
World Bank Document · The World Bank Report No: ICR 00001446 IMPLEMENTATION COMPLETION AND RESULTS...
94
Document of The World Bank Report No: ICR 00001446 IMPLEMENTATION COMPLETION AND RESULTS REPORT (IBRD-70680) ON A LOAN IN THE AMOUNT OF US$17.0 MILLION TO THE REPUBLIC OF COSTA RICA FOR A HEALTH SECTOR STRENGTHENING AND MODERNIZATION PROJECT June 25, 2010 Human Development Sector Management Unit Central America Country Management Unit Latin America and The Caribbean Regional office Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized
Transcript of World Bank Document · The World Bank Report No: ICR 00001446 IMPLEMENTATION COMPLETION AND RESULTS...

Document of The World Bank
Report No: ICR 00001446
IMPLEMENTATION COMPLETION AND RESULTS REPORT (IBRD-70680)
ON A
LOAN
IN THE AMOUNT OF US$17.0 MILLION
TO THE
REPUBLIC OF COSTA RICA
FOR A
HEALTH SECTOR STRENGTHENING AND MODERNIZATION PROJECT
June 25, 2010
Human Development Sector Management Unit Central America Country Management Unit Latin America and The Caribbean Regional office
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
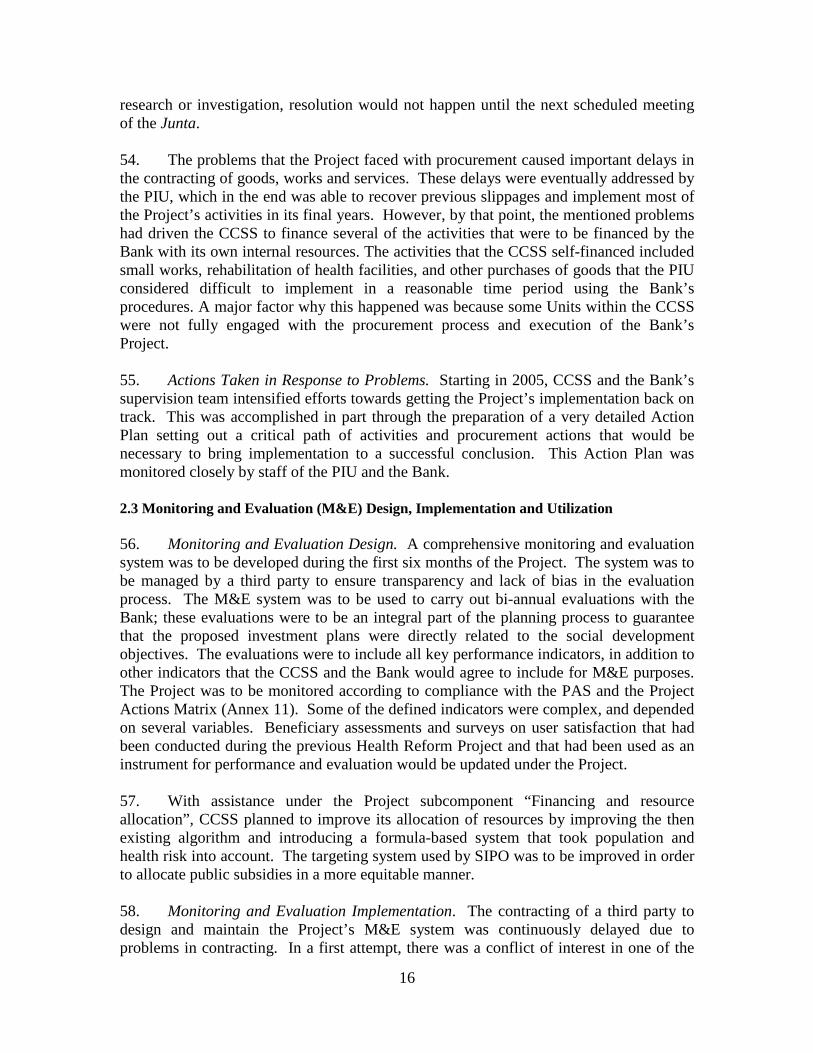
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
CURRENCY EQUIVALENTS (Exchange Rate Effective June 15, 2010)
Currency Unit = Costa Rican Colón 0,001853 = US$ 1
US$ 1.00 = 539.601 CRC
FISCAL YEAR ABBREVIATIONS AND ACRONYMS
CBR Cost Benefit Ratio CCSS Caja Costarricense de Seguro Social
Costa Rican Social Security Institute CEO Chief Executive Officer CGO Contraloria General de la República
General Comptroller´s Office DRG Diagnostic Related Groups EBAIS Equipos Básicos de Atención de Salud
Basic Health Care Teams HRP Health Reform Project IDB Inter-American Development Bank IMAS Instituto Mixto de Ayuda Social del Estado
State Social Welfare Institute M&E Monitoring and Evaluation MOH Ministry of Health MOF Ministry of Finance OM Operations Manual PAS Policy Activity Schedule PASP National Health Plan PCU Project Coordination Unit PDO Project Development Objectives PESS Strategic Health Service Plan PHC Primary Health Care PIU Project Implementation Unit SINCERE Sistema Centralizado de Recaudación
Centralized Collection System SIPO Sistema de Identificación de la Población Objetiva
Population Identification System
Vice President:Pamela Cox
Country Director:Laura Frigenti
Sector Manager:Keith Hansen
Project Team Leader:Rafael A. Cortez
ICR Team Leader:Rafael A. Cortez
ICR Primary Author:Suzana de Campos Abbott

