Zygoma implant-supported midfacial - Constantin Alexander.pdf
13
Zygoma implant-supported midfacial prosthetic rehabilitation: a 4-year follow-up study including assessment of quality of life Constantin Alexander Landes Authors’ affiliation: Constantin Alexander Landes, Maxillofacial and Plastic Facial Surgery, The J.-W. Goethe University Medical Centre, Frankfurt, Germany Correspondence to: Dr Dr Constantin Alexander Landes Klinik fu ¨ r Kiefer und plastische Gesichtschirurgie Johann-Wolfgang Goethe Universita ¨t Frankfurt Theodor-Stern-Kai 7 60596 Frankfurt am Main Germany Tel.: þ 49-69-6301-5879 Fax: þ 49-69-6301-5644 e-mail: [email protected] Key words: maxillary defect, maxillectomy, midfacial rehabilitation, prosthetic cantilever, zygoma implant, Zygomaticus fixture Abstract Objective: Successful prosthetic rehabilitation is crucial for quality of life in cases of large maxillary defects when surgical reconstruction is not advisable because of general health or patient refusal. For this purpose, the extended indications for Zygomaticus s fixtures in different defect types were evaluated. Patients and methods: Twelve patients received 28 zygoma implants and 23 dental implants (if a segment of alveolar process was available) and were followed-up 14–53 months. Zygoma implants were positioned classically in the maxillary molar region and to reduce leverage, a premolar and a canine position was developed. The quality of life was assessed by a validated questionnaire after complete rehabilitation. Results: Cumulative zygoma implant survival was 82%. Three losses occurred because of persistent infection and gradual loosening. Lost implants were immediately replaced in adjacent bone. Insufficient implant length within soft tissue reconstructions was prone to chronic infection by pocketing and recurrent overgrowth of granulating tissue. Longer implants were free of soft tissue inhibition, yet prone to overloading and high leverage in cases when no anterior alveolar process and dental implants were present. Zygoma implant success was therefore 71%, including the new premolar and canine Zygomatikusfixture- position. Periotest s values increased from 0 to þ 7 to the fourth year, peri-implant bleeding and plaque index were decreasing from 56% to 0% and 33% to 0%, respectively, and good general quality of life with the priorities on chewing and activity was noted. Conclusion: Zygoma implants can reliably anchor the midfacial maxillary prostheses and enable a quality of life comparable with autologous maxillary reconstruction. They can be replaced immediately if local infection or loosening should occur. A premolar and canine position reduce leverage when no anterior alveolar process is present. The patient can alternatively be provided with dental implants. Patients with severe maxillary defects have major difficulties to re-establish their mas- tication, speaking, soft tissue projection and, therefore, social integration. When the options of local bone augmentation and elevation of the sinus floor do not supply sufficient bone for safe dental im- plant positioning (Triplett & Schow 1996), myocutaneous or osteo-myocutaneous tis- sue transfer is an alternative (Swartz et al. 1996; Rogers et al. 2003). However, some patients prefer to avoid secondary morbid- ity from reconstructive procedures, and others are limited by their general health condition. These individuals benefit from an oronasal obturator prosthesis. However, Copyright r Blackwell Munksgaard 2005 Date: Accepted 25 April 2004 To cite this article: Landes CA. Zygoma implant-supported midfacial prosthetic rehabilitation: a 4-year follow-up study including assessment of quality of life. Clin. Oral Impl. Res. 16, 2005; 313–325 doi: 10.1111/j.1600-0501.2005.01096.x 313
Transcript of Zygoma implant-supported midfacial - Constantin Alexander.pdf

Zygoma implant-supported midfacialprosthetic rehabilitation: a 4-yearfollow-up study including assessmentof quality of life
Constantin AlexanderLandes
Authors’ affiliation:Constantin Alexander Landes, Maxillofacial andPlastic Facial Surgery, The J.-W. Goethe UniversityMedical Centre, Frankfurt, Germany
Correspondence to:Dr Dr Constantin Alexander LandesKlinik fur Kiefer und plastische GesichtschirurgieJohann-Wolfgang Goethe UniversitatFrankfurtTheodor-Stern-Kai 760596Frankfurt am MainGermanyTel.: þ49-69-6301-5879Fax: þ49-69-6301-5644e-mail: [email protected]
Key words: maxillary defect, maxillectomy, midfacial rehabilitation, prosthetic cantilever,
zygoma implant, Zygomaticus fixture
Abstract
Objective: Successful prosthetic rehabilitation is crucial for quality of life in cases of large
maxillary defects when surgical reconstruction is not advisable because of general health or
patient refusal. For this purpose, the extended indications for Zygomaticuss fixtures in
different defect types were evaluated.
Patients and methods: Twelve patients received 28 zygoma implants and 23 dental
implants (if a segment of alveolar process was available) and were followed-up 14–53
months. Zygoma implants were positioned classically in the maxillary molar region and to
reduce leverage, a premolar and a canine position was developed. The quality of life was
assessed by a validated questionnaire after complete rehabilitation.
Results: Cumulative zygoma implant survival was 82%. Three losses occurred because of
persistent infection and gradual loosening. Lost implants were immediately replaced in
adjacent bone. Insufficient implant length within soft tissue reconstructions was prone to
chronic infection by pocketing and recurrent overgrowth of granulating tissue. Longer
implants were free of soft tissue inhibition, yet prone to overloading and high leverage in
cases when no anterior alveolar process and dental implants were present. Zygoma implant
success was therefore 71%, including the new premolar and canine Zygomatikusfixture-
position. Periotests values increased from 0 to þ7 to the fourth year, peri-implant bleeding
and plaque index were decreasing from 56% to 0% and 33% to 0%, respectively, and
good general quality of life with the priorities on chewing and activity was noted.
Conclusion: Zygoma implants can reliably anchor the midfacial maxillary prostheses and
enable a quality of life comparable with autologous maxillary reconstruction. They can be
replaced immediately if local infection or loosening should occur. A premolar and canine
position reduce leverage when no anterior alveolar process is present. The patient can
alternatively be provided with dental implants.
Patients with severe maxillary defects have
major difficulties to re-establish their mas-
tication, speaking, soft tissue projection
and, therefore, social integration. When
the options of local bone augmentation
and elevation of the sinus floor do not
supply sufficient bone for safe dental im-
plant positioning (Triplett & Schow 1996),
myocutaneous or osteo-myocutaneous tis-
sue transfer is an alternative (Swartz et al.
1996; Rogers et al. 2003). However, some
patients prefer to avoid secondary morbid-
ity from reconstructive procedures, and
others are limited by their general health
condition. These individuals benefit from
an oronasal obturator prosthesis. However,Copyright r Blackwell Munksgaard 2005
Date:Accepted 25 April 2004
To cite this article:Landes CA. Zygoma implant-supported midfacialprosthetic rehabilitation: a 4-year follow-up studyincluding assessment of quality of life.Clin. Oral Impl. Res. 16, 2005; 313–325doi: 10.1111/j.1600-0501.2005.01096.x
313

in cases of extensive palatomaxillary resec-
tion, these obturators tend to be unstable,
and residual anchoring teeth are frequently
overloaded and may be consecutively lost.
Furthermore, little frictional or capillary
retention is available when the patient is
edentulous and oronasal communication
present (Keller et al. 1987; Sakuraba et al.
2003). A dental-implant-retained obturator
frequently sustains high cantilever forces on
the anterior implants because of lack of
dorsal support, resulting in attachment loss
and finally implant loss (Parel et al. 2001).
Prosthetic rehabilitation in total alveolar
atrophy employing single bilateral Zygoma-
ticusfixturess (Branemark-System, Nobel-
Biocare Norden AB, Gothenburg, Sweden)
supporting the molar region and anterior
dental implants in residual canine alveolar
process are clinically established with
accruing follow-up (Reichert et al. 1999;
Bedrossian & Stumpel 2001; Bedrossian
et al. 2002; Malevez et al. 2004). This
study evaluates zygoma implants alone
and in combination with dental implants
as prosthetic anchors for better social re-
integration of patients suffering from max-
illary defects. Particular attention was
given to extended zygoma implant indica-
tions in 450% maxillectomies to reduce
leverage. Zygoma implant success and sur-
vival, as well as the quality of life, were
evaluated.
Patients and methods
Twelve patients received 28 zygoma im-
plants (Zygomaticusfixtures, Branemark-
System, Nobel-Biocare Norden AB).
Twenty-three additional dental implants
were inserted when a partial alveolar pro-
cess (i.e. a residual alveolar segment) was
present. Average age at implantation was
59 years (24–79 years), and 10 females and
two males were included, see Table 1. The
first patient suffered from total absence of
the maxillary alveolar process when all
teeth had been extracted at 20 years of
age because of amelogenesis imperfecta.
