







Languages
Pages
Legal


Basic ABG Interpretation
Jose Socrates ‘DEE’ EvardoneYear Level I
Department of Internal MedicineCebu Doctors University Hospital
arterial blood gas (ABG)• test that measures the:
– 1) oxygen tension (PaO2), – 2) carbon dioxide tension (PaCO2), – 3) acidity (pH), – 4) oxyhemoglobin saturation (SaO2), and– 5) bicarbonate (HCO3) concentration in
arterial blood. • Some blood gas analyzers also measure the
methemoglobin, carboxyhemoglobin levels
ARTERIAL BLOOD GASES• ARTERIAL SAMPLING• Needle puncture
– - Site selection– - Collateral circulation– - Technique– - Complications
• Indwelling catheters• SPECIMEN CARE• TRANSPORT• ANALYSIS• INTERPRETATION
– Normal values

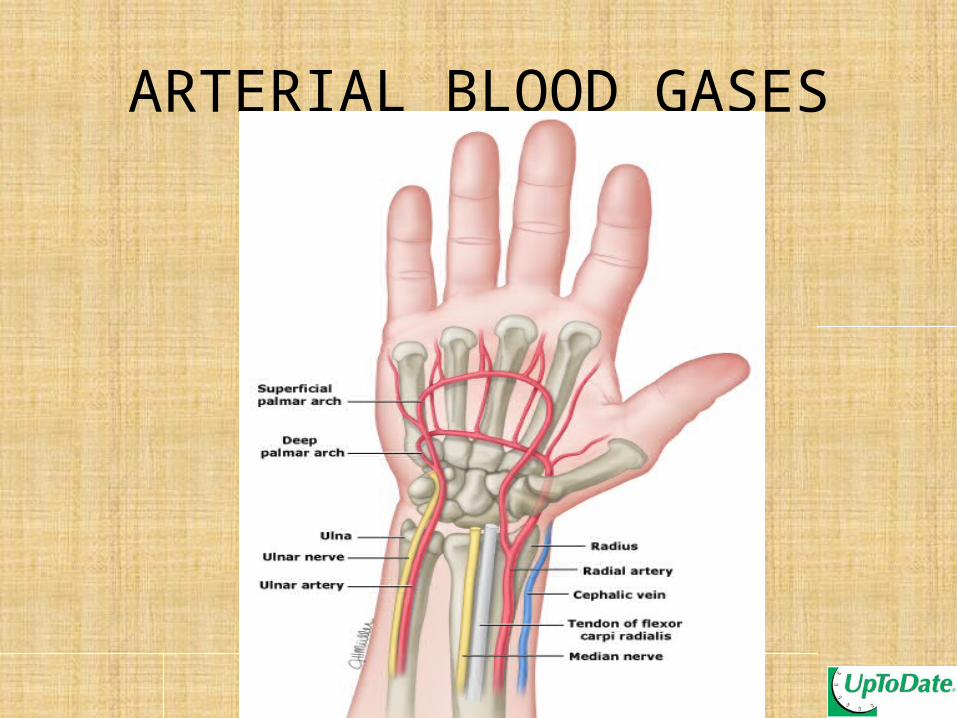
ARTERIAL BLOOD GASES• ARTERIAL SAMPLING:• Common sites include:
– 1) radial, – 2) femoral, – 3) brachial, – 4) dorsalis pedis, or – 5) axillary artery
• the radial artery is used most often because it is – accessible, – easily positioned, and– more comfortable for the patient than the alternative
sites

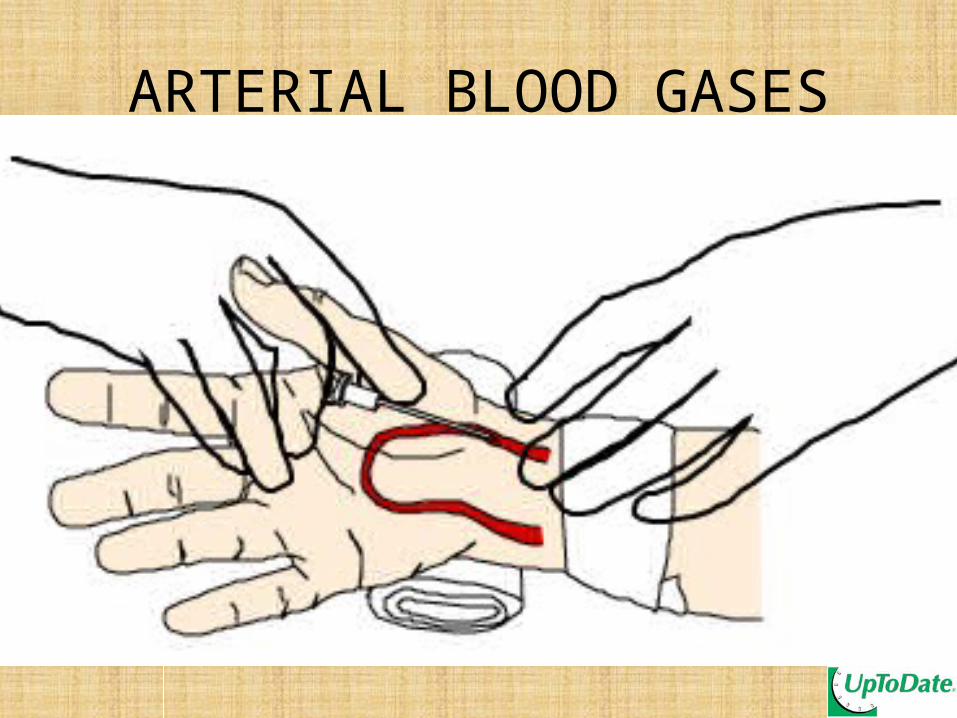
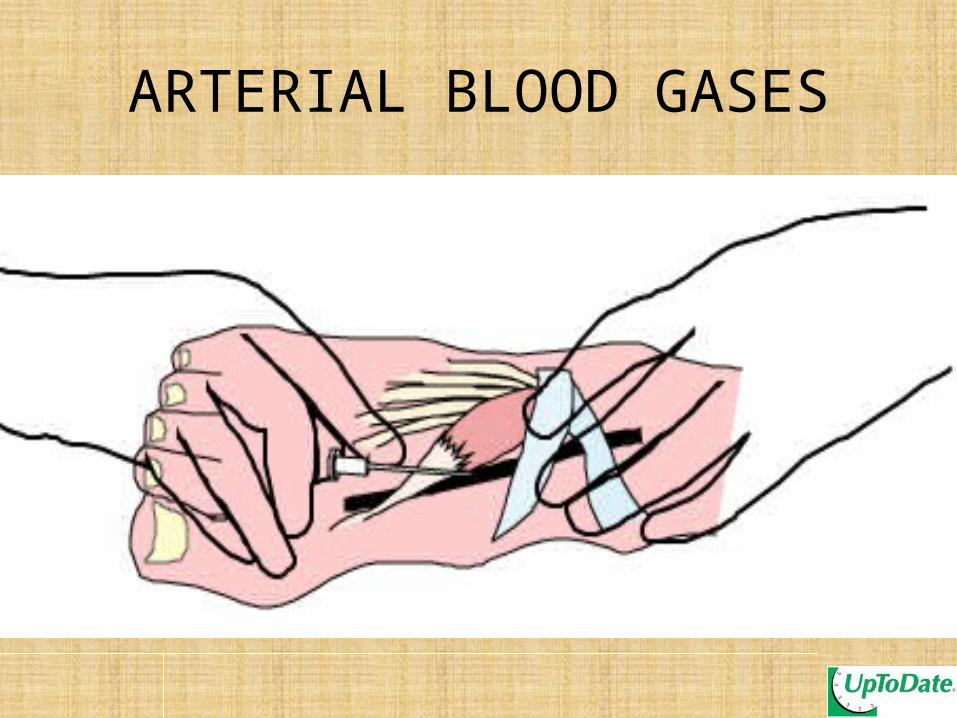
ARTERIAL BLOOD GASESTechnique
●Local analgesia ●The seal of a heparinized syringe should be broken by pulling its plunger. ●the artery should be punctured with the needle at a 30 to 45 degree angle relative to the skin●rolled between the hands ●pressure applied to the puncture site for five to ten minutes to achieve hemostasis.
30-45-degree angle (for radial artery),
45-60-degree angle (for brachial artery),
45-90-degree angle (for femoral artery) with the bevel of the needle turned up
ARTERIAL BLOOD GASES
ARTERIAL BLOOD GASES

