Your Best Shot: Training Your Staff to Give Safe Injections · PDF file1 Your Best Shot:...
31
1 Your Best Shot: Training Your Staff to Give Safe Injections Emily Lutterloh, MD, MPH Director, Bureau of Healthcare Associated Infections, NYSDOH and Ernest J. Clement, RN, MSN, CIC Epidemiologist/Infection Preventionist, Bureau of Healthcare Associated Infections, NYSDOH Program Sponsors New York State Department of Health Empire State Public Health Training Center University at Albany, School of Public Health 2
Transcript of Your Best Shot: Training Your Staff to Give Safe Injections · PDF file1 Your Best Shot:...

1
Your Best Shot: Training Your Staff to
Give Safe InjectionsEmily Lutterloh, MD, MPH
Director, Bureau of Healthcare Associated Infections, NYSDOH
and
Ernest J. Clement, RN, MSN, CIC
Epidemiologist/Infection Preventionist,Bureau of Healthcare Associated Infections, NYSDOH
Program Sponsors
New York State Department of Health
Empire State Public Health Training Center University at Albany, School of Public Health
2

2
Program Guidelines No Sound? Make sure your computer speakers/ sound
is turned on! You may have to turn up the volume.
If you experience any technological problems during the program, try exiting and logging in again.
This program will be recorded and available for on demand viewing within 1 week.
Contact info: [email protected] / 518-402-0330
3
Handouts & CEs
http://www.empirestatephtc.org/events.cfm
View and print handouts
CME, CNE, CECHs credits
evaluation and post-test required
Viewing as a group?
Please submit sign in sheet via fax 518-402-1137 or email [email protected]
4

3
Click here to submit a question
Questions & Answers at end of program
Program Goal
To provide safe injection practices information and resources that can be incorporated into
patient safety and infection control staff education activities.
6

4
Program Objectives
Identify five components of an effective safe injections case study used as part ofstaff training.
Identify one to three disciplines within the learner’s institution or practice setting that could benefit from safe injection education.
Identify four resources the learner could use as part of a safe injections training program in their facility.
7
What is Injection Safety?
A safe injection prevents: Harms such as needlestick injuries Transmission of infectious diseases between
patients and between healthcare providersand patients
A safe injection does not: Harm the patient Expose the provider to any avoidable risks Result in waste that is dangerous
for the community.
8

5
What are Some Examples ofUnsafe Injection Practices?
Using the same syringe to administer medication to more than one patient, even if the needleis changed.
Accessing a medication vial with a syringe that has already been used to administer medication to a patient and then using medication from that vial for other patients.
Accessing a bag of IV fluid with a syringe that has already been used to flush a patient's IV catheter and then using the same bag as a common source of IV flush for more than one patient.
9
Source: CDC Injection Safetyhttp://www.cdc.gov/injectionsafety/
Myths & Facts I
Myth
Changing the needle makes a syringe safe for re-use
Syringes can be reused as long as injection is given through an intervening length of tubing
Fact Once used, both needle and
syringe are contaminated and must be discarded. Microscopic backflow into the syringe can occur when removing the needle.
Everything from the IV bag to the patient's IV catheter is a single, interconnected unit. Distance from patient, gravity, or infusion pressure do not ensure syringe won’t be contaminated
10

6
Myths & Facts II
Myth No visible blood in IV
tubing or syringe means the equipment is safe for reuse.
Single-dose vials with large volumes that appear to contain multiple doses can be used for more than one patient.
Fact
HBV, HCV, and HIV can be present in sufficient quantities to produce infections without visible blood.
Single-dose vials should not be used for more than one patient regardless of vial size or volume.
11
Case Study 1: Sharing syringes between patients
New nursing graduate just off orientation
Working on the night shift
Needleless system and pre-filled saline syringes for flushing IV lines
12

7
Case Study 1: Sharing syringes between patients
Staff noticed used saline flush syringes lying on medication cart
During orientation there was no improper use of saline syringes observed
13
Case Study 1: Sharing syringes between patients
The facility interviewed the nurse abouther practices Concern about re-use of the syringes
Nurse could not say syringes were never shared between patients
The facility decided to notify patients
Over 200 patients recommended to be tested for HBV, HCV, and HIV
14

