Wpa borderline intellectual functioning
20
BORDERLINE INTELLECTUAL FUNCTIONING: A complex picture of deficits and problems in no-man´s land 1. Villablanca Serveis Assistencials, Reus, Spain. 2. Fundació Villablanca, Reus, Spain; IISPV, URV, CIBERSAM. 3. University of Sydney, Sydney, Australia. A.Torres 1 , M. Fernández 1 , M.J. Cortés 2 , A. Folch 2 , L. Salvador- Carulla 3 , R. Martínez-Leal 2
-
Upload
rafael-martinez -
Category
Documents
-
view
233 -
download
8
description
Â
Transcript of Wpa borderline intellectual functioning
BORDERLINE INTELLECTUAL
FUNCTIONING: A complex picture of deficits and problems in no-man´s land
1. Villablanca Serveis Assistencials, Reus, Spain.
2. Fundació Villablanca, Reus, Spain; IISPV, URV, CIBERSAM.
3.University of Sydney, Sydney, Australia.
A. Torres 1, M. Fernández 1, M.J. Cortés2, A. Folch2, L. Salvador-Carulla3, R. Martínez-Leal 2
DEFINITION
� It’s not a medical condition, neither a disease, there is no code for diagnosis in any classification (DSM or ICD-10).
� It could be considered a health metacondition (like pregnancy) where special attention is required at certain times.
� There are concerns in health services about where and � There are concerns in health services about where and how these people must be attended.
� There are not enough data about the complications that occur in Borderline Intellectual Functning (BIF), and the prevalence of added disorders and other problems is not well-known
� Salvador-Carulla L, Ruiz Gutierrez-Colosía M, Nadal M, Grupo CONFIL. Documento de Consenso sobre el funcionamiento intelectual límite. Madrid: Obra Social Caja Madrid; 2010
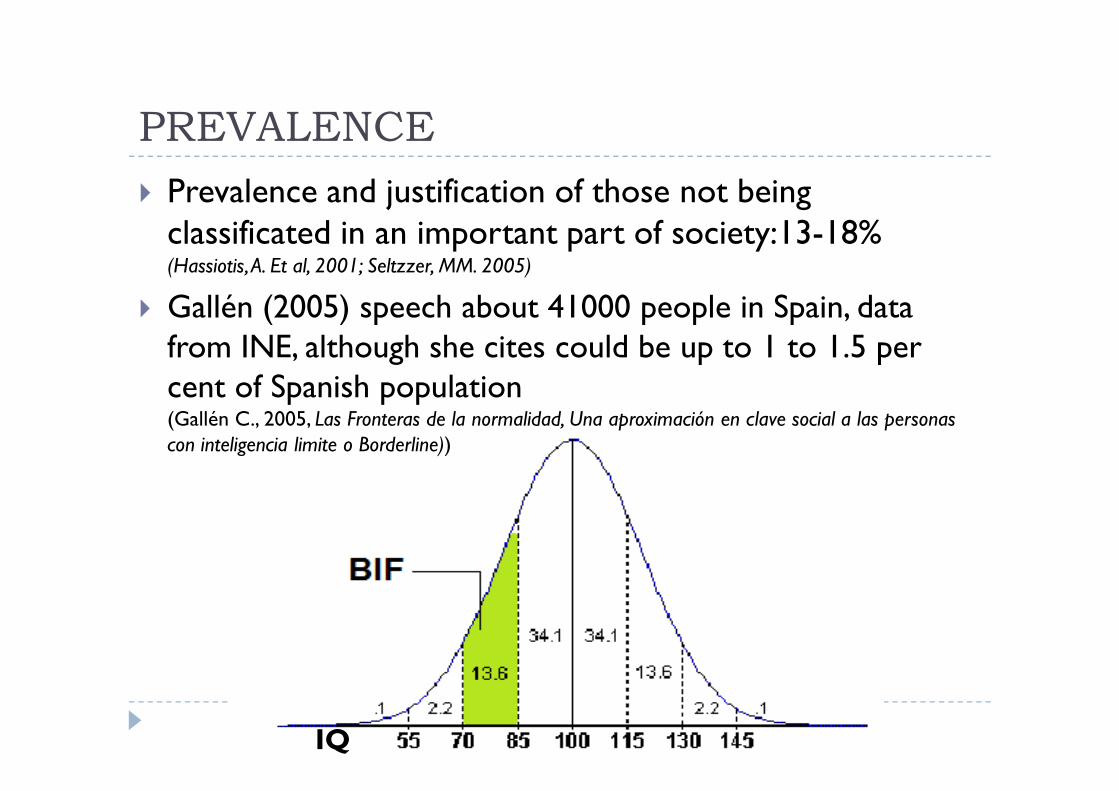
PREVALENCE
� Prevalence and justification of those not being classificated in an important part of society:13-18% (Hassiotis, A. Et al, 2001; Seltzzer, MM. 2005)
� Gallén (2005) speech about 41000 people in Spain, data from INE, although she cites could be up to 1 to 1.5 per cent of Spanish populationcent of Spanish population(Gallén C., 2005, Las Fronteras de la normalidad, Una aproximación en clave social a las personas con inteligencia limite o Borderline))
IQ
Mounting evidence suggest...