ARTERIAL BLOOD GASES

ARTERIAL BLOOD GASES

ARTERIAL BLOOD GASES

ARTERIAL BLOOD GASES

ARTERIAL BLOOD GASES
ARTERIAL BLOOD GASES

ARTERIAL BLOOD GASES

ARTERIAL BLOOD GASES

ARTERIAL BLOOD GASES
ARTERIAL BLOOD GASESSPECIMEN CARE
Gas diffusion through the plastic syringe is a potential source of error.
- Using a glass syringe- placed on ice and analyzed within 15
minutes

ARTERIAL BLOOD GASESSPECIMEN CARE
The HEPARINdecrease in the pH dilute the PaCO2
heparin solution should be minimized and at least 2 mL of blood should be obtained

ARTERIAL BLOOD GASESSPECIMEN CARE
Air bubbles that exceed 1 to 2 percent of the blood volume
falsely high PaO2 falsely low PaCO2
gently removing the bubbles without agitation and analyzing the sample as soon as possible
ARTERIAL BLOOD GASESINTERPRETATION
"Oxygenation and mechanisms of hypoxemia“ and
"Simple and mixed acid-base disorders"
ARTERIAL BLOOD GASES"Oxygenation and mechanisms of
hypoxemia“MEASURES OF OXYGENATION:
1) Arterial oxygen saturation (SaO2)2) Arterial oxygen tension (PaO2)3) A-a oxygen gradient4) PaO2/FiO2 ratio5) a-A oxygen ratio6) Oxygenation index

ARTERIAL BLOOD GASESArterial oxygen
saturation (SaO2)

ARTERIAL BLOOD GASESArterial oxygen
tension (PaO2)

ARTERIAL BLOOD GASES
A-a oxygen gradientA-a oxygen gradient = PAO2 - PaO2
A-a gradient = 2.5 + 0.21 x age in years
ARTERIAL BLOOD GASES
PaO2/FiO2 ratioA normal PaO2/FiO2 ratio is 300 to 500 mmHgless than 300 mmHg indicating abnormal gas exchange less than 200 mmHg indicates severe hypoxemia

ARTERIAL BLOOD GASES
a-A oxygen ratioa-A oxygen ratio = PaO2 ÷ PAO2
lower limit of normal is 0.77-0.82 most reliable when the FiO2 is less than 0.55
ARTERIAL BLOOD GASES
Oxygenation index OI = [mean airway pressure x
FiO2 ÷ PaO2] x 100

ARTERIAL BLOOD GASESMECHANISMS OF HYPOXEMIA
HypoventilationV/Q mismatch
Right-to-left shuntDiffusion limitation
Reduced inspired oxygen tension
ARTERIAL BLOOD GASES
"Simple and mixed acid-base disorders"

ARTERIAL BLOOD GASESNormal Values
(Harrisons)

Normal Values
• pH = 7.35 – 7.45• pCO2 = 35 – 45 mmHg lungs(Reference Value = 40)
• HCO3 = 22 – 26 mmol/L kidneys(Reference value = 24)
Definition Of Terms
• Acidemia- Arterial pH < 7.56• Alkalemia- Arterial pH > 7.45• Acidosis- A process that tends to lower the
extracellular pH (Hydrogen ion concentration increases)
• Alkalosis- A process that tends to raise the extracellular pH (hydrogen ion concentration decreases)

Definition Of Terms
• Metabolic acidosis- A disorder that reduces the serum Hc03 and pH
• Metabolic Alkalosis- A disorder that elevates serum Hc03 and pH
• Respiratory Acidosis- A disorder that elevates the arterial pC02 and reduces the pH
• Respiratory Alkalosis- A disorder that reduces the arterial pC02 and elevates the pH
Definition Of Terms
• Simple Acid Base Disorder- Appropriate Respiratory or Renal Compensation for the Disorder
• Mixed Acid Base Disorder- Presence of More than one acid base Disorder



ARTERIAL BLOOD GAS ANALYSIS• 1) Look at the pH
– Acidemia or alkalemia– The cause is in the same direction
• 2) Look at pCO2– Decreased in alkalosis– Increased in acidosis
• 3) Look at HCO3– Decreased in acidosis– Increased in alkalosis
• 4) Remember, the body does NOT overcompensate
• 5) Compensation can be COMPLETE or INCOMPLETE
Example # 1PH – 7.34pCO2 – 52HCO3 - 19

ARTERIAL BLOOD GAS ANALYSIS• 1) Look at the pH
– Acidemia or alkalemia– The cause is in the same direction
• 2) Look at pCO2– Decreased in alkalosis– Increased in acidosis
• 3) Look at HCO3– Decreased in acidosis– Increased in alkalosis
• 4) Remember, the body does NOT overcompensate• 5) Compensation can be COMPLETE or INCOMPLETE
Example # 2PH – 7.34pCO2 – 50HCO3 - 31

ARTERIAL BLOOD GAS ANALYSIS• 1) Look at the pH
– Acidemia or alkalemia– The cause is in the same direction
• 2) Look at pCO2– Decreased in alkalosis– Increased in acidosis
• 3) Look at HCO3– Decreased in acidosis– Increased in alkalosis
• 4) Remember, the body does NOT overcompensate• 5) Compensation can be COMPLETE or INCOMPLETE
Example # 3PH – 7.38pCO2 – 24HCO3 - 19

ARTERIAL BLOOD GAS ANALYSIS• 1) Look at the pH
– Acidemia or alkalemia– The cause is in the same direction
• 2) Look at pCO2– Decreased in alkalosis– Increased in acidosis
• 3) Look at HCO3– Decreased in acidosis– Increased in alkalosis
• 4) Remember, the body does NOT overcompensate• 5) Compensation can be COMPLETE or INCOMPLETE
Example # 4PH – 7.46pCO2 – 42HCO3 - 31
ARTERIAL BLOOD GAS ANALYSIS• 1) Look at the pH
– Acidemia or alkalemia– The cause is in the same direction
• 2) Look at pCO2– Decreased in alkalosis– Increased in acidosis
• 3) Look at HCO3– Decreased in acidosis– Increased in alkalosis
• 4) Remember, the body does NOT overcompensate• 5) Compensation can be COMPLETE or INCOMPLETE
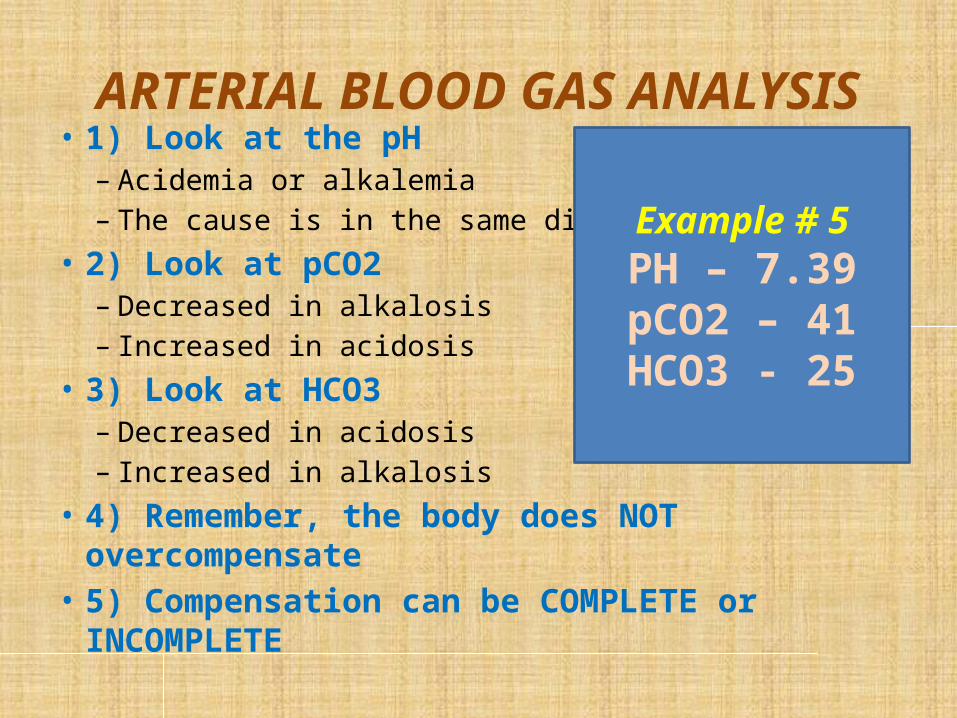
Example # 5PH – 7.39pCO2 – 41HCO3 - 25

