






Languages
Pages
Legal


AAMC Group on Faculty Practice Annual SymposiumNovember 4, 2011
Mark A. Kelley, M.D.
CEO, Henry Ford Medical Group

Profile of HFHS
• 95 y.o. hospital-based health system with―6 hospitals - flagship (HFH) in downtown
Detroit ―Health Alliance Plan - 500,000 HMO
members ―Employed physician practice (HFMG) -
1200 physicians in 30 locations ―$4B net revenue

What Is HFMG?
• A 40-specialty academic Medical Group practicing in 30 HFMG Medical Centers
• Employing 1,300 Senior Staff Physicians & Researchers along with 3,100 non-physician providers and support staff
• HFMG generates $750M in net revenue, which represents about 33% of total HFHS provider revenues
• 70% of the business in traditional fee-for-service, with the other 30% being global capitated (120,000 HMO members)
• Physicians generate 2.1M clinic visits annually
3

HFMG Medical Center
HFMG MC & UC
MC & 24 Hour ER
Hospital & ER
Macomb UC
Wyandotte MC & ED

HFMG Facts
• HFMG is the third largest academic group practice in the nation ($1.5B GPR) only behind Mayo and Cleveland Clinics
• HFMG generates 10,000 clinic visits per business
day
• The Group trains over 700 residents and fellows
• One-third of all physicians in the state of Michigan have been trained by HFMG

HFMG Structure
• Organized as blend of group and academic practice
• NOT a separate corporation but considered a separate business
• Led by HFMG CEO, COO, Chairs, Center Directors
• Elected Board of Governors

Henry Ford Medical Group and Medical Staff Governance Structure
Board of Governors
Bylaws & Governance
Professional Standards &
Conduct
Hospital Clinical Practice
Committee (formerly ka HMEC)
Research
Education
Institutional Animal Care & Use Committee
Institutional Review Board
Continuing Medical Education
Graduate Medical Education
Undergraduate Medical Educ.
Salary Manage-
ment
QualityCouncil
Credentials
Human Resources
Finance
5/4/2011
Biomedical EthicsCancer CoordinatingExecutive Committee, Institutional Critical Care
CPRInfection ControlInpatient Pharmacy and TherapeuticsMedical RecordsOperating Room Executive
Operating Room Quality Assurance
Practice Support
Committee
Organ ProcurementRadiation SafetySafety Disaster EnvironmentalTech. AssessmentTransfusion MedicineTrauma CareUtilization Management Ambulatory Nurse CouncilComplimentary & Integrative Medicine Advisory CouncilPharmacy
CEOHFMG
Physician Health &
Effectiveness
Salary Appeal

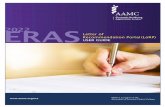
23.7%
17.8%
3.9%6.6%
16.3%
20.0%
3.7%
5.4%0.3% 2.1%
Henry Ford Medical Group2010 Payor Mix by Gross Revenue
Medicare
Medicare HMO
Medicaid
Medicaid HMO
Blue Cross
HAP Capitated
Other Managed Care
Commercial
Workers Comp
Self Pay

Annual Compensation Process
• Governed by the SMC and Board of Governors
• National and local market indicators used to assess HFMG competitiveness
• SMC also reviews interdepartmental compensation equity vis-à-vis prevailing market conditions
• Final compensation pool value is determined by CEO of HFMG, in collaboration with System Trustees

Total Cash Compensation (TCC)
• $170M Senior Staff Payroll
• 85% of TCC is base salary; 15% incentive
• TCC includes Base, Incentive and Moonlighting pay
• We use several types of wRVU-based incentive plans
• Incentive Plans have been in place since April 1998

The Elements of Every Practice
• Governance― Trustees (if any) ― Broad of Governors (peers)― Administrative Structure (operations)
• Economics― Revenue, expense, growth― Compensation― Funds flow in and out of the practice
• Academic Responsibilities (if any)• External Forces : economic, regulatory

Why Does the Practice Exist?
• Make $$ for: ― Shareholders of the Practice― Hospital/Corporation― Medical School/University― Research
• Provide Education• Conduct Research• Serve the Community
What are Your Priorities ?

HFMG’S Priorities (in Order)
• Take Great Care of Patients in Every Dimension
• Recruit and Retain the Best
• Create the Future of Medicine through Innovation and Medical Education
• Use Society’s Resources Wisely

How You See Your Medical Staff

How Others May See Your Staff

Worry #1 : Recruiting/Retaining Talent
• Establishing and Maintaining High Standards• Compensation• Leadership Development/Succession Planning• Generational issues – pro and con• Primary Care as Endangered Species• Advantages in academic practice
―Steady stream of new talent―The workhorse assistant professor

Who is in Charge?
Dean, Hospital CEO, Other? Department Chair?

Worry #2 –Governance and Leadership
• Chairs – team captains …or “autocratic Dukes” ?
• Administrators –Partners …or “Suits”―Practice/department managers―Finance team―Facility managers
• Board of Governors―Role --Operational vs. Strategic―Helpful for Peer review
• Tip : Trustees usually think like patients

…I can destroy You with…..

…FUNDS FLOW !

Worry #3 – Funds Flow
• No practice can live off professional revenue alone
• Downstream revenue counts the most • A consolidated bottom line and collaboration,
make funds flow irrelevant (like Mayo/Cleveland Clinics)
• Separate and competing bottom lines foster internal warfare
Those distracted by internal politics are conquered by those committed to growth

Run a Tight Ship (Minus the Mutiny)

Worry #4—Practice Discipline (just like Taking Care of Patients)
• Achievable/Understandable Goals• Accurate Data -- “What is the truth”?• Problems are made to be solved• Performance Expectations
― Transparent dashboards and consistent metrics― “Making Rounds” on the Practice with quarterly
reviews― Intelligent decisions at the unit level
Tip: no end runs; no upward delegation; no special deals that cannot be universally applied

Does Everyone Know the Plays and How We Keep Score ?

Worry #5 --Economics
• Top Line― Who negotiates your contracts, determines payer
mix, does your billing/collection?― Fee for Service vs. Bundled Payments –ready or
not? • Expenses
― Internal, what you control in your practice― External— e.g. allocations/overhead, taxes
• How do you manage? ― What do your docs understand? ― What benchmarks do you use?

Worry #6 –Fostering Quality
• Outpatient Practice― “Consumerism” –Access, Press-Ganey―HEDIS and other Pay for Performance― “Appropriateness”
• Inpatient Performance―Readmissions―Harm events―HCAPs/Core Measures

Yoda’s Rule: There is no “Try” – Only “Do, or Not Do”

Worry #7 –Competing Priorities
• Typical Tensions―Faculty time --Teaching and/or research vs.
practice―Profit at the expense of academics―Academic core in the midst of a non-academic
enterprise• Stay focused on your mission and make it part of
every message
Tip: Not everything is equally important, avoid institutional A.D.D.

Feel Like an Island in an Archipelago ?

Worry #8 –Islands Inhibit Progress
• Islands Within the Practice― Departments, divisions, inpatient vs. ambulatory― Docs vs. administrators― Researchers, educators, clinicians
• Islands in the Organization― Hospital vs. practice― School vs. hospital― Practice vs. everyone else
Archipelagos Survive Only When the Islands are United ( e.g. Japan, Great Britain)

Ready for Health Reform?



Defend Your Mission…But Embrace Change
Top Related