WOUNDED HEALER Clare Gerada A sense of belonging is vital ... WOUNDED HEALER Clare Gerada A sense of...
11
comment comment I n Malta, 21 September is a national holiday. It celebrates the country gaining independence from the UK in 1964. As well as being British I’m also Maltese, although I’ve never lived there, and in recent years (no doubt sparked by the trauma of Brexit) I’ve found myself identifying more with my heritage. I’ve obtained my Maltese passport and ID card and even gone as far as learning the language, an impossible mix of Arabic and Italian. This Independence Day, I was surrounded by other Maltese people at a central London hotel owned and run by a Maltese chain, and I felt that I belonged. Not just because the people looked like me (short and dark) or because we shared similar surnames (although Gerada is still uncommon), but because of our many connections. The population of Malta is tiny at around half a million, meaning that, given the large families, almost everyone is connected by family, village of birth, school, or work. Two minutes into a conversation with anyone Maltese you’ll find yourself comparing these connections, intensifying the sense of belonging. The hotel event also made me reflect on how important belonging has been for me in my role as a doctor: having shared experiences and a community behind you is vital for wellbeing. Becoming a doctor is more than just mechanically learning the vast amount of information needed to diagnose and treat disease—it’s about becoming one with the profession. If that sounds like a form of indoctrination, to some extent it is, which can be harmful if it leads to professional stigma around workplace stress or mental illness. However, many customs and practices that have developed over centuries, which doctors become familiar with through their training, also protect us in the job expected of us. From their first day at medical school, students learn these rules of belonging—not in formal lectures, ward rounds, and tutorials but as part of the informal, hidden curriculum that happens in the spaces between. Doctors’ medical identity is immensely strong, both in terms of the individual as a clinician and as a group (medicine), creating a total profession: doctor. The personal and professional become so intertwined that many doctors, even when retired or unable to work, still use the “Dr” title. Connections and belonging are important, then, for professional survival and mental wellbeing. Sadly, medical training and practice now make it harder to form them, which in my view contributes to the distress we see among doctors. Just as I’ve found ways to connect with my heritage in the face of Brexit stress, others in the medical community can do similar. We can, in our own way, all come together to connect with and support each other. Clare Gerada, GP partner, Hurley Group, London [email protected] Cite this as: BMJ 2019;367:l6029 the bmj | 26 October 2019 147 Connections and belonging are important for professional survival and mental wellbeing WOUNDED HEALER Clare Gerada A sense of belonging is vital for doctors “How many readers feel as scared as I do these days?” DAVID OLIVER “I’m connected to my community by many overlapping relationships” HELEN SALISBURY PLUS Widening the assisted dying debate; GP access balanced with continuity of care
Transcript of WOUNDED HEALER Clare Gerada A sense of belonging is vital ... WOUNDED HEALER Clare Gerada A sense of...

commentcomment
In Malta, 21 September is a national holiday. It celebrates the country gaining independence from the UK in 1964. As well as being British I’m also Maltese, although I’ve never lived there, and in recent years (no doubt sparked by the
trauma of Brexit) I’ve found myself identifying more with my heritage. I’ve obtained my Maltese passport and ID card and even gone as far as learning the language, an impossible mix of Arabic and Italian.
This Independence Day, I was surrounded by other Maltese people at a central London hotel owned and run by a Maltese chain, and I felt that I belonged. Not just because the people looked like me (short and dark) or because we shared similar surnames (although Gerada is still uncommon), but because of our many connections. The population of Malta is tiny at around half a million, meaning that, given the large families, almost everyone is connected by family, village of birth, school, or work. Two minutes into a conversation with anyone Maltese you’ll find yourself comparing these connections, intensifying the sense of belonging.
The hotel event also made me reflect on how important belonging has been for me in my role as a doctor: having shared experiences and a community behind you is vital for wellbeing. Becoming a doctor is more than just mechanically learning the vast amount of information needed to diagnose and treat disease—it’s about becoming one with the profession.
If that sounds like a form of indoctrination, to some extent it is, which can be harmful if it leads to professional stigma around workplace stress or mental illness. However, many customs and practices that have developed over centuries, which doctors become familiar with through their training, also protect us in the job expected of us. From their first day at medical school, students learn these rules of belonging—not in formal lectures, ward rounds,
and tutorials but as part of the informal, hidden curriculum that happens in the spaces between.
Doctors’ medical identity is immensely strong, both in terms of the individual as a clinician and as a group (medicine), creating a total profession: doctor. The personal and professional become so intertwined that many doctors, even when retired or unable to work, still use the “Dr” title.
Connections and belonging are important, then, for professional survival and mental wellbeing. Sadly, medical training and practice now make it harder to form them, which in my view contributes to the distress we see among doctors.
Just as I’ve found ways to connect with my heritage in the face of Brexit stress, others in the medical community can do similar. We can, in our own way, all come together to connect with and support each other.Clare Gerada, GP partner, Hurley Group, London [email protected] this as: BMJ 2019;367:l6029
the bmj | 26 October 2019 147
Connections and belonging are important for professional survival and mental wellbeing
WOUNDED HEALER Clare Gerada
A sense of belonging is vital for doctors
“How many readers feel as scared as I do these days?” DAVID OLIVER “I’m connected to my community by many overlapping relationships” HELEN SALISBURY PLUS Widening the assisted dying debate; GP access balanced with continuity of care

148 26 October 2019 | the bmj
The Australian state of Victoria has become the latest jurisdiction to legalise assisted dying, joining Belgium, Canada, Luxembourg, the Netherlands, and several
US states. While still illegal in the UK, there are signs assisted dying is inching towards legalisation. In March the Royal College of Physicians adopted a position of neutrality, and the BMA and Royal College of General Practitioners are to consult members on potentially changing their opposition.
Much of the public debate remains binary: yes or no. But this is a dangerous oversimplification. Assisted dying laws exist along a continuum. For example, in Oregon, it is only available to people who have a terminal illness expected to result in death within six months. In Belgium, assisted dying is available to people with unrelievable mental or physical suffering, regardless of life expectancy.
The most recent three bills to appear before the UK parliament have advocated a law similar to Oregon’s. But we argue that the six month rule is arbitrary, discriminatory, and difficult to implement
because clinicians’ predictions of life expectancy are frequently inaccurate.
Although there is a legal precedent in the UK for defining terminal illness as a prognosis of six months or less, there is growing opposition to the definition. A recent report by the All-Party Parliamentary Group for Terminal Illness described it as “outdated, arbitrary, and not based on clinical reality” and recommended the definition be uncoupled from a timeframe.
Not a rational positionCampaigners support for the six month rule may reflect that the “terminal” nature of illness is key to public support. The 2005 British Social Attitudes survey found that support for assisted dying fell from 80% to 45% for illnesses that were incurable and painful, but not terminal. The thought of assisted dying for people with less than six months to live may seem more palatable; but this is not a rational position.
