WSVMA Annual Conference · o Pulse oximeter o Thermometer ... Handbook of Veterinary Anesthesia....
12
WSVMA Annual Conference Anesthesia and Pain Management: Considerations for Veterinary Technicians Spokane Convention Center Spokane, Washington October 1-3, 2010 Joshua Schulz, BVSc US Veterinary Services Pfizer Animal Health, Olympia, WA
Transcript of WSVMA Annual Conference · o Pulse oximeter o Thermometer ... Handbook of Veterinary Anesthesia....
WSVMA Annual Conference
Anesthesia and Pain Management:Considerations for
Veterinary Technicians
Spokane Convention CenterSpokane, Washington
October 1-3, 2010
Joshua Schulz, BVScUS Veterinary Services
Pfizer Animal Health, Olympia, WA
Dr. Joshua Schulz Pfizer Animal Health
Olympia, WA Biography: Dr. Schulz has been an Associate Veterinarian at Steamboat Animal Hospital in Olympia, WA since graduating from the University of Queensland (Brisbane, Australia) in 2004. His veterinary interests include surgery, canine reproduction and pain management. He is certified as a PennHIP veterinarian. Dr. Schulz joined Pfizer Animal Health in April 2010 as the Area Veterinarian for the Pacific Northwest. His duties include providing technical veterinary support for the sales team of Pfizer and the clinics they serve. This includes in-clinic consultations, seminars, wet labs and speaking engagements concerning Pfizer products and general animal health. Contact Email: [email protected]
Balancing Anesthesia I: Considerations in Managing Pain Dr. Joshua Schulz
Pfizer Animal Health *Daily Sentiment: “Hands down, a caring, educated and experienced technician is absolutely the best monitoring equipment a veterinarian has in the clinic. I would not be a very good veterinarian if it wasn’t for my technicians.”
Dr. Josh Schulz
Foundations of Pain Management: What is pain? Why treat it?
• “…a subjective experience that accompanies the neurophysiologic process of pain
recognition” (nociception) — Wikipedia.org
• Physiologic pain protects the body from damaging stimuli. Pain is nature’s “alarm.”
• Pathologic pain is ongoing pain produced by tissue injury, inflammation.
• “…an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.” (nociception)
• “…the inability to communicate in no way negates the possibility that an individual is
experiencing pain and is in need of appropriate pain relieving treatment.” — International Association for the Study of Pain
• … animal pain and suffering are clinically important conditions that adversely affect an
animal’s quality of life…pain assessment is considered part of every patient evaluation regardless of the presenting complaint. It is better to prevent pain than to treat it.
— JAVMA editorial staff. AVMA adopts position regarding animal pain. J Am Vet Med Assoc 2001 Jun 1; 218(11):1694.
• When evaluating our animal patients, we must remember that even though an animal is
lying quietly, it still may be in need of pain relief — perhaps more than the animal that is vocalizing.
1
• We have a responsibility to treat and manage pain in our veterinary patients. Consideration should be given to evaluate it as the 4th / 5th vital sign as proposed by the American Pain Society in the mid 90’s (others: temperature, pulse, respiration and +/- blood pressure)
• Previously, pain treatment was more out of empathy and ethical obligation. Research in
recent years revealing a more thorough understanding of the physiological pathways of pain in animals now demand attempts at full pain control in animals
• Incorporating pain management into the veterinary practice helps everyone.
It benefits the patient - improved quality of life and reduced complications. It benefits clients - enhancement of the human–animal bond. It benefits the veterinary staff – increased safety; improved morale, pride, and job satisfaction; and a less stressful environment (e.g. post op noise and stress??).
Pathways of Pain: Understanding Pain Pathways/Physiology (Fig. 1)
• Nociception
o Transduction o Transmission o Modulation
• Perception
• Negative Consequences of Pain • increased oxygen consumption • decreased cardiac output • protein catabolism • inappetance • hyperglycemia • increased heart rate • Hypertension • delayed wound healing • retention of sodium and water • platelet aggregation • immune suppression • cardiac arrhythmias • exhaustion
Consequences of untreated pain Wind Up pain - “Wind-up pain” is a heightened sensitivity that results in altered pain thresholds, both peripherally and centrally, such that pain is experienced in areas unrelated to the original source. Wind-up causes a worsening of acute pain
2
Historical Myths about Pain
• Animals do not feel pain as much as humans • Post-operative pain is good for the patient
• Pain speed healing process
• Pain relief masks other physiologically important signs (e.g. pulse, respiration, blood
pressure)
• Multiple (analgesic) drug use is dangerous
• Pet owners wont pay for pain relief
Veterinarian/Technicians Role in Recognizing and Assessing Pain
• Repeated evaluation of patients o Signs of Pain
• Pain Scoring Systems • Gut feeling? Techs are very good at this:
If there is ANY question as to whether or not an animal is in pain, you can “ask” that animal how it feels: consider a “test dose” of an analgesic drug and monitor the animal’s response. More importantly, we can learn to anticipate pain. The level of pain associated with surgery can be anticipated to some extent. In general, the more tissue trauma, the more pain, because pain is proportional to increasing levels of circulating cytokines.