8
Five Components of an Effective Safe Injection Case Study
Infection control breach What went wrong?
Root cause Why did it go wrong?
Barrier(s) to correct procedure What contributed to the breach? What could have been done to stop it?
Sequelae (potential or actual) What harm was done?
Corrective Actions How can patient harm be mitigated? How can similar breaches be prevented in the future?
15
Case Study 1: What was the breach?
Sharing syringes between multiple patients
16

9
Case Study 1: What was the root cause?
Unclear, possibilities include:• Nursing education and/or orientation might not have
included safe injection procedures• Taught what to do but not what not to do and why?; lack of
awareness of written procedures?
• Belief in myths regarding the potential for syringe contamination
• e.g., myths about lack of contamination if no back pressure on plunger, no aspiration, no needle, injection into IV tubing, etc.?
• Syringes used for flushing contained more saline than needed for task?
• Pressure to conserve resources?17
Case Study 1: Were there barriers to performing
the correct procedure?
None identified, possibilities include: Lack of appropriate supplies?
Lack of understanding of supply acquisition?
Difficult or inconvenient to obtain supplies?
18

10
Case Study 1: What are the sequelae?
Potential cross-contamination between patients (e.g. bacteria, bloodborne viruses)
Disciplinary action against healthcare provider (loss of employment, potential actionsagainst license)
Lawsuits
Negative press
Loss of trust in healthcare by consumers
19
Case Study 1: What are some potential
corrective actions?
Include safe injection practices education in basic nursing education and facility orientation programs.
Incorporate injection safety competencies into evaluations.
Instruct what to do, and what not to do.
20

11
Why Case Studies?
Connecting to real-life situations adds impact Audiences may relate to clinical scenarios
Knowing the recommendations may not always translate into correct clinical practice Need to bridge the gap between general
recommendations and specific daily practice
Examples may help
Important to understand consequencesof unsafe practice
21
Why Case Studies?
Large volume vials Everyone knows single use means for one patient
only, but staff using a large volume vial of medication may assume it is multi-use
22
when it is actually single-use

12
Why Case Studies?
We all know that reusing a syringe on another patient is wrong, even if there is no needle or the needle is changed. Everyone knows this… right?
23
For use by one patient multiple times, not for multiple patients
Why Case Studies?
Staff may not realize that insulin pens are really syringes with removable needles
24

13
Case Study 2: IV Bag as Common Source of Flush
Nebraska, September 2002 Four patients diagnosed with HCV
Cluster reported by a gastroenterologist to Nebraska Department of Health
All patients had received cancer chemotherapy at one clinic
All had HCV genotype 3a
25Macedo de Oliveira, et al. Ann Int Med 2005;142:898-903
Case Study 2: IV Bag as Common Source of Flush
Clinic independently owned and operated within a hospital complex Approximately 500 patients per month
One oncologist, a registered nurse, a certified nurse assistant, and a secretary
26Macedo de Oliveira, et al. Ann Int Med 2005;142:898-903

14
Case Study 2: IV Bag as Common Source of Flush
Epi investigation revealed No active infection control program
RN responsible for all central venous catheter (CVC) care, medication administration, and blood collection Reused disposable syringes to withdraw saline solution
from 500-ml bags (potentially used for 25-50 patients) after withdrawing blood from central venous catheters
Hospital and clinic notified of infection control concerns in February and April 2001.
27
Case Study 2: IV Bag as Common Source of Flush
RN dismissed for infection control breaches in July 2001 (19 mos prior to outbreak identification)
Physician oversight of practices
28

15
Case Study 2: IV Bag as Common Source of Flush
Investigators reviewed records of 367 patients treated at the clinic between March 2000 and July 2001
99/367 HCV positive 95/99 (96%) had detectable virus (genotype 3a)
All 99 had CVC flushes on the same days as one patient with prior history of HCV (genotype 3a)
Only 20 exhibited clinical signs of HCV
2/99 spontaneously cleared HCV
29
Case Study 2: What was the breach?
Using IV bag of fluid as a common source for multiple patients
30
“Single dose container”