� Mental health problems in people with BIF are not well addressed bygeneral psychiatry (Wieland, J. Et al, 2014)
� A reduced sleep duration, an increased rate of stage shifts and awakenings. (Esposito, M. 2014, 2010)
� Emotional and behavioural problems as well as a lack of social competencein youngers (Nestler, J. & Goldbeck, L., 2011)
� Increased rates of suicidal behaviour in young people with BIF and social � Increased rates of suicidal behaviour in young people with BIF and social disadvantages (Hassiotis, A. 2011)
� Problems with motor skill performance and higher-order executivefunctions (Hartman, E. Et al; 2010; Vuijk P et al, 2010)
� More emotional, substance use, personality, adaptation and social problemsin adults (Hassiotis, A, 1999)
� Higher rates of mental health problems in children (Emerson, E., 2010)
� Worse prognosis of mental health problems in BIF population (Chaplin, R; 2006)
Background
� Data about BIF are very scarce.
� Are there real differences among BIF and mild ID regardingfunctioning and adaptive behaviour?
� Is functioning taken into account for the differential diagnosis?
OBJECTIVESOBJECTIVES
-To compare the level of impairments presented by BIF and ID.
-To present information about mental health conditions in BIF.
Methodology: NATIONAL SURVEY
(EDAD 2008)
� Specific for disability
� Interviewed more than 33000 people with disability
� 2840 had intellectual disability –including BIF-
� Geographical representation, taking into account residencesand private homes in the community.
The interview included a modified version of the International � The interview included a modified version of the International Classification of Functioning (WHO).
� Variables:
-Sex -ID/BIF
-Age -ICF areas of functioning
-Living arrangements
