Yes, Materi 16 Januari 2013
42
Outpatient Management of Premature Infants Hartono Gunardi Dept of Child Health, FKUI-RSCM
-
Upload
hendra-setyawan -
Category
Documents
-
view
219 -
download
0
Transcript of Yes, Materi 16 Januari 2013

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 1/42
Outpatient Management of Premature Infants
Hartono Gunardi
Dept of Child Health, FKUI-RSCM
7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 2/42
Objectives
• Screening
•Monitoring premature infants• Intervention
•Morbidities

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 3/42
• National ~ 9%
• Premature/LBW prevalence in RSCM, Jakarta :
1998 : 17.8%
2008 : 26.8%
• Advances in neonatal care allow prematureinfants prone to a range of long termcomplications.
Premature infants
United Nations Statistics Division. The State of the World’s Children 2009.Perinatologi FKUI-RSCM. 2009.
7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 4/42
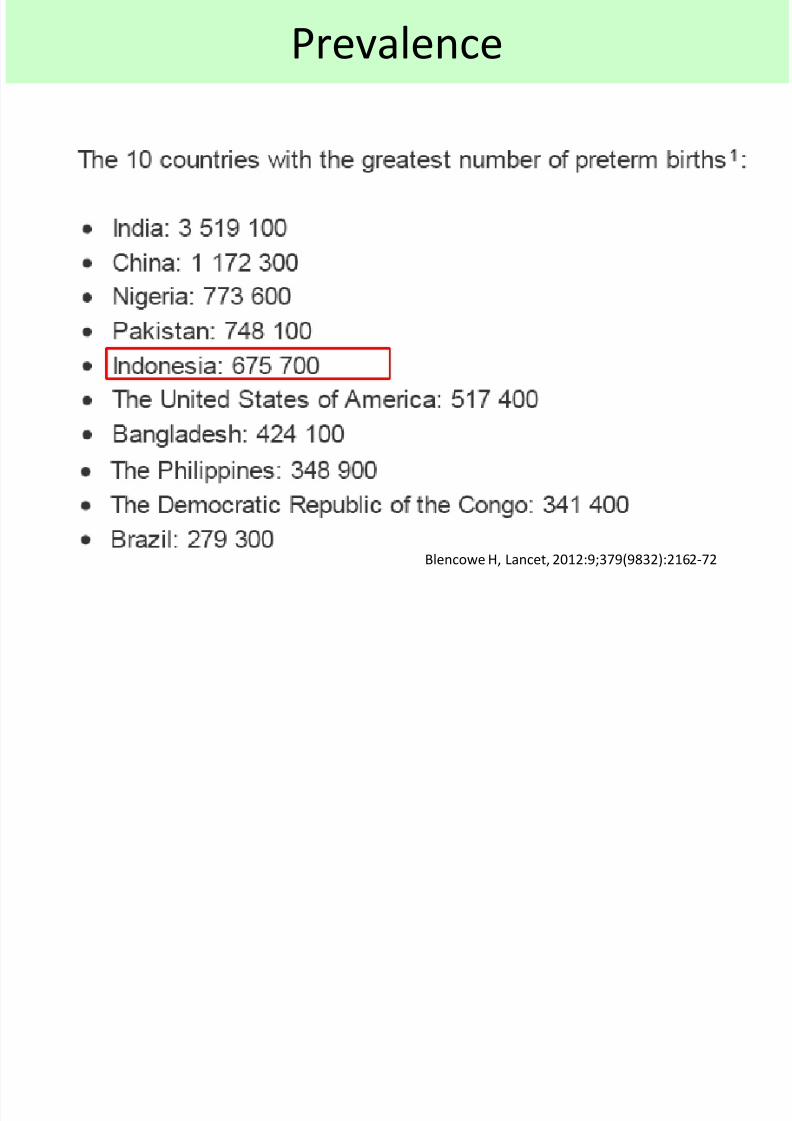
Prevalence
Blencowe H, Lancet, 2012:9;379(9832):2162-72
7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 5/42
• Depends : gestational age, birth weight,
perinatal insults, etc
•
Risk : growth failuredevelopmental problem (e.g.cerebral palsy)
vision and hearing losses
needs growth & development monitoring
Outcome premature infants

