinus Venosus ASD.(10% of ASD)
• Ostium primum ASD
04/15/23 DR. M. S. PRASAD 22
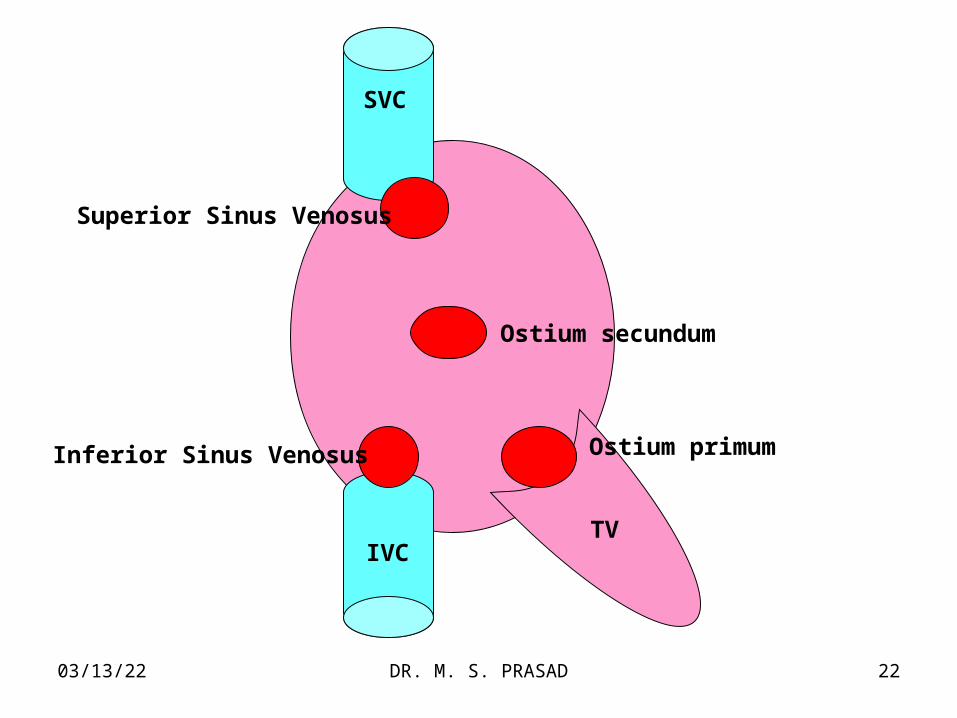
SVC
IVCTV
Ostium primum
Ostium secundum
Superior Sinus Venosus
Inferior Sinus Venosus
04/15/23 DR. M. S. PRASAD 23
• Ostium secundum ASD constitutes 5-10% of CHD.
• Ostium Secundum Defect is 3 times more common in girls than in boys.
• PAPVR may be present.
04/15/23 DR. M. S. PRASAD 24
Secundum ASDSecundum ASD
• Spontaneous closure up to 2-3 years may occur.
• Symptoms in childhood are rare.
• Life expectancy virtually normal if closure undertaken in childhood.
04/15/23 DR. M. S. PRASAD 25
Sinus VenosusSinus Venosus
• Spontaneous closure does not occur.
• Natural history same as secundum ASD.
04/15/23 DR. M. S. PRASAD 26
ASD
• History: Usually asymptomatic.• Physical Examination:
– Thin built.– There is absence of sinus arrhythmia.– Wide & fixed splitting of 2nd Heart Sound.– Ejection Systolic Murmur.
• ECG• CXR• Echocardiogram
04/15/23 DR. M. S. PRASAD 27
ASDASD• ECG:
– Features of RBBB– rsR/ pattern V1
– Mild RVH– RAD
• CXR:– Cardiomegaly– Prominent Pulmonary Conus.– Increased Pulmonary Vascular Markings.
• Echocardiography– Diagnostic,– shows exact location.
