





Languages
Pages
Legal


Acute Stroke Management
an ED perspective
Tanya Frost
Acute Stroke Nurse
Eastern Health
Overview
bull Little about me
bull Stroke Care aims
bull Treatments
bull Streamline of service regardless of access
bull Treatment Times
Box Hill Hospital
bull Primary Stroke Centre
bull Situated in the Eastern Suburbs of Melbourne
bull 621 Bed tertiary Hospital (Monash University)
bull Catchment = 2800km Population = 850000
Maroondah Hospital
bull A little further outhellip Eastern Suburbs
bull Even further outhellip Eastern Suburbs
Angliss Hospital
Stroke is a medical emergency
bull Second largest cause of death
bull Leading cause of disability
bull 15th of all strokes occur in people under 55 years old
bull 15th die within 1 month
bull 13rd die within 12 months
bull 88 of survivors live at homendash Most with persistent disability
bull Cost burden of asymp $214 billionyear
Stroke Care
bull Recognition of Symptoms
ndash Access help
bull Diagnose stroke
ndash where is the lesion
ndash Focal neurological signs
bull Treat as able
ndash tPA
ndash ECR
ndash Fever Sugar Temperature
access tohellip
bull Stroke Unit Care
bull Secondary Prevention
ndash Medications
ndash Education
ndash Risk Factor modification
bull Mechanism
ndash Large Vessel
ndash Cardio embolic
ndash Small artery occlusion
ndash Stroke of other determined
etiology
ndash Stroke of undertermined
etiology
ndash Unknown
bull Allied Health
Research
What is strokehellip
Acute loss of oxygen supply
Therefore the aim is
Return of oxygen supply
tPA
bull Thrombolytic given within 45hrs of Sx onset
bull Not appropriate for every patient
bull Angioedema 1-2
ndash Associated with ACEi use
ndash Antihistamine and steroid
bull Bleeding Risk
ndash Symptomatic Haemorrhage 4-6
ndash Other bleeding
ECR
bull Endovascular clot retrieval
ECR Suitability
Slid
e u
se
d w
ith
pe
rmis
sio
n o
f D
r B
ruce
Cam
pb
ell
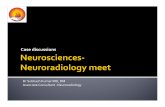
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Boehringer Ingelheim
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Skye Coote
The ldquogolden half-hourrdquo
T= -10
Suspected
stroke patient
hospital
pre-notification
Stroke team
Notified
0 min
Patient arrives
Met at triage by
stroke and ED team
le 10 min
Triage
direct-to-CT
rapid (basic)
stroke assessment
IVB
le 25 min
CT scan
completed amp
interpreted
le 30 min
t-PA
given if patient
is eligible
Slide courtesy of Skye Coote
bull Pts who arrive within
the golden hour are
twice as likely to be
treated
bull Improved patient
outcomes
andhellip
bull Walk out of hospital
Identification of Stroke
bull An immediate life threatening emergency
needing an ambulance may include
Ambiguous stroke Sx
bull Dizziness
bull Drowsiness
bull Visual disturbance
bull Ataxia
bull Numbness
bull Tingling
bull Canrsquot understand surroundings
Ambulance Pre-notification
bull Patients name amp DOB
bull Quick story
ndash Symptoms
ndash Time of onset
ndash Vitals signs amp GCS
bull 18G IVC (if able)
bull ED ldquoCode strokerdquo paged
bull CT freed
bull Labels created
bull Pt remains on AV monitor
Code Stroke
bull Pt met at door by
ndash Stroke Nurse
ndash Stroke Registrar
ndash HMO
bull Assessed for suitability for
direct to CT
ndash ABCD (Brief)
ndash Verify patient details- labels
ndash Triage is brief (Cat 2)
Direct to CT
bull Walk and Talk stroke assessments
bull Senior clinician begins assessing
bull Pt transferred onto CT table
ndash Off stretcher time
bull Non Contrast CT Brain
ndash Rule out blood
ndash HMO ndash IVC and pathology
bull Red stream staff bring equipment
ndash Trolley airway basket monitoring
bull CT Angiogram amp Perfusion
ndash Routine investigation
CT interpretation
bull Real time review
bull NIHSS- stroke
assessments continue
bull Call to Consultant
bull Swap monitors
bull Contact familyGP
bull tPA decision made
ndash Give tPA on CT table
ndash Must have all informationhellip
bull LVO- ECR consideration
Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

Overview
bull Little about me
bull Stroke Care aims
bull Treatments
bull Streamline of service regardless of access
bull Treatment Times
Box Hill Hospital
bull Primary Stroke Centre
bull Situated in the Eastern Suburbs of Melbourne
bull 621 Bed tertiary Hospital (Monash University)
bull Catchment = 2800km Population = 850000
Maroondah Hospital
bull A little further outhellip Eastern Suburbs
bull Even further outhellip Eastern Suburbs
Angliss Hospital
Stroke is a medical emergency
bull Second largest cause of death
bull Leading cause of disability
bull 15th of all strokes occur in people under 55 years old
bull 15th die within 1 month
bull 13rd die within 12 months
bull 88 of survivors live at homendash Most with persistent disability
bull Cost burden of asymp $214 billionyear
Stroke Care
bull Recognition of Symptoms
ndash Access help
bull Diagnose stroke
ndash where is the lesion
ndash Focal neurological signs
bull Treat as able
ndash tPA
ndash ECR
ndash Fever Sugar Temperature
access tohellip
bull Stroke Unit Care
bull Secondary Prevention
ndash Medications
ndash Education
ndash Risk Factor modification
bull Mechanism
ndash Large Vessel
ndash Cardio embolic
ndash Small artery occlusion
ndash Stroke of other determined
etiology
ndash Stroke of undertermined
etiology
ndash Unknown
bull Allied Health
Research
What is strokehellip
Acute loss of oxygen supply
Therefore the aim is
Return of oxygen supply
tPA
bull Thrombolytic given within 45hrs of Sx onset
bull Not appropriate for every patient
bull Angioedema 1-2
ndash Associated with ACEi use
ndash Antihistamine and steroid
bull Bleeding Risk
ndash Symptomatic Haemorrhage 4-6
ndash Other bleeding
ECR
bull Endovascular clot retrieval
ECR Suitability
Slid
e u
se
d w
ith
pe
rmis
sio
n o
f D
r B
ruce
Cam
pb
ell
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Boehringer Ingelheim
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Skye Coote
The ldquogolden half-hourrdquo
T= -10
Suspected
stroke patient
hospital
pre-notification
Stroke team
Notified
0 min
Patient arrives
Met at triage by
stroke and ED team
le 10 min
Triage
direct-to-CT
rapid (basic)
stroke assessment
IVB
le 25 min
CT scan
completed amp
interpreted
le 30 min
t-PA
given if patient
is eligible
Slide courtesy of Skye Coote
bull Pts who arrive within
the golden hour are
twice as likely to be
treated
bull Improved patient
outcomes
andhellip
bull Walk out of hospital
Identification of Stroke
bull An immediate life threatening emergency
needing an ambulance may include
Ambiguous stroke Sx
bull Dizziness
bull Drowsiness
bull Visual disturbance
bull Ataxia
bull Numbness
bull Tingling
bull Canrsquot understand surroundings
Ambulance Pre-notification
bull Patients name amp DOB
bull Quick story
ndash Symptoms
ndash Time of onset
ndash Vitals signs amp GCS
bull 18G IVC (if able)
bull ED ldquoCode strokerdquo paged
bull CT freed
bull Labels created
bull Pt remains on AV monitor
Code Stroke
bull Pt met at door by
ndash Stroke Nurse
ndash Stroke Registrar
ndash HMO
bull Assessed for suitability for
direct to CT
ndash ABCD (Brief)
ndash Verify patient details- labels
ndash Triage is brief (Cat 2)
Direct to CT
bull Walk and Talk stroke assessments
bull Senior clinician begins assessing
bull Pt transferred onto CT table
ndash Off stretcher time
bull Non Contrast CT Brain
ndash Rule out blood
ndash HMO ndash IVC and pathology
bull Red stream staff bring equipment
ndash Trolley airway basket monitoring
bull CT Angiogram amp Perfusion
ndash Routine investigation
CT interpretation
bull Real time review
bull NIHSS- stroke
assessments continue
bull Call to Consultant
bull Swap monitors
bull Contact familyGP
bull tPA decision made
ndash Give tPA on CT table
ndash Must have all informationhellip
bull LVO- ECR consideration
Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