Earlier osteoplasty and a Le Fort I osteo-
tomy resulted in complete bone-transplant
resorption making dental implant place-
ment apart from the left canine region
impossible. The second patient had had
cleft lip, alveolar process and palate, a
severely scarred hard and soft palate pre-
senting with a complex defect with con-
comitant loss of the alveolar process
because of long-time edentulousness and
atrophy. A local osteoplasty was considered
hazardous for postoperative bone exposure
and resorption because of local scars after
multiple palatal reconstructive surgery. A
free combined bone-soft tissue flap with
microvascular anastomosis was considered
overtreatment. Patient no. 3 had a max-
illary osteosarcoma and refused free flap
reconstruction out of concern for masking a
tumor recurrence. The patient initially had
a 2/3 maxillectomy after the ablation of the
recurrence this defect became a 3/4 max-
illectomy. Patient no. 4 had a hemimax-
illectomy of a palatal squamous cell
carcinoma with cardiopulmonary disease
at 72 years, precluding major reconstruc-
tion. Patient no. 5 had palatal adenoid-
cystic carcinoma ablated 4.5 years ago
with hemimaxillectomy and successful re-
habilitation by a tooth retained obturator.
The retaining teeth had been lost because
of local cantilever overloading from absent
dorsal prosthesis support. A new obturator
retention without major surgery was re-
quested by the patient and major recon-
structive surgery was contraindicated.
Patient 6 had a recurrent malignant mixed
salivary carcinoma and cardiopulmonary
disease at 77 years of age. The tumor
recurred during follow-up, resulting in a
total maxillectomy. Patients no. 7–9 and
11 with hemimaxillectomy after palatal
and maxillary sinus squamous cell carcin-
oma ablation had cardiopulmonary disease.
Case no. 10 with an ameloblastoma (3/4
maxillectomy) is a diagnosed anxiety dis-
order and no. 12 a depressive disorder
making elaborate reconstructive operations
a high-risk intervention.
Implants were inserted intraoperatively
up to 59 months postoperatively, an aver-
age of 16 months later. For example, pa-
tient no. 6 received implants at the time of
tumor resection when frozen margins were
tumor free. Patients no. 1 and 2 were not
included in the calculation of the time
interval to the primary operation, as these
were more than 20 years previously. Six
patients received preoperative chemother-
apy and five patients were postoperative-
ly irradiated. When irradiation was
performed, the implants were inserted
on average after an 18-month disease-free
interval.
The implantation was performed under
general anaesthesia and 1 g of Cephalexine
(Rocephins, Roche, Basel, Switzerland)
intraoperatively and 250 mg of oral Cefur-
oxim (Elobacts, Cascan, Bad Oldeslone,
Germany) postoperatively twice for 5 days
were given. Resorbable stitches were used.
The insertion was readily performed accor-
ding to the technique given by Reichert
et al. (1999) and Parel et al. (2001). The
zygoma implant required a vestibular
Le-Fort I incision from the canine to the
molar area and local mucoperiosteal mobi-
lization. Thus, intraoral access to the zygo-
matic buttress area was directly created
after a partial maxillary resection. Alterna-
tively, when an intact maxillary sinus was
present, a suitable window in the anterior
wall was created. After the anterolateral
sinus mucosa had been mobilized, piloting
and implant placement were carried out
under direct visualization of the receptor
site from the sinus opening. Transcuta-
neous palpation of the exit area ensured
that the peripheral cortex was punctured.
When the diameter of the drill-hole was
correct, the tip of the inserted fixture could
be palpated transcutaneously piercing the
cortex by 1 or 2 mm. The patient’s indivi-
dual number of zygoma implants and den-
tal implants, implant length, position,
diameter, brand and abutment type can be
seen in Table 2. Complications and dura-
tion of follow-up are shown in Table 3. All
implants were allowed to heal for 6 months
and were loaded in succession. After the
healing period, the abutment procedure
followed under local anaesthesia, in three
cases combined with a peri-implant soft-
tissue reduction. All patients were seen at
monthly to 6-month intervals depending
on their primary affliction. The mean Perio-
tests-values (Gulden-Medizin technik,
Beusheim, Germany) (Lukas & Schulte
1990), peri-implant bleeding indices (PBIs)
and plaque indices (PIs), (Loe 1967) were me-
asured after implant loading at 6 months,
and every 6 months. Probing depths could
not be measured when zygoma implants
had bulky local flaps and hypertrophic
sinus mucosa at their point of mucosal pene-
tration. Follow-up radiographs 12 months
after insertion or 6 months after loading
and every following year were scrutinized
for peri-implant radiolucencies. Dental to-
mograms gave inferior information and
therefore in preoperative, postoperative
Landes . Zygoma implant-supported midfacial prosthetic rehabilitation
314 | Clin. Oral Impl. Res. 16, 2005 / 313–325

Tab
le1.
Th
eb
en
chm
ark
pati
en
td
ata
,d
iag
no
ses,
pre
op
era
tive
chem
oth
era
py,
am
ou
nt
of
rese
ctio
nan
dp
ost
op
era
tive
irra
dia
tio
n
Pati
en
tn
o.
Ag
eat
pri
mary
op
era
tio
n(y
ears
)
Dia
gn
ose
sD
efe
ctsi
zeo
rext
en
to
ftu
mo
rab
lati
on
Ch
em
oth
era
py
Rad
iati
on
(Gy)
Ind
icati
on
for
zyg
om
aim
pla
nts
vs.
op
era
tive
maxi
llary
reco
nst
ruct
ion
Tim
eg
ap
toim
pla
nta
tio
n(m
on
ths)
120
Am
elo
gen
esi
sim
perf
ect
a,
lon
g-t
ime
full
pro
sth
esi
sTo
tal
ab
sen
ceo
fM
axi
llary
alv
eo
lus
Ost
eo
pla
sty
fail
ure
460
215
Bil
ate
ral
cleft
lip
an
dp
ala
te,
lon
g-t
ime
full
pro
sth
esi
sLa
rge
med
ian
defe
ct,
40%
of
the
hard
pala
tean
dalv
eo
lus,
seve
resc
arr
ing
Seve
rem
uco
-peri
ost
eal
scarr
ing
,h
igh
risk
for
ost
eo
pla
sty
reso
rpti
on
460
319
Maxi
llary
an
do
rbit
al
ost
eo
sarc
om
aT4N
0M
02/3
maxi
llect
om
yC
arb
op
lati
n-e
top
osi
dp
ho
sph
ate
45
Co
nce
alm
en
to
fre
cid
ive
by
free
flap
59
471
Maxi
llary
squ
am
ou
sce
llca
rcin
om
aT4N
1M
0H
em
imaxi
llect
om
y,so
ftti
ssu
ep
ala
tal
reco
nst
ruct
ion
61.5
Hig
her
ag
e,
card
iop
ulm
on
ary
dis
ease
6
558
Pala
tal
ad
en
oid
cyst
icca
rcin
om
a,
T4N
0M
0H
em
imaxi
llect
om
yLi
mit
ed
too
thlo
ssb
eca
use
of
ove
rlo
ad
ing
aft
er
4.5
years
too
th-b
orn
eo
btu
rato
rre
hab
ilit
ati
on
54
677
Recu
rren
tm
axi
llary
mix
ed
sali
vary
carc
ino
ma
T4N
0M
0To
tal
maxi
llect
om
yH
igh
er
ag
e,
card
iop
ulm
on
ary
dis
ease
0
757
Maxi
llary
squ
am
ou
sce
llca
rcin
om
aT4N
1M
0H
em
imaxi
llect
om
yPre
op
era
tive
cisp
lati
nem
bo
liza
tio
n51.3
Card
iop
ulm
on
ary
dis
ease
10
860
Maxi
llary
squ
am
ou
sce
llca
rcin
om
aT4N
0M
0H
em
imaxi
llect
om
y,so
ftti
ssu
ep
ala
tal
reco
nst
ruct
ion
wit
hlo
cal
flap
Cis
pla
tin
em
bo
liza
tio
np
reo
pera
tive
ly,
fou
rcy
cles
of
Do
xeta
cel
po
sto
pera
tive
ly
58
Card
iop
ulm
on
ary
dis
ease
9
977
Maxi
llary
squ
am
ou
sce
llca
rcin
om
a,
T4N
0M
0H
em
imaxi
llect
om
y,so
ftti
ssu
ep
ala
tal
reco
nst
ruct
ion
wit
hlo
cal
flap
Pre
op
era
tive
cisp
lati
nem
bo
liza
tio
nH
igh
er
ag
e,
card
iop
ulm
on
ary
dis
ease
6
10
46
Larg
em
axi
llary
am
elo
bla
sto
ma
3/4
maxi
llext
om
yLa
tep
rim
ary
inte
rvie
w,
gen
era
lan
xiety
dis
ord
er
14
11
52
Maxi
llary
squ
am
ou
sce
llca
rcin
om
aT4N
1M
0H
em
imaxi
llect
om
yPre
op
era
tive
cisp
lati
nem
bo
liza
tio
n51.3
Card
iop
ulm
on
ary
dis
ease
11
319
Maxi
llary
ost
eo
sarc
om
are
curr
en
ceT4N
0M
03/4
maxi
llect
om
y,p
ala
tal
soft
tiss
ue
reco
nst
ruct
ion
wit
hlo
cal
flap
45
Co
nce
alm
en
to
fre
cid
ive
by
free
flap
15
679
Mali
gn
an
tm
ixed
sali
vary
tum
or
recu
rren
ceT2N
0M
0To
tal
maxi
llect
om
yH
igh
er
ag
e,
card
iop
ulm
on
ary
dis
ease
,m
ult
iple
po
ssib
lyco
nce
ale
dtu
mo
rre
curr
en
ces
0
12
60
Maxi
llary
squ
am
ou
sce
llca
rcin
om
aT4N
0M
0H
em
imaxi
llect
om
y,so
ftti
ssu
ep
ala
tal
reco
nst
ruct
ion
wit
hlo
cal
flap
Pre
op
era
tive
cisp
lati
n-e
mb
oli
zati
on
Dep
ress
ive
dis
ord
er
3
Th
eti
me
gap
betw
een
op
era
tio
no
rir
rad
iati
on
toth
eim
pla
nt
inse
rtio
nis
list
ed
.N
ote
that
pati
en
ts3
an
d6
are
list
ed
twic
eas
they
had
two
pro
ced
ure
so
fzy
go
ma
imp
lan
tin
sert
ion
.