Instituto Nacional de Estadística, 2010. Encuesta de Discapacidad, Autonomia Personal y Dependencia EDAD-2008.
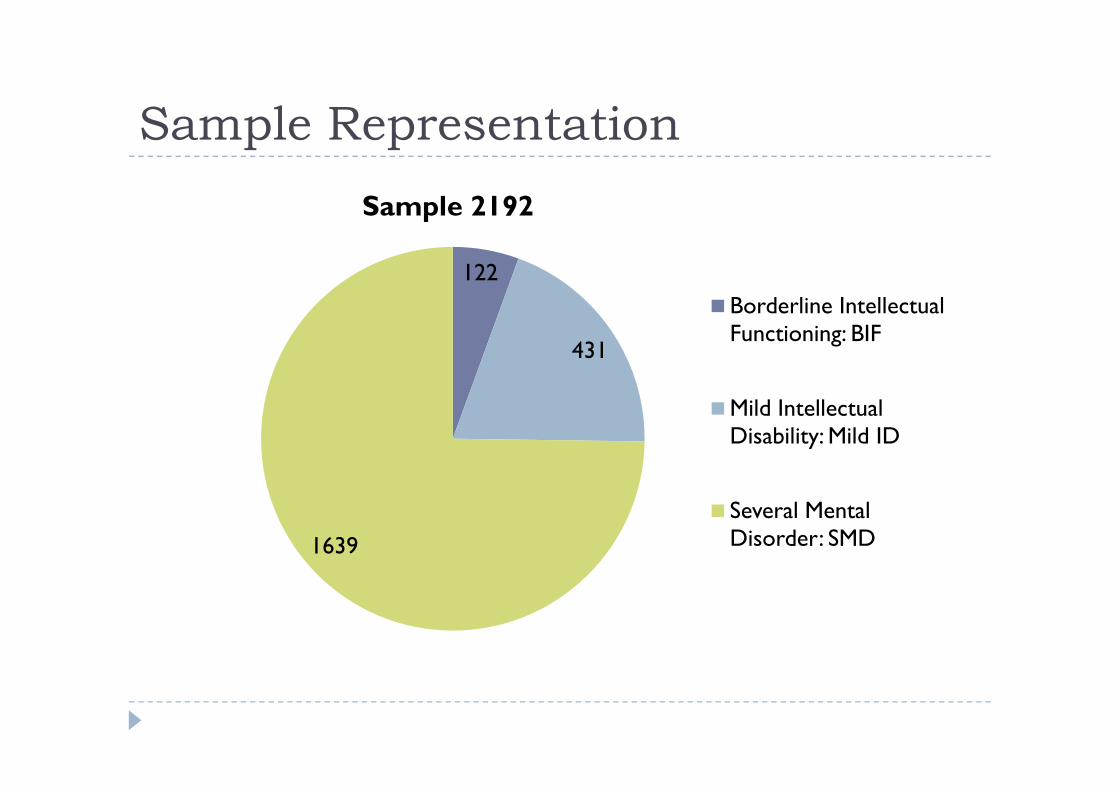
Sample Representation
122
431
Sample 2192
Borderline Intellectual Functioning: BIF
Mild Intellectual
1639
Mild Intellectual Disability: Mild ID
Several Mental Disorder: SMD
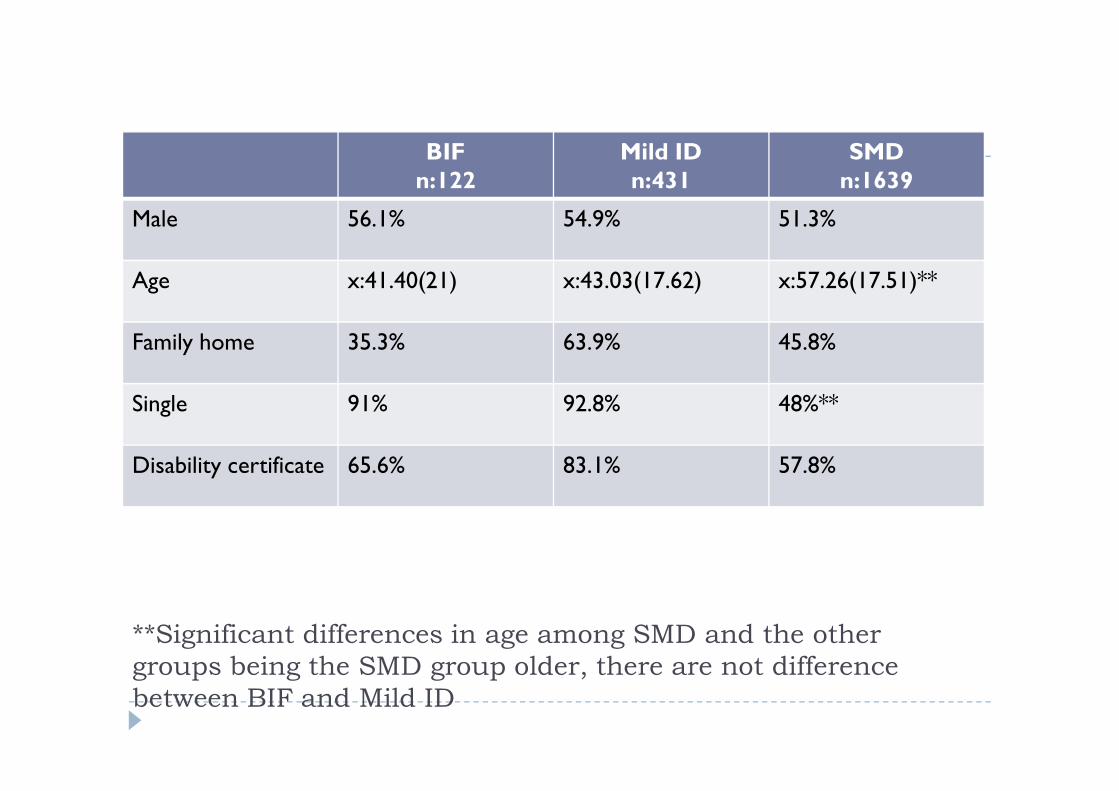
BIFn:122
Mild IDn:431
SMDn:1639
Male 56.1% 54.9% 51.3%
Age x:41.40(21) x:43.03(17.62) x:57.26(17.51)**
Family home 35.3% 63.9% 45.8%
Single 91% 92.8% 48%**
**Significant differences in age among SMD and the other
groups being the SMD group older, there are not difference
between BIF and Mild ID
Single 91% 92.8% 48%**
Disability certificate 65.6% 83.1% 57.8%
RESULTS
Persons with BIF have similar problems to those with mildID in important areas such as:� VISION and HEARING
� COMMUNICATION
� TASK PERFORMANCE and LEARNING