The six month rule is discriminatory. Arguably, the people most likely to feel the need for assistance to die are those who face a longer period of suffering. Omid T, a British citizen, who chose an assisted death last year
in Switzerland rather than face the prospect of slow progressive deterioration from multi systems atrophy, would not have been eligible for assisted dying under a six month law. A law that excludes those with arguably the greatest need is unjustifiable.
It is estimated that by 2060 there will be almost 50 million people globally dying each year with palliative care needs, and that the number of people with dementia who experience serious health related suffering before they die will increase fourfold. How should society and policy makers respond to this escalation in suffering? Palliative care services are patchy: in England, investment varies from around £50 to more than £2000 per person per year. Significant investment is needed to ensure availability of palliative care for those who might benefit from it.
The assisted dying debate has long been characterised by extreme polarity. On the surface, our views on legalisation are fundamentally different. But having dug beneath the surface we have found that, while approaching the issue from opposite directions, we agree on much and share some
Within days of becoming prime minister, Boris Johnson signalled his intention to tackle the problem of access to GP appointments.
Shortening waiting times may seem a must-do for general practice, but equally important is providing access to the right person. Continuity of care has a wide range of positive effects such as lower mortality rates for some conditions, fewer hospital admissions and emergency department attendance, reduced system costs, higher patient and clinician satisfaction, and better clinical measures for some conditions.
With a national review of access to general practice services due to report this autumn, what is the best way to ensure continuity and access are given equal weight?
First, patients and carers need support to understand why a fast appointment with a stranger may not be better than waiting to see somebody you know. They also need to know how to achieve continuity when it is desired.
Second is the need for triage to assess patients and steer them to any member of a multi-professional team. Hundreds of practices use telephones or electronic questionnaires for an initial assessment. But questions remain about whether clinicians or non-clinicians should do the assessment, how to provide continuity, whether digital
For GPs’ patients continuity of care is as important as access
There is a need for triage to assess patients and steer them to any member of a multi-professional team
PERSONAL VIEW Katherine Sleeman, Iain Chalmers
Assisted dying: a six months limit is discriminatory and arbitary Much of the public debate around legalisation remains binary: yes or no. But this is a dangerous oversimplification, argue Katherine Sleeman and Iain Chalmers who, despite their apparent polar opposite views, have found they share many concerns
BMJ OPINION Rebecca Rosen

the bmj | 26 October 2019 149
essential concerns. Specifically, the use of evidence over anecdote, and rationality over hyperbole, to guide laws and decision making; the basic premise that laws should protect both personal choice and security; the need to cut inequalities, including access to palliative care for people with life limiting illnesses; the importance of dignity during as well as at the end of life; the importance of relieving suffering; and the limits of palliative care to relieve all suffering.
Although assisted dying is not yet legal in the UK, it is likely only a matter of time. Instead of arguing for or against, we need a more nuanced debate; to talk about what sort of law and what level of predicted risk is acceptable; which populations are most at risk; and how these harms can be mitigated. Katherine Sleeman, NIHR clinician scientist, honorary consultant in palliative medicine [email protected] Chalmers, retired health services researcher, King’s College London Cite this as: BMJ 2019;367:l6093
Last week Helen Salisbury wrote in her BMJ column about the fear of getting things wrong as a GP. Medical practice, by its nature and the disposition of
many doctors, has always entailed worry, however well trained or confident we are. But, if worry becomes more generalised anxiety or escalates to fear, the threat to our mental health or ability to function in demanding jobs seems stark.
The BMA recently published a report on what needs to change to improve NHS doctors’ working lives. Before reading it I’d become conscious of growing fear and anxiety, in myself and in colleagues. If I was running scared—a long serving doctor, secure in my job, with a series of national leadership roles behind me—then wasn’t this a wider problem?
There are some clear pressure points. These were elegantly categorised in a recent article in the BMA’s The Doctor as “systemic, endemic, interpersonal, environmental, and sociocultural.” A continually under-resourced, short staffed system, increasingly unable to meet demand, begins to feel unsafe. There’s relentless pressure to discharge people or prevent them being admitted. The sheer number of patients, means corner cutting and workarounds. We have to accept, balance, and mitigate risk to patients, even as systems outside hospital are under even more strain. We work on wards facing epic nursing shortfalls, often with inadequate IT or logistics. Even if our decisions and communication are sound, there’s much else we can’t control.
Add to this the rising complexity of patients, relentless political
and media scrutiny, and growing public expectation and dissatisfaction, and anxiety seems inevitable.
Doctors increasingly fear blame or formal complaints, regulatory action, or loss of livelihood or reputation. We may fear for our sleep, mental or physical health, or ability to keep going. We may worry about the job’s impact on our family. Fear of inability to sustain our career into our 60s is common. We may also fear losing our skills, not having the time to keep them up to date, and no longer being safe in our practice.
Maybe we also fear that, if we do have health problems or perhaps resort to addictive behaviours to cope, this will come to light and damage us further. Endemic staffing gaps and our loyalty to patients and colleagues are strong imperatives to keep going when perhaps we should not. When generalised chronic anxiety takes hold, some worries can be blown out of proportion so we lose peace of mind—not from what has happened but from what we imagine might happen.
The BMA’s Chaand Nagpaul says the NHS now has a culture “where blame stifles learning, contributing to the vicious cycle of low morale so staff leave. This unsafe, underfunded environment is as damaging for patients as it is for doctors.”
The evidence set out in the BMA report supports that view. I wonder how many readers feel as scared as I do these days, and how we doctors might help solve the
problem of fear.David Oliver, consultant, geriatrics and
acute general medicine, Berkshire [email protected] Twitter @mancunianmedicCite this as: BMJ 2019;367:l6030
triage creates inequalities, acceptability to patients, and impact on workload.
Third, booking systems can be designed to combine rapid access and continuity. This requires enough clinical staff to cover both. Some practices with total telephone triage have built in systems that let patients see their usual doctor, but this is not yet universal.
Finally, scale is important. A case study conducted by the Nuffield Trust describes the pivotal role of receptionists, who use their knowledge of complex patients and the interests of clinicians, and their collegial relationships to nuance appointment booking and promote continuity for selected patients. Rebecca Rosen, senior fellow in health policy, the Nuffield Trust
Instead of arguing for or against, we need a more nuanced debate
I wonder how many readers feel as scared as I do these days
BMJ OPINION Rebecca Rosen
ACUTE PERSPECTIVE David Oliver
Fear in medical practice

150 26 October 2019 | the bmj
“I saw you out running the other day, doc.” Given the choice, would you prefer to work in a practice near where you live or opt for the anonymity
that distance provides? Laziness won out over privacy when I joined my practice, so I live in the community I serve, and my commute is three minutes by bike.
