







Languages
Pages
Legal

MOLECULAR BASISof CANCER
NON-lethal genetic damage A tumor is formed by the clonal
expansion of a single precursor cell (monoclonal)
Four classes of normal regulatory genes PROTO-oncogenes Oncogenes Oncoproteins DNA repair genes Apoptosis genes
Carcinogenesis is a multistep process
CARCINOGENESIS
Carcinogenesis is a multistep process at both the phenotypic and the genetic levels.
It starts with a genetic damage: Environmental
Chemical Radiation Viral
Inhereted

Carcinogenesis
Genetic damage lead to “ mutation” single cell which has the genetic damage
undergoes neoplastic prliferation ( clonal expansion) forming the tumor mass

TRANSFORMATION &PROGRESSION
Self-sufficiency in growth signals Insensitivity to growth-inhibiting
signals Evasion of apoptosis Defects in DNA repair: “Spell checker” Limitless replicative potential:
Telomerase Angiogenesis Invasive ability Metastatic ability
Carcinogenesis
Remember the cell cycle !! Binding of a growth factor to its receptor on
the cell membrane Activation of the growth factor receptor
leading to activation of signal-transducing proteins
Transmission of the signal to the nucleus Induction of the DNA transcription Entry in the cell cycle and cell division
6
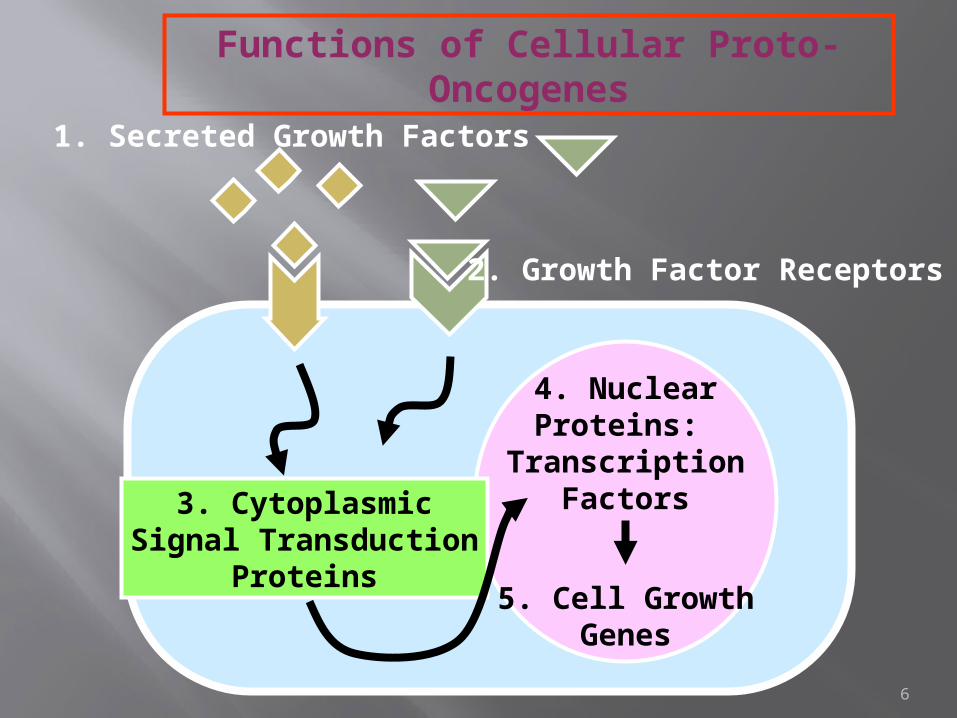
4. NuclearProteins:
TranscriptionFactors
5. Cell GrowthGenes
3. CytoplasmicSignal Transduction
Proteins
1. Secreted Growth Factors
2. Growth Factor Receptors
Functions of Cellular Proto-Oncogenes
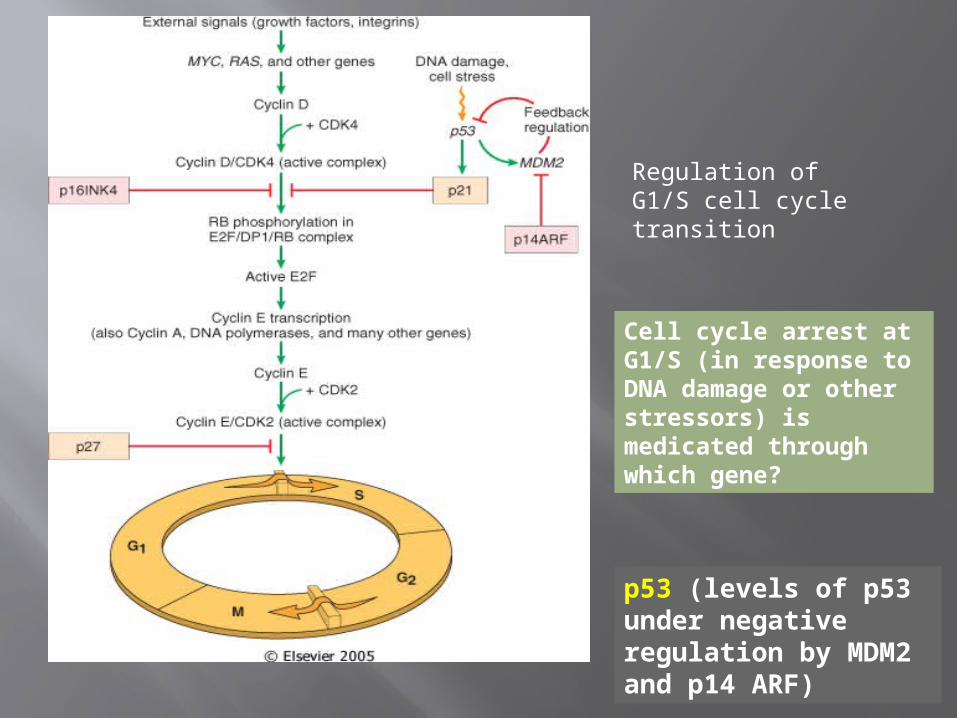
Regulation of G1/S cell cycle transition
Cell cycle arrest at G1/S (in response to DNA damage or other stressors) is medicated through which gene?
p53 (levels of p53 under negative regulation by MDM2 and p14 ARF)
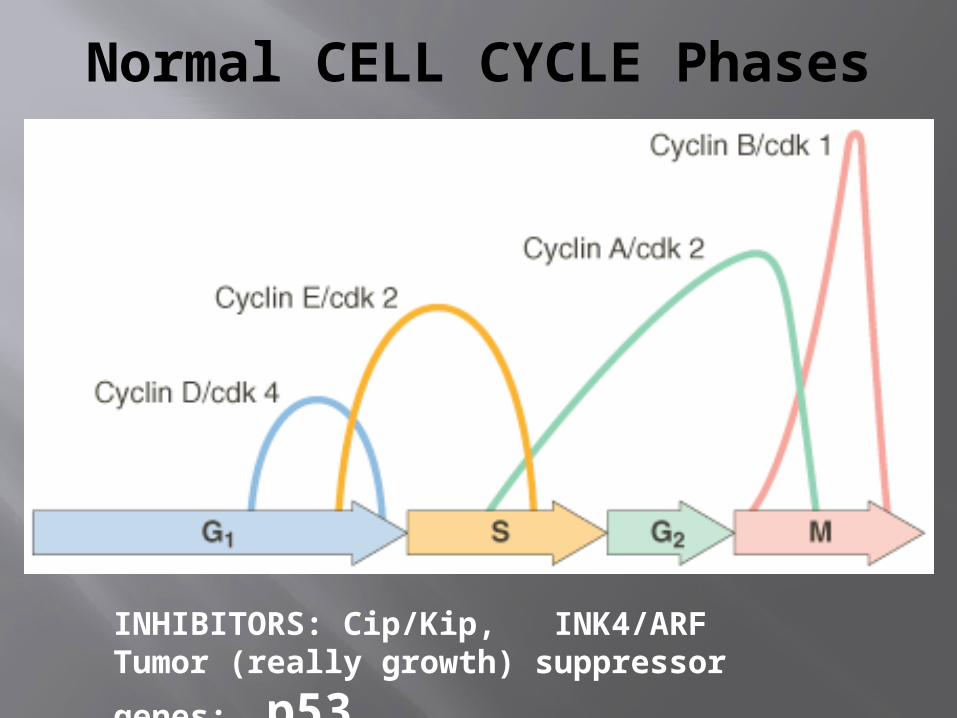
Normal CELL CYCLE Phases
INHIBITORS: Cip/Kip, INK4/ARFTumor (really growth) suppressor
genes: p53
cyclins and cyclin-dependent kinases
-cyclins are only expressed at specific stages of the cell cycle
-cyclin-dependent kinases are expressed constitutively, but must bind cyclins for
activation; phosphorylation of target proteins essential for progression through
cell cycle

