







Languages
Pages
Legal

1
Resistance and Tropism - Maraviroc
Lisa K. Naeger, Ph.D.
Division of Antiviral ProductsFood and Drug Administration
April 24, 2007 FDA Antiviral Advisory Committee Meeting
2
Maraviroc Resistance and Tropism
• Novel Target–host receptor
• Unique Resistance Issues–resistance to MVC–tropism switching –outgrowth of CXCR4-tropic virus

3
Baseline Analyses Studies 1027 and 1028
• Genotypic susceptibility scores (GSS) and phenotypic susceptibility scores (PSS) were balanced across treatment groups– median GSS = 1 – median PSS = 2
Heavily treatment-experienced population• 67% had overall susceptibility scores <2• 30% had one potentially active drug in their OBT• 14% had no potentially active drug in their OBT

4
Tropism at Baseline
• 2560 screened; 56% were CCR5-tropic
• 90% of enrolled subjects had CCR5-tropic virus at Baseline
– 4% had Dual-mixed tropic virus
– 5% had non-typable virus
5
Why Did Subjects Fail MVC Treatment in Studies 1027 and 1028?
• CCR5 to CXCR4 co-receptor switch through virus mutation
• Outgrowth of MVC resistant CCR5-tropic viruses
• Outgrowth of CXCR4-tropic viruses undetected at baseline
• Resistance to Optimized Background Therapy• Host CCR5 genotype

6
FDA Censored Dataset for “As-Treated” Analyses
FDA Censored: Subjects who• Discontinued while suppressed (<400 copies/mL)• Discontinued with >400 copies/mL between Baseline and Week 4 • Discontinued between Baseline and Week 8 with at least 0.5 log decrease and no rebound (previous ≥2 log decrease with 1 log increase)
Overall Number of subjects in Pfizer virology dataset 1050
Overall number of subjects in virology dataset from FDA
962
FDA Censored 88
Studies 1027 and 1028

7
Tropism at Failure
8
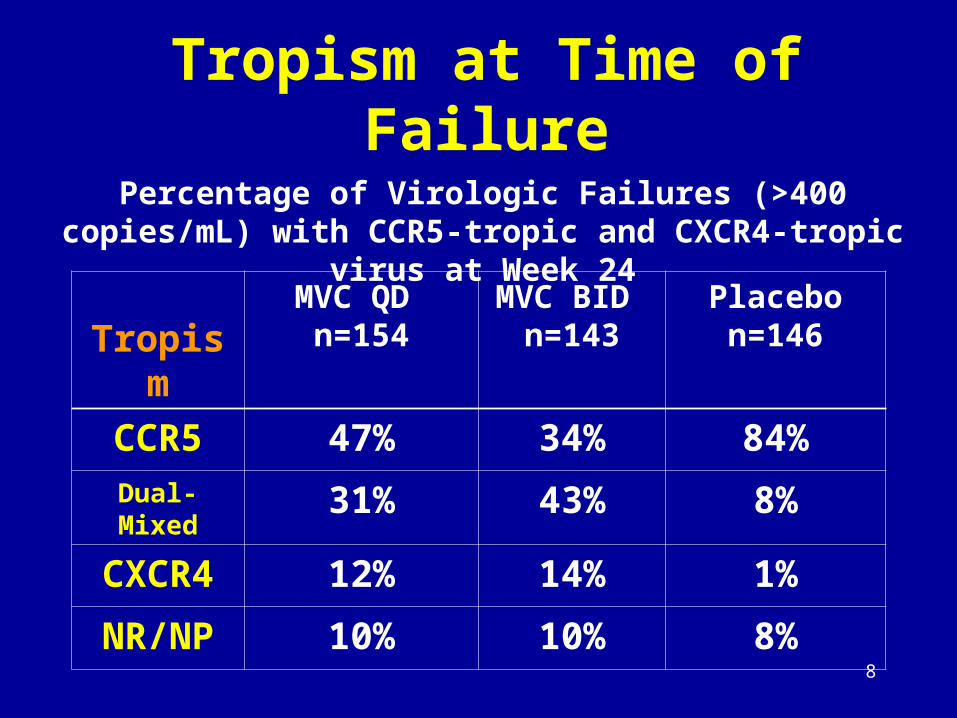
Tropism at Time of Failure
Percentage of Virologic Failures (>400 copies/mL) with CCR5-tropic and CXCR4-tropic virus at Week 24
TropismMVC QD
n=154MVC BID
n=143Placebo n=146
CCR5 47% 34% 84%Dual-Mixed 31% 43% 8%
CXCR4 12% 14% 1%
NR/NP 10% 10% 8%