ARTERIAL BLOOD GAS ANALYSIS• 1) Look at the pH
– Acidemia or alkalemia– The cause is in the same direction
• 2) Look at pCO2– Decreased in alkalosis– Increased in acidosis
• 3) Look at HCO3– Decreased in acidosis– Increased in alkalosis
• 4) Remember, the body does NOT overcompensate• 5) Compensation can be COMPLETE or INCOMPLETE
Example # 6PH – 7.41pCO2 – 51HCO3 - 33
Calculations for the Medicine Floors

Normal Values(Harrisons)

A 45 y.o. doctor ran a 6:12 mile, then fell down on all 4’s
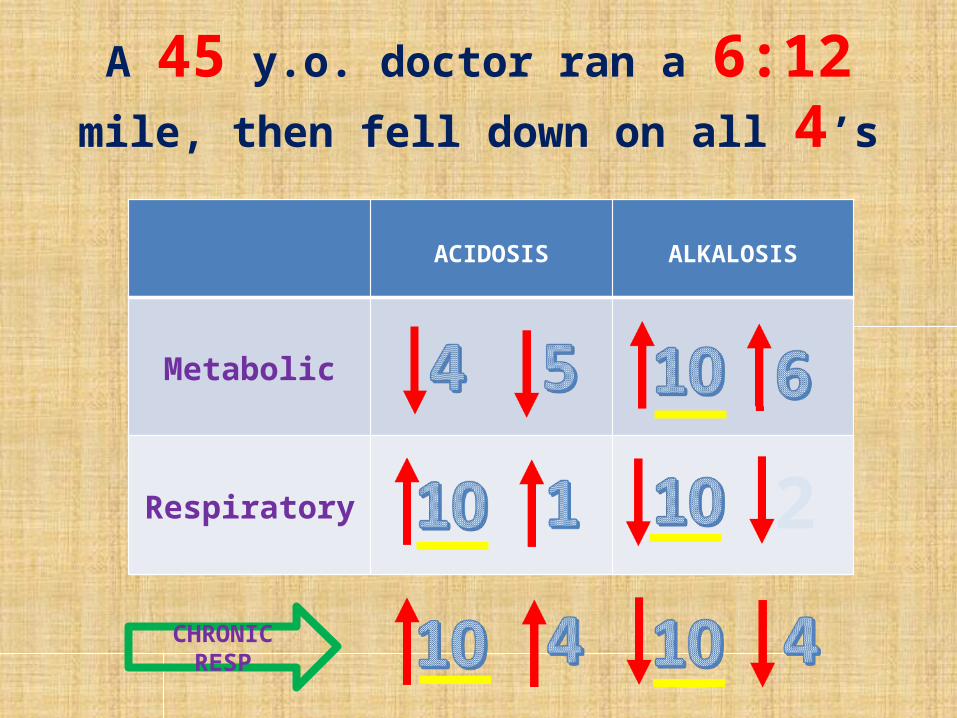
A 45 y.o. doctor ran a 6:12 mile, then fell
down on all 4’s
ACIDOSIS ALKALOSIS
Metabolic
Respiratory 2
CHRONIC RESP

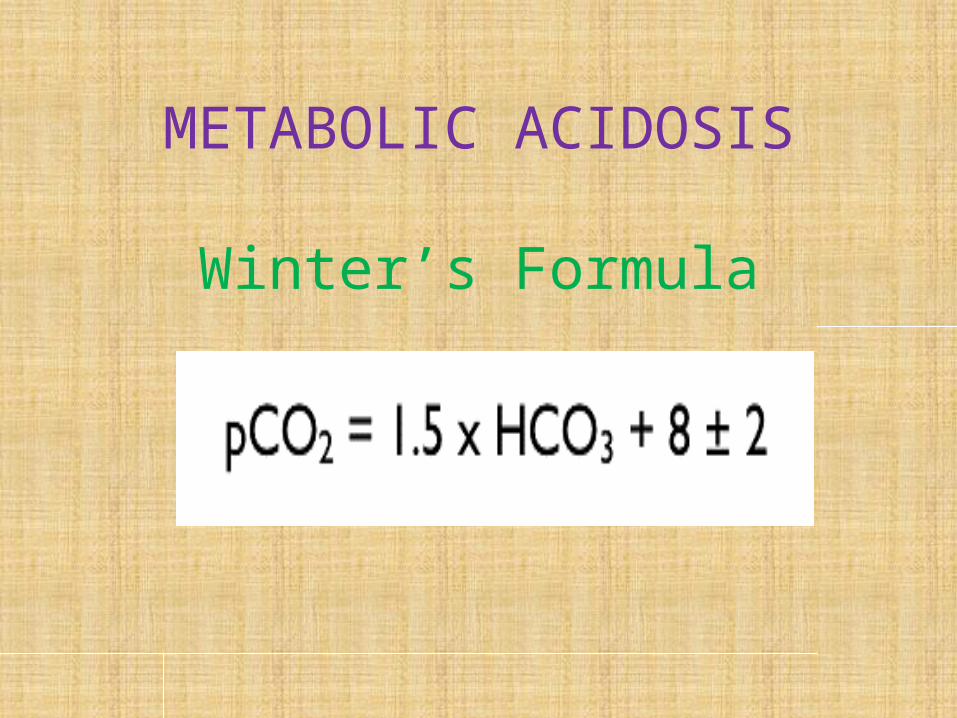
METABOLIC ACIDOSIS
Winter’s Formula

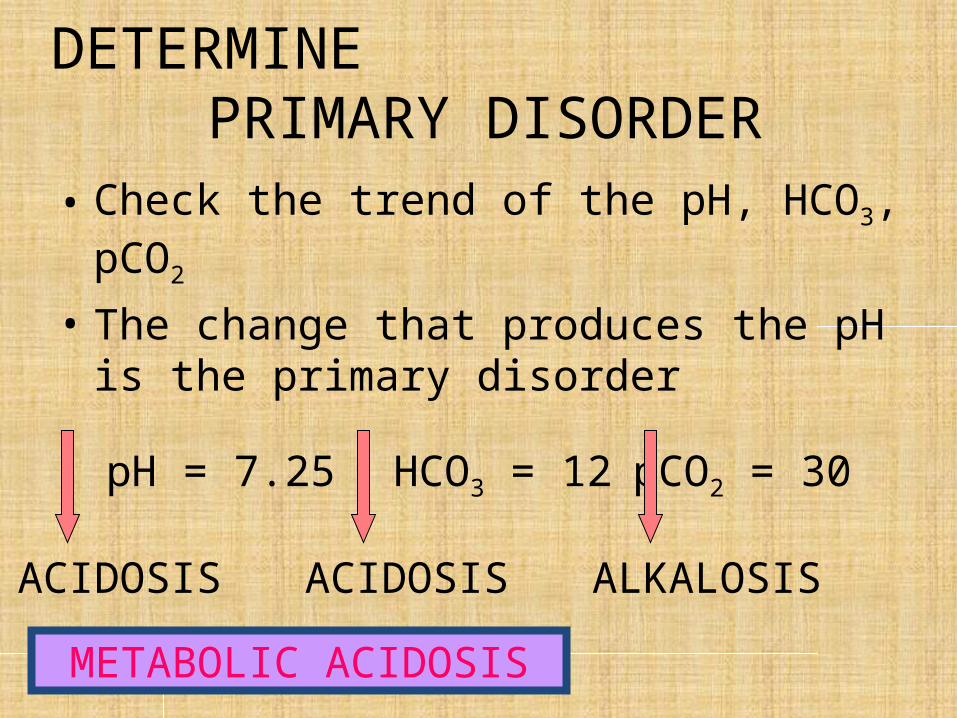
DETERMINE PRIMARY DISORDER
• Check the trend of the pH, HCO3, pCO2
• The change that produces the pH is the primary disorder
pH = 7.25 HCO3 = 12 pCO2 = 30
ACIDOSIS ACIDOSIS ALKALOSIS
METABOLIC ACIDOSIS

