







Languages
Pages
Legal

POSTGRAD. MED. J. (I964), 40, 36
ACUTE SUPPURATIVE PERICARDITISWith Death from Ruptured Mycotic Aneurysm of the Aorta
J. D. FITZGERALD, M.B.,(N.U.I.), B.Sc., M.R.C.P.(Ed.)*MARTIN W. McNICOL, M.B.(Glasg.), M.R.C.P.t
From the Sully Hospital, Penarth, Glam.
ACUTE suppurative pericarditis is a rare disease,usually resulting from a local cause, or associatedwith a debilitating illness. The prognosis has beenmuch improved by antibiotics, but treatrnent isstill difficult. The case reported here is one in whichsuppurative pericarditis was apparently a primarycondition; after a protracted illness, the patient diedas a result of a complication that has not beenpreviously recorded.
Case ReportThe patient, a 52-year-old male pharmacist, was
admitted to Sully Hospital on 20.5.6i. Six weeks earlierhe had noted lassitude and a feeling of vague ill health.Ten days later he developed slight itching in both earsand a dry throat. He was put to bed and was givenoxytetracycline ig./day for five days with some improve-ment. Eight days later the dry throat and itching in theears recurred, and were now accompanied by fever andlow backache. He was again put to bed and was givenbenzyl penicillin I megaunit/day for seven days, followedby phenethicillin ig./day and 'virugon'. There was aslight improvement and he was then sent for a chestX-ray which showed a small right pleural effusion. Hewas therefore admitted to Cardiff Royal Infirmary.Examination there showed the signs of a right pleuraleffusion, and an enlarged but not tender liver. 200 ml.of blood-stained fluid were removed by pleural aspira-tion; the fluid contained 99% red cells with I% neutro-phils, and was sterile on culture. The patient was trans-ferred to Sully Hospital for further investigation.He was a moderately obese man. Though afebrile
(T.98°F.), he looked ill and was very distressed andrestless. The jugular venous pressure was elevated andshowed no pulsation. There was no peripheral cedema.Pulse regular, rate ioo/min.; blood pressure 130/90mm. Hg. A protodiastolic triple rhythm was present;there were no cardiac murmurs and no pericardialfriction rub was heard. Examination of the chest showedthe signs of a right pleural effusion. The abdomen wasvery distended and tympanitic; the liver and spleenwere not enlarged and bowels sounds were present.The other systems showed no abnormality.
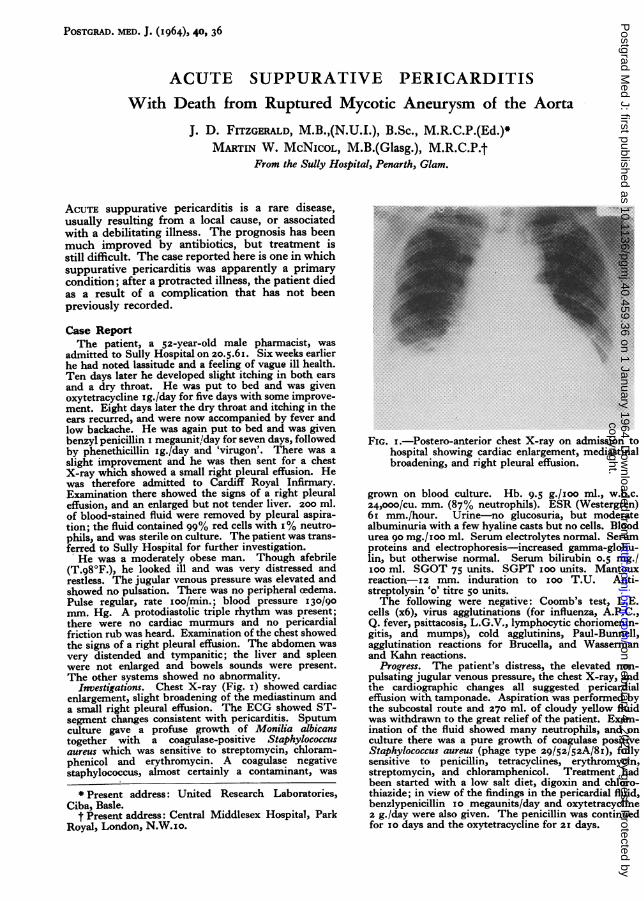
Investigations. Chest X-ray (Fig. I) showed cardiacenlargement, slight broadening of the mediastinum anda small right pleural effusion. The ECG showed ST-segment changes consistent with pericarditis. Sputumculture gave a profuse growth of Monilia albicanstogether with a coagulase-positive Staphylococcstsaureus which was sensitive to streptomycin, chloram-phenicol and erythromycin. A coagulase negativestaphylococcus, almost certainly a contaminant, was
Present address: United Research Laboratories,Ciba, Basle.
t Present address: Central Middlesex Hospital, ParkRoyal, London, N.W.IO.
