Www.TheNationalCouncil.org The NATIONAL COUNCIL for Community Behavioral Healthcare Linda Rosenberg...
60
www.TheNationalCouncil.org The NATIONAL COUNCIL for Community Behavioral Healthcare Linda Rosenberg MSW President and CEO Arizona 2010
-
Upload
evelyn-sanders -
Category
Documents
-
view
215 -
download
0
Transcript of Www.TheNationalCouncil.org The NATIONAL COUNCIL for Community Behavioral Healthcare Linda Rosenberg...

www.TheNationalCouncil.org
The NATIONAL COUNCIL for Community Behavioral Healthcare Linda Rosenberg MSW President and CEO
Arizona 2010

www.TheNationalCouncil.org
This Afternoon…>National Council – Working
on Success>Parity, Technology and
Healthcare Reform
>Behavioral Health Organization Readiness: What’s Needed to Succeed in the New Healthcare
Ecosystem

www.TheNationalCouncil.org
Tipping Point
>Behavioral Health is essential to health
>Prevention/early intervention is possible
>Treatment is effective
>People recover

www.TheNationalCouncil.org
Services are cost effective

www.TheNationalCouncil.org
Lobbying
>US Chamber of Commerce $52,750,000
>General Electric $23,660,000>Pharmaceutical Research & Mfrs of
America $22,733,400>American Medical Assn $22,132,000>American Hospital Assn $19,734,545>AARP $19,540,000

www.TheNationalCouncil.org
Public Policy - Success 2008/09
>Community Mental Health Services Improvement Act – 7 million for primary care into mental health organizations***
>Medicaid Regulatory Moratorium***>Medicare HR 6331 (2010 to 2014)>Second Chance Act and MIOTCRA>Veterans M H Outreach & Access Act>M H Parity & Addiction Equity Act of 2008 >Recovery Act - FMAP

www.TheNationalCouncil.org
Success – Healthcare Reform
Amendments to reform that passed in one or both chambers:> FQBHC (House Energy and Commerce Committee)> Inclusion of therapeutic foster care in Medicaid (Senate Finance Committee) > $50 million authorization for behavioral-primary care integration grants (Senate
HELP Committee)> CMHCs included as eligible providers in Medicaid medical home demonstration
program (Senate Finance Committee)> Mental illness classified as eligible chronic illness for Medicaid medical home
demo (Senate Finance Committee)
> >

www.TheNationalCouncil.org
“Must Haves” for success…
>Broad and strong membership. >Effective communications with
members, media, advocates, policymakers & public.
>Reputation for quality - expert education & practice improvement initiatives.
>Assertive public policy agenda. >Strategic alliances - industry leadership.

www.TheNationalCouncil.org
Membership Growth

www.TheNationalCouncil.org
Summary of 2010 Member Engagement>1,720 members>76% have participated in at
least one activity; 67% in 2009>27% involved in fifteen or more
activities/programs; 14% involved in 20 or more
>24% (410) not involved

www.TheNationalCouncil.org
Highly Engaged Members
> Colorado West (Glenwood Springs, CO)> Meridian Behavioral Healthcare (Gainesville, FL)> NHS Human Services (Lafayette Hill, PA)> Rushford Center, Inc. (Meriden, CT)> Mental Health Center of Denver (Denver, CO)> Oakland County Community MH (Auburn Hills, MI)> Centerstone (Nashville, TN)> The Center for Health Care Services (San Antonio, TX)> Heritage Behavioral Health (Decatur, IL)> Mental Health Center of Boulder and Broomfield
Counties (Boulder, CO)

www.TheNationalCouncil.org
Response to Action Alerts

www.TheNationalCouncil.org
Effective Communications
> Public Policy Update and Alerts > National Council Magazine > Technical Assistance Newsletter> Addictions/Co-occurring Newsletter> Journal of Behavioral Health Services &
Research> Print Media and social media – online
communities, blogging, and tweeting > Annual Conference> Webinars – 1400 lines for
“Understanding Anxiety”;604 for “Contracting with VA” 414 lines for “Accountable Care”

