







Languages
Pages
Legal


1
CQC’s new approach to inspecting and regulating GP and OOH providers
January 2015
WelcomeAmanda Reynolds
Inspection manager (acting)
2
3
Our purpose and role
Our purposeWe make sure health and social care services provide people with safe, effective, compassionate, high-quality care and we encourage care services to improve.
Our roleWe monitor, inspect and regulate services to make sure they meet fundamental standards of quality and safety and we publish what we find, including performance ratings to help people choose care.We will be a strong, independent, expert inspectorate that is always on the side of people who use services.
4
Developing the changes
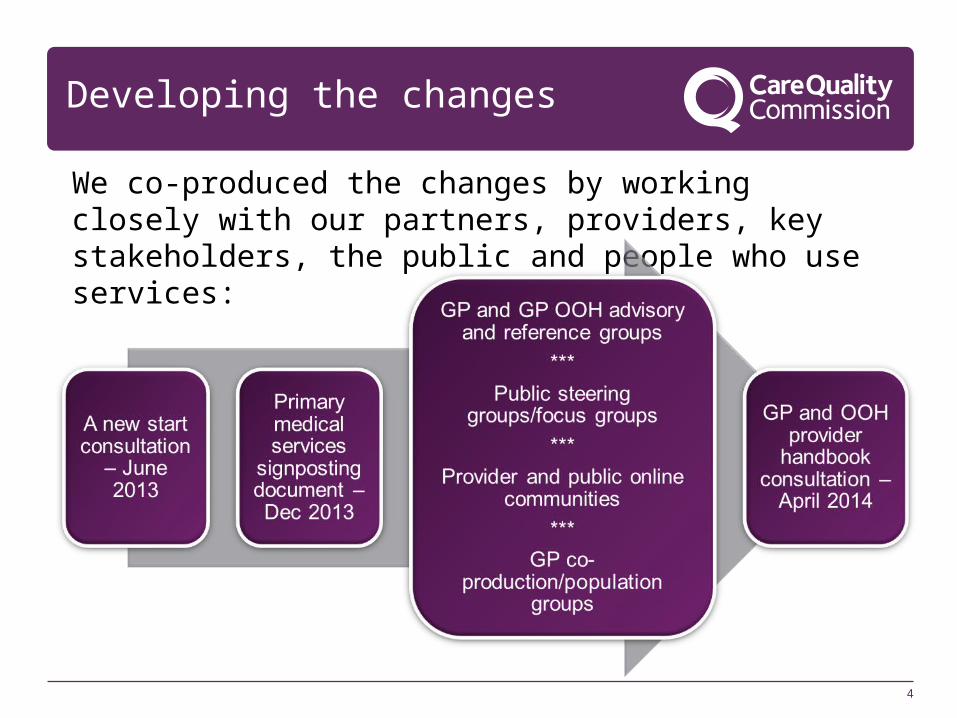
We co-produced the changes by working closely with our partners, providers, key stakeholders, the public and people who use services:
5
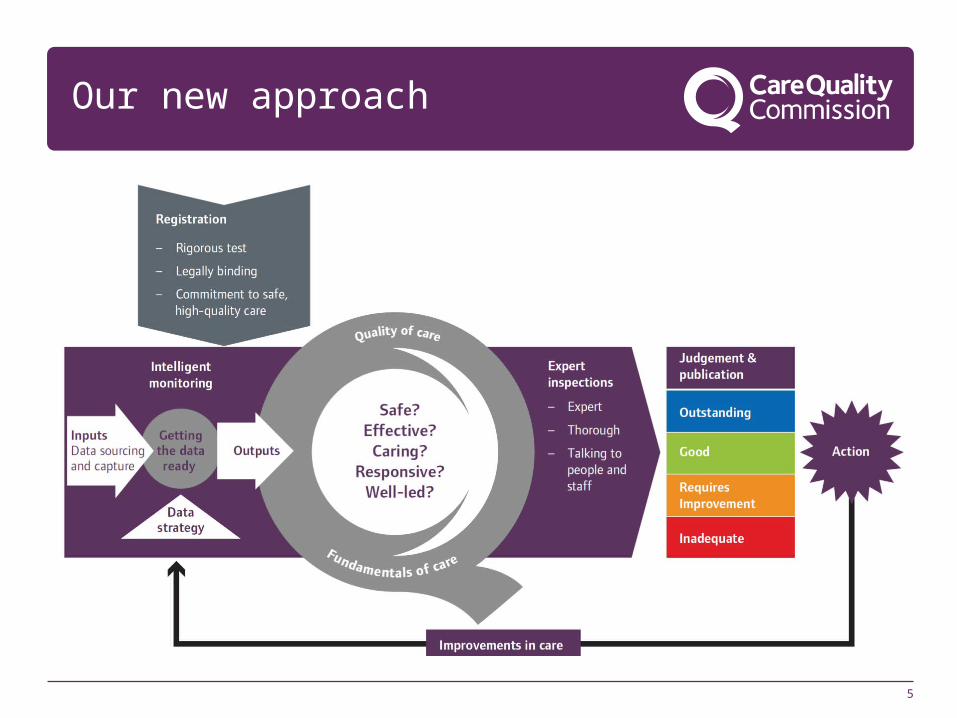
Our new approach
What are we doing differently?