FIG. I.-Postero-anterior chest X-ray on admission tohospital showing cardiac enlargement, mediastinalbroadening, and right pleural effusion.
grown on blood culture. Hb. 9.5 g./xoo ml., w.b.c.24,000/cu. mm. (87% neutrophils). ESR (Westergren)6i mm./hour. Urine-no glucosuria, but moderatealbuminuria with a few hyaline casts but no cells. Bloodurea go mg./0oo ml. Serum electrolytes normal. Serumproteins and electrophoresis-increased gamma-globu-lin, but otherwise normal. Serum bilirubin 0.5 mg./0OO ml. SGOT 75 units. SGPT ioo units. Mantouxreaction-12 mm. induration to Ioo T.U. Anti-streptolysin 'o' titre 50 units.The following were negative: Coomb's test, L.E.
cells (x6), virus agglutinations (for influenza, A.P.C.,Q. fever, psittacosis, L.G.V., lymphocytic choriomenin-gitis, and mumps), cold agglutinins, Paul-Bunnell,agglutination reactions for Brucella, and Wassermanand Kahn reactions.
Progress. The patient's distress, the elevated non-pulsating jugular venous pressure, the chest X-ray, andthe cardiographic changes all suggested pericardialeffusion with tamponade. Aspiration was performed bythe subcostal route and 270 ml. of cloudy yellow fluidwas withdrawn to the great relief of the patient. Exam-ination of the fluid showed many neutrophils, and onculture there was a pure growth of coagulase positiveStaphylococcus aureus (phage type 29/52/52A/8i), fullysensitive to penicillin, tetracyclines, erythromycin,streptomycin, and chloramphenicol. Treatment hadbeen started with a low salt diet, digoxin and chloro-thiazide; in view of the findings in the pericardial fluid,benzlypenicillin io megaunits/day and oxytetracycline2 g./day were also given. The penicillin was continuedfor io days and the oxytetracycline for 2I days.
copyright. on F
ebruary 4, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.40.459.36 on 1 January 1964. D
ownloaded from
January I964 FITZGERALD and McNICOL: Acute Suppurative Pericarditis 37
.. ....... ..
..............
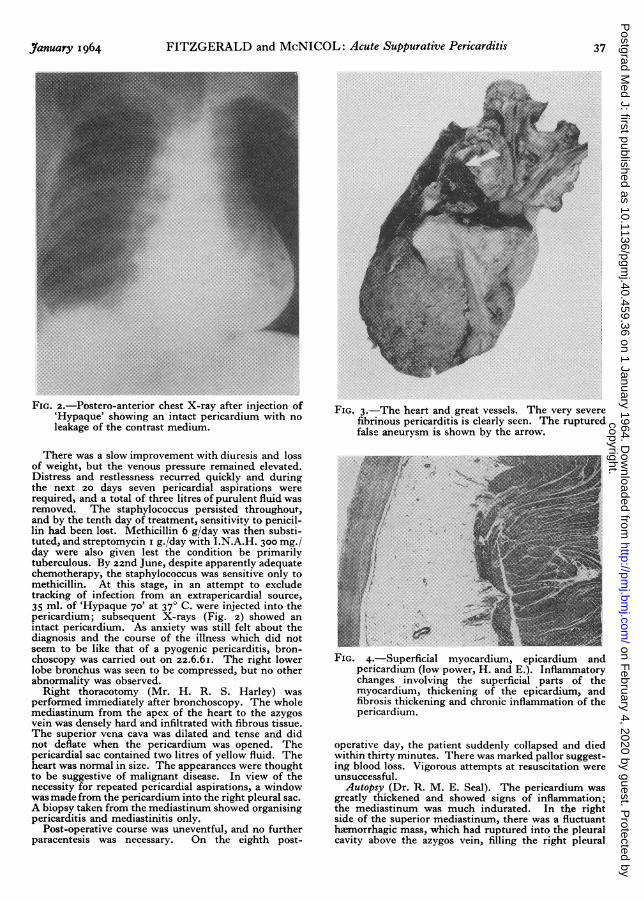
FIG. 2.-Postero-anterior chest X-ray after inj'ection of'Hypaque' showing an intact pericardium with no
leakage of the contrast medium.