Box Hill Hospital
bull Primary Stroke Centre
bull Situated in the Eastern Suburbs of Melbourne
bull 621 Bed tertiary Hospital (Monash University)
bull Catchment = 2800km Population = 850000
Maroondah Hospital
bull A little further outhellip Eastern Suburbs
bull Even further outhellip Eastern Suburbs
Angliss Hospital
Stroke is a medical emergency
bull Second largest cause of death
bull Leading cause of disability
bull 15th of all strokes occur in people under 55 years old
bull 15th die within 1 month
bull 13rd die within 12 months
bull 88 of survivors live at homendash Most with persistent disability
bull Cost burden of asymp $214 billionyear
Stroke Care
bull Recognition of Symptoms
ndash Access help
bull Diagnose stroke
ndash where is the lesion
ndash Focal neurological signs
bull Treat as able
ndash tPA
ndash ECR
ndash Fever Sugar Temperature
access tohellip
bull Stroke Unit Care
bull Secondary Prevention
ndash Medications
ndash Education
ndash Risk Factor modification
bull Mechanism
ndash Large Vessel
ndash Cardio embolic
ndash Small artery occlusion
ndash Stroke of other determined
etiology
ndash Stroke of undertermined
etiology
ndash Unknown
bull Allied Health
Research
What is strokehellip
Acute loss of oxygen supply
Therefore the aim is
Return of oxygen supply
tPA
bull Thrombolytic given within 45hrs of Sx onset
bull Not appropriate for every patient
bull Angioedema 1-2
ndash Associated with ACEi use
ndash Antihistamine and steroid
bull Bleeding Risk
ndash Symptomatic Haemorrhage 4-6
ndash Other bleeding
ECR
bull Endovascular clot retrieval
ECR Suitability
Slid
e u
se
d w
ith
pe
rmis
sio
n o
f D
r B
ruce
Cam
pb
ell
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Boehringer Ingelheim
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Skye Coote
The ldquogolden half-hourrdquo
T= -10
Suspected
stroke patient
hospital
pre-notification
Stroke team
Notified
0 min
Patient arrives
Met at triage by
stroke and ED team
le 10 min
Triage
direct-to-CT
rapid (basic)
stroke assessment
IVB
le 25 min
CT scan
completed amp
interpreted
le 30 min
t-PA
given if patient
is eligible
Slide courtesy of Skye Coote
bull Pts who arrive within
the golden hour are
twice as likely to be
treated
bull Improved patient
outcomes
andhellip
bull Walk out of hospital
Identification of Stroke
bull An immediate life threatening emergency
needing an ambulance may include
Ambiguous stroke Sx
bull Dizziness
bull Drowsiness
bull Visual disturbance
bull Ataxia
bull Numbness
bull Tingling
bull Canrsquot understand surroundings
Ambulance Pre-notification
bull Patients name amp DOB
bull Quick story
ndash Symptoms
ndash Time of onset
ndash Vitals signs amp GCS
bull 18G IVC (if able)
bull ED ldquoCode strokerdquo paged
bull CT freed
bull Labels created
bull Pt remains on AV monitor
Code Stroke
bull Pt met at door by
ndash Stroke Nurse
ndash Stroke Registrar
ndash HMO
bull Assessed for suitability for
direct to CT
ndash ABCD (Brief)
ndash Verify patient details- labels
ndash Triage is brief (Cat 2)
Direct to CT
bull Walk and Talk stroke assessments
bull Senior clinician begins assessing
bull Pt transferred onto CT table
ndash Off stretcher time
bull Non Contrast CT Brain
ndash Rule out blood
ndash HMO ndash IVC and pathology
bull Red stream staff bring equipment
ndash Trolley airway basket monitoring
bull CT Angiogram amp Perfusion
ndash Routine investigation
CT interpretation
bull Real time review
bull NIHSS- stroke
assessments continue
bull Call to Consultant
bull Swap monitors
bull Contact familyGP
bull tPA decision made
ndash Give tPA on CT table
ndash Must have all informationhellip
bull LVO- ECR consideration
Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