COUNTRY Health Sector Strengthening and Modernization II Project
CONTENTS
Data Sheet B. Key Dates ....................................................................................................................iC. Ratings Summary ........................................................................................................iD. Sector and Theme Codes............................................................................................iiE. Bank Staff...................................................................................................................iiF. Results Framework Analysis ......................................................................................iiG. Ratings of Project Performance in ISRs ...................................................................xiH. Restructuring (if any) ...............................................................................................xiiI. Disbursement Profile ................................................................................................xii1. Project Context, Development Objectives and Design...............................................12. Key Factors Affecting Implementation and Outcomes ............................................103. Assessment of Outcomes ..........................................................................................194. Assessment of Risk to Development Outcome.........................................................305. Assessment of Bank and Borrower Performance .....................................................316. Lessons Learned........................................................................................................357. Comments on Issues Raised by Borrower/Implementing Agencies/Partners...........36Annex 1. Project Costs and Financing..........................................................................37Annex 2. Outputs by Component..................................................................................38Annex 3. Economic and Financial Analysis .................................................................54Annex 4. Bank Lending and Implementation Support/Supervision Processes.............55Annex 5. Beneficiary Survey Results (User Satisfaction Survey 2007).......................57Annex 6. Stakeholder Workshop Report and Results...................................................62Annex 7. Summary of Borrower’s ICR and/or Comments on Draft ICR.....................63Annex 8. Comments of Co-financiers and Other Partners/Stakeholders......................66Annex 9. List of Supporting Documents ......................................................................67Annex 10. Policy Activity Schedule (PAS)..................................................................68Annex 11: Project Actions Matrix ...............................................................................73Annex 12: Changes in Administration, CCSS Leadership, Project Management, and Reporting Relationships................................................................................................78MAP
i
A. Basic Information
Country: Costa Rica Project Name:
Health Sector Strengthening and Modernization II Project
Project ID: P073892 L/C/TF Number(s): IBRD-70680
ICR Date: 06/30/2010 ICR Type: Core ICR
Lending Instrument: SIL Borrower: GOVERNMENT OF COSTA RICA
Original Total Commitment:
USD 17.0M Disbursed Amount: USD 13.3M
Revised Amount: USD 13.3M
Environmental Category: C
Implementing Agencies: Caja Costarricense del Seguro Social
Cofinanciers and Other External Partners:
B. Key Dates
Process Date Process Original Date Revised / Actual Date(s)
Concept Review: 05/15/2001 Effectiveness: 01/06/2003 01/06/2003
Appraisal: 05/22/2001 Restructuring(s):
Approval: 07/12/2001 Mid-term Review:
Closing: 12/31/2006 12/31/2009
C. Ratings Summary C.1 Performance Rating by ICR
Outcomes: Moderately Satisfactory
Risk to Development Outcome: Low or Negligible
Bank Performance: Moderately Satisfactory
Borrower Performance: Moderately Satisfactory
C.2 Detailed Ratings of Bank and Borrower Performance (by ICR) Bank Ratings Borrower Ratings
Quality at Entry: Moderately SatisfactoryGovernment: Moderately Satisfactory
Quality of Supervision:Moderately SatisfactoryImplementing Agency/Agencies:
Moderately Satisfactory
Overall Bank Performance:
Moderately SatisfactoryOverall Borrower Performance:
Moderately Satisfactory

ii
C.3 Quality at Entry and Implementation Performance Indicators Implementation
Performance Indicators QAG Assessments
(if any) Rating
Potential Problem Project at any time (Yes/No):
No Quality at Entry (QEA):
None
Problem Project at any time (Yes/No):
No Quality of Supervision (QSA):
None
DO rating before Closing/Inactive status:
Moderately Satisfactory
D. Sector and Theme Codes Original Actual
Sector Code (as % of total Bank financing)
Central government administration 5 5
Health 95 95
Theme Code (as % of total Bank financing)
Administrative and civil service reform 25 25
Decentralization 25 25
Health system performance 50 50
E. Bank Staff Positions At ICR At Approval
Vice President: Pamela Cox David de Ferranti
Country Director: Laura Frigenti D-M Dowsett-Coirolo
Sector Manager: Keith E. Hansen Charles C. Griffin
Project Team Leader: Rafael A. Cortez Maria-Luisa Escobar
ICR Team Leader: Rafael A. Cortez
ICR Primary Author: Suzana Nagele de Campos Abbott
F. Results Framework Analysis Project Development Objectives (from Project Appraisal Document)This project aims to improve health system performance and financial sustainability by supporting the ongoing policy changes in the health sector in Costa Rica. Most of these changes are part of second-phase reforms in the Costa Rican Social Security Institute (Caja Costarricense de Seguro Social, or CCSS). For the short- to medium-term, these policy changes will: (a) align the organizational and functional structure of the CCSS with recent changes separating financing, purchasing and provision of health services at all levels; (b) promote improvements in quality and fulfillment of consumer rights, as

