


![Uykan, Zekeriya; Jäntti, Riku Composite vector ... · UYKAN and JANTTI/Turk J Elec Eng & Comp Sci SDC [6] received much attention within the DAS academic community, and following](https://static.fdocuments.in/doc/165x107/6064d77e5ba3771e9668db5f/uykan-zekeriya-jntti-riku-composite-vector-uykan-and-janttiturk-j-elec.jpg)




Languages
Pages
Legal


/ 421
Upper Respiratory Upper Respiratory Tract InfectionsTract Infections
Saudi Diploma in Family Medicine Center of Post Graduate Studies in Family Medicine
Dr. Zekeriya Aktü[email protected]
www.aile.netUtilized work: Dr. Aynur Engin, Cumhuriyet University, Sivas, Turkey and Dr. Ela Eker, Trakya University, Edirne, Turkey
/ 422
• Acute tonsillitis• Acute pharyngitis• Acute otitis media• Acute sinusitis• Common cold• Acute laryngitis• Otitis externa• Mastoiditis• Acute apiglottis
Upper Respiratory Tract Infections

/ 423
Objectives
• At the end of this session, the participants should be able to;– List upper respiratory tract infections– Make differential diagnosis between URTI– Define criteria for antibiotic use– Apply and interpret the McIsaac scoring

/ 424
• Bacteria– S. pyogenes– C. diphteriae– N. gonorrhoeae
• Viruses– Epstein-Barr virus– Adenovirus– Influenza A, B– Coxsackie A – Parainfluenzae
Tonsilitis-pharyngitis

/ 425
• < 3 years 100 % viral
• 5-15 years– 15-30 % GABHS
• Adult– 10 % GABHS
Causative organisms

/ 426
• Spreads by close contact and through air• Spread more in crowded areas (KG, school,
army..)• Most common among 5-15 age group• More frequent among lower socio-
economic classes• Most common during winter and spring• Incubation period 2-4 days
Due to streptococci:
/ 427
Sore throat Anterior cervical LAP Fever > 38 C Difficulty in swallowing Headache, fatigue Muscle pain Nausea, vomiting
Signs/symptoms
Tonsillar hyperemia / exudates
Soft palate petechiaAbsence of coughingAbsence of nose dripAbsence of hoarseness

/ 428
• Having additional rhinitis, hoarseness, conjunctivitis and cough
• Pharyngitis is accompanied by conjunctivitis in adenovirus infections
• Oral vesicles, ulcers point to viruses
Viral tonsillitis/pharyngitis

/ 429
• GABHS• EBV • Adenovirus• Primary HIV infection• Candida albicans• Francisella tularensis
Exudates

/ 4210
• GABHS• Epstein-Barr virus• Adenovirus• Human herpesvirus type 6• Tularemia• HIV infection
Lymphadenopathy

/ 4211
• Throat swab– Gold standard
• Rapid antigen test– If negative need swab
• ASO– May remain + for 1 year
• WBC count• Peripheral smear
Laboratory

/ 4212
• Pathogens looked for– Group A beta hemolytic streptococci– C. diphteriae (rare)– N. gonorrhoeae (rare)
• If GABHS do we need antibiogram?– Is there resistence to penicilline?
Throat Culture
/ 4213
• Supurative complications– Abscess
– Sinusitis, otitis, mastoiditis
– Cavernous sinus thrombosis
– Toxic shock syndrome
– Cervical lymphadenitis
– Septic arthritis, osteomyelitis
– Recurrent tonsillitis/pharyngitis
• Nonsupurative complications– Acute romatoid fever
– Acute glomerulonephritis
Tonsillitis due to Streptococci

/ 4214
• Prevention of complications
• Symptomatic improvement
• Bacterial eradication
• Prevention of contamination
• Reducing unnecessary antibiotic use
Aim of Treatment
/ 4215
• Many different antibiotics can eradicate GABHS from pharynx
• Starting treatment within 9 days is enough to prevent ARF
Treatment

/ 4216
• Tetracycline
• Sulphonamides
• Co-trimoxasole
• Cloramphenicole
• Aminoglycosides
Antibiotics NOT to be used

/ 4217
• Control culture after full dose treatment?– NO
• If history of ARF:– Take control culture after treatment
• No need to screen or treat carriers
GABHS

/ 4218
• Developed by Mc Isaac and friends
• Decreases antibiotic usage by 48%
• No increase in throat swabs
Mc Isaac Scoring
http://www.cmaj.ca/cgi/content/abstract/163/7/811