Maroondah Hospital
bull A little further outhellip Eastern Suburbs
bull Even further outhellip Eastern Suburbs
Angliss Hospital
Stroke is a medical emergency
bull Second largest cause of death
bull Leading cause of disability
bull 15th of all strokes occur in people under 55 years old
bull 15th die within 1 month
bull 13rd die within 12 months
bull 88 of survivors live at homendash Most with persistent disability
bull Cost burden of asymp $214 billionyear
Stroke Care
bull Recognition of Symptoms
ndash Access help
bull Diagnose stroke
ndash where is the lesion
ndash Focal neurological signs
bull Treat as able
ndash tPA
ndash ECR
ndash Fever Sugar Temperature
access tohellip
bull Stroke Unit Care
bull Secondary Prevention
ndash Medications
ndash Education
ndash Risk Factor modification
bull Mechanism
ndash Large Vessel
ndash Cardio embolic
ndash Small artery occlusion
ndash Stroke of other determined
etiology
ndash Stroke of undertermined
etiology
ndash Unknown
bull Allied Health
Research
What is strokehellip
Acute loss of oxygen supply
Therefore the aim is
Return of oxygen supply
tPA
bull Thrombolytic given within 45hrs of Sx onset
bull Not appropriate for every patient
bull Angioedema 1-2
ndash Associated with ACEi use
ndash Antihistamine and steroid
bull Bleeding Risk
ndash Symptomatic Haemorrhage 4-6
ndash Other bleeding
ECR
bull Endovascular clot retrieval
ECR Suitability
Slid
e u
se
d w
ith
pe
rmis
sio
n o
f D
r B
ruce
Cam
pb
ell
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Boehringer Ingelheim
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Skye Coote
The ldquogolden half-hourrdquo
T= -10
Suspected
stroke patient
hospital
pre-notification
Stroke team
Notified
0 min
Patient arrives
Met at triage by
stroke and ED team
le 10 min
Triage
direct-to-CT
rapid (basic)
stroke assessment
IVB
le 25 min
CT scan
completed amp
interpreted
le 30 min
t-PA
given if patient
is eligible
Slide courtesy of Skye Coote
bull Pts who arrive within
the golden hour are
twice as likely to be
treated
bull Improved patient
outcomes
andhellip
bull Walk out of hospital
Identification of Stroke
bull An immediate life threatening emergency
needing an ambulance may include
Ambiguous stroke Sx
bull Dizziness
bull Drowsiness
bull Visual disturbance
bull Ataxia
bull Numbness
bull Tingling
bull Canrsquot understand surroundings
Ambulance Pre-notification
bull Patients name amp DOB
bull Quick story
ndash Symptoms
ndash Time of onset
ndash Vitals signs amp GCS
bull 18G IVC (if able)
bull ED ldquoCode strokerdquo paged
bull CT freed
bull Labels created
bull Pt remains on AV monitor
Code Stroke
bull Pt met at door by
ndash Stroke Nurse
ndash Stroke Registrar
ndash HMO
bull Assessed for suitability for
direct to CT
ndash ABCD (Brief)
ndash Verify patient details- labels
ndash Triage is brief (Cat 2)
Direct to CT
bull Walk and Talk stroke assessments
bull Senior clinician begins assessing
bull Pt transferred onto CT table
ndash Off stretcher time
bull Non Contrast CT Brain
ndash Rule out blood
ndash HMO ndash IVC and pathology
bull Red stream staff bring equipment
ndash Trolley airway basket monitoring
bull CT Angiogram amp Perfusion
ndash Routine investigation
CT interpretation
bull Real time review
bull NIHSS- stroke
assessments continue
bull Call to Consultant
bull Swap monitors
bull Contact familyGP
bull tPA decision made
ndash Give tPA on CT table
ndash Must have all informationhellip
bull LVO- ECR consideration
Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

Stroke is a medical emergency
bull Second largest cause of death
bull Leading cause of disability
bull 15th of all strokes occur in people under 55 years old
bull 15th die within 1 month
bull 13rd die within 12 months
bull 88 of survivors live at homendash Most with persistent disability
bull Cost burden of asymp $214 billionyear
Stroke Care
bull Recognition of Symptoms
ndash Access help
bull Diagnose stroke
ndash where is the lesion
ndash Focal neurological signs
bull Treat as able
ndash tPA
ndash ECR
ndash Fever Sugar Temperature
access tohellip
bull Stroke Unit Care
bull Secondary Prevention
ndash Medications
ndash Education
ndash Risk Factor modification
bull Mechanism
ndash Large Vessel
ndash Cardio embolic
ndash Small artery occlusion
ndash Stroke of other determined
etiology
ndash Stroke of undertermined
etiology
ndash Unknown
bull Allied Health
Research
What is strokehellip
Acute loss of oxygen supply
Therefore the aim is
Return of oxygen supply
tPA
bull Thrombolytic given within 45hrs of Sx onset
bull Not appropriate for every patient
bull Angioedema 1-2
ndash Associated with ACEi use
ndash Antihistamine and steroid
bull Bleeding Risk
ndash Symptomatic Haemorrhage 4-6
ndash Other bleeding
ECR
bull Endovascular clot retrieval
ECR Suitability
Slid
e u
se
d w
ith
pe
rmis
sio
n o
f D
r B
ruce
Cam
pb
ell
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Boehringer Ingelheim
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Skye Coote
The ldquogolden half-hourrdquo
T= -10
Suspected
stroke patient
hospital
pre-notification
Stroke team
Notified
0 min
Patient arrives
Met at triage by
stroke and ED team
le 10 min
Triage
direct-to-CT
rapid (basic)
stroke assessment
IVB
le 25 min
CT scan
completed amp
interpreted
le 30 min
t-PA
given if patient
is eligible
Slide courtesy of Skye Coote
bull Pts who arrive within
the golden hour are
twice as likely to be
treated
bull Improved patient
outcomes
andhellip
bull Walk out of hospital
Identification of Stroke
bull An immediate life threatening emergency
needing an ambulance may include
Ambiguous stroke Sx
bull Dizziness
bull Drowsiness
bull Visual disturbance
bull Ataxia
bull Numbness
bull Tingling
bull Canrsquot understand surroundings
Ambulance Pre-notification
bull Patients name amp DOB
bull Quick story
ndash Symptoms
ndash Time of onset
ndash Vitals signs amp GCS
bull 18G IVC (if able)
bull ED ldquoCode strokerdquo paged
bull CT freed
bull Labels created
bull Pt remains on AV monitor
Code Stroke
bull Pt met at door by
ndash Stroke Nurse
ndash Stroke Registrar
ndash HMO
bull Assessed for suitability for
direct to CT
ndash ABCD (Brief)
ndash Verify patient details- labels
ndash Triage is brief (Cat 2)
Direct to CT
bull Walk and Talk stroke assessments
bull Senior clinician begins assessing
bull Pt transferred onto CT table
ndash Off stretcher time
bull Non Contrast CT Brain
ndash Rule out blood
ndash HMO ndash IVC and pathology
bull Red stream staff bring equipment
ndash Trolley airway basket monitoring
bull CT Angiogram amp Perfusion
ndash Routine investigation
CT interpretation
bull Real time review
bull NIHSS- stroke
assessments continue
bull Call to Consultant
bull Swap monitors
bull Contact familyGP
bull tPA decision made
ndash Give tPA on CT table
ndash Must have all informationhellip
bull LVO- ECR consideration
Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