iii
well as the efficiency and effectiveness of the Ministry of Health (MH) as a regulatory agency, by strengthening the institutional and regulatory framework; (c) improve the quality and efficiency of the CCSS health delivery system by supporting decentralization of decision-making, consolidation of the primary care delivery network based on a population-based system, and introduction of performance-based incentives for providers; (d) reduce inefficiencies in the pharmaceutical sub-sector and promote rational drug use by introducing changes in the planning, purchasing and distribution of pharmaceuticals and supplies; and (e) develop financial mechanisms that will improve the equitable distribution of resources, improve efficiency in the provider payment mechanisms and strengthen the CCSSs capacity to collect payroll contributions. Revised Project Development Objectives (as approved by original approving authority)
(a) PDO Indicator(s)
Indicator Baseline Value
Original Target Values (from
approval documents)
Formally Revised Target Values
Actual Value Achieved at
Completion or Target Years
Indicator 1 :
New organizational structure of the CCSS based on separation of financing, purchasing and provision, and according to desconcentration process approved and implemented.
Value quantitative or Qualitative)
0
Organizational structure of the CCSS completed (June 2007) Organizational structure under implementation (June 2008)
Norms on the separation of financing, purchasing and provision executed (with counterpart funds). Diagnostic of the supply side.
Date achieved 06/30/2001 12/31/2009 11/01/2009 Comments (incl. % achievement)
Achieved (100%)
(b) Intermediate Outcome Indicator(s)
Indicator Baseline Value
Original Target Values (from
approval documents)
Formally Revised
Target Values
Actual Value Achieved at
Completion or Target Years
Indicator 1 : % of public and private hospitals accredited by MOH. Value (quantitative or Qualitative)
04 public hospitals plus 2 private hospitals
Pilot carried out in 3 public hospitals and 1 private
iv
hospital Date achieved 06/30/2001 12/31/2009 11/01/2009 Comments (incl. % achievement)
Partially Achieved
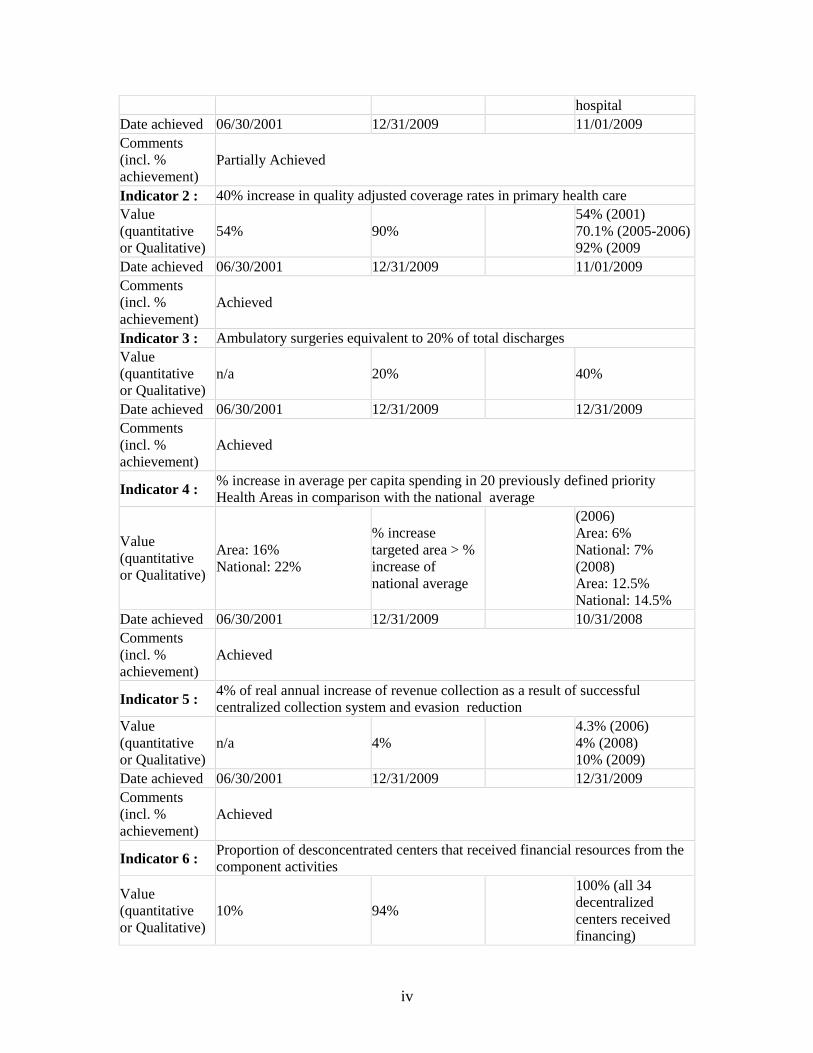
Indicator 2 : 40% increase in quality adjusted coverage rates in primary health care Value (quantitative or Qualitative)
54% 90% 54% (2001) 70.1% (2005-2006)92% (2009
Date achieved 06/30/2001 12/31/2009 11/01/2009 Comments (incl. % achievement)
Achieved
Indicator 3 : Ambulatory surgeries equivalent to 20% of total discharges Value (quantitative or Qualitative)
n/a 20% 40%
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Achieved
Indicator 4 : % increase in average per capita spending in 20 previously defined priority Health Areas in comparison with the national average
Value (quantitative or Qualitative)
Area: 16% National: 22%
% increase targeted area > % increase of national average
(2006) Area: 6% National: 7% (2008) Area: 12.5% National: 14.5%
Date achieved 06/30/2001 12/31/2009 10/31/2008 Comments (incl. % achievement)
Achieved
Indicator 5 : 4% of real annual increase of revenue collection as a result of successful centralized collection system and evasion reduction
Value (quantitative or Qualitative)
n/a 4% 4.3% (2006) 4% (2008) 10% (2009)
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Achieved
Indicator 6 : Proportion of desconcentrated centers that received financial resources from the component activities
Value (quantitative or Qualitative)
10% 94%
100% (all 34 decentralized centers received financing)

v
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Achieved
Indicator 7 : Proportion of the budget on drugs controlled by a computing system
Value (quantitative or Qualitative)
075% (June 2008) 100% (Dec. 2009)
35% (2006) 43% (June 2007) 75% (June 2008) 100% (Nov 2009)
Date achieved 06/30/2001 12/31/2009 11/01/2009 Comments (incl. % achievement)
Achieved
Indicator 8 : New strategy for human resource management approved and implemented Value (quantitative or Qualitative)
0Strategy approved and implemented
Strategy approved and implemented
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Achieved
Indicator 9 : At least 60% of contracts with CCSS health care providers include outcome indicators operating under performance contracts
Value (quantitative or Qualitative)
0
60% of contracts with CCSS health care providers include outcome indicators operating under performance contracts
100% of contracts with CCSS health care providers include outcome indicators operating under performance contracts
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Achieved
Indicator 10 : % increase in lower income patients’ satisfaction with CCSS health care providers
Value (quantitative or Qualitative)
84% 89% 2002: 84% 2004: 87% 2009: N/A
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Partially Achieved
Indicator 11 : Design and validation of the CCSS’ Strategic Plan (through 2025, with targets for 2006-2011)
Value (quantitative
0CCSS’ Strategic Plan Designed and
CCSS’ Strategic Plan Designed and

vi
or Qualitative) validated validated Date achieved 06/30/2001 12/31/2009 12/31/2006 Comments (incl. % achievement)
Achieved
Indicator 12 : Training workshop on the strategic Plan Value (quantitative or Qualitative)
0Training workshop conducted
Training workshop conducted
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Achieved (100%)
Indicator 13 : Number of health administrators trained in accordance with strategy prepared by CENDEISSS that come from the Health Areas with the lowest levels of efficiency
Value (quantitative or Qualitative)
0
20 health administrators and 73 medical directors trained
20 health administrators and 73 medical directors trained
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Achieved (100%)
Indicator 14 : Human resourcestrengthening and restructuring implemented according to MOH program: at least 500 people trained on management, public health, health economics and epidemiology.
Value (quantitative or Qualitative)
0 500people trained 110 people trained
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Partially Achieved (22%)
Indicator 15 : 50% of MOH regions having assumed the implementation of regulatory activitiesValue (quantitative or Qualitative)
050% of MOH regions
25% of MOH regions
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Partially achieved
Indicator 16 : Feasibility study for the development of new regulatory agencies to support the MOH in the execution of epidemiological surveillance, environment, food and drug testing and regulation.
Value (quantitative or Qualitative)
0Feasibility study conducted
Training of 10 MOH staff on environmental

