World Bank Documentdocuments.worldbank.org/curated/pt/...IMCI Integrated Management of Childhood...
26
Document of The World Bank Report No: NCO00001074 NOTE ON CANCELLED OPERATION REPORT (IDA-H4120) IN THE AMOUNT OF SDR 7.4 MILLION (US$12 MILLION EQUIVALENT) TO THE STATE OF ERITREA FOR AN INTEGRATED EARLY CHILDHOOD DEVELOPMENT PROJECT II June 23, 2010 Human Development Unit AFTED Country Department AFCE2 Africa Region This document has a restricted distribution and may be used by recipients only in the performance of their official duties. Its contents may not otherwise be disclosed without World Bank authorization. Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized
Transcript of World Bank Documentdocuments.worldbank.org/curated/pt/...IMCI Integrated Management of Childhood...
Document of The World Bank
Report No: NCO00001074
NOTE ON CANCELLED OPERATION REPORT (IDA-H4120)
IN THE AMOUNT OF SDR 7.4 MILLION (US$12 MILLION EQUIVALENT)
TO THE
STATE OF ERITREA
FOR AN
INTEGRATED EARLY CHILDHOOD DEVELOPMENT PROJECT II
June 23, 2010
Human Development Unit AFTED Country Department AFCE2 Africa Region This document has a restricted distribution and may be used by recipients only in the performance of their official duties. Its contents may not otherwise be disclosed without World Bank authorization.
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
CURRENCY EQUIVALENTS
(Exchange Rate Effective April 1, 2010)
Currency Unit = Eritrean Nakfa ERN 1.00 = US$ 0.067 US$ 1.00 = 14.10 ERN
FISCAL YEAR
January 1 – December 31
ABBREVIATIONS AND ACRONYMS
C-GMP Community-Growth Monitoring Program HH/C-IMCI Household and Community Integrated Management of Childhood
Illness CAS Country Assistance Strategy CCG Community Caregiver CDD Community Driven Development CFR Case Fatality Rate CHW Community Health Worker CRC Convention on the Right of the Child DP Development Partner ECD Early Childhood Development ECE Early Childhood Education ECEC Early Childhood Education & Care EDHS Eritrea Demographic and Health Survey EPDF Education Program Development Fund ESIP Education Sector Investment Program GDP Gross Domestic Product GoE Government of Eritrea GMP Growth Monitoring and Promotion HAMSET HIV/AIDS; Malaria; Sexually Transmitted Diseases; Tuberculosis HIV/AIDS Human Immunodeficiency Virus/Acquired Immune Deficiency
Syndrome HIPC Heavily Indebted Poor Country Initiative HH Household ICR Implementation Completion Report IDA International Development Association IEC Information, Education, Communication IECDP Integrated Early Childhood Development Project IEG Internal Evaluation Group IMCI Integrated Management of Childhood Illnesses ISN Interim Strategy Note KG Kindergarten M&E Monitoring and Evaluation
MoE Ministry of Education MoH Ministry of Health MoLHW Ministry of Labor and Human Welfare MDG Millennium Development Goal MMR Maternal Mortality Rate NSS Nutrition Surveillance System NUEW National Union of Eritrean Women NUEY National Union of Eritrean Youth OVC Orphan and Vulnerable Children PDO Project Development Objective PMT Project Management Team PPA Participatory Poverty Assessment PSC Policy Steering Committee RRC Regional Resource Center SSA Sub Saharan Africa TSC Technical Steering Committee UNICEF United Nations Children’s Fund USAID United States Agency for International Development WHO World Health Organization
Vice President: Obiageli Katryn Ezekwesili
Country Director: Johannes C.M. Zutt
Sector Manager: Christopher J. Thomas
