







Languages
Pages
Legal


CONTEMPORARY HEART FAILURE THERAPYA Brief Primer for the Clinician
Zachary D. Goldberger, MD, FACC, FAHA, FHRS, FACPAssistant Professor of Medicine
UW School of MedicineDivision of Cardiology
Harborview Medical [email protected]

Objectives
• Outline four novel therapies for chronic heart failure
• Describe indications, (very) brief pharmacology
• Emphasize evidence-base, management, cost
• Incorporate standard practice vs contemporary therapies

• 65-year-old man with HFrEF (LVEF 30%) is admitted in ADHF. After aggressive diuresis, you decide to reinitiate his outpatient regimen
• He is taking metoprolol succinate 25 mg daily, along with enalapril 5 mg bid, both prescribed 2 weeks ago (he never started them)
• His outpatient cardiologist was considering initiating spironolactone at his next follow-up appointment
Case 1

Along with reinitiating beta-blocker and furosemide, which option would you choose?a) Reinitiate enalapril 5 mg bidb) Initiate sacubritil-valsartan (Entresto) 200
mg bidc) Substitute lisinopril 5 mg bid for enalapril d) Add valsartan 80 mg bid to enalapril 5 mg
bide) Continue his prior regimen, and start
spironolactone

ARNIs: Mechanism
↓ Vasoconstriction↓ Blood pressure↓ Sympathetic tone↓ Aldosterone↓ Fibrosis↓ Hypertrophy↑ Natriuresis/diuresis

Ø n=8442Ø LVEF ≤35%, NYHA class II-IV HF Ø BNP level ≥150 pg/mL or NT-proBNP ≥600 pg/mLØ BNP ≥100 pg/ml or an NT-proBNP ≥400 pg/mL if hospitalized within 12
monthsØ SBP ≥100 mmHgØ eGFR ≥30 mL/min/m2
Ø Normal potassium levelØ Tolerant to ACE inhibitor/ARB therapy equivalent to at least enalapril
10 mg twice daily for ≥4 weeks
Sacubitril-valsartan 200 mg bidvs enalapril 10 mg bid
ARNIs: Evidence-Base
McMurray JJV et al. N Engl J Med 2014; 371:993-1004.
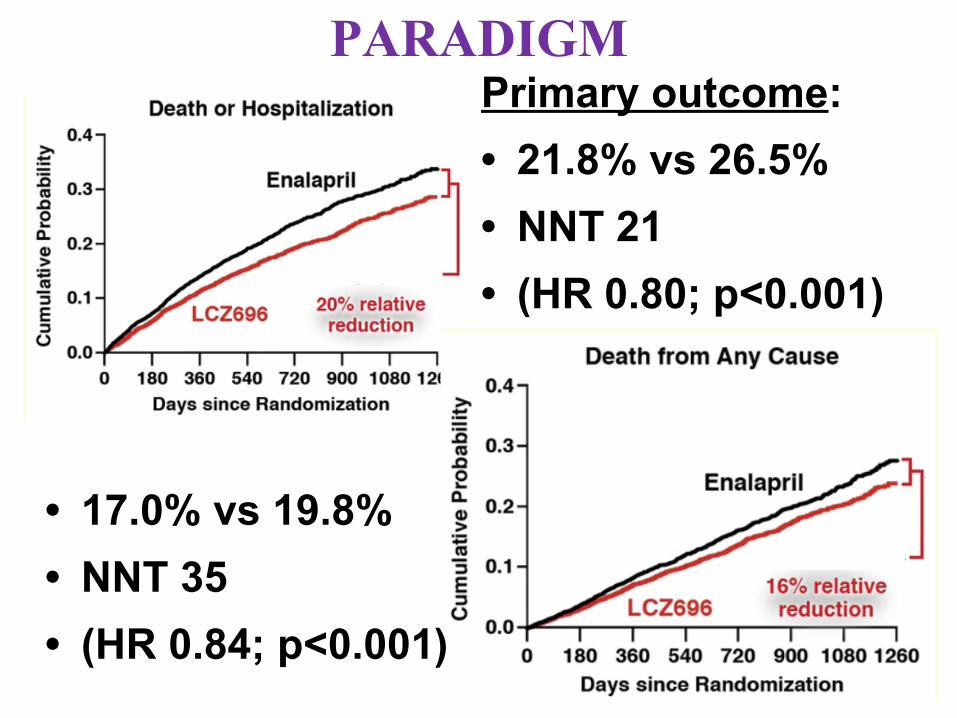
Primary outcome:• 21.8% vs 26.5% • NNT 21• (HR 0.80; p<0.001)
• 17.0% vs 19.8% • NNT 35• (HR 0.84; p<0.001)
PARADIGM