9
Resistance to Optimized Background Therapy

10
Responders (<400 copies/mL) by Susceptibility Score at Baseline
0
10
20
30
40
50
60
70
80
90
0 1 2 3+
MVC QDMVC BIDPlacebo
Overall Susceptibility Score
11
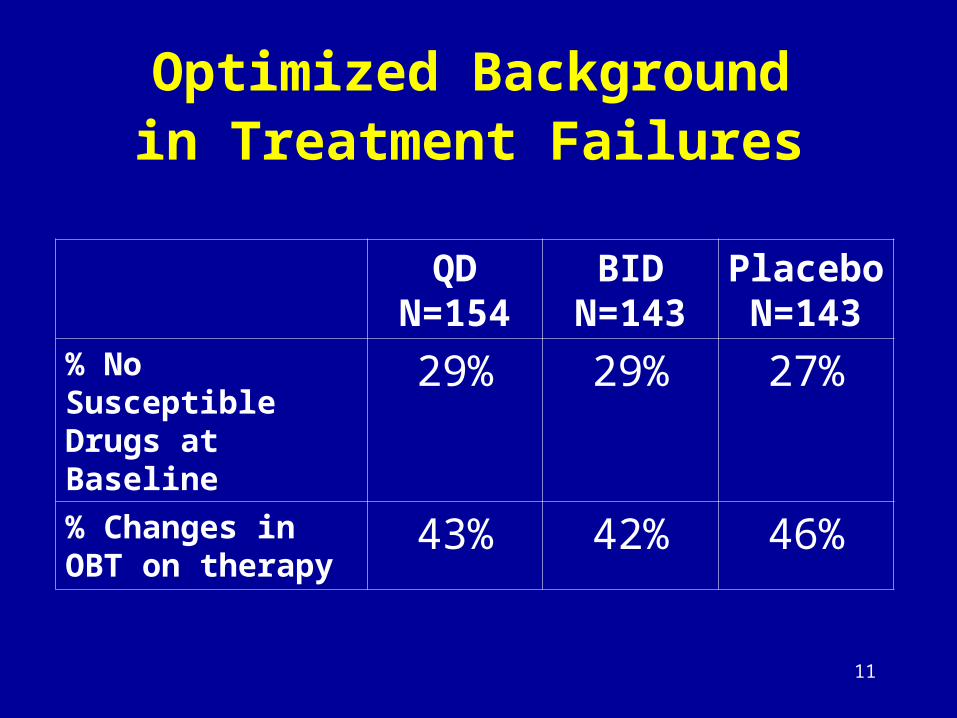
Optimized Background in Treatment Failures
QDN=154
BIDN=143
PlaceboN=143
% No SusceptibleDrugs at Baseline
29% 29% 27%
% Changes inOBT on therapy
43% 42% 46%
12
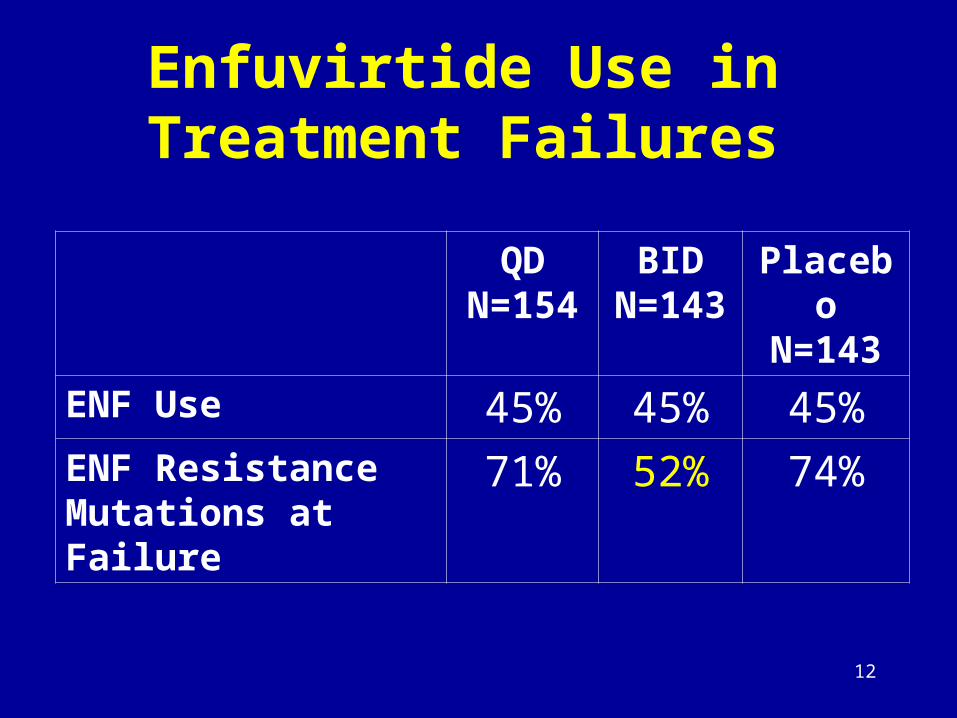
Enfuvirtide Use inTreatment Failures
QDN=154
BIDN=143
PlaceboN=143
ENF Use 45% 45% 45%ENF Resistance Mutations at Failure
71% 52% 74%