Project Team Leader: Carla Bertoncino
NCO Team Leader : Carla Bertoncino

STATE OF ERITREA Integrated Early Childhood Development Project II
CONTENTS
Data Sheet A. Basic Information
B. Key Dates C. Ratings Summary D. Sector and Theme Codes E. Bank Staff F. Ratings of Program Performance in ISRs
1. Context, Project Development Objectives, and Design .............................................. 12. Post-Approval Experience and Reasons for Cancellation......................................... 163. Assessment of Bank Performance............................................................................. 164. Assessment of Borrower Performance...................................................................... 165. Lessons Learned........................................................................................................ 17Annex 1. Bank Lending and Implementation Support/Supervision Processes............. 18Annex 2. List of Supporting Documents....................................................................... 19MAP
i
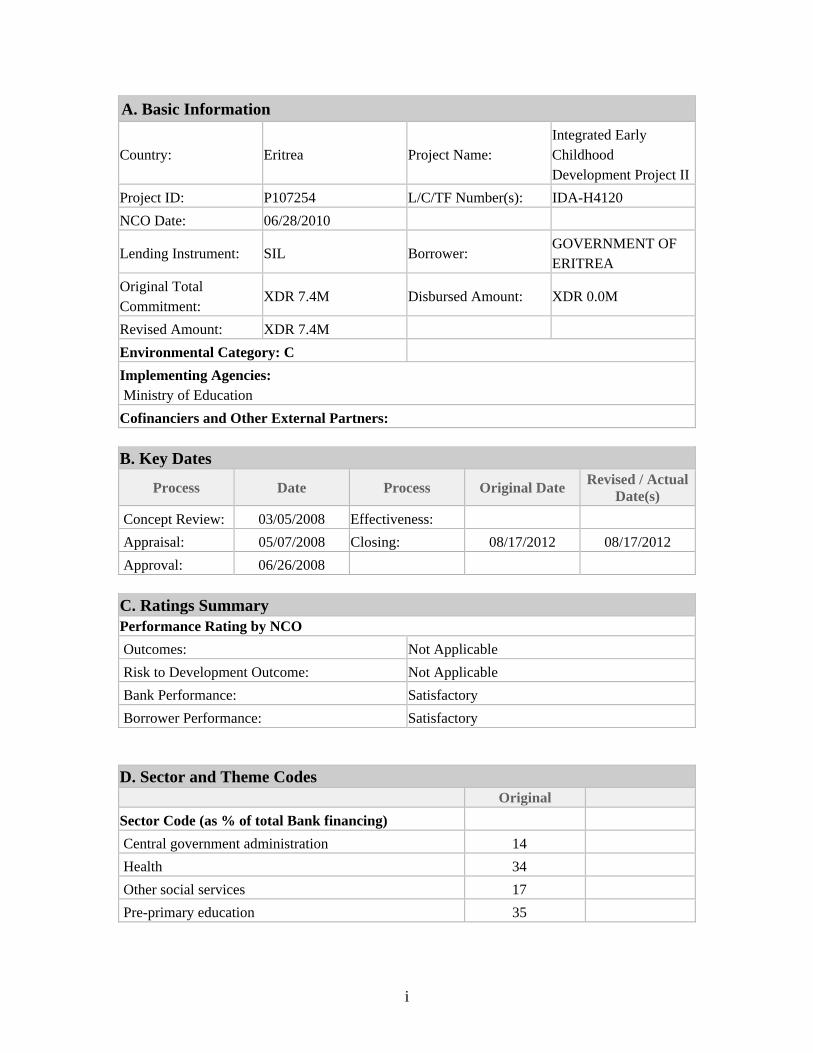
A. Basic Information
Country: Eritrea Project Name: Integrated Early Childhood Development Project II
Project ID: P107254 L/C/TF Number(s): IDA-H4120
NCO Date: 06/28/2010
Lending Instrument: SIL Borrower: GOVERNMENT OF ERITREA
Original Total Commitment:
XDR 7.4M Disbursed Amount: XDR 0.0M
Revised Amount: XDR 7.4M
Environmental Category: C
Implementing Agencies: Ministry of Education
Cofinanciers and Other External Partners: B. Key Dates
Process Date Process Original Date Revised / Actual
Date(s)
Concept Review: 03/05/2008 Effectiveness:
Appraisal: 05/07/2008 Closing: 08/17/2012 08/17/2012
Approval: 06/26/2008 C. Ratings Summary Performance Rating by NCO
Outcomes: Not Applicable
Risk to Development Outcome: Not Applicable
Bank Performance: Satisfactory
Borrower Performance: Satisfactory D. Sector and Theme Codes
Original
Sector Code (as % of total Bank financing)
Central government administration 14
Health 34
Other social services 17
Pre-primary education 35
ii
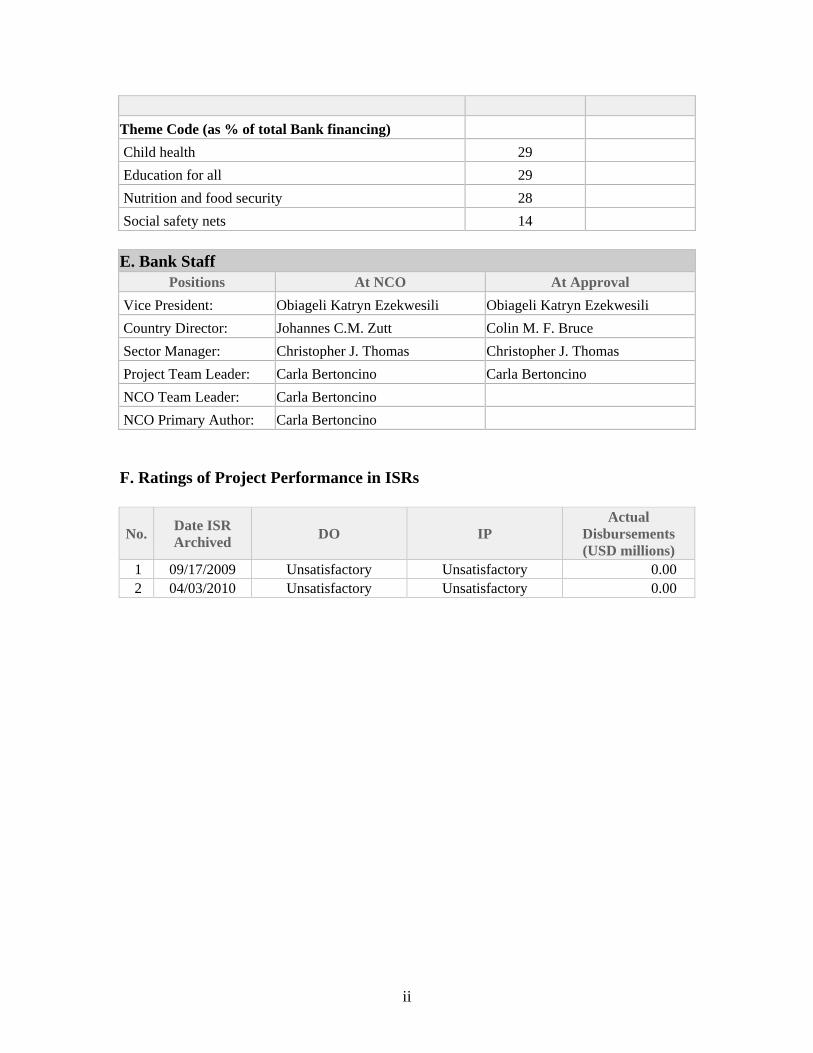
Theme Code (as % of total Bank financing)
Child health 29
Education for all 29
Nutrition and food security 28
Social safety nets 14 E. Bank Staff
Positions At NCO At Approval
Vice President: Obiageli Katryn Ezekwesili Obiageli Katryn Ezekwesili
Country Director: Johannes C.M. Zutt Colin M. F. Bruce
Sector Manager: Christopher J. Thomas Christopher J. Thomas
Project Team Leader: Carla Bertoncino Carla Bertoncino
NCO Team Leader: Carla Bertoncino
NCO Primary Author: Carla Bertoncino F. Ratings of Project Performance in ISRs
No. Date ISR Archived
DO IP Actual
Disbursements (USD millions)
1 09/17/2009 Unsatisfactory Unsatisfactory 0.00 2 04/03/2010 Unsatisfactory Unsatisfactory 0.00

1
1. Context, Project Development Objectives, and Design A. Country and Sector Issues at the Time of Appraisal
1. The last Interim Strategy Note (ISN 2005-07 Report No. 31665-ER), which was discussed at the Board in March 2005, focused on support for economic and fiscal reforms. GoE also considered participation in the Heavily Indebted Poor Country Initiative (HIPC) for which it remained potentially eligible to receive debt relief. However, client commitment to the necessary reforms was uneven over the course of the ISN and as a consequence the Bank shifted focus to maximize improved service delivery through the existing portfolio, largely centered on human development, and select analytical work.