16
Case Study 2: What was the root cause?
Unclear, possibilities include:• High volume clinic with one RN?
Pressure to cut corners related to high through-put in the clinic (trying to save time, resources, etc.)?
• Lack of sufficient oversight of professional staff?
• Belief in myths regarding the potential for syringe contamination (e.g., no visible blood = no contamination)?
31
Case Study 2: Were there barrier(s) to the
correct procedure?
None identified, possibilities include: Lack of appropriate supplies (e.g., vials of normal
saline for flushing IVs)?
32

17
Case Study 2: What were the sequelae?
Spread of HCV to multiple patients and deaths related to HCV Disciplinary action against healthcare providers (loss of employment, loss of license)Clinic voluntarily closed October 2002
(1 month after outbreak identification)
Lawsuits Negative press Loss of trust in healthcare by consumers
33
Case Study 2: What are some corrective actions?
Establish and maintain an effective infection control program
Include safe injections in infection control training upon hire and at least annually thereafter Include examples pertinent to audience’s practice
Monitor the practice of those under your supervision
Have a mechanism to recognize and address infection breaches in a timely manner
34

18
Examples of Investigations Related to Unsafe Injections
Investigation Practice Setting Professions Involved
Sharing insulin pens Acute (3) and long term care (1) facilities
Nursing
Sharing diabetes care equipment without appropriate reprocessing
Long term psychiatric care facility,Adult care facility
Nursing
Reusing contaminated multi‐use vials
Pain management clinic MD (anesthesia)
Flu vaccine syringe reuse Private practices (3) MD (1 OB/GYN, 2 GP)
Allergy skin testingneedle reuse
Clinic affiliated with hospital
MD (fellow)
Inadequate med prep area Dialysis facility MD (renal), Nursing
Improper storage ofinjection equipment
Private practice MD (dermatology), Nursing
IV tubing reuse Hospital (2) Nursing35
36

19
Excuses for Unsafe Injections
We all know not to re-use needles. What’s the big fuss?
My colleagues all do it like this, so it must be okay.
That’s just something the government bureaucrats tell us to do, but no one really does it.
That’s not how I trained.
It’s wasteful and expensive; I can’t afford it.
You can’t really transmit hepatitis that way!
The policies in place when I came here say to do itthis way, so it must be okay.
37
Pictures from Investigations
38

20
Pictures from Investigations
39
Pictures from Investigations
40
Opened, unlabeled vials ready for use on next patient left unattended in an exam room
21
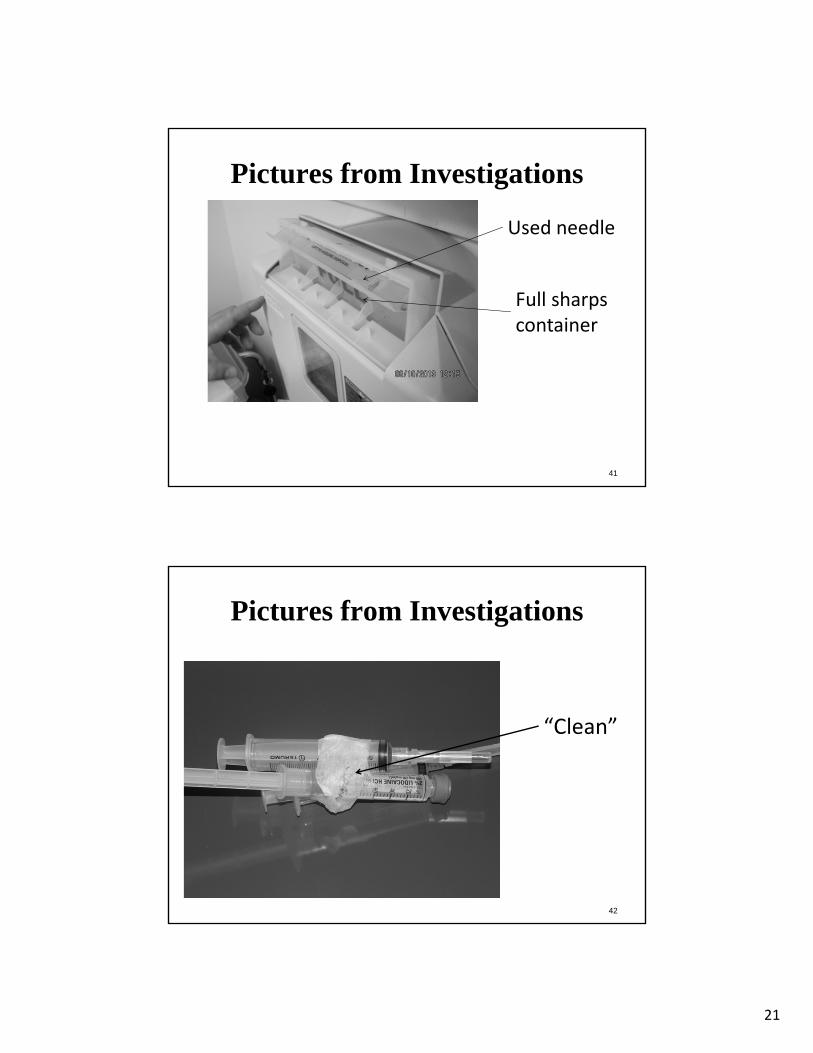
Pictures from Investigations
41
Used needle
Full sharps container
Pictures from Investigations
42
“Clean”