There was a slow improvement with diuresis and lossof weight, but the venous pressure remained elevated.Distress and restlessness recurred quickly and duringthe next 20 days seven pericardial aspirations wererequired, and a total of three litres of purulent fluid wasremoved. The staphylococcus persisted throughout,and by the tenth day of treatment, sensitivity to penicil-lin had been lost. Methicillin 6 g/day was then substi-tuted, and streptomycin i g./day with I.N.A.H. 300 mg./day were also given lest the condition be primarilytuberculous. By 22nd June, despite apparently adequatechemotherapy, the staphylococcus was sensitive only tomethicillin. At this stage, in an attempt to excludetracking of infection from an extrapericardial source,35 ml. of 'Hypaque 70' at 370 C. were injected into thepericardium; subsequent X-rays (Fig. 2) showed anintact pericardium. As anxiety was still felt about thediagnosis and the course of the illness which did notseem to be like that of a pyogenic pericarditis, bron-choscopy was carried out on 22.6.6I. The right lowerlobe bronchus was seen to be compressed, but no otherabnormality was observed.
Right thoracotomy (Mr. H. R. S. Harley) wasperformed immediately after bronchoscopy. The wholemediastinum from the apex of the heart to the azygosvein was densely hard and infiltrated with fibrous tissue.The superior vena cava was dilated and tense and didnot deflate when the pericardium was opened. Thepericardial sac contained two litres of yellow fluid. Theheart was normal in size. The appearances were thoughtto be suggestive of malignant disease. In view of thenecessity for repeated pericardial aspirations, a windowwas made from the pericardium into the right pleural sac.A biopsy taken from the mediastinum showed organisingpericarditis and mediastinitis only.
Post-operative course was uneventful, and no furtherparacentesis was necessary. On the eighth post-
..: ....::.:.. . .. ... ....... .. . . . . . . . . . . ... . . ...
:. .....:
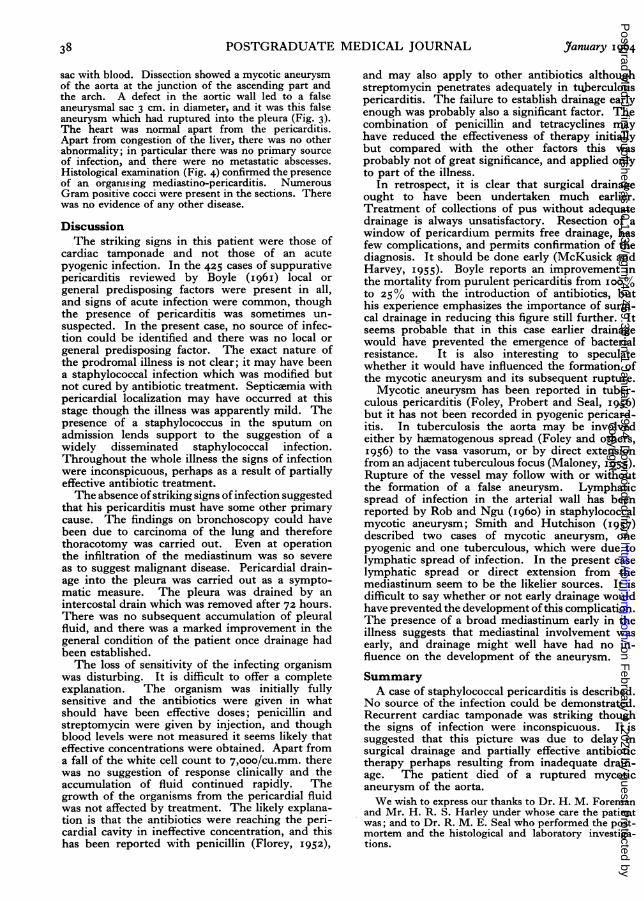
FIG. 3.-The heart and great vessels. The very severefibrinous pericarditis is clearly seen. The rupturedfalse aneurysm is shown by the arrow.