2. Domestic policies had not been conducive to growth. While effective in addressing macroeconomic imbalances, they acted as a constraint on economic growth resulting in a decline in annual gross domestic product (GDP) growth per capita since 2005. In recognition of this, the GoE had started to adopt a strategy intended to revitalize the economy by: (i) improving broad-based growth through rural development; (ii) exploiting valuable mineral deposits; (iii) developing tourism and commercial fishing; and (v) encouraging investment in newly-established economic tax-free zones. Despite the weak overall economic performance, the government support for the social sectors had remained strong and World Bank assistance had achieved positive results in the health and early childhood and education sectors. 3. In general, reliable data was difficult to obtain then as it is now. The last household survey and Participatory Poverty Assessment (PPA), undertaken in 2003, had estimated around two thirds of the population as living below the poverty line. Women remained among the most disadvantaged: forty-seven percent of households were headed by women, half of these widows as a result of Eritrea’s turbulent history, and they were overwhelmingly poor – as high as 85 percent according to the PPA. There had been limited progress toward achieving the Millennium Development Goals (MDGs), but gains had been made in health indicators and to some extent education outcomes where development partners had continued to provide support.
Sector Issues – Health, Nutrition and Food Security, Education and Early Childhood Development
2
Health
4. At the time this project was prepared, Eritrea had made admirable progress in improving the health of its people since independence, especially in malaria, HIV/AIDS and child survival. Malaria morbidity and mortality had been reduced more than 80 percent since 1999 owing to good control efforts, making Eritrea one of few SSA countries to have met the Abuja Roll Back Malaria targets. HIV prevalence in Eritrea was relatively low at 2.4 percent of the adult population, compared to the Sub-Saharan Africa (SSA) average of 7 percent. According to the latest demographic and health surveys (DHS), between 1995 and 2002, infant mortality had fallen dramatically from 72 to 48 deaths per 1,000 live births, and under-five mortality from 136 to 93 deaths per 1,000 live births. Around 76 percent of children aged 12-23 months were fully immunized 5. Despite such achievements, several health challenges remained. Child health improvement was still an unfinished agenda. While there had been dramatic reductions in infant and under-five mortality as discussed above, the neonatal mortality rate remained around 25 per 1,000 live births. Poor access to safe water and sanitation contributed to diarrhea, which was the leading cause of illness in children. Maternal health was another challenge, with the most recent estimate for maternal mortality ratio (MMR) at 450 per 100,000. Disparity in reproductive health outcomes was large, with MMR many times higher in remote areas such as the Southern Red Sea region than in the capital city of Asmara. The rate of health facility deliveries was much higher in urban areas (62 percent) than in rural areas (8.6 percent). The GoE had a strategy under implementation to address these issues, supported in large part by the HIV/AIDS, Malaria, Sexually Transmitted Diseases, and Tuberculosis Project (HAMSET) I and II. Nutrition and Food Security
6. Malnutrition was a major concern in Eritrea. Data collected at the end of 2006 for the final evaluation for the previous Integrated Early Childhood Development (IECD) project had estimated that 42 percent of children less than 3 years old were malnourished, of which 13 percent were severely underweight. 7. Causes of malnutrition in young children included both its ‘immediate’ determinants such as child health and nutrition practices as well as the broader context of food security/food availability. The IECD Project implemented earlier showed that food security problems could dampen the overall impact of health/nutrition interventions, and that any reversal would require both additional efforts at the local level through programs such as Growth Monitoring and Promotion (GMP)1 and addressing food security issues. 8. Some 40 percent of the Eritrean population was estimated to be chronically food insecure due to the cumulative effects of repeated droughts, deforestation, and soil erosion and degradation. Despite relatively good harvests in the two years preceding this
1 A community-based approach that helps prevent and treat malnutrition in young children through both education/training and therapeutic feeding interventions.
3
appraisal, the prices of essential food items and cereals had been increasing - possibly the impact of higher global food prices. Global food prices had risen by 26 percent in the previous three years, and along with other resource-poor, small SSA countries, Eritrea had suffered significantly in terms of trade shocks as a result of increased commodity prices. Eritrea’s food security strategy attempted to mitigate the impact on household consumption through centrally managed food supplies and rationed availability of basic commodities at fixed prices. Wheat, sorghum, and barley could be sold only to the GoE, and were therefore subject to price controls. Fair price shops sold sorghum, sugar, beans, oil, tea, and pasta, which were rationed for eligible residents based on family size. It is important to emphasize that there was no independent assessment of the success of this strategy. The GoE and European Union (EC) had agreed to a new program of support focused on food security/rural development, road infrastructure and regional connections, and capacity building. Overall, food security remained a major risk in Eritrea, and was a specific concern for this operation. 9. In line with international best practice, the government had adopted a two-pronged strategy to deal with malnutrition issues:
(a) A strong program with the support of the World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF) to address issues of community nutrition, including GMP. The program was aimed at engaging families and communities to help prevent severe malnutrition (for children who are moderately malnourished) through educational programs/behavioral change as well as referral of severely malnourished children to health units for community-based therapeutic and supplemental feeding.
(b) Prioritization of food security. The Food Security Strategy, 2003, aimed to make “food of sufficient quantity and acceptable quality readily accessible to all at an affordable price at any time and place within the country.” To lower aid-dependence, a food-for-work policy had been introduced in 2006 to replace free distribution of food aid. A grain board and a crop early warning system had been established to manage food supplies. The Board had intervened in the market for food in times of scarcity, to stem price increases and was expected to hold sufficient stocks so that in times of drought, food could be supplied immediately from domestic sources. A food security fund had also been set up to ensure that the government could purchase an additional three months worth of food on the world market to supplement the stocks kept by the grain board.
Education 10. In the education sector, primary school attendance had increased rapidly following independence, but at the time of appraisal only 50 percent of children were completing primary school, compared to a SSA average of 57 percent. On the supply side there were insufficient numbers of primary schools, textbooks, and trained teachers to provide quality education. On the demand side, a large nomadic population posed particular challenges for getting all children into school. The GoE recognized that the
4
development of human capital would be critical for future economic prospects. The IECD program was intended to help address both supply and demand side challenges by promoting young children’s healthy growth, better development of language abilities and social skills thus improving their school readiness. Early Childhood Education and Development 11. Enrolment in preschools (4 and 5 year olds) was limited but had increased substantially - by about 6 times over the period 2000-2006 - and net enrolment had risen from about 4.5 percent to 19 percent, owing largely to a strong community-based approach supported by the IECD project. In addition, due in part to the government program the IECD project contributed to, there had been a substantial decrease in repetition and dropout rates in grade 1. In spite of this achievement, there was a vast majority of rural children who still did not have access to pre-school and early childcare. Some development partners such as UNICEF had been providing assistance to the government in the area of Early Childhood Education (ECE) policy, including support on capacity building for ECE policy making and program development. 12. As part of its broad-based growth strategy, the GoE regarded Early Childhood Development (ECD), and the psychosocial protection of vulnerable children as a fundamental condition to achieving its long-term development goals. There was a keen awareness of the importance of investing in young children and the long-term economic and social returns it could generate. In line with this principle, the GoE had ratified the Convention on the Rights of the Child (CRC) in 1994. The government had formulated policy guidelines for Early Childhood Education and Care (ECEC) in 1995 and for primary health care, food security and HIV/AIDS in 1998. Several articles in the 1997 national constitution also affirm the ECD imperative. These sectoral policies had culminated in the finalization of the draft Integrated ECD Policy in 2005. With funding from the Education Program Development Fund (EPDF) the Bank gave the GoE technical assistance to cost the implementation of the program endorsed by the Policy. This preliminary costing exercise provided the development partners (DPs) with information of the financing gap, and the Bank task team was engaged in a dialogue with the GoE to explore further fiscal space issues and financing options.