Carcinogenesis
5- Cyclins and cyclins- dependent kinases (CDKs) Progression of cells through cell cycles is
regulated by CDKs after they are activated by binding with cyclins
Mutations that dysregulate cyclins and CDKs will lead to cell proliferation …e.g. Cyclin D genes are overexpressed in breast,
esophagus and liver cancers. CDK4 is amplified in melanoma and sarcomas

Carcinogenesis
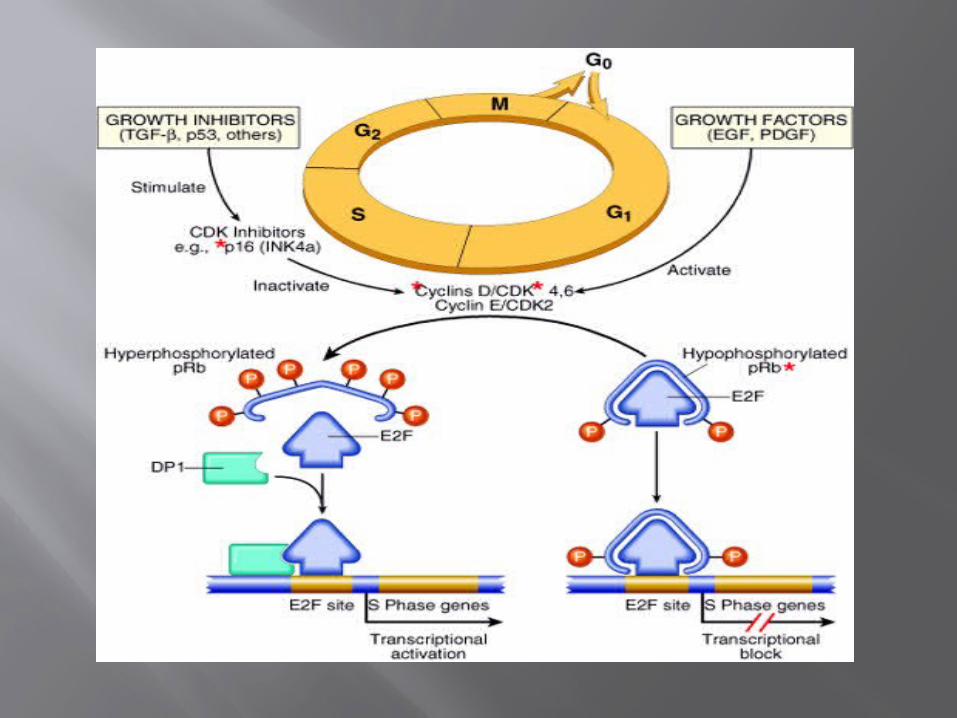
RB gene exists in “ active “ and “ inactive” forms
If active will stop the advancing from G1 to S phase in cell cycle
If cell is stimulated by growth factors inactivation of RB gene brake is released cells start cell cycle …G1 SM …then RB gene is activated again

13Hanahan and Weinberg, Cell 100: 57, 2000
Apoptosis
Oncogenes
Tumor Suppressor
Inv. and MetsAngiogenesis
Cell cycle

Four classes of normal regulatory genes PROTO-oncogenes Oncogenes Oncoproteins DNA repair genes Apoptosis genes
Carcinogenesis is a multistep process
15
ONCOGENES
Oncogenes are mutated forms of cellular proto-oncogenes.
Proto-oncogenes code for cellular proteins which regulate normal cell growth and differentiation.
ONCOGENES Are MUTATIONS of NORMAL
genes (PROTO-oncogenes)Growth FactorsGrowth Factor ReceptorsSignal Transduction Proteins
(RAS)Nuclear Regulatory ProteinsCell Cycle Regulators
Oncogenes code for Oncoproteins
Mutations that confer these properties fall into two categories
Oncogene : a cancer-causing gene that has been
mutated to cause an increase in activity, or the activity becomes constitutive,
or a new activity is acquired. -a mutation in a single allele is sufficient to
transform cells (dominant). -originally identified as viral proteins that
resembled normal human proteins. -the term "proto-oncogene" refers to the
normal protein that has not been mutated

tumor Suppressor gene Mutation of tumor
suppressor gene cause a loss offunction.
-mutations are required in both alleles to transform cells (recessive)

19
Class I: Growth Factors
Class II: Receptors for Growth Factors and Hormones
Class III: Intracellular Signal Transducers
Class IV: Nuclear Transcription Factors
Class V: Cell-Cycle Control Proteins
Five types of proteins encoded by proto-oncogenes participate in
control of cell growth:


1
2
3
4
4 types of genetic mutations that contribute to cancer
Categories of oncogenes A. Growth factors -generally not directly involved
transformation, but increased expression seen as part of
an autocrine loop due to changes in other steps in the same pathway

growth factor receptors
-They are transmembrane proteins with an external ligand binding domain and an
internal tyrsosine kinase domain. -oncogenic mutations can result in
dimerization and activation in the absence of
ligand -more commonly, increased activity is a
result of overexpression of receptors

Growth factor receptors
They are transmembrane proteins with an external ligand binding domain and an
internal tyrsosine kinase domain. -Oncogenic mutations can result in
dimerization and activation in the absence of
ligand -More commonly, increased activity is a
result of overexpression of receptors.
signal transducers
-Activated directly or indirectly by growth factor receptors
-Activation of signal transducers triggers a phosporylation cascade that ultimately
results in changes in gene expression at the transcriptional level.
-mutations in RAS , a GTPase, are the most common oncogenic
abnormality in tumors -failure to hydrolyze GTP locks RAS in its
active form.