� SOCIAL INTERACTIONS
Persons with BIF are more independent in areas such as:� AUTONOMY and SELF CARE
� DOMESTIC SKILLS
More than 60% of persons with BIF living in thecommunity presented some type of Mental Disorder.
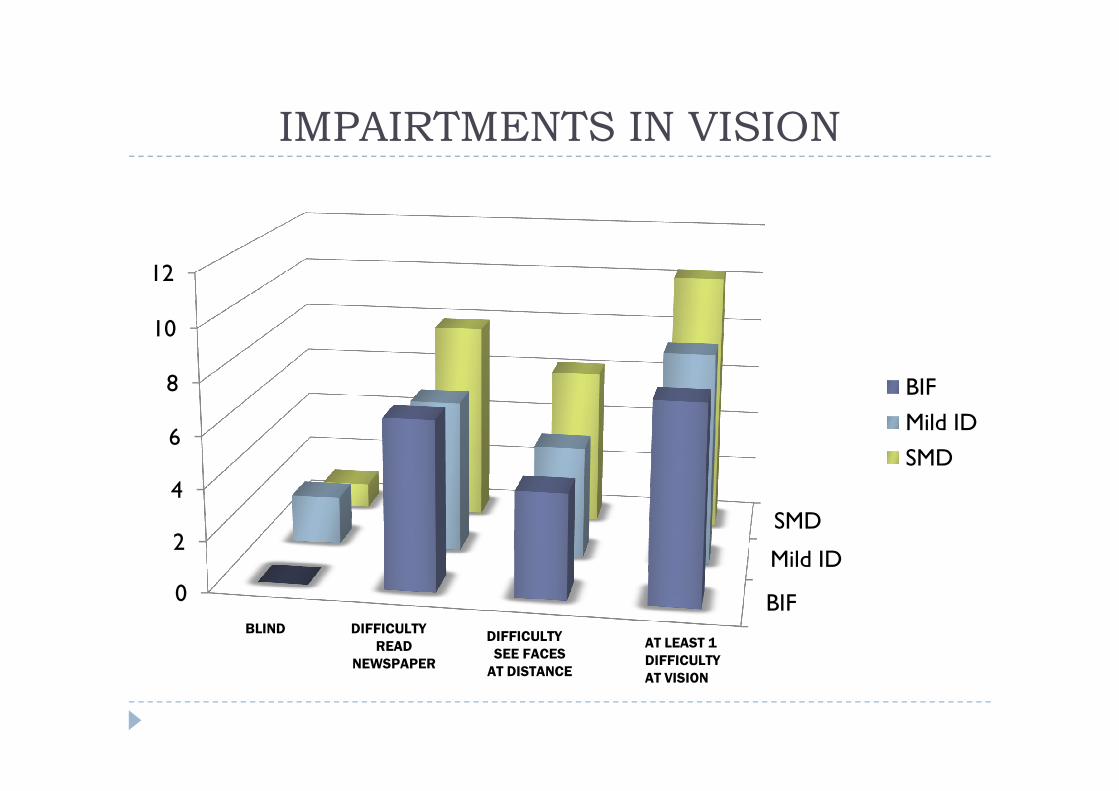
IMPAIRTMENTS IN VISION
8
10
12
BIF
BIF
Mild ID
SMD
0
2
4
6
8 BIF
Mild ID
SMD
BLIND DIFFICULTY
READ
NEWSPAPER
AT LEAST 1
DIFFICULTY
AT VISION
DIFFICULTY
SEE FACES
AT DISTANCE
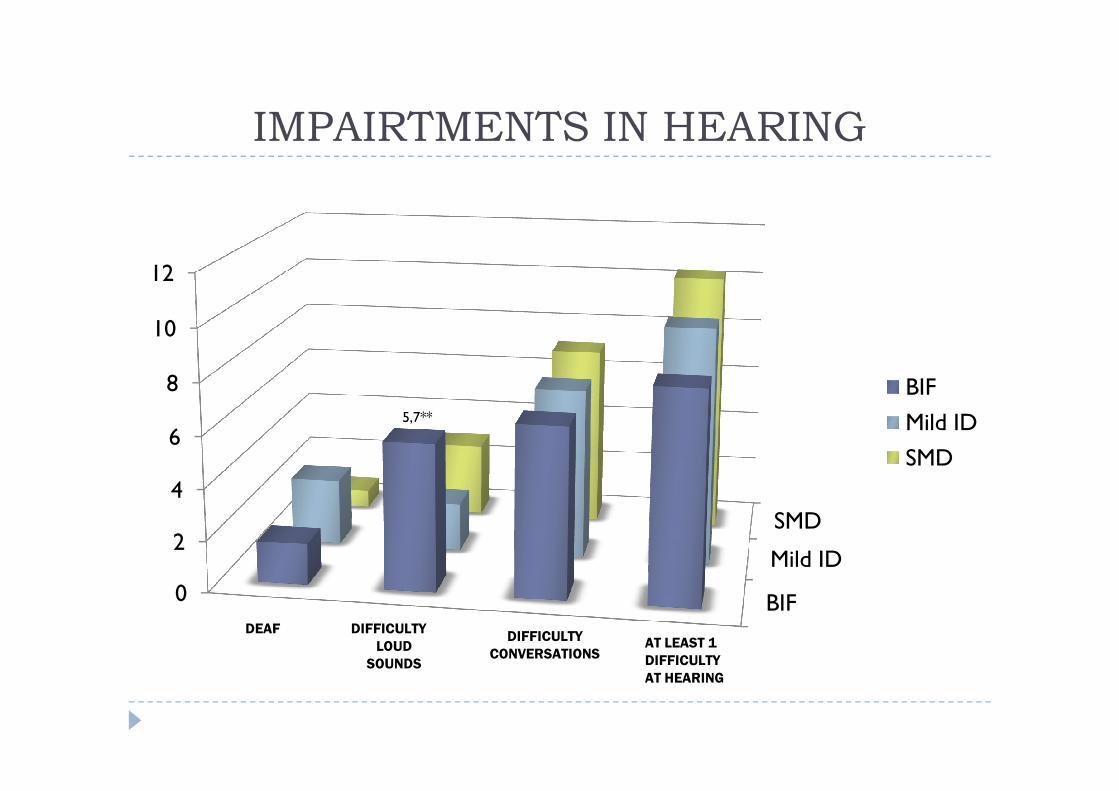
IMPAIRTMENTS IN HEARING
8
10
12
BIF
BIF
Mild ID
SMD
0
2
4
6
8
5,7**
BIF
Mild ID
SMD
DEAF DIFFICULTY
LOUD
SOUNDS
AT LEAST 1
DIFFICULTY
AT HEARING
DIFFICULTY
CONVERSATIONS
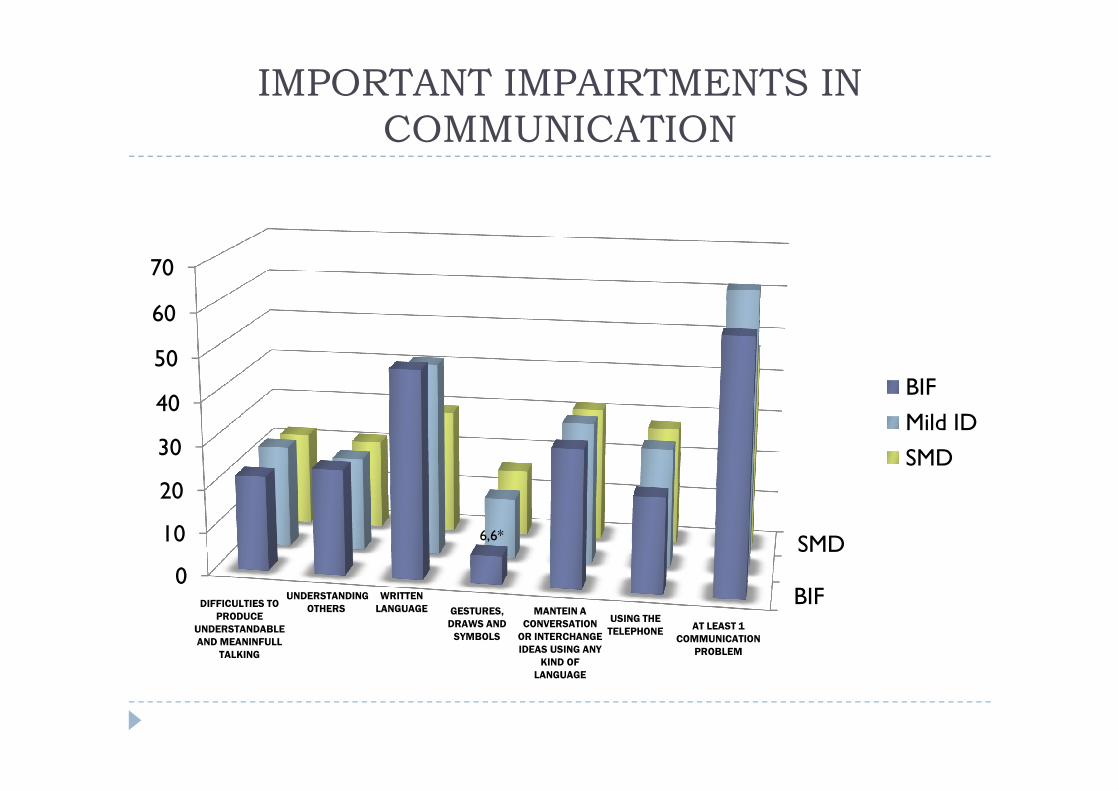
IMPORTANT IMPAIRTMENTS IN
COMMUNICATION
40
50
60
70
BIF
BIF
SMD
0
10
20
30
40
6,6*
BIF
Mild ID
SMD
DIFFICULTIES TO
PRODUCE
UNDERSTANDABLE
AND MEANINFULL
TALKING
UNDERSTANDING
OTHERS GESTURES,