13. The IECD policy also provided a framework for government, regional, administration, institution, communities, families and international and national development partners to invest in and implement integrated ECD programs that contributed towards realizing the well-being of young children. 14. Different ministries were implementing sector-specific policies and programs related to ECD:
• The Ministry of Education (MoE) implemented the ECEC policy, supporting equal access to and improved quality of ECEC interventions, and the promotion of cost-effective community-based interventions that
5
promoted and strengthen community responsibility with the intent to achieve sustainability of interventions.
• The Ministry of Health (MOH) had prepared policy guidelines on food security and nutrition that focused on children and mothers because of their observed vulnerability to malnutrition.
• The Ministry of Labor and Human Welfare (MOLHW) had programs in place to strengthen the traditional safety nets with a focus on supporting children in need of special protection, especially orphans.
• On the civil society side, the National Union of Eritrean Women (NUEW) and the National Union of Eritrean Youth (NUEY) were actively engaged in advocacy efforts that promoted the rights and well-being of women and children.
15. The GoE recognized that ECD interventions yielded strong and sustainable results when they are integrated at the community level with support from all administrative levels in the government. This recognition, as well as the GoE’s firm commitment to ECD, is reflectedin the National Decentralization Policy (Proclamation No. 86/96 for the Establishment of Regional Administration) whose framework played a critical role in enhancing effective ECD implementation as demonstrated by the performance of the IECD project (see paragraph 17). This policy aimed to devolve program management responsibility to regions (zobas), sub-regions (sub-zobas), and communities as a means of improving performance, financial transparency and accountability, effectiveness and sustainability. B. Rationale for Bank Involvement 16. The international evidence on the link between nutrition and pre-schooling and school readiness is strong: weight-for-age (underweight) at age 2 is a strong predictor of stunting; malnutrition in early years is linked to 0.7 grades loss of schooling and 7 month delay in starting school. Malnourished children are more likely to drop out and/or repeat grades, iodine-deficiency robs children of 13 IQ points on average, and anemia reduces performance on cognitive tests (IQ) by 8 points. For these reasons, early childhood development continued to be a priority within government’s social sector policies for humanitarian as well as economic development. 17. The IECD project, launched in September 2000, with support from the World Bank, the Italian Cooperation and counterpart funding from the Government of Eritrea closed on March 31, 2007. The implementation had been satisfactory and project objectives largely achieved. Of the three self-standing ECD operations of this kind in Sub-Saharan Africa since the mid ‘90s, the Eritrea IECD project stood out for the commitment shown by the Government and other development partners in achieving satisfactory results. Moreover, the Implementation Completion Report (ICR) had confirmed the relevance of the IECD Project Development Objective (PDO) – an assessment shared by the Internal Evaluation Group (IEG) and crucial in the decision to process this operation as a repeater. The proposed operation would have helped consolidate the achievements made in the IECD project through a targeted, integrated
6
program of support that mitigated the risks identified in the prior operation and built on its successes. It would have taken advantage of the implementation arrangements that were already in place and still operational in the project areas. 18. IECD also remained an area of focus for the development partners – mainly WHO for Integrated Management of Childhood Illnesses (IMCI), and UNICEF for GMP and household and community based IMCI. The Bank’s involvement in the proposed repeater project provided an opportunity to build on the lessons from the IECD project and support the Government in enhancing the quality and deepening the integration of relevant ECD interventions in targeted areas. The Bank’s comparative advantage in reviewing public sector financing and sustainability issues was expected to help the Government scale up successfully effective ECD interventions, without losing sight of fiscal constraints. IECD II would also have provided a learning foundation for future ECD options elsewhere in the region, as well as an opportunity to show the achievements of integrated ECD to other international partners. 19. The proposed operation met the criteria for Bank’s new financing in Eritrea listed in the Interim Strategy Note (ISN):
• The Bank had a comparative advantage and a history of positive engagement and results (which the IECD project demonstrated).
• There was an appropriate sector policy framework in place, agreement with the GoE on the remaining policy issues, and a plan for their implementation (including a strong IECD Policy).
• There was demonstrated willingness by the GoE to take on board Bank technical and policy advice in the sector (the GoE had requested such support).
• The results were estimated to be sustainable under realistic macroeconomic projections, with risk mitigation through the planned experiment with the community grant scheme program embedded in the project design and a plan for longer term Bank-government engagement on financing strategies.
• The project-level risks were considered moderate following mitigation measures.
• The development impact was expected to be considerable in terms of either direct improvements in well-being or in terms of galvanizing economic growth (based on the positive experience with similar interventions in the previous Eritrea IECD project and generally accepted research on the benefits of ECD).