Transcription factors
-Transcription factors contain DNA binding domains.
Sequences Regulate expression of genes essential
for passage through the cell cycle, or regulation of apoptosis.
-

CategoryPROTO- Oncogene
Mode of Activation
Associated Human Tumor
GFsPDGF-β chain SIS Overexpression Astrocytoma
OsteosarcomaFibroblast growth factors
HST-1 Overexpression Stomach cancer
INT-2 Amplification Bladder cancer
Breast cancerMelanoma
TGFα TGFα Overexpression Astrocytomas
Hepatocellular carcinomas
HGF HGF Overexpression Thyroid cancer

CategoryPROTO- Oncogene
Mode of Activation
Associated Human Tumor
GF ReceptorsEGF-receptor family
ERB-B1 (ECFR)
Overexpression Squamous cell carcinomas of lung, gliomas
ERB-B2 Amplification Breast and ovarian cancers
CSF-1 receptor FMS Point mutation Leukemia
Receptor for neurotrophic factors
RET Point mutation Multiple endocrine neoplasia 2A and B, familial medullary thyroid carcinomas
PDGF receptor PDGF-R Overexpression Gliomas
Receptor for stem cell (steel) factor
KIT Point mutation Gastrointestinal stromal tumors and other soft tissue tumors
CategoryPROTO- Oncogene
Mode of Activation
Associated Human Tumor
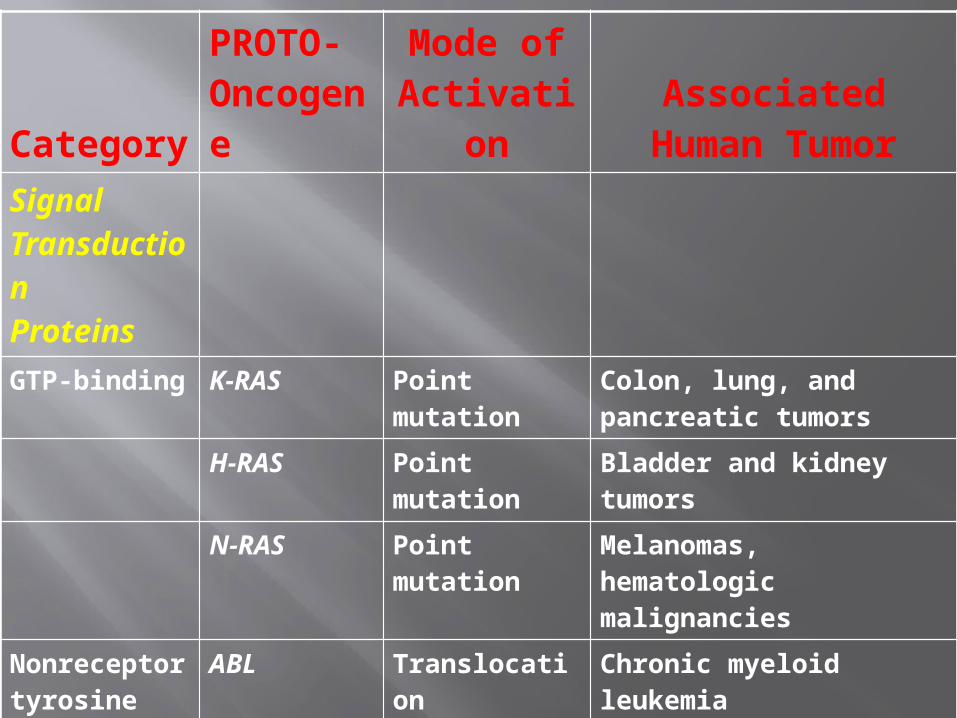
Signal TransductionProteins
GTP-binding K-RAS Point mutation Colon, lung, and pancreatic tumors
H-RAS Point mutation Bladder and kidney tumors
N-RAS Point mutation Melanomas, hematologic malignancies
Nonreceptor tyrosine kinase
ABL Translocation Chronic myeloid leukemia
Acute lymphoblastic leukemia
RAS signal transduction
BRAF Point mutation Melanomas
WNT signal transduction
β-catenin Point mutation Hepatoblastomas, hepatocellular carcinoma
CategoryPROTO- Oncogene
Mode of Activation Associated Human
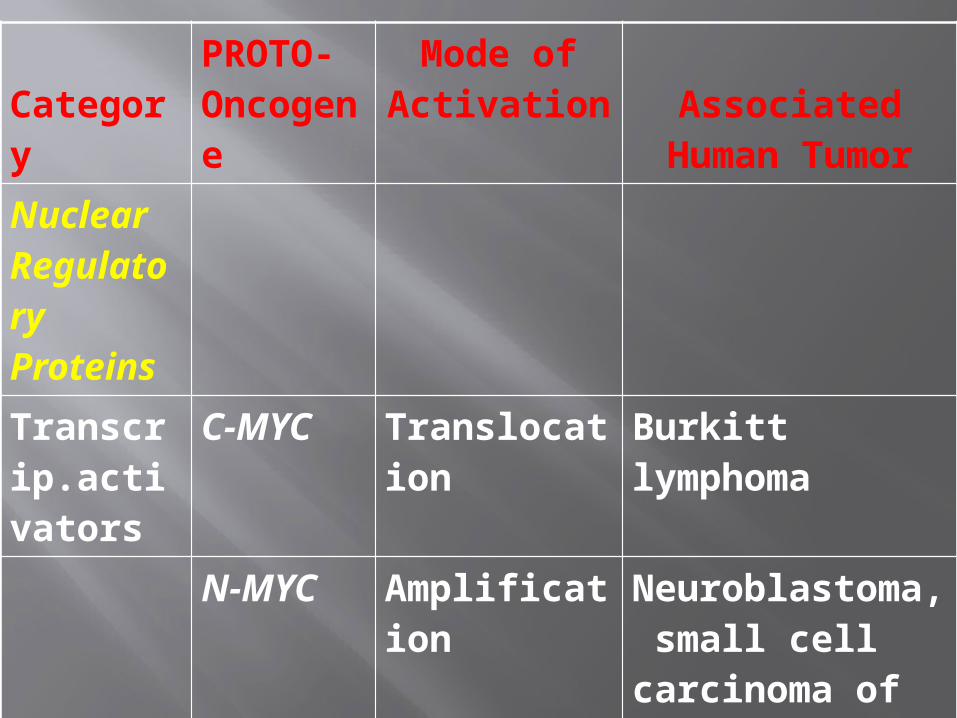
TumorNuclear Regulatory Proteins
Transcrip.activators
C-MYC Translocation Burkitt lymphoma
N-MYC Amplification Neuroblastoma, small cell carcinoma of lung
L-MYC Amplification Small cell carcinoma of lung

