Would it be Enough to Balance Ohio’s System of Long-term Services and Supports (LTCSS)?
13
Would it be Enough to Balance Ohio’s System of Long-term Services and Supports (LTCSS)? 35th Annual Ohio Professional & Student Conference on Aging April 15, 2011 Shahla Mehdizadeh, Ph.D. Robert Applebaum, Ph.D.
description
Would it be Enough to Balance Ohio’s System of Long-term Services and Supports (LTCSS)?. 35th Annual Ohio Professional & Student Conference on Aging April 15, 2011. Shahla Mehdizadeh, Ph.D. Robert Applebaum, Ph.D. Outline. 1) Ohio’s system of LTCSS, how out of balance is it? - PowerPoint PPT Presentation
Transcript of Would it be Enough to Balance Ohio’s System of Long-term Services and Supports (LTCSS)?

Would it be Enough to Balance Ohio’s System of Long-term
Services and Supports (LTCSS)?
35th Annual Ohio Professional & Student Conference on Aging
April 15, 2011
Shahla Mehdizadeh, Ph.D.Robert Applebaum, Ph.D.

Outline
• 1) Ohio’s system of LTCSS, how out of balance is it?
• 2) How does balancing impact needs for care, and state’s budget?
• 3) Are there other efforts that policy makers need to consider?

Ohio's Total Medicaid Expenditures for Facilities and HCBS
Ohio's Medicaid Expenditures for Facilities and HCBS, 2009
32%68%
NF & ICFDD HCBS
$4.85 Billions of dollars
79%
21%
77%
23%
73%
27%
70%
30%
70%
30%
68%
32%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2004 2005 2006 2007 2008 2009
Percent Distribution of Ohio Medicaid Long-Term Services and Supports Expenditures for Facilitities and HCBS Over Time
NF & ICFDD HCBS

Ohio's Total Medicaid Utilization of Facilities and HCBS Waiver Programs
Distribution of Ohio's Medicaid Utilization of Services & Supports in Facilitites and HCBS,
2009
HCBS52%
Facilities48%
58%
42%
57%
43%
53%
48%
52%
48%
50%
50%
48%
52%
0%
20%
40%
60%
80%
100%
120%
2004 2005 2006 2007 2008 2009
Distribution of Ohio's Utilization of Long-Term Services & Supports in Facilitites and HCBS, Over Time
Facilities HCBS
118,032 Person Months

Medicaid Expenditures for LTCSS, 2009(in Millions of Dollars)
NF & ICFDDNursing Home (80%) $2,543.7 ICFDD (44%) $744.2
HCBS Waivers PASSPORT $341.0 Individual Options $807.7
Ohio Home Care $196.9 Level One $58.4
Transitions Aging Carve-Out $44.1
Transitions Developmental Disabilities $68.2
Assisted Living $19.4PACE $22.5
Choices $7.0
Total HCBS waivers $631.2 Total HCBS waivers $934.3

Projections of Population with Severe Disability and LTCSS Utilization (Medicaid Only) in 2005-2010
Year Total Population
Population with Severe Disability*
Home and Communit
y-based
Facility- based
Total
2005 11,464,042 304,511 50,865 59,727 110,592(36.2%)
2007 11,584,158 308,573 53,010 59,679 112,689(36.5%)
2009 11,542,645 309,012 64,090 56,949 121,039(39.2%)
2010 11,536,504 308,847 64,055 56,920 120,975(39.2%)
Severe Disability is defined to match Ohio’s Medicaid Level of Care for NF or IFDD
Utilization of services and supports, paid by Medicaid, in 2010 is assumed to follow the same patterns as 2009.

How Can the State of Ohio Manage the Increasing Demand for Services & Supports? Possible Scenarios:
Status Quo: consumers health and disability, use of informal care, including assistive devices, and utilization rate of facility-based care will stay the same as it is today
Less facility-based care: By encouraging the use of alternatives to facility-based care the use of nursing home and ICF/MR will be reduced annually by 1%.
Reduced demand for formal care: Through education, home modification, creation of aging friendly communities and introduction of assistive devices and technology demand for formal care will be reduced by 1% annually.Optimistic: Through education and case management reducing demand for formal care and by diversion and intervention shifting some facility-Based care utilization to community-based use. This scenario entails 1% reduction in formal care and 1% reduction in use of facility-based care annually.