The disadvantages are obvious: it’s harder to keep public and private personas separate. If I want to let my hair down I need to put a little distance between myself and my surgery, or I risk comments the following week about my graceless dancing or ill advised Catwoman fancy dress. As doctors we’re expected to practise what we preach, so it’s good to be seen exercising but bad to overindulge in alcohol in public. And a poker face is necessary when gossip at the school gates touches on people or situations you know about from the surgery. When you’re privy to personal details—not only physical and mental illnesses but also domestic violence, debt, and despair—some social gatherings can be uncomfortable.
Not everyone chooses to live and work in the same neighbourhood. In years gone by many GPs consulted in their front room, lived at their surgery, and were on call day and night. Although our long hours culture can make home seem like just somewhere to sleep, I’m still grateful that “living above the shop” is no longer the norm.
One worry is that patients may try to consult with you in local shops. This rarely happens as most people respect the unwritten rules. On the occasions I’ve been present at a minor accident I’ve found the gratitude offered for simple advice is disproportionate to the effort involved.
When I was a student a friend of mine worked as a GP in a rough part of Amsterdam. Walking home one evening, she was accosted by a stranger, but help rapidly arrived and her potential mugger was sent packing with cries of, “Leave her alone, she’s our doctor!” In my neighbourhood I’m unlikely to need that kind of protection, but I do benefit from that sense of belonging.
It’s a feeling of connectedness to the community because of the multiple overlapping relationships with my neighbours. Over the years I’ve helped them look after their health, while they’ve taught my children at school, offered advice about vegetables down at the allotments, or stayed open all hours for when I run out of milk.
If I ever do feel the need to escape there’s the option of becoming a dis-located doctor in cyberspace, consulting by smartphone app—but for now I’m grateful for community, continuity, and that sense of belonging.Helen Salisbury, GP, Oxford
[email protected] Twitter @HelenRSalisbury
Cite this as: BMJ 2019;367:l6031
Listen and subscribe to The BMJ podcast on Apple Podcasts, Spotify, and other major podcast apps.
Edited by Kelly Brendel, deputy digital content editor, The BMJ
Direct-to-consumer genetic tests and disease riskDirect-to-consumer genetic tests are becoming more popular but are there problems with them? This podcast explores their limitations.“Many genetic variations are only part of a wider picture,” says Rachel Horton, a clinical training fellow. “There are other factors—like your age and environmental risk factors such as smoking—that might influence whether it causes a condition in a particular person. But often the perception is very much if you’ve got this variant that will happen.”As Anneke Lucassen, chair of the British Society of Genetic Medicine, explains, “The more we look at healthy people, the more we realise that if you look at their genetic code you might find all sorts of variation that has been published as being quite nasty and predictive, but they’ve been living into old age without any signs of that.”
Statins for primary preventionA recent analysis article looked at the evidence we have for changing clinical guidelines to increase the number of healthy people who could be eligible for statins. In this podcast, one of the authors, Paula Byrne, discusses the uncertainty that remains about the benefits of using statins for primary prevention. “It would empower both doctors and patients if there was more acceptance of the uncertainty. The debate has become very polarised and people are almost frightened to stake a position on it. If we’re really honest and say this is the best evidence we have, this is the best we can do, and this is the best I can advise you, that would be really helpful.”
If I want to let my hair down I need to put a little distance between myself and my surgery
PRIMARY COLOUR Helen Salisbury
Living above the shopLATEST PODCASTS
the bmj | 26 October 2019 151
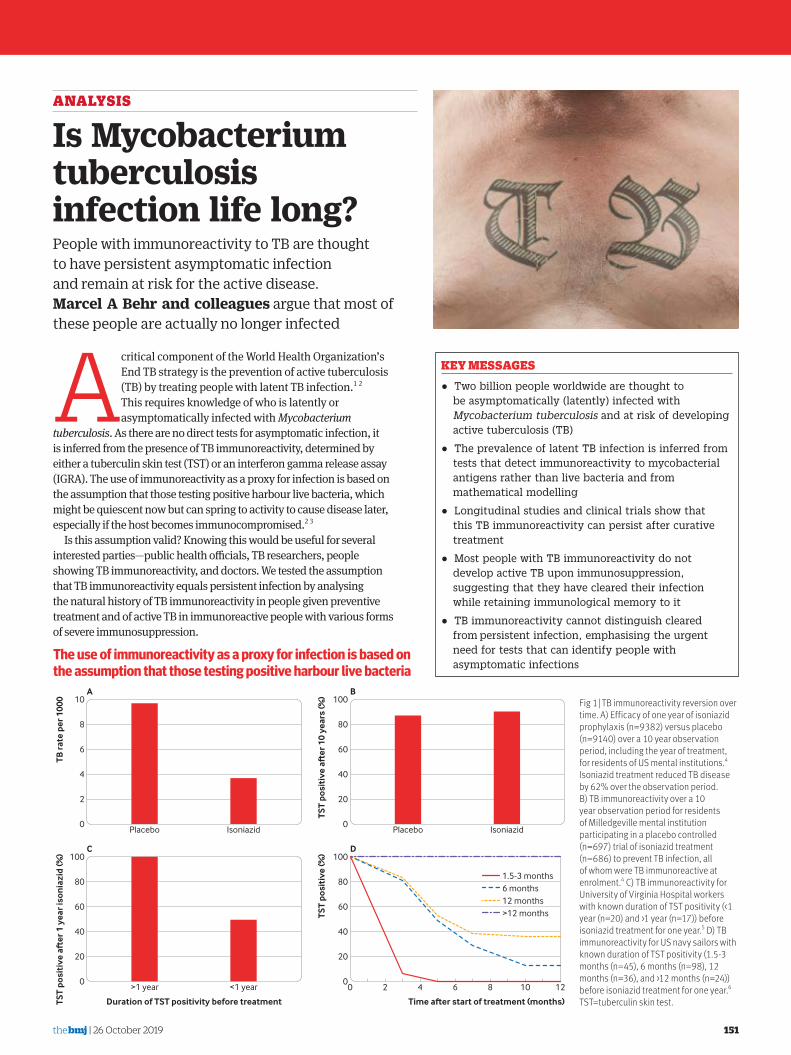
A critical component of the World Health Organization’s End TB strategy is the prevention of active tuberculosis (TB) by treating people with latent TB infection.1 2 This requires knowledge of who is latently or asymptomatically infected with Mycobacterium
tuberculosis. As there are no direct tests for asymptomatic infection, it is inferred from the presence of TB immunoreactivity, determined by either a tuberculin skin test (TST) or an interferon gamma release assay (IGRA). The use of immunoreactivity as a proxy for infection is based on the assumption that those testing positive harbour live bacteria, which might be quiescent now but can spring to activity to cause disease later, especially if the host becomes immunocompromised.2 3
Is this assumption valid? Knowing this would be useful for several interested parties—public health officials, TB researchers, people showing TB immunoreactivity, and doctors. We tested the assumption that TB immunoreactivity equals persistent infection by analysing the natural history of TB immunoreactivity in people given preventive treatment and of active TB in immunoreactive people with various forms of severe immunosuppression.