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 6/42
Growth Development
• Greater weight gain before reaching term appears tobe associated with improved neurodevelopmental
outcome.
• Study of 613 infants ( GA < 33 wks) that
greater weight gain,
BMI, before 40 wks PMA
head growth (term)
higher Bayley MDI and PDI scores at 18 months
CA
Belfort MB,et al. Pediatrics 2011; 128:e899.
7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 7/42
Eye & hearing screening
7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 8/42
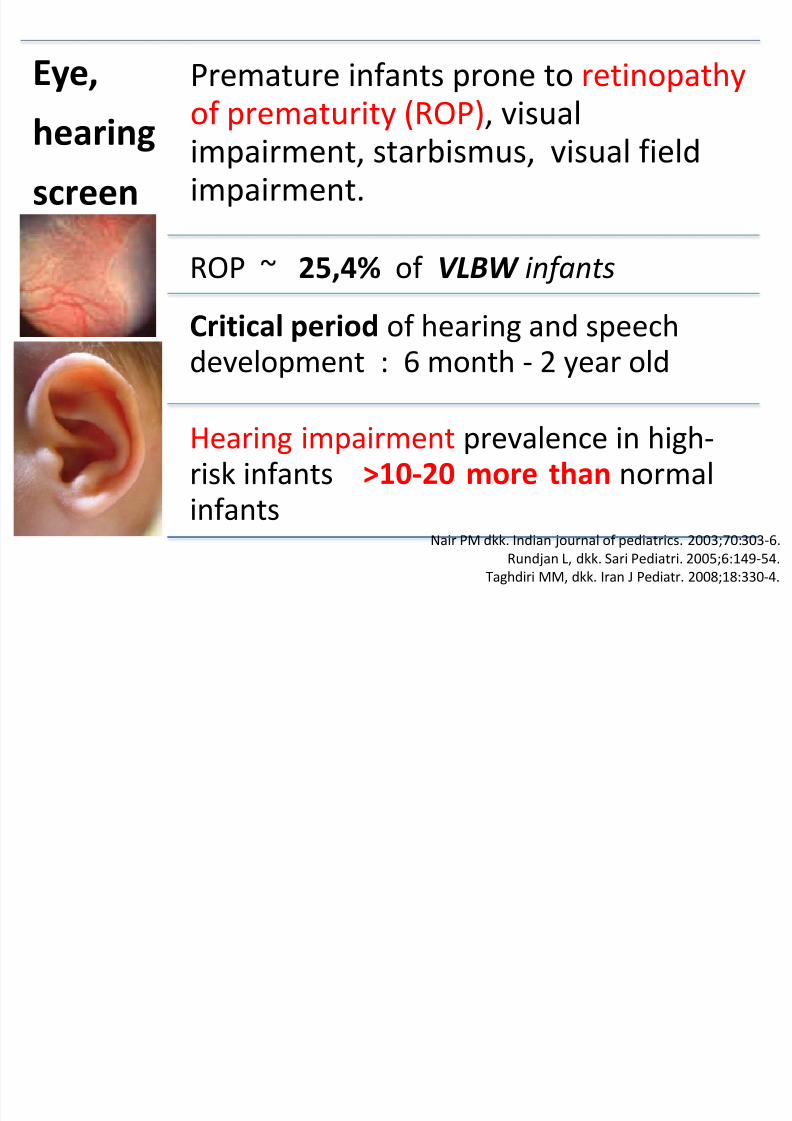
Eye,
hearingscreen
Premature infants prone to retinopathyof prematurity (ROP), visual
impairment, starbismus, visual fieldimpairment.
ROP ~ 25,4% of VLBW infants
Critical period of hearing and speechdevelopment : 6 month - 2 year old