C. Higher Level Objectives to which the Project Contributed 20. The design and implementation of the second phase of the IECD program was consistent with and supported the government’s IECD policy and the Bank’s ISN focus on human development. Through the longer term impact IECD activities were expected to have on health and education, IECD II would contribute to a number of MDGs relating to maternal and child health, nutrition, and primary education as well as poverty reduction. The impact of this project would have been especially high because it focused
7
on the well-being of young children, especially those who were disadvantaged by poverty and post-conflict conditions. 21. Building on the success of the IECD project, this operation set the ground work for a long term scaling up of ECD throughout Eritrea. By consolidating the integrated program in targeted villages and helping ensure its sustainability through optimal public funding and community participation, this project would pave the way for a large scale replication and scaling up of the programs across the country in the following 7-10 years. This operation, therefore, provided the extra technical assistance and financial ‘push’ so as to ensure that the achievements of the previous operation were sustained and given momentum for the longer term. D. Lending Instrument 22. This project was a follow-on operation, processed as a fast-tracked Specific Investment Loan (SIL), and financed through an IDA Grant. The proposed duration of the project was four years. E. Project Development Objective and Key Indicators 23. As a repeater and more focused operation, the PDO for IECD II was to improve the health, nutrition, and access to pre-school education of Eritrean children aged 6 and under in the project villages. A particular effort was to be made across components/activities to ensure that all Orphans and Vulnerable Children (OVC) in the target villages would benefit equally from the project. 24. A crucial lesson had been learned from the previous project in terms of the indicators for nutrition and early education. Reducing malnutrition is a higher level outcome and, as such, one that the Country Strategy itself is responsible for – as opposed to an operation or even a subset of HD interventions. In light of this it was suggested that the PDO achievement of IECD II be measured by simpler, more reliable, and more easily measurable indicators than used in the first project. Similarly, ECEC can impact repetition and dropout rates in lower primary school only after 5-7 years of uninterrupted implementation and, therefore, would not be monitored in this project. A set of intermediate outcomes and indicators had been agreed upon. 25. These were the proposed PDO indicators:
(i) Combined case fatality rate (CFR) from the five main childhood illnesses in the project villages; and
(ii) percent of children enrolled at the correct age (4 and 5 year olds) in
kindergartens (KGs) and community caregivers (CCGs) in the project villages.
26. Although not as part of its results framework, IECD II would continue tracking malnutrition rates in the project villages, while the MoH would continue monitoring it nationwide through its Nutrition Surveillance System (NSS). Likewise, the MoE would
8
keep monitoring the primary education indicators, including repetition and dropout rates. In terms of the longer term impact that ECD has on children’s health, growth, education outcomes and quality of adult life, an evaluation was being planned in the context of the Africa Impact Evaluation in Education Program in the World Bank. 27. During the previous project the capacity to collect and integrate information from the implementing line ministries had been developed significantly. At the village level, capacity needed strengthening in order to mainstream the use of the monitoring and evaluation (M&E) feedback loop. IECD II would address this need by implementing the village level M&E feedback loop in the target villages at the onset of the project through proper training and support for the village administrators. F. Project Components and Implementation Arrangements 28. The proposed IECD II would have consolidated and strengthened the existing IECD interventions to address young children's needs in the areas of maternal and child health and nutrition, and ECEC through three main components, namely: (i) maternal and child health and nutrition; (ii) ECEC; and (iii) project management, monitoring and evaluation, advocacy and strategic communication. 29. The project would have provided services and support for maternal and young children's needs: health care, nutrition, cognitive stimulation, and early education. It would have continued equipping parents, mothers, caregivers and the community with knowledge and services to support child growth and development, targeted at various stages of the young child's development. Mothers and caregivers would have been provided with knowledge on how to deal with childhood illnesses, improve existing nutrition behaviors, and the value of cognitive stimulation in the early years. Health clinics and communities would be equipped to address the major childhood illnesses. Access to early childhood education through preschool centers would have also been improved. 30. Interventions were to target 3502villages, where the project would finance integrated services over the life of the project. Of these, 185 villages were in ‘ready to implement’ status given that most of them already had implementation structures, and also had the CCG/KG centers and ongoing GMP interventions. The remaining 165 villages were those with ongoing CCG/KG centers, and they would have become fully integrated within the first two years of the proposed operation, as health and nutrition interventions were rolled in. Among other inputs, the proposed operation would have supported the recurrent costs of the interventions while the communities prepared and
2 Villages in rural areas in Eritrea are uniformly disadvantaged in access to basic social services. The target 350 villages for IECD II were chosen on the basis of: (i) prior IECD coverage; and (ii) readiness to implement an integrated package of ECD services based on availability of pre-school centers, and planned health and nutrition activities (per MoH’s program).
9
implemented an experimental grant program, the objective of which was to generate a stream of income to help defray recurrent costs of running CCGs/KGs and Community Health Workers (CHW)/GMP interventions over the long term. 31. The proposed operation would have utilized the implementation arrangements that were already in place at all administrative levels, including at the central, zoba, and sub-zoba levels. At the central level, the model of a project management team (PMT) with the responsibility of coordinating all project activities - with guidance from the policy steering committee (PSC) and the technical support committee (TSC) - would continue as in the previous project. These teams and committees were operational at the time of appraisal. At the village level, the proposed operation would have utilized existing village administrators, mainstreaming the task of coordinating the integrated interventions at the community/village level. Maternal & Child Health and Nutrition (US$4.3 million)
32. This component aimed to: (i) improve case management and skills of health workers, community health workers (Household/Community - HH/C-IMCI, covering children aged 5 and under) through training in prevention and treatment of childhood illnesses with the highest morbidity and mortality, and prevention of malnutrition in children under five years of age; (ii) improve the nutritional status of children 2 years and under, and pregnant and nursing mothers through improving health and nutrition practices in communities, with particular emphasis on exclusive breastfeeding during the first six months from birth; improving household and community response to childhood illnesses, nutrition issues, and quality of care provided to pregnant mothers and young children at home; and (iii) empower communities and caregivers to improve family/child health care practices through promotion of a supportive and enabling environment at the household and community level for children’s survival, growth and development; improving appropriate and timely health care seeking behavior when children need assistance outside home; and increasing compliance to recommended treatment and advice from health professionals. The unallocated amount of US$1 million was to be used to meet any unforeseen needs, e.g. to procure therapeutic feeding should an episode of food insecurity arise in the project areas during implementation. The GoE Policy Steering Committee, in consultation with the Bank, would determine how to use this amount as the project was implemented, according to demand and effectiveness of interventions. 33. This component would have addressed two essential requisites for HH/C-IMCI and GMP to be effective: (i) provision of essential IMCI drugs3 as close to the communities as possible with appropriate training of persons responsible for dispensing them; and (ii) implementing protocols for treatment and management of severe and moderate malnutrition, including provision of therapeutic feeding. For these two interventions, the government was expected to work closely with other partners providing
3 These are basic drugs, e.g. paracetamol, co-trimoxasol, Oral Rehydration Salts.

10
support to GoE, especially UNICEF which has expertise in the area of HH/C-IMCI and GMP implementation. The project would finance: relevant training for Health Workers, CHWs and GMP promoters; HH/C-IMCI medicine kits, including drugs to equip CHWs; eventual therapeutic feeding to prevent and cure severe malnutrition cases.