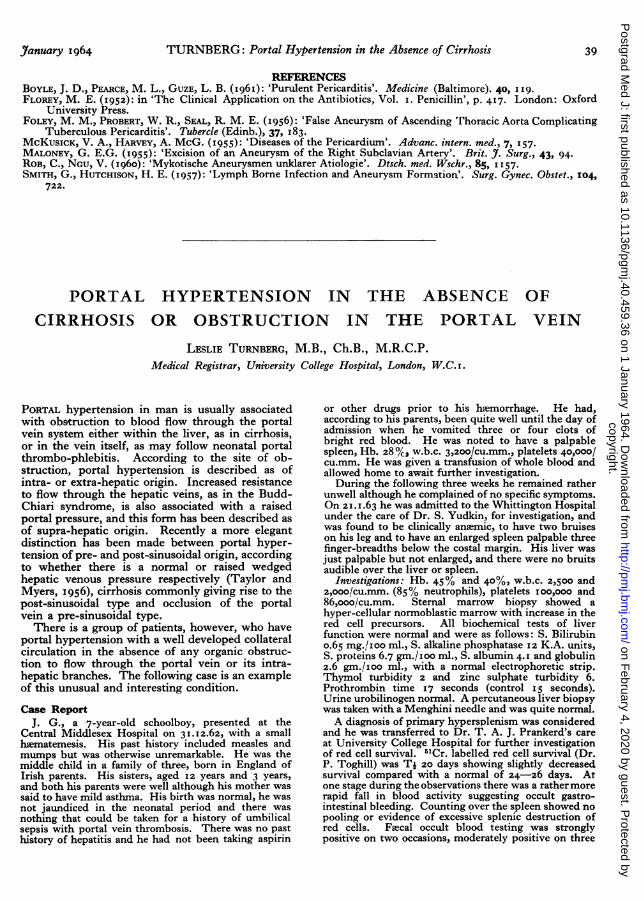
FIG 4 Superficial myocardium, epicardium andpericardium (low power, H. and E.). Inflammatorychanges involving the superficial parts of themyocardium, thickening of the epicardium, andfibrosis thickening and chronic inflammation of thepericardium.
operative day, the patient suddenly collapsed and diedwithin thirty minutes. There was marked pallor suggest-ing blood loss. Vigorous attempts at resuscitation wereunsuccessful.
Autopsy (Dr. R. M. E. Seal). The pericardium wasgreatly thickened and showed signs of inflammation;the mediastinum was much indurated. In the rightside of the superior mediastinum, there was a fluctuanthemorrhagic mass, which had ruptured into the pleuralcavity above the azygos vein, filling the right pleural
copyright. on F
ebruary 4, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.40.459.36 on 1 January 1964. D
ownloaded from
POSTGRADUATE MEDICAL JOURNAL
sac with blood. Dissection showed a mycotic aneurysmof the aorta at the junction of the ascending part andthe arch. A defect in the aortic wall led to a falseaneurysmal sac 3 cm. in diameter, and it was this falseaneurysm which had ruptured into the pleura (Fig. 3).The heart was normal apart from the pericarditis.Apart from congestion of the liver, there was no otherabnormality; in particular there was no primary sourceof infection, and there were no metastatic abscesses.Histological examination (Fig. 4) confirmed the presenceof an organising mediastino-pericarditis. NumerousGram positive cocci were present in the sections. Therewas no evidence of any other disease.
DiscussionThe striking signs in this patient were those of
cardiac tamponade and not those of an acutepyogenic infection. In the 425 cases of suppurativepericarditis reviewed by Boyle (I96I) local orgeneral predisposing factors were present in all,and signs of acute infection were common, thoughthe presence of pericarditis was sometimes un-suspected. In the present case, no source of infec-tion could be identified and there was no local orgeneral predisposing factor. The exact nature ofthe prodromal illness is not clear; it may have beena staphylococcal infection which was modified butnot cured by antibiotic treatment. Septiczemia withpericardial localization may have occurred at thisstage though the illness was apparently mild. Thepresence of a staphylococcus in the sputum onadmission lends support to the suggestion of awidely disseminated staphylococcal infection.Throughout the whole illness the signs of infectionwere inconspicuous, perhaps as a result of partiallyeffective antibiotic treatment.The absence of striking signs of infection suggested
that his pericarditis must have some other primarycause. The findings on bronchoscopy could havebeen due to carcinoma of the lung and thereforethoracotomy was carried out. Even at operationthe infiltration of the mediastinum was so severeas to suggest malignant disease. Pericardial drain-age into the pleura was carried out as a sympto-matic measure. The pleura was drained by anintercostal drain which was removed after 72 hours.There was no subsequent accumulation of pleuralfluid, and there was a marked improvement in thegeneral condition of the patient once drainage hadbeen established.The loss of sensitivity of the infecting organism
was disturbing. It is difficult to offer a completeexplanation. The organism was initially fullysensitive and the antibiotics were given in whatshould have been effective doses; penicillin andstreptomycin were given by injection, and thoughblood levels were not measured it seems likely thateffective concentrations were obtained. Apart froma fall of the white cell count to 7,ooo/cu.mm. therewas no suggestion of response clinically and theaccumulation of fluid continued rapidly. Thegrowth of the organisms from the pericardial fluidwas not affected by treatment. The likely explana-tion is that the antibiotics were reaching the peri-cardial cavity in ineffective concentration, and thishas been reported with penicillin (Florey, I952),
and may also apply to other antibiotics althoughstreptomycin penetrates adequately in tuberculouspericarditis. The failure to establish drainage earlyenough was probably also a significant factor. Thecombination of penicillin and tetracyclines mayhave reduced the effectiveness of therapy initiallybut compared with the other factors this wasprobably not of great significance, and applied onlyto part of the illness.