DETERMINE PRIMARY DISORDER
• Check the trend of the pH, HCO3, pCO2
• The change that produces the pH is the primary disorder
pH = 7.25 HCO3 = 28 pCO2 = 60
ACIDOSIS ALKALOSIS ACIDOSIS
RESPIRATORY ACIDOSIS

DETERMINE PRIMARY DISORDER
• Check the trend of the pH, HCO3, pCO2
• The change that produces the pH is the primary disorder
pH = 7.55 HCO3 = 19 pCO2 = 20
ALKALOSIS ACIDOSIS ALKALOSIS
RESPIRATORY ALKALOSIS

DETERMINE PRIMARY DISORDER
• If the trend is the same, check the percent difference
• The bigger %difference is the 10 disorder
pH = 7.25 HCO3 = 16 pCO2 = 60
ACIDOSIS ACIDOSIS ACIDOSIS
RESPIRATORY ACIDOSIS
(24- 16)/24 = 0.33 (60-40)/40 = 0.5

DETERMINE PRIMARY DISORDER
• If the trend is the same, check the percent difference
• The bigger %difference is the 10 disorder
pH = 7.55 HCO3 = 38 pCO2 = 30
ALKALOSIS ALKALOSIS ALKALOSIS
METABOLIC ALKALOSIS
(38-24)/24 = 0.58 (40-30)/40 = 0.25

CHECK THECOMPENSATORY RESPONSE

• PREDICTION OF COMPENSATORY RESPONSES ON SIMPLE ACID BASE DISORDERS
• Metabolic Acidosis PaCO2 = (1.5 X HCO3) + 8
• Metabolic Alkalosis PaCO2 will increase 0.75 mmHg per meq/L increase in HCO3
• Respiratory Acidosis Acute HCO3 will increase 1 meql/L per 10 mmHg increase
in PaCO2Chronic HCO3 will increase 4 meq/L per 10 mmHg increase
in PaCO2• Respiratory Alkalosis
Acute HCO3 will decrease 2 meq/L per 10 mmHg decrease in PaCO2
Chronic HCO3 will decrease 4 meq/L per 10 mmHg decrease in PaCO2

COMPENSATORY RESPONSE
METABOLIC ACIDOSIS
PaCO2 = (1.5 X HCO3) + 8
HCO3 =12 pCO2 =1.5 X 12 + 8 = 26
pCO2 = 1.5 X 7 + 8 = 18.5HCO3 =7
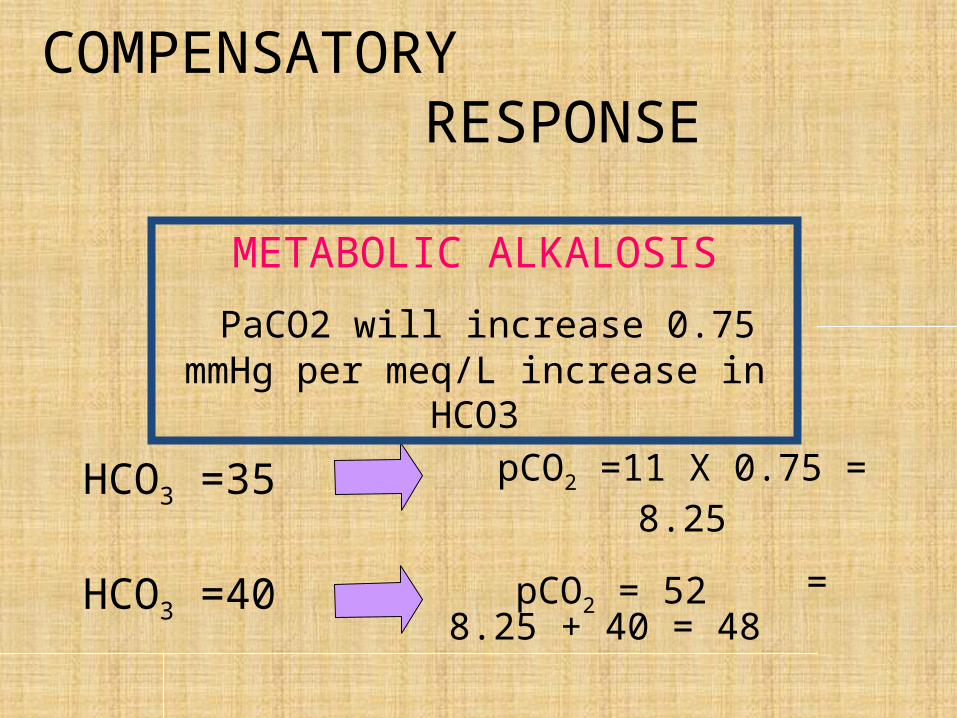
COMPENSATORY RESPONSE
HCO3 =35 pCO2 =11 X 0.75 = 8.25
= 8.25 + 40 = 48 pCO2 = 52HCO3 =40
METABOLIC ALKALOSIS
PaCO2 will increase 0.75 mmHg per meq/L increase in HCO3

COMPENSATORY RESPONSE
pCO2 =55 HCO3 = 25.5
HCO3 = 28pCO2 =80
ACUTE RESPIRATORY ACIDOSIS
HCO3 will increase 1 meq/L per 10 mmHg increase in PaCO2

COMPENSATORY RESPONSE
RESPIRATORY ALKALOSIS Acute: HCO3 will decrease 2 meq/L per 10 mmHg decrease in PaCO2

Check for Secondary Acid Base Disorders
Primary Acid Base Disorder
Compensation Secondary Base Disorder
Metabolic Acidosis Actual reduction of pC02 from baseline is HIGHER than that of calculated compensation
Secondary RESPIRATORY ALKALOSIS is present
Actual reduction of pC02 from baseline is LESS than that of calculated compensation
Secondary RESPIRATORY ACIDOSIS is present

Check for Secondary Acid Base Disorders
Primary Acid Base Disorder
Compensation Secondary Base Disorder
Metabolic Alkalosis Actual increase of Pc02 from baseline is HIGHER than that of calculated compensation
Secondary RESPIRATORY ACIDOSIS is present
Actual reduction of pC02 from baseline is LESS than that of calculated compensation
Secondary RESPIRATORY ACIDOSIS is present