Early Childhood Education and Care (US$6.6 million) 34. This component aimed to: (i) consolidate quality in ECEC services in the 350 target villages through refresher training for service care providers, provision of enhanced learning materials and teaching aids for the KGs and CCGs, professional capacity building for all new ECEC service providers, parenting enrichment training (through training 2500 adult education facilitators), and introduction of pre-school based delivery of preventive health services; (ii) enhance inclusion of OVCs (mainly orphans) through the community based program that aimed to integrate orphans into families. It was estimated that 4400 orphans would have been re-united with families through provision of OVC grants to support income generating schemes for the benefit of the families; and (iii) pilot grant scheme program of ECD services at the community level through establishing a mechanism of providing small community grants that the communities could have used to acquire and build assets. Approximately 50 to 100 villages would have been selected to implement the pilot of the community grants scheme. The approach would have been scaled up in all project villages based on evidence of success4 and would have taken into account the lessons learned from the pilot villages. There would have been process established of continuous assessment and feedback of experiences in the implementation of community grants. In order to maximize learning from the pilot, villages would have been selected to represent the microclimatic/agricultural variety in the country (e.g. lowlands vs. highlands), as well as low and high capacity levels. A detailed implementation plan would guide the roll-out of the pilot community grants scheme as well as the subsequent scaling-up. If successful, such an approach would have both empowered communities and helped improve the quality and sustainability of ECE programs. An independent evaluation of the approach was planned by the third year of the project.
35. Furthermore, the ongoing Regional Resource Centers (RRC) built in Phase I would have been further strengthened and supported to become centers of excellence for ECD in each zoba, including ensuring its use in training programs and illustrating model teaching, monitoring and evaluation. UNICEF would have provided support to the MOE in assessing the needs and requirements of these RRCs and in helping to strengthen their services. The Project would have financed: relevant technical assistance and training for ECEC supervisors and adult education facilitators; in-service training for KG teachers, CCGs, as well as sensitization of lower primary school teachers and directors on ECD issues; learning materials and teaching aids for KGs and CCGs; and community grants to develop community level sustainability of ECD interventions. Project Management, Monitoring, Evaluation, Advocacy and Strategic Communication (US$1.8 million)
4 Based on the capacity of the pilot community to contribute to the recurrent costs of the ECD program.
11
36. This component aimed to: (i) strengthen project management and implementation through an efficient system of coordinating project activities across the Ministries of Health and Education and at various administrative levels; timely monitoring, supervision and evaluation, including collecting relevant data and information, analyses, and reporting on results; and ensuring reliable and timely procurement functions and financial management and reporting; and (ii) implement effective Advocacy and Strategic Communications, through various communication mechanisms and exchanges of information/ knowledge for increasing awareness of parents and caregivers with regard to their children’s health, nutrition, education and psychosocial development. The Project would have financed: operating costs; consultancies (including auditing costs); training; printing of advocacy and communication materials. G. Risk Analysis Risk Identification and Mitigation Strategies Matrix Risk factors Description of risk Risk
rating Mitigation measures Rating
of residual
risk I. Country-Level Risks Capacity constraints Weak capacity to manage
projects could lead to waste and reduce the effectiveness of available resources.
S • Improve counterpart capacity through the design of Bank projects.
• Coordinate closely with partners who are also providing assistance to build government capacity (EC and UN agencies).
S
Fiduciary Risks Analytic work on public financial management (PFM) in Eritrea not available. Limited available information indicates PFM weaknesses (e.g., weak budget-policy link, low level of fiscal transparency, non-availability of budget plan or budget execution information outside of government). Findings of a World Bank review in 2002, which were still valid, include: i) the country did not have a sound procurement system in place; ii) the procurement practices were less than fully transparent; iii) institutional capacity was
H • Maintain offer of support for design or financing of capacity building for public financial management and procurement to upgrade practices.
• Ensure satisfactory fiduciary practices (procurement and financial management) in Bank-financed projects through project-specific measures.
• Monitor assessments of corruption from other development partners for signs of problems.
H
12
weak, and vi) open competitive bidding was infrequently used, etc.
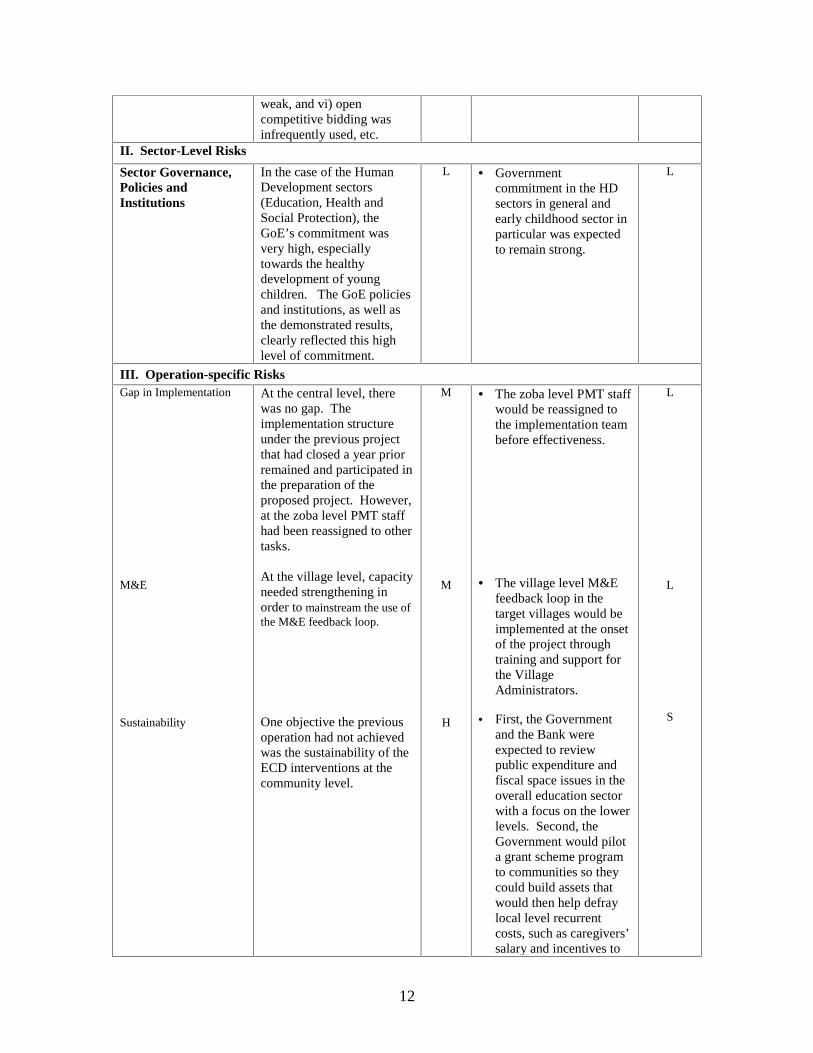
II. Sector-Level Risks
Sector Governance, Policies and Institutions
In the case of the Human Development sectors (Education, Health and Social Protection), the GoE’s commitment was very high, especially towards the healthy development of young children. The GoE policies and institutions, as well as the demonstrated results, clearly reflected this high level of commitment.