Stroke Care
bull Recognition of Symptoms
ndash Access help
bull Diagnose stroke
ndash where is the lesion
ndash Focal neurological signs
bull Treat as able
ndash tPA
ndash ECR
ndash Fever Sugar Temperature
access tohellip
bull Stroke Unit Care
bull Secondary Prevention
ndash Medications
ndash Education
ndash Risk Factor modification
bull Mechanism
ndash Large Vessel
ndash Cardio embolic
ndash Small artery occlusion
ndash Stroke of other determined
etiology
ndash Stroke of undertermined
etiology
ndash Unknown
bull Allied Health
Research
What is strokehellip
Acute loss of oxygen supply
Therefore the aim is
Return of oxygen supply
tPA
bull Thrombolytic given within 45hrs of Sx onset
bull Not appropriate for every patient
bull Angioedema 1-2
ndash Associated with ACEi use
ndash Antihistamine and steroid
bull Bleeding Risk
ndash Symptomatic Haemorrhage 4-6
ndash Other bleeding
ECR
bull Endovascular clot retrieval
ECR Suitability
Slid
e u
se
d w
ith
pe
rmis
sio
n o
f D
r B
ruce
Cam
pb
ell
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Boehringer Ingelheim
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Skye Coote
The ldquogolden half-hourrdquo
T= -10
Suspected
stroke patient
hospital
pre-notification
Stroke team
Notified
0 min
Patient arrives
Met at triage by
stroke and ED team
le 10 min
Triage
direct-to-CT
rapid (basic)
stroke assessment
IVB
le 25 min
CT scan
completed amp
interpreted
le 30 min
t-PA
given if patient
is eligible
Slide courtesy of Skye Coote
bull Pts who arrive within
the golden hour are
twice as likely to be
treated
bull Improved patient
outcomes
andhellip
bull Walk out of hospital
Identification of Stroke
bull An immediate life threatening emergency
needing an ambulance may include
Ambiguous stroke Sx
bull Dizziness
bull Drowsiness
bull Visual disturbance
bull Ataxia
bull Numbness
bull Tingling
bull Canrsquot understand surroundings
Ambulance Pre-notification
bull Patients name amp DOB
bull Quick story
ndash Symptoms
ndash Time of onset
ndash Vitals signs amp GCS
bull 18G IVC (if able)
bull ED ldquoCode strokerdquo paged
bull CT freed
bull Labels created
bull Pt remains on AV monitor
Code Stroke
bull Pt met at door by
ndash Stroke Nurse
ndash Stroke Registrar
ndash HMO
bull Assessed for suitability for
direct to CT
ndash ABCD (Brief)
ndash Verify patient details- labels
ndash Triage is brief (Cat 2)
Direct to CT
bull Walk and Talk stroke assessments
bull Senior clinician begins assessing
bull Pt transferred onto CT table
ndash Off stretcher time
bull Non Contrast CT Brain
ndash Rule out blood
ndash HMO ndash IVC and pathology
bull Red stream staff bring equipment
ndash Trolley airway basket monitoring
bull CT Angiogram amp Perfusion
ndash Routine investigation
CT interpretation
bull Real time review
bull NIHSS- stroke
assessments continue
bull Call to Consultant
bull Swap monitors
bull Contact familyGP
bull tPA decision made
ndash Give tPA on CT table
ndash Must have all informationhellip
bull LVO- ECR consideration
Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

Research
What is strokehellip
Acute loss of oxygen supply
Therefore the aim is
Return of oxygen supply
tPA
bull Thrombolytic given within 45hrs of Sx onset
bull Not appropriate for every patient
bull Angioedema 1-2
ndash Associated with ACEi use
ndash Antihistamine and steroid
bull Bleeding Risk
ndash Symptomatic Haemorrhage 4-6
ndash Other bleeding
ECR
bull Endovascular clot retrieval
ECR Suitability
Slid
e u
se
d w
ith
pe
rmis
sio
n o
f D
r B
ruce
Cam
pb
ell
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Boehringer Ingelheim
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Skye Coote
The ldquogolden half-hourrdquo
T= -10
Suspected
stroke patient
hospital
pre-notification
Stroke team
Notified
0 min
Patient arrives
Met at triage by
stroke and ED team
le 10 min
Triage
direct-to-CT
rapid (basic)
stroke assessment
IVB
le 25 min
CT scan
completed amp
interpreted
le 30 min
t-PA
given if patient
is eligible
Slide courtesy of Skye Coote
bull Pts who arrive within
the golden hour are
twice as likely to be
treated
bull Improved patient
outcomes
andhellip
bull Walk out of hospital
Identification of Stroke
bull An immediate life threatening emergency
needing an ambulance may include
Ambiguous stroke Sx
bull Dizziness
bull Drowsiness
bull Visual disturbance
bull Ataxia
bull Numbness
bull Tingling
bull Canrsquot understand surroundings
Ambulance Pre-notification
bull Patients name amp DOB
bull Quick story
ndash Symptoms
ndash Time of onset
ndash Vitals signs amp GCS
bull 18G IVC (if able)
bull ED ldquoCode strokerdquo paged
bull CT freed
bull Labels created
bull Pt remains on AV monitor
Code Stroke
bull Pt met at door by
ndash Stroke Nurse
ndash Stroke Registrar
ndash HMO
bull Assessed for suitability for
direct to CT
ndash ABCD (Brief)
ndash Verify patient details- labels
ndash Triage is brief (Cat 2)
Direct to CT
bull Walk and Talk stroke assessments
bull Senior clinician begins assessing
bull Pt transferred onto CT table
ndash Off stretcher time
bull Non Contrast CT Brain
ndash Rule out blood
ndash HMO ndash IVC and pathology
bull Red stream staff bring equipment
ndash Trolley airway basket monitoring
bull CT Angiogram amp Perfusion
ndash Routine investigation
CT interpretation
bull Real time review
bull NIHSS- stroke
assessments continue
bull Call to Consultant
bull Swap monitors
bull Contact familyGP
bull tPA decision made
ndash Give tPA on CT table
ndash Must have all informationhellip
bull LVO- ECR consideration
Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

What is strokehellip
Acute loss of oxygen supply
Therefore the aim is
Return of oxygen supply
tPA
bull Thrombolytic given within 45hrs of Sx onset
bull Not appropriate for every patient
bull Angioedema 1-2
ndash Associated with ACEi use
ndash Antihistamine and steroid
bull Bleeding Risk
ndash Symptomatic Haemorrhage 4-6
ndash Other bleeding
ECR
bull Endovascular clot retrieval
ECR Suitability
Slid
e u
se
d w
ith
pe
rmis
sio
n o
f D
r B
ruce
Cam
pb
ell
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Boehringer Ingelheim
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Skye Coote
The ldquogolden half-hourrdquo
T= -10
Suspected
stroke patient
hospital
pre-notification
Stroke team
Notified
0 min
Patient arrives
Met at triage by
stroke and ED team
le 10 min
Triage
direct-to-CT
rapid (basic)
stroke assessment
IVB
le 25 min
CT scan
completed amp
interpreted
le 30 min
t-PA
given if patient
is eligible
Slide courtesy of Skye Coote
bull Pts who arrive within
the golden hour are
twice as likely to be
treated
bull Improved patient
outcomes
andhellip
bull Walk out of hospital
Identification of Stroke
bull An immediate life threatening emergency
needing an ambulance may include
Ambiguous stroke Sx
bull Dizziness
bull Drowsiness
bull Visual disturbance
bull Ataxia
bull Numbness
bull Tingling
bull Canrsquot understand surroundings
Ambulance Pre-notification
bull Patients name amp DOB
bull Quick story
ndash Symptoms
ndash Time of onset
ndash Vitals signs amp GCS
bull 18G IVC (if able)
bull ED ldquoCode strokerdquo paged
bull CT freed
bull Labels created
bull Pt remains on AV monitor
Code Stroke
bull Pt met at door by
ndash Stroke Nurse
ndash Stroke Registrar
ndash HMO
bull Assessed for suitability for
direct to CT
ndash ABCD (Brief)
ndash Verify patient details- labels
ndash Triage is brief (Cat 2)
Direct to CT
bull Walk and Talk stroke assessments
bull Senior clinician begins assessing
bull Pt transferred onto CT table
ndash Off stretcher time
bull Non Contrast CT Brain
ndash Rule out blood
ndash HMO ndash IVC and pathology
bull Red stream staff bring equipment
ndash Trolley airway basket monitoring
bull CT Angiogram amp Perfusion
ndash Routine investigation
CT interpretation
bull Real time review
bull NIHSS- stroke
assessments continue
bull Call to Consultant
bull Swap monitors
bull Contact familyGP
bull tPA decision made
ndash Give tPA on CT table
ndash Must have all informationhellip
bull LVO- ECR consideration
Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