KEY MESSAGES
• Two billion people worldwide are thought to be asymptomatically (latently) infected with Mycobacterium tuberculosis and at risk of developing active tuberculosis (TB)
• The prevalence of latent TB infection is inferred from tests that detect immunoreactivity to mycobacterial antigens rather than live bacteria and from mathematical modelling
• Longitudinal studies and clinical trials show that this TB immunoreactivity can persist after curative treatment
• Most people with TB immunoreactivity do not develop active TB upon immunosuppression, suggesting that they have cleared their infection while retaining immunological memory to it
• TB immunoreactivity cannot distinguish cleared from persistent infection, emphasising the urgent need for tests that can identify people with asymptomatic infections
ANALYSIS
Is Mycobacterium tuberculosis infection life long?People with immunoreactivity to TB are thought to have persistent asymptomatic infection and remain at risk for the active disease. Marcel A Behr and colleagues argue that most of these people are actually no longer infected
A
TB ra
te p
er 1
000
Placebo Isoniazid
1.5-3 months6 months12 months>12 months
0
40
60
100
80
20
0
4
6
10
8
2
B
TST
posi
tive
a
er 1
0 ye
ars
(%)
Placebo Isoniazid
C
TST
posi
tive
a
er 1
yea
r iso
nia
zid
(%)
>1 year <1 year0
40
60
100
80
20
0
40
60
100
80
20
D
Time aer start of treatment (months)Duration of TST positivity before treatment
TST
posi
tive
(%)
0 2 4 6 8 10 12
Fig 1 | TB immunoreactivity reversion over time. A) Efficacy of one year of isoniazid prophylaxis (n=9382) versus placebo (n=9140) over a 10 year observation period, including the year of treatment, for residents of US mental institutions.4 Isoniazid treatment reduced TB disease by 62% over the observation period. B) TB immunoreactivity over a 10 year observation period for residents of Milledgeville mental institution participating in a placebo controlled (n=697) trial of isoniazid treatment (n=686) to prevent TB infection, all of whom were TB immunoreactive at enrolment.4 C) TB immunoreactivity for University of Virginia Hospital workers with known duration of TST positivity (<1 year (n=20) and >1 year (n=17)) before isoniazid treatment for one year.5 D) TB immunoreactivity for US navy sailors with known duration of TST positivity (1.5-3 months (n=45), 6 months (n=98), 12 months (n=36), and >12 months (n=24)) before isoniazid treatment for one year.6 TST=tuberculin skin test.
The use of immunoreactivity as a proxy for infection is based on the assumption that those testing positive harbour live bacteria

152 26 October 2019 | the bmj
Immunoreactivity does not reflect continued infectionFor TB immunoreactivity to be a reliable proxy for persistent TB infection, it must track faithfully with infection. This means that people whose infection is cured should become non-reactive. Multiple studies show that this is not the case. The large US isoniazid chemoprophylaxis trial conducted between 1956 and 1966 showed that treatment of people with TB immunoreactivity (TST results ≥10 mm) for one year lowered the incidence of active TB by 60-70% over the next nine years (fig 1A).4 Yet the treated people remained positive on TST up to nine years after treatment (fig 1B), showing that TB immunoreactivity can outlast elimination of infection by at least nine years.
This finding was validated by two studies that provided mechanistic insights. Among hospital employees, Atuk and Hunt showed that patients who had positive results on TSTs for more than a year before treatment remained so after treatment, whereas 50% of those who had been positive for less than a year became negative or had smaller TST induration size (fig 1C).5 Houk and colleagues’ study of US navy sailors treated with isoniazid for TB infection provided more granularity.6 All who were immunoreactive for more than a year before treatment remained so after treatment; among the remainder, those who were immunoreactive the longest were most likely to remain so after isoniazid treatment (fig 1D). These findings are consistent with the development of a lasting immunological memory that becomes more robust with longer exposure to antigen. Finally, the finding that TB immunoreactivity outlasts infection holds in the context of active TB—people remain immunoreactive after completing treatment with highly effective multidrug regimens.7 8
So TB immunoreactivity is not a marker for the presence of continued TB infection. Rather it serves as a sign of having been infected with TB but does not reflect the outcome—bacterial clearance versus persistence.
Immunosuppression and risk of TBImmunosuppression—through HIV infection or medical intervention (tumour necrosis factor (TNF) inhibition, solid organ transplantation, and haematopoietic stem cell transplantation)—is associated with an increased risk of active TB in multiple studies. We used these studies to infer the frequency of persistent infection in people showing TB immunoreactivity (see supplementary table 1 and supplementary methods for details on data sources and analysis).
TNF inhibitionTNF is known to be a potent determinant of resistance to TB in animal disease models.9 10 The increased risk of TB in humans receiving the anti-TNF antibody infliximab was shown first in 2001 in a large US patient cohort11 and then in three subsequent studies in the US, France, and Spain (supplementary table 1 and supplementary methods).12-14 In these studies, performed before isoniazid prophylaxis was routinely given to TB immunoreactive patients, 0.6-4.9% of people with positive TSTs developed TB; the rest remained free of TB over the next 1.5 to 3 years.11-14 Because the majority of cases occurred early after starting anti-TNF treatment (median time of three months), TB probably resulted from pre-existing remote infection rather than from newly acquired infection. Together, these analyses show that >95% of people with positive TSTs do not have quiescent bacteria that can be roused by TNF suppression.