Hearing impairment prevalence in high-risk infants >10-20 more than normalinfants
Nair PM dkk. Indian journal of pediatrics. 2003;70:303-6.
Rundjan L, dkk. Sari Pediatri. 2005;6:149-54.
Taghdiri MM, dkk. Iran J Pediatr. 2008;18:330-4.
7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 9/42
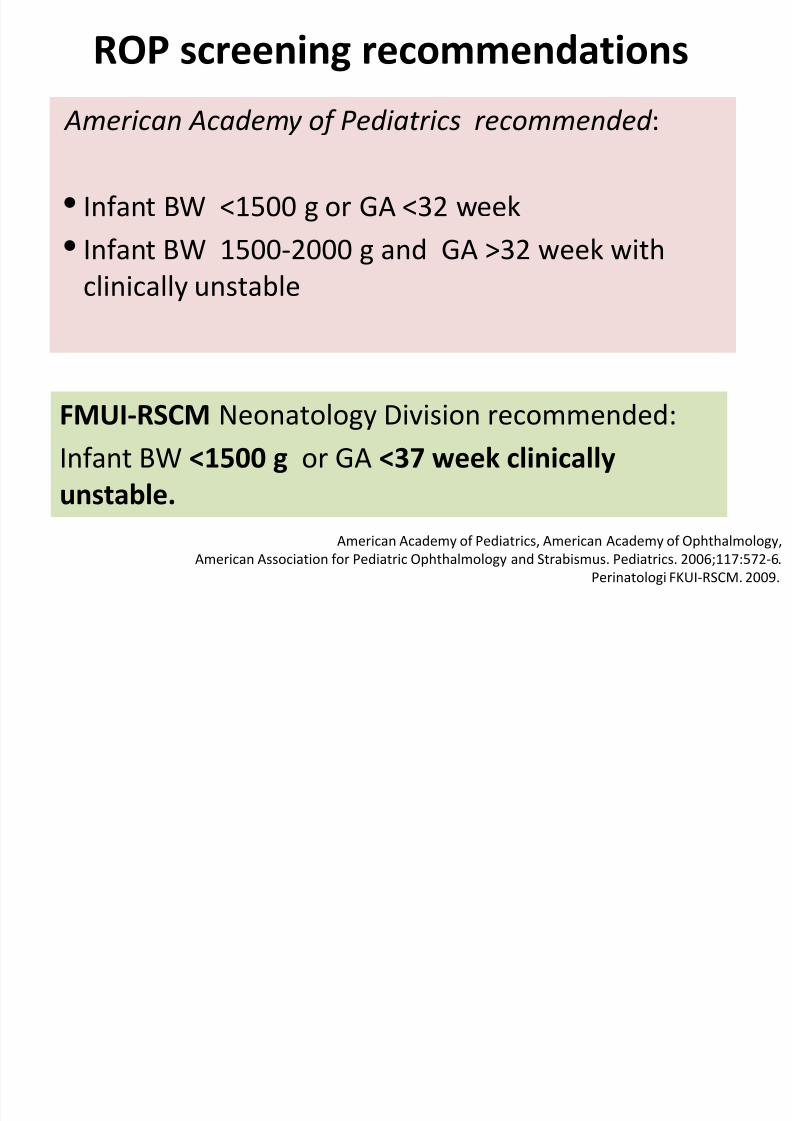
ROP screening recommendations
American Academy of Pediatrics, American Academy of Ophthalmology,
American Association for Pediatric Ophthalmology and Strabismus. Pediatrics. 2006;117:572-6.
Perinatologi FKUI-RSCM. 2009.
FMUI-RSCM Neonatology Division recommended:Infant BW <1500 g or GA <37 week clinically
unstable.
American Academy of Pediatrics recommended :
• Infant BW <1500 g or GA <32 week
• Infant BW 1500-2000 g and GA >32 week with
clinically unstable