tPA
bull Thrombolytic given within 45hrs of Sx onset
bull Not appropriate for every patient
bull Angioedema 1-2
ndash Associated with ACEi use
ndash Antihistamine and steroid
bull Bleeding Risk
ndash Symptomatic Haemorrhage 4-6
ndash Other bleeding
ECR
bull Endovascular clot retrieval
ECR Suitability
Slid
e u
se
d w
ith
pe
rmis
sio
n o
f D
r B
ruce
Cam
pb
ell
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Boehringer Ingelheim
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Skye Coote
The ldquogolden half-hourrdquo
T= -10
Suspected
stroke patient
hospital
pre-notification
Stroke team
Notified
0 min
Patient arrives
Met at triage by
stroke and ED team
le 10 min
Triage
direct-to-CT
rapid (basic)
stroke assessment
IVB
le 25 min
CT scan
completed amp
interpreted
le 30 min
t-PA
given if patient
is eligible
Slide courtesy of Skye Coote
bull Pts who arrive within
the golden hour are
twice as likely to be
treated
bull Improved patient
outcomes
andhellip
bull Walk out of hospital
Identification of Stroke
bull An immediate life threatening emergency
needing an ambulance may include
Ambiguous stroke Sx
bull Dizziness
bull Drowsiness
bull Visual disturbance
bull Ataxia
bull Numbness
bull Tingling
bull Canrsquot understand surroundings
Ambulance Pre-notification
bull Patients name amp DOB
bull Quick story
ndash Symptoms
ndash Time of onset
ndash Vitals signs amp GCS
bull 18G IVC (if able)
bull ED ldquoCode strokerdquo paged
bull CT freed
bull Labels created
bull Pt remains on AV monitor
Code Stroke
bull Pt met at door by
ndash Stroke Nurse
ndash Stroke Registrar
ndash HMO
bull Assessed for suitability for
direct to CT
ndash ABCD (Brief)
ndash Verify patient details- labels
ndash Triage is brief (Cat 2)
Direct to CT
bull Walk and Talk stroke assessments
bull Senior clinician begins assessing
bull Pt transferred onto CT table
ndash Off stretcher time
bull Non Contrast CT Brain
ndash Rule out blood
ndash HMO ndash IVC and pathology
bull Red stream staff bring equipment
ndash Trolley airway basket monitoring
bull CT Angiogram amp Perfusion
ndash Routine investigation
CT interpretation
bull Real time review
bull NIHSS- stroke
assessments continue
bull Call to Consultant
bull Swap monitors
bull Contact familyGP
bull tPA decision made
ndash Give tPA on CT table
ndash Must have all informationhellip
bull LVO- ECR consideration
Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

ECR
bull Endovascular clot retrieval
ECR Suitability
Slid
e u
se
d w
ith
pe
rmis
sio
n o
f D
r B
ruce
Cam
pb
ell
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Boehringer Ingelheim
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Skye Coote
The ldquogolden half-hourrdquo
T= -10
Suspected
stroke patient
hospital
pre-notification
Stroke team
Notified
0 min
Patient arrives
Met at triage by
stroke and ED team
le 10 min
Triage
direct-to-CT
rapid (basic)
stroke assessment
IVB
le 25 min
CT scan
completed amp
interpreted
le 30 min
t-PA
given if patient
is eligible
Slide courtesy of Skye Coote
bull Pts who arrive within
the golden hour are
twice as likely to be
treated
bull Improved patient
outcomes
andhellip
bull Walk out of hospital
Identification of Stroke
bull An immediate life threatening emergency
needing an ambulance may include
Ambiguous stroke Sx
bull Dizziness
bull Drowsiness
bull Visual disturbance
bull Ataxia
bull Numbness
bull Tingling
bull Canrsquot understand surroundings
Ambulance Pre-notification
bull Patients name amp DOB
bull Quick story
ndash Symptoms
ndash Time of onset
ndash Vitals signs amp GCS
bull 18G IVC (if able)
bull ED ldquoCode strokerdquo paged
bull CT freed
bull Labels created
bull Pt remains on AV monitor
Code Stroke
bull Pt met at door by
ndash Stroke Nurse
ndash Stroke Registrar
ndash HMO
bull Assessed for suitability for
direct to CT
ndash ABCD (Brief)
ndash Verify patient details- labels
ndash Triage is brief (Cat 2)
Direct to CT
bull Walk and Talk stroke assessments
bull Senior clinician begins assessing
bull Pt transferred onto CT table
ndash Off stretcher time
bull Non Contrast CT Brain
ndash Rule out blood
ndash HMO ndash IVC and pathology
bull Red stream staff bring equipment
ndash Trolley airway basket monitoring
bull CT Angiogram amp Perfusion
ndash Routine investigation
CT interpretation
bull Real time review
bull NIHSS- stroke
assessments continue
bull Call to Consultant
bull Swap monitors
bull Contact familyGP
bull tPA decision made
ndash Give tPA on CT table
ndash Must have all informationhellip
bull LVO- ECR consideration
Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