• Inspection teams of specialist inspectors, GPs, practice nurses or practice managers.
• Inspections of a number of practices carried out in a CCG area over a 2-4 week period.
• Introductions of ratings for GP practices telling patients whether they are: outstanding, good or whether they require improvement or are inadequate.
• Strengthening our Intelligent Monitoring of providers using nationally held data and local intelligence.
• New ways of gathering patient views both before and during inspection.
• Develop a clear approach to responding to failing practices, working with NHS England.
Our key questions
Is the quality of care:•Safe? people are protected from abuse and avoidable harm.
•Effective? people’s care, treatment and support achieves good outcomes, promotes a good quality of life and is based on the best available evidence.
•Caring? staff involve and treat people with compassion, kindness, dignity and respect.
•Responsive? services are organised so that they meet people’s needs.
•Well-led? the leadership, management and governance of the organisation assures the delivery of high-quality care, supports learning and innovation, and promotes an open and fair culture.
7
Intelligent monitoring
• Intelligent Monitoring is a tool to help our inspectors understand the areas of care that need to be followed up.
• Looks at set of indicators including patient experience and statistical measures of performance.
• The indicators relate to the five questions we ask all services.
• The indicators will be used to raise questions, not make judgements – our ratings do that.
8
Key lines of enquiry
• For each of the five key questions there are between three to five key lines of enquiry (KLOEs).
• For each KLOE we have identified characteristics of good.
• They support consistency and ensure we focus on areas that matter most.
• KLOEs are supported by guidance on key things to consider; these are called prompts.
9