13
Overall Susceptibility Scores of Treatment Failures by Tropism
OSSCXCR4-tropic
n=29CCR5-tropic
n=163Dual/Mixed
n=94All
n=320
0-1 80% 55% 63% 60%
2 17% 24% 23% 23%
≥3 3% 19% 11% 15%
14
Virology Sub-Studies
Comprehensive analysis requested –Treatment failures and/or
–Change in HIV co-receptor tropism

15
Failure with CCR5-Tropic Virus:
• Determine maraviroc susceptibility in cell culture
• Nucleotide sequence analysis of the gp120 region to identify amino acid substitutions
• Nucleotide sequence analysis of protease and RT regions

16
Failure with CXCR4-Tropic Virus:
• Baseline and on-treatment clonal evaluation of virus to determine the relative number of CXCR4-tropic and CCR5-tropic viral isolates.
• Nucleotide sequence analysis of the gp120 region to identify amino acid changes that may contribute to a co-receptor switch to CXCR4
• Phylogenetic analysis to determine the relationship of emerging CXCR4-tropic virus to the CCR5-tropic virus at baseline
• Nucleotide sequence analysis of protease and RT

17
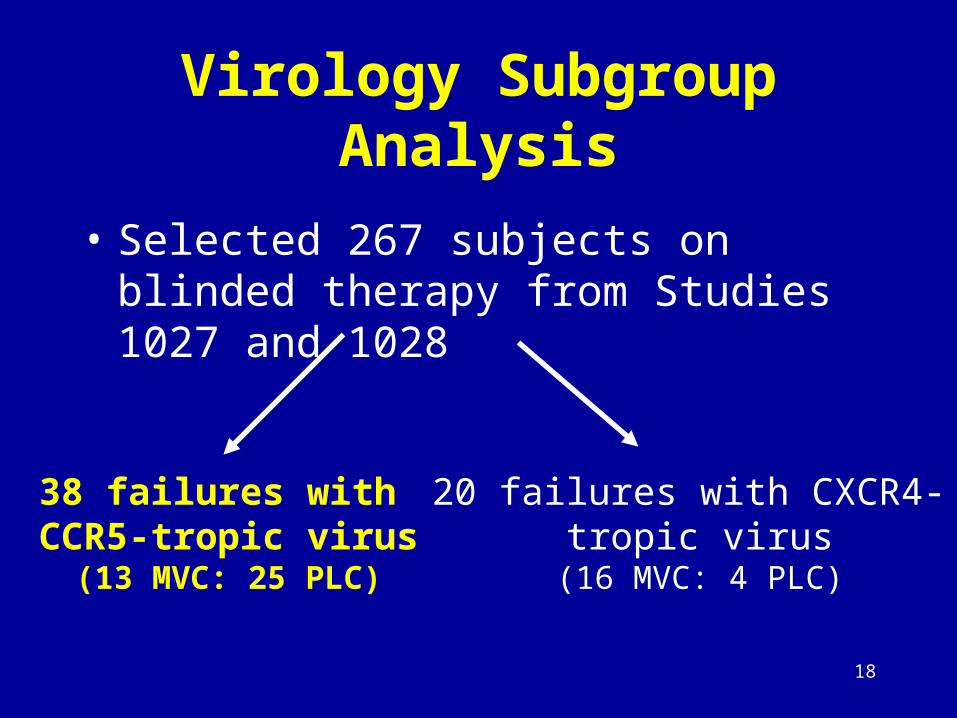
Virology Subgroup Analysis
• Selected 267 subjects on blinded therapy from Studies 1027 and 1028
38 failures with CCR5-tropic virus(13 MVC: 25 PLC)
20 failures with CXCR4- tropic virus
(16 MVC: 4 PLC)
18
Virology Subgroup Analysis
• Selected 267 subjects on blinded therapy from Studies 1027 and 1028
38 failures with CCR5-tropic virus
(13 MVC: 25 PLC)
20 failures with CXCR4- tropic virus
(16 MVC: 4 PLC)
19
Subjects Failing with CCR5-Tropic Virus
• Virus from 2 subjects had 3-fold shifts in MVC susceptibility at failure
• All other subjects on maraviroc had EC50 FC values <2-fold within the normal range of the Monogram assay (0.32-1.95)

20