PARADIGM
• Sacubitril-valsartan superior to enalapril in: Ø CV deathØ HF hospitalizationØ All-cause deathØ HF symptoms / physical limitations

PARADIGM Shift?
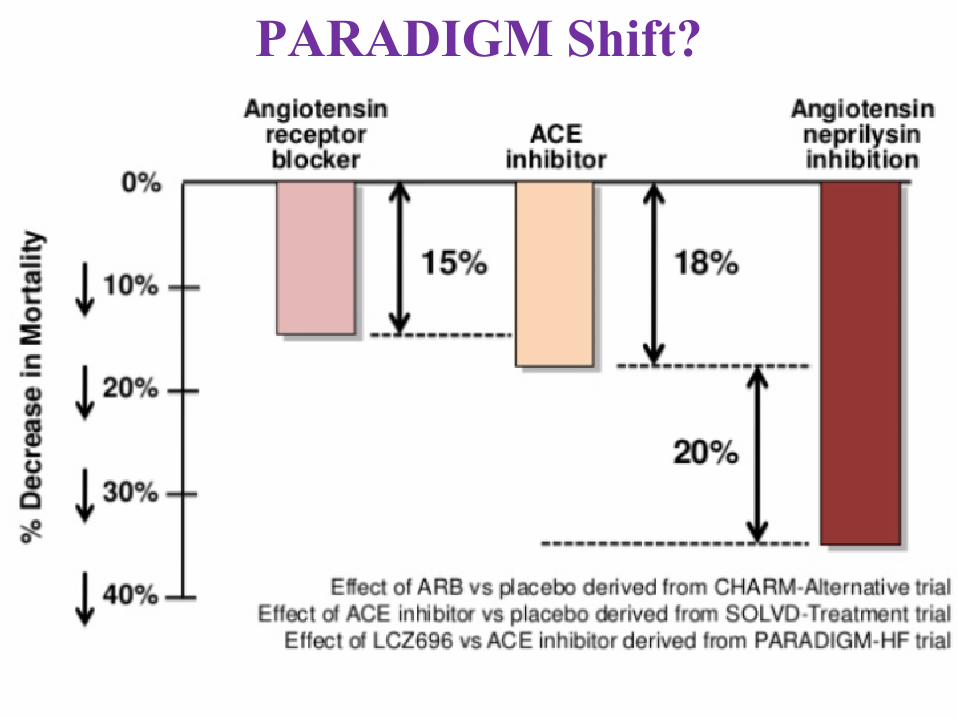
PARADIGM Shift?