Landes . Zygoma implant-supported midfacial prosthetic rehabilitation
315 | Clin. Oral Impl. Res. 16, 2005 / 313–325

Tab
le2.
Th
ed
en
tal
statu
s,su
rgery
data
an
dp
rost
heti
ctr
eatm
en
t
Pati
en
tn
o.
Ag
eat
imp
lan
tati
on
(years
)
Den
tal
statu
sN
o.
of
zyg
om
aim
pla
nts
Imp
lan
tati
on
site
Zyg
om
aim
pla
nt
len
gth
(mm
)
Loca
lan
ato
my,
nu
mb
er,
loca
tio
nan
db
ran
do
fth
ead
dit
ion
al
den
tal
maxi
llary
imp
lan
tsPro
sth
eti
ctr
eatm
en
taft
er
6m
on
ths
heali
ng
peri
od
147
Ed
en
tulo
us
216,2
645,4
5B
ilate
ral
sin
gle
zyg
om
afi
xtu
re,
on
ed
en
tal
imp
lan
tat
23
resi
du
al
bo
ne
tran
spla
nt,
man
dib
leed
en
tulo
us
1O
ne
Bra
nem
ark
10�
4m
mfi
xtu
rere
gio
23
Th
ree
ind
ivid
ual
go
ldte
lesc
op
es
an
do
verd
en
ture
268
Ed
en
tulo
us
216,2
645,4
5B
ilate
ral
sin
gle
zyg
om
afi
xtu
re,
no
alv
eo
lus
pre
sen
t,m
an
dib
leed
en
tulo
us
0Tw
oin
div
idu
al
go
ldte
lesc
op
es
an
do
verd
en
ture
324
Part
iall
yd
en
tate
216,1
535,3
0D
en
tate
resi
du
al
alv
eo
lus
at
23–2
7,
man
dib
leco
mp
lete
lyd
en
tate
0Tw
om
ag
neti
cte
lesc
op
es
an
dp
art
ial
den
ture
wit
hb
race
sto
reta
inin
gte
eth
472
Ed
en
tulo
us
216,2
635,3
5N
oalv
eo
lus
pre
sen
t,d
en
tal
imp
lan
tin
sert
ion
on
lym
ed
ial,
incl
ud
ing
nasa
lsp
ine,
man
dib
leed
en
tulo
us
1O
ne
med
ian
Bra
nem
ark
10�
4m
mfi
xtu
reTh
ree
ind
ivid
ual
go
ldte
lesc
op
es
an
do
verd
en
ture
562
Part
iall
yd
en
tate
126
45
Teeth
24,
25
were
lost
beca
use
of
ove
rlo
ad
ing
an
dd
ors
al
can
tile
ver
forc
es,
resi
du
al
maxi
lla
an
dm
an
dib
led
en
tate
2Tw
oB
ran
em
ark
MK
IV4�
13
mm
fixt
ure
sat
reg
io24,
25
Th
ree
ind
ivid
ual
go
ldte
lesc
op
es
an
do
verd
en
ture
677
Ed
en
tulo
us
216,2
645,4
5N
oalv
eo
lus
aft
er
tota
lm
axi
llect
om
y(a
part
fro
mth
eo
rbit
al
flo
or)
,m
an
dib
leed
en
tulo
us
0Tw
oin
div
idu
al
go
ldte
lesc
op
es
an
do
verd
en
ture
758
Ed
en
tulo
us
116
30
Seve
realv
eo
lar
atr
op
hy
den
tal
imp
lan
tin
sert
ion
on
lyp
oss
ible
incl
ud
ing
the
nasa
lsp
ine,
man
dib
leed
en
tulo
us
1O
ne
med
ian
Bra
nem
ark
10�
4m
mfi
xtu
reTw
ore
ad
y-m
ad
eb
all
ab
utm
en
tsan
do
verd
en
ture
861
Ed
en
tulo
us
126
35
Suffi
cien
tan
teri
or
alv
eo
lar
bo
ne
for
ad
dit
ion
al
den
tal
imp
lan
tp
lace
men
t,m
an
dib
leed
en
tulo
us
5Fi
veIT
ISL
Aso
lid
scre
ws
12�
4.1
mm
reg
io15,
13,
11,
21,
23
Six
read
y-m
ad
eb
all
ab
utm
en
tsan
do
verd
en
ture
977
Part
iall
yd
en
tate
215,1
630,3
5A
nte
rio
rd
en
tate
pati
en
t,w
ith
ed
en
tulo
us
alv
eo
lus
an
teri
or
toth
ezy
go
ma
imp
lan
ts,
man
dib
leed
en
tulo
us
2Tw
oIT
ISL
Aso
lid
scre
ws
reg
io11,
13
Go
lden
ind
ivid
ual
bar-
ab
utm
en
tan
do
verd
en
ture
10
47
Ed
en
tulo
us
225,2
630,3
5C
on
trala
tera
led
etu
lou
salv
eo
lus,
man
dib
leed
en
tulo
us
4Fo
ur
ITI
SLA
soli
dsc
rew
sre
gio
12,
13,
14,
15
Fou
rin
div
idu
al
go
ldte
lesc
op
es
an
do
verd
en
ture
11
53
Part
iall
yd
en
tate
215,1
630,3
5C
on
trala
tera
led
etu
lou
salv
eo
lus,
resi
du
al
maxi
llary
inci
sors
man
dib
leed
en
tulo
us
4Fo
ur
ITI
SLA
soli
dsc
rew
sre
gio
11,
21,
23,
25
Six
ind
ivid
ual
go
ldte
lesc
op
es
an
do
verd
en
ture
327
Part
iall
yd
en
tate
416,1
5,1
3,2
335,4
0,3
5,4
0R
esi
du
al
alv
eo
lus
at
teeth
24–2
7,
man
dib
leco
mp
lete
lyd
en
tate
1O
ne
Bra
nem
ark
MK
IV15
mm
fixt
ure
reg
io26
betw
een
resi
du
al
teeth
Go
lden
ind
ivid
ual
bar-
ab
utm
en
tan
dp
art
ial
den
ture
,si
ng
lecr
ow
nsu
pra
stru
ctu
reto
imp
lan
tat
26
679
Ed
en
tulo
us
315,2
5,2
640,4
0,4
5N
oalv
eo
lus
aft
er
tota
lm
axi
llect
om
y(a
part
fro
mo
rbit
al
flo
or)
,m
an
dib
leed
en
tulo
us
0Fo
ur
ind
ivid
ual
go
ldte
lesc
op
es
an
do
verd
en
ture
12
60
Ed
en
tulo
us
216,2
635,3
5Ed
en
tulo
us
an
teri
or
alv
eo
lus
pre
sen
t,m
an
dib
leed
en
tulo
us,
fou
rin
terf
ora
min
al
ITI-
imp
lan
ts
2Tw
oIT
ISL
Aso
lid
scre
ws
reg
io13,
23
Two
ind
ivid
ual
para
llel
barc
lip
san
do
verd
en
ture
Pati
en
ts3
an
d6
req
uir
ed
zyg
om
aim
pla
nt
rep
lace
men
tb
eca
use
of
chro
nic
infl
am
mati
on
inco
nju
nct
ion
wit
ho
verl
oad
an
dco
nse
cuti
velo
ose
nin
g.
Landes . Zygoma implant-supported midfacial prosthetic rehabilitation
316 | Clin. Oral Impl. Res. 16, 2005 / 313–325

Tab
le3.
Data
fro
mth
efo
llo
w-u
pin
clu
din
gco
mp
lica
tio
ns
an
dlo
sses,
peri
od
on
tal
para
mete
rsan
dsc
ore
sat
the
qu
ali
tyo
fli
feq
uest
ion
nair
e
Landes . Zygoma implant-supported midfacial prosthetic rehabilitation
317 | Clin. Oral Impl. Res. 16, 2005 / 313–325

and follow-up, the occipitomental Water’s
projection was preferred. The dental im-
plants were, however, judged based on
dental tomograms.
Weber two-point discrimination deter-
mined the accuracy of skin sensitive discri-
mination; that is, the distance between two
points that must be spanned before subjects
report feeling two distinct sensations. Static
or moving assessment measures the adapt-
ing fiber-receptor system. When this test
was bilaterally equal in those dermal seg-
ments innervated by the infraorbital and
zygomaticofacial nerve, a positive result
was noted (Dellon 1978). When there was
bilateral maxillary resection, the supraorbi-
tal segment was examined and the area of
lesser sensitivity in comparison noted as
negative. Likewise negative results were
recorded when it was known the nerve
had been intra-operatively cut.