www.TheNationalCouncil.org
National Council LIVE Webinars
Healthcare Reform Implementation Series
Are You Ready to Become a Federally Qualified Health Center (FQHC)?
Thu, August 1212:30 pm eastern, 11:30 am central, 10:30 am mountain,
9:30 am pacific, 8:30 am Alaska

www.TheNationalCouncil.org
Reputation for Quality
>Access and Retention Initiatives>Healthcare Collaborative/Learning
Communities >Workforce: Middle Management
Academy; Psychiatric Leadership Project; CEO University
>Mental Health First Aid

www.TheNationalCouncil.org
Access and Retention
Reduce Waiting Times
Reduce No-Shows
Increase Admissions
Increase Continuation
If you don’t measure it you can’t improve it!

www.TheNationalCouncil.org
Outcomes…
Total Annual Savings: > Produced an average annual savings of
$199,989.43 per CBHO> 34% reduction in staff time> 18% reduction in the client time> 40% reduction in client wait time to treatment> Based on 28 grant CBHOs: Florida (7), Ohio (12), &
Wyoming (9), total annual savings$5,599,703.99
Phase III started in June - 45 organizations in WA, PA & MI

www.TheNationalCouncil.org
Behavioral and Primary Care Learning Communities
>149 pairs of Community Behavioral Health Organizations and Federally Qualified Health Centers serving 98,000 consumers
Outcomes>Screening, detection and treatment of behavioral
health disorders in primary care resulting in increased depression free days
> Increased screening and treatment for physical health issues in CBHOs with improved chronic illness health outcomes - diabetes, heart disease, and COPD
> >

www.TheNationalCouncil.org
Psychiatric Leadership Program
> Executive leadership program for medical directors in community behavioral health organizations.
> One-year comprehensive curriculum designed to develop and enhance leadership and professional development.
> Participation since 2008 – 35 medical directors from agencies that serve more than 420,000 clients each year.

www.TheNationalCouncil.org
Mental Health First Aid USA
> 800+ instructors certified> 10,000 Mental Health First Aiders
• Law enforcement and corrections officers• Primary care workers• School and college workers• Faith community leaders• Mental health/substance use consumers and
families• Caring citizens
> 1,500,000+ media impressions

www.TheNationalCouncil.org
> Parity, technology and reform will trigger dramatic changes in how health and MH/SU services are organized.
> These changes will create a tipping point in how the healthcare needs of persons with serious mental illness and the MH/SU healthcare needs of all Americans are addressed.
> Which will change the way MH/SU services are funded and fit into the new healthcare ecosystem.
Parity, Technology and Healthcare Reform Will Change Everything

www.TheNationalCouncil.org
22
Parity - General Information on Interim Final Regulations
> Apply for plan years beginning July 1, 2010> General rule – parity applies if a plan offers
medical/surgical and MH/SUD benefits (> 50 employees)
> A plan may not apply any financial requirement or treatment limitation to mental health or substance use disorder benefits in any classification that is more restrictive than the predominant financial requirement or treatment limitation for substantially all medical/surgical benefits in the same classification

www.TheNationalCouncil.org
23
Analyzing Plan Benefits
A requirement/limit applies to substantially all medical/surgical benefits in a classification if it applies to at least 2/3 of benefits in the classification -If not, it cannot be applied to MH/SUD benefits
> Example: If 70% of the projected payments for inpatient, in-network medical/surgical benefits were subject to a $15 copay…. then… no inpatient, in-network MH/SUD could be subject to a copay greater than $15
MH/SUD and medical/surgical benefits must accumulate toward the same, combined deductible - separate but equal deductibles are not allowed

www.TheNationalCouncil.org
24
> Definition - Not expressed numerically - list of examples:• -Medical management (e.g., utilization
review, preauthorization, concurrent review, retrospective review, case management, etc.)
• -Prescription drug formulary design• -Standards for provider participation in a
network, including reimbursement rates• -Fail-first or step therapy protocols• -Conditioning benefits on completing a
course of treatment
Non-quantitative Treatment Limitations