DRAWS AND
SYMBOLS
MANTEIN A
CONVERSATION
OR INTERCHANGE
IDEAS USING ANY
KIND OF
LANGUAGE
USING THE
TELEPHONE
WRITTEN
LANGUAGE
AT LEAST 1
COMMUNICATION
PROBLEM
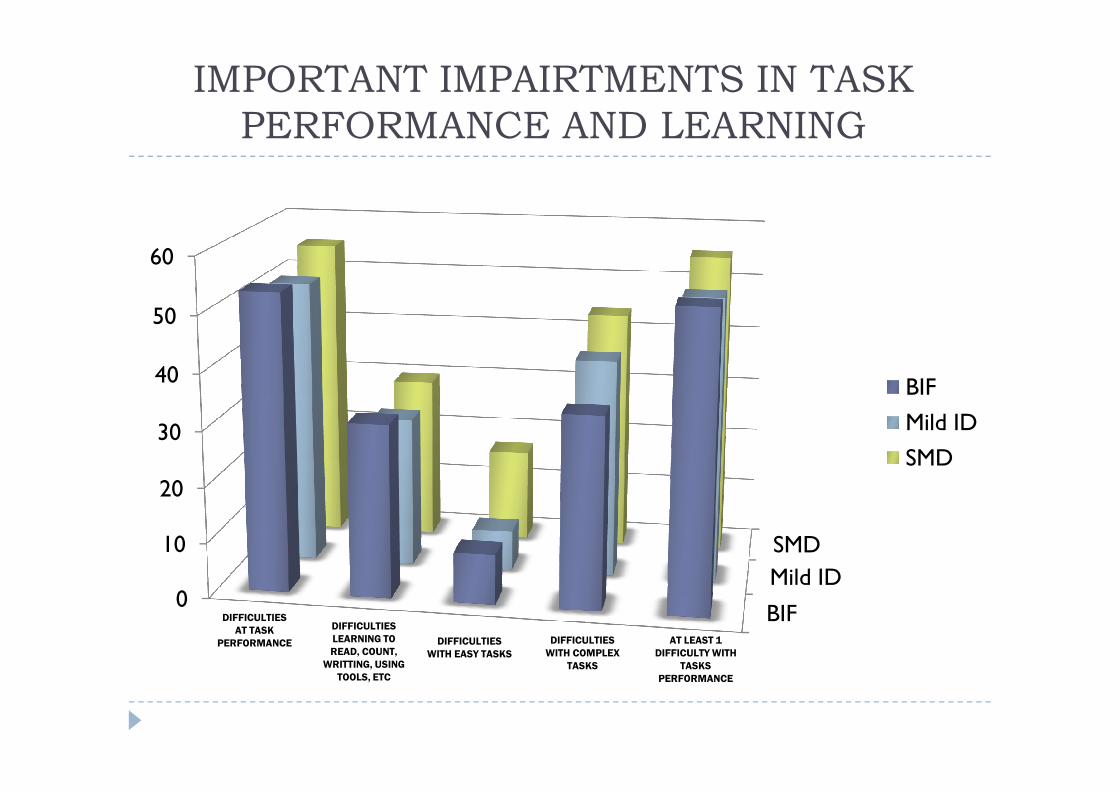
IMPORTANT IMPAIRTMENTS IN TASK
PERFORMANCE AND LEARNING
40
50
60
BIF
BIF
Mild ID
SMD
0
10
20
30
BIF
Mild ID
SMD
DIFFICULTIES
AT TASK
PERFORMANCE
DIFFICULTIES
LEARNING TO
READ, COUNT,
WRITTING, USING
TOOLS, ETC
DIFFICULTIES
WITH COMPLEX
TASKS
AT LEAST 1
DIFFICULTY WITH
TASKS
PERFORMANCE
DIFFICULTIES
WITH EASY TASKS
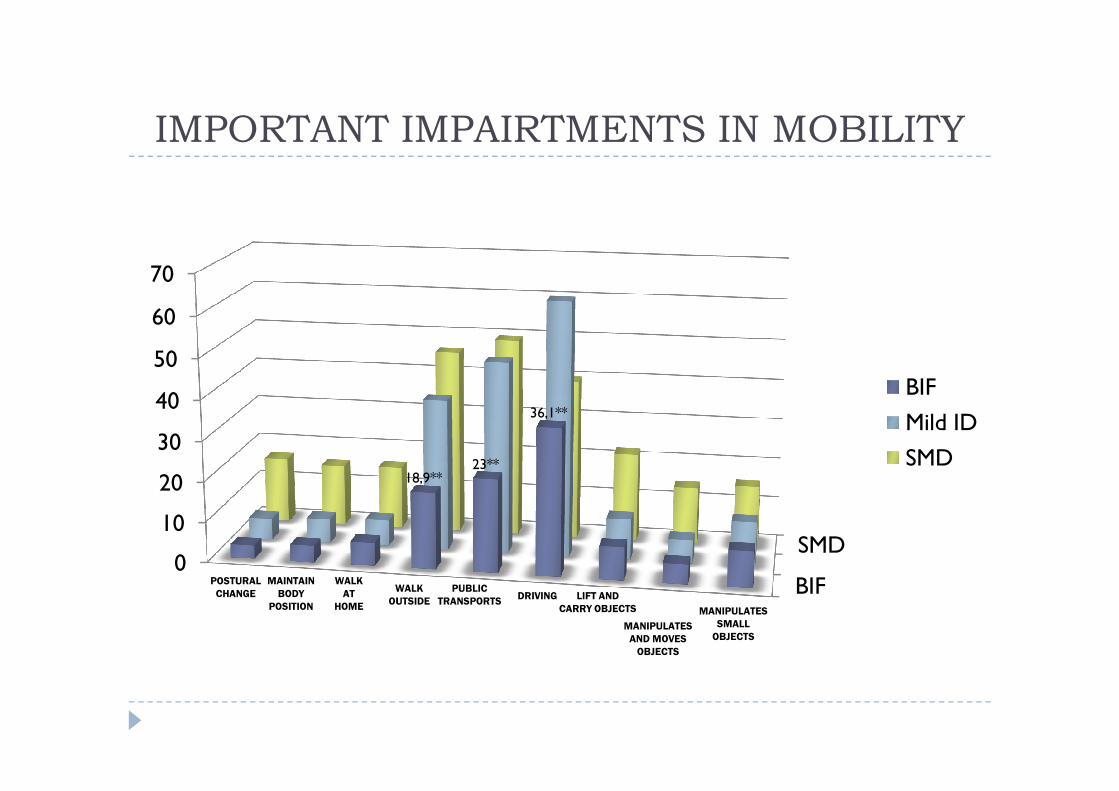
IMPORTANT IMPAIRTMENTS IN MOBILITY
40
50
60
70
BIF
BIF
SMD0
10
20
30
40
18,9**23**
36,1**
BIF
Mild ID
SMD
POSTURAL
CHANGE
MAINTAIN
BODY
POSITION
WALK
OUTSIDE
PUBLIC
TRANSPORTSDRIVING
MANIPULATES
AND MOVES
OBJECTS
LIFT AND
CARRY OBJECTS MANIPULATES
SMALL
OBJECTS
WALK
AT
HOME
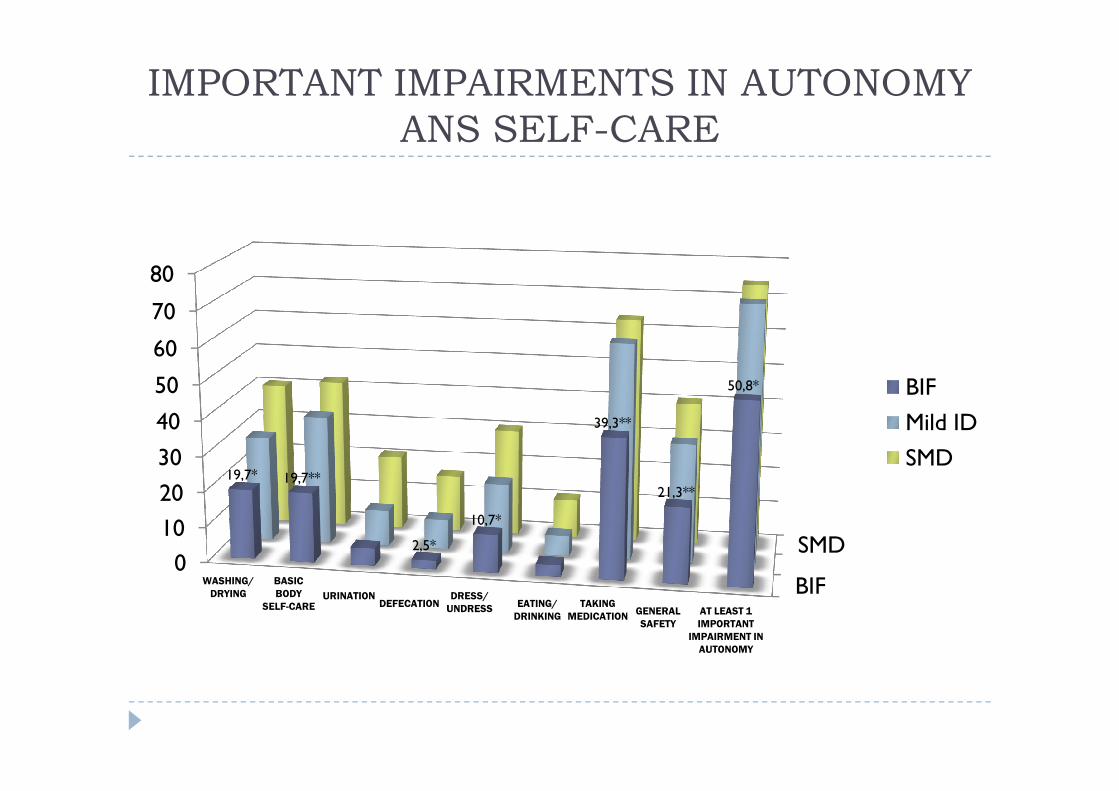