The Kaplan–Meier analysis was made for
implant success after the following criteria:
clinical mobility 0–1, no peri-implant
radiolucency, no prevalent peri-implant
infection with purulent secretion, no pain,
discomfort or dysaesthesia related to the
implant placement (adapted after Buser
et al. 1990). Survival referred simply to
whether the implant was in situ or not.
After the completion of the prosthetic re-
habilitation, 6 months after implant inser-
tion all patients were asked to fill out a
University of Washington Quality-of-Life
scale questionnaire (UW-QOL, Weymuller
et al. 2001; Rogers et al. 2002). The UW-
QOL is a validated 12-item questionnaire,
completed by the patient and emphasizing
critical issues of oral, head and neck tu-
mors and their treatment, i.e. pain, appear-
ance, activity, recreation, swallowing,
chewing, speech, shoulder mobility, taste,
saliva, mood and anxiety. Version 4 in-
cludes the psychological dimension of
quality of life (Rogers et al. 2002, 2003).
An importance rating on an individual
basis, two health-related quality-of-life
questions and one general quality-of-life
question are included. The domains are
scored from no symptoms (i.e. pain) to
severe symptoms in four or five grades,
the corresponding values are 100, 75, 50,
25 and 0 or 100, 67, 33 and 0, respectively.
These can be applied in individual long-
itudinal follow-up and the composite UW-
QOL score is obtained by averaging the
domain scores. In this study, the time-
point average percentage and percentile of
maximum life quality (i.e. minimum
pathology after completed prosthetic reha-
bilitation) were evaluated.
Results
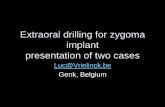
With a follow-up of 14–53 months the
Kaplan–Meier cumulative 4-year zygoma
implant survival/in situ rate was 82% (see
Tables 3 and 4, Fig. 1). Assuming intra-
individual dependence, 83% of patients
had no zygoma implant loss (Chuang et al.
2001). The rate of chronic zygoma implant
infection was 11% and all were lost during
follow-up. One loaded implant loss within
the first year probably was because of local
overloading (patient no. 6) (see Fig. 2). It
was explanted, two zygomafixtures were
immediately inserted anterior and dorsal to
the original implant slot. At the right
zygoma, a parallel zygomafixture was posi-
tioned anterior to support the premolar
region. Seven identical ‘pairs’ of parallel
zygomafixtures were inserted in six pa-
tients in an identical fashion to reduce the
prosthetic leverage and support the pre-
molar region. The patient with two implant
losses in the second year (no. 3) had
chronic infection around two zygomafix-
tures that were buried in granulation tissue
(Fig. 3). After replacement by a right-sided
pair of parallel zygoma implants, one addi-
tional third zygoma implant was positioned
anteriorly on each side and supported the
canine region. This should once more re-
duce leverage on the zygoma implants and
consecutive overloading from anterior bi-
ting and mastication, as addressed in patient
no. 6 (Fig. 2). Insufficient zygoma implant
length within flap reconstructions was
prone to recurrent local infection by pock-
eting and overgrowth of granulating tissue
(i.e. patients no. 3 and 10). In the last case
two implants for the above reason could
not become integrated in the prosthetic
rehabilitation. Although these implants
were osseointegrated and they survived,
they could not be counted as successes.
Longer implants were free of soft tissue
inhibition yet prone to overloading by
high leverage as seen in Fig. 2. PI, PBI at
the end of the follow-up can be seen in
Table 3 decreasing from 56% to 0% and
33% to 0%, which may be attributed to
repeated personal hygiene instruction and
better compliance once local scarring had
set and the prostheses were incorporated
into the patient’s body concept. No im-
plant had infection or purulent secretion at
the end of the follow-up.
All implants were clinically stable, and
the latest Periotests values can be seen in
Table 3 increasing from average 0 to 7 in
the fourth year. No peri-implant radio-
lucencies were noted on Water projections
at the end of follow-up. Because of over-
projection of the cranial base peri-implant
bone loss could not be evaluated.
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
1 3
%
Implant survival (in white) and success (in black) was assessed for a 4 year follow-up
2 4
Fig. 1. Kaplan-Meier analysis of implant survival and success.
Landes . Zygoma implant-supported midfacial prosthetic rehabilitation
318 | Clin. Oral Impl. Res. 16, 2005 / 313–325

The zygomaticofacial nerve sensitivity
was intact in all cases except patient no. 3
who had it resected at tumor removal. The
infraorbital nerve was never severed during
zygoma implant insertion, however, five of
12 patients had primary nerve resection
when tumor ablation was performed (see
Table 3). No patient reported foreign-body
sensation, dysaesthesia coming from the
implants or pain on implant percussion.
Therefore, a zygoma implant success
rate of 71% was reached when the three
losses and two zygoma implants that could
not be loaded were subtracted (Fig. 1).
Assuming intraindividual dependence 75%
of patients had immediately successful
treatment (Chuang et al. 2001).
As abutments gold or magnetic tele-
scopes were used in nine prostheses. Three
prostheses had individual bar-clips and two
ready-made ball abutments. Two patients,
because of implant removal and tumor
recurrence ablation, required a second pros-
thesis. Only the first prosthesis in patient
no. 3 braced the remaining teeth, all other
cases did not. After recurrence, the bar-clip
was sufficient for retention.
The UW-QOL questionnaire was re-
turned in eight cases after prosthetic treat-
ment (80%), two cases were not oral tumor
or cancer patients (nos. 1 and 2) and, there-
fore, the questionnaire did not apply to
them (presented in Tables 3 and 4). Half
of the patients did not register any pain, the
other half only had accidental to moderate
pain. One case reported painkiller taking
at intervals because of scarring, impaired
swallowing, xerostomia and mucositis
after irradiation (no. 11). The majority of
cases noted little changes in their outward
appearance, however, two complained of
major changes in conjunction with exen-
teration (Fig. 3, no. 3) or severe local radio-
dermatitis of the cheek and malar complex
(no. 11). All patients noted none to min-
imal limitation in activities. Three patients
reported 100% and five medium chewing
capacity. Speech without limitation was
noted by 63% of the patients, the remain-
der reported minor difficulties but were
heard speaking on the telephone. Taste in
all cases was 75–100% present. Most pa-
tients reported adequate saliva, but two had
xerostomia. Except in one young osteo-
sarcoma case with exenteration (Fig. 3,
patient no. 3), all reported good emotional
stability and little anxiety. The patientTab
le4.
Th
eU
niv
ers
ity
of
Wash
ing
ton
Qu
ali
ty-o
f-Li
fe(U
W-Q
OL)
inh
ead
an
dn
eck
can
cer
qu
est
ion
nair
esc
ore
s
Item
no
.Sy
mp
tom
0%
25%
30%
50%
70%
75%
100%
Mean
(%)
%B
est
sco
re
1Pain
11
24
78
50
2A
pp
eara
nce
26
63
03
Act
ivit
y7
178.1
13
4R
ecr
eati
on
62
82
25
5Sw
all
ow
ing
17
92
88
6C
hew
ing
53
69
38
7Sp
eech
35
89
63
8Sh
ou
lder
21
579
63
9Ta
ste
26
94
75
10
Sali
va1
16
76
79
11
Mo
od
16
172
13
12
An
xiety
16
169
13
Pain
Ap
peara
nce
Act
ivit
yR
ecr
eati
on
Swall
ow
ing
Ch
ew
ing
Speech
Sho
uld
er
Tast
eSa
liva
Mo
od
An
xiety
13
Pri
ori
ties
21
33
13
21
12
Mu
chw
ors
eW
ors
eId
en
tica
l/m
od
era
teB
ett
er/
go
od
Mu
chb
ett
er
Exc
ell
en
tM
ean
(%)
%O
pti
mal
valu
e
14
Healt
h-r
ela
ted
qu
ali
tyo
fli
feco
mp
are
dw
ith
the
pre
thera
-p
eu
tic
situ
ati
on
12
12
2Id
en
tica
l54
0
15
Healt
h-r
ela
ted
qu
ali
tyo
fli
fein
the
last
7d
ays
16
1B
ett
er
67
0
16
Gen
era
lq
uali
tyo
fli
fe5
3G
oo
d73
0
Resu
lts
of
eig
ht
of
ten
pati
en
tsw
ho
retu
rned
their
an
swere
dU
W-Q
OL
qu
est
ion
nair
e.
Pati
en
tsw
ere
mo
stco
nce
rned
wit
hch
ew
ing
,re
creati
on
an
dact
ivit
yin
gen
era
l.Th
eg
en
era
lli
feq
uali
tyw
as
go
od
,m
ost
pati
en
tsexp
eri
en
ced
iden
tica
lh
ealt
h-r
ela
ted
qu
ali
tyo
fli
feco
mp
are
dw
ith
the
pre
thera
peu
tic
situ
ati
on
.