www.TheNationalCouncil.org
Health Information Technology
>The Obama Administration made a “down payment” on healthcare reform with the passage of the HITECH Act in 2009.
>Supports the adoption and meaningful use of Health Information Technology

www.TheNationalCouncil.org
Who is a Medicaid Eligible Provider?
Eligible Providers in Medicaid
Eligible Professionals
Physicians
Nurse Practitioners
Certified Nurse-Midwives
Dentists
Physician Assistants working in a Federally Qualified Health Center or rural health clinic that is so led by a PA
Eligible Hospitals
Acute Care Hospitals (now including CAHs)
Children’s Hospitals

www.TheNationalCouncil.org
Incentive Payments for Medicaid EPs
First Calendar Year for which the EP receives Incentive Payment

www.TheNationalCouncil.org
Conceptual Approach to Meaningful Use

www.TheNationalCouncil.org
HIT Extension for Behavioral Health Services Act (HR 5040)
> National Council driven - Introduced in the House on April 15 by Kennedy and Murphy
> Makes psychiatric hospitals, mental health and substance abuse treatment facilities eligible for facility payments
> Adds psychologists & social workers to listHill Day effect:> Currently Have 68 House Co-Sponsors > Introduced in Senate by Sheldon Whitehouse (D-RI), co-
sponsored by Sherrod Brown (D-OH), Al Franken (D-MN), Frank Lautenberg (D-NJ), Jeanne Shaheen (D-NH), and Debbie Stabenow (D-MI).

www.TheNationalCouncil.org
Healthcare Reform and the Behavioral Health Safety Net …We are on the cusp of the second (and most significant) wave of public behavioral health change in the last 25 years.

www.TheNationalCouncil.org
Healthcare Reform’s Four Key Strategies
The second (and most significant) wave of public behavioral health change in the last 25 years.
31

www.TheNationalCouncil.org
Insurance Reform
• Requires guaranteed issue and renewal
• Prohibits annual and lifetime limits• Bans pre-existing condition exclusions• Create essential benefits package that
provides comprehensive services including MH/SU at Parity
• Requires plans to spend 80%/85% of premiums on clinical services
• Creates federal Health Insurance Rate Authority

www.TheNationalCouncil.org
Coverage Expansion
> Requires most individuals to have coverage
> Provides credits & subsidies up to 400% Poverty
> Employer coverage requirements (>50 employees)
> Small business tax credits> Creates State Health Insurance
Exchanges> Expands Medicaid

www.TheNationalCouncil.org
Medicaid Reforms

www.TheNationalCouncil.org
Unmet U.S. Mental Health Needs
Source: Unmet Mental Healthcare Needs in the Health and Behavioral Healthcare Safety Net

www.TheNationalCouncil.org
National Healthcare Reform Strategies - the MH/SU Safety NetThe underfunding problem is even greater in Substance Use• In Treatment: 2.3 million
• Not in Treatment: 23 million
How do we even begin to address these gaps asstates and health plansrealize they have to provide SU servicesat parity?
In Treatment ~2.3 million
“Abuse/Dependence” ~23 million
“Unhealthy Use” ?? million
Little/No Substance Use

www.TheNationalCouncil.org
Coverage Expansion: Most Members of the Safety Net Will Have Coverage Including SUDs & MH
37
Impact of U.S. Health Reform on Coverage for Non-ElderlySenate Finance Committee Reform Bill
Current Reform Reform ReformLaw 2019 Impact Total Impact(Millions) (Millions) (Millions) %
Medicaid/CHIP 35 15 50 43%Private/Other Insured 193 16 209 8%Covered Non-Elderly 228 31 259
> $15 to $23 billion more spending for MH/SU from insurance expansion
• 15 Million increase in Medicaid enrollees (43%)
• 16 Million increase in Privately Insured
Senate Healthcare Reform Bill 2019Medicaid & SCHIP Expansion $87,000,000,000Healthcare Exchange Subsidies $106,000,000,000Total Expansion Funding $193,000,000,000
Behavioral Health Spending @ 8% $15,440,000,000Behavioral Health Spending @ 10% $19,300,000,000Behavioral Health Spending @ 12% $23,160,000,000