In retrospect, it is clear that surgical drainageought to have been undertaken much earlier.Treatment of collections of pus without adequatedrainage is always unsatisfactory. Resection of awindow of pericardium permits free drainage, hasfew complications, and permits confirmation of thediagnosis. It should be done early (McKusick andHarvey, I955). Boyle reports an improvement inthe mortality from purulent pericarditis from ioo%to 25% with the introduction of antibiotics, buthis experience emphasizes the importance of surgi-cal drainage in reducing this figure still further. Itseems probable that in this case earlier drainagewould have prevented the emergence of bacterialresistance. It is also interesting to speculatewhether it would have influenced the formation ofthe mycotic aneurysm and its subsequent rupture.
Mycotic aneurysm has been reported in tuber-culous pericarditis (Foley, Probert and Seal, 1956)but it has not been recorded in pyogenic pericard-itis. In tuberculosis the aorta may be involvedeither by heematogenous spread (Foley and others,I956) to the vasa vasorum, or by direct extensionfrom an adjacent tuberculous focus (Maloney, I955).Rupture of the vessel may follow with or withoutthe formation of a false aneurysm. Lymphaticspread of infection in the arterial wall has beenreported by Rob and Ngu (I960) in staphylococcalmycotic aneurysm; Smith and Hutchison (I'957)described two cases of mycotic aneurysm, onepyogenic and one tuberculous, which were due tolymphatic spread of infection. In the present caselymphatic spread or direct extension from themediastinum seem to be the likelier sources. It isdifficult to say whether or not early drainage wouldhave prevented the development of this complication.The presence of a broad mediastinum early in theillness suggests that mediastinal involvement wasearly, and drainage might well have had no in-fluence on the development of the aneurysm.
SummaryA case of staphylococcal pericarditis is described.
No source of the infection could be demonstrated.Recurrent cardiac tamponade was striking thoughthe signs of infection were inconspicuous. It issuggested that this picture was due to delay insurgical drainage and partially effective antibiotictherapy perhaps resulting from inadequate drain-age. The patient died of a ruptured mycoticaneurysm of the aorta.We wish to express our thanks to Dr. H. M. Foreman
and Mr. H. R. S. Harley under who3e care the patientwas; and to Dr. R. M. E. Seal who performed the post-mortem and the histological and laboratory investiga-tions.
38 ,7anuary 1964copyright.
on February 4, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.40.459.36 on 1 January 1964. Dow
nloaded from
January 1964 TURNBERG: Portal Hypertension in the Absence of Cirrhosis 39
REFERENCESBOYLE, J. D., PEARCE, M. L., GUZE, L. B. (I96I): 'Purulent Pericarditis'. Medicine (Baltimore). 40, I19.FLOREY, M. E. (1952): in 'The Clinical Application on the Antibiotics, Vol. i. Penicillin', p. 417. London: Oxford
University Press.Foixy, M. M., PROBERT, W. R., SEAL, R. M. E. (I956): 'False Aneurysm of Ascending rhoracic Aorta Complicating
Tuberculous Pericarditis'. Tubercle (Edinb.), 37, I83.McKusICK, V. A., HARvEY, A. McG. (1955): 'Diseases of the Pericardium'. Advanc. intern. med., 7, I57.MALONEY, G. E.G. (1955): 'Excision of an Aneurysm of the Right Subclavian Artery'. Brit. 5t. Surg., 43, 94.ROB, C., NGU, V. (I960): 'Mykotische Aneurysmen unklarer Atiologie'. Dtsch. med. Wschr., 85, I157.SMITH, G., HUTCHISON, H. E. (1957): 'Lymph Borne Infection and Aneurysm Formation'. Surg. Gynec. Obstet., 104,
722.