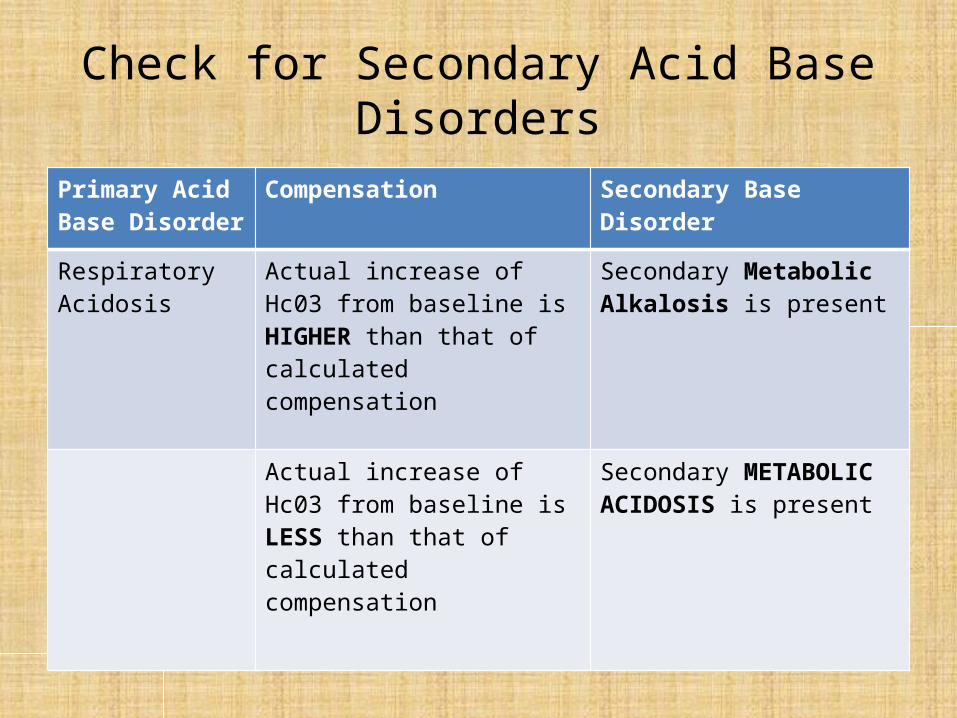
Check for Secondary Acid Base Disorders
Primary Acid Base Disorder
Compensation Secondary Base Disorder
Respiratory Acidosis
Actual increase of Hc03 from baseline is HIGHER than that of calculated compensation
Secondary Metabolic Alkalosis is present
Actual increase of Hc03 from baseline is LESS than that of calculated compensation
Secondary METABOLIC ACIDOSIS is present
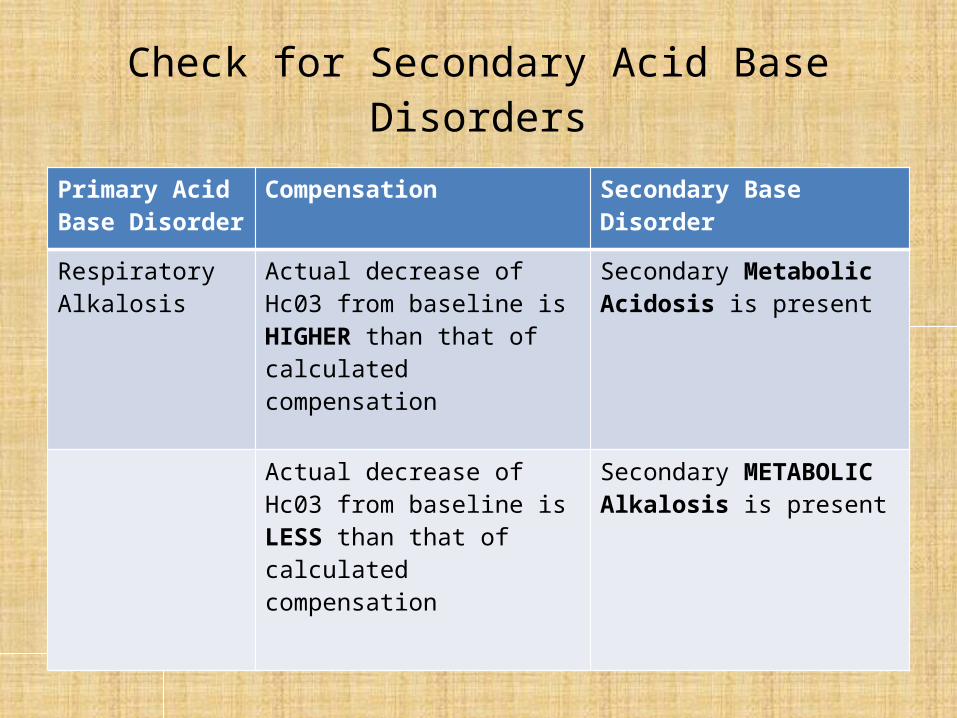
Check for Secondary Acid Base Disorders
Primary Acid Base Disorder
Compensation Secondary Base Disorder
Respiratory Alkalosis
Actual decrease of Hc03 from baseline is HIGHER than that of calculated compensation
Secondary Metabolic Acidosis is present
Actual decrease of Hc03 from baseline is LESS than that of calculated compensation
Secondary METABOLIC Alkalosis is present

ANION GAP
Na – (HCO3 + Cl) = 10-12 mmol/L
Na = 135 HCO3 = 15 Cl = 97 RBS = 100 mg%
AG = 135 – 112 = 23
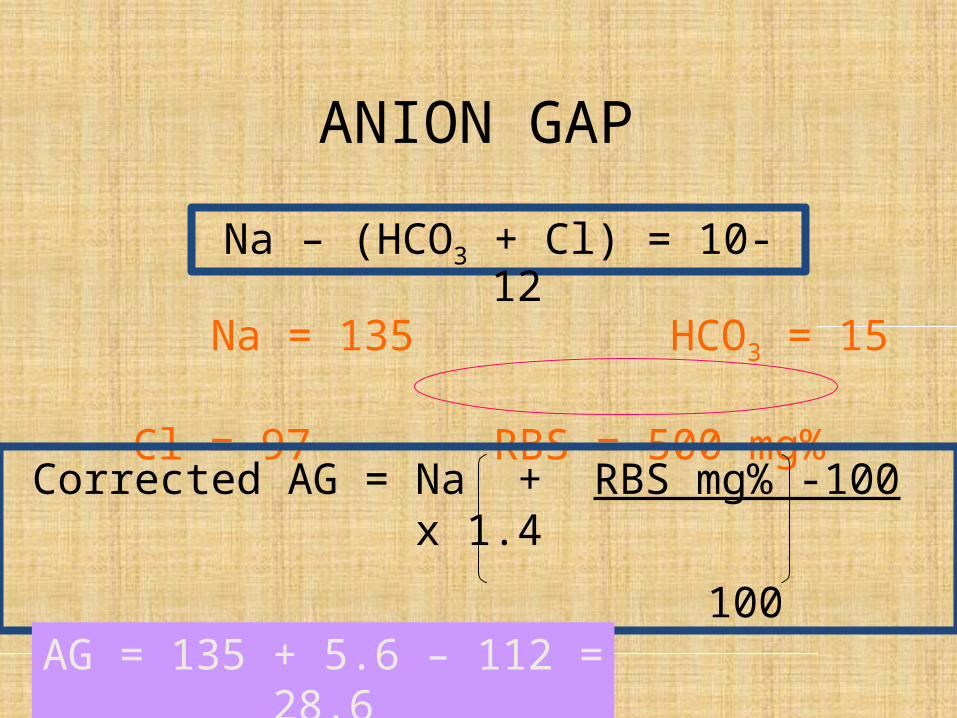
ANION GAP
Na – (HCO3 + Cl) = 10-12
Na = 135 HCO3 = 15 Cl = 97 RBS = 500 mg%
Corrected AG = Na + RBS mg% -100 x 1.4
100
AG = 135 + 5.6 – 112 = 28.6
DETERMINE CLUES FROM THE
CLINICAL SETTING