04/15/23 DR. M. S. PRASAD 28
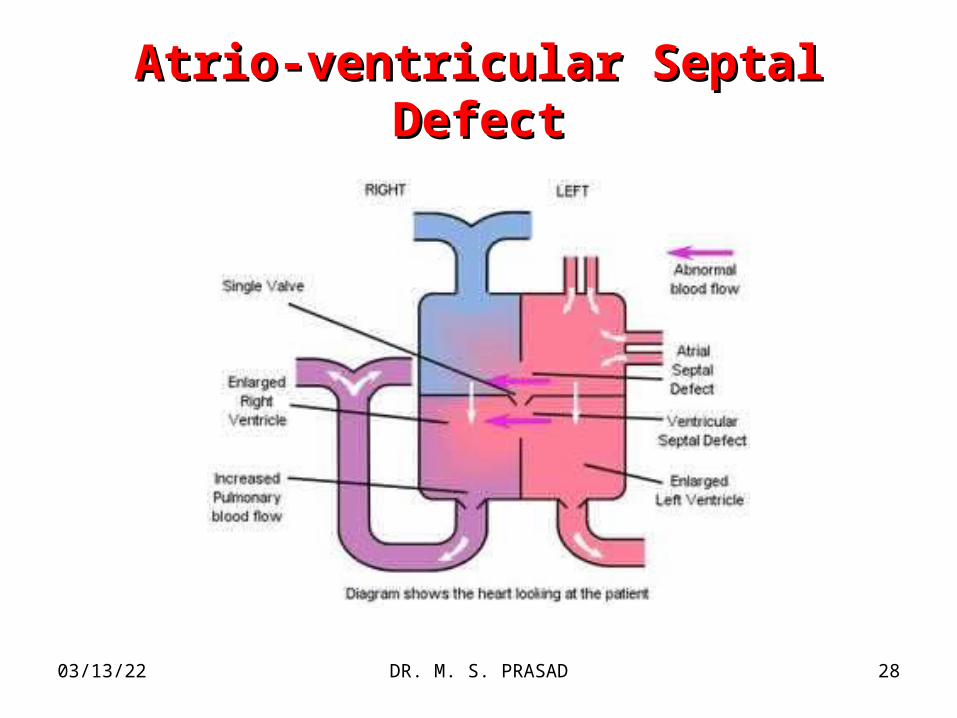
Atrio-ventricular Septal DefectAtrio-ventricular Septal Defect
04/15/23 DR. M. S. PRASAD 29
Atrio-Ventricular Septal DefectAtrio-Ventricular Septal Defect
• Partial (ostium primum) AVSD– Atrial Shunting,– Mitral Valve is always defective,– LV RA shunting may occur.
• Complete AVSD– Strong association with Down’s Syndrome,– Atrial and Ventricular shunting,– AV regurgitation.
04/15/23 DR. M. S. PRASAD 30
Clinical FeaturesClinical Features
• FTT
• Clinical signs of CHF,
• Signs of the most prominent lesion (ASD, Regurgitation, others)
04/15/23 DR. M. S. PRASAD 31
ManagementManagement
• Management of CHF,
• Corrective surgery.