vii
legislation, who are staffed in 8 of 9 regions.
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Partially achieved
Indicator 17 : 50% of MOH successfully implementing management agreements (Compromisos de Gestión) and performance evaluation systems
Value (quantitative or Qualitative) Date achieved
Comments (incl. % achievement)
Not carried out. This was never expected to be carried out by the MOH and should not have been included in the PAD. As a result of the changes in the health system, all health facilities from the MOH were transferred to CCSS management.
Indicator 18 : Regulation for quality assurance in providers, including hospitals, clinics, pharmacies, laboratories and others
Value (quantitative or Qualitative)
0Accreditation standards developed
Accreditation standards developed
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Achieved
Indicator 19 : % of health care workers at central, regional and local levels that are trained in leadership, public negotiation and strategic planning
Value (quantitative or Qualitative)
0 110 persons 100% (110 persons trained)
Date achieved 06/30/2001 12/31/2009 12/31/2006 Comments (incl. % achievement)
Achieved
Indicator 20 : Number of professionals at the central and regional level trained in environmental legislation
Value (quantitative or Qualitative)
0
10 professionals at the central and regional level trained
100% (10 professionals at the central and regional level trained )
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Achieved (100%)
Indicator 21 : Design the MOH Strategic Institutional Plan for 2007-2009 Value (quantitative
0 Plan Designed Plan Designed

viii
or Qualitative) Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Achieved (100%)
Indicator 22 : Implement communication plan on the MOH’s regulatory functions Value (quantitative or Qualitative)
0Communication Plan implemented
Plan designed and in process of being implemented.
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Partially achieved (50%)
Indicator 23 :
At least 70 percent of all healthcare providers (including at least 20 hospitals) have been included in the Regulation on Deconcentration and are operating in accordance with the Law and the Addendum to the management agreements (Compromisos de Gestión)
Value (quantitative or Qualitative)
0 70%
100% of all health providers have been included, including 15 hospitals.
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Achieved
Indicator 24 : Approval by the CCSS Board of strategies and investment plan to increase and to improve ambulatory solutions
Value (quantitative or Qualitative)
0strategies and investment plan approved by CCSS
Approved and implemented
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Achieved
Indicator 25 : At least 10 CCSS hospitals with a professional manager as CEO and working under rules and procedures of the Desconcentration norms (Reglamento de Desconcentración)
Value (quantitative or Qualitative)
0 10 hospitals
All hospitals have either professional manager or a medical doctor with training in hospital administration as CEO
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Achieved (100%)

ix
Indicator 26 : Continuation of the EBAIS model by consolidating all EBAIS opened until 2001 and by opening 100 more EBAIS and consolidating all EBAIS in the territory
Value (quantitative or Qualitative)
n/a 100 new EBAIS 962 EBAIS exist in the country
Date achieved 06/30/2001 12/31/2009 12/31/2008 Comments (incl. % achievement)
Achieved (100%)
Indicator 27 : % of first level health centers that have been trained in decentralized health management
Value (quantitative or Qualitative)
0 90% 55%
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Partially achieved
Indicator 28 : 40% decrease of time between initial bid and delivery of pharmaceuticals Value (quantitative or Qualitative)
0 40%decrease 50% decrease
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Achieved
Indicator 29 : 75% decrease of total pharmaceutical budget spent on warehouse storage costs Value (quantitative or Qualitative)
n/a n/a n/a
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
n/a
Indicator 30 : Design and implementation of an information system for accounting and inventory control in CCSS
Value (quantitative or Qualitative)
0Information system designed and implemented
System operating centrally and in all health centers
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Achieved (100%)
Indicator 31 : Improved equity by reducing the gap between the average per capita spending in health in the Brunca Region and the National Average by 50%, and then by another 50%
Value (quantitative
0 60%the gap between average per capita

x
or Qualitative) spending in the Brunca Region and the National Average was only 13.1% against a gap of 46% in 2002
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Achieved
Indicator 32 : Improved equity by reducing the gap between the average per capita spending in health in the Brunca Region and the National Average by 50%, and then by another 50%
Value (quantitative or Qualitative)
0 60%
the gap between average per capita spending in the Brunca Region and the National Average was only 13.1% against a gap of 46% in 2002
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Achieved
Indicator 33 : At least 40% of CCSS Health Areas have been surveyed and incorporated into SIPO
Value (quantitative or Qualitative)
n/a n/a
Changed to ’Ficha Familiar’ (household card), and implemented in one of five regions in the country (Sistema de Información Geroreferencial de la Región Huetar Atlántica)
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Partially achieved
Indicator 34 : Implementation of GDRs in hospital administration (based on an updated version of the software)
Value (quantitative or Qualitative)
0Implementation of GDRs in hospital administration
Implemented in 100% of hospitals.
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments Achieved (100%)