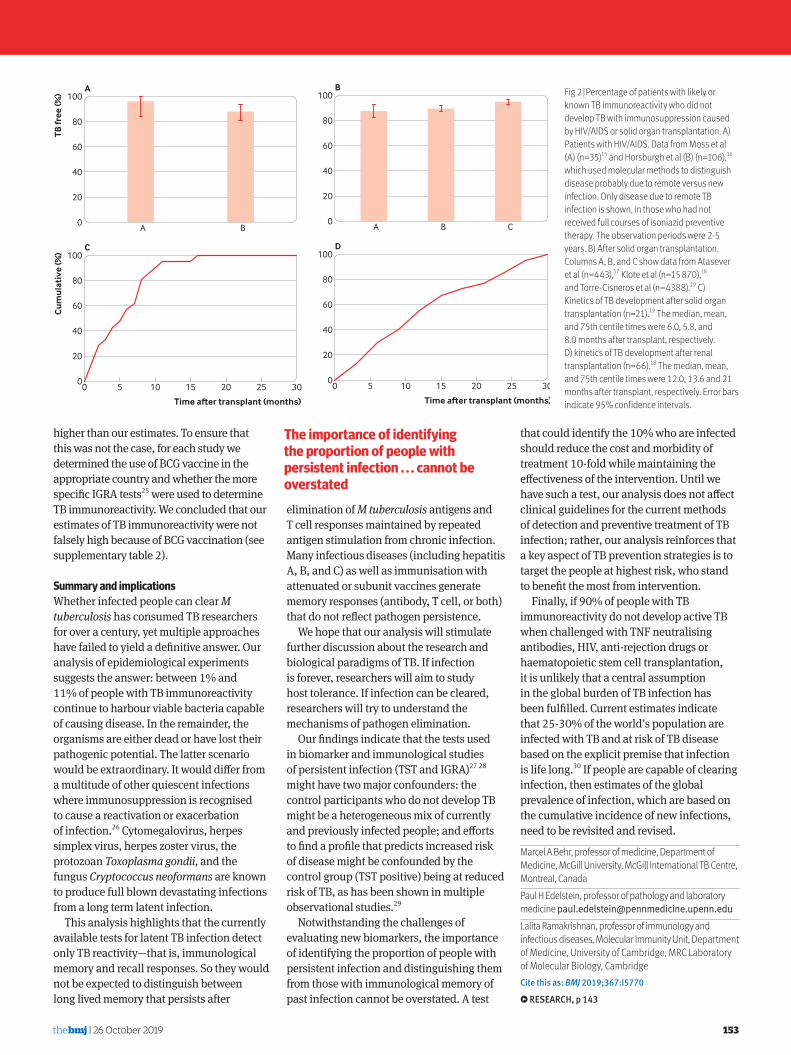
HIVCell mediated immunity, especially that mediated by CD4+ T lymphocytes, is another critical defence against TB, as shown by the increased rates of TB in people with HIV. Two studies on TB in patients with HIV were done at a time when preventive TB treatment was not routinely given to patients with HIV who were TB immunoreactive. Both studies used bacterial genotyping to distinguish newly acquired from pre-existing remote TB infection, showing that 88.7% and 97.5% of people with positive TSTs remained free of TB from their remote infection over a five year period (fig 2A).15 16
Solid organ transplantationLong term medical suppression of cell mediated immunity is the cornerstone of preventing rejection after allogeneic organ transplantation. Three studies of solid organ transplant recipients who did not receive isoniazid prophylaxis were done in
Spain, Turkey, and the US. Most of these patients remained free of TB (88.7-95.6%) over observation periods of up to 2.5 years (fig 2B).17-19 The maximum reported rate of TB in people with positive TSTs was 11.3%. TB occurred later in the transplant population than in the population receiving TNF inhibition, with a median of six months for a cohort comprising mostly non-renal transplants (67%) and 12 months for renal transplants (from a different study of exclusively renal transplants) (figs 2C and 2D). This could reflect a later temporal role for cell mediated immunity in the control of TB. The shorter time to TB in non-renal transplant recipients might reflect the higher degree of immunosuppression used. Some of the later cases might have been from newly acquired infection after the transplant, in which case the estimated risk attributable to remote infection would be even lower.
Haematopoietic stem cell transplantationHaematopoietic stem cell transplantation results in the most profound and rapid immunosuppression affecting both innate and adaptive arms of immunity; this is the most likely form of immunosuppression to cause any quiescent M tuberculosis to become active. We identified four cohorts of TB immunoreactive people in India, South Korea, Taiwan, and the US who underwent haematopoietic stem cell transplantation without receiving isoniazid prophylaxis.20-23 The proportion of these cohorts that developed TB was less than 10%. In the US cohort, none of 29 participants with TB immunoreactivity developed TB after a total of 89 person years of observation. The three other studies were performed in countries with intermediate to high TB burden, yet only 7-10% of people developed TB. The median times to TB development after transplantation were 258, 368, and 445 days for the Indian, South Korean, and Taiwanese studies (fig 4B), respectively, indicating that some of these cases might have been due to new infection rather than activation of their remote infection.
BCG and false positivesBCG vaccination can result in false positive results on TSTs in those vaccinated when older than 1 year of age.24 This could have falsely inflated the number of people estimated to be TB immunoreactive in the studies that we analysed. If so, the proportion of TB immunoreactive people who developed TB associated with immunosuppression would have been
US sailors were treated in the late 1960s with isoniazid for TB infection
the bmj | 26 October 2019 153
higher than our estimates. To ensure that this was not the case, for each study we determined the use of BCG vaccine in the appropriate country and whether the more specific IGRA tests25 were used to determine TB immunoreactivity. We concluded that our estimates of TB immunoreactivity were not falsely high because of BCG vaccination (see supplementary table 2).
Summary and implicationsWhether infected people can clear M tuberculosis has consumed TB researchers for over a century, yet multiple approaches have failed to yield a definitive answer. Our analysis of epidemiological experiments suggests the answer: between 1% and 11% of people with TB immunoreactivity continue to harbour viable bacteria capable of causing disease. In the remainder, the organisms are either dead or have lost their pathogenic potential. The latter scenario would be extraordinary. It would differ from a multitude of other quiescent infections where immunosuppression is recognised to cause a reactivation or exacerbation of infection.26 Cytomegalovirus, herpes simplex virus, herpes zoster virus, the protozoan Toxoplasma gondii, and the fungus Cryptococcus neoformans are known to produce full blown devastating infections from a long term latent infection.
This analysis highlights that the currently available tests for latent TB infection detect only TB reactivity—that is, immunological memory and recall responses. So they would not be expected to distinguish between long lived memory that persists after
elimination of M tuberculosis antigens and T cell responses maintained by repeated antigen stimulation from chronic infection. Many infectious diseases (including hepatitis A, B, and C) as well as immunisation with attenuated or subunit vaccines generate memory responses (antibody, T cell, or both) that do not reflect pathogen persistence.
We hope that our analysis will stimulate further discussion about the research and biological paradigms of TB. If infection is forever, researchers will aim to study host tolerance. If infection can be cleared, researchers will try to understand the mechanisms of pathogen elimination.
Our findings indicate that the tests used in biomarker and immunological studies of persistent infection (TST and IGRA)27 28 might have two major confounders: the control participants who do not develop TB might be a heterogeneous mix of currently and previously infected people; and efforts to find a profile that predicts increased risk of disease might be confounded by the control group (TST positive) being at reduced risk of TB, as has been shown in multiple observational studies.29
Notwithstanding the challenges of evaluating new biomarkers, the importance of identifying the proportion of people with persistent infection and distinguishing them from those with immunological memory of past infection cannot be overstated. A test
that could identify the 10% who are infected should reduce the cost and morbidity of treatment 10-fold while maintaining the effectiveness of the intervention. Until we have such a test, our analysis does not affect clinical guidelines for the current methods of detection and preventive treatment of TB infection; rather, our analysis reinforces that a key aspect of TB prevention strategies is to target the people at highest risk, who stand to benefit the most from intervention.
Finally, if 90% of people with TB immunoreactivity do not develop active TB when challenged with TNF neutralising antibodies, HIV, anti-rejection drugs or haematopoietic stem cell transplantation, it is unlikely that a central assumption in the global burden of TB infection has been fulfilled. Current estimates indicate that 25-30% of the world’s population are infected with TB and at risk of TB disease based on the explicit premise that infection is life long.30 If people are capable of clearing infection, then estimates of the global prevalence of infection, which are based on the cumulative incidence of new infections, need to be revisited and revised.