2) Activation Growth-Promoting OncogenesWhich signal transduction pathway is continuously activated by mutant RAS?
MAP kinase pathway
Point mutations of ras are seen in what % of all human malignancies?
15-20%
MYC It is a protooncogene Found on Chromosome 8 Member of Myc protein family
Includes N-myc and L-myc
C-MYC
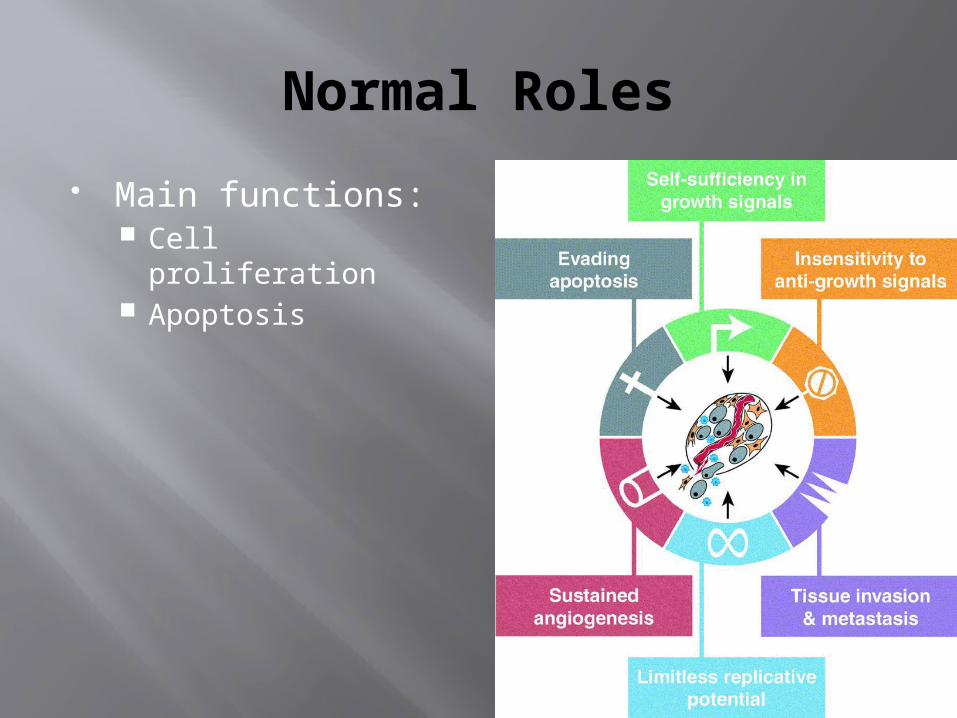
Normal Roles
Main functions: Cell proliferation Apoptosis
The MYC protein can either activate or repress the transcription of other genes.
Activated by MYC are growth-promoting genes, including cyclin
dependent kinas (CDKs), Genes repressed by MYC THE CDK inhibitors (CDKIs)
Dysregulation of MYC promotes TUMORIGENESIS by increasing expression of genes that promote proliferation in turn inactivates the inhibitors.

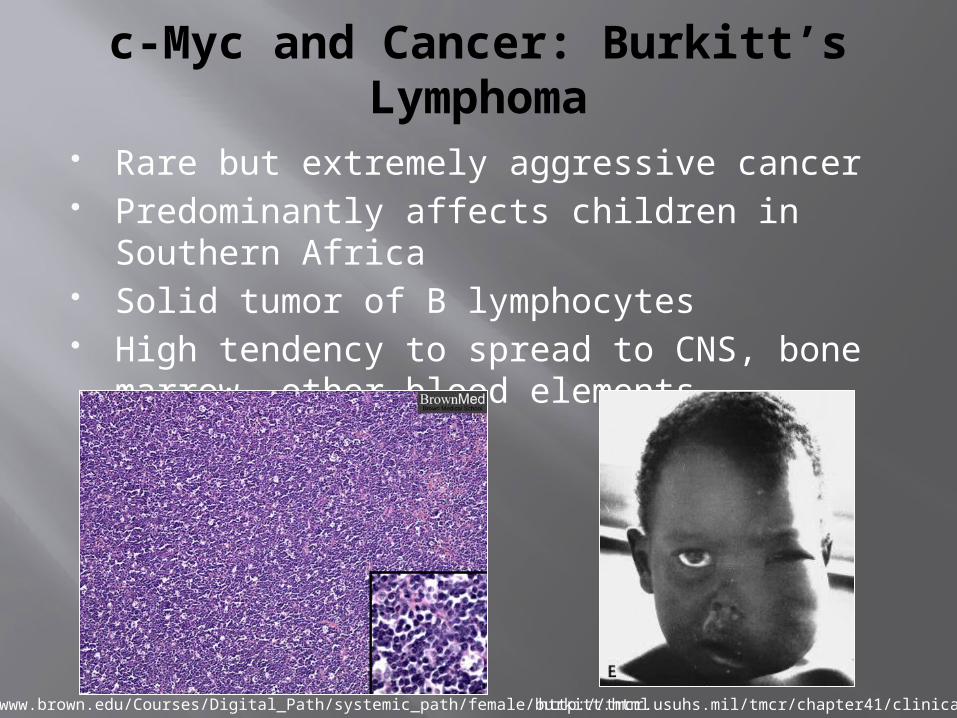
c-Myc and Cancer: Burkitt’s Lymphoma
c-Myc was first discovered in lymphoma patients
Reciprocal translocation from chromosome 8 to chromosome 14
http://www.ncbi.nlm.nih.gov/books/bv.fcgi?call=bv.View..ShowSection&rid=gnd.section.92
http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/B/BurkittLymphoma.html
c-Myc and Cancer: Burkitt’s Lymphoma
Rare but extremely aggressive cancer Predominantly affects children in Southern
Africa Solid tumor of B lymphocytes High tendency to spread to CNS, bone
marrow, other blood elements
http://www.brown.edu/Courses/Digital_Path/systemic_path/female/burkitt.htmlhttp://tmcr.usuhs.mil/tmcr/chapter41/clinical.htm

c-Myc and Cancer
Over-expressed in 70% of all human cancers
Translocated in 90% of all Burkitt’s lymphoma cases 90% of gynecological cancers 80% of breast cancers 70% of colon cancers
Contributes to more than 70,000 cancer deaths annually in the U.S.
REMEMBER
Translocation in Burkitt lymphoma, a B cell tumor. (t9:22)
Amplified in breast, colon, lung, and many other cancers;
Amplified in N-MYC NEUROBLASTOMAS L-MYC small cell cancers of
lung.

Tumor supressor gene
. Tumor suppressor were originally identified as inherited mutations that confer a
predisposition to cancer (familial form).
Inactivation of tumor suppressors can occur Sporadically -sequential inactivation of both alleles in somatic
cells You may hear the term haploinsufficiency , which refers to inactivation of a single allele contributing to malignancy. -usually not the initiating event, but exacerbating. Viral inactivation -HPV expresses proteins that inhibit Rb and p53
function.

Tumor Suppressor genes
RB gene P53 gene APC/Beta Catenin INK4/ARF locus TGF beta pathway NF-1 NF-2 VHL WT-1Caderins

RB gene
It is a tumor suppressor gene It is located on chromosome 13 It regulates G1 /S transition
phase. It occurs in active
hypophosphorylated and inactive hyperphosphorylaed state

RB gene
A Loss of RB function confers a predisposition to retinoblastoma.
occurs in both the familial form (early onset)
and sporadic form.

Retinoblastoma
Red reflex Leukocoria
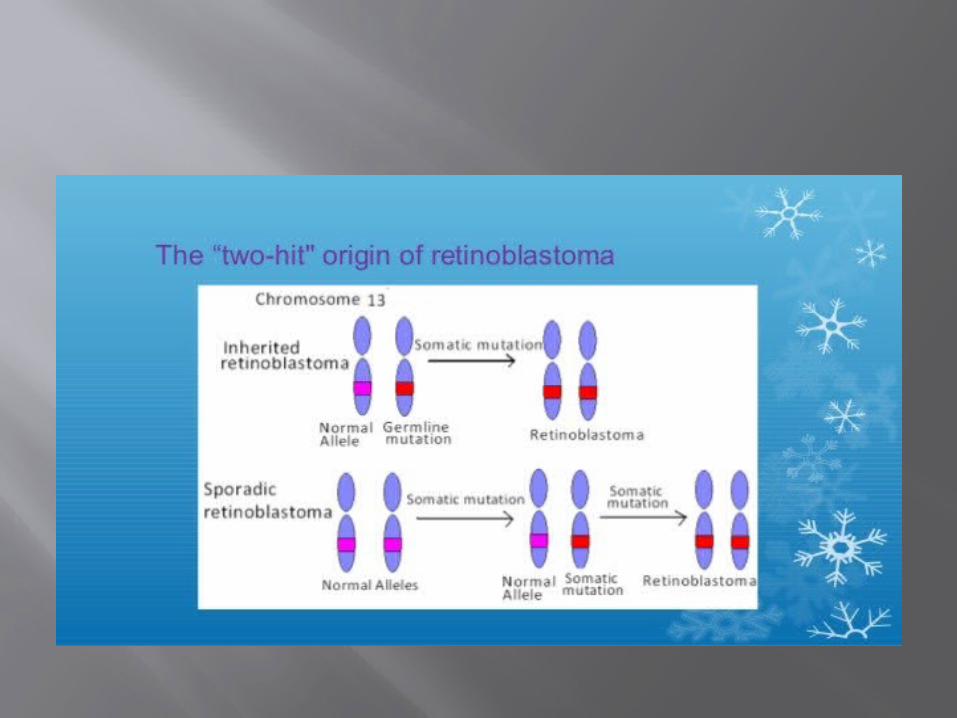
Knudson, in 1974, proposed two-hit hypothesis, which in molecular terms can be stated as follows:
1. Two mutations (hits) are required to produce retinoblastoma. Both of the normal
alleles of the RB locus must be inactivated (hence the two hits) for the development of retinoblastoma.
2.In familial cases, children inherit one defective copy of the RB gene in the germ line; the other copy is normal. Retinoblastoma develops when the normal RB gene is
lost in retinoblasts as a result of somatic mutation.
3.In sporadic cases, both normal RB alleles are lost by somatic mutation in one of the retinoblasts.
The end result is the same: a retinal cell that has lost both of the
normal copies of the RB gene becomes cancerous.