Prescription Monthly Retail Price (goodrx.com)
Generic Discount Program Price
Carvedilol 25 mg bid $73.99 $4Lisinopril 40 mg daily $22.39 $4Losartan 100 mg bid $184.86 $10Metoprolol succinate 200 mg daily
$70.99 $15
Spironolactone 25 mg daily $28.88 $4Sacubitril/valsartan 97/103 mg bid
$421.48 n/a
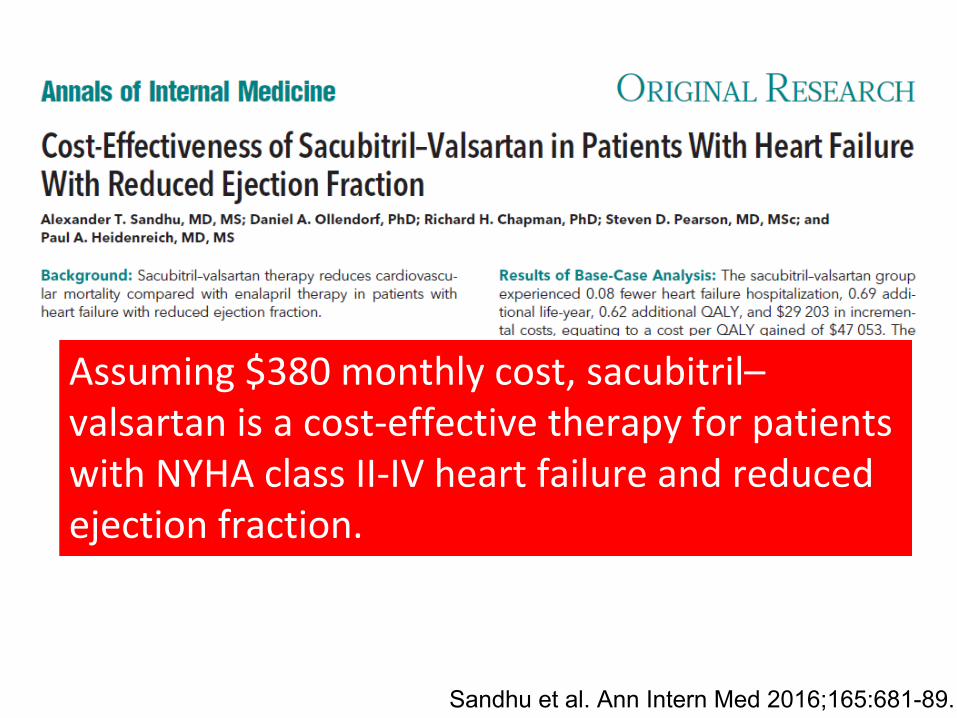
Assuming $380 monthly cost, sacubitril–valsartan is a cost-effective therapy for patients with NYHA class II-IV heart failure and reduced ejection fraction.
Sandhu et al. Ann Intern Med 2016;165:681-89.

• ARNI for patient who have tolerated ACE/ARB (equivalent to enalapril 10 mg bid) for ≥4 weeks
• NEED a 36-hour ACE inhibitor washout period prior to starting sacubitril-valsartan
ARNI: Management

• ACE inhibitor/ARB: start within 24-48 hours, hemodynamically stable, prior to hospital discharge
• Initiate mineralocorticoid receptor antagonist prior to / soon after discharge, unless there are concerns about potassium (e.g., recent uptitration of ACE/ARB prior to admit)
• Ensure frequent HF follow-up for dose adjustments, optimization
Initial HF Regimen Options

ARNIs: In the Guidelines
Yancy et al. 2016 ACC/AHA/HFSA focused update on new pharmacological therapy for heart failure. Circulation, 2016.
The clinical strategy of inhibition of the renin-angiotensin system with ACE inhibitors OR ARBs OR ARNI in conjunction with evidence-based beta blockers, and aldosterone antagonists in selected patients, is recommended for patients with chronic HFrEF to reduce morbidity and mortality.
I
ACE: A
ARB: A
ARNI: B-R
In patients with chronic symptomatic HFrEF NYHA class II or III who tolerate an ACE inhibitor or ARB, replacement by an ARNI is recommended to further reduce morbidity and mortality.
I B-R
ARNI should not be administered concomitantly with ACE inhibitors or within 36 hours of the last dose of an ACE inhibitor
III B-R

You are evaluating a patient admitted 3 days ago with a mild HFrEF exacerbation, now ready for discharge. Which of the following suggests a high risk for future adverse events?
a) Heart rate 90 bpmb) Blood pressure 110/70 mmHgc) Respiratory rate 14/mind) SpO2 94%, ambient air
Case 2

• Elevated HR associated with worse CV outcomes
• Ivabradine has beneficial effects
• Heart rate control vs abnormal neurohormonal mileau?
Heart Rate in Heart Failure

• Novel heart rate-lowering agent
• Selective inhibition of If (“funny”) current in sinoatrial node
• Action limited to heart rate reduction
Ivabradine: Mechanism

Olshansky B. J Am Coll Cardiol 2013; 61(8):793-801.

