Www.bakerdconsulting.com Healthcare Reform Business implications and the current state of play...
30
www.bakerdconsulting.com Healthcare Reform Business implications and the current state of play Session 2 July 1, 2009 1:00 PM EDT You may listen to the audio online or you may dial: 1-866-642-1665 Pass Code 342441 1
-
Upload
dora-riley -
Category
Documents
-
view
213 -
download
0
Transcript of Www.bakerdconsulting.com Healthcare Reform Business implications and the current state of play...
www.bakerdconsulting.com
Healthcare ReformBusiness implications and the
current state of playSession 2
July 1, 2009 1:00 PM EDT
You may listen to the audio online or you may dial:
1-866-642-1665Pass Code 342441
1

Agenda
Update on timing and process Overview of key provisions Detailed review Discussion
2

Update on timing and processHouse
• Tri-Committee draft and hearings (July)• Tri-Committee markup (July)• Floor (July)
Senate• HELP markup (July)• Finance draft and markup (July)• Floor (July/September)
Conference• Conference Committee and floor (August/September)
If Unsuccessful … • Reconciliation (October)• Medicare Package (December)
3
TIMING

Key health reform provisions
Coverage1. Expanded eligibility for sub-populations
The young, the poor, early retirees, small business
2. Pooling mechanisms to ensure access Individual and employer mandates
3. Mandated benefit packages Part D donut hole reforms
4. Market reforms Guaranteed access, cost-share limits, community
rating
5. “Public option” or “Coop Plan”
4
COVERAGE

Key health reform provisions (cont.)
Improve Quality1. Coordinated care and medical home models2. Comparative Effectiveness Research3. Prevention Trust Fund
Reduce Cost - Reform the Delivery System1. Payment bundling across episodes of care
(ACE and Care Transitions)2. Aligning provider incentives
(ACOs and Gainshare)3. Value-based purchasing4. Physician payment reform
5
QUALITY – DELIVERY SYSTEMS

6
Key health reform provisions (cont.)
Sources of Pay-Fors
1. Medicare Advantage Part C Plans ($177 billion)– Capped payment – Competitive bidding
PAYING FOR REFORM

7
Key health reform provisions (cont.)
Sources of Pay-Fors (cont.)
2. Pharma ($100 billion)– Donut hole rebates– Medicaid rebates for Part D duals ($75 billion)– “Follow-on Biologics”– Drug importation– Part D price negotiation– 340B expansions
PAYING FOR REFORM

8
Key health reform provisions (cont.)
Sources of Pay-Fors (cont.)
3. Devices ($30-50 billion) – High-growth, over-valued” sectors (DME)– Imaging ($6 billion)– End federal preemption
4. Home Health – High-growth, “over-valued” sector– One-yr payment freeze– Accelerate inflation update cuts
PAYING FOR REFORM

9
Key health reform provisions (cont.)
Sources of Pay-Fors (cont.)
5. Hospitals ($200 billion)– DSH reimbursement (75% reduction) ($106 billion)– On top of other delivery system reforms
6. Multiple Providers– Share (50%) productivity adjustments ($110 billion)– Not clear on medical liability reform
PAYING FOR REFORM

10
Key health reform provisions (cont.)
Sources of Pay-Fors (cont.)
7. Fraud and Abuse – Physician payments (e.g., Physician Payment
Sunshine Act)– Self-referral restrictions (specialty hospital,
imaging, etc.)– Increased funding for OIG and agency fraud efforts
PAYING FOR REFORM

11
CER agenda took shape through ARRA; healthcare reform will make it
permanent
April 29, 2009– Senate Finance Committee whitepaper
June 9, 2009– Comparative Effectiveness Research Act of 2009 (Baucus,
Conrad) June 19, 2009
– House Tri-Committee bill June 29, 2009
– Federal Coordinating Council recommendations June 30, 2009
– Institute of Medicine Report July 30, 2009
– Secretary’s Report to Congress
COMPARATIVE EFFECTIVENESS
“Now the Federal Government must make progress and deliver results. . .”