www.TheNationalCouncil.org
Expected Effect of Health Care Reform Legislation on Arizona Coverage Rates
> 81,095 people in Arizona who were previously uninsured are newly eligible and expected to enroll in Medicaid
> That is a reduction in Arizona’s uninsured rates of 13.6%

www.TheNationalCouncil.org
Expected Effect of Health Care Reform Legislation on Arizona Coverage Rates

www.TheNationalCouncil.org
Service Delivery Redesign and Payment Reform
> $700 Billion Question: Will the current legislative and regulatory tools at our disposal be enough to improve the health status of Americans and bend the cost curve?
> MH/SU Question: Is the answer to the above question the same for Americans with mental health and/or substance use disorders?

www.TheNationalCouncil.org
Healthcare Reform: Root Cause Analysis
> Wrong incentives and many disincentives that lead to:• Lack of Access • Overuse of unnecessary, high cost tests and procedures• Underuse of prevention, primary care and behavioral health services• Medical errors
> As much as 30 percent of costs (over $700 billion per year) can be eliminated without reducing quality

www.TheNationalCouncil.org
Emerging Delivery System and Payment Reform Models
Where the U.S. Healthcare System is headed (at a glance)
Increase Preventive Care
Promote Early Intervention
Improve the Coordination of Care
Expand the use of Evidence-Informed Care
Decrease Overuse and Underuse of Services
Reduce Error Rates
Institute for Healthcare Improvement Triple Aim- Improve the Health of the Population- Enhance Patient Experience (quality, access, reliability)- Reduce (or at least) Control Costs
42
Person Centered
HC Homes
Inpatient: Reducing Errors & Waste

www.TheNationalCouncil.org
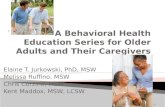
> Need to invert the Resource Allocation Triangle
> Primary Care must become a desirable occupation and…
> Decrease demand in the specialty and acute care systems
Acute Care
Specialty Care
Prevention, Primary
Care
Current Resource Allocation
Prevention & Primary Care
Specialty Care
Acute Care
Needed Resource Allocation
Payment Reforms

www.TheNationalCouncil.org
Payment reforms linked to demonstrating outcomes - managing costs
The payor environment:> Medicare already federal incubator of design changes
(Medical Home pilots underway)> Commercial and self-insured plans (Boeing, GHC, Aetna, United
Health) running Medical Home pilots> Insurance Exchanges, larger Medicaid programs, and new Dual
Eligible (Medi-Medi) plans will be state incubators of changesQuestions…> How will Medicaid programs implement parity and medical
homes?> How many Dual Eligible Plans develop?> Will MH/SU providers be on Exchange and Dual Eligible
Provider Networks?
Payment Reforms

www.TheNationalCouncil.org
Payment Reforms - 1915 (i)
Patient Protection & Affordable Care Act improve option
> State plan services now covered that were previously only available through 1915 (c) and 1115 waivers. No longer tied to “cost neutrality.”
> Increases income to 300% of FPL> Allows states to target to specific populations,
like persons with psychiatric disabilities. > Must be developed through a person-centered
process-beneficiaries, can self-direct their services
> Patient Protection Act added category of services of “other” allowing broader range of interventions.