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 10/42
Eye screening : when to perform
• First at clinically stable 2 weeks CA or 32-
33 weeks GA (ROP screening)
• Other ophthalmologic abnormalities:reduced visual acuity, strabismus, myopia
Referral to ophthalmology at 6 – 12 months
• Further eye exam : at 1-2 year, 3-4 year, 4-5year, and 5-6 year old
Wang CJ, dkk. Pediatrics. 2006;117:2080-92.
7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 11/42
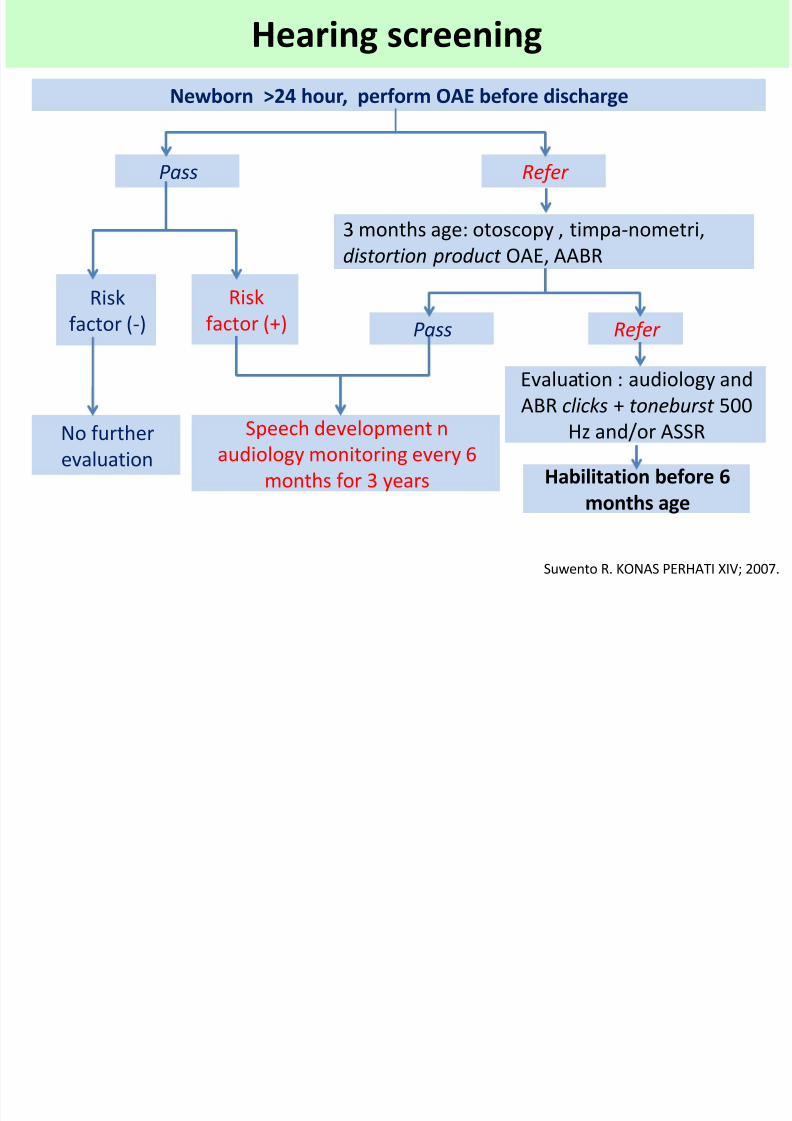
Hearing screening
Suwento R. KONAS PERHATI XIV; 2007.
Newborn >24 hour, perform OAE before discharge
Pass Refer
3 months age: otoscopy , timpa-nometri,
distortion product OAE, AABR
Pass Refer
Risk
factor (-)
Risk
factor (+)
No further
evaluation
Speech development n
audiology monitoring every 6
months for 3 years
Evaluation : audiology and
ABR clicks + toneburst 500Hz and/or ASSR
Habilitation before 6
months age