04/15/23 DR. M. S. PRASAD 32
04/15/23 DR. M. S. PRASAD 33
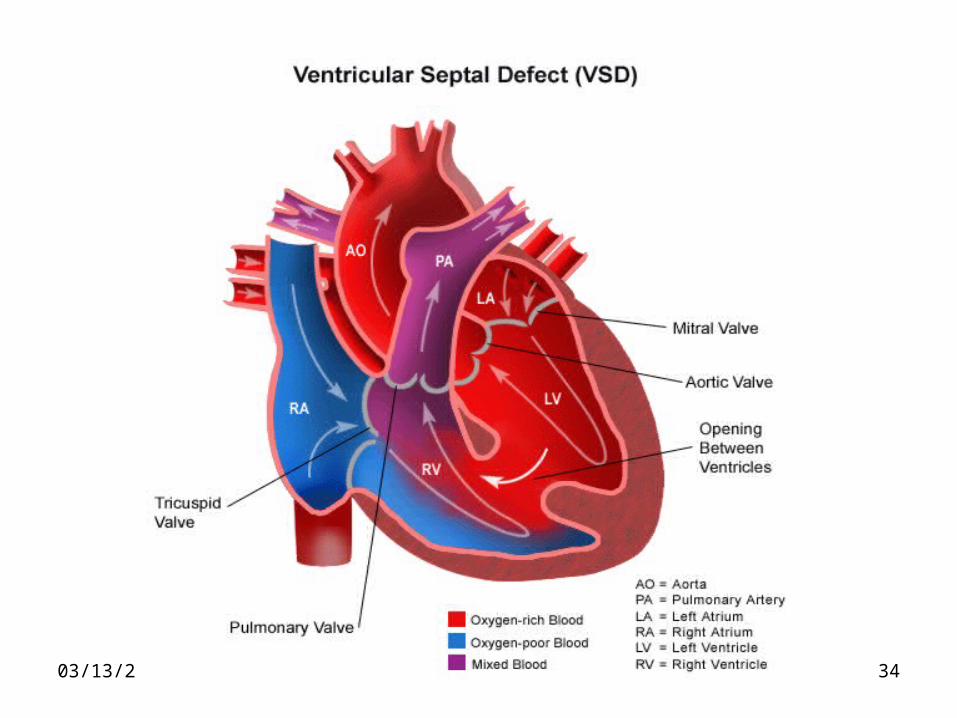
Ventricular Septal Defect (VSD)Ventricular Septal Defect (VSD)
VSD is the most common cardiac malformation and accounts for 32% of CHD
04/15/23 DR. M. S. PRASAD 34
04/15/23 DR. M. S. PRASAD 35
Types of VSDTypes of VSD
• Membranous.
• Muscular.
• Swiss Cheese Septum.
• Membranous.
• Muscular.
• Swiss Cheese Septum.
04/15/23 DR. M. S. PRASAD 36
VSD: PathopyhsiologyVSD: Pathopyhsiology
• LV pressure higher than RV.
• Blood passes through the defect to RV.
• RV load is increased.
• PA receives more volume than expected.
• This extremely large pulmonary blood flow results into Pulmonary Hypertension.
04/15/23 DR. M. S. PRASAD 37
Clinical ManifestationsClinical Manifestations

04/15/23 DR. M. S. PRASAD 38
Small VSDSmall VSD
• Asymptomatic.
• Cardiac lesion is usually found during routine physical examination.
• A loud, harsh, or blowing systolic murmur best heard over the lower left sternal border.
04/15/23 DR. M. S. PRASAD 39
Large VSDLarge VSD• Patients with large defects typically
develop CHF.
• Excessive pulmonary blood flow and Pulmonary Hypertension
• Dyspnoea or effort intolerance.
• Poor Growth.
04/15/23 DR. M. S. PRASAD 40
Large VSD Large VSD (continued)
• Profuse Perspiration (Sweating).
• Recurrent RTI.
• Feeding difficulty,
• Systolic Murmur: less harsh, more blowing
• Loud P2
04/15/23 DR. M. S. PRASAD 41
VSD: VSD: DiagnosisDiagnosis• Most common Acyanotic CHD.• CXR:
– Small VSD: Normal.– Large VSD:
• Cardiomegaly.• Increased Pulmonary Vascular Markings.
• ECG:– Small VSD: Normal.– Large VSD: Biventricular Hypertrophy.
• Echocardiogram• Cardiac Catheterization.
04/15/23 DR. M. S. PRASAD 42
Natural HistoryNatural History
• 65% of VSD present at birth close spontaneously.
• Remaining cases:– FTT,– Feeding difficulty,– Signs of VSD and CHF.

04/15/23 DR. M. S. PRASAD 43
ManagementManagement
• Manage CHF,
• Surgical closure.