xi
(incl. % achievement)
Indicator 35 : Implementation of GDRs in hospital administration (based on an updated version of the software)
Value (quantitative or Qualitative)
0Implementation of GDRs in hospital administration
Implemented in 100% of hospitals.
Date achieved 06/30/2001 12/31/2009 12/31/2009 Comments (incl. % achievement)
Achieved
G. Ratings of Project Performance in ISRs
No. Date ISR Archived DO IP
Actual Disbursements (USD millions)
1 12/05/2001 Satisfactory Satisfactory 0.00 2 06/12/2002 Satisfactory Satisfactory 0.00 3 12/05/2002 Satisfactory Satisfactory 0.00 4 06/12/2003 Satisfactory Satisfactory 0.17 5 12/11/2003 Satisfactory Satisfactory 1.06 6 05/26/2004 Satisfactory Satisfactory 1.06 7 12/09/2004 Satisfactory Unsatisfactory 1.29
8 04/28/2005 Moderately
Unsatisfactory Unsatisfactory 1.49
9 06/23/2005 Moderately
Unsatisfactory Unsatisfactory 1.49
10 12/29/2005 Moderately
Unsatisfactory Unsatisfactory 1.49
11 06/21/2006 Moderately
Unsatisfactory Unsatisfactory 1.89
12 10/27/2006 Moderately
Unsatisfactory Unsatisfactory 2.30
13 12/19/2006 Moderately SatisfactoryModerately Satisfactory 2.30 14 06/19/2007 Moderately SatisfactoryModerately Satisfactory 2.61 15 12/20/2007 Moderately SatisfactoryModerately Satisfactory 3.46
16 06/30/2008 Moderately
Unsatisfactory Moderately
Unsatisfactory 5.17
17 12/29/2008 Moderately SatisfactoryModerately Satisfactory 7.00
18 06/19/2009 Moderately SatisfactoryModerately
Unsatisfactory 8.24
19 12/18/2009 Moderately SatisfactoryModerately Satisfactory 10.89 20 06/16/2010 Moderately SatisfactoryModerately Satisfactory 13.31

xii
H. Restructuring (if any) Not Applicable
I. Disbursement Profile

1
1. Project Context, Development Objectives and Design
1.1 Context at Appraisal 1. At the time of appraisal of the Second Health Sector Strengthening and Modernization Project (the Project) in 2001, the challenges that Costa Rica faced in its health sector were unique in Latin America: to maintain very good health conditions and a high level of access, while at the same time correcting underlying causes of inefficiencies and inequities in health service delivery so that an even higher level of performance could be achieved and sustained in the future. Over the ten years prior to appraisal, Costa Rica’s health indicators had continued to improve. Infant mortality was estimated at 10.3 per 1,000 live births, life expectancy had reached 77.6 years, and social insurance covered 85 percent of the population. Costa Rica’s health conditions were the best in Latin America, and in line with those of OECD countries. 2. In the early 1990s, Costa Rica introduced reforms to its health system whereby responsibility for provision of primary care was transferred from the Ministry of Health (MOH) to the Costa Rican Social Security Institute (Caja Costarricense de Seguro Social, or CCSS), and a population-based model of care was extended to relatively underserved rural populations. The reform brought several institutional and health care delivery changes. First, population-based “health areas” (Areas de Salud) were created, each covering approximately 50,000 people. The health areas represented a reorganization of the primary health care model. Each health area had about 10 Basic Health Care Teams (Equipos Básicos de Atención Integral en Salud, or EBAIS), which were introduced under the reforms. One EBAIS consisted of a physician, a nurse and a technician. In addition, reform brought the approval of a desconcentration law that increased autonomy of CCSS providers (“Ley 7852, Ley de Desconcentración”); and introduction of new management arrangements. 3. At the time of appraisal, significant improvements had occurred as a result of this reform process. Management contracts for health areas and major hospitals had been implemented successfully, generating innovation in hospital management and the use of budgets proposed on the basis of health outcomes. The monitoring of processes and evaluation of results had become fundamental to health care delivery in Costa Rica. 4. In spite of this progress, there were strong signals that further improvements in health service delivery were needed in order to address uneven quality and health outcomes. Quality deficits were still apparent at the level of primary health care—quality-adjusted coverage rates for key programs were about half as high as direct coverage rates. 5. More importantly, however, reforms in finance, organization and management required timely and strong follow-through to ensure that the health sector’s good performance could be sustained in the future. The present and expected future financial burden on the public sector was significant. In 2000, Costa Rica already allocated an

2
estimated nine percent of GDP to investments in health care, and changes in the country’s epidemiological and demographic profile were increasing pressure on health care spending. While Costa Rica did not envisage reducing government spending on health, the country was conscious of the need to allocate resources more equitably and efficiently in order to obtain better results and curtail future increases in health spending. While the health system guaranteed universal coverage, there were opportunities for improvement in assuring that good quality services reached disadvantages populations and that government resources were well targeted. 6. In this context, the Government, and the CCSS in particular, were eager to consolidate the 1990 reform and take on new challenges. The CCSS had plans to improve the allocation of resources by improving its existing algorithm and introducing a formula-based system that took into account population and health risk. The targeting system was to be improved to allocate public subsidies in a more equitable manner. CCSS planned to introduce a system whereby budget would be allocated based on performance, and sought to use incentive packages for health workers to motivate productivity and efficiency, to introduce mechanisms to reduce waiting lists and to make expenditures on pharmaceuticals more efficient. 7. At the time, Costa Rica faced three main categories of challenges in its health sector: (a) institutional strengthening and regulation; (b) health care service delivery; and (c) financing and resource allocation. In institutional strengthening and regulation,several pieces of legislation had major implications for the health sector, yet existing institutional and managerial structures and capacities were not prepared for their implementation. In addition, both public and private sub-sectors lacked appropriate regulation in many key areas of health care delivery, and medical education and continuing education required modernization and investment. Health care service delivery also required strengthening and adjustment. The health care delivery model needed to shift from costly inpatient to more efficient outpatient care for certain conditions and interventions. The pharmaceutical supply chain management was also inefficient, and out of step with other sector reforms. Investment in hospital infrastructure and equipment had lagged behind demand, inhibiting efficiency and quality. Information systems for providers remained weak, and increased attention to prevention and promotion was warranted. Finally, the system for health care financing and resource allocation was only weakly linked to health needs, performance or outcomes, as the introduction of annual performance agreements had not been fully supported by the required changes in the resource allocation model needed to ensure greater equity and improved targeting. 8. During Appraisal, the Government was seen as considering the health sector as an essential determinant of Costa Rica’s economic and social development, assigning to the sector a priority that was reflected in sustained high levels of spending and active policy attention at the highest levels. Building on previous successes that had been partially financed by the Bank under the Health Reform Project1, the Government had identified
1 Costa Rica Health Sector Reform Project, Loan No. 3654-CR dated December 6, 1993 for US$22 million, ICR Report No.25713 dated May 14, 2003.