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 12/42
• Parameters : weight, length, head
circumference
• Schedule : a weekly to biweekly( first 4-6 weeks
after discharge) grows normally : 1st year : monthly, then
1-5 year: every three months,
> 5 year : every 6 months. poor growth : monitor biweekly to monthlyand needs evaluation + intervention.
Growth monitoring

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 13/42
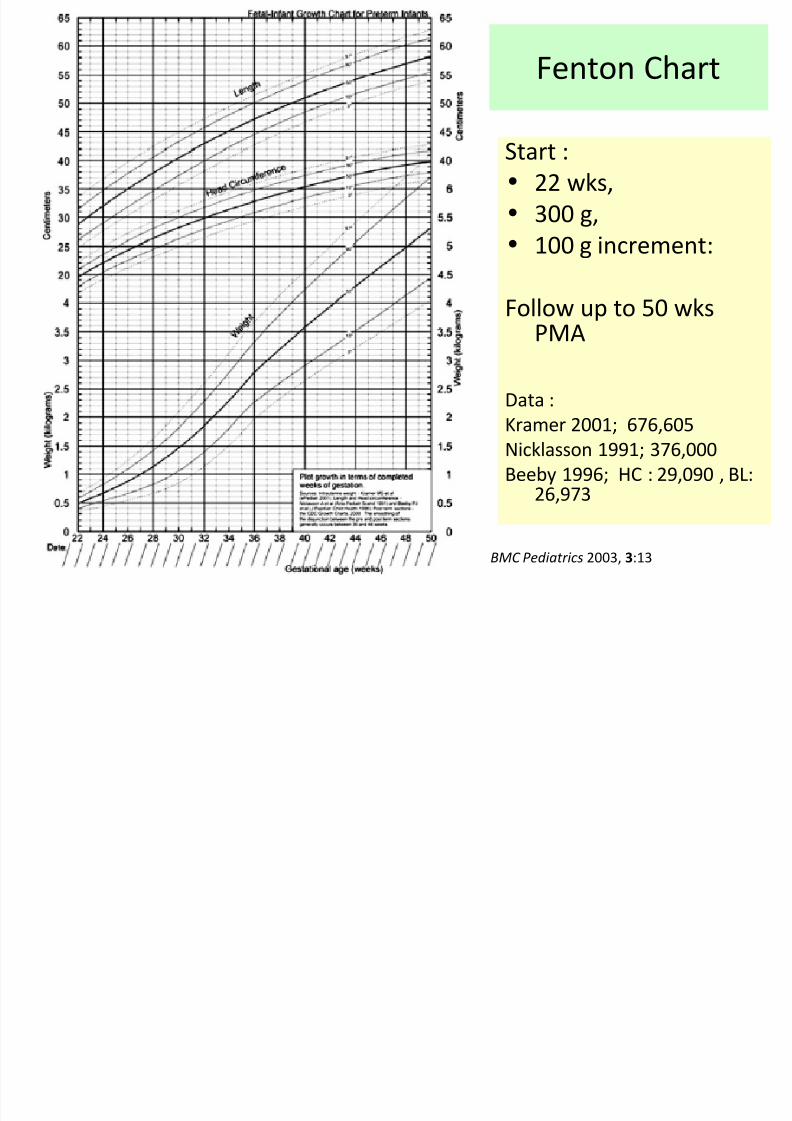
Growth chart for preterm
1. Fenton preterm infant growth
chart (2003)
22 weeks to 50 weeks (PMA)
2. Then : a. WHO growth chart
b. CDC growth chart
Fenton TR. BMC Pediatrics 2003, 3:13
7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 14/42
Start :
• 22 wks,
• 300 g,
• 100 g increment:
Follow up to 50 wksPMA
Data :
Kramer 2001; 676,605
Nicklasson 1991; 376,000
Beeby 1996; HC : 29,090 , BL:26,973