ECR Suitability
Slid
e u
se
d w
ith
pe
rmis
sio
n o
f D
r B
ruce
Cam
pb
ell
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Boehringer Ingelheim
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Skye Coote
The ldquogolden half-hourrdquo
T= -10
Suspected
stroke patient
hospital
pre-notification
Stroke team
Notified
0 min
Patient arrives
Met at triage by
stroke and ED team
le 10 min
Triage
direct-to-CT
rapid (basic)
stroke assessment
IVB
le 25 min
CT scan
completed amp
interpreted
le 30 min
t-PA
given if patient
is eligible
Slide courtesy of Skye Coote
bull Pts who arrive within
the golden hour are
twice as likely to be
treated
bull Improved patient
outcomes
andhellip
bull Walk out of hospital
Identification of Stroke
bull An immediate life threatening emergency
needing an ambulance may include
Ambiguous stroke Sx
bull Dizziness
bull Drowsiness
bull Visual disturbance
bull Ataxia
bull Numbness
bull Tingling
bull Canrsquot understand surroundings
Ambulance Pre-notification
bull Patients name amp DOB
bull Quick story
ndash Symptoms
ndash Time of onset
ndash Vitals signs amp GCS
bull 18G IVC (if able)
bull ED ldquoCode strokerdquo paged
bull CT freed
bull Labels created
bull Pt remains on AV monitor
Code Stroke
bull Pt met at door by
ndash Stroke Nurse
ndash Stroke Registrar
ndash HMO
bull Assessed for suitability for
direct to CT
ndash ABCD (Brief)
ndash Verify patient details- labels
ndash Triage is brief (Cat 2)
Direct to CT
bull Walk and Talk stroke assessments
bull Senior clinician begins assessing
bull Pt transferred onto CT table
ndash Off stretcher time
bull Non Contrast CT Brain
ndash Rule out blood
ndash HMO ndash IVC and pathology
bull Red stream staff bring equipment
ndash Trolley airway basket monitoring
bull CT Angiogram amp Perfusion
ndash Routine investigation
CT interpretation
bull Real time review
bull NIHSS- stroke
assessments continue
bull Call to Consultant
bull Swap monitors
bull Contact familyGP
bull tPA decision made
ndash Give tPA on CT table
ndash Must have all informationhellip
bull LVO- ECR consideration
Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Boehringer Ingelheim
The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Skye Coote
The ldquogolden half-hourrdquo
T= -10
Suspected
stroke patient
hospital
pre-notification
Stroke team
Notified
0 min
Patient arrives
Met at triage by
stroke and ED team
le 10 min
Triage
direct-to-CT
rapid (basic)
stroke assessment
IVB
le 25 min
CT scan
completed amp
interpreted
le 30 min
t-PA
given if patient
is eligible
Slide courtesy of Skye Coote
bull Pts who arrive within
the golden hour are
twice as likely to be
treated
bull Improved patient
outcomes
andhellip
bull Walk out of hospital
Identification of Stroke
bull An immediate life threatening emergency
needing an ambulance may include
Ambiguous stroke Sx
bull Dizziness
bull Drowsiness
bull Visual disturbance
bull Ataxia
bull Numbness
bull Tingling
bull Canrsquot understand surroundings
Ambulance Pre-notification
bull Patients name amp DOB
bull Quick story
ndash Symptoms
ndash Time of onset
ndash Vitals signs amp GCS
bull 18G IVC (if able)
bull ED ldquoCode strokerdquo paged
bull CT freed
bull Labels created
bull Pt remains on AV monitor
Code Stroke
bull Pt met at door by
ndash Stroke Nurse
ndash Stroke Registrar
ndash HMO
bull Assessed for suitability for
direct to CT
ndash ABCD (Brief)
ndash Verify patient details- labels
ndash Triage is brief (Cat 2)
Direct to CT
bull Walk and Talk stroke assessments
bull Senior clinician begins assessing
bull Pt transferred onto CT table
ndash Off stretcher time
bull Non Contrast CT Brain
ndash Rule out blood
ndash HMO ndash IVC and pathology
bull Red stream staff bring equipment
ndash Trolley airway basket monitoring
bull CT Angiogram amp Perfusion
ndash Routine investigation
CT interpretation
bull Real time review
bull NIHSS- stroke
assessments continue
bull Call to Consultant
bull Swap monitors
bull Contact familyGP
bull tPA decision made
ndash Give tPA on CT table
ndash Must have all informationhellip
bull LVO- ECR consideration
Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

The ldquogolden hourrdquo
T=0
Suspected
stroke patient
arrives at
stroke unit
le10 min
Initial MD evaluation
(including patient
history lab work
initiation amp NIHSS)
le 15 min
Stroke team
Notified
le 25 min
CT scan
initiated
le 45 min
CT amp labs
interpreted
le 60 min
rt-PA
given if patient
is eligible
Slide courtesy of Skye Coote
The ldquogolden half-hourrdquo
T= -10
Suspected
stroke patient
hospital
pre-notification
Stroke team
Notified
0 min
Patient arrives
Met at triage by
stroke and ED team
le 10 min
Triage
direct-to-CT
rapid (basic)
stroke assessment
IVB
le 25 min
CT scan
completed amp
interpreted
le 30 min
t-PA
given if patient
is eligible
Slide courtesy of Skye Coote
bull Pts who arrive within
the golden hour are
twice as likely to be
treated
bull Improved patient
outcomes
andhellip
bull Walk out of hospital
Identification of Stroke
bull An immediate life threatening emergency
needing an ambulance may include
Ambiguous stroke Sx
bull Dizziness
bull Drowsiness
bull Visual disturbance
bull Ataxia
bull Numbness
bull Tingling
bull Canrsquot understand surroundings
Ambulance Pre-notification
bull Patients name amp DOB
bull Quick story
ndash Symptoms
ndash Time of onset
ndash Vitals signs amp GCS
bull 18G IVC (if able)
bull ED ldquoCode strokerdquo paged
bull CT freed
bull Labels created
bull Pt remains on AV monitor
Code Stroke
bull Pt met at door by
ndash Stroke Nurse
ndash Stroke Registrar
ndash HMO
bull Assessed for suitability for
direct to CT
ndash ABCD (Brief)
ndash Verify patient details- labels
ndash Triage is brief (Cat 2)
Direct to CT
bull Walk and Talk stroke assessments
bull Senior clinician begins assessing
bull Pt transferred onto CT table
ndash Off stretcher time
bull Non Contrast CT Brain
ndash Rule out blood
ndash HMO ndash IVC and pathology
bull Red stream staff bring equipment
ndash Trolley airway basket monitoring
bull CT Angiogram amp Perfusion
ndash Routine investigation
CT interpretation
bull Real time review
bull NIHSS- stroke
assessments continue
bull Call to Consultant
bull Swap monitors
bull Contact familyGP
bull tPA decision made
ndash Give tPA on CT table
ndash Must have all informationhellip
bull LVO- ECR consideration
Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

The ldquogolden half-hourrdquo
T= -10
Suspected
stroke patient
hospital
pre-notification
Stroke team
Notified
0 min
Patient arrives
Met at triage by
stroke and ED team
le 10 min
Triage
direct-to-CT
rapid (basic)
stroke assessment
IVB
le 25 min
CT scan
completed amp
interpreted
le 30 min
t-PA
given if patient
is eligible
Slide courtesy of Skye Coote
bull Pts who arrive within
the golden hour are
twice as likely to be
treated
bull Improved patient
outcomes
andhellip
bull Walk out of hospital
Identification of Stroke
bull An immediate life threatening emergency
needing an ambulance may include
Ambiguous stroke Sx
bull Dizziness
bull Drowsiness
bull Visual disturbance
bull Ataxia
bull Numbness
bull Tingling
bull Canrsquot understand surroundings
Ambulance Pre-notification
bull Patients name amp DOB
bull Quick story
ndash Symptoms
ndash Time of onset
ndash Vitals signs amp GCS
bull 18G IVC (if able)
bull ED ldquoCode strokerdquo paged
bull CT freed
bull Labels created
bull Pt remains on AV monitor
Code Stroke
bull Pt met at door by
ndash Stroke Nurse
ndash Stroke Registrar
ndash HMO
bull Assessed for suitability for
direct to CT
ndash ABCD (Brief)
ndash Verify patient details- labels
ndash Triage is brief (Cat 2)
Direct to CT
bull Walk and Talk stroke assessments
bull Senior clinician begins assessing
bull Pt transferred onto CT table
ndash Off stretcher time
bull Non Contrast CT Brain
ndash Rule out blood
ndash HMO ndash IVC and pathology
bull Red stream staff bring equipment
ndash Trolley airway basket monitoring
bull CT Angiogram amp Perfusion
ndash Routine investigation
CT interpretation
bull Real time review
bull NIHSS- stroke
assessments continue
bull Call to Consultant
bull Swap monitors
bull Contact familyGP
bull tPA decision made
ndash Give tPA on CT table
ndash Must have all informationhellip
bull LVO- ECR consideration
Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