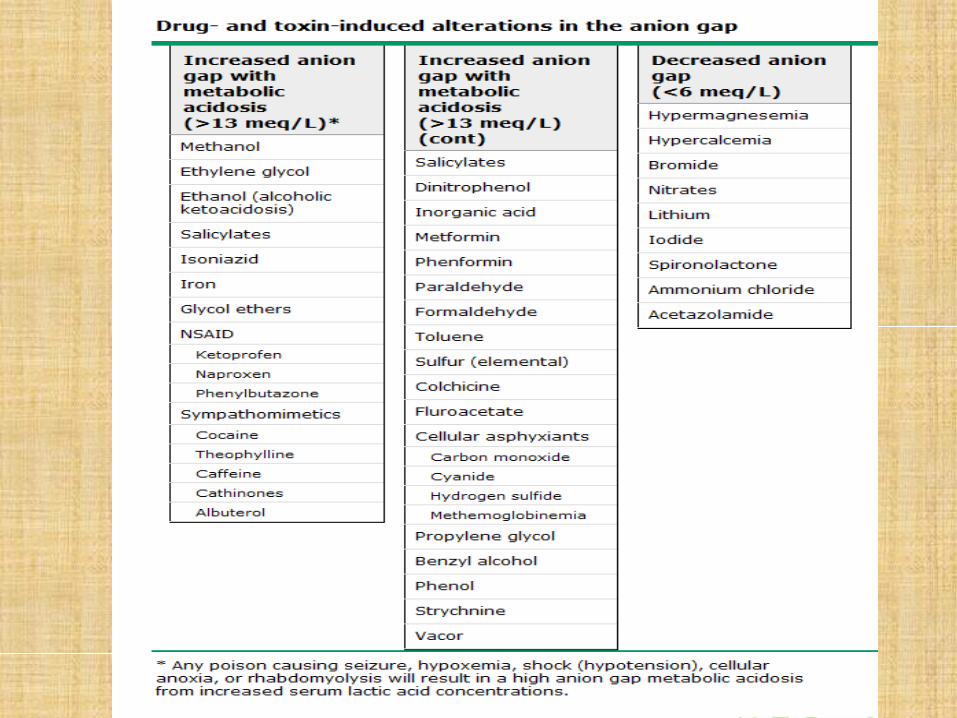
CLUES FROM CLINICAL SETTINGHIGH ANION GAP METABOLIC ACIDOSIS
(HAGMA)M Methanol
U Uremia
D Diabetic Ketoacidosis
P Paraldehyde
I Isoniazid, Iron
L Lactic Acidosis
E Ethylene Glycol, Ethanol
S Salicylates
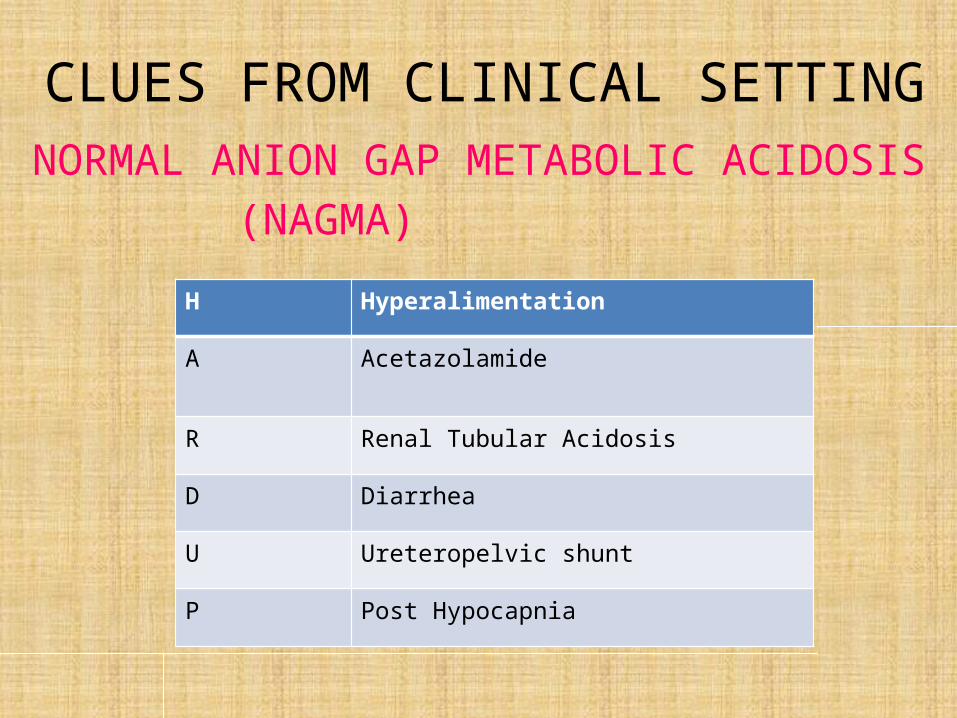
CLUES FROM CLINICAL SETTINGNORMAL ANION GAP METABOLIC ACIDOSIS
(NAGMA)H Hyperalimentation
A Acetazolamide
R Renal Tubular Acidosis
D Diarrhea
U Ureteropelvic shunt
P Post Hypocapnia

CLUES FROM CLINICAL SETTING
METABOLIC ALKALOSIS Vomiting
Remote diuretic usePost hypercapneaChronic diarrhea
Cystic fibrosisAcute alkali administration
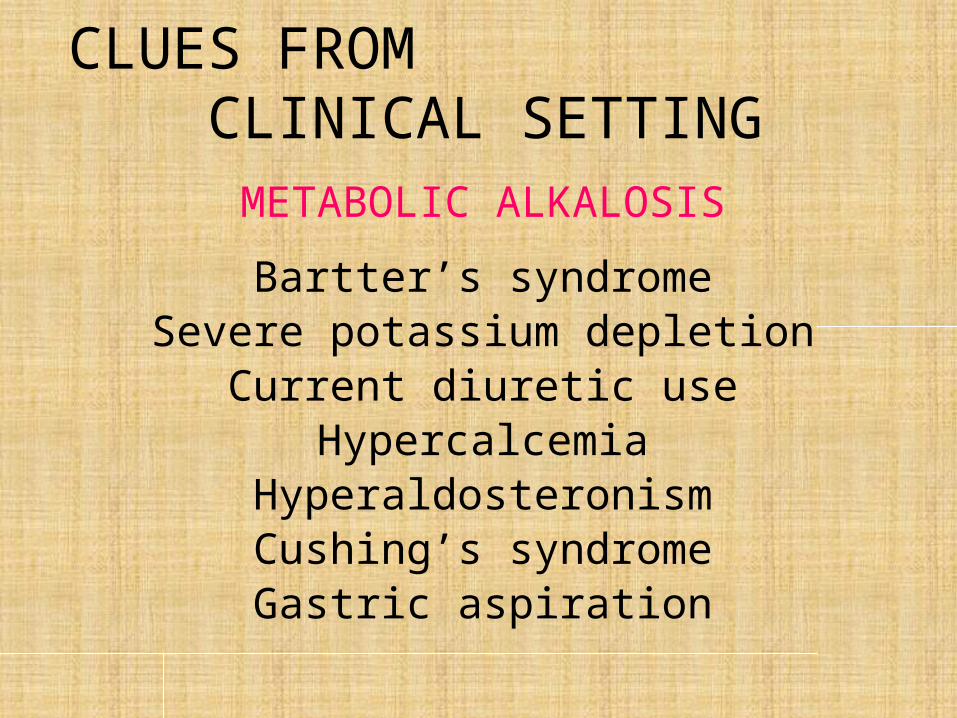
CLUES FROM CLINICAL SETTING
METABOLIC ALKALOSIS
Bartter’s syndromeSevere potassium depletion
Current diuretic useHypercalcemia
HyperaldosteronismCushing’s syndrome
Gastric aspiration
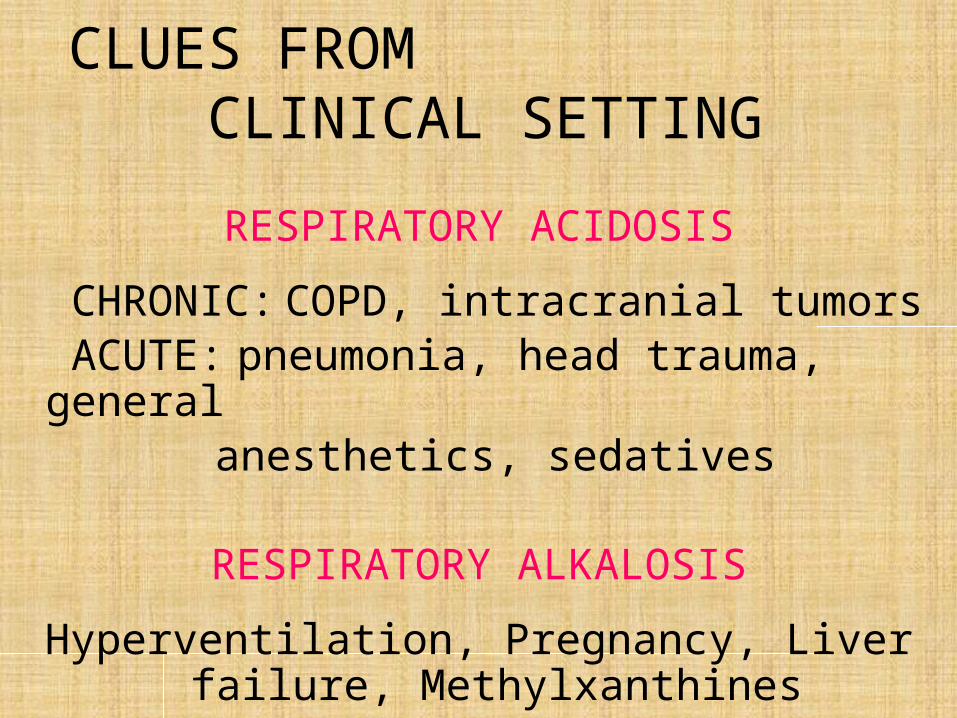
CLUES FROM CLINICAL SETTING
RESPIRATORY ACIDOSIS
CHRONIC: COPD, intracranial tumors ACUTE: pneumonia, head trauma, general
anesthetics, sedatives
RESPIRATORY ALKALOSIS
Hyperventilation, Pregnancy, Liver failure, Methylxanthines