IMPORTANT IMPAIRMENTS IN AUTONOMY
ANS SELF-CARE
50
60
70
80
50,8* BIF
BIF
SMD0
10
20
30
40
50
19,7* 19,7**
2,5*
10,7*
39,3**
21,3**
BIF
Mild ID
SMD
WASHING/
DRYING
BASIC
BODY
SELF-CARE DEFECATIONDRESS/
UNDRESSEATING/
DRINKINGGENERAL
SAFETY
TAKING
MEDICATION
URINATION
AT LEAST 1
IMPORTANT
IMPAIRMENT IN
AUTONOMY
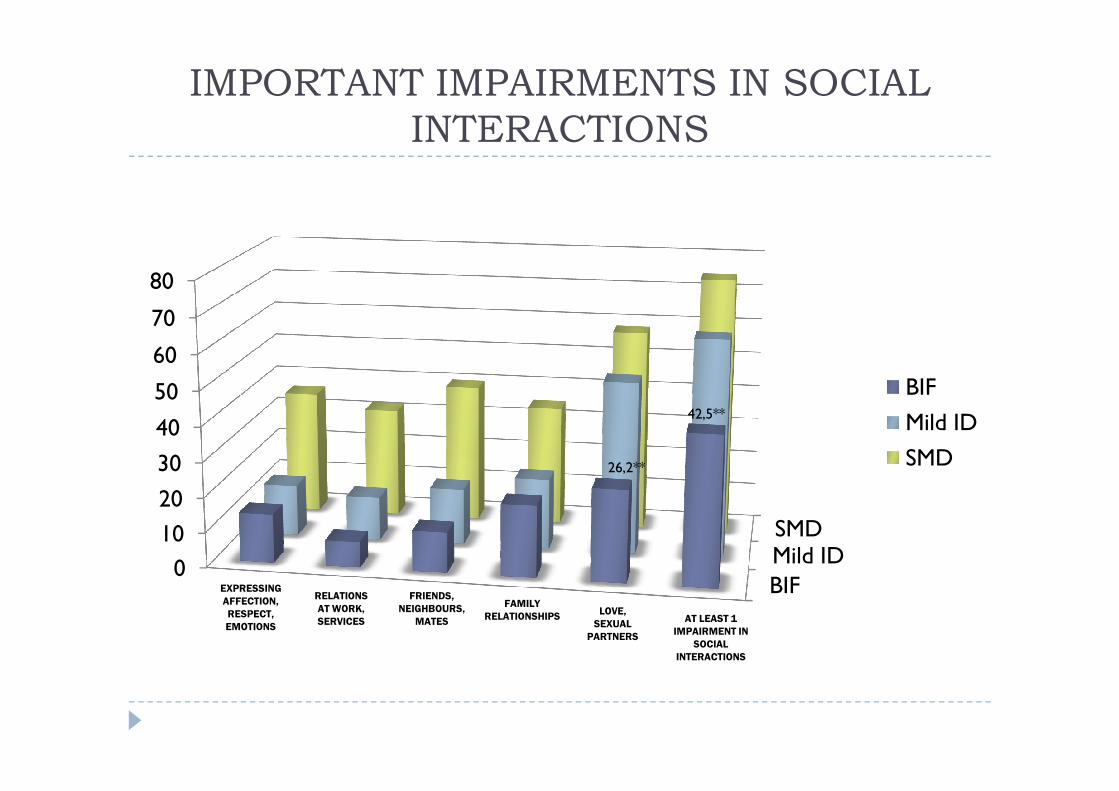
IMPORTANT IMPAIRMENTS IN SOCIAL
INTERACTIONS
50
60
70
80
BIF
BIF
Mild IDSMD
0
10
20
30
40
50
26,2**
42,5**
BIF
Mild ID
SMD
EXPRESSING
AFFECTION,
RESPECT,
EMOTIONS
FRIENDS,
NEIGHBOURS,
MATES
FAMILY
RELATIONSHIPSLOVE,
SEXUAL
PARTNERS
RELATIONS
AT WORK,
SERVICES AT LEAST 1
IMPAIRMENT IN
SOCIAL
INTERACTIONS
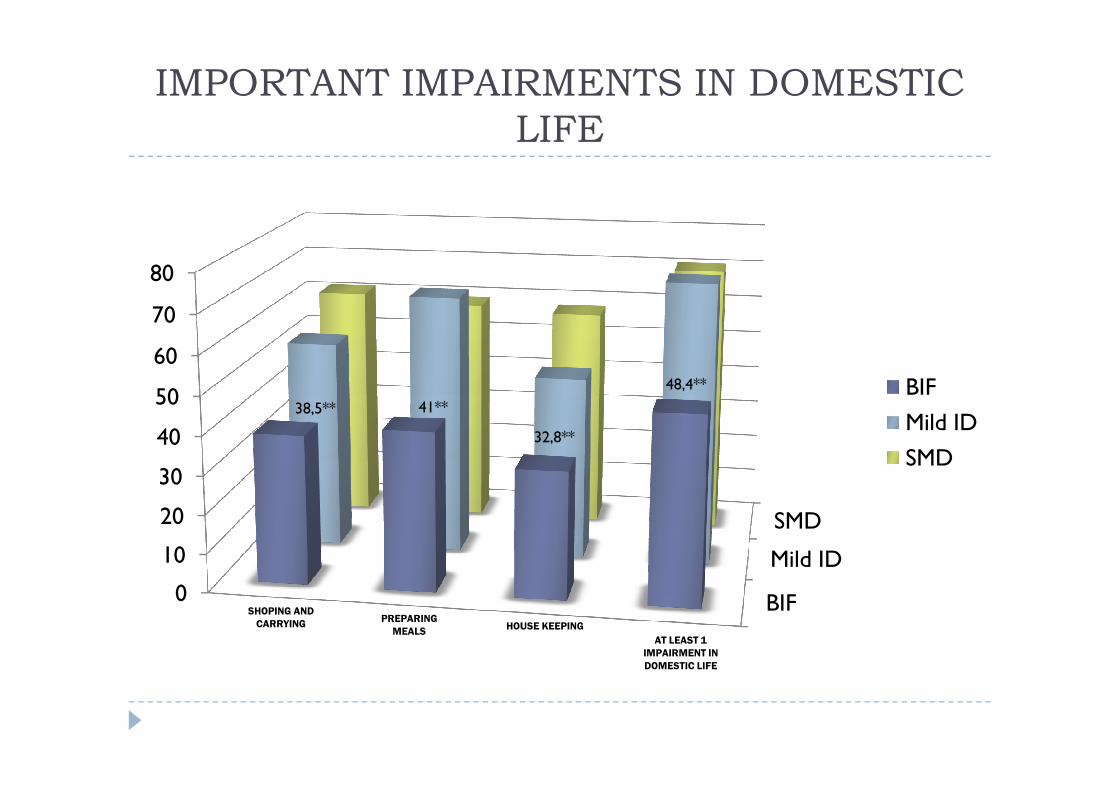
IMPORTANT IMPAIRMENTS IN DOMESTIC
LIFE
50
60
70
80
48,4** BIF
BIF
Mild ID
SMD
0
10
20
30
40
5038,5** 41**
32,8**
BIF
Mild ID
SMD
SHOPING AND
CARRYINGPREPARING
MEALSHOUSE KEEPING
AT LEAST 1
IMPAIRMENT IN