/ 4219
Clinical Findings Score
Fever > 38 C 1
Absence of coughing 1
Tonsillary hypertrophy or exudates
1 (If < 6 years give 0)
Sensitivity at the anterior cervical nodes
1
Age 3 – 14 1
Age > 45 -1
Mc Isaac Scoring
/ 4220
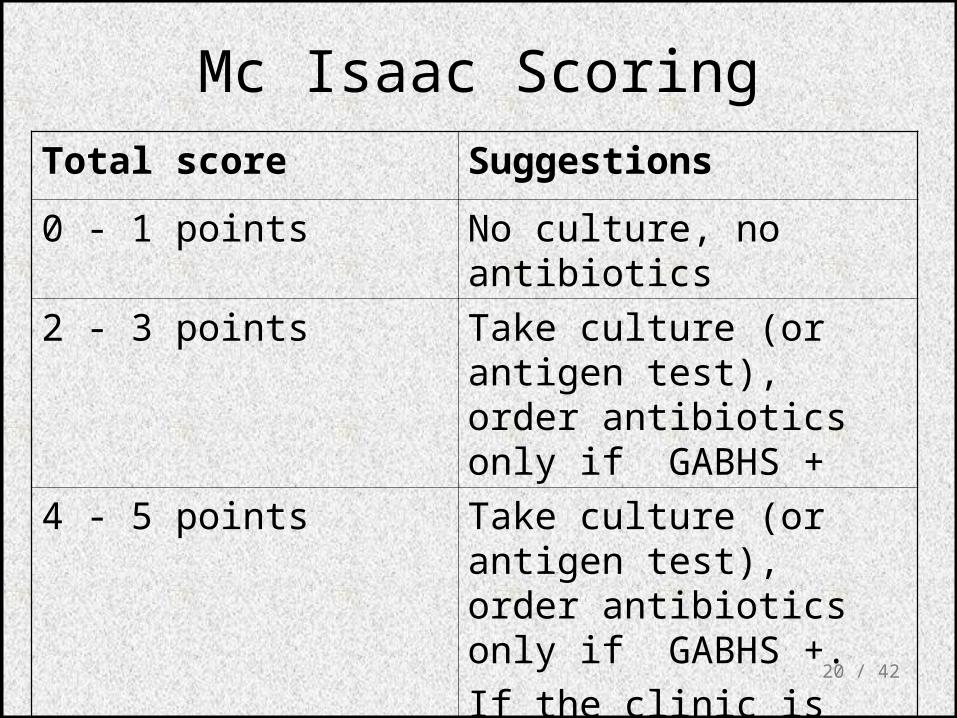
Total score Suggestions
0 - 1 points No culture, no antibiotics
2 - 3 points Take culture (or antigen test), order antibiotics only if GABHS +
4 - 5 points Take culture (or antigen test), order antibiotics only if GABHS +.
If the clinic is severe, start antibiotics without testing
Mc Isaac Scoring

/ 4221
ORAL
Penicilline V Children:2x250 mg or 3x250mg,10 days
Adults:3x500 mg or 4x500mg,10 days
PARENTERAL
Benzathine penicilline Adults:<27kg:600 000 U single dose, IM
>27 kg:1.200 000 U single dose, IM
ALLERGY TO PENICILLINE
Erithromycine estolate 20-40 mg/kg/day, 2x1 or 3x1, 10 days
Erithromycine ethyl succinate
40 mg/kg/day, 2x1 or 3x1, 10 days
Antibiotics in Tonsillitis/pharyngitis due to GABHS
/ 4222
• AOM• AOM not responding to treatment: Sustained
clinical and autoscopy findings despite 48-72 therapy
• Recurrent atitis media: 3 AOM attacks within 6 moths or 4 attacks within 1 year
Acute Otitis Media

/ 4223
• S. pneumoniae 30%• H. İnfluenzae 20%• M. Catarrhalis 15%• S. pyogenes 3%• S. aureus 2%• No growth 10-30%• Chronic otitis media: P. aeruginosa, S. aureus,
anaerobic bacteria
AOM causes

/ 4224
• 85% of children up to 3 years experience at least one,
• 50% of children up to 3 years experience at least two attacks
• AOM is usually self-limited. Rarely benefits from antibiotics.
• 81 % undergo spontaneus resolution.
Acute Otitis Media