Subjects Failing with CCR5-Tropic Virus
• Viruses from 5 subjects showed evidence of a lower plateau in maximum percentage inhibition
• All had novel amino acid changes in the V3 loop at time of failure

21
Genotypic Changes on Maraviroc in gp120
• V3 loop sequences were heterogeneous
with multiple substitutions
• Changes at either amino position 13 or 26 were seen in the V3 loop in 5/5 subjects with MVC-associated lower plateaus in MPI

22
Role of the V3 Loop Amino Acid Substitutions in MVC Resistance
• Site-Directed Mutagenesis• In 2 subjects
– Mutating amino acids in baseline clones resulted in the MVC resistance phenotype of <95% MPI
– Back-mutation of the amino acid changes of the failure clones resulted in a MVC-sensitive phenotype

23
Some Subjects had No Phenotypic Markers of MVC Resistance
• 7 subjects receiving MVC showed no phenotypic markers of MVC resistance
• 5/7 had evidence of reduced susceptibility to 1 or more drugs in OBT at screening and/or failure
24
Virology Subgroup Analysis
• Selected 267 subjects on blinded therapy from Studies 1027 and 1028
38 failures with CCR5-tropic virus(13 MVC: 25 PLC)
20 failures with CXCR4- tropic virus
(16 MVC: 4 PLC)

25
Clonal EvaluationOne subject:
192 pre-treatmentclones
48 on-treatmentclones
Pink = R5Green = X4Blue = dual/mixed

26
20 Treatment Failure Subjects with CXCR4-Tropic Virus
• 14 subjects– CXCR4-tropic ‘on-treatment’ clones shared a
common ancestor with a pre-treatment CXCR4-tropic virus.
• 6 subjects– CXCR4-tropic ‘on-treatment’ clones were genetically
distinct from both the ‘pre-treatment’ and ‘on-treatment’ R5 population.
– The V3 loop sequences differed by 7-17 amino acid residues from the nearest R5 sequence on the phylogenetic tree.