04/15/23 DR. M. S. PRASAD 44
Patent Ductus ArteriosusPatent Ductus Arteriosus(PDA)(PDA)
04/15/23 DR. M. S. PRASAD 45
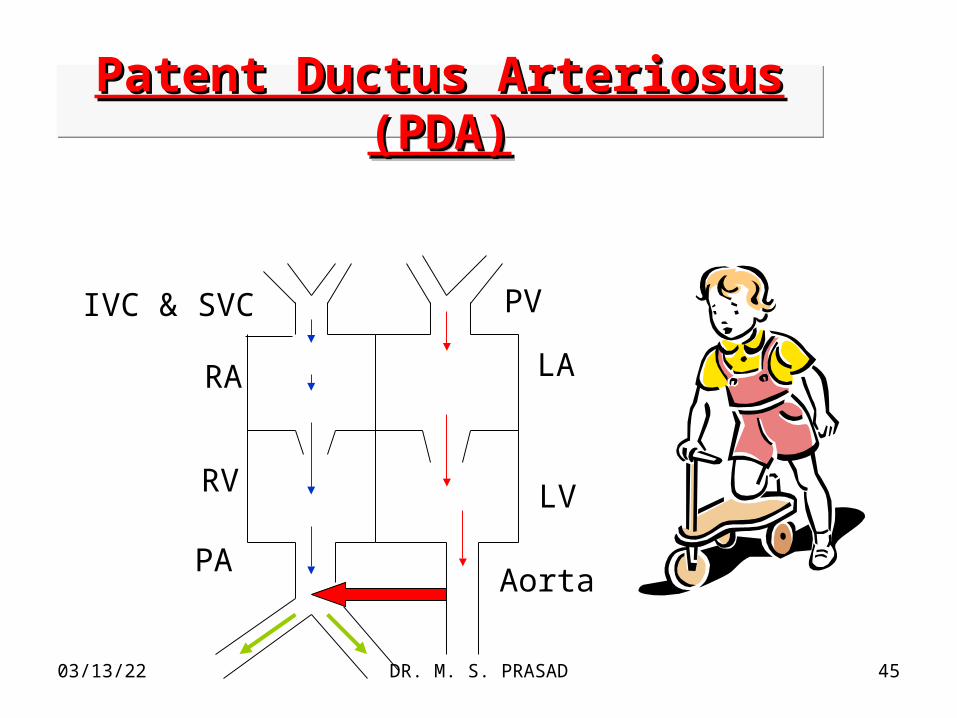
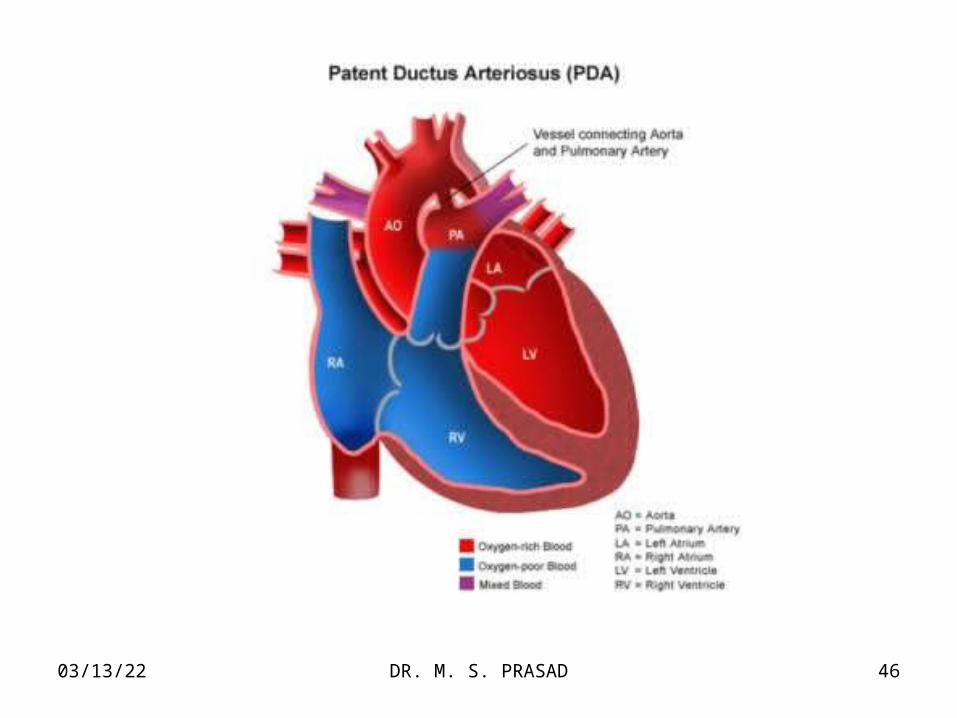
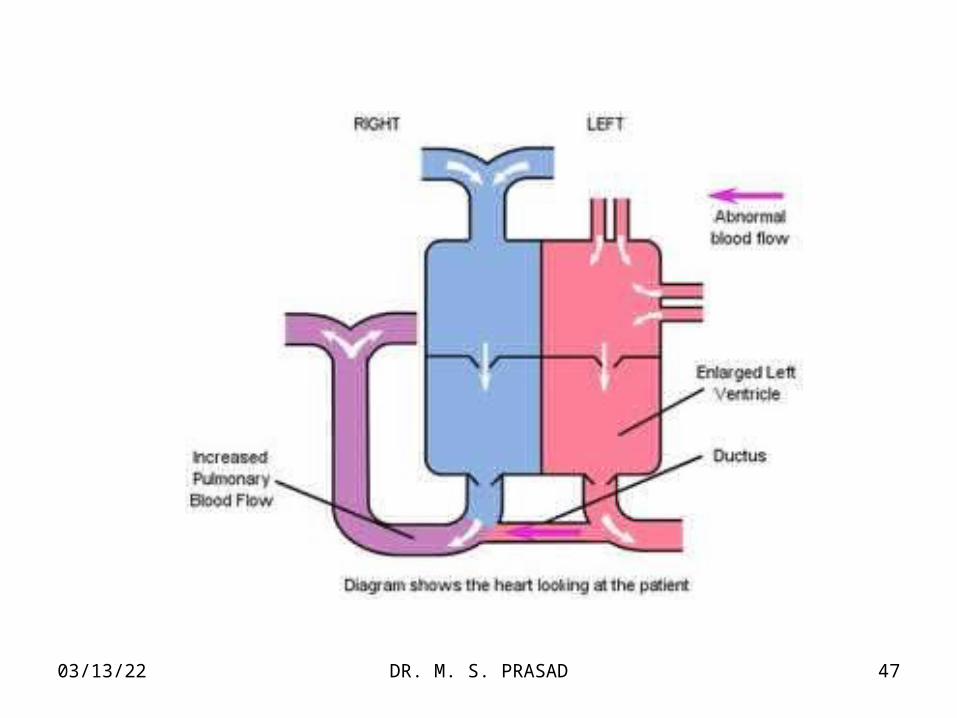
Patent Ductus Arteriosus Patent Ductus Arteriosus (PDA)(PDA)
Patent Ductus Arteriosus Patent Ductus Arteriosus (PDA)(PDA)
PAAorta
RA
RV
LA
LV
PVIVC & SVC
04/15/23 DR. M. S. PRASAD 46
04/15/23 DR. M. S. PRASAD 47
04/15/23 DR. M. S. PRASAD 48
PDAPDA• More in females [2:1]
• Maternal Rubella in early pregnancy.
• Common in premature infants.
• 10% of PDA is associated with other CHD.
04/15/23 DR. M. S. PRASAD 49
PDA: Clinical ManifestationsPDA: Clinical Manifestations
• Wide Pulse Pressure.• Bounding Peripheral Pulses.• Cardiac Enlargement.• Thrill.