www.TheNationalCouncil.org
> Fee for Service is headed towards extinction> FFS layer shrinking over time> Being replaced with case rate or capitation with a pay
for performance layer
46
Value-Based Purchasing – Medical Homes/Accountable Care Orgs
Case Rate
Fee for Service/PPS
Bonus
· Prevention, Early Intervention, Care Management for Chronic Medical Conditions
· Per Service Payment· Prospective Payment System (PPS)
Settlement (FQHC model) to cover shortfalls
· Share in Savings from Reduced Total Healthcare Expenditures (bending the curve)
Person Centered
HC Homes

www.TheNationalCouncil.org
> Congress and CMS: ACO have at least one hospital, minimum of 50 physicians (primary & specialists), be in business at least 3-5 years, serve at least 5,000 patients• If ACO met pre-established quality goals, it would
receive an incentive payment• Penalties assessed if care didn’t meet quality goals • Incentive payments and penalties split between
members of the ACO• Providers in ACO to follow best practices, be
patient-centered & contribute to best clinical practices to build evidenced-based medicine standards
Accountable Care Organizations (ACOs)

www.TheNationalCouncil.org
> ACOs to analyze patient experiences across a population and inform quality improvement strategies• Vertical integration of primary care, specialty, hospital
providers who share risk for quality and total healthcare costs> ACOs achieve this by addressing 3 barriers
• Tackle fragmented payment/delivery systems by fostering local, organizational accountability for continuum of care including outcomes, quality and costs
• Focus provider payments on improved health outcomes, better quality, and reduced costs
• Support patient choice by providing information on treatment risks and benefits
> MH/SU providers must prepare to be a part of ACOs and advocate for bi-directional integration
Accountable Care Organizations (ACOs)

www.TheNationalCouncil.org
> Ongoing Relationship with a PCP
> Care Team who collectively take responsibility for ongoing care
> Provides all healthcare or makes Appropriate Referrals
> Care is Coordinated and/or Integrated
> Quality and Safety are hallmarks
> Enhanced Access to care is available
> Payment appropriately recognizes the Added ValueSee the www.pcpcc.net site for more information
49
Patient Centered Medical/Healthcare Homes Principles

www.TheNationalCouncil.org
New Paradigm - Primary Care in Behavioral Health OrganizationsFunding starting to open up for embedding primary medical care into CBHOs, a critical component of meeting the needs of adults with serious mental illness
50
Clinical Design for Adults with Low to Moderate and Youth with Low to
High BH Risk and Complexity
Primary Care Clinic with Behavioral
Health Clinicians
embedded, providing
assessment, PCP
consultation, care
management and direct
service
Partnership/Linkage with
Specialty CBHO for persons who need their care stepped up to
address increased risk and complexity with ability to step back to Primary Care
Clinical Design for Adults with Moderate to High BH Risk and
Complexity
Community Behavioral Healthcare Organization with an embedded
Primary Care Medical Clinic with ability to address the full range of
primary healthcare needs of persons with moderate to high
behavioral health risk and complexity
Food Mart
CBHOFood MartCBHO

www.TheNationalCouncil.org
New Paradigm – Financing Specialty Behavioral Health
> FQBHC status creates single set of national standards that can serve as a blueprint for the types of services and infrastructure that need to be in place to better support the full healthcare needs of persons with serious mental health and substance use disorders
> In addition, the FQBHC designation creates a single, common platform of assumptions, approaches, and expectations for FQHCs and FQBHCs to partner in providing person-centered healthcare homes
> The ability to achieve FQBHC designation and the accompanying financial benefits are necessary for Community Behavioral Healthcare Organizations to be able to adapt to the changes that will occur in healthcare system 51

www.TheNationalCouncil.org
What We Can Do
>There is one critical thing you must all do to be ready for healthcare reform – you have to be at the table for the discussions taking place in your communities, states and at the national level. If behavioral healthcare providers and stakeholders don’t succeed in that task, your consumers, your organization and the overall healthcare system may suffer.”

www.TheNationalCouncil.org
Be At The Table> Actively Pursue Relationship-Building with leaders in the
healthcare community – Hospital CEO, Health Plans, Multi-Specialty Clinic Medical Directors, Medicaid Directors, the Chairs of the Legislature’s Health Care Committees, etc.
> Explore Developing a Regional Health Authority that integrates management and funding of health, behavioral health, public health, housing, and social services.
> Influence State and Health Plan Decision-Making Process regarding Parity, ACOs, Medical Home Standards and Payment Models, Health Insurance Exchanges, and Medicaid Expansion.
> Become a Founding Member of your Local Accountable Care Organization - if one hasn’t begun, start it!