12
Structure of CER entity differs but focus of Senate and House versions is similar
Senate proposes non-profit institute for patient-centered
outcomes research Board of Governors
– Includes stakeholder reps Set priorities, carry out agenda
– Contract with Fed Agencies (e.g., AHRQ) or private sector
Comparative clinical effectiveness Advisory panels as needed
– Topics, methods, rare disease Transparency and public comment CER for coverage only if:
– Stakeholder input– Subgroup analysis conducted– GAO report required
Funding through Patient Centered Outcomes Research Trust
House proposes Center within AHRQ
CER Commission – Includes stakeholder reps
“Conduct, support, synthesize research”, set priorities and methods
Consider impact of CER on racial, ethnic minorities, patient subgroups
Set protocols to disseminate results
CER Trust Fund created through Medicare and private payer contributions per beneficiary
COMPARATIVE EFFECTIVENESS

13
FCC framework developed to identify priorities for CER
COMPARATIVE EFFECTIVENESS

14
COMPARATIVE EFFECTIVENESS
15
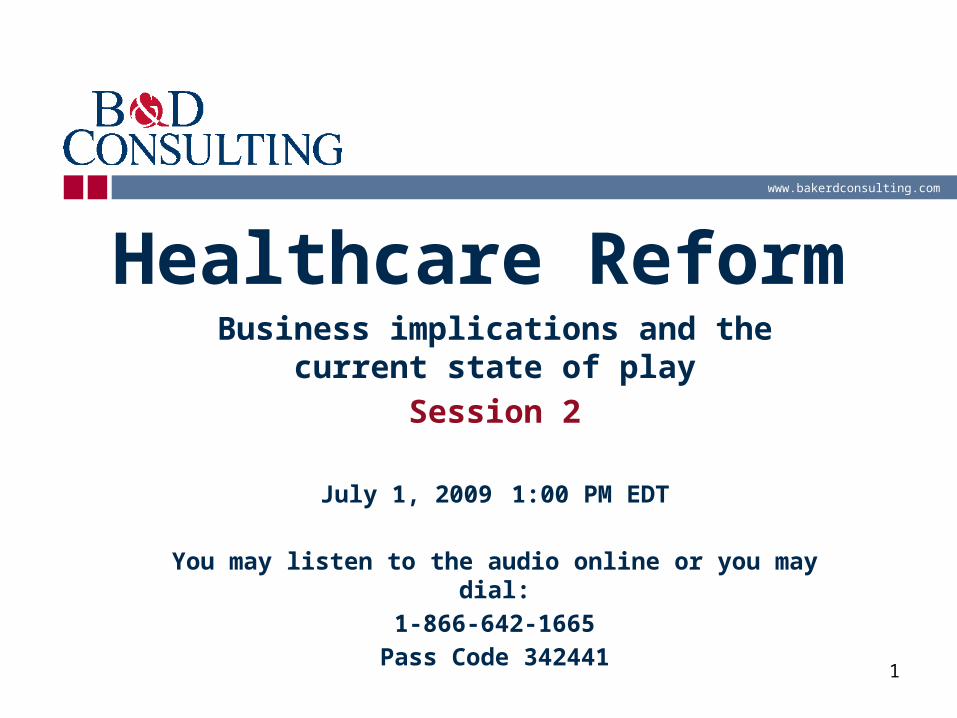
FCC identified major gaps in existing assets
COMPARATIVE EFFECTIVENESS

16
FCC’s key priority is building data infrastructure for short and longer-
term use Data infrastructure requires large,
upfront infusion of cash– Comprehensive databases and research
tools• Build, expand, link longitudinal,
administrative data• Expand high-impact registries (e.g., SEER)• Distributed data networks with EHRs from
practice• FDA and private sector safety data
– Ensure privacy, security
COMPARATIVE EFFECTIVENESS