3
specific plans to address the challenges it faced in institutional strengthening and regulation health care service provision, and financing and resource allocation. 9. To address the health sector’s institutional challenges, the Government was supporting efforts to reorganize and decentralize the CCSS’ functions, strengthen capacity of the newly autonomous health sector entities and complete the transformation of the MOH into an effective regulator. For improving the effectiveness and efficiency of the health care provision, the Government intended to encourage the shift away from over-dependence on inpatient service and introduce decentralized purchasing and distribution of pharmaceuticals, based on price and quality bidding processes by the health care facilities. To address challenges with respect to financing and resource allocation, the Government was committed to consolidate CCSS revenue collection for all areas of the country through improvement and extension of the Centralized Collection System (Sistema Centralizado de Recaudación - SICERE), developing effective supervision to reduce evasion and improve efficiency in collection, using Diagnostic Related Groups (DRGs) as a basis of reimbursement to complete the transition from allocations based on historical budgets to a performance-based system, and improving the targeting of resources toward underserved populations. 10. The Bank had supported Costa Rica in its 1993 health sector reform under a US$22 million loan for the Health Sector Reform Project. As it tackled even more complex tasks in the health sector, the Government sought the Bank’s continued technical and financial support under a follow-on project. The Project was fully consistent with the Bank’s Country Assistance Strategy (CAS)2, which identified health sector improvements as a critical -- and leading -- element in improvement of social programs. The CAS also highlighted the importance of improving efficiency, strengthening the referral system, channeling increasing resources to disadvantaged areas thereby improving equity, and integrating curative and preventive services. The Project was also consistent with a Social Expenditures Review that emphasized the need to improve resource allocation and equity, and develop mechanisms to encourage private sector participation. Finally, the Project was consistent with the Bank’s Health, Nutrition and Population (HNP) Strategy in that it recognized: (a) the Bank’s comparative advantage in the areas of system strengthening; (b) the importance of supporting reforms that separate the functions of financing, purchasing and provision of health services; and (c) the overall institutional mission to address the needs of poor and underserved populations.
1.2 Original Project Development Objectives (PDO) and Key Indicators 11. The Project aimed to improve health system performance and financial sustainability by supporting the policy changes that were ongoing in Costa Rica’s health
2 Costa Rica Country Assistance Strategy, Report No. R-93-57 dated March 10, 1993.

4
sector. Most of these changes were part of second-phase reforms in the CCSS. For the short- to medium-term, these policy changes aimed to: (a) align the organizational and functional structure of the CCSS with recent changes separating the financing, purchasing and provision of health services at all levels; (b) promote improvements in quality and fulfillment of consumer rights, as well as the efficiency and effectiveness of the MOH as a regulatory agency, by strengthening the institutional and regulatory framework; (c) improve the quality and efficiency of the CCSS health delivery system by supporting decentralization of decision-making, consolidation of the primary care delivery network through a population-based system, and introduction of performance-based incentives for providers; (d) reduce inefficiencies in the pharmaceutical sub-sector and promote rational drug use by introducing changes in the planning, purchasing and distribution of pharmaceuticals and supplies; and (e) develop financial mechanisms that would improve the equitable distribution of resources, improve efficiency in the provider payment mechanisms and strengthen CCSS’ capacity to collect payroll contributions. 12. Progress towards the Project’s Development Objectives would be measured through a monitoring and evaluation (M&E) system that would build on established information systems. The evaluation would collect and compare data before (baseline), during and after project implementation. For some outcome measures, comparisons would also be made between geographic areas that were supported by project interventions and those that were not, adjusting for certain factors. 13. The M&E system was designed to permit measurement of three types of indicators: (a) input indicators associated with investments/expenditures; (b) process indicators associated with completion of key project activities; and (c) outcome and/or impact indicators that were aimed at measuring the Project’s results in relation to its objectives. The number of indicators that were to be measured by the M&E system was extensive. The key output/impact-related performance indicators included the following:
¾ Coverage of priority primary health care (PHC) programs, as measured by the difference between the absolute coverage rates and quality-adjusted coverage rates. (The programs included well baby care, well child care, adolescent health, women’s health, adult health and elderly health.);
¾ Percentage of the population newly covered by the primary care model (EBAIS); ¾ Percentage of public and private providers accredited by the MOH; ¾ New organizational structure for the CCSS (based on separation of financing,
purchasing and provision functions) approved and implemented; ¾ Design and implementation of systems to improve equity in the distribution of
CCSS funds; ¾ New strategy for human resources management, including recruitment, staff
redeployment and training plans; ¾ Percentage of CCSS hospitals that have a professional manager as CEO; ¾ Percentage of hospitals operating under the rules and procedures of the Ley de
Desconcentración and corresponding regulations; ¾ Percentage of CCSS health care providers with performance contracts; ¾ Satisfaction of low-income patients with health service providers;

5
¾ Percentage change in ambulatory and inpatient surgery rates; ¾ Percentage of total pharmaceutical budget spent on rented, versus owned,
warehouse space; and ¾ Average processing time between initial bid and warehouse delivery of
pharmaceuticals.
1.3 Revised PDO (as approved by original approving authority) and Key Indicators, and reasons/justification The Project’s Development Objectives were not revised.
1.4 Main Beneficiaries 14. By providing support to the ongoing modernization in the CCSS and the MOH, the Project identified its expected beneficiaries as the four million persons covered by CCSS who would obtain better quality services (as described below), with a reduction in waiting times. The implementation of a management information system that would allow for more effective identification of the most disadvantaged CCSS members would improve targeting for an estimated 350,000 families. CCSS employees were expected to benefit from the implementation of the CCSS decentralization policy that would provide hospital managers more autonomy as well as additional resources to improve working conditions. 15. The Project was expected to result in the following benefits that would accrue to all CCSS beneficiaries: (a) universal coverage of the population under the EBAIS primary care model; (b) a MOH that was better prepared to enforce minimum quality standards for healthcare providers and to develop national health policy; (c) a CCSS organizational structure that would better respond to the needs of a decentralized framework and to the separation of functions; (d) reductions in unnecessary hospitalizations by increasing ambulatory surgery; (e) fewer instances where pharmacies run out of medicine stocks and a more efficient pharmaceutical supply chain; and (f) a more equitable distribution of resources.
1.5 Original Components 16. The Project consisted of two components described below: Component I, Policy Design and Implementation (estimated total cost US$20.75 million), would provide financing to develop the strategies and instruments required to achieve the objectives set forth in the Policy Activity Schedule (PAS, Annex 10). The strategies and instruments of the PAS focused on guaranteeing access to and provision of quality, effective and efficient health services in the CCSS. This component was to be executed through two main mechanisms, outlined below. 17. The first mechanism was to support the PAS’ objectives through financing of local and foreign consultants, information systems, development of supply chain