Landes . Zygoma implant-supported midfacial prosthetic rehabilitation
319 | Clin. Oral Impl. Res. 16, 2005 / 313–325

priorities in judging successful rehabilita-
tion were in descending order: chewing,
activity, recreational activity and speech,
emotional stability, and pain. Appearance,
swallowing, shoulder mobility and xero-
stomia were noted by one patient to be
major concern (no. 11). Half of the patients
reported better health-related quality of life
than before treatment onset. The other
reported worsening of their general health.
However, the general quality-of-life aver-
age was reported to be much better.
Discussion
The use of the zygomatic bone as implant
site in conjunction with ablative tumor
surgery has been previously described
(Parel et al. 1986; Vuillemin et al. 1990;
Jensen et al. 1992; Izzo et al. 1994; Rou-
manas et al. 1994; Evans et al. 1996;
Weischer et al. 1997; Reichert et al.
1999). Autologous bone grafting, myocuta-
neous or osteo-myocutaneous tissue trans-
fer implies major surgery. Considerable
donor site morbidity may occur although
satisfactory success rates have been well-
documented (Breine & Branemark 1980;
Isaksson 1994; Hurzeler et al. 1996;
Swartz et al. 1996; Lekholm et al. 1999;
Rogers et al. 2003). For zygomafixtures,
survival rates of 65% to 75% were reported
when they were inserted after ablative
tumor surgery (Weingart et al. 1992), and
a similar 71% zygoma implant success
was found in the present study in 4-year
follow-up. Only multi-centre studies pro-
vide cases in adequate numbers for a defect-
specific success analysis. The value of a
homogenous collective for clinical use is
limited as most centres face variant defect
severity in few patients. Large maxillary
cleft-palate defects are a sequel of no better
up-to-date treatment today for elderly pa-
tients. Extended maxillary resections are
individually different for each patient. Dif-
ferent treatment regimens and safety mar-
gins are used for different malignomas at
different centers. Detailed analysis of mul-
tiple cases, with examination of the tech-
nical possibilities using zygomafixtures
broadens the indication range. Similar to
Malevez et al. (2004), the intimacy of bone
to implant contact and marginal bone loss
were difficult to evaluate. Water’s projec-
tion seemed reliable for judging peri-im-
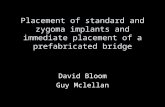
Fig. 2. (a, b) Patient no. 6, aged 77 years, suffered from recurrent malignant maxillary salivary gland carcinoma
and cardiopulmonary disease precluded operative maxillary reconstruction. At first one zygoma implant on
each side provided obturator retention by telescopes. The left loaded zygoma implant was lost within the first
year probably because of overload and leverage. Before the left implant definitely failed, a local infection with
extraoral fistulation occurred. (c, d) Furthermore, a local recurrent tumor was resected and the left fixture was
explanted. Three new implants were immediately positioned as can be seen on the Water’s projection. Two
implants were positioned on the left, anterior and posterior to the original implant site. A second implant was
positioned anterior in the right zygoma to support the premolar region as well. (e, f) The telescoped fixtures
piercing the bulky mucosa, an absent alveolar process and the complete rehabilitation can be seen.
Landes . Zygoma implant-supported midfacial prosthetic rehabilitation
320 | Clin. Oral Impl. Res. 16, 2005 / 313–325

plant radiolucency when compared with
CT and dental tomograms.
In this study 17% of patients faced zy-
goma implant losses. However, uneventful
and successful replacement was possible.
Parel et al. (2001) reported that zygoma
implant-borne dorsal defect prosthesis sup-
port decreased the leverage on the remain-
ing teeth and anterior dental implants. This
concept is supported by the fact that zy-
goma implants are overloaded when posi-
tioned in the molar region in the absence of
an anterior maxilla. Parallel anterior zy-
goma implants enabled a trapezoid pros-
thesis support. Moreover, anteroposterior
zygomafixtures created support in the can-
ine region as called for by Reichert et al.
(1999). Four factors of zygoma implant
failure could be determined: overloading
leverage in extensive maxillectomy, over-
growth of local soft tissues restricting the
abutment connection, recurrent infection
triggered by the above factors and tumor
recurrence. The latter did not force zygoma
implant removal in this series as recur-
rences did not occur at implant sites. The
follow-up did not show implant fatigue
fractures as hypothesized (Reichert et al.
1999) because of the long arm of lever.
Reichert et al. (1999) and this study used
zygoma implants in cases when patients
refused the morbidity of bone transplanta-
tion from the iliac crest or fibula and when
the general condition did not permit major
reconstruction. The authors report five
indications for zygoma implants: tumor
ablation maxillectomy, osteoplasty failure,
osteoplasty avoidance, local stress relief
after osteoplasty and an alternative to si-
nus-lifting or sinuslift failure. Implant po-
sitioning in the alveolar crest or slightly
palatinal could not be maintained in bigger
maxillary defects. The implant head should
then rest close to the residual bone to
reduce leverage. However, it should not
be submerged in soft tissue to reduce the
risk of a local infection. Lastly soft tissue
thickness over the residual bone should be
kept to a minimum. Soft-tissue flaps create
deep peri-implant pockets that are prone to
infection.
Microporous implant surfaces compared
with machined surfaces have higher re-
moval torques after osseointegration and
the data documents a superior osseointe-
gration (Buser et al. 1991; Cochran et al.
1996). Therefore, SLA dental implants
were used in patients no. 8–12. Micropor-
ous surface in zygoma implants should be
prospectively considered. Wide opening of
the mouth with tongue protusion required
for zygoma implant insertion causes an
increased risk of intraoperative contamina-
tion. The vicinity to sinus mucosa and
moving gingiva at the implant-shaft are
unfavourable (see Fig. 2d) with open-lying
thread convolutions. A feasible compro-
mise may be a microporous surface re-
stricted to the zygoma implant tip.
Nkenke et al. (2003) evaluated the zygo-
matic bone diameter and report highly
trabecular bone quality. Employment of
at least four cortical portions is recom-
mended (i.e. the alveolar process at the
molar region and the cortex of the zygo-
Fig. 3. (a) Patient no. 3, aged 24 years, with re-
current maxillary and orbital osteosarcoma after
exenteration, 2/3 maxillectomy and soft-tissue
reconstruction with local flaps. Two zygoma
implants had been furnished with magnetic tele-
scopes. In the second year of loading both devel-
oped chronic infection, were buried in granulation
tissue and finally lost. (b) The infected and loo-
sened implants were removed, an anterior recur-
rence was resected and two parallel longer implants
were repositioned to support the molar and premo-
lar region as can be seen on the Water’s projec-
tion. One additional anterior angulated zygoma
implant was positioned to rest in the zygomatic
body on each side and support the canine region
after 3/4-maxillectomy. (c, d) A bar-clip abutment
yielded sufficient stabilization a dental implant at
regio 26 was not needed for retention and there-
fore, treated with a single crown. (e, f) Complete rehabilitation with reconstructed eyelids and eye
epithesis.
Landes . Zygoma implant-supported midfacial prosthetic rehabilitation
321 | Clin. Oral Impl. Res. 16, 2005 / 313–325

Tab
le5.
Co
mp
ari
son
of
zyg
om
aim
pla
nt
an
do
btu
rato
rre
hab
ilit
ate
din
div
idu
als
fro
mth
isst
ud
yto
two
case
seri
es
rep
ort
ed
by
Ro
gers
et
al.
(2003)
zyg
om
aim
pla
nts
an
do
btu
rato
rp
rost
hesi
s-n¼
8
Free
deep
circ
um
flex
ilia
cart
ery
flap
reco
nst
ruct
ion
,n¼
20
Free
fib
ula
reco
nst
ruct
ion
,n¼
16
Ob
tura
tor
pro
sth
esi
sw
ith
-o
ut
imp
lan
tre
ten
tio
n,
n¼
28
Free
flap
maxi
llary
reco
nst
ruct
ion
,n¼
18
Zyg
om
aim
-p
lan
tsan
do
btu
rato
rp
rost
hesi
s,n¼
8
Free
deep
cir-
cum
flex
ilia
cart
ery
flap
reco
nst
ruct
ion
,n¼
20
Free
fib
ula
reco
nst
ruct
ion
,n¼
16
Ob
tura
tor
pro
sth
esi
sw
ith
ou
tim
-p
lan
tre
ten
tio
n,
n¼
28
Free
flap
maxi
llary
reco
nst
ruct
ion
,n¼
18
Mean
(%)
%B
est
sco
rePain
78
75
67
90
88
50
45
46
60
72
Ap
peara
nce
63
60
65
63
76
05
810
28
Act
ivit
y78
66
65
73
71
13
10
15
30
28
Recr
eati
on
81
73
71
80
75
25
20
23
30
33
Swall
ow
ing
91
79
52
91
88
88
60
870
67
Ch
ew
ing
69
55
31
60
58
38
25
820
28
Speech
89
75
74
79
76
63
35
21
30
33
Sho
uld
er
79
83
79
91
95
63
67
69
70
83
Tast
e94
76
45
75
55
14
Sali
va76
69
64
79
39
36
Mo
od
72
78
77
13
45
29
An
xiety
69
78
75
13
53
36
Ave
rag
e78
72
64
78
78
43
38
26
40
47
Ro
gers
et
al.