Key lines of enquiry continued…
11
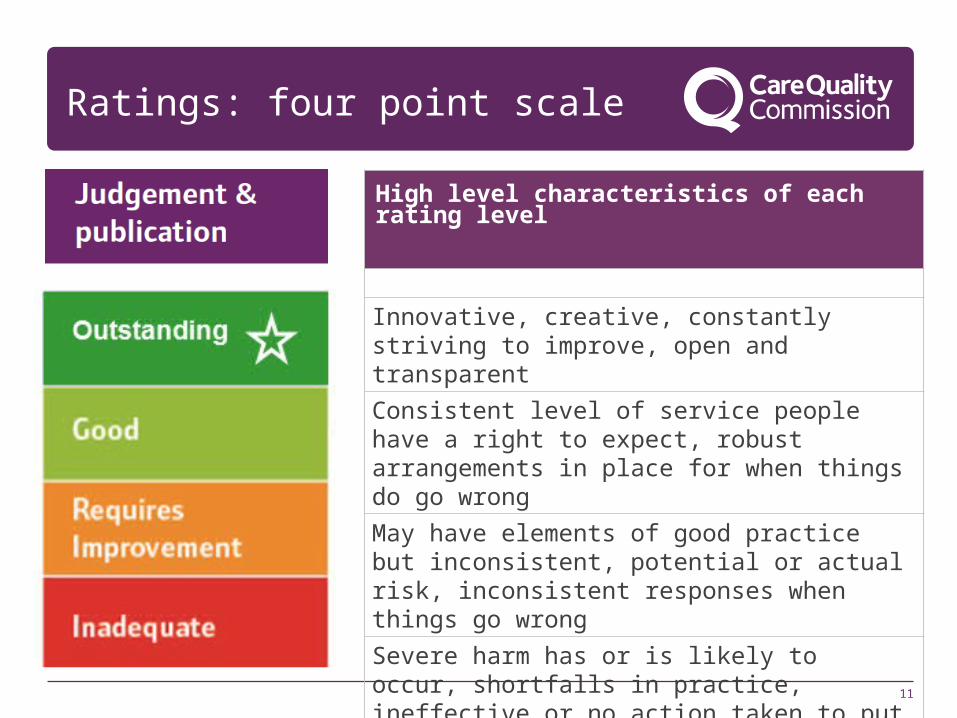
Ratings: four point scale
High level characteristics of each rating level
Innovative, creative, constantly striving to improve, open and transparent
Consistent level of service people have a right to expect, robust arrangements in place for when things do go wrong
May have elements of good practice but inconsistent, potential or actual risk, inconsistent responses when things go wrong
Severe harm has or is likely to occur, shortfalls in practice, ineffective or no action taken to put things right or improve
12
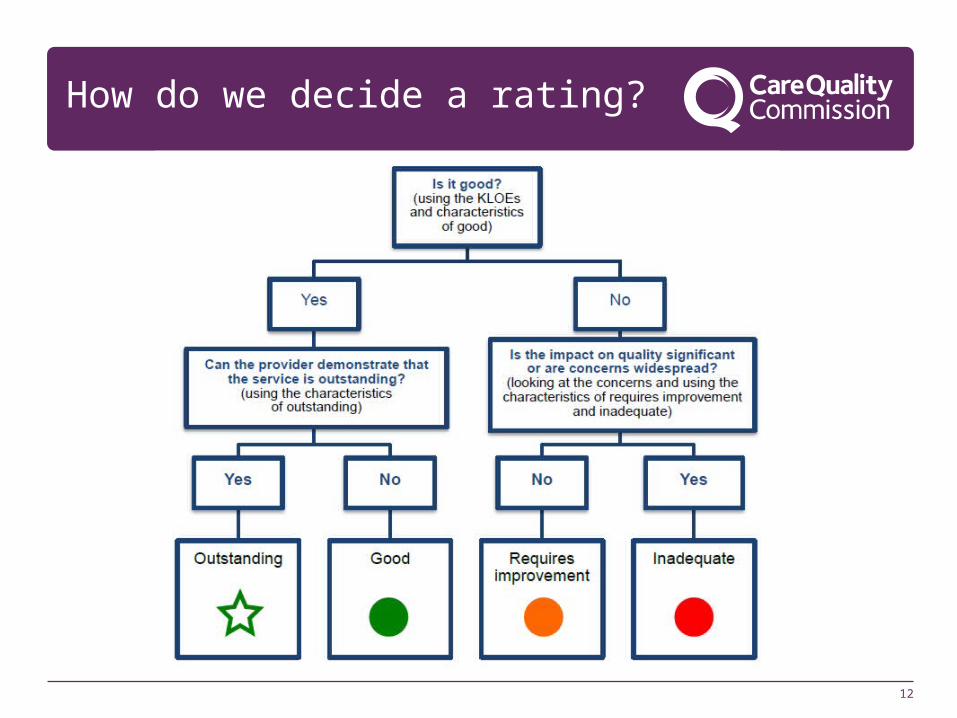
How do we decide a rating?
13
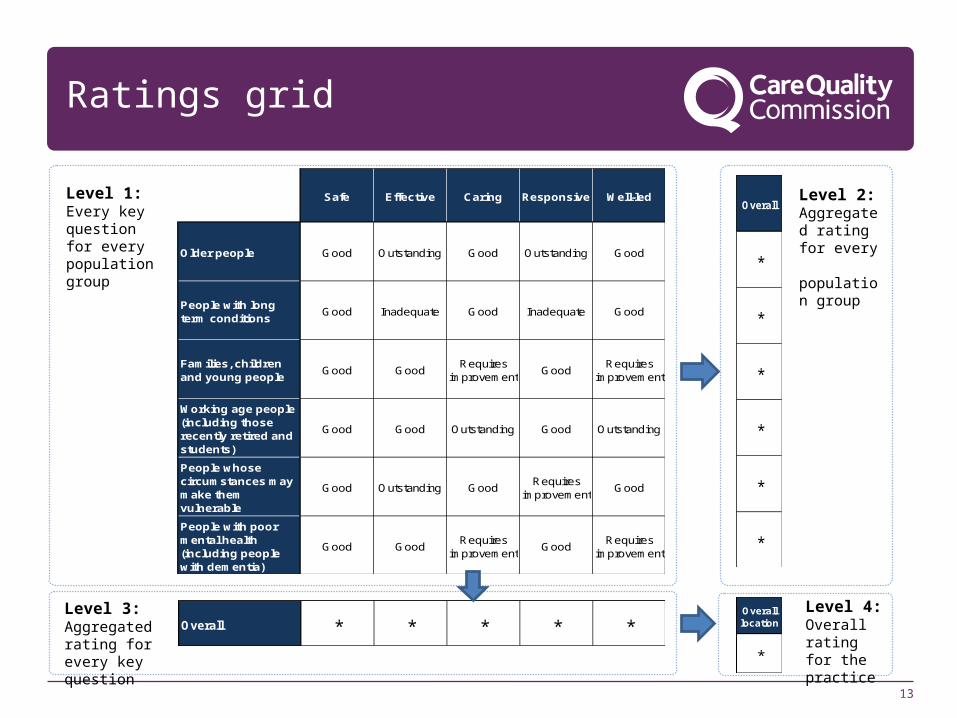
Ratings grid
Level 1: Every key question for every population group
Safe Effective Caring Responsive Well-led
Older people Good Outstanding Good Outstanding Good
People with long term conditions
Good Inadequate Good Inadequate Good
Families, children and young people
Good GoodRequires
improvementGood
Requires improvement
Working age people (including those recently retired and students)
Good Good Outstanding Good Outstanding
People whose circumstances may make them vulnerable
Good Outstanding GoodRequires
improvementGood
People with poor mental health (including people with dementia)
Good GoodRequires
improvementGood
Requires improvement
Overall
*
*
*
*
*
*
Level 2: Aggregated rating for every population group
Overall * * * * *Level 3: Aggregated rating for every key question
Level 4: Overall rating for the practice
Overall location
*
Population groups
Inspectors will judge how well services meet the needs of six different population groups:
•Older people
•People with long-term conditions
•Families, children and young people
•Working-age people, including those recently retired and students
•People whose circumstances may make them vulnerable
•People experiencing poor mental health (including people with dementia).