17
COMPARATIVE EFFECTIVENESS

18
The IOM urged Congress to “establish a robust CER
enterprise” Develop infrastructure to carry out sustainable CER strategy
Consultative process based on– Condition-level criteria
• Burden of disease, cost, variability– Priority topic
• Gaps in knowledge, results would improve health
– Balanced portfolio of topics to address broad societal needs, including focus on subgroups/rare diseases
– High priority topics included prevention, systems of care, drug, device, surgery, monitoring
COMPARATIVE EFFECTIVENESS
19
Listening sessions honed focus of recommendations
1268 research topics proposed– IOM winnowed to 82, then added 18 more to fill
in gaps– Half focus on delivery system– One-third address health disparities, functional
limitations Cardiovascular disease, geriatrics,
neurology, oncology, pediatrics are priorities
COMPARATIVE EFFECTIVENESS

20Source: IOM Report, June 30, 2009
COMPARATIVE EFFECTIVENESS
21
IOM presented 100 priorities in quartiles
First quartile priorities included:– Treatment strategies for atrial fibrillation– Impact of upper endoscopy on GERD outcomes– Compare CER results dissemination methods– Effectiveness of biologics for inflammatory
diseases– Screening methods for MRSA – Imaging modalities to diagnose cancer
Next quartiles include important questions, too, but were ranked lower in consensus process
IOM notes priorities will change over time
COMPARATIVE EFFECTIVENESS

22
Stakeholders should consider business strategy in light of CER
update Access to decision makers and influencers Evolving, interoperable data systems
– Distributed model may require least new infrastructure development
Opportunity to reframe market space Impact on coverage determination process
– Length, participants, public comment and response Transparency of process
– New reporting/data collection burden Focus on impact of product/service within health
system “Clinical” effectiveness language persists
– Role of economic analysis
COMPARATIVE EFFECTIVENESS

23
Senate proposal would give MedPAC regulatory authority
Currently, an independent agency created in 1997 to advise Congress on Medicare program– 17 members with diverse backgrounds appointed by
Comptroller General Medicare Payment and Access Commission would oversee
payment and coverage policy– Determine payment policy, methodology, rates, units and amounts of
payment for all providers and services– Set coverage policy to ensure stable premiums and access– Ensure financial stability of Medicare Program
• Authority/requirement to reduce Program spending by 1.5 percent/year
– Presidential appointment with Senate confirmation– GAO study and annual report required
Current MedPAC Commissioners become Council of Health and Economic Advisors
MEDPAC REFORM

24
New oversight for Medicare program
Congressional Joint Committee on Medicare
Demonstration projects moved out of CMS to HHS– Authority to expand demonstrations– Eliminate budget neutrality
requirements
MEDPAC REFORM

25
Public OptionPrimary approaches Federal model (Schumer) Coop model (Conrad) Fall-back option (Snowe)
Primary components Financing Provider payment Regulation Participation
PUBLIC OPTION

26
Bundling strategies
Primary approaches Across Episodes of Care (ACE Demo) Post-Acute Care (Care Transitions
Demo)

27
Bundling strategies
Primary components ACE Demo
– Amount of payment– Payment recipient– Coordinator of care– Measuring results– Transparency
BUNDLING

28
Bundling strategies
Primary components Care Transitions Demo
– Amount of payment– Payment recipient– Coordinator of care– Measuring results– Transparency
BUNDLING

29
What should you be doing now?
Assume FFS model transitions to payment for quality/efficiency
Focus on your business plan, business model, with 3-year horizon
Consider roles of new decision makers, regulatory authorities– Requirements for annual cuts to Medicare program spend– Five-year review of payment policy, amounts
• Position of product/service within broader delivery system• Impact on quality of care, access• Role for innovation
BUSINESS IMPACT/IMPLICATIONS

30
Vince Ventimiglia Senior Vice [email protected]
Ed Dougherty Senior Vice [email protected]
Join us for our next session