Why Retinoblastoma is autosomal dominant?
Retinoblastoma families only a single somatic mutation is required for expression of the disease,.
Loss of heterozygosity(LOH)
In hereditary retinoblastoma, an affected child inherits one defective Rb allele together with one normal gene. This is heterozygous state.
It is not associated with changes in the retina because 50% of the Rb gene product is sufficient to prevent
the development of retinoblastoma. If the remaining normal Rb allele is inactivated by
deletion or mutation, the loss of its suppressor function leads to the appearance of a neoplasm.
This genetic process is referred to as loss of heterozygosity.

The importance of Rb lies in its regulation of
the G1/S checkpoint

loss of normal cell cycle control leads to malignant transformation
the four key regulators of the cell cycle (CDKN2A, cyclin D,CDK4, Rb) is mutated in most human cancers.

Functional deletion of RB
Human papillomavirus(HPV) produce E7 protein and the protein E7 binds to the hypophosphorylated form of Rb in place of E2F leading to uncontrolled growth.
SPORADIC (Non-hereditary)
Unilateral, unifocal. 60% of all cases. Present later. Children of the
affected are normal. Chromosomal
anomaly is a somatic mutation. Relatives have a low
risk of RB development
FAMILIAL (Hereditary)
85% bilateral, multifocal. 40% % of all cases. Present earlier. Children of the affected
have 45% chance of inheritance.
Chromosomal anomaly is a Germline mutation.
Autosomal dominant with high penetrance.
The median age at presentation is 2 years, although the tumor may be present at birth.
Clinical features poor vision,
strabismus, A whitish hue to
the pupil ("cat's eye reflex"),
pain and tenderness in the eye.
P53
The TP53 gene which encodes p53 resides on the short arm of chromosome 17.

In healthy unstressed cells,
p53 is short half life (20 min)
It undergo destruction by MDM2.
IT HAS DIFFERENT NAMES “GUARDIAN OF THE
GENOME.” GATE KEEPER.
MOLECULAR POLICE MAN.
When cell is stressed, When ever there is a DNA Damage ATM (ataxia telangiectasia mutated) are
activated. These activated complexes release P53
from MDM2 and increase its half-life and
enhance its ability to drive the transcription of target genes. Hundreds of genes whose transcription is triggered by p53 have been found.
Functions of P53
1.Temporary cell cycle arrest. 2.permanent cell cycle arrest 3.Triggering of programmed
cell death (termed apoptosis). 4.p53 plays a central role in
maintaining the integrity of the genome.

P53 is activated by the following
.DNA damage by irradiation, chemicals,
uv light and Free radicle injury and senescence.
Inactivation of P53
Point mutationsMDM2 –degrade P53E6 protein-From HPV
p53-mediated cell cycle arrest in response to DNA damage in
The late G1 phase and is caused mainly by p53-dependent
transcription of the CDKI gene CDKN1A (p21)belongs to KIP/CIP group of CDKI.

P53 induces expression of DNA damage repair genes to reapir the damaged DNA.
p53-induced apoptosis of cells with irreversible DNA damage is the ultimate protective mechanism against neoplastic transformation by pro-apoptotic genes such as BAX.
70% of human cancers have a defect in P53 gene, Most commonly in Breast , colon and lung
cancer

Li-Fraumeni syndrome.
Less commonly, some patients inherit a mutant TP53 allele The disease is called the
Li-Fraumeni syndrome.

patients with Li-Fraumeni syndrome develop tumors at a younger age and may develop multiple primary tumors.
25-fold greater chance of developing a malignant tumor by age 50 in a person with mutant single allele.
sarcomas, breast cancer, leukemia, brain tumors, and
carcinomas of the adrenal cortex. patients with Li-Fraumeni syndrome develop tumors at a younger
age and may develop multiple primary tumors.
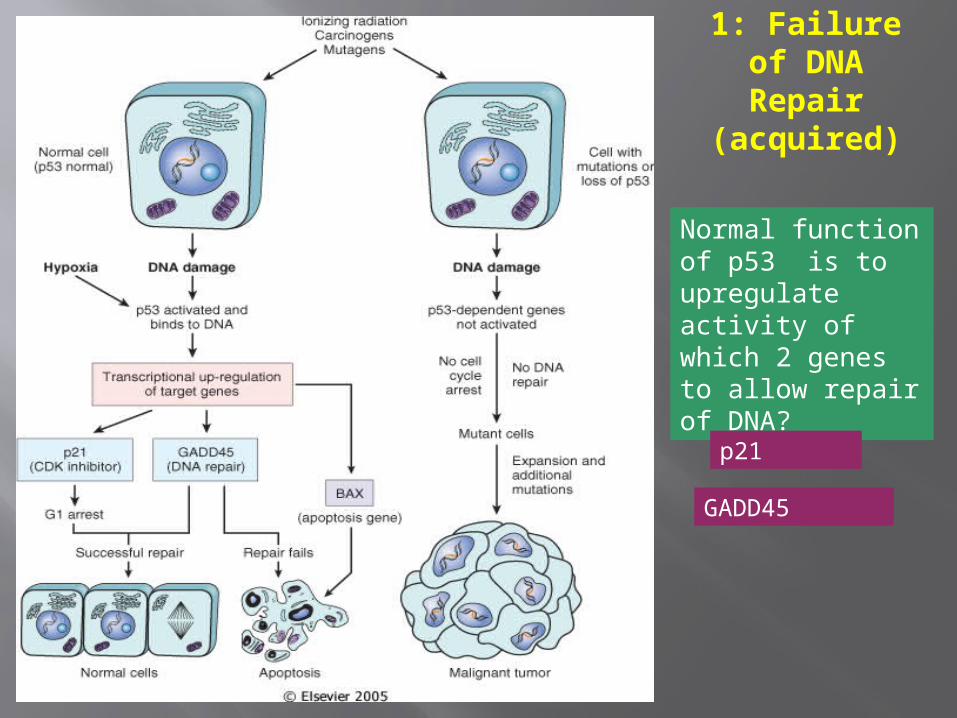
1: Failure of DNA Repair (acquired)
Normal function of p53 is to upregulate activity of which 2 genes to allow repair of DNA?
p21
GADD45