bull Pts who arrive within
the golden hour are
twice as likely to be
treated
bull Improved patient
outcomes
andhellip
bull Walk out of hospital
Identification of Stroke
bull An immediate life threatening emergency
needing an ambulance may include
Ambiguous stroke Sx
bull Dizziness
bull Drowsiness
bull Visual disturbance
bull Ataxia
bull Numbness
bull Tingling
bull Canrsquot understand surroundings
Ambulance Pre-notification
bull Patients name amp DOB
bull Quick story
ndash Symptoms
ndash Time of onset
ndash Vitals signs amp GCS
bull 18G IVC (if able)
bull ED ldquoCode strokerdquo paged
bull CT freed
bull Labels created
bull Pt remains on AV monitor
Code Stroke
bull Pt met at door by
ndash Stroke Nurse
ndash Stroke Registrar
ndash HMO
bull Assessed for suitability for
direct to CT
ndash ABCD (Brief)
ndash Verify patient details- labels
ndash Triage is brief (Cat 2)
Direct to CT
bull Walk and Talk stroke assessments
bull Senior clinician begins assessing
bull Pt transferred onto CT table
ndash Off stretcher time
bull Non Contrast CT Brain
ndash Rule out blood
ndash HMO ndash IVC and pathology
bull Red stream staff bring equipment
ndash Trolley airway basket monitoring
bull CT Angiogram amp Perfusion
ndash Routine investigation
CT interpretation
bull Real time review
bull NIHSS- stroke
assessments continue
bull Call to Consultant
bull Swap monitors
bull Contact familyGP
bull tPA decision made
ndash Give tPA on CT table
ndash Must have all informationhellip
bull LVO- ECR consideration
Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

Identification of Stroke
bull An immediate life threatening emergency
needing an ambulance may include
Ambiguous stroke Sx
bull Dizziness
bull Drowsiness
bull Visual disturbance
bull Ataxia
bull Numbness
bull Tingling
bull Canrsquot understand surroundings
Ambulance Pre-notification
bull Patients name amp DOB
bull Quick story
ndash Symptoms
ndash Time of onset
ndash Vitals signs amp GCS
bull 18G IVC (if able)
bull ED ldquoCode strokerdquo paged
bull CT freed
bull Labels created
bull Pt remains on AV monitor
Code Stroke
bull Pt met at door by
ndash Stroke Nurse
ndash Stroke Registrar
ndash HMO
bull Assessed for suitability for
direct to CT
ndash ABCD (Brief)
ndash Verify patient details- labels
ndash Triage is brief (Cat 2)
Direct to CT
bull Walk and Talk stroke assessments
bull Senior clinician begins assessing
bull Pt transferred onto CT table
ndash Off stretcher time
bull Non Contrast CT Brain
ndash Rule out blood
ndash HMO ndash IVC and pathology
bull Red stream staff bring equipment
ndash Trolley airway basket monitoring
bull CT Angiogram amp Perfusion
ndash Routine investigation
CT interpretation
bull Real time review
bull NIHSS- stroke
assessments continue
bull Call to Consultant
bull Swap monitors
bull Contact familyGP
bull tPA decision made
ndash Give tPA on CT table
ndash Must have all informationhellip
bull LVO- ECR consideration
Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

Ambiguous stroke Sx
bull Dizziness
bull Drowsiness
bull Visual disturbance
bull Ataxia
bull Numbness
bull Tingling
bull Canrsquot understand surroundings
Ambulance Pre-notification
bull Patients name amp DOB
bull Quick story
ndash Symptoms
ndash Time of onset
ndash Vitals signs amp GCS
bull 18G IVC (if able)
bull ED ldquoCode strokerdquo paged
bull CT freed
bull Labels created
bull Pt remains on AV monitor
Code Stroke
bull Pt met at door by
ndash Stroke Nurse
ndash Stroke Registrar
ndash HMO
bull Assessed for suitability for
direct to CT
ndash ABCD (Brief)
ndash Verify patient details- labels
ndash Triage is brief (Cat 2)
Direct to CT
bull Walk and Talk stroke assessments
bull Senior clinician begins assessing
bull Pt transferred onto CT table
ndash Off stretcher time
bull Non Contrast CT Brain
ndash Rule out blood
ndash HMO ndash IVC and pathology
bull Red stream staff bring equipment
ndash Trolley airway basket monitoring
bull CT Angiogram amp Perfusion
ndash Routine investigation
CT interpretation
bull Real time review
bull NIHSS- stroke
assessments continue
bull Call to Consultant
bull Swap monitors
bull Contact familyGP
bull tPA decision made
ndash Give tPA on CT table
ndash Must have all informationhellip
bull LVO- ECR consideration
Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

Ambulance Pre-notification
bull Patients name amp DOB
bull Quick story
ndash Symptoms
ndash Time of onset
ndash Vitals signs amp GCS
bull 18G IVC (if able)
bull ED ldquoCode strokerdquo paged
bull CT freed
bull Labels created
bull Pt remains on AV monitor
Code Stroke
bull Pt met at door by
ndash Stroke Nurse
ndash Stroke Registrar
ndash HMO
bull Assessed for suitability for
direct to CT
ndash ABCD (Brief)
ndash Verify patient details- labels
ndash Triage is brief (Cat 2)
Direct to CT
bull Walk and Talk stroke assessments
bull Senior clinician begins assessing
bull Pt transferred onto CT table
ndash Off stretcher time
bull Non Contrast CT Brain
ndash Rule out blood
ndash HMO ndash IVC and pathology
bull Red stream staff bring equipment
ndash Trolley airway basket monitoring
bull CT Angiogram amp Perfusion
ndash Routine investigation
CT interpretation
bull Real time review
bull NIHSS- stroke
assessments continue
bull Call to Consultant
bull Swap monitors
bull Contact familyGP
bull tPA decision made
ndash Give tPA on CT table
ndash Must have all informationhellip
bull LVO- ECR consideration
Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

Code Stroke
bull Pt met at door by
ndash Stroke Nurse
ndash Stroke Registrar
ndash HMO
bull Assessed for suitability for
direct to CT
ndash ABCD (Brief)
ndash Verify patient details- labels
ndash Triage is brief (Cat 2)
Direct to CT
bull Walk and Talk stroke assessments
bull Senior clinician begins assessing
bull Pt transferred onto CT table
ndash Off stretcher time
bull Non Contrast CT Brain
ndash Rule out blood
ndash HMO ndash IVC and pathology
bull Red stream staff bring equipment
ndash Trolley airway basket monitoring
bull CT Angiogram amp Perfusion
ndash Routine investigation
CT interpretation
bull Real time review
bull NIHSS- stroke
assessments continue
bull Call to Consultant
bull Swap monitors
bull Contact familyGP
bull tPA decision made
ndash Give tPA on CT table
ndash Must have all informationhellip
bull LVO- ECR consideration
Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