/ 4225
• Symptoms– Autalgia– Ear draining– Hearing loss– Fever– Fatigue– Irritability– Tinnitus, vertigo
• Otoscopic findings– Tympanic membrane
erythema– Inflammation– Bulging– Effusion
• Hearing loss
Signs and Symptoms

/ 4226
First choice
Amoxicilline 40 mg/kg/day, 3 doses
Trimet./Sulfamethoxazole 8mg TM/40mg SMX/kg 2 dose
Second choice
Amoxicilline/clavulanate 45 mg/kg/day, 2 doses
Erythromycin 40-50 mg/kg/day, 3 doses
Reurrent AOM prophylaxis
Sulfisoxazole 75 mg/kg/day, single dose 3-6 mo
Amoxicilline 20 mg/kg/day, sinle dose 3-6 mo
Antibiotics

/ 4227
Acute sinusitis• Str. pneumoniae %41
• H. influenzae %35
• M. catarrhalis %8
• Others %16Strep. pyogenes S. aureus
Rhinovirus
Parainfluenzae
Veilonella, peptokoccus
Chronic sinusitis• Anaerob bakteria:
Bactroides, Fusobacterium
• S. aureus
• Strep. pyogenes
• Str. pneumoniae
• Gram (-) bakteria
• Fungi
Acute Rhinitis / Sinusitis

/ 4228
• Paranasal sinuses:– Frontal– Ethmoid– Maxillary– Sphenoid
• Most common during childhood– Maxillary– Ethmoid
• After age 10 – Frontal
Acute Sinusitis

/ 4229
/ 4230
• Anatomical: septal deviation,
• Mukociliary functions: cystic fibrosis, immotile cilia synd.
• Systemic dis., immune deficiency.: DM, AIDS, CRF
• Allergy: Nasal poliposis, asthma
• Neoplasia
• Environmental: smoking, air pollution, trauma...
Predisposition to Sinusitis

/ 4231
• Most important: Headache and postnasal dripping• Face congestion• Fever, fatigue, headache increased by leaning
forward• Nose obstruction• Nose dripping• Purulent secretions (rhinoscopy)• Sensitivity over the sinuses• Halitosis
Acute Rhinosinusitis

/ 4232
Rhinitis
• Increased symptoms after 5 days
• Symptoms lasting > 10 days
• Decreasing viral symptoms, nasal secretion becoming more purulent
are indicative for acute rhinosinusitis
Acute rhinosinusitis

/ 4233
• Direct x-ray– Diffuse opacification– Mucosal thickening >4 mm– air-fluid level
• Sinus aspiration– Rarely performed
• Nasal endoskopy• Tomography
– More sensitive compared with direct x-ray
– Indicated before surgery
Diagnosis

/ 4234
• Ampirical– Specific microbiologic diagnosis difficult
• Primary pathogens– S. pneumoniae– H. influenzae
Treatment

/ 4235
• Antibiotics questionable
• Stalman: 192 patients. No difference between placebo and doxycycline.
• Van Buchem: 214 patients. No difference between amoxycilline and placebo.
• Lindbaek: 130 patients. compared Pen V, Amoxycilline and placebo. 86 % of patients receiving antibiotics and 57% of patients receiving placebo improved.
Treatment
/ 4236
• Amoxycilline (Alfoxil) 3x500mg/d PO 10 d
• Amoxycilline/clavulonate (Augmentin) 3x625 mg/d PO 10 d
• Sefprosil(Serozil) 2x1000 mg/d PO 10 d
• Sefuroxim (Zinnat) 2x250 mg/d PO 10 d
• Azithromycine (Zitromax) First day 1x500 mg, then 1x250 mg/d PO 5 d
Antibiotics for Sinusitis

/ 4237
• Decongestants– Short duration 3-5 days
• Antihistamines– If allergy
• Normal saline
• Local steroids
Support Therapy

/ 4238
• Adults Rhinovirus
• Children Parainfluenzae and RSV
Common Cold

/ 4239
• Fatigue
• Feeling cold, shuddering
• Nose burning, obstruction, running
• Sneezing
• Fever
Common Cold

/ 4240
• Causes epidemics and pandemics
• Highly contagious
• Viral infection.
Influenza (flu)
/ 4241
Cause
• 80 % Influenzae virus
• Parainfluenza %2-9
• Rhinovirus %3
• Adenovirus %4

/ 4242
• Sudden onset after 12-24 hours incubation
• General weakness and fatigue
• Feeling cold, shivering, temp. Up to 39-40 C
• No sore throat or running nose
• Severe back, muscle and joint pain
Influenza
Top Related