Ivabradine: Mechanism
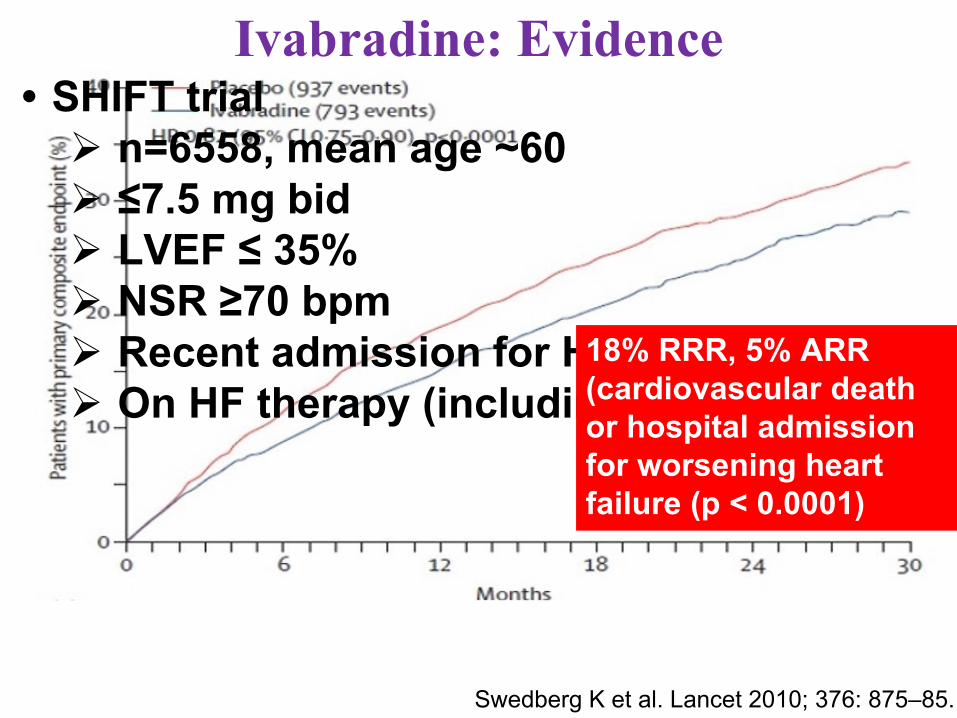
Ivabradine: Evidence
Swedberg K et al. Lancet 2010; 376: 875–85.
• SHIFT trialØ n=6558, mean age ~60Ø ≤7.5 mg bidØ LVEF ≤ 35%Ø NSR ≥70 bpmØ Recent admission for HFØ On HF therapy (including ß-blockers)
18% RRR, 5% ARR (cardiovascular death or hospital admission for worsening heart failure (p < 0.0001)

Swedberg K et al. Lancet 2010; 376:875–85.
Effect on 1° endpoint driven by Ø26% RRR (5%
ARR) HF admissions
Ø26% RRR (2% ARR) in HF death
Ivabradine: Evidence (2)

90% on beta-blockers, but only 26% on target doses (and 56% at ≥50% target dose)
Beta-Blocker Effect?
Beta-blocker
First dose(mg)
Target dose (mg)
Clinical trial mean dose (mg)
SHIFT trial mean dose (mg)
Bisoprolol 1.25 10 8.6 (CIBIS II)
6.2
Carvedilol 3.125 50 37 (CAPRICORN)
25
Metoprolol succinate
12.5/25 200 159 (MERIT-HF)
90
Nebivolol 1.25 10 7.7 (SENIORS)
5.9

Optimal Heart Rate?Patients with lowest heart rate (<60 bpm) had fewer primary events patients in the higher heart-rate groups
Böhm M et al. Lancet 2010;376:886-94.

Are these results generalizable? Which of the following patients with NYHA Class III HFrEF may not benefit?
a) 65-year-old with permanent atrial fibrillation and an average HR of 98 bpm
b) 70-year-old woman on carvedilol 12.5 mg bid, HR 85 bpm, BP 95/60 mmHg
c) 67-year-old with HR 80 bpm, s/p STEMI and PCI to the LAD 6 months ago, on metoprolol succinate 100 mg bid
Generalizable?

Ivabradine: In the GuidelinesIvabradine can be beneficial to reduce HF hospitalization for patients with symptomatic (NYHA class II-III) stable chronic HFrEF (LVEF ≤35%) who are receiving GDEM, including a beta blocker at maximum tolerated dose, and who are in sinus rhythm with a heart rate of 70 bpm or greater at rest
IIa B-R
Ivabradine is reasonable for ongoing management in patients with symptomaticInappropriate sinus tachycardia
IIa B-R
Yancy CW et al. 2016 ACC/AHA/HFSA focused update on new pharmacological therapy for heart failure. Circulation, 2016.Page RL et al. 2015 ACC/AHA/HRS guideline for the management of adult patients with supraventricular tachycardia. Circulation, 2015.