22
Pictures from Investigations
43
“flu vaccine” syringe with 1‐ml of fluid
Pictures from Investigations
44
Medication vial stored in refrigerator with staff food

23
Pictures from Investigations
45
Single‐dose vial of propofol with vented spike for use on multiple patients
ResourcesNYS One & Only Campaign Partner Website http://www.oneandonlycampaign.org/partner/new-york
Healthcare provider andpatient education materials
Newsletter and links to recent alerts and advisories regarding safe injections
46

24
One & Only Campaign Educational Materials
47
Resources
Centers for Disease Control and Prevention: Injection Safety Website
http://www.cdc.gov/injectionsafety/
48

25
Resources
CDC: Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings, 2007 http://www.cdc.gov/hicpac/pdf/isolation/Isolation2007.pdf
Contains recommendations for safe injection practices with references
49
Resources
CDC: Recommended Practices for Preventing Bloodborne Pathogen Transmission during Blood Glucose Monitoring and Insulin Administration in Healthcare Settings
http://www.cdc.gov/injectionsafety/blood-glucose-monitoring.html#Recommended
50

26
Resources
US Food and Drug Administration (FDA) -
Information for Healthcare Professionals: Risk of Transmission of Blood-borne Pathogens from Shared Use of Insulin Pens
http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/DrugSafetyInformationforHeathcareProfessionals/ucm133352.htm
51
References
52
Case/Outbreak Reports:
Bacterial ContaminationAbe K et al. Outbreak of Burkholderia cepacia bloodstream infection at an
outpatient hematology and oncology practice. ICHE 2007;28:1311-1313. Cohen AL et al. Outbreak of Serratia marcescens bloodstream and central
nervous system infections after interventional pain management procedures. Clin J Pain 2008;24:374-380
Groshskopf LA et al. Serratia liquefaciens Bloodstream Infections from contamination of epoetin alfa at a hemodialysis center. NEJM2001;344:1491-1497.

27
References
Diabetes Testing
Centers for Disease Control and Prevention. Notes from the field: Deaths from acute hepatitis B virus infection associated with assisted blood glucose monitoring in an assisted-living facility – North Carolina, August-October 2010. MMWR 2011;60:182.
Centers for Disease Control and Prevention. Transmission of hepatitis B virus among persons undergoing blood glucose monitoring in long-term-care facilities–Mississippi, North Carolina, and Los Angeles County, California, 2003-2004. MMWR 2005;54:220-223.
Farkas K, Jermendy G. Transmission of hepatitis B infection during home blood glucose monitoring. Diabetic Medicine 1997;14:263.
53
References
Diabetes Testing (continued)
Gotz HM, et.al. A cluster of hepatitis B virus infections associated with incorrect use of a capillary blood sampling device in a nursing home in the Netherlands, 2007. Eurosurveillance 2008;13:1-5.
Polish LB, et al. Nosocomial transmission of hepatitis B virus associated with a spring-loaded finger-stick device. N Engl J Med 1992;326:721-5.
Stapleton J. Transmission of hepatitis B during blood glucose monitoring. JAMA 1985;253:3250.
54