CASE 1
56F with vomiting and diarrhea 3 days ago despite intake of loperamide. Her last urine
output was 12 hours ago.
PE showed BP = 80/60, HR = 110, RR = 28. There is poor skin turgor.
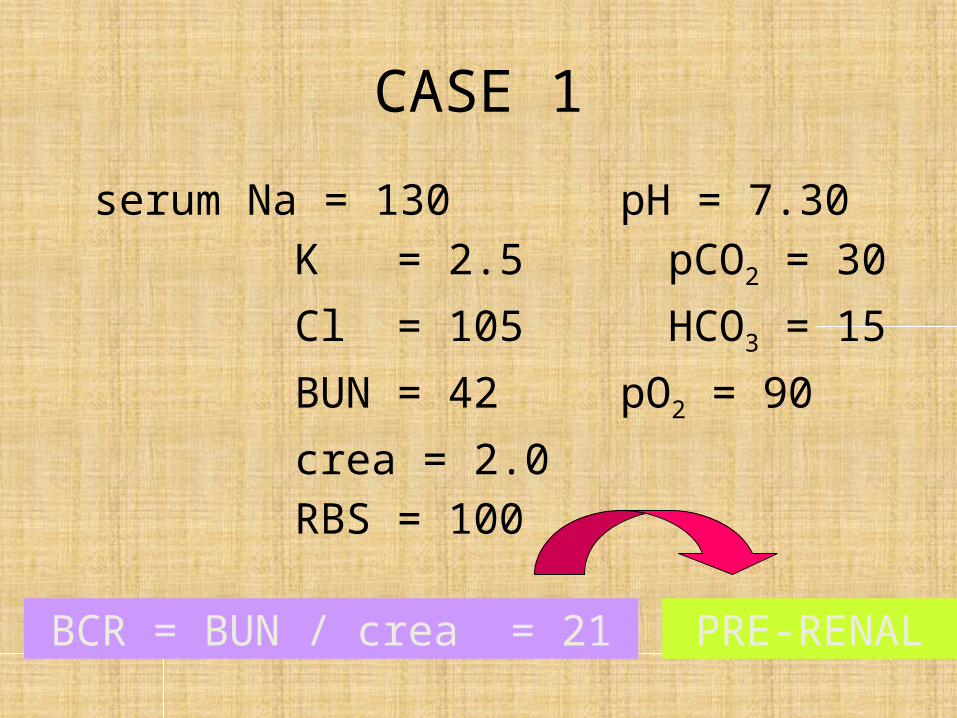
CASE 1
serum Na = 130 pH = 7.30 K = 2.5 pCO2 = 30 Cl = 105 HCO3 = 15 BUN = 42 pO2 = 90 crea = 2.0 RBS = 100
BCR = BUN / crea = 21 PRE-RENAL

CASE 1
serum Na = 130 pH = 7.30 K = 2.5 pCO2 = 30 Cl = 105 HCO3 = 15 BUN = 42 pO2 = 90 crea = 2.0 RBS = 100
pH = acidosis, pCO2 =alk, HCO3 = acidosis
Metabolic Acidosis

CASE 1
serum Na = 130 pH = 7.30 K = 2.5 pCO2 = 30 Cl = 105 HCO3 = 15 BUN = 42 pO2 = 90 crea = 2.0 RBS = 100
pCO2 = 15 x 1.5 + 8 = 30.5Compensated
Metabolic Acidosis

CASE 1
serum Na = 130 pH = 7.30 K = 2.5 pCO2 = 30 Cl = 105 HCO3 = 15 BUN = 42 pO2 = 90 crea = 2.0 RBS = 100
AG= 130 – (105+15) = 10 NAGMA

CASE 2
19F, fashion model, is surprised to find her K=2.7 mmol/L because she was normokalemic 6
months ago. She admits to being on a diet of fruit and vegetables but denies vomiting and
the use of diuretics or laxatives. She is asymptomatic. BP = 90/55 with subtle signs of
volume contraction.

CASE 2
serum Na 138 63 K 2.7 34 Cl 96 0 HCO3 30 0 pH 7.45 5.6 pCO2 45
Metabolic Alkalosis
Plasma Urine
pH = alk, pCO2 =acidosis HCO3 = alkalosis
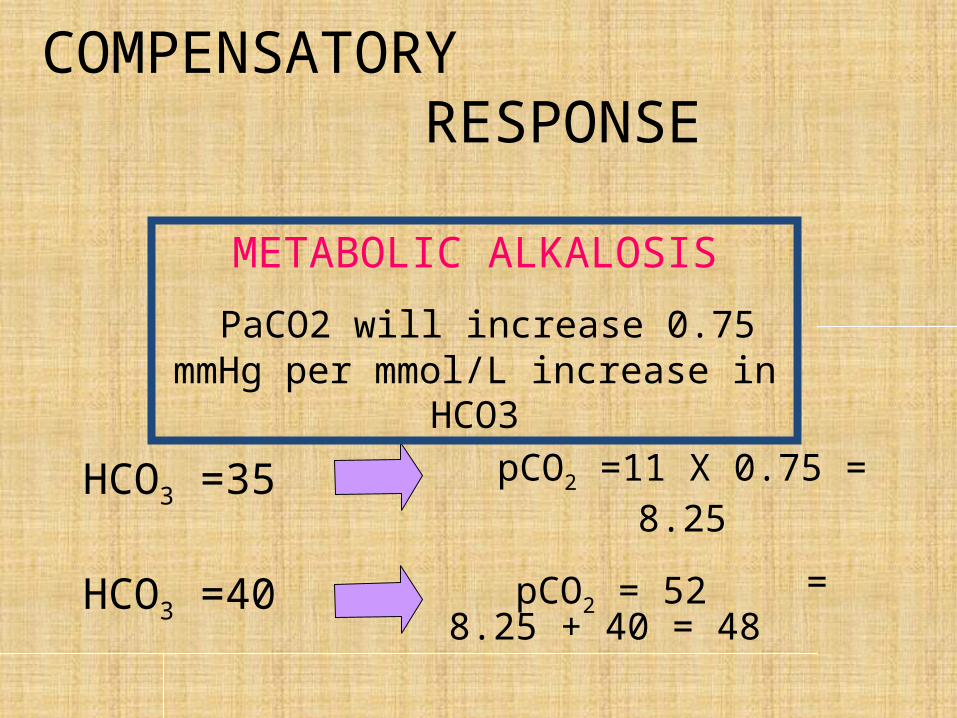
COMPENSATORY RESPONSE
HCO3 =35 pCO2 =11 X 0.75 = 8.25
= 8.25 + 40 = 48 pCO2 = 52HCO3 =40
METABOLIC ALKALOSIS
PaCO2 will increase 0.75 mmHg per mmol/L increase in HCO3


CASE 3
AG= 138 – (96+30) = 12 NAG
Plasma Urineserum Na 138 63
K 2.7 34 Cl 96 0 HCO3 30 0 pH 7.45 5.6 pCO2 45