Summary
p53 inhibits G1 progression only in response to DNA damage
-normally p53 is very unstable, due to proteolytic degradation triggered by mdm2
.p53 is phosphorylated in response to DNA damage; mdm2 no longer binds p53
-p53 upregulates expression of p21, which in turn inhibits G1/S CDKs.
c. In response to excessive DNA damage, p53 can trigger apoptosis
Tumor (really “GROWTH”) suppressor genes
TGF-β COLON E-cadherin STOMACH NF-1,2 NEURAL TUMORS APC/β-cadherin GI, MELANOMA SMADs GI RB RETINOBLASTOMA P53 EVERYTHING!! WT-1 WILMS TUMOR p16 (INK4a) GI, BREAST BRCA-1,2 BREAST KLF6 PROSTATE
Evasion of APOPTOSIS
BCL-2 p53 MYC
DNA REPAIR GENE DEFECTS
DNA repair is like a spell checker HNPCC (Hereditary Non-Polyposis
Colon Cancer [Lynch]): TGF-β, β-catenin, BAX
Xeroderma Pigmentosum: UV fixing gene
Ataxia Telangiectasia: ATM gene Bloom Syndrome: defective helicase Fanconi anemia

LIMITLESS REPLICATIVE POTENTIAL
TELOMERES determine the limited number of duplications a cell will have, like a cat with nine lives.
TELOMERASE, present in >90% of human cancers, changes telomeres so they will have UNLIMITED replicative potential
TUMOR ANGIOGENESIS Q: How close to a blood vessel must a cell
be? A: 1-2 mm
Activation of VEGF and FGF-b
Tumor size is regulated (allowed) by angiogenesis/anti-angiogenesis balance

TRANSFORMATION
GROWTHBM INVASION
ANGIOGENESISINTRAVASATIONEMBOLIZATION
ADHESIONEXTRAVASATIONMETASTATIC GROWTH
etc.

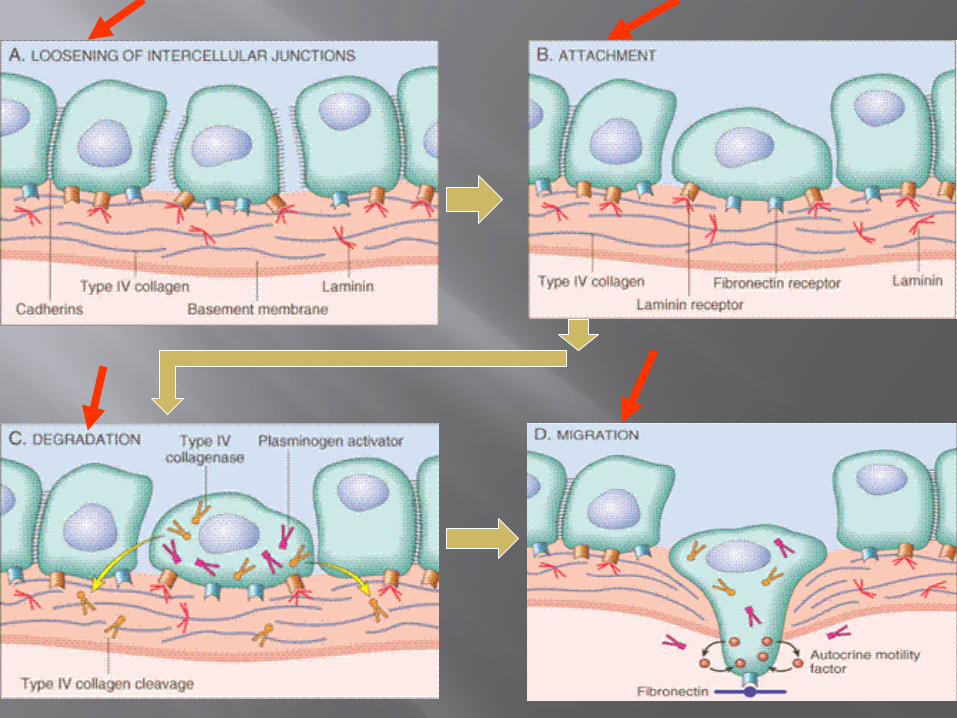
Invasion Factors
Detachment ("loosening up") of the tumor cells from each other
Attachment to matrix components
Degradation of ECM, e.g., collagenase, etc.
Migration of tumor cells
METASTATIC SUPPRESSOR GENES?
NM23 KAI-1 KiSS

CHROMOSOME CHANGESin CANCER
TRANSLOCATIONS and INVERSIONS
Occur in MOST Lymphomas/Leukemias
Occur in MANY (and growing numbers) of NON-hematologic malignancies also

Malignancy Translocation Affected Genes
Chronic myeloid leukemia (9;22)(q34;q11) Ab1 9q34
bcr 22q11
Acute leukemias (AML and ALL) (4;11)(q21;q23) AF4 4q21
MLL 11q23
(6;11)(q27;q23) AF6 6q27
MLL 11q23
Burkitt lymphoma (8;14)(q24;q32) c-myc 8q24
IgH 14q32
Mantle cell lymphoma (11;14)(q13;q32) Cyclin D 11q13
IgH 14q32
Follicular lymphoma (14;18)(q32;q21) IgH 14q32
bcl-2 18q21
T-cell acute lymphoblastic leukemia (8;14)(q24;q11) c-myc 8q24
TCR-α 14q11
(10;14)(q24;q11) Hox 11 10q24
TCR-α 14q11
Ewing sarcoma (11;22)(q24;q12) Fl-1 11q24
EWS 22q12
Carcinogenesis is “MULTISTEP” NO single oncogene causes cancer
BOTH several oncogenes AND
several tumor suppressor genes must be involved
Gatekeeper/Caretaker conceptGatekeepers: ONCOGENES and
TUMOR SUPPRESSOR GENES
Caretakers: DNA REPAIR GENES Tumor “PROGRESSION”
ANGIOGENESIS HETEROGENEITY from original single cell

Carcinogenesis:
Initiation/Promotion concept: BOTH initiators AND promotors are needed NEITHER can cause cancer by itself
INITIATORS (carcinogens) cause MUTATIONS
PROMOTORS are NOT carcinogenic by themselves, and MUST take effect AFTER initiation, NOT before
PROMOTORS enhance the proliferation of initiated cells


Q: WHO are the usual suspects?
Inflammation?
Teratogenesis?
Immune Suppression?
Neoplasia? Mutations?

A: The SAME 3 that are
ALWAYS blamed! 1) Chemicals 2) Radiation 3) Infectious Pathogens

CHEMICAL CARCINOGENS:INITIATORS
DIRECT β-Propiolactone Dimeth. sulfate Diepoxybutane Anticancer drugs
(cyclophosphamide, chlorambucil, nitrosoureas, and others)
Acylating Agents 1-Acetyl-imidazole Dimethylcarbamyl
chloride
“PRO”CARCINOGENS
Polycyclic and Heterocyclic Aromatic Hydrocarbons
Aromatic Amines, Amides, Azo Dyes
Natural Plant and Microbial Products Aflatoxin B1 Hepatomas Griseofulvin Antifungal Cycasin from cycads Safrole from sassafras Betel nuts Oral SCC
CHEMICAL CARCINOGENS:INITIATORS
OTHERS Nitrosamine and amides (tar,
nitrites) Vinyl chloride angiosarcoma in
Kentucky Nickel Chromium Insecticides Fungicides PolyChlorinated Biphenyls (PCBs)
CHEMICAL CARCINOGENS:PROMOTORS
HORMONES PHORBOL ESTERS (TPA), activate
kinase C PHENOLS DRUGS, many
“Initiated” cells respond and proliferate FASTER to promotors than normal cells
RADIATION CARCINOGENS
UV: BCC, SCC, MM (i.e., all 3)
IONIZING: photons and particulate Hematopoetic and Thyroid (90%/15yrs)
tumors in fallout victims Solid tumors either less susceptible or
require a longer latency period than LEUK/LYMPH
BCCs in Therapeutic Radiation
VIRAL CARCINOGENESIS
HPV SCC EBV Burkitt Lymphoma HBV HepatoCellular Carcinoma
(Hepatoma) HTLV1 T-Cell Malignancies KSHV Kaposi Sarcoma
H. pylori CARCINOGENESIS
100% of gastric lymphomas (i.e., M.A.L.T.-omas)
Gastric CARCINOMAS also!
HOST DEFENSES
IMMUNE SURVEILLENCE
CONCEPT
CD8+ T-Cells NK cells MACROPHAGES ANTIBODIES