LSB & below left clavicle.
• Machinery Murmur.• CHF
04/15/23 DR. M. S. PRASAD 50
PDA: DiagnosisPDA: Diagnosis
• ECG: Normal/LVH/BVH
• CXR: Prominent PA & Increased PVM.
• Echocardiogram: from the suprasternal notch.
• Colour & Pulsed Doppler Examination.
• Cardiac Catheterization.
04/15/23 DR. M. S. PRASAD 51
04/15/23 DR. M. S. PRASAD 52
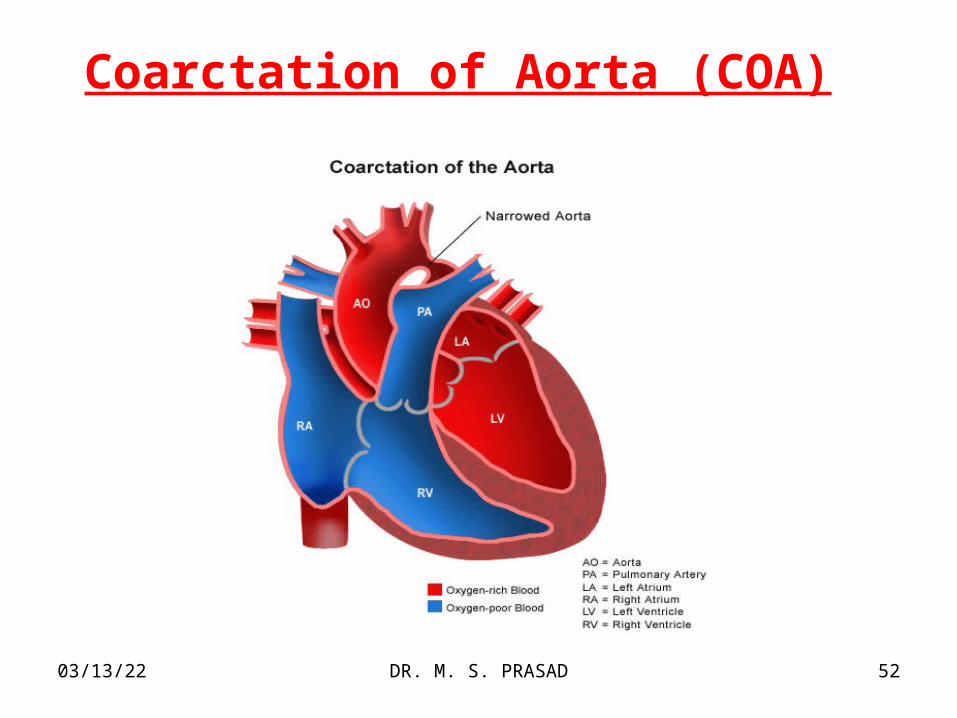
Coarctation of Aorta (COA)
04/15/23 DR. M. S. PRASAD 53
COACOA• COA is a localized or segmental
constriction [narrowing] of aorta
• The size of constriction may vary.
04/15/23 DR. M. S. PRASAD 54
COACOA• It may be at one point or multiple points.
• It may involve a long segment continuously.
• Involvement of long segment is known as “Tubular Hypoplasia”.
• Sometimes, the the aorta becomes completely atretic and results in an “Interrupted Aortic Arch”.
04/15/23 DR. M. S. PRASAD 55
COACOA• The COA may occur at any point from the
Transverse Arch to the iliac bifurcation.
• 98% occur just below the origin of the left subclavian artery at the origin of the ductus arteriosus [juxtaductal COA].
04/15/23 DR. M. S. PRASAD 56
Coarctation of Aorta
• Two times more common in males.
• M:F = 2:1
04/15/23 DR. M. S. PRASAD 57
Types of COATypes of COA
o Infantile Type.