Marcel A Behr, professor of medicine, Department of Medicine, McGill University, McGill International TB Centre, Montreal, CanadaPaul H Edelstein, professor of pathology and laboratory medicine [email protected] Lalita Ramakrishnan, professor of immunology and infectious diseases, Molecular Immunity Unit, Department of Medicine, University of Cambridge, MRC Laboratory of Molecular Biology, Cambridge Cite this as: BMJ 2019;367:l5770
Ж RESEARCH, p 143
A
TB fr
ee (%
)
A B0
40
60
100
80
20
TB fr
ee (%
)
A B C0
40
60
100
80
20
B
C
0
40
60
100
80
20
D
Time aer transplant (months)
Cu
mu
lati
ve (%
)
0 5 10 15 20 25 300
40
60
100
80
20
Time aer transplant (months)
Cu
mu
lati
ve (%
)
0 5 10 15 20 25 30
A
TB fr
ee (%
)
A B0
40
60
100
80
20
TB fr
ee (%
)
A B C0
40
60
100
80
20
B
C
0
40
60
100
80
20
D
Time aer transplant (months)
Cu
mu
lati
ve (%
)
0 5 10 15 20 25 300
40
60
100
80
20
Time aer transplant (months)
Cu
mu
lati
ve (%
)
0 5 10 15 20 25 30
Fig 2 | Percentage of patients with likely or known TB immunoreactivity who did not develop TB with immunosuppression caused by HIV/AIDS or solid organ transplantation. A) Patients with HIV/AIDS. Data from Moss et al (A) (n=35)15 and Horsburgh et al (B) (n=106),16 which used molecular methods to distinguish disease probably due to remote versus new infection. Only disease due to remote TB infection is shown, in those who had not received full courses of isoniazid preventive therapy. The observation periods were 2-5 years. B) After solid organ transplantation. Columns A, B, and C show data from Atasever et al (n=443),17 Klote et al (n=15 870),18 and Torre-Cisneros et al (n=4388).19 C) Kinetics of TB development after solid organ transplantation (n=21).19 The median, mean, and 75th centile times were 6.0, 5.8, and 8.0 months after transplant, respectively. D) kinetics of TB development after renal transplantation (n=66).18 The median, mean, and 75th centile times were 12.0, 13.6 and 21 months after transplant, respectively. Error bars indicate 95% confidence intervals.
The importance of identifying the proportion of people with persistent infection . . . cannot be overstated

154 26 October 2019 | the bmj
BMJ OPINION Anthony Harries
In the absence of a true test for latent TB we need shorter, safer preventive treatmentsTreating latent tuberculosis infection (LTBI) is a key component of the WHO’s End TB strategy, which aims to end the TB epidemic by 2030. This neglected but vital intervention was given further emphasis in September 2018 at the UN high level meeting on TB, where world leaders committed to treating at least 30 million people for LTBI by 2022, including 4 million children under 5 years of age, 20 million household contacts of people affected by TB, and 6 million people with HIV.
In this context, Marcel Behr and colleagues continue their thought provoking journey of questioning established dogma (p 151). In 2018, they provided robust evidence to support the assertion that people infected with M tuberculosis tend to progress to disease over an incubation period of two months to two years rather than over their lifetime. In a new Analysis, they go on to question the widely held assumption that M tuberculosis infection is for life.
As the authors point out, there is no perfect way to directly diagnose LTBI. The diagnosis is made in people with no evidence of active TB by measuring the immunological response to M tuberculosis antigens using the tuberculin skin test or interferon gamma release assay. Infection is inferred rather than proven.
Behr and colleagues test the assumption that TB immunoreactivity is the same as lifelong infection in two ways: by analysing studies of the natural history of TB immunoreactivity in people given treatment and by
assessing the risk of active TB in immunoreactive people who develop severe immunosuppression.
Data from longitudinal studies and clinical trials show that immunoreactivity persists after successful treatment of either LTBI or active TB, with persistence being most prolonged in those with the longest duration of immunoreactivity before starting treatment. Epidemiological studies also show that most people with TB immunoreactivity who become severely immunosuppressed owing to HIV, solid organ transplantation, haematopoietic stem cell transplantation, or tumour necrosis factor inhibition remain free of active TB.
Persuasive argumentWhat should we take from this new analysis? In terms of understanding LTBI, Behr and colleagues’ argument is persuasive that TB immunoreactivity is a sign of having been infected with M tuberculosis and not a marker of continued infection. Their analysis suggests that about 10% of people with TB immunoreactivity harbour viable organisms capable of causing disease in the right circumstances, such as immunosuppression; in the remainder, M tuberculosis bacteria are likely to be permanently dormant or dead.
This perspective reinforces the urgent need for clinically useful and affordable biomarkers that can clearly distinguish between persistent infection and immunological memory of a past infection. The journey
of discovery, development, and deployment of a biomarker that can guide clinical decisions is not likely to be quick or easy. But it is a journey that must be taken, and if successful would enable precise identification of those who are truly infected and at most risk of developing active TB.
In the meantime, we have no choice but to continue to treat those with LTBI if we want to honour our promises to end TB. The current preventive policy is to treat those at the highest risk of TB, such as people with HIV or young household contacts of a person with TB, without testing for LTBI. For other high risk groups, including patients with silicosis, patients in renal failure, and certain vulnerable groups, the preventive policy is to systematically test for LTBI before treatment. We need to recognise, however, we might be treating many people who do not require this intervention because they do not have latent infection. This would be acceptable if the treatment was short and entirely safe. Unfortunately, this is not the case.
Isoniazid is the current drug of choice for treating LTBI, often for six months, but it can cause peripheral neuropathy or drug induced hepatitis, which if unrecognised or identified too late can be fatal. Shorter and safer alternative regimens are now available, the most attractive being a three month course of weekly rifapentine and isoniazid (12 doses). Two important hurdles in making this regimen widely available are country specific approval and the huge cost of rifapentine.
TB programmes need to embrace new shorter treatment durations, and global advocacy and activism are needed to make the drugs affordable in the countries where they are most needed. At the same time, TB programmes need to agitate for an easy to use and inexpensive biomarker that truly identifies LTBI.
Anthony Harries, senior adviser, International Union Against Tuberculosis and Lung Disease, Paris, and honorary professor, London School of Hygiene and Tropical Medicine
TB programmes need to agitate for an easy to use and inexpensive biomarker that truly identifies LTBI
The Mantoux tuberculin skin test measures a person’s immunilogical response to antigens—inferring rather than proving infection
SCIE
NCE
SO
URCE
/SPL

the bmj | 26 October 2019 155
LETTERS Selected from rapid responses on bmj.com
Mahase mentions that obesity among nurses and unregistered care workers is “concerning” (Seven Days in Medicine, 15 June). Although senior leaders should lead through example, I think that all healthcare staff should become exercise champions.