www.TheNationalCouncil.org
When You’re At The Table
Under an Accountable Care Organization and Primary Care Practice Medical Home Models the Value of Behavioral Health Services will depend upon our ability to:
1. Be Accessible (Fast Access to all Needed Services)2. Be Efficient (Provide high Quality Services at Lowest Possible
Cost)3. Produce Outcomes!
• Engaged Clients and Natural Support Network• Help Clients Self Manage Their Wellness and Recovery• Greatly Reduce Need for Disruptive/ High Cost Services
(both medical and behavioral services)

www.TheNationalCouncil.org
Healthcare Home Participation> Decide your Healthcare Home involvement level – Full
Integration, Partnership or Linkages? And begin.> Provide Primary Care Services in the Behavioral Health
Center – either provide basic set of screening, education and linkage to primary care; or be part of full scope Person Centered Healthcare Home.
> Provide Behavioral Health Services in Primary Care – support mental health/substance use care in primary care using clinical practices appropriate to those settings.
> Develop Linkages as Specialty Behavioral Healthcare Providers to Medical Homes – ensure medical home pts. can get rapid access to quality behavioral health services .
> Develop a Strategy for Your Participation in FQHC Expansion – decide how you’ll help FQHC system double in size over the next five years.

www.TheNationalCouncil.org
Measure and Get Paid> Develop Technology Infrastructure to Integrate
Clinical, Quality, and Finance – including HER for each clinician that includes pt. registries and data warehouse that integrates clinical, quality and financial data.
> Build High Performing Quality Improvement Infrastructure – through quality management process that includes annual plan to address quality assurance, quality improvement, risk management, utilization/resource management, credentialing, and performance contracting.
> Develop Effective Revenue Cycle Management Infrastructure – building on the service delivery process to capture and collect every dollar owed to the organization.
> Prepare to Participate in the Health Insurance Exchanges – ramp up ability to work with Private Insurance Plans, ACOs, and Employers that will be operating under parity.

www.TheNationalCouncil.org
Measure and Get Paid
>Prepare for Value-Based Purchasing – including infrastructure to support Case Rates, Capitation, and Pay for Performance Bonus Arrangements.
>Develop Bullet-Proof Compliance Plan for era of increased scrutiny overseen by compliance officer that ensures internal monitoring/ auditing.
>Review Your Human Resources Function and Plan for Workforce Expansion in order to be prepared for the newly covered population and increased demand in 2014; and as public recognizes importance of quality behavioral healthcare.

www.TheNationalCouncil.org
Help Consumers Get Coverage and Services
>Support Parity Implementation through the active monitoring and reporting of parity violations and the education of consumers, advocates, community groups, health plans, state officials and others about how to comply with the private health plan and Medicaid parity regulations.
>Develop an Enrollment Strategy for Your Uninsured Consumers and Potential Consumers that identifies persons eligible for coverage through Medicaid and the Exchange, assist with enrollment process, and advocate for the removal of structural barriers.

www.TheNationalCouncil.org
• What can you tell me about your readiness to:1. Participate in Healthcare Homes2. Facilitate Rapid Access3. Match Need with Type and Level of Care4. Practice Stepped Care (Up and Down)5. Provide Care Management for High Cost Patients6. Measure Individual Improvement and Adjust Care7. Participate in P4P Bonus Arrangement8. Manage Under Case Rates9. Play in the ACO/IHS World10. Operate in an Insurance World, Contracting with Insurers11. Advocate for Consumers Affected by Non-Compliance with
Parity12. Support Consumer Access to Medicaid and the Exchanges
• And what needs to be added to the list?
Reform Implementation Checklist

www.TheNationalCouncil.org
“The most effective way to cope with change is to help create it”
L.W. Lynett