L • Government commitment in the HD sectors in general and early childhood sector in particular was expected to remain strong.
L
III. Operation-specific Risks Gap in Implementation
M&E
Sustainability
At the central level, there was no gap. The implementation structure under the previous project that had closed a year prior remained and participated in the preparation of the proposed project. However, at the zoba level PMT staff had been reassigned to other tasks. At the village level, capacity needed strengthening in order to mainstream the use of the M&E feedback loop.
One objective the previous operation had not achieved was the sustainability of the ECD interventions at the community level.
M
M
H
• The zoba level PMT staff would be reassigned to the implementation team before effectiveness.
• The village level M&E feedback loop in the target villages would be implemented at the onset of the project through training and support for the Village Administrators.
• First, the Government
and the Bank were expected to review public expenditure and fiscal space issues in the overall education sector with a focus on the lower levels. Second, the Government would pilot a grant scheme program to communities so they could build assets that would then help defray local level recurrent costs, such as caregivers’ salary and incentives to
L
L
S
13
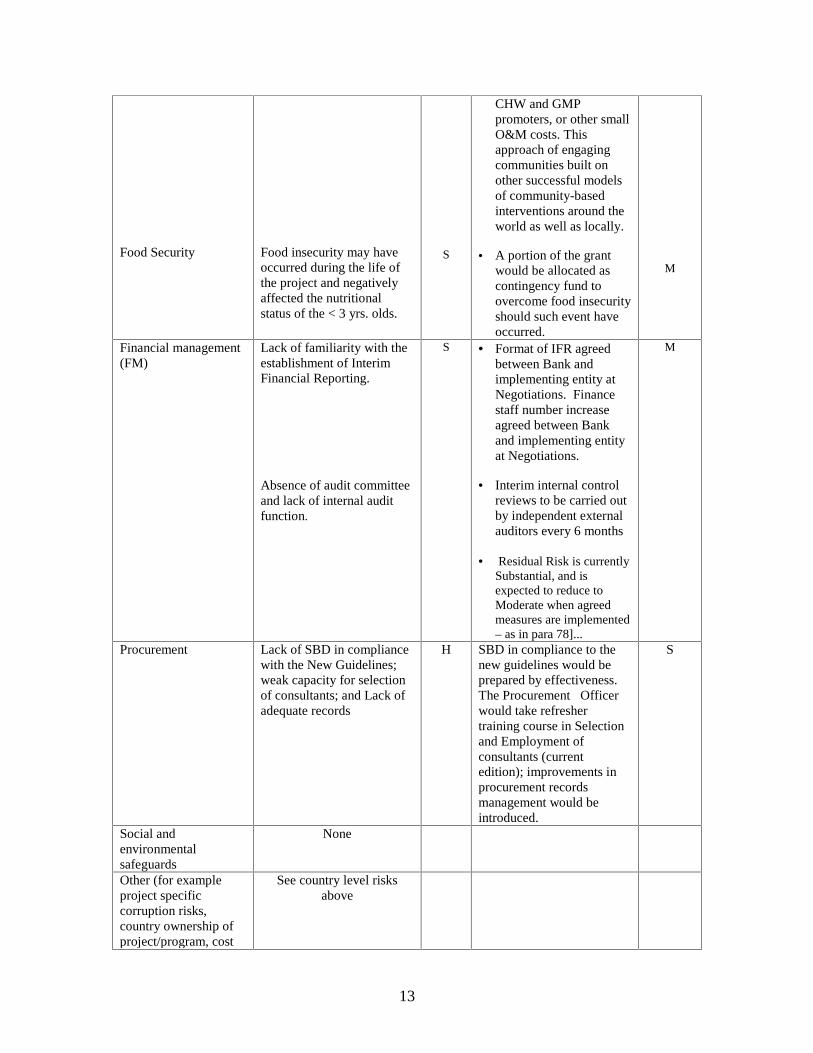
Food Security
Food insecurity may have occurred during the life of the project and negatively affected the nutritional status of the < 3 yrs. olds.
S
CHW and GMP promoters, or other small O&M costs. This approach of engaging communities built on other successful models of community-based interventions around the world as well as locally.
• A portion of the grant would be allocated as contingency fund to overcome food insecurity should such event have occurred.
M
Financial management (FM)
Lack of familiarity with the establishment of Interim Financial Reporting.
Absence of audit committee and lack of internal audit function.
S • Format of IFR agreed between Bank and implementing entity at Negotiations. Finance staff number increase agreed between Bank and implementing entity at Negotiations.
• Interim internal control
reviews to be carried out by independent external auditors every 6 months
• Residual Risk is currently Substantial, and is expected to reduce to Moderate when agreed measures are implemented – as in para 78]...
M
Procurement Lack of SBD in compliance with the New Guidelines; weak capacity for selection of consultants; and Lack of adequate records
H SBD in compliance to the new guidelines would be prepared by effectiveness. The Procurement Officer would take refresher training course in Selection and Employment of consultants (current edition); improvements in procurement records management would be introduced.
S
Social and environmental safeguards
None
Other (for example project specific corruption risks, country ownership of project/program, cost
See country level risks above
14
escalation, prevalence of failures in similar projects, adverse external developments affecting costs/benefits of the project )
IV. The Overall Residual Risk: Substantial
H = High; S = Substantial; M = Moderate; L = Low Quality at Entry
Quality at Entry was not assessed, but the preparation team strove to assure it by basing the design of the operation on the successful features of its predecessor as summarized in the following section.
H. Lessons Learned and Reflected in the Project Design 37. The following lessons learned, most of them described in detail in the Implementation Completion Report (ICR) of IECD, were reflected in the project design.
a) Integration of Nutrition and HH/C-IMCI, and contingency plans. IECD demonstrated that nutrition interventions are successful when integrated with health interventions. Furthermore, in environments that can experience food insecurity episodes, it is essential to have a contingency plan that can be activated fast if needed, which the proposed project includes in its design.
b) National ownership and buy-in is important in achieving development
outcomes. Clearly, the achievements realized in IECD result from the GoE not viewing its role as purely that of a beneficiary or facilitator. The commitment and responsiveness shown by the GoE was that of a majority shareholder whose development interests were the paramount considerations in all deliberations made and decisions taken. Such support and interest was forthcoming during the preparation of this repeater operation.
c) Role of Project Units. Different from the traditional PIUs which carry out
implementation for and report to the line ministries, the PMT in IECD coordinated the line ministries’ implementation of decentralized, multi-sectoral operations. It also facilitated the communication across levels of administration, and performed the FM and procurement functions on behalf of the line ministries, with their technical inputs. This model worked well, with the PMT reporting to the Policy Steering Committee, chaired by the Ministry of Education, and receiving guidance from the Technical Support Committee, chaired by the Director General of General Education. The same structure would continue in IECD II, with a greater focus on mainstreaming the program at the village level (at the zoba and subzoba levels, the IECD program is already almost fully mainstreamed).