Target Points of Pain and Analgesic Options Pharmacological Options for Pain – Can more be better?
• NSAIDs – target inflammation and pain pathways • Opioids – target pain receptors all over the body • Alpha-2 agonists - sedation and analgesia • Local Anesthetics – block pain signals • Others
Target Points of Pharmacological Agents in Pain Pathway
• Transduction– NSAIDs, local anesthetics, opioids, corticosteroids
3
• Transmission - Local anesthetics, α-2 agonists • Modulation – NSAIDs, local anesthetics, opioids, α-2 agonists, others(TCA’s, NMDA
antagonists, anticonvulsants, etc) • Perception – general anesthetics, opioids, α-2 agonists, benzodiazepines,
phenothiazines Other Concepts in multimodal pain management
• Preemptive Analgesia o Studies show: before is better! o Avoids “catch up” analgesia which requires higher doses and increased risk of
side effects
• Multimodal analgesia – attack different sites / receptors Studies show: more is better!
• Acute pain options o Pharmacological interventions – traditional and non-traditional drugs o Heat/Cold therapy o Bandages post op
• Chronic pain options
o Pharmacologic interventions- traditional and non-traditional drugs E.g. NSAIDs, opioids, TCA’s, Anticonvulsants, NMDA antagonists
o Physiotherapy/rehab o Heat/Cold therapy o Weight loss o Electrical stimulation/TENS o Acupuncture
4

Balancing Anesthesia II: Considerations in Sedation
and Anesthetic Protocols Dr. Joshua Schulz
Pfizer Animal Health Brief history of origins of anesthesia
• Use of roots and plants for pain in ancient and medieval societies o opium, mandrake, mangradora, coca, etc
• Late 1800s - birth of modern anesthesia
o Physician Crawford Williamson Long (1842, tumor removal) o Horace Wells (1844 tooth extraction) o William Thomas Green Morton (1846, dental procedure).
• Physician Oliver Wendell Holmes suggested term “anesthesia.”
Definitions:
• Sedation – reduction of stress, irritability or excitement; induces relaxation • Tranquilization – reduction of anxiety without sedation or analgesia • Analgesia – absence of pain or reduction in its intensity • Anesthesia – “no sensation” or absence of the perception of pain
*** Good anesthesia always incorporates good analgesia! *** Balanced Anesthesia provides all of the following (Fig. 2)
• Sedation/Relaxation – cooperative patients = safer, easier handling for staff • Analgesia – reduced pain in patients • Unconsciousness – total relaxation and loss of pain sensation
Balanced anesthesia/sedation
• Single drugs – require large volumes to achieve anesthesia/analgesia • Multidrug protocols – target positive effects, decrease side effects = increased margin of
safety • Target points of main pharmacological agents in anesthesia (Fig. 1)
4 Phases of Balanced Anesthesia (Fig. 3) • Premedication – cooperative patient, dose sparing effects on injectable and gas anesthesia • Induction – to effect – always! Different patients and premeds influence anesthetic
requirements • Maintenance – monitoring keys • Recovery - don’t assume patient is done/safe
5
Perioperative Pain management • Preemptive analgesia • Perioperative pain options • Post-operative pain control
Keys to Successful surgical outcomes Monitoring
• Diligent attention to patient vitals o Cardiovascular – heart rate, rhythm, pulse quality o Respiratory – rate, rhythm, lung sounds o BP – mean and systolic o Temp o Anesthetic depth – eye position, pupil size, jaw tone
• Use of Instrumentation/Monitors as adjunct to patient monitoring o Blood pressure o Pulse oximeter o Thermometer o Capnography/ETCO2 o ECG
• Trends: the real the story • Experience and “feel” of the technician
Others:
• Mask/Box induction - • TIVA – boluses or CRI infusion -
Questions/Topics?