2015 NICE guidance proposed quality statements on physical activity for NHS staff, patients, and carers. But about 70% of respondents to the 2018 NHS staff survey said that their organisation did not take positive action on health and wellbeing.
Muir Gray said that we should “get GPs moving themselves.” By developing a passion for healthy living, staff will not only
become healthier but will also be better placed to promote the lifestyle to others.
Instead of top down policy documents, we should be supporting keen individuals in hospitals and communities, regardless of rank or background, to drive local movements. Those who are the most passionate about exercise should be given the platform to lead. Mairead McErlean clinical pharmacist , London Cite this as: BMJ 2019;367:l5998
Improve pavements and cycle routes To help patients take more exercise we need to make it easier for them. This is not a medical intervention directly, but we can try to motivate local and national governments. In many countries, people are put off public transport, even though walking to a bus stop or a railway station would be a convenient way of exercising. Roads and cars are subsidised, but public transport isn’t. Pavements and cycle routes are afterthoughts and are often diverted to make way for motorised vehicles. We need to convince governments that changing their policies are win-win decisions, by improving health, reducing pollution, and making living environments much more pleasant. Michael Peel, GP , Weston-super-Mare Cite this as: BMJ 2019;367:l5997
“Get a note from your doctor” Building exercise into daily routines is useful, but some people like to go to a gym. Particularly after an illness, people might feel safer exercising in controlled surroundings than dealing with, for example, weather and uneven footpaths.
Sadly, many gyms require people (especially those who have been ill or have common conditions such as hypertension) to obtain a letter from a doctor to absolve the gym of liability if the gym member becomes unwell while exercising. The familiar “get a note from your doctor” situation.
This puts people in the position of having to ask overworked GPs for a note and possibly (as it isn’t NHS work or part of a GP’s contractual duties) having to pay for it, which is a barrier to them accessing the benefits of exercise in the gym.
Has a strategy been devised to get around this? Or to prevent gyms from requiring such notes? Peter M B English, public health physician , Epsom Cite this as: BMJ 2019;367:l5992
Authors’ reply
We agree that physician influence on physical activity is moderate at best, as seen
in NICE guidance. The effect of environment is clearly outlined in UK government documents, including Everybody Active, Every Day , which includes sections on active society and active environment. The effect of physician advice can be seen in smoking cessation, where it is only one element of many—we anticipate that a multiagency approach will be required to support doctors’ efforts in consultations.
Patients having to request fitness assessments before attending a gym is inappropriate. Not all gyms require letters, and there are usually options tailored for all people. “Social prescribing” and active lifestyle coordinators can help patients access suitable physical activity.
We agree that making physical activity more accessible is key and that a healthy workforce is an integral part of a physical activity strategy, as stated in Everybody Active, Every Day . NICE guidance clearly outlines physical activity in the work environment, which includes the NHS. Christine Haseler, GP , Gloucester ; Ranulf Crooke, GP , Fairford; Tobias Haseler, GP specialty trainee , London Cite this as: BMJ 2019;367:l6065
EXERCISE AND PATIENTSLETTER OF THE WEEK
How doctors can help to promote physical activity
21 September 2019366:337-378 No 8214 | ISSN 1759-2151
Understanding vaping harms p 349
The rise of counterfeit drugs p 350
Flawed cancer drug evidence p 354
Hypertension in pregnancy p 367
1 CPD hour in the education section
Physical activity: are we hypocrites? Haseler et al’s article on discussing physical activity with patients is helpful (Practice Pointer, 21 September). Doctors of all specialties should be more proactive in encouraging patients to exercise more, eat more healthily, and lose weight. Every presentation—be it to a GP, the emergency department, or a medical ward—is an opportunity to promote physical activity. I like the “ask-assess-advise” strategy we sometimes use for smoking cessation. The non-judgmental phrasing is helpful, and I will incorporate it into my practice.
As I read, however, I realised that my conscience was saying: “You don’t do 150 minutes of exercise a week.” We would not expect a patient to take advice from someone claiming to be a doctor who had no medical qualifications. Can we really expect a patient to follow this advice if we are not meeting the mark? I suspect this hypocrisy is part of the reason we often do not offer this advice to our patients.
NHS employers and postgraduate training programmes should do more to facilitate healthy lifestyles for staff; a weekly rostered exercise break would show society that the NHS was serious about physical exercise. I would not be surprised if it also led to reduced stress and increased staff productivity. David J Jones, acute care common stem specialty trainee year 2 , Margate
Cite this as: BMJ 2019;367:l5985
EXERCISE CHAMPIONS
Let passionate staff take the lead

the bmj | 26 October 2019 167
OBITUARIES
Kenneth Michael CitronConsultant physician (b 1925; q Guy’s Hospital, London, 1948; MD, FRCP), died from heart failure on 11 September 2019Kenneth Michael Citron was appointed consultant physician at the Royal Brompton Hospital and honorary senior lecturer at the cardiothoracic institute in 1959. He chaired a series of multicentre controlled clinical trials of anti-tuberculosis chemotherapy, which established short course chemotherapy in the UK. He was chairman of the Joint Tuberculosis Committee, adviser in tuberculosis and respiratory medicine to the chief medical officer at the Department of Health, and was involved with critical decisions about the future of the schools’ vaccination programme in the 1980s, when tuberculosis was re-emerging in the UK. He retired from the NHS in 1990. Kenneth always enjoyed life to the full. He leaves his wife, Sue; a son; a daughter in law; and four grandchildren.Janet H Darbyshire Cite this as: BMJ 2019;366:l5620
Varun Kumar SinghNeurologist (b 1948; q 1974; MD, MRCP), died from pneumonia and septicaemia on 21 February 2019Varun Kumar Singh came to England from India in 1975 and spent 18 months in Hayward’s Heath, Sussex. He then worked in Dover, Bristol, London, Stoke-on-Trent, and Kent. He met his future wife, Sue Levett, in 1979; their daughter, Leanne, was born in 1980, and their son, Ishan, in 1984. Finding opportunities scarce in the NHS at that time, Varun went to work in Saudi Arabia and then became consultant neurologist at Waikato Hospital in Hamilton, New Zealand, in 1987. He returned to England in 2001 and eventually secured a position as consultant neurologist at Derriford Hospital in Plymouth, before moving to the Walton Centre in Liverpool in 2009. He retired two years later, although he continued to do occasional locum work. He leaves Sue, Leanne, and Ishan.Sue Singh-Levett Cite this as: BMJ 2019;366:l5662
Caroline DeysFamily planning campaigner and GP (b 1938; q Barts 1962; DO), died from complications arising from an ischaemic foot on 6 May 2019Caroline Merula Deys worked on the successful campaign to legalise abortion in the UK, leading to the 1967 Abortion Act. She developed and ran a domiciliary family planning service in rural Cambridgeshire in 1968-69. Having moved to London, Deys worked out of the Marie Stopes Memorial Centre from February 1970, performing around 4750 vasectomies over the decade. In 1972, she was charged with serious professional misconduct before the General Medical Council for allegedly “promoting her own professional advantage” in a tabloid feature. She was acquitted, having successfully argued she was promoting vasectomies not herself, and the GMC subsequently revised its rules. She set up a singlehanded general practice in Highgate in the early 1980s. She leaves two children and one grandchild.Henry W W Potts Cite this as: BMJ 2019;366:l5761