28
References
55
Medication handlingBennett SN et al. Post-operative infections traced to contamination of an
intravenous anesthetic, propofol. NEJM 1995;333:147-154.Comstock RD et al. A large nosocomial outbreak of hepatitis C and hepatitis B
among patients receiving pain remediation treatments. ICHE 2004;25:576-583.
Fischer GE et al. Hepatitis C virus infections from unsafe injection practices at an endoscopy clinic in Las Vegas, Nevada, 2007-2008. CID 2010;51:267-273.
Gutelius B et al. Multiple clusters of hepatitis virus infections associated with anesthesia for outpatient endoscopy procedures. Gastroenterology2010;139:163-170.
Macedo de Oliveira A et al. An outbreak of hepatitis C virus infections among outpatients at a hematology/oncology clinic. AIM 2005;142:898-903.
Samandari T et al. A large outbreak of hepatitis B virus infections associated with frequent injections at a physician’s office. ICHE 2005;26:745-750.
References
Contamination of syringes/blood glucose equipment:
Hughes RR. Syringe contamination following intramuscular and subcutaneous injections. J R Army Med Corps 1948;87:156-68.
Louie RF, Lau MJ, Lee JH, et al. Multicenter study of the prevalence of blood contamination on point-of-care glucose meters and recommendations for controlling contamination. Point of Care 2005;4:158-163.
Lutz CT, Bell CE Jr, Wedner HJ, Krogstad DJ. Allergy testing of multiple patients should no longer be performed with common syringes. N Engl J Med 1984;310:1335-7.
Plott RN, Wagner RF Jr, Tyring SK. Iatrogenic contamination of multidosevials in simulated use: a reassessment of current patient injection technique. Arch Dermatol 1990;126:1441-4.
Trepanier CA, Lessard MR, Brochu JB, Denault PH. Risk of cross infection related to the multiple use of disposable syringes. Can J Anaesth1990;37:156-9.
56
29
ReferencesGuidelines/Recommendations
Thompson ND et al. Nonhospital health care-associated hepatitis B and C virus transmission: United States, 1998-2008. Ann Intern Med2009;150:33-39.
Thompson ND, Perz JF. Eliminating the blood: Ongoing outbreaks of hepatitis B virus infection and the need for innovative glucose monitoring techniques. J Diabetes Sci Technol 2009;3(2):283-288.
Klonoff DC, Perz JF. Assisted monitoring of blood glucose: Special safety needs for a new paradigm in testing glucose.J Diabetes Sci Technol 2010;4(5):1027-1031
57
ReferencesEnvironmental survival of hepatitis viruses
Alfurayh O. et al. Hand contamination with hepatitis C virus in staff looking after hepatitis C-positive hemodialysis patients. Am J Nephrol 2000;20:103-106.
Bond WW, Favero MS, Petersen NJ, et al. Survival of hepatitis B virus after drying and storage for one week. Lancet 1981;1(8219):550-1.
Ciesek S et al. How stable is the hepatitis C virus (HCV)? Environmental stabilityof HCV and its susceptibility to chemical biocides. JID 2010:201 (15 June);1859-1866
Doerrbecker J et al. Inactivation and survival of hepatitis C virus on inanimate surfaces. J ID 2011:204(15 December);1831-1838.
Kamili S et al. Infectivity of hepatitis C virus in plasma after drying and storing at room temperature. Infect Control Hosp Epidemiol 2007;28:519-524
Paintsil E et al. Survival of hepatitis C virus in syringes: Implication for transmission among injection drug users. JID 2010:202(1 October);984-990
58

30
Click here to submit a question
Questions?
Handouts & CEs
http://www.empirestatephtc.org/events.cfm
View and print handouts
CME, CNE, CECHs credits
evaluation and post-test required
Viewing as a group?
Please submit sign in sheet via fax 518-402-1137 or email [email protected]
60

31
Thank you!!
This program has been recorded and will be available for on demand viewing within 1 week at: http://www.empirestatephtc.org/events.cfm
61