6
solutions, including e-procurement, equipment for EBAIS, training in health policy, clinical practice and management and study tours to incorporate international “best practice” into the Costa Rican health sector. The second mechanism for execution of this component provided for the allocation of an estimated US$9 million to decentralized subprojects with hospitals and health areas. Under this mechanism, health care providers that complied with the CCSS criteria for autonomy would assume direct responsibility over the procurement process for equipment, rehabilitation of infrastructure related to ambulatory care, information systems, consultant services and other innovative projects approved by the Project Coordinating Unit (PCU). This component was expected to support the CCSS’ overall policy to devolve responsibility to health care providers, allow greater decision making for administrators and speed up the procurement process. 18. Component 1 was designed to be implemented through activities supporting the CCSS, the MOH and sector coordination. The CCSS board would have an active role in evaluating and approving the critical strategies and instruments developed by the Project, and internal CCSS management units would have the responsibility of implementing the changes within the institution. For activities implemented by the MOH, the PCU would make resources available for the development of the proposed activities and would coordinate implementation with the Ministry. 19. The Project would support the following main activities for each of the PAS Areas: Institutional Strengthening and Evaluation (estimated cost US$4.6 million)
The objective of this PAS area was to strengthen and improve the CCSS and the MOH to allow each institution to better execute their functions and roles within the national health system. Strategies and instruments would focus on each institution’s organizational structure and functional divisions, human resource strategies and the regulatory framework, for the following activities: 20. Supporting the implementation of CCSS and MOH organizational and institutional restructuring processes that were designed and initiated under the Health Sector Reform Project (HRP) which was approved in 1993. Continued implementation would require ongoing support to redesign internal processes and organizational designs, to ensure that the organizational and functional structures ‘fit’ with the new roles in the health system:
¾ Providing ongoing support to the CCSS Purchasing Department (Dirección de Compra) to allow for further development of outcome-based indicators and to support the implementation of the national health plan (PASP) and the strategic health service plan (PESS);
¾ Strengthening of the systems related to planning, procurement and distribution of pharmaceuticals and medical supplies to CCSS providers, focusing on improving transparency, reducing inefficiencies, promoting rational use policies and re-engineering processes to reduce stock shortages, spoilage and theft;

7
¾ Supporting improved sector coordination among human development actors: CCSS, MOH, the Ministry of Education, and IMAS3; and
¾ Assisting the MOH with the development of regulations for quality assurance that promote a strengthened stewardship function for MOH.
Health Care Service Delivery (estimated cost US$12.3 million)
21. The objective of this PAS area was to strengthen the CCSS provider network to improve the quality, efficiency and effectiveness of health care services. The strategies and instruments developed would support the CCSS decentralization policy aimed at improving provider capacity to manage resources and improve responsiveness to consumer needs at the facility level, invest in ambulatory solutions that would allow the CCSS to consolidate and extend the implementation of the primary care model (EBAIS) and develop new instruments to improve supply chain efficiency for pharmaceuticals and medical supplies. 22. The activities in the area of implementation of the decentralized incentive framework would be financed by two different mechanisms, as described above. Under the first mechanism, providers undergoing decentralization would be supported in their efforts to decentralize, increase efficiency and promote greater use of ambulatory solutions through strategic planning and bidding processes supported by the CCSS and the PCU. This support was to be complemented by the use of grants for the implementation of subprojects that promoted decentralization and developed institutional capacity among health care providers. These grants, that were to be approved ex-ante by the CCSS, would finance two distinct types of activities: (a) subprojects to strengthen the provider’s capacity to assume decentralized management and improve the quality of care to patients; and (b) subprojects to increase ambulatory interventions, reduce waiting times and improve patient focus through the introduction of innovative interventions. 23. To support the improvements in the provider network, the Project would focus on:
¾ Support to CCSS providers throughout the implementation of the decentralization process, ensuring that they receive technical assistance and training required for a timely and successful implementation;
¾ Development and implementation of a comprehensive strategy to increase ambulatory solutions that leads to greater quality, user satisfaction and efficiency for CCSS hospitals. This would include ambulatory surgery, home care and other innovative solutions;
¾ Supporting providers through the implementation of policies related to decentralized purchasing of pharmaceutical and medical supplies. The actions would focus on building capacity in CCSS providers to assume their new responsibilities under the decentralization law; and
3 The project planned to support IMAS’ institutional modernization since it was responsible to update the Poverty Information (SIPO).

8
¾ Continuing to support the implementation of EBAIS in low-income regions that had not been fully developed under the prior Health Sector Reform Project and consolidate the development of the model in those areas that required additional support.
Financing and Resource Allocation (estimated cost US$3.84 million)
24. This PAS area was to support the development of resource allocation mechanisms that would promote greater equity in the CCSS and develop reimbursement mechanisms for providers that promoted incentives to increase quality and efficiency in the delivery network. It would do so through support to the following activities:
¾ Design and implementation of algorithms to improve equity in the distribution of CCSS resources to health areas;
¾ Implementation of the SIPO Population Identification information system (Sistema de Identificación de la Población Objetiva) to improve targeting of public subsidies to CCSS beneficiaries;
¾ Implementation of provider reimbursement mechanisms for health areas and hospitals that sought to introduce incentives to improve efficiency and quality of services, building upon previous developments in the areas of DRGs and capitation payments;
¾ Roll-out of the SICERE system to extend coverage of the CCSS collection system to the remaining branch offices; and
¾ Support to the CCSS in the development of actions required to ensure implementation of the Workers Protection Law (Ley de Protección del Trabajador).
25. Component II, Monitoring & Evaluation and Project Management (estimated total cost US$2.75 million) would support the development of an M&E system to provide for a comprehensive evaluation of the Project’s results as well as routine monitoring. This component also included resources to establish and sustain information, education and communication campaigns related to the modernization process. Resources were also to be provided to support the day-to-day operations of the Project Coordinating Unit that would assist the CCSS and other agencies involved in the reform process. The component was designed to finance local and international consultants, computers and office equipment, and the recurrent expenditures associated with management of the PCU.
1.6 Revised Components 26. The components were not revised during implementation. However, there was a cancellation of US$3 million in loan proceeds on June 13, 2005 (notified June 30, 2005), since IMAS failed to sign an agreement with the CCSS to implement the project activities for which it would have been responsible: specifically, the update of the Poverty Information System (SIPO) and support for IMAS’ institutional modernization. The reasons for which this agreement was not signed had to do with lack of accordance in the