DOMESTIC LIFE
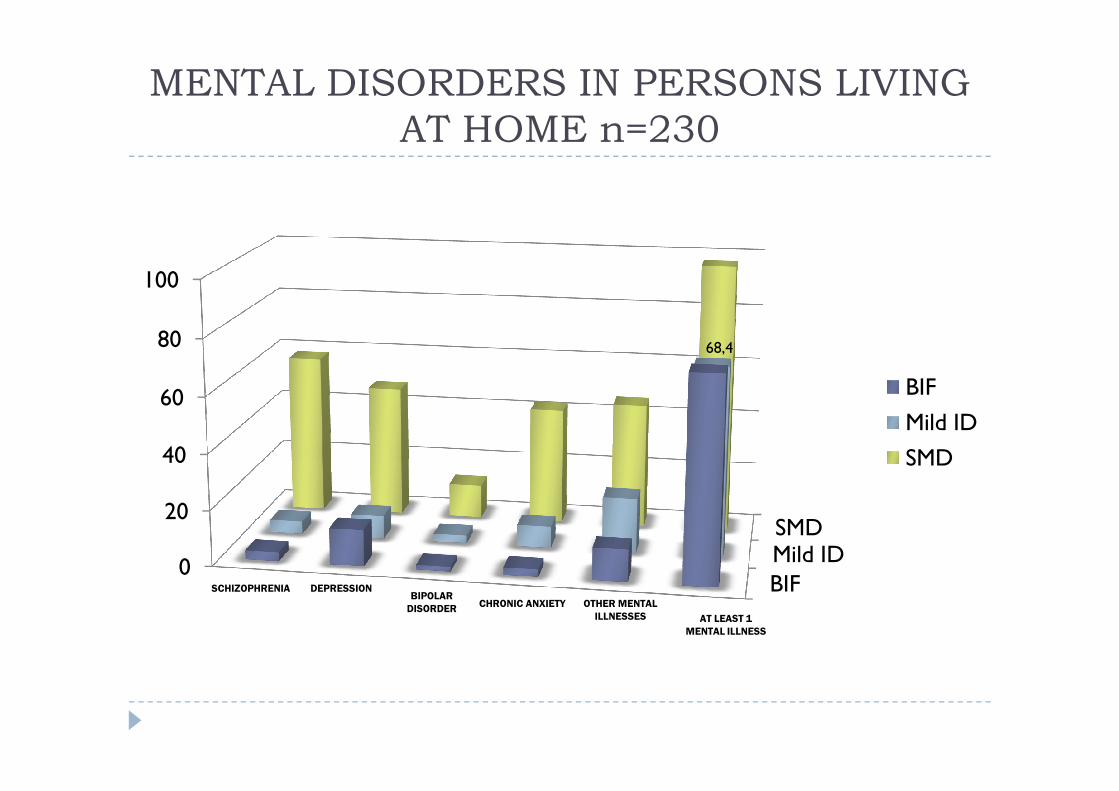
MENTAL DISORDERS IN PERSONS LIVING
AT HOME n=230
60
80
100
68,4
BIF
BIF
Mild IDSMD
0
20
40
60 BIF
Mild ID
SMD
SCHIZOPHRENIA DEPRESSIONBIPOLAR
DISORDEROTHER MENTAL
ILLNESSES
CHRONIC ANXIETY
AT LEAST 1
MENTAL ILLNESS
CONCLUSIONS
� There is a large number of persons classified as havingBIF that present limitations in important areas of functioning at the same level as persons with mild ID
� A high proportion of people with BIF living in thecommunity present some type of Mental Disorder
� Controversy about the delimitation of the entities of BIF and ID and the relative importance of theintelligence coefficient is supported by these results.
� Further research and better proffesional training are needed in order to dillucidate whether and when more intensive services or care should be available for persons with BIF.

THANK YOU