Direct to CT
bull Walk and Talk stroke assessments
bull Senior clinician begins assessing
bull Pt transferred onto CT table
ndash Off stretcher time
bull Non Contrast CT Brain
ndash Rule out blood
ndash HMO ndash IVC and pathology
bull Red stream staff bring equipment
ndash Trolley airway basket monitoring
bull CT Angiogram amp Perfusion
ndash Routine investigation
CT interpretation
bull Real time review
bull NIHSS- stroke
assessments continue
bull Call to Consultant
bull Swap monitors
bull Contact familyGP
bull tPA decision made
ndash Give tPA on CT table
ndash Must have all informationhellip
bull LVO- ECR consideration
Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

CT interpretation
bull Real time review
bull NIHSS- stroke
assessments continue
bull Call to Consultant
bull Swap monitors
bull Contact familyGP
bull tPA decision made
ndash Give tPA on CT table
ndash Must have all informationhellip
bull LVO- ECR consideration
Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

Victorian Stroke Telemedicine
bull What every stroke patient needs
ndash Identification
ndash CT
ndash Onset time
ndash Bleeding Risk past history and
medications
bull Process the same though the
team is different
ndash Time factors
bull Read the CT scanhellip
Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

Thrombolysis
bull CT- back to cubicle
bull Undressed and checked
bull Connected to monitor
bull 12 Lead ECG
bull +- second IVC
bull Explanation to pt and family
bull Paperwork
bull Considerations for transfer out
DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

DIDO
bull Door in Door Out Time
bull How long does it take to get
ndash Story
ndash CT scan
ndash Contraindications to treatment
ndash Decision to treat
ndash Pt out the doorhellip ECR 37 for the year
Best 41 mins
Longest 227 mins
Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

Stroke Team
bull Stroke Nurse ED Nurse
bull Registrar 247
bull HMO ED Dr
bull CT notification
bull Labels
bull Equipment
bull Run an acute stroke
presentation like a
codehellip
bull Everyone has their
roles
bull BHH Ed has similar
(if not better) DTN
times out of hours
as in hours
Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

Barriers to treatment
bull Public awareness of stroke symptoms ndash delayed presentation
bull Ambulance calls go through central base and ED
ndash not direct to stroke teamneurologist
bull Lack of response to ambulance pre-notification
ndash team not present on patient arrival
ndash May have implications for future notifications
bull Lack of stroke recognition by ED staff
ndash Delays in calling Code Stroke
bull Stroke trials with extended time frames keeping ED informed
bull Going via resus for monitoring and assessment
bull ED resources
bull Awaiting results of multi-modal images to make a decision
Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

Barriers to treatment
bull ED medical review before notification to stroke doctor
ndash Despite ambulance notification of a stroke patient
ndash Impact on calling in after-hours radiography staff
bull Time delay in calling stroke doctor
ndash Time taken for stroke doctor to come in to hospital
bull Radiographer offsite after 7pm ndash limited cover
ndash Lack of in-house CT interpretation
ndash off site service ndash slow
bull Reduced staff to assist with drawing up
ndash delayed CTndashN times
bull Delays in CT images being loaded for external viewing
Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

Enablers to treatment
bull Being a stroke thrombolysis receiving hospital
bull Ambulance preference
bull Increased frequency of stroke increases ED awareness
ndash notifications
bull More than one CT scanner
ndash Relationship with CT staff
bull Team work across multiple disciplines
bull Role definition
bull Champions
bull Executive buy in
bull Medical support
Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

Take Home message
bull Think FAST
bull Nothing can be decided without a CT
bull Stroke team are the people around you
bull Get expert helphellip VST
bull Transfer protocols
bull Efficiency and safety
bull Despite your size you can have massive
impacthellip
Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

Referencesbull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163
bull Collateral flow predicts response to endovascular therapy for acute ischaemic stroke
bull A randomised trial for tenecteplase versus alteplase for acute ischaemic stroke
bull Antithrombotic therapy for acute Ischaemic stroke
bull Mr clean and memery lapses
bull Mr rescue emerging therapy critiques
bull Developing practice reccomendations for endovascular revascularisation for acute ischaemic stroke
bull Endovascular treatment for acute ischaemic stroke Stroke Collateral flow Predicts Response to Endovascular Therapy for Acute Ischaemic
Stroke201142693-699)
bull httpmusommarshalledugraphicdesignibooksNervous20NormalhtmlprettyPhoto[pp_gal]9
bull Lippencotts Illustrated reviews Neuroscience
bull Mr Clean Polishes Stroke Outcome with endovascular therapy
bull Endovascular Mechanical Thrombectomy of an occluded superior division branch of the L) MCA for acute cardioembolic stroke
bull Predictors of functional dependance despite successful revascularisation in large vessel occlusion strokes
bull Stroke The Impact of Recanalization on Ischemic Stroke Outcome A Meta-Analysis Joung-Ho Rha and Jeffrey L Saver Stroke 200738967-973
originally published online February 1 2007
bull Clinical guidelines for acute stroke management 2010
bull Lees et al Lancet 20103751695-1703
More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

More References
bull Nursing Critical Care Issue Volume 11(3) May 2016 p 28ndash36
bull Lackland DT Roccella EJ Deutsch AF et al Factors influencing the decline in stroke mortality a statement from the American Heart
AssociationAmerican Stroke Association Stroke 201445(1)315ndash353
bull Bhatia R Hill M D Shobha N Menon B Bal S Kochar P Demchuk A M (2010) Low Rates of Acute Recanalization With Intravenous
Recombinant Tissue Plasminogen Activator in Ischemic Stroke Real-World Experience and a Call for Action Stroke 41(10) 2254-2258 doi
101161strokeaha110592535
bull Berkhemer O A Fransen P S S Beumer D van den Berg L A Lingsma H F Yoo A J Dippel D W J (2015) A Randomized Trial of
Intraarterial Treatment for Acute Ischemic Stroke New England Journal of Medicine 372(1) 11-20 doi doi101056NEJMoa1411587
bull Campbell B C V Mitchell P J Kleinig T J Dewey H M Churilov L Yassi N Davis S M (2015) Endovascular Therapy for Ischemic
Stroke with Perfusion-Imaging Selection New England Journal of Medicine 372(11) 1009-1018 doi doi101056NEJMoa1414792
bull Goyal M Demchuk A M Menon B K Eesa M Rempel J L Thornton J Hill M D (2015) Randomized Assessment of Rapid Endovascular
Treatment of Ischemic Stroke New England Journal of Medicine 372(11) 1019-1030 doi doi101056NEJMoa1414905
bull Saver J L Goyal M Bonafe A Diener H-C Levy E I Pereira V M Hacke W (2015) Stent-retriever thrombectomy after intravenous t-PA
vs t-PA alone in stroke New England Journal of Medicine
bull Jovin T G Chamorro A Cobo E de Miquel M A Molina C A Rovira A Daacutevalos A (2015) Thrombectomy within 8 Hours after Symptom
Onset in Ischemic Stroke New England Journal of Medicine 372(24) 2296-2306 doi doi101056NEJMoa1503780
bull Goyal M Menon B K van Zwam W H Dippel D W J Mitchell P J Demchuk A M Jovin T G Endovascular thrombectomy after large-
vessel ischaemic stroke a meta-analysis of individual patient data from five randomised trials The Lancet doi 101016S0140-6736(16)00163-X
Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau

Thank you
bull Tanya Frost
Acute Stroke Nurse
TanyaFrosteasternhealthorgau
Top Related