6

Figure 1 – Pain Pathways and Drug Sites of Action
7
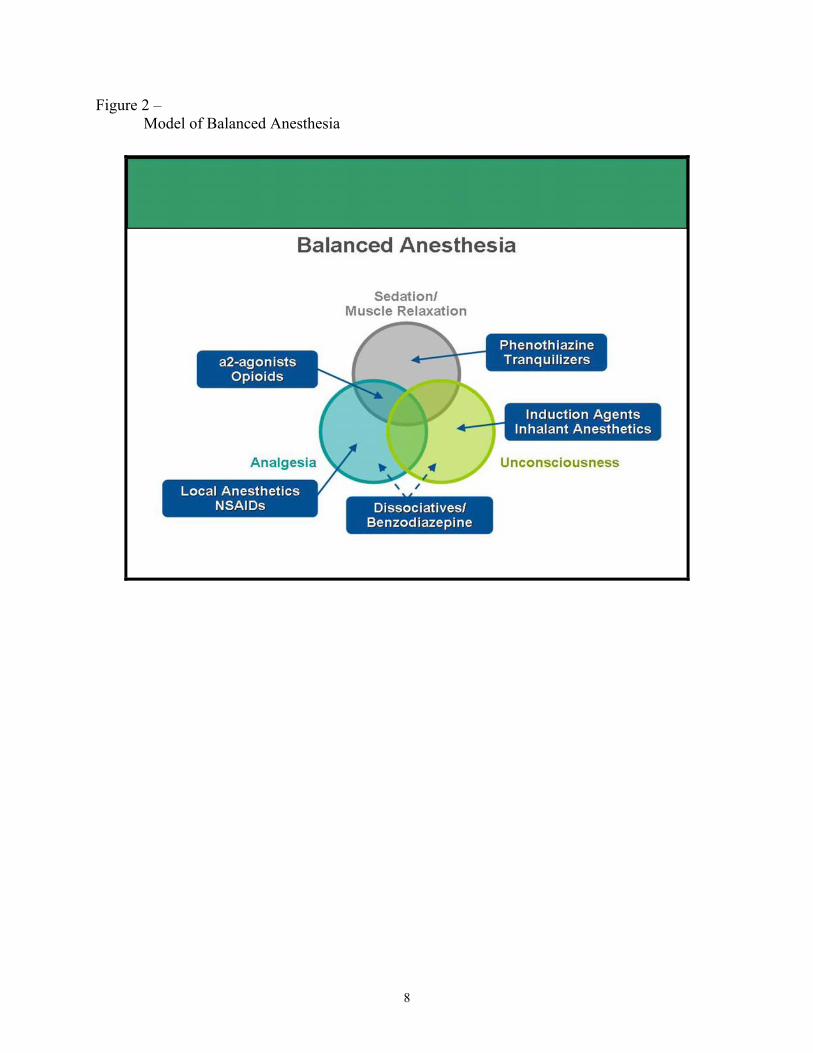
Figure 2 – Model of Balanced Anesthesia
8

Figure 3 – 4 Phases of Anesthesia
9

10
Suggested References: Anesthesia/Pain Management
Gaynor J, Muir W. Handbook of Veterinary Pain Management. St. Louis, MO: Elsevier Publishing, 2002. Muir WW, Hubbell JA. Handbook of Veterinary Anesthesia. 4th ed. St. Louis, MO: Elsevier Publishing, 2006. Tranquilli WJ, Grimm KA, Lamont LA. Pain Management for the Small Animal Practitioner—A Made-Easy Series Book. 2nd ed. Jackson, WY: Teton NewMedia, 2004. AAHA/AAFP Pain Management Guidelines for Dogs & Cats; J Am Anim Hosp Assoc 2007;43:235-248.The American Animal Hospital Association and the American Association of Feline Practitioners AAHA/AAFP Pain Management Guidelines Task Force Members: Peter Hellyer, DVM, MS, DACVA; Ilona Rodan, DVM, DABVP (Feline Practice); Jane Brunt, DVM; Robin Downing, DVM, CVA, DAAPM; James E. Hagedorn, DVM, DABVP; Sheilah Ann Robertson, BVMS (Hons), PhD, DACVA, DECVA, MRCVS