(2003)
AC
om
pa-
riso
no
fth
elo
ng
-term
mo
rbid
ity
foll
ow
ing
deep
circ
um
flex
ilia
can
dfi
bu
lafr
ee
flap
sfo
rre
con
stru
ctio
nfo
llo
win
gh
ead
an
dn
eck
can
cer.
Pla
stic
an
dre
con
stru
ctiv
esu
rgery
112:
1517–1
525.
Ro
gers
et
al.
(2003)
Healt
h-
rela
ted
qu
ali
tyo
fli
feaft
er
maxi
llect
om
y:a
com
pari
son
betw
een
pro
sth
eti
co
btu
rati
on
an
dfr
ee
flap
.Jo
urn
al
of
Ora
lan
dM
axi
llo
faci
al
Surg
ery
61:
174–1
81.
Ro
gers
et
al.
(2003)
Aco
mp
ar-
iso
no
fth
elo
ng
-term
mo
rbid
ity
foll
ow
ing
deep
circ
um
flex
ilia
can
dfi
bu
lafr
ee
flap
sfo
rre
con
stru
ctio
nfo
llo
win
gh
ead
an
dn
eck
can
cer.
Pla
stic
an
dre
con
stru
ctiv
esu
rgery
112:
1517–1
525.
Ro
gers
et
al.
(2003)
Healt
h-r
ela
ted
qu
ali
tyo
fli
feaft
er
maxi
llect
om
y:a
com
pari
son
betw
een
pro
sth
eti
co
btu
rati
on
an
dfr
ee
flap
.Jo
urn
al
of
Ora
lan
dM
axi
llo
faci
al
Surg
ery
61:1
74–1
81.
%o
fp
ati
en
tssc
ori
ng
go
od
or
bett
er
(all
/th
ose
wh
osc
ore
dg
oo
do
rb
ett
er)
Healt
h-r
ela
ted
qu
alit
yo
flif
ein
the
last
7d
ays
88
(7/8
)74
(14/1
9)
50
(7/1
4)
Gen
era
lq
uali
tyo
fli
fe100
(8/8
)68
(13/1
9)
50
(7/1
4)
Th
efi
rst
com
pare
sm
axi
llo
faci
al
free
bo
ne
reco
nst
ruct
ion
fro
mth
eil
iac
crest
(fre
ed
eep
circ
um
flex
ilia
cart
ery
flap
)w
ith
free
fib
ula
.Th
ese
con
d,
tho
ug
hu
sin
gU
niv
ers
ity
of
Wash
ing
ton
Qu
ali
ty-o
f-Li
fe
(UW
-QO
L)ve
rsio
n1
wit
hli
mit
ed
com
pati
bil
ity
com
pare
so
btu
rato
rre
hab
ilit
ate
dm
axi
llect
om
yp
ati
en
tsvs
.fr
ee-fl
ap
reco
nst
ruct
ion
.Th
ele
ftco
lum
nare
the
mean
sco
res,
the
rig
ht
dark
shad
ed
gre
yth
eb
est
sco
rep
erc
en
tag
es.
Belo
ware
the
ave
rag
esc
ore
sfo
rb
lun
tco
mp
ari
son
.H
ealt
hre
late
dan
dg
en
era
lq
uali
tyo
fli
fesc
ore
sw
ere
no
tim
ple
men
ted
inU
W-Q
OL
vers
ion
1as
em
plo
yed
by
the
seco
nd
stu
dy.
Landes . Zygoma implant-supported midfacial prosthetic rehabilitation
322 | Clin. Oral Impl. Res. 16, 2005 / 313–325

matic bone). The inherent angle of 451
proved adequate and was readily connected
to abutments in all cases (Uchida et al.
2001). Schramm et al. (2000) in patients
and Steenberghe et al. (2003) in cadavers
use Computer and CT-assisted navigation
for an exact placement below 1 mm and 31,
which was not imperative in this series.
Navigation is adequate when navigation-
supported tumor ablation is performed
and the equipment is ready to use. In the
present study, the bone volume was suffi-
cient and the placement was not difficult.
Navigation by itself remains expensive and
prolongs the operation time but can sup-
port exact placement and optimum bone
utilization. Navigation-supported zygoma
implant positioning across the temporal
fossa could (Jensen et al. 1992) include
two more cortical fractions from the zygo-
matic arch. Although parallel zygoma im-
plant positioning was achieved manually,
inserting a third zygoma implant may be
facilitated through navigation not to jeopar-
dise the orbital floor. All zygoma implants
were stable even when inserted in only two
zygomatic cortical portions.
All patients gained good oronasal sealing,
speech and feeding, as well as midfacial and
upper lip projection according to their own
perception. To further measure individual
perception of rehabilitation, quality-of-life
assessment is mandatory. Multiple vari-
ables have to be considered in ‘successful’
rehabilitation. A constant struggle by a
patient overstrained in manual dexterity
to incorporate and remove an obturator
prosthesis or a prosthesis that yields no
chewing or speech cannot be called a suc-
cess. Preoperative, 6 and 12 months post-
operative ratings by patients with head and
neck cancer rated in a study similar to this
included, in descending order: speech,
chewing, swallowing, activity and appear-
ance (Rogers et al. 2002, 2003). A compar-
ison of zygoma implant rehabilitated
individuals’ UW-QOL scores to maxillofa-
cial cancer patients reconstructed with iliac
bone (deep circumflex iliac artery flap
(DCIA)) and free fibula bone is shown in
Table 5. A second study of maxillectomy
patients either reconstructed by obturator
or a free flap is added (Rogers et al. 2002,
2003). The zygoma implant-borne prosthe-
sis case series scored highest in activities
and recreation, swallowing, chewing,
speech, taste and saliva quality. Simple
obturator cases had the least pain and
equally good swallowing while free flap
maxillary reconstruction scored best for
appearance. Mood and anxiety were better
in DCIA and fibula reconstructed indivi-
duals. Health-related quality of life in the
last 7 days was superior for the zygoma
implant rehabilitated followed by DCIA.
The general quality of life in all cases was
good or better for zygoma implant rehabil-
itated, followed by DCIA and still 50% of
the fibula-rehabilitated patients. ANOVA
with a¼0.5 significance level revealed
significant differences for the score
averages: Po0.01 at F¼ 3.2. Therefore,
the outcome differences cannot be attri-
buted to chance. Reports using obturator
prostheses find better outcomes in small
defects when sufficient speech, chewing
and swallowing abilities are maintained
(Kornblith et al. 1996). Free graft recon-
struction was established partly to solve
the disadvantages of the obturator: nasal
leakage, cleaning, frequent prosthetic cor-
rections (Brown 1996; Cordeiro & Santa-
maria 2000) by itself or in combination
with an obturator (Sakuraba et al. 2003).
Large maxillary and orbitomaxillary defects
are difficult to fit with acceptable pros-
theses and impaired vision complicates
prosthesis handling. Various methods
have been described for large defect closure
(Pollice & Frodel 1998; Truitt et al. 1999;
Baumann & Ewers 2000) and the experi-
ences were cataloged as algorithms (Brown
et al. 2000; Cordeiro & Santamaria 2000).
To the DCIA flap (Brown 1996) came the
rectus abdominis and radial flap (Cordeiro
& Santamaria 2000), fibula (Futran &
Haller 1999) and subscapular artery flaps
(Uglesic et al. 2000). Dental implants can
be inserted into revascularized bone. How-
ever in many cases, resorption is high and
unless prefabricated transplants are used
(Breine & Branemark 1980). The best
choice remains obturation or free tissue
transfer (Rogers et al. 2003). Donor site
and overall morbidity has been variably
reported and the patient adapts to the pre-
valent reconstruction. If the patient’s
general health and consent permit, pre-
fabricated free transplants should be con-
sidered first. Zygoma implants can be
reliably used even in total maxillectomy.
However severe defects involving the orbi-
tonasal complex should remain a primary
indication for reconstructive surgery.
Resume
La rehabilitation prothetique reussie est cruciale
pour la qualite de vie dans les cas de lesions max-
illaires etendues quand la reconstruction chirurgicale
n’est pas envisageable du a des problemes generaux
ou a un refus du patient. Pour cette raison, les
indications etendues des implants Zygomaticuss
dans differents types de lesions ont ete evaluees.
Douze patients ont recu 28 implants zygoma et 23
implants dentaires (si un segment du rebord alveo-
laire etait disponible) et ont ete suivis entre 14 et 53
mois. Les implants zygoma ont ete positionnes
classiquement dans la region molaire maxillaire et
pour reduire la force de levier une position premo-
laire et une canine ont ete choisies. La qualite de vie
a ete evaluee par un questionnaire a la fin du
traitement. La survie cumulatif de l’implant zygoma
etait de 82%. Trois pertes ont ete constatees dues a
une infection persistante et une perte progressive.