COA associated with arch hypoplasia was referred to as Infantile Type because its severity led to its recognition in early infancy.
o Adult Type.
Adult Type referred to isolated juxtaductal COA, which if mild, was not usually recognized until later childhood.
04/15/23 DR. M. S. PRASAD 58
COA: Clinical Manifestations
• Weakness and pain after exercise.
• Hypertension on routine physical examination.
• Classis Sign: Disparity in pulsation and B. P. in the arms and legs.
04/15/23 DR. M. S. PRASAD 59
COA: Diagnosis
• Mainly on clinical grounds.
• CXR & ECG: not much helpful.
• Pulsed and continuous wave Doppler studies are helpful.
04/15/23 DR. M. S. PRASAD 60
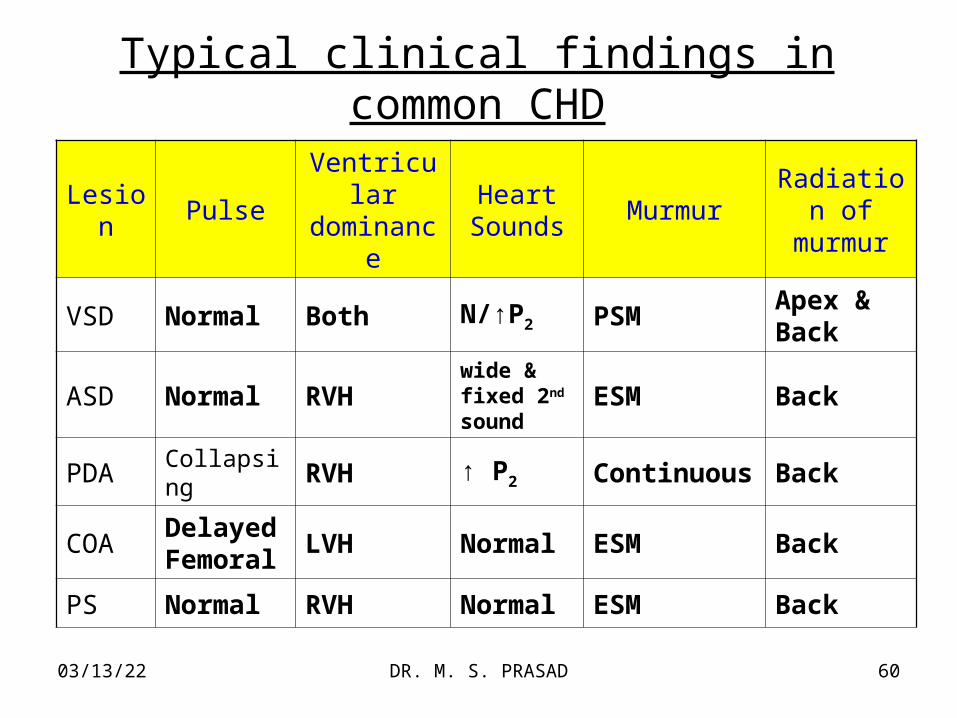
Typical clinical findings in common CHD
Lesion PulseVentricular dominance
Heart Sounds
MurmurRadiation of murmur
VSD Normal Both N/↑P2 PSMApex & Back
ASD Normal RVHwide & fixed 2nd sound
ESM Back
PDA Collapsing RVH ↑ P2 Continuous Back
COADelayed Femoral
LVH Normal ESM Back
PS Normal RVH Normal ESM Back
04/15/23 DR. M. S. PRASAD 61
या� दे�वी� सवीभू�ते�षु� विवीद्या�रूपे�ण स�स्थि�ते�, नमस्तेस्या� नमस्तेस्या� नमस्तेस्या� नम� नम� ||
04/15/23 DR. M. S. PRASAD 62
Did you meet your objectives?Did you meet your objectives?
• Can you define Congenital Heart Disease (CHD)? and
• Can you describe common types of Acyanotic CHD?
• Yes, very good. • No, discuss again next time.
Top Related