15
d) Monitoring and Evaluation. It is very common to underestimate the risk of insufficient M&E capacity, especially in multi-sectoral, decentralized operations as these require both horizontal and vertical links, in turn calling for a complex/integrated M&E framework. A thorough assessment of the capacity to operationalize such a framework, including the relative readiness of the participating line ministries, and a corresponding risk mitigation strategy should clarified in projects of this type. The preparation of IECD II has taken this lesson into account by simplifying the M&E framework and clearly defining the roles and responsibilities for M&E, including M&E at the village level.
e) Component Design and Relevant Policies. Considering the intent of
delivering an integrated package of services, it would be advisable to design project components around the level of implementation (e.g. community, regional, national) as opposed to the lines of the interventions, as was the case initially under IECD. This project is designed to fully integrate its services at the village level.
f) Development Partners Engagement and Coordination. Of the three self-
standing ECD projects in Sub-Saharan Africa implemented recently (Kenya, Uganda and Eritrea), IECD was the only one that largely achieved its objectives. A major lesson to be learnt from the evaluation of the three operations is that a formal, well coordinated partnership among all the involved development partners, local and international, is necessary for a successful outcome. This was not the case in any of these projects. In Eritrea, an informal partnership worked because of: (i) the project almost exclusively built on existing interventions supported by the GoE and other development agencies; (ii) the small number of development partners; and (iii) the GoE’s unwavering commitment and consistent guidance. IECD II builds on these experiences by continuing to work closely with WHO and UNICEF.
g) Limited community ownership and capacity. One strong lesson from the
relative low impact area of IECD is that communities need time to understand the benefits of interventions, and need to be supported to develop their own plans for sustainability. IECD II proposes to set right this aspect through the grant scheme program embedded in its design, continuous technical support, and intensive sensitization campaigns.

16
2. Post-Approval Experience and Reasons for Cancellation. (main events leading to cancellation, steps taken to resolve problems, exogenous factors, identification of causes and responsibility if project failed, implications of failure): 38. It may help to state upfront that the reason for the cancellation was nothing to do with project content or design, and was entirely extraneous to the IECD project itself. The Financing Agreement (FA) for this operation was signed on August 28, 2008. When, ten days later, the GoE received the Supplemental Letter (SL) to the FA for signature, an immediate reply was sent informing the Bank that the GoE saw no justification in signing the SL since it had already subscribed to the standard General FA, and therefore to IDA’s General Conditions. The Bank’s numerous attempts to persuade the GOE to sign the SL proved unfruitful and eventually the Grant was withdrawn with a letter to the GoE dated December 18, 2008. After the Grant withdrawal, several high level exchanges took place between the GoE and the Bank to remedy the situation and avoid a severe loss for Eritrea (a total of USD 29.5 million for IECD II and the additional financing for a power sector operation combined) but the impasse could not be overcome.
3. Assessment of Bank Performance (lending process/ensuring Quality at Entry, supervision and implementation assistance role, compliance with Bank policies, justification for rating):
In terms of lending process and quality at entry, the Bank performance is rated Satisfactory. Mindful of the importance to make a seamless transition from the first to the second phase of the IECD program, as well as to avoid losing the uncommitted balance under the IDA 14 allocation for the country5, the Bank proactively engaged the GoE to start preparing IECD II early on, during the completion and closing process of its predecessor. However, it was not until March 2008 that the GoE officially decided how it wished to use its residual IDA allocation, and the Bank team prepared the operation for Board approval in three months without being able to avail itself of the simplified procedure for repeater operations due to the country level high risk rating that ultimately required a Regional Operations Committee review. As regards the signing process, the Bank performance was less than satisfactory as it failed to send the SL together with the FA as an integral part of the negotiated package. There is no basis for rating the supervision and implementation assistance role as this operation was never declared effective.
4. Assessment of Borrower Performance (government and implementing agency performance, compliance with covenants, justification for rating):
5 The IDA 14 cycle was due to close June 30, 2008.
17
The Borrower performance during the lending process is rated Satisfactory as the GoE fully kept up with the extremely tight schedule the task team had to follow. By the time the FA was signed, the GoE had already met all the conditions for effectiveness. Credit should be given to the GoE for including the ECD caregivers hired under the IECD project in the teacher payroll even in the absence of a second phase. There is no basis for rating the Borrower implementation performance as this operation never became effective.
5. Lessons Learned (both project-specific and of wide general application)
Not applicable
18
Annex 1. Bank Lending and Implementation Support/Supervision Processes
(a) Task Team members
Names Title Unit Responsibility/Specialty
Lending Carla Bertoncino Economist AFTED TTL Harold H. Alderman Adviser AFTHD Henry Amena Amuguni Financial Management Specialist AFTFM Efrem Fitwi Procurement Analyst AFTPC Arun R. Joshi Sr. Education Spec. AFTED Yi-Kyoung Lee Health Specialist AFTHE Son Nam Nguyen Sr. Health Spec. ECSHD Dung-Kim Pham Operations Officer AFTED Nightingale Rukuba-Ngaiza Sr. Counsel LEGAF Luis M. Schwarz Senior Finance Officer LOAFC Helen Giorghis Taddese Program Assistant ConsultantSaba Solomon Tekle Executive Assistant AFMER Christopher D. Walker Lead Specialist AFTHE Samuel Iyasu Zerom Resource Management Analyst AFTRM
Supervision/NCO
Carla Bertoncino Economist AFTEDNCO Team
Leader
(b) Staff Time and Cost Staff Time and Cost (Bank Budget Only)
Stage of Project Cycle No. of staff weeks USD Thousands (including
travel and consultant costs)Lending
FY08 190.96
Total: 190.96 Supervision/NCO
Total: 0.00

19
Annex 2. List of Supporting Documents Implementation Completion Report for IECD Project Appraisal Document for IECD II Implementation Status Reports for IECD II
45
MAP