Fenton Chart
BMC Pediatrics 2003, 3:13
7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 15/42
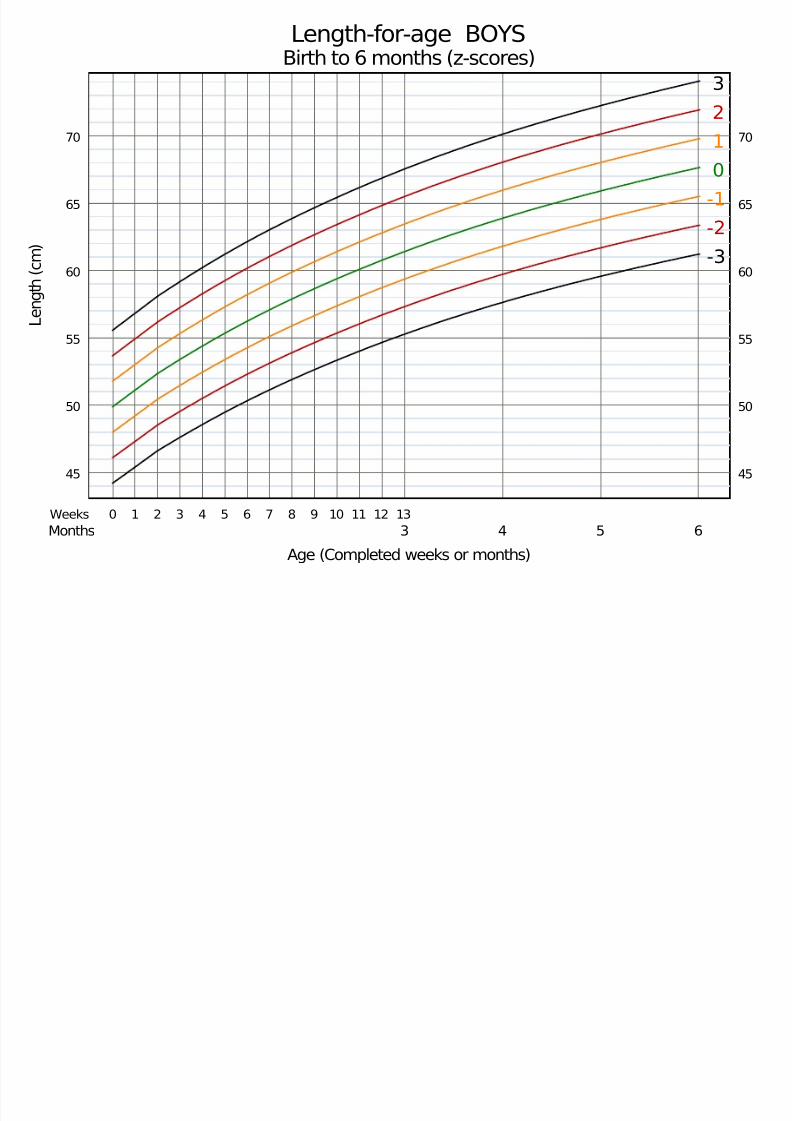
Age (Completed weeks or months)
L e n g t h ( c m )
Length-for-age BOYSBirth to 6 months (z-scores)
-3
-2
-1
0
1
2
3
0 1 2 3 4 5 6 7 8 9 10 11 12 13
3 4 5 6
Weeks
Months
45
50
55
60
65
70
45
50
55
60
65
70
7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 16/42
Corrected age
Corrected age = chronological age−
prematurity
Through 24 months of age
• Eg. A baby, GA 32 week, chronological age 4month.
Corrected age = 4 months – (40-32 weeks)
= 2 months
7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 17/42
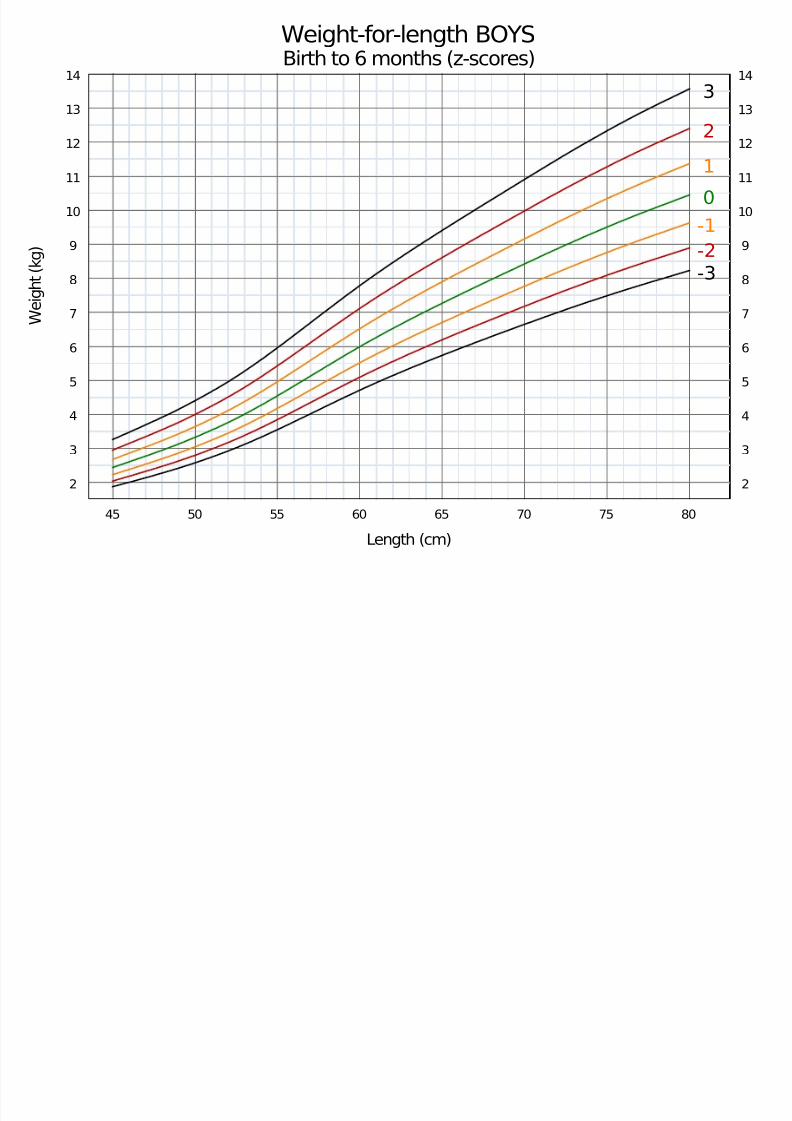
W e i g h t
( k g )
Weight-for-length BOYSBirth to 6 months (z-scores)
Length (cm)
-3
-2
-1
0
12
3
45 50 55 60 65 70 75 80
2
3
4
5
6
7
8
9
10
11
12
13
14
2
3
4
5
6
7
8
9
10
11
12
13
14