Comparison of the Cumulative Impact of Different Scenarios on Demand for Long-Term Care Services and Supports in 2020
Type of Program/Setting
2009Number (Percent)
Status Quo
Less Facility-Based Care(Net chg from 2009)
Reduced Demand for Care (Net chg from 2009)
Optimistic1% Less Demand1% Less F-based
Nursing Home 49,650(41.1%)
468 -536-68
-554-86
-1,027-554 -473
ICF/MR 7,299(6.0%)
77 -82-5
-73+4
-159 -73 -86
HCBS 37,623(31.1%)
386 +600+986
-3860
87-386 +473
ID/DD waivers
22,916(18.9%)
232 +77+309
-241-9
-155 -241 86
Other 3,551(2.9%)
41 2061
-365
-41 -36 -5
Total in 2020 121,039 in 2009
136,400 136,400 122,100 122,100

Estimated Cost of Medicaid Long-Term Care Expenditures in 2020 for Different Scenarios
Different Scenarios
0% 1.5% 3% CMS predicted rate
Status Quo 136,400 ($5.5) 136,400 ($6.7) 136,400 ($8.1) 136,400 ($8.6)
Less Facility-based Care
136,400 ($5.3) 136,400 ($6.4) 136,400 ($7.8) 136,400 ($8.2)
Reduced Demand for Care
122,100 ($5.0) 122,100 ($6.0) 122,100 ($7.3) 122,100 ($7.7)
Optimistic 122,100 ($4.7) 122,100 ($5.8) 122,100 ($7.0) 122,100 ($7.4)
Different Annual Inflation Rates Assumption (number of people & costs in billions of dollars)

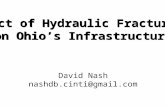
Allocation of Ohio State-Only General Revenue Funds, 2008 (about 22 billion dollars)
Higher Educ. 12% Human Services 27%
Education 40%Local Government
5%
Corrections 8%
General Gov. 8%
Just Medicaid 24%

Possible Inflation and REAL Budget (State and Fed. GRF) Growth Rates and % of Budget Needs to be Allocated to
LTCSS(2020 Budget and Medicaid LTCSS in Billions of Dollars)
Medicaid LTCSS
Expenditures(Status Quo)
2010_2015 (0%)
2015_2020 (1%)
2010_2020 (1%)
2010_2020 (2%)
2010_2020 (3%)
2020 Total Budget
― ($25.85) ($26.9) ($29.4) ($32.10)
Inflation rate 0%
($5.5) 21.3% 20.5% 18.7 17.13%
1.5% ($6.7) 25.9% 24.9% 22.8% 20.9%3% ($8.1) 31.0% 30.1% 27.6% 25.2%
CMS predicted
rate
($8.6) 33.0% 32.0% 29.3% 27.0%

Summary Between now and the year 2020 the combined total of average
daily census for NF, ICF/MR and all the HCBS Medicaid waivers will increase by about 1250-1300 every year.
In the absence of any additional efforts, beyond what state is currently doing to “balance the system”, and if there is no inflation in the next 11 years, the total Medicaid expenditures for long-term care services and supports will be one-half billion higher in 2020 than it was in 2009 (10% higher than today).
If the inflation rate is fixed at 1.5% then total Medicaid expenditures will be $6.7 billion up from $5.0 billion in 2009 (an increase of 34%);
And, if the inflation rate is fixed at 3.0% then total Medicaid expenditures will be $8.1 billion (an increase of 62%)

There Are Ways in Which an Individual May Mediate the Gap Between the ‘Functional Limitation' and
‘Disability'.“These may be classified into four broad categories: Environmental modification: through change of residence or
installing architectural enhancements. 2. Ability modification: through rehabilitation or the use of
assistive devices. 3. Compensation: through the acquisition of personal
assistance or other community services. 4. Role-redefinition and behavioral change: through changing
expectation about abilities and accomplishments. This most often involves changes in performance, such as going out less frequently or allowing more time to accomplish tasks.”
Source: Agree, E. (1999). The influence of personal care and assistive devices on the measurement of disability. Social Science & Medicine. Volume 48, Issue 4: 427-443