Les implants perdus ont ete immediatement re-
places dans l’os adjacent. Une longueur implantaire
insuffisante a l’interieur des reconstructions de tis-
sus mous favorisait une infection chronique par
poches grandissantes et une reapparition de tissus
granuleux envahissants. Les implants plus longs
n’avaient pas d’inhibition des tissus mous mais
etaient sensibles a une charge trop importante et a
une force de levier trop elevee dans les cas ou aucun
rebord alveolaire anterieur et donc des implants
dentaires n’etaient presents. Le succes de l’implant
zygoma etait de 71%, incluant le nouveau zygoma-
ticus position implantaire aux niveaux premolaire et
canin. Des valeurs Periotests augmentaient de 0 a
þ7 apres quatre annees, le saignement paroımplan-
taire et l’indice de plaque diminuaient de 56 a 0% et
de 33 a 0%, et une bonne de qualite de vie avec des
priorites telles que la mastication et l’activite ont ete
notees. Les implants zygoma peuvent donc de man-
iere certaine ancrer des protheses maxillaires mi-
faciales et permettre une qualite de vie comparable
aux reconstructions maxillaires autogenes. Ils peu-
vent etre remplaces immediatement si une infection
locale ou une perte de stabilite survenait. Une
position premolaire et canine reduit l’effet de levier
quand il n’y a pas de rebord alveolaire anterieur
present. Ce patient peut eventuellement aussi rece-
voir des implants classiques.
Zusammenfassung
Ziel: Bei grossen Oberkieferdefekten ist die erfol-
greiche prothetische Rekonstruktion fur eine gute
Lebensqualitat entscheidend. Dies ist besonders
dann wichtig, wenn ein schlechter Allgemeinzu-
stand des Patienten die Behandlung verunmoglicht,
oder er die chirurgische Rekonstruktion verweigert.
Fur solche Falle erweiterte man den Indikationsber-
eich der Zygomaticuss-Implantate und untersuchte
sie bei verschiedenen Defekttypen.
Patienten und Methoden: Zwolf Patienten erhielten
28 Jochbeinimplantate und 23 Zahnimplantate (so-
fern noch ein Segment vom Alveolarfortsatzes
vorhanden war) und wurden wahrend 14 bis 53
Monaten nachuntersucht. Die Jochbeinimplantate
setzte man in der klassischen Region der Oberkie-
fermolaren. Um die Hebelkraft zu reduzieren,
Landes . Zygoma implant-supported midfacial prosthetic rehabilitation
323 | Clin. Oral Impl. Res. 16, 2005 / 313–325

suchte man auch eine Abstutzung in der Eckzahn-
und Pramolarenregion. Zur Beurteilung der Lebens-
qualitat unterbreitete man dem Patienten nach Ab-
schluss der Rehabilitation einen vorbereiteten
Fragebogen.
Resultate: Die kumulative uberlebensrate der Joch-
beinimplantate betrug 82%. Man verzeichnete drei
Implantatverluste auf Grund einer persistierenden
Infektion und einer schrittweisen Lockerung. Die
verlorengegangenen Implantate konnten im benach-
barten Knochen gleich wieder ersetzt werden. War
das Implantat ungenugend lang, so neigte das wie-
deraufgebaute Weichgewebe darum zu chronischen
Infekten mit Taschenbildung und es kam wiederholt
zu einem uberschiessenden Wachstum von Gra-
nulationsgewebe. Langere Implantate zeigten diese
Probleme nicht, neigten dafur aber zu uberlastungen
und waren grossen Hebelkraften unterworfen, wenn
im anterioren Bereich der Alveolarfortsatz oder un-
terstutzende Zahnimplantate fehlten. Die Erfolgs-
rate des Zygoma-Implantates betrug daher 71%.
Darin eingeschlossen waren die neuen Lokalisatio-
nen der Zygomaticus-Implantate im Pramolaren-
und Eckzahnbereich. Die Periotests-Werte nahmen
bis zum vierten Jahr von 0 auf þ 7 zu, die Blutung
um die Implantate und der Plaqueindex nahmen ab
von 56% auf 0% und 33% auf 0%. Ebenso konnte
man eine gute Lebensqualitat bezuglich Kaukomfort
und sonstiger Aktivitaten verzeichnen.
Zusammenfassung: Zygoma-Implantate konnen
Oberkieferprothesen in zuverlassiger Art im Mittel-
gesicht verankern und so zu einer Lebensqualitat
verhelfen, die einer autologen Oberkieferrekon-
struktion vergleichbar ist. Sie konnen immediat
ersetzt werden, wenn lokale Infekte auftreten, oder
sie sich losen sollten. Eine Positionierung in der
Pramolaren- oder Eckzahnregion vermindert die
Hebelwirkung, wenn der Alveolarkamm im ante-
rioren Bereich fehlt. Als Alternative stehen dem
Patienten die Zahnimplantate zur Verfugung.
Resumen
Objetivo: La rehabilitacion protesica exitosa es cru-
cial para la calidad de vida en los casos de defectos
maxilares extensos en los que la reconstruccion
quirurgica no es aconsejable debido a salud general
o rechazo del paciente. Para este proposito, se eva-
luaron las indicaciones extendidas para las fijaciones
Zygomaticuss en diferentes tipos de defectos.
Pacientes y Metodos: Doce pacientes recibieron 28
implantes zigomaticos y 23 implantes dentales (si
un segmento del proceso alveolar se encontraba
disponible) y se siguieron de 14 a 53 meses. Los
implantes zigomaticos se posicionaron clasicamente
en la region molar y para reducir la palanca se
desarrollo una posicion premolar o canina. Se valoro
la calidad de vida por medio de un cuestionario
validado tras la completa rehabilitacion.
Resultados: La supervivencias acumulada del im-
plante zigomatico fue del 82%. Hubo tres perdidas
debido a infeccion persistente y aflojamiento gra-
dual. Los implantes perdidos fueron inmediatamente
reemplazados en el hueso adyacente. Una longitud
insuficiente del implante dentro del tejido blando
tendio a infecciones cronicas por formacion de bolsas
y sobrecrecimiento recurrente de tejido de granula-
cion. Unos implantes mas largos se liberaron de la
inhibicion del tejido blando aunque tendieron a
sobrecarga y mayor palanca en los casos sin proceso
alveolar y sin implantes dentales. Por lo tanto el
exito de los implantes zigomaticos fue del 71%,
incluyendo las nuevas posiciones premolares y
caninas de fijacion zigomatica. Los valores de Peri-
otests se incrementaron de 0 a þ7 al 4 ano, el
sangrado periimplantario y el ındice de placa dis-
minuyeron del 56 al 0%, y se noto una buena
calidad general de vida con las prioridades de masti-
cacion y actividad.
Conclusion: Los implantes zigomaticos pueden an-
clar fiablemente las protesis mediofaciales maxilares
y permitir una calidad de vida comparable a la
reconstruccion maxilar antologa. Se pueden sustituir
inmediatamente si ocurre una infeccion local o un
aflojamiento. Una posicion premolar o canina re-
duce la palanca cuando no existe proceso alveolar
anterior. El paciente puede ser suministrado alter-
nativamente con implantes dentales.
References
Baumann, A. & Ewers, R. (2000) Application of the
buccal fat pad in oral reconstruction. Journal of
Oral and Maxillofacial Surgery 58: 392–393.
Bedrossian, E. & Stumpel, L.J. 3rd (2001) Immedi-
ate stabilisation at stage II of zygomatic implants:
rationale and technique. Journal of Prosthetic
Dentistry 86: 10–14.
Bedrossian, E., Stumpel, L. 3rd, Beckely, M. &
Indersano, T. (2002) The zygomatic implant:
preliminary data on treatment of severely resorbed
maxillae. A clinical report. International Journal
of Oral & Maxillofacial Implants 17: 861–865.
Breine, U. & Branemark, P.I. (1980) Reconstruction
of alveolar jaw bone. An experimental and clinical
study of immediate and performed autologous
bone grafts in combination with osseointegrated
implants. Scandinavian Journal of Plastic and
Reconstructive Surgery and Hand Surgery 14:
23–48.
Brown, J.S. (1996) Deep circumflex iliac artery free
flap with internal oblique muscle as a new
method of immediate reconstruction of maxillec-
tomy defect. Head and Neck 18: 412–421.
Brown, J.S., Rogers, S.N., McNally, D.N. & Boyle,
M. (2000) A modified classification of the max-
illectomy defect. Head and Neck 22: 17–26.
Buser, D., Schenk, R.K., Steinemann, S., Fiorellini,
J.P., Fox, C.H. & Stich, H. (1991) Influence of
surface characteristics on bone integration of tita-
nium implants. A histomorphometric study in
miniature pigs. Journal of Biomedical Materials
Research 25: 889–902.
Buser, D., Weber, H.P. & Lang, N.P. (1990) Tissue
integration of non-submerged implants. 1-year
results of a prospective study with 100 ITI hol-
low-cylinder and hollow-screw implants. Clinical
Oral Implants Research 1: 33–40.
Chuang, S.K., Tian, L., Wie, L.J. & Dodson, T.B.
(2001) Kaplan-Meier analysis of dental implant
survival: a strategy for estimating survival with
clustered observations. Journal of Dental Re-
search 80: 2016–2020.
Cochran, D.L., Nummikoski, P.V., Higginbottom,
F.L., Hermann, J.S., Makins, S.R. & Buser, D.
(1996) Evaluation of an endosseous titanium
implant with a sandblasted and acid etched
surface in the canine mandible: radiographic
results. Clinical Oral Implants Research 7:
240–252.