Ivabradine should be considered in chronic HF patients treated with β-blockers whose heart rate remains elevated regardless of efforts to maximize β-blocker dose.
Ivabradine: When to Prescribe
Cost (per GoodRx)Ø5 mg bid Ø$422-438 for one month rx

Device-Based Technology• ICDs offer significant mortality reduction in
patients with symptomatic HF and LVEF ≤35• CRT has also improved outcomes in
patients with wide QRS (e.g., LBBB)• Some models offer features designed to
predict exacerbations, and potentially avoid rehospitalization

Intrathoracic Impedance Monitoring
• Optivol® (Medtronic)• Measures intrathoracic impedance
(inversely correlated with pulmonary edema, PCWP)

Optivol
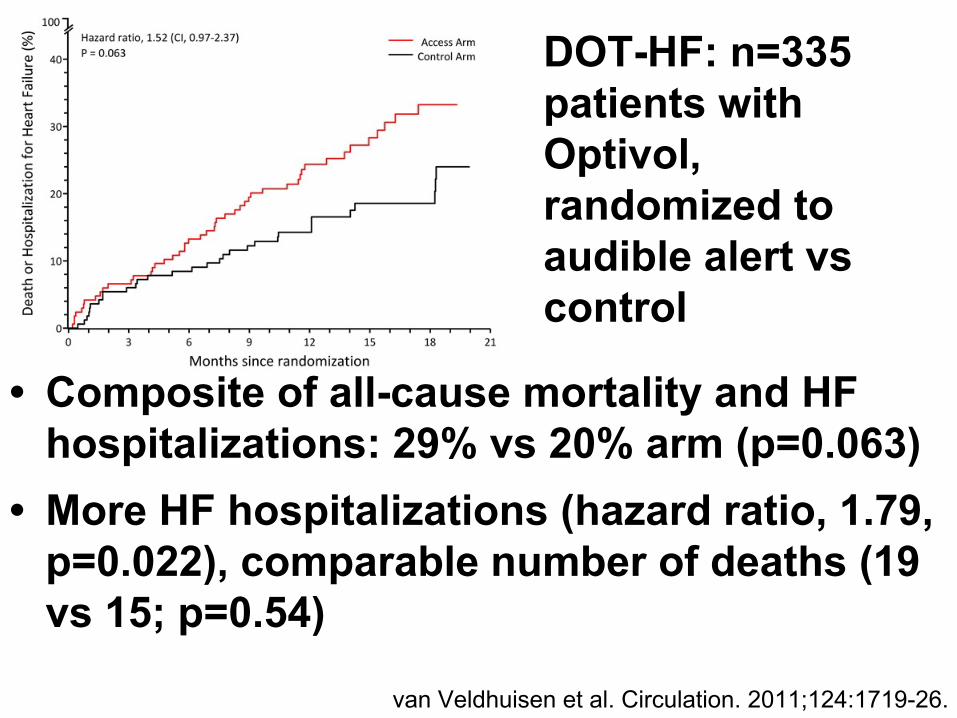
van Veldhuisen et al. Circulation. 2011;124:1719-26.