CASE 3Plasma Urine
serum Na 138 63 K 2.7 34 Cl 96 0 HCO3 30 0 pH 7.45 5.6 pCO2 45
What is the cause of the acid base disorder?
CASE 4
73M with long standing COPD (pCO2 stable at 52-58 mmHg), cor pulmonale, and peripheral
edema had been taking furosemide for 6 months. Five days ago, he had anorexia,
malaise, and productive cough. He continued his medications until he developed nausea.
Later he was found disoriented and somnolent

CASE 4
PE: BP 110/70, HR 110, RR 24, T=40respiratory distressprolonged expiratory phasepostural drop in BPdrowsy, disorientedscattered rhonchi and rales BLFsdistant heart soundstrace pitting edema
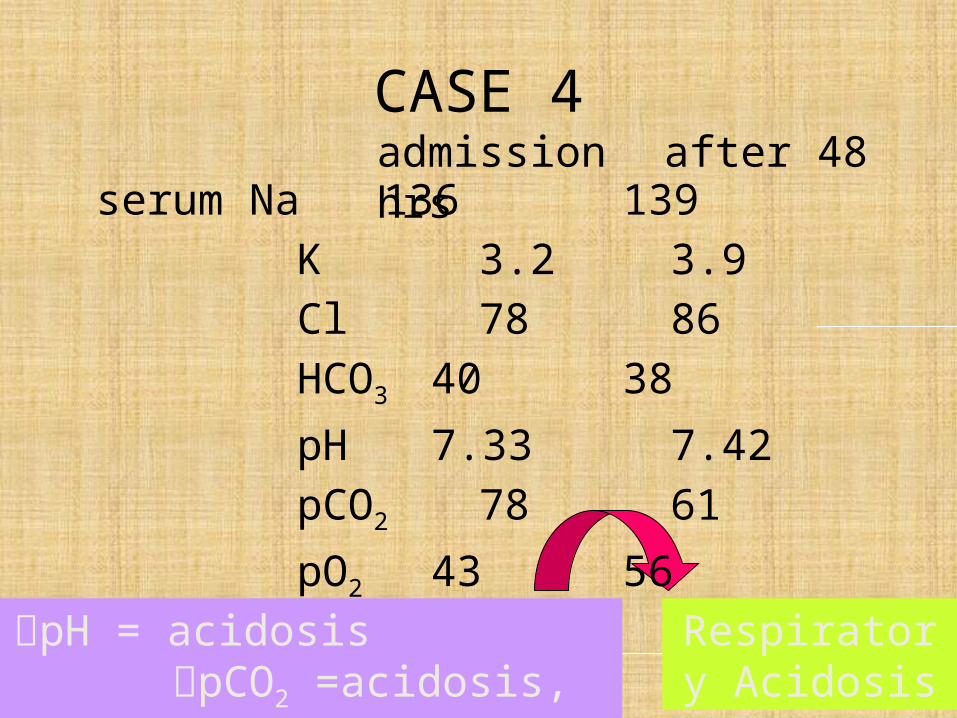
CASE 4admission after 48 hrs
pH = acidosis pCO2 =acidosis, HCO3 = alk
Respiratory Acidosis
serum Na 136 139 K 3.2 3.9 Cl 78 86 HCO3 40 38 pH 7.33 7.42 pCO2 78 61 pO2 43 56

COMPENSATORY RESPONSE
pCO2 =55 HCO3 = 25.5
HCO3 = 28pCO2 =80
ACUTE RESPIRATORY ACIDOSIS
HCO3 will increase 1 mmol/L per 10 mmHg increase in PaCO2

serum Na 136 139 K 3.2 3.9 Cl 78 86 HCO3 40 38 pH 7.33 7.42 pCO2 78 61 pO2 43 56
CASE 4admission after 48 hrs
HCO3 = 25.5
Respiratory Acidosis & M. Alkalosis
Check for Secondary Acid Base Disorders
Primary Acid Base Disorder
Compensation Secondary Base Disorder
Respiratory Acidosis
Actual increase of Hc03 from baseline is HIGHER than that of calculated compensation
Secondary Metabolic Alkalosis is present
Actual increase of Hc03 from baseline is LESS than that of calculated compensation
Secondary METABOLIC ACIDOSIS is present

CASE 5
42M, alcoholic, brought to the ER intoxicated. He was found at Rizal park in a pool of
vomitus. PE showed unkempt and incoherent patient with a markedly contracted ECF
volume. T=390 C with crackles on the RULF.

serum Na = 130 pH = 7.53 K = 2.9 pCO2 = 25 Cl = 80 HCO3 = 20 BUN = 34 pO2 = 60 crea = 1.4 alb = 38 RBS = 15 mmol/L
CASE 5
PRE-RENALBCR = 24
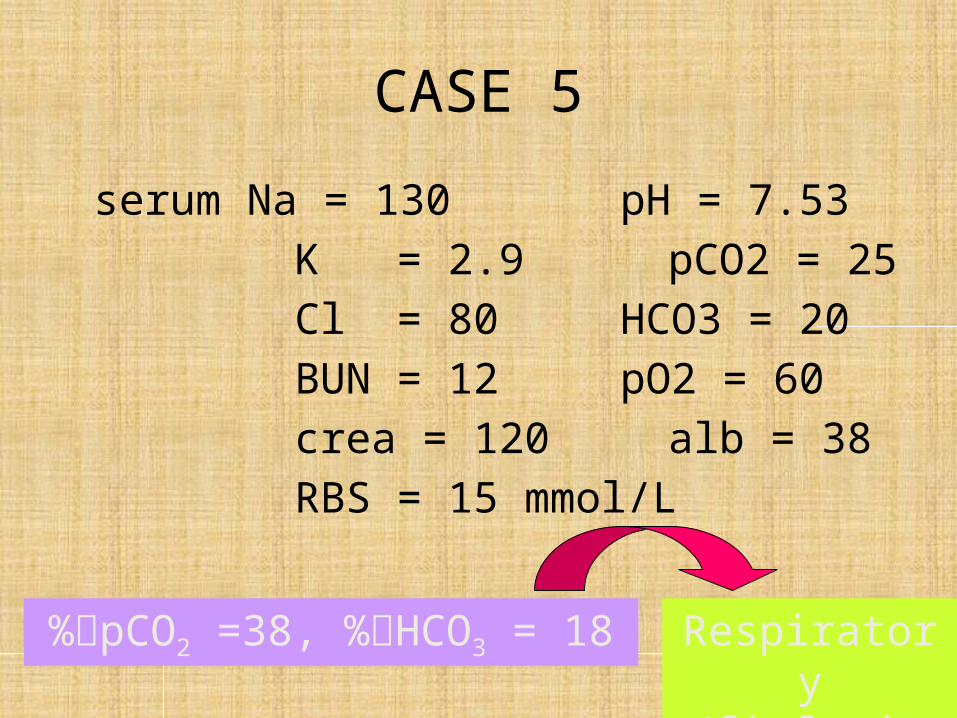
serum Na = 130 pH = 7.53 K = 2.9 pCO2 = 25 Cl = 80 HCO3 = 20 BUN = 12 pO2 = 60 crea = 120 alb = 38 RBS = 15 mmol/L
CASE 5
Respiratory Alkalosis
%pCO2 =38, %HCO3 = 18

COMPENSATORY RESPONSE
RESPIRATORY ALKALOSIS Acute: HCO3 will decrease 2 mmol/L per 10 mmHg decrease in PaCO2

serum Na = 130 pH = 7.53 K = 2.9 pCO2 = 25 Cl = 80 HCO3 = 20 BUN = 12 pO2 = 60 crea = 120 alb = 38 RBS = 15 mmol/L
CASE 5
Compensated Respiratory
AlkalosisHCO3 = 21

serum Na = 130 pH = 7.53 K = 2.9 pCO2 = 25 Cl = 80 HCO3 = 20 BUN = 12 pO2 = 60 crea = 120 alb = 38 RBS = 15 mmol/L
CASE 5
HAGMA + RAlkAG = 130 – (80 + 20) = 30
QUESTIONS?
Top Related