Peter Lance d’AmbrumenilGeneral practitioner (b 1950; q Barts 1975), died from motor neurone disease on 20 December 2018Peter Lance d’Ambrumenil became frustrated by the constraints of the NHS after eight years as a GP principal and moved to Catcott in Somerset, where he did private practice, conducted medical examinations, and entered medicolegal practice. He subsequently developed an aeromedical practice and founded a business specialising in transferring and repatriating seriously and critically ill patients by air, with himself as senior flight surgeon. He also spent several years working as a GP in the Falkland Islands. For the last 16 years of his life he struggled with accelerated and resistant hypertension, which caused him much anxiety, but this was not what brought about his early death. In 2018 he was dignosed with motor neurone disease, which progressed rapidly. He leaves his wife, Sarah, and two sons.John Cherry Cite this as: BMJ 2019;366:l5758
Walter Sefton SuffernConsultant general physician and cardiologist Harrogate and Ripon (b 1919; q Leeds 1942; MD, FRCP), died from anaemia, atrial fibrillation, and frailty of old age on 4 August 2019Walter Sefton Suffern was born in Belfast and educated at Leeds Grammar School and Leeds Medical School. In December 1942, he married a fellow medic, Alison Palmer, and within weeks set sail on an Atlantic convoy to North Africa and the Royal Army Medical Corps. Sefton returned to England in 1945 to find Alison in hospital with rheumatic fever. He developed his interest in cardiology, with fellowships to Stockholm and Philadelphia. First appointed as a consultant physician to hospitals in the Airedale area, he moved to Harrogate and Ripon in 1959. After retiring in 1984, he continued to enjoy fly fishing, golf, and bridge. Alison predeceased him in 2016. Sefton leaves three children, nine grandchildren, and five great grandchildren.Alisdair Stewart, Hilary Fyson, Diana Page, Richard Suffern Cite this as: BMJ 2019;366:l5618
Mian AllahdinConsultant physician and professor of medicine (b 1931; q Dow Medical College, Karachi, Pakistan, 1960; MRCP, FRCP Ed), died on 5 September 2019 after struggling with lung cancerMian Allahdin came to the UK in 1964. He worked for 10 years in York, Taunton, and Inverness, where he did his postgraduate training. He was a consultant physician at the West Middlesex University Hospital, London, but soon moved to Hong Kong, where he served at the Queen Elizabeth Hospital for three years. In 1977 he joined Bolan Medical College in Baluchistan, Pakistan, as an assistant professor and later professor of medicine. His area of interest was cardiology. He was passionate about providing good care for his patients and trained a large number of students. He leaves Surriya, his wife of 64 years, and three daughters (two of whom are medical consultants and the third a lawyer).Sabeena Allahdin Cite this as: BMJ 2019;366:l5617
Longer versions are on bmj.com. Submit obituaries with a contact telephone number to [email protected]

168 26 October 2019 | the bmj
John Henderson, who died at the age of 61, was an outstanding paediatrician and clinical scientist. He specialised in diseases of the respiratory system, and after training in the UK and Australia he was appointed as a consultant in Bristol and led an excellent regional service for many years.
He was a superb clinician and ensured that his patients had the most up to date and effective treatments for their condition.
AsthmaOne of his major interests was asthma, which affects one in 10 children, or 1.1 million across the UK. It causes many deaths, and it is estimated that the NHS spends more than £1bn on treating asthma each year.
Henderson was active wherever children had breathing problems. He was especially proud of the retrieval service that he set up to bring patients from the far reaches of Devon and Cornwall, ensuring they were in an optimal state when they arrived in Bristol. Ambulance journeys of up to four hours were not unusual.
Henderson spent a great deal of time working in the intensive care unit and was an expert in artificial ventilation. He also set up a service in the region for children who had breathing problems associated with sleep.
But he was not content just to give the best treatment and care. He wanted to understand the reasons children became ill, why some children develop asthma, and why some are more severely affected than others.
Bristol is fortunate in having set up, in 1991, the Avon Longitudinal Study of Parents
and Children (ALSPAC), also known as Children of the 90s. This enrolled 14 000 pregnant women and their babies and collected enormous amounts of information about their background. With permission, DNA was taken from children, who have been followed up regularly.
To an inquiring mind, this is a treasure trove—the answers to what causes children to get different types of asthma, for example, could be hidden in the ALSPAC data. Over the past 30 years, huge advances have been made in genetics, and linking the epidemiological data from ALSPAC with the new genetics has led to many important insights.
Henderson looked at patterns of wheeze, finding that they have different risk factors and need different types of treatment. There are importantly differing associations with genes, and Henderson made pivotal contributions to the discovery and understanding of asthma heterogeneity (asthma genes). The full harvest of this work is yet to come.
Early life and careerAlexander John William Henderson was born in Renfrew, the eldest of four children. His father was in sales and his mother a nurse. Because of his father’s work the family moved regularly around Scotland before settling in York, where he went to Archbishop Holgate’s Grammar School, becoming a boarder when the family moved again, to the Cotswolds.
His lifelong pattern of forming few but strong friendships stems from these early days. He met his
wife, Nicola, on a blind date involving a picnic on Barnes Common in London, and this enticed him to move south from Manchester and take a post at Great Ormond Street Hospital. Recognising that he would never persuade his new wife to move north, he settled for Bristol and the south west for the rest of his career.
Henderson was pivotal in bringing together five British birth cohort studies with ALSPAC into a consortium, the STELAR e-laboratory, which vastly improved the power to make major discoveries. His organisational skills led to his being asked to lead the reorganisation of teaching at the Bristol medical school, which for many years had struggled with student satisfaction ratings at the lower end of national league tables.
His diplomacy and determination led to a new curriculum, and a streamlined and coordinated approach using all of the major hospitals in the south west resulted in a rise in student satisfaction to a top 10 position.
Henderson got a buzz from change management and being an enabler. He became frustrated only when he was working with people who were unable to see the benefits of trying something different.
He was a passionate follower of the Scottish rugby team, and his faith that one day Scotland would win in Cardiff was touching. He loved being outdoors and exploring the countryside. He leaves Nicky and their two sons.Alan Craft, paediatric oncologist, emeritus professor of child health, Newcastle University [email protected] this as: BMJ 2019;366:l5359
OBITUARIES
Henderson wanted to understand the reasons children became ill, why some develop asthma, and why some are more severely affected than others
John HendersonPaediatric respiratory epidemiologist and clinical scientist
Alexander John William Henderson (b 1958; q Manchester 1981; MD), died from pancreatic cancer on 24 July 2019