14
What to expect from an inspection
• We will send you a letter two weeks before we inspect (unless we are responding to concerns) and our inspector will call you.
• On the day, we will ask you to tell us (and give us evidence) about the good care you give, and we will want to talk to staff and patients to find out more.
• At the end of the inspection, we will tell you our initial thoughts.
• We will write up our report and send it to you to check for factual accuracy before we publish it on our website.
15
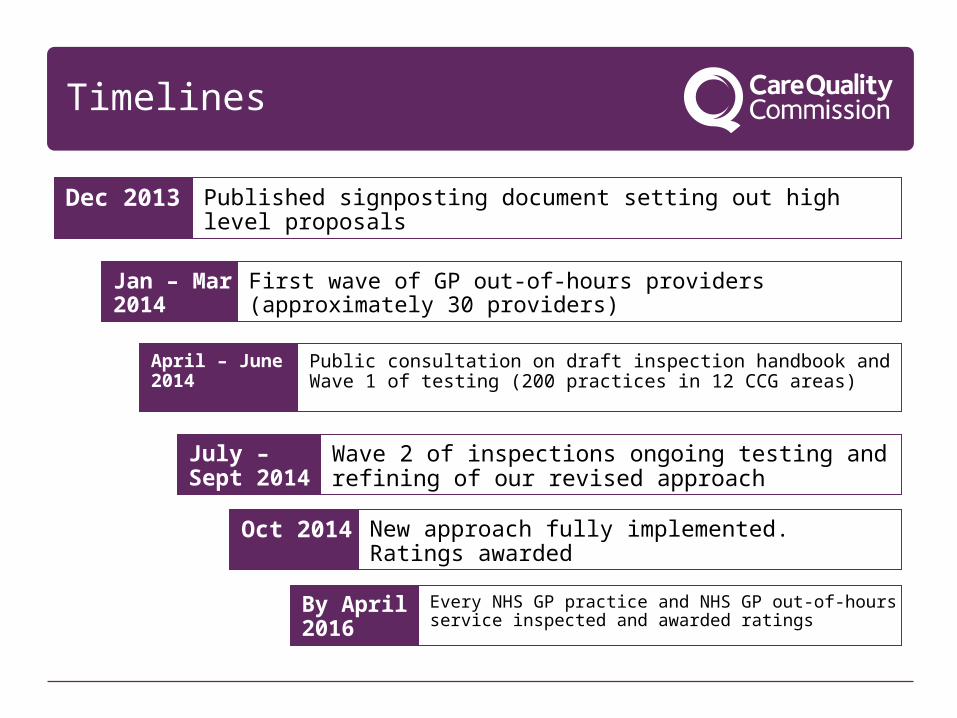
Timelines
Published signposting document setting out high level proposalsDec 2013
First wave of GP out-of-hours providers (approximately 30 providers)
Jan – Mar 2014
Public consultation on draft inspection handbook and Wave 1 of testing (200 practices in 12 CCG areas)
April – June 2014
Wave 2 of inspections ongoing testing and refining of our revised approach
July – Sept 2014
Oct 2014 New approach fully implemented. Ratings awarded
By April 2016
Every NHS GP practice and NHS GP out-of-hours service inspected and awarded ratings

17
Find out more
• Website:www.cqc.org.uk
• Twitter:@CQCforGPs
• Join our provider onlinecommunity: https://communities.cqc.org.uk/provider
18
Thank you
Top Related