27
Greatest Proportion of MVC Failures had Dual-Mixed or CXCR4-Tropic Virus
• Mutation from a CCR5 progenitor -Tropism switch
• Outgrowth of undetected CXCR4-virus at screening
28
Why Did Subjects Fail Treatment in MVC Studies 1027 and 1028?
• Outgrowth of CXCR4-using viruses not detected at screening
• CCR5-using viruses: some are resistance to MVC
• Resistance to OBT
• CCR5 receptor genotype?
29
What is the Outcome of Failures who had CXCR4-Tropic Virus Emerge on
MVC Treatment?
• Evolution to a CXCR4-utilizing HIV may result in a more virulent virus
• Concern that MVC use will result in worse outcomes for patients because of outgrowth of CXCR4-tropic virus

30
CD4+ Cell Counts Mean (median) Change in CD4 counts from Baseline
LOCF24
Tropism at Failure QD
N=154BID
N=143PlaceboN=146
R5 123 (93)N=72
128 (110)N=48
38 (11)N=122
CXCR4 60 (33)N=18
52 (31)N=20
76N=1
Dual-Mixed 47 (25)N=48
63 (58)N=61
43 (14)N=11
NR/NP 70 (70)N=16
99 (103)N=14
63 (29)N=12
31
Follow-Up on Failures with CXCR4-Tropic Virus
• Viral load
• CD4+ cell counts
• HIV co-receptor tropism
• AIDS defining events

32
Follow-Up Data (n=20)
• 2/3 had changed tropism back to CCR5 or dual-mixed • For the subjects with CCR5- or dual/mixed-tropic virus at
end of follow-up, the median time to last follow-up was approximately 5 months (range 18 days to 8 months).
• In contrast, the follow-up time for the subjects who remained CXCR4-tropic at the last follow-up visit was one month or less (median time was approximately 11 days).
Number# X4-tropic
Virus at Follow-up# DecreasedCD4+ cells
Mean changeCD4+ cells
20 35% (7) 50% (10) -21
33
Follow-Up Data (n=20)
• Viral loads remained similar to the value at treatment failure
• No new category C AIDS-defining events were reported
• 4 subjects went on a new ARV treatment – viral loads decreased – CD4+ cell count increased
34
Tropism Summary
• ~50-60% subjects failed with CXCR4- or dual/mixed-tropic virus in the MVC arms
• Prominent reason for failure in these studies was outgrowth of a minor CXCR4-tropic virus population not detected at screening

35
Resistance Summary
• Maraviroc treatment failure with CCR5-tropic virus also occurred
– phenotypic and genotypic resistance to MVC
– resistance to Optimized Background Therapy
• CCR5 host receptor genotype?

36
Maraviroc Resistance
• Lower plateaus in MPI were detected in viruses from 5 subjects failing maraviroc regimens
• Changes in the V3 sequence of gp160 correlated with the presence of lower plateaus and maraviroc resistance

37
Back-Up Slides
Lisa K. Naeger, Ph.D.
Division of Antiviral ProductsFood and Drug Administration
April 24, 2007 FDA Antiviral Advisory Committee Meeting

38
Failures with 32 Deletion/WT or CCR5 Promoter Haplotypes
QD BID Placebo
D32/WT 8% (13/154) 3% (5/143) 6% (9/143)
WT/WT 84% (130/154) 89% (127/143) 85% (122/143)
P1 46% (71/154) 41% (59/143) 46% (31/143)
P4 11% (17/154) 12% (17/143) 12% (143)
P1/P4 33% (51/143) 34% (49/143) 31% (45/143)
Top Related