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 18/42
Catch up
• 30-80% since birth to adolescence
• Catch-up growth : reaching 5th – 10th
percentile on standard growth chart
(WHO/CDC), mostly first 6 months
• Sequence : head circumference, then weight
and length.
• Individual, and influenced by multifactor.
Paul B, dkk. Indian journal of public health. 2008;52:16-20.
Roggero P, dkk. The journal of maternal-fetal & neonatal medicine. 2011;24 Suppl 1:144-6.Hill AS, dkk Pediatric nursing. 2009;35:181-8.
7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 19/42
Head circumference
•
Slow head growth is ~developmental delay.
• VLBW whose HC < normal at 8 mo CA had :
poor cognitive function
poor academic achievement
poor behavior
compared to controls with normal head size.
• Rapid increase HC: may indicate post hemorrhagic
hydrocephalusHack M, et al. N Engl J Med 1991; 325:231.
at 8 year

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 20/42
Consider cranial US for signs/symptoms
hydrocephalus
– Widely spaced sutures
– Tense fontanel– Irritability
– Alterations in behavior/activity level
–Frequent downward deviation of eyes“sunsetting”
Head circumference
7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 21/42
Developmental monitoring
• Corrected age until 2 year
• Surveillance : at every visit
Kuesioner Pra Skrining Perkembangan
Milestones
Parents Evaluation of Developmental Status
(PEDS)
• Screening : Denver II or Bailey Infant Neurodevelopmental Screener ( BINS)

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 22/42
Source : Denver Prescreening Develop. Questionairre (PDQ)
Age : 3 months – 6 years, duration 10 – 15 minutes
Content : 10 questions for each age groups. Answered by
parents. Yes, if child can do. No, if can not do
Interpretation : Yes < 7 probable delay
yes 7 – 8 repeat next weekyes > 9 generally no delay
Sensitivity : 43 – 75 %
Spesificity : 83 %
KUESIONER PRA SKRINING PERKEMBANGAN

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 23/42

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 24/42

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 25/42
Interventions
• Breast milk
• Kangaroo mother care
•
Fe supplementation• Touch therapy
• Music therapy

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 26/42
Long-term Human Milk Benefits
Patel AL et al. NeoReviews 2007;8;e459-66.
• 300 of the VLBW preterminfants at 7.5 to 8 years of age
Subject
•Higher IQ 8.3-point advantage in IQ (P<0.0001)
• Fewer MDI score of <85(P=0.036)
Outcomes

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 27/42
Kangaroo mother care
• Improved growth and breast feeding rate
• Reduced nosocomial infections
• Higher MDI and PDI scores on the Bayley Scales of
Infant Development-II of 25-34 week preterms on
6 months corrected age
• Higher DQ scores on the Griffiths Mental
Development Scales at 12 months corrected age
Charpak N et al. Pediatrics 2001;108:1072-9.
Feldman R et al. Pediatrics 2002;110:16-26.
Tessier R et al. Infant Behav Dev 2003;26:384-97.

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 28/42
Massage/Touch therapy
• Tactile and kinestetics stimulation
Ferber SG et al. Infant Behav Dev 2005;28:74–81.
Field TM et al. Pediatrics 1986;77:654-8.
Sizub J, Westrup B. Arch Dis Child Fetal Neonatal 2004;89:F384-9.

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 29/42
Massage/Touch therapy
• As a pacifying or stress-
reducing effect promoted
behavioral organization
• Optimized mother–infant
interactions (at 3 months of
age)
• Increased daily weight gain,
and shortened hospital stayFerber SG et al. Infant Behav Dev 2005;28:74–81.
Field TM et al. Pediatrics 1986;77:654-8.
Sizub J, Westrup B. Arch Dis Child Fetal Neonatal 2004;89:F384-9.

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 30/42
Massage/Touch therapy

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 31/42

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 32/42
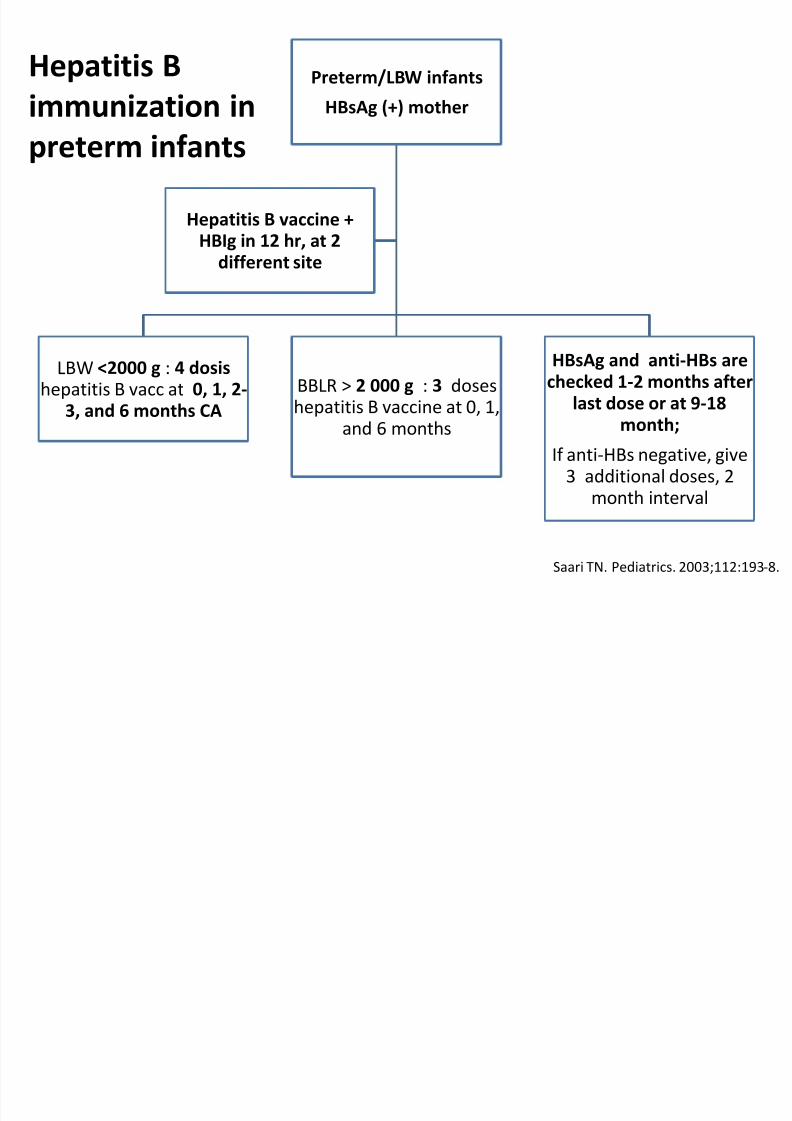
Preterm/LBW infants) less likely
to receive immunizations in atimely fashion (high rates of medical complication)
For immunization =
chronological age
Same schedule,
except hepatitis B
• Same dose
• Immunogenicity, eficacy,tolerability
LBW <2000 g with HBsAg (-)mother : Hep B vaccine at 1-2
month or BW >2000 g
Immunization of high-risk infants
Siregar SP. Pedoman Imunisasi di Indonesia. 2008.
D'Angio CT. Paediatric drugs. 2007;9:17-32.Hendrarto TW. Pedoman Imunisasi di Indonesia. 2008.
7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 33/42