• Composite of all-cause mortality and HF hospitalizations: 29% vs 20% arm (p=0.063)
• More HF hospitalizations (hazard ratio, 1.79, p=0.022), comparable number of deaths (19 vs 15; p=0.54)
DOT-HF: n=335 patients with Optivol, randomized to audible alert vs control
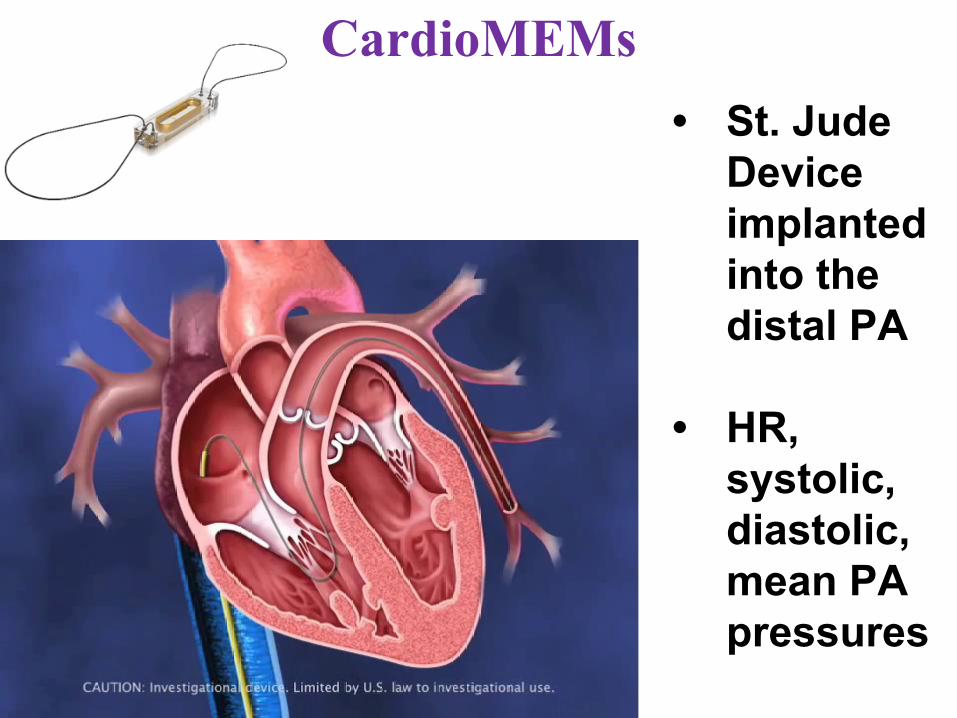
CardioMEMs• St. Jude
Device implanted into the distal PA
• HR, systolic, diastolic, mean PA pressures
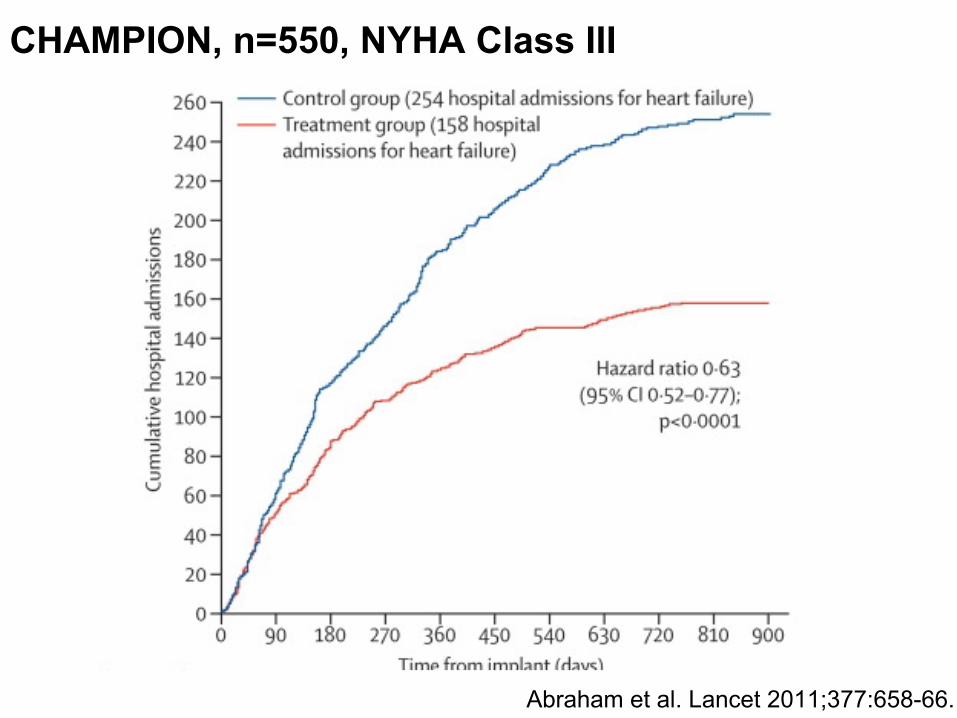
CHAMPION, n=550, NYHA Class III
Abraham et al. Lancet 2011;377:658-66.

Conclusions• Sacubitril-valsartan is a game-changer,
superior to ACE/ARB (may replace), and likely first-line; costs may be prohibitive
• Ivabradine targets HR: lower than 70 bpm on optimal BB therapy likely saves lives
• Novel device monitoring offers promise, but outcomes are unclear, infrastructure may pose limitations
Top Related