How do tumor cellsescape immune surveillance?
Mutation, like microbes
↓ MHC molecules on tumor cell surface Lack of CO-stimulation molecules, e.g.,
(CD28, ICOS), not just Ag-Ab recognition
Immunosuppressive agents Antigen masking Apoptosis of cytotoxic T-Cells (CD8),
i.e., the damn tumor cell KILLS the T-cell!
Effects of TUMOR on the HOST
Location anatomic ENCROACHMENT HORMONE production Bleeding, Infection ACUTE symptoms, e.g., rupture,
infarction METASTASES
CACHEXIA Reduced diet: Fat
loss>Muscle loss Cachexia: Fat loss AND
Muscle loss TNF (α by default) IL-(6) PIF (Proteolysis Inducing
Factor)
Cancer Cachexia
Progressive weakness, loss of appetite, anemia and profound weight loss (>20%)
Often correlates with tumor mass & spread
Etiology includes a generalized increase in metabolism and central effects of tumor on hypothalamus
Probably related to macrophage production of TNF-a
Paraneoplastic Syndromes
Due to Products released by tumor Cushing’s Syndrome
Adrenal, Lung Ca – ACTH Inappropriate ADH syndrome
(Hyponatremia) – lung ca Hypothalamic tumors (vasopressin) Hypercalcemia – Ca is the common cause.
– lung. Hypoglycemia - insulin or insulin like
activities Fibrosarcoma, Cerebellar hemangioma.

PARA-Neoplastic Syndromes Endocrine (next)
Nerve/Muscle, e.g., myasthenia w. lung ca.
Skin: e.g., acanthosis nigricans, dermatomyositis
Bone/Joint/Soft tissue: HPOA (Hypertrophic Pulmonary OsteoArthropathy)
Vascular: Trousseau, Endocarditis Hematologic: Anemias Renal: e.g., Nephrotic Syndrome
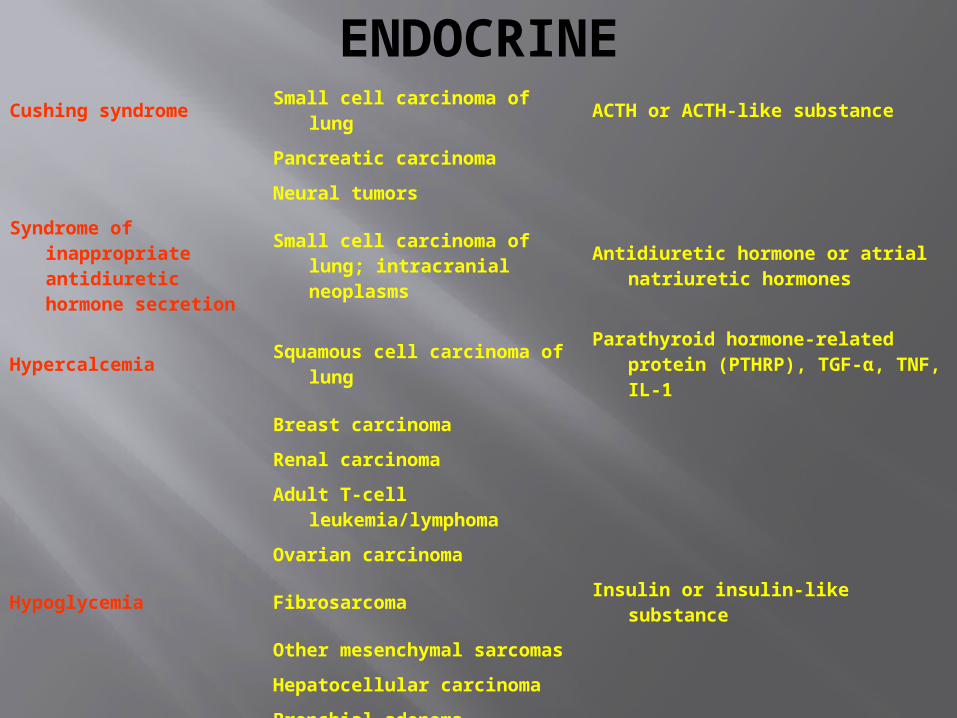
ENDOCRINECushing syndrome Small cell carcinoma of lung ACTH or ACTH-like substance
Pancreatic carcinoma
Neural tumors
Syndrome of inappropriate antidiuretic hormone secretion
Small cell carcinoma of lung; intracranial neoplasms
Antidiuretic hormone or atrial natriuretic hormones
Hypercalcemia Squamous cell carcinoma of lungParathyroid hormone-related protein
(PTHRP), TGF-α, TNF, IL-1
Breast carcinoma
Renal carcinoma
Adult T-cell leukemia/lymphoma
Ovarian carcinoma
Hypoglycemia Fibrosarcoma Insulin or insulin-like substance
Other mesenchymal sarcomas
Hepatocellular carcinoma
Carcinoid syndrome Bronchial adenoma (carcinoid) Serotonin, bradykinin
Pancreatic carcinoma
Gastric carcinoma
Polycythemia Renal carcinoma Erythropoietin
Cerebellar hemangioma
Hepatocellular carcinoma
GRADING/STAGING
GRADING: HOW “DIFFERENTIATED” ARE THE CELLS?
STAGING: HOW MUCH ANATOMIC EXTENSION? TNM
Which one of the above do you think is more important?

Grading & Staging of Tumor
Grading – Cellular Differentiation (Microscopic)
Staging – Progression or Spread (clinical)
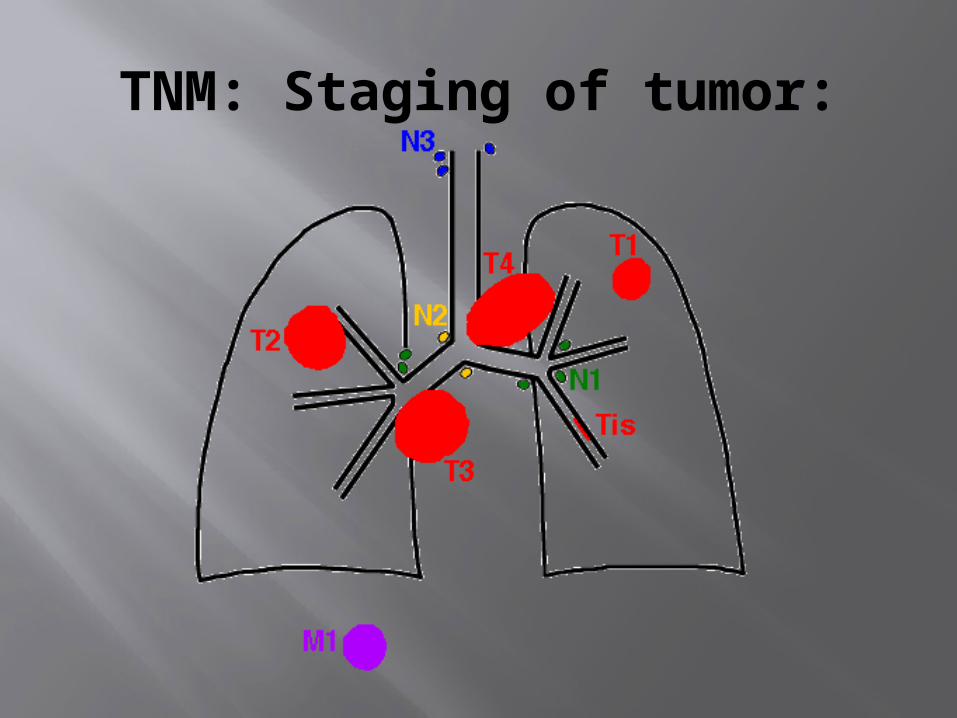
TNM: Staging of tumor:

WELL?(pearls)
MODERATE?(intercellular bridges)
POOR?(WTF!?!)
GRADING for Squamous Cell Carcinoma

ADENOCARCINOMA GRADINGLet’s have some FUN!

LAB DIAGNOSIS BIOPSY CYTOLOGY: (exfoliative) CYTOLOGY: (FNA, Fine
Needle Aspirate)
IMMUNOHISTOCHEMISTRY
Categorization of undifferentiated tumors
Leukemias/Lymphomas Site of origin Receptors, e.g., ERA,
PRA

TUMOR MARKERS.











Prostatic Carcinoma-Bone Lung Carcinoma-Adrenals &
Brain Neuroblastoma-Liver & Bone Less common sites
of metastases include skin, muscle thyroid,
breast….etc.

CA LUNG-Smoking CA CERVIX-Sexual transmission of HPV CA BLADDER -Rubber Industry CA LIVER --Aflatoxin & HBV infection CA THYROID-Radiation ANGIOSARCOMA of Liver-Plastic(PVC) MESOTHELIOMA -Asbestos
Effects of tumor on body
Location of tumor is of importance 1- Mass effect by pressing on vital areas e.g. airway, intestine , BV, brain, nerve obstruction, infarction , paralysis…etc 2- Local destruction of epithelial surface
or BV ulceration , bleeding , infection3-
Hormonal activity

CANCER CACHEXIA
Wasting syndrome characterized by anorexia , loss of body fat & weight, with marked weakness, anemia & fever.
Reduced food intake but high metabolic rate
Possibly due to release of cytokines by tumor cells & macrophages
Para neoplastic syndrome
Systemic symptoms that can't be explained by effects of local or distant spread of tumor
or hormones appropriate to tumor tissue. Due to ectopic production of hormones or
other factors They may precede the tumor or mimic
metastases They occur in about10%-15%of malignant
tumors.
DIAGNOSIS
History & clinical examination Radiographic techniques 1- X ray 2CT scan 3- MRI 4-Ultrasound 5-Laboratory tests : general & specialized
This is very important as many cancers a recurable if they are diagnosed early.
Specific symptoms should be followed upe.g. Abnormal bleeding Change of voice Change in a nevus Abnormal lump in breast
An ulcer that does not heal……etc.
Self examination of the breast- Mammography- Serial PAP smears for the cervix- Serial sputum cytology in smokers- Serial urine cytology in some cases, e.g. workers in rubber
Screening for genetic mutations in familial cancers.
Cytological methods :
Study of cells :- Smear- FNA, Brush, Fluid tapping…etc Papanicolaou stain (PAP)often used. False(+), False (-)- A negative report
does not exclude malignancy, repeat- Advise biopsy, even if (+ )
1-Morphological Methods :
Biopsy of tissue: Needle & core biopsy , Endoscopic Biopsy, or open surgical biopsy
Frozen Section (Rapid technique) Paraffin Section ( 36-48 hrs. or longer ) H&E, Special histochemical stains stains)
or by IMMUNOHISTOCHEMICALMethods

Tumor markers represent biochemical indicators of the presence of a tumor.
Their uses are to I - Confirm diagnosis. II -Determine the response to treatment . III - Detect early relapse. Present in serum or urine. Many are present in normal & tumor
tissue, so they are not very specific but their level is important.
Types of tumor marker
Hormones Human Chorionic Gonadotrophic
Hormone( HCG)Elevated levels are seen in
Pregnancy& Gestational Trophoblastic Disease
Calcitonin useful in diagnosis of some thyroid carcinomas
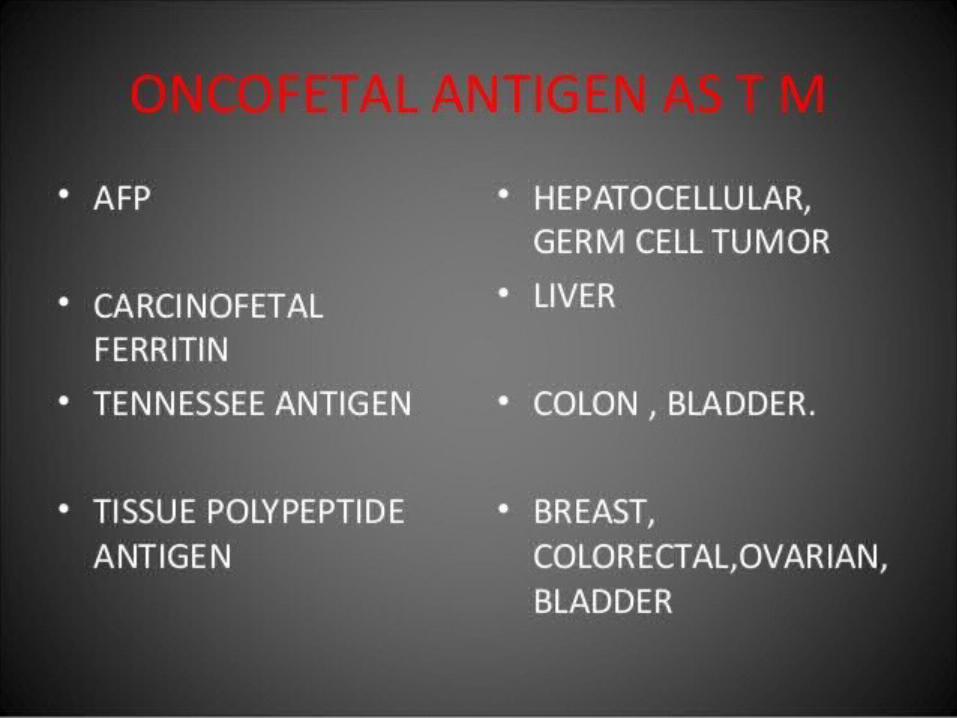
Oncofetal antigens
Carcinoembryonic Antigen ( CEA ) : in fetal tissue & some malignancies
Colorectal CA & Pancreatic CA Alpha Fetoprotein (AFP):Cirrhosis :
Elevated Hepatocellular carcinoma : Extremely high
ISOENZYMES
Prostatic Acid Phosphatase ( PAP ) levels seen in Metastatic prostatic
CA Useful in : Staging prostatic CA Assessment of prognosis Response to th
erapy.

Several mucins
MUC-1 in breast CA CA-125 in ovarian CA CA-19-9 in pancreatic &
hepatobiliary CA
Top Related