Cordeiro, P.G. & Santamaria, E. (2000) A classifica-
tion system and algorithm for reconstruction of
Landes . Zygoma implant-supported midfacial prosthetic rehabilitation
324 | Clin. Oral Impl. Res. 16, 2005 / 313–325

maxillectomy and midfacial defects. Plastic and
Reconstructive Surgery 105: 2331–2346.
Dellon, A.L. (1978) The moving two-point discrim-
ination test: clinical evaluation of the quickly
adapting fiber/receptor system. Journal of Hand
Surgery 3: 474–481.
Evans, J.H., Schweiger, J.W. & Wright, R.F. (1996)
Craniofacial osseointegration of a large midfacial
bone anchored in combination maxillofacial pros-
thesis: a clinical report. Journal of Prosthetic
Dentistry 75: 483–486.
Futran, N.D. & Haller, J.R. (1999) Considerations
for free-flap reconstruction of the hard palate.
Archives of Otolaryngology, Head and Neck
Surgery 125: 665–669.
Hurzeler, M.K., Kirsch, A., Ackermann, K.-L. &
Quinones, C.R. (1996) Reconstruction of the
severely resorbed maxilla with dental implants
in the augmented maxillary sinus: a 5-year clin-
ical investigation. International Journal of Oral &
Maxillofacial Implants 11: 466–475.
Isaksson, S. (1994) Evaluation of three bone grafting
techniques for severely resorbed maxillae in con-
junction with immediate endosseous implants.
International Journal of Oral & Maxillofacial
Implants 9: 679–688.
Izzo, S.R., Berger, J.R., Joseph, A.C. & Lazow, S.K.
(1994) Reconstruction after total maxillectomy
using an implant retained prosthesis: a case report.
International Journal of Oral & Maxillofacial
Implants 9: 593–595.
Jensen, T.O., Brownd, C. & Blacker, J. (1992)
Nasofacial prostheses supported by osseointeg-
rated implants. International Journal of Oral &
Maxillofacial Implants 7: 203–207.
Keller, E.E., van Roeckel, N.B., Desjardins, R.P. &
Tolams, D.E. (1987) Prosthetic-surgical recon-
struction of the severely resorbed maxilla with
iliac bone grafting and tissue-integrated pros-
theses. International Journal of Oral & Maxillo-
facial Implants 2: 155–165.
Kornblith, A.B., Zlotolow, I.M., Gooen, J., Huryn,
J.M., Lerner, T., Strong, E.W., Shah, J.P., Spiro,
R.H. & Holland, J.C. (1996) Quality of life of
maxillectomy patients using an obturator prosthe-
sis. Head and Neck 18: 323–334.
Lekholm, U., Wannfors, S., Isaksson, B. & Adiels-
son, B. (1999) Oral implants in combination with
bone grafts. A 3-year retrospective multicenter
study using the Branemark implant system. Inter-
national Journal of Oral and Maxillofacial Sur-
gery 28: 181–187.
Loe, H. (1967) The gingival index, the plaque index
and the retention index system. Journal of Perio-
dontology 38: 610–616.
Lukas, D. & Schulte, W. (1990) Periotest, a dy-
namic procedure for the diagnosis of the human
periodontium. Clinical Physics and Physiological
Measurement 11: 65–75.
Malevez, C., Abarca, W., Durdu, F. & Daelemans,
P. (2004) Clinical outcome of 103 consecutive
zygomatic implants. Clinical Oral Implants Re-
search 15: 18–22.
Nkenke, E., Hahn, M., Lell, M., Wiltfang, J.,
Schulze-Musgau, S., Stech, B., Radespiel-Troger,
S. & Neukam, F.W. (2003) Anatomic site evalua-
tion of the zygomatic bone for dental implant
placement. Clinical Oral Implants Research 14:
72–79.
Parel, S.M., Branemark, P.I., Ohrnell, L.O. &
Svensson, B. (2001) Remote implant anchorage
for the rehabilitation of maxillary defects. The
Journal of Prosthetic Dentistry 86: 377–386.
Parel, S.M., Holt, G.R., Branemark, P.I. & Tjell-
strom, A. (1986) Osseointegration and facial
prosthetics. International Journal of Oral &
Maxillofacial Implants 1: 27–29.
Pollice, P.A. & Frodel, J.L. (1998) Secondary recon-
struction of upper midface and orbit after total
maxillectomy. Archives of Otolaryngology, Head
and Neck Surgery 124: 802–808.
Reichert, T.E., Kunkel, M., Wahlmann, U. &
Wagner, W. (1999) Das Zygoma-Implantat – In-
dikationen und erste Erfahrungen. Zeitschrift fur
Zahnarztliche Implantologie 15: 65–70.
Rogers, S.N., Gwanne, S., Lowe, D., Humphris, G.,
Yueh, B. & Weymuller, E.A. (2002) The addition
of mood and anxiety domains to the University of
Washington Quality of Life scale. Head and Neck
24: 521–529.
Rogers, S.N., Laher, S.H., Overend, L. & Lowe, D.
(2002) Importance-rating using the University of
Washington Quality of Life questionnaire in pa-
tients treated by primary surgery for oral and
oro-pharyngeal cancer. Journal of Craniomaxillo-
facial Surgery 30: 125–132.
Rogers, S.N., Lakshmiah, S.R., Narayan, B., Lowe,
D., Brownson, P., Brown, J.S. & Vaughan, E.D.
(2003) A comparison of the long-term morbidity
following deep circumflex iliac and fibula free
flaps for reconstruction following head and neck
cancer. Plastic and Reconstructive Surgery 112:
1517–1525.
Rogers, S.N., Lowe, D., McNally, D., Brown, J.S. &
Vaughan, E.D. (2003) Health-related quality of life
after maxillectomy: a comparison between pros-
thetic obturation and free flap. Journal of Oral
and Maxillofacial Surgery 61: 174–181.
Roumanas, E., Nishimura, R., Beumer, J., Moy, P.,
Weinlander, M. & Lorant, J. (1994) Craniofacial
defects and osseointegrated implants: six-year
follow-up report on the success rates of craniofa-
cial implants at UCLA. International Journal of
Oral & Maxillofacial Implants 9: 579–585.
Sakuraba, W., Kimata, Y., Ota, Y., Uchiyama, K.,
Harii, K. & Ebihara, S. (2003) Simple maxillary
reconstruction using free tissue transfer and pros-
theses. Plastic and Reconstructive Surgery 111:
594–598.
Schramm, A., Gellrich, N.C., Schimming, R. &
Schmelzeisen, R. 2000 [Computer assisted inser-
tion of zygomatic implants (Branemark System)
after extensive tumor surgery]. Mund Kiefer Ge-
sichtschirurgie 4: 292–295.
Swartz, W.M., Banis, J.C., Newton, E.D., Ramasa-
try, S.S., Jones, N.F & Acland, R. (1996) the
osteocutaneous flap for mandibular and maxillary
reconstruction. Plastic and Reconstructive Sur-
gery 77: 530–545.
Van Steenberghe, D., Malevez, C., Cleynenbreugel,
J., Serhal, C.B., Dhoore, E., Schutyser, F., Sue-
tens, P. & Jacobs, R. (2003) Accuracy of drilling
guides for transfer from three-dimensional CT-
based planning to placement of zygoma implants
in human cadavers. Clinical Oral Implants Re-
search 14: 131–136.
Triplett, R.G. & Schow, S.R. (1996) Autologous
bone-grafts and endosseous implants: comple-
mentary techniques. Journal of Oral and Max-
illofacial Surgery 54: 486–494.
Truitt, T.O., Gleich, L.L., Huntress, G.P. & Gluck-
man, J.L. (1999) Surgical management of hard
palate malignancies. Otolaryngology, Head and
Neck Surgery 121: 548–552.
Uchida, Y., Goto, M., Katsuki, T. & Akioshi, T.
(2001) Measurement of the maxilla and zygoma
as an aid in installing zygomatic implants.
Journal of Oral and Maxillofacial Surgery 59:
1193–1198.
Uglesic, V., Virag M, . & Varga, S. (2000) Recon-
struction following radical maxillectomy with
flaps supplied by the subscapular artery. Journal
of Craniomaxillofacial Surgery 28: 153–160.
Vuillemin, T., Raveh, J., Ladrach, K. & Roux, M.
(1990) Reconstruction following hemimaxillec-
tomy. Schweizer Monatsschrift Zahnmedizin
100: 1082–1087.
Weingart, D., Schilli, W. & Strub, J.R. (1992) Pre-
prosthetic surgery and implantology. Schweizer
Monatsschrift Zahnmedizin 102: 1075–1982.
Weischer, T., Schettler, D. & Mohr, C. (1997)
Titanium implants in the zygoma as retaining
elements after hemimaxillectomy. International
Journal of Oral & Maxillofacial Implants 12:
211–214.
Weymuller, E.A., Alsarraf, R., Yueh, B., Deleyannis,
F.W. & Coltrera, M.D. (2001) Analysis of the
performance characteristics of the University of
Washington Quality of Life instrument and its
modification (UW-QOL-R). Archives of Otolar-
yngology, Head and Neck Surgery 127: 489–493.
Landes . Zygoma implant-supported midfacial prosthetic rehabilitation
325 | Clin. Oral Impl. Res. 16, 2005 / 313–325