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 34/42
Immunization of Preterm infants
•LBW infants still hospitalized at 2 mo CA: give BCG,DPT, IPV (inactivated polio vaccine) and Hib, PCV
immunization, if clinically stable and no contra
indication.
• No increase of adverse events in preterm infants
• Apnoe might occur in 72 hours (most often in 12-24
hours) after DTPw in ELBW infants with <31 weeks
gestational age.
D'Angio CT, dkk. Pediatrics. 1995;96:18-22.
Khalak R, dkk. Pediatrics. 1998;101:597-603.Botham SJ, dkk. Journal of paediatrics and child health. 1997;33:418-21.
b d
7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 35/42
Morbidities
Cardiovacular : PDA, VSD
Hypertension : BPD, umbilikal artery cath
Respiratory : BPD, recurrent wheeze
GI : GER, colic, constipation
7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 36/42
ANEMIA of PREMATURITY
•
AOP is a normocytic, normochromic,hyporegenerative anemia characterized by a
low serum EPO level.
• AOP typically occurs at 3 to 12 weeks after birth in
infants less than 32 weeks gestation
• Nadir for preterm : Hb 7 – 10 g/dL at 4 – 8 wks;
for term infants : Hb 11 g/dL at 8 – 12 wks
Recommendation of Fe suplementation (IDAI)

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 37/42
0-2 year
2-12 th
Lab
• Preterm/LBW: 3mg/kgBB/day since 1
mo - 2 year• Term infants: 2 mg/kgBB/day
since 4 mo - 2 year
• Infant max dose = 15 mg/day,OD
• 1 mg/kgBB/day, 2x/week for3 months every year
• Hb check annually from 2year until teenager. If anemia, look for etioloogy
Recommendation of Fe suplementation (IDAI)
Ikatan Dokter Anak Indonesia. http://www.idai.or.id/rekomendasi.asp.
7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 38/42
Neurological abnormalities
• Major : Spastic diplegia, hypotonia,
hydrosefalus, microsephaly, mental
retardation
• Minor : Ataxia , coordination problem, specific
learning disorders, ADHD, cognitive
disturbance

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 39/42
•
Surgical problemsIngunal or umbilical hernia,
chryptorchidism, hydrocel
•Psycho-social problems Child abuse and neglect ,
behaviour-emotional problems.
7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 40/42
Growth Development Monitoring : until ?
• American Academy of Pediatrics 1996:
Growth and development of preterm or high-
risk infants should be monitored until 7-10
years.

7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 41/42
Conclusion
• Premature infants are prone to have growth
neurodevelopmental problem.
• Families of premature infants should be
guided to comprehensive follow-up and early
intervention.
• Close monitoring is needed to identify,
stimulate/intervene to have betterneurodevelopmental outcome.
7/28/2019 Yes, Materi 16 Januari 2013
http://slidepdf.com/reader/full/yes-materi-16-januari-2013 42/42
Thank you