PORTAL HYPERTENSION IN THE ABSENCE OFCIRRHOSIS OR OBSTRUCTION IN THE PORTAL VEIN
LESLIE TURNBERG, M.B., Ch.B., M.R.C.P.Medical Registrar, University College Hospital, London, W.C.I.
PORTAL hypertension in man is usually associatedwith obstruction to blood flow through the portalvein system either within the liver, as in cirrhosis,or in the vein itself, as may follow neonatal portalthrombo-phlebitis. According to the site of ob-struction, portal hypertension is described as ofintra- or extra-hepatic origin. Increased resistanceto flow through the hepatic veins, as in the Budd-Chiari syndrome, is also associated with a raisedportal pressure, and this form has been described asof supra-hepatic origin. Recently a more elegantdistinction has been made between portal hyper-tension of pre- and post-sinusoidal origin, accordingto whether there is a normal or raised wedgedhepatic venous pressure respectively (Taylor andMyers, 1956), cirrhosis commonly giving rise to thepost-sinusoidal type and occlusion of the portalvein a pre-sinusoidal type.There is a group of patients, however, who have
portal hypertension with a well developed collateralcirculation in the absence of any organic obstruc-tion to flow through the portal vein or its intra-hepatic branches. The following case is an exampleof this unusual and interesting condition.
Case ReportJ. G., a 7-year-old schoolboy, presented at the
Central Middlesex Hospital on 31.12.62, with a smallhlimatemesis. His past history included measles andmumps but was otherwise unremarkable. He was themiddle child in a family of three, born in England ofIrish parents. His sisters, aged I2 years and 3 years,and both his parents were well although his mother wassaid to have mild asthma. His birth was normal, he wasnot jaundiced in the neonatal period and there wasnothing that could be taken for a history of umbilicalsepsis with portal vein thrombosis. There was no pasthistory of hepatitis and he had not been taking aspirin
or other drugs prior to his hoemorrhage. He had,according to his parents, been quite well until the day ofadmission when he vomited three or four clots ofbright red blood. He was noted to have a palpablespleen, Hb. 28 0/c w.b.c. 3,200/cu.mm., platelets 40,000/cu.mm. He was given a transfusion of whole blood andallowed home to await further investigation.During the following three weeks he remained rather
unwell although he complained of no specific symptoms.On 21.I.63 he was admitted to the Whittington Hospitalunder the care of Dr. S. Yudkin, for investigation, andwas found to be clinically anemic, to have two bruiseson his leg and to have an enlarged spleen palpable threefinger-breadths below the costal margin. His liver wasjust palpable but not enlarged, and there were no bruitsaudible over the liver or spleen.
Investigations: Hb. 45% and 40%, w.b.c. 2,500 and2,000/cu.mm. (85% neutrophils), platelets ioo,ooo and86,ooo/cu.mm. Sternal marrow biopsy showed ahyper-cellular normoblastic marrow with increase in thered cell precursors. All biochemical tests of liverfunction were normal and were as follows: S. Bilirubino.65 mg./ioo ml., S. alkaline phosphatase 12 K.A. units,S. proteins 6.7 gm./Ioo ml., S. albumin 4.I and globulin2.6 gm./ioo ml., with a normal electrophoretic strip.Thymol turbidity 2 and zinc sulphate turbidity 6.Prothrombin time I7 seconds (control I5 seconds).Urine urobilinogen normal. A percutaneous liver biopsywas taken with a Menghini needle and was quite normal.A diagnosis of primary hypersplenism was considered
and he was transferred to Dr. T. A. J. Prankerd's careat University College Hospital for further investigationof red cell survival. 5'Cr. labelled red cell survival (Dr.P. Toghill) was Ti 20 days showing slightly decreasedsurvival compared with a normal of 24-26 days. Atone stage during the observations there was a rather morerapid fall in blood activity suggesting occult gastro-intestinal bleeding. Counting over the spleen showed nopooling or evidence of excessive splenic destruction ofred cells. Feecal occult blood testing was stronglypositive on two occasions, moderately positive on three
copyright. on F
ebruary 4, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.40.459.36 on 1 January 1964. D
ownloaded from
Top Related