9
country on what was required to ensure successful project implementation prior to Project approval. This is further explained later in the document (paragraphs 47 and 60).
1.7 Other significant changes 27. In addition to the US$3 million cancellation described above, there were several reallocations, closing date extensions, and minor modifications to the Project’s implementation arrangements. The Closing Date extensions were in response to the major delays in reaching loan effectiveness, and later in getting the Project off the ground, as well as circumstances in Costa Rica related to other externally-financed Health Projects. In addition, several activities originally included under the Project were carried out with government resources. 28. On April 27, 2006, the Bank agreed to a reallocation of loan proceeds to reflect higher than expected expenditures on goods and ambulatory solutions subprojects, and lower than expected expenditures on consultant services, training and decentralization subprojects. 29. On July 21, 2006, the Bank agreed to amend the Project Agreement to modify the Procurement Schedule to: (a) allow for the use of National Competitive Bidding for the procurement of works estimated to cost between US$350,000 equivalent and US$3.0 million equivalent, up to an aggregate of US$6.0 million equivalent; (b) increase the aggregate limits of goods procured under shopping procedures from US$2.5 million equivalent to US$6.3 million equivalent; (c) increase the aggregate limit of procurement of small works under lump-sum, fixed-price contracts awarded on the basis of three quotations from US$1.350 million equivalent to US$4.0 million equivalent, and (d) to increase the aggregate limit for consultant services procured with selection based on consultant qualifications. 30. On December 21, 2006, the Bank agreed to extend the loan’s December 31, 2006 Closing Date by eighteen months until June 30, 2008. 31. On April 28, 2008, the Bank agreed to again extend the loan’s Closing Date by an additional eighteen months until December 31, 2009. 32. On May 13, 2008, the Bank agreed to amend the Loan Agreement to increase the disbursement percentages to 100% across all expenditure categories and, in order to facilitate this, to apply the Country Financing Parameters for Costa Rica to the Project, inter alia, which does not permit taxes to be considered as an eligible expenditure. 33. On December 8, 2009, the Bank agreed to a reallocation of loan proceeds to reflect higher than expected expenditures on consultant services, training and decentralization subprojects, and lower than expected expenditures on goods and ambulatory solutions subprojects.
Category of Expenditure
Original Loan
Allocation after
Reallocation April 27,
Reallocation December
Final Allocation

10
Allocation Cancellation 2006 8, 2009 US $million
(1) Goods (except as under (4))
1.5 1.5 4.1 3.8 3.84
(2) Consultants’ Services and Audits (except as under (4))
6.0 3.5 2.1 2.3 2.2
(3) Training (except as under (4))
1.3 0.8 0.5 0.8 0.76
(4) Subprojects (a) Goods, works, consultants’ services and/or training for Decentralization Subprojects
4.0 4.0 3.3 4.7 4.63
(b) Goods, works, consultants’ services and/or training for Ambulatory Care Subprojects
2.5 2.5 3.55 1.7 1.7
Fee 0.17 0.17 0.17 0.17 0.17 Unallocated 1.53 1.53 0.28 0.53 0.69 TOTAL 17.0 14.0 14.0 14.0 14.0
2. Key Factors Affecting Implementation and Outcomes
2.1 Project Preparation, Design and Quality at Entry 34. Background Analysis. The background analysis that went into the Project’s preparation was extensive, drawing on the Bank’s longstanding support for Costa Rica’s health reform since it began in the 1990s. The prior Health Reform Project was completed in 2001 and the achievement of its development objectives was rated Highly Satisfactory.4 As a result, support for the Project was the logical next step in the Bank’s assistance, as it would provide continuing support for the implementation of Costa Rica’s health reform especially in the areas of institutional strengthening and regulation; health care service provision; and financing and resource allocation. 35. The PAD described lessons of experience from the HRP, similar Bank-financed projects in Latin America, and other projects financed by the Bank in Costa Rica. The lessons included those related to: (i) the process of designing and evaluating management contracts; (ii) the need for technical assistance to support the process of decentralization
4 Implementation Completion Report for the Health Sector Reform Project, Loan No.3654 –CR, dated December 6, 1993, Report No.25713

11
and bringing more autonomy to hospitals and health care areas; (iii) the fact that improvements in the planning, procurement and delivery of pharmaceuticals are some of the most difficult changes to introduce; (iv) the fact that the successful primary health care model (EBAIS) requires specific changes to be implemented in urban settings; (v) coordination with other reform efforts supported by other donors (e.g., restructuring of the MOH, then financed by the IDB), had proven successful; and (vi) prior misunderstandings between the requirements of the National Procurement Law (Ley de Contratación Administrativa), which exempted international financing agreements, and the hierarchy of Bank norms and procedures applicable to Bank-financed projects. 36. Previous Bank-financed projects in Costa Rica had experienced delays in procurement due to differences in the Government’s procurement policies and procedures and the Bank’s guidelines. As a result, the preparation team sought a legal opinion from the Government to the effect that since the Project involved external financing, the Bank’s procurement guidelines would take precedence over local legislation. The PIU decided to follow both guidelines simultaneously, which explains some delays in the completion of procurement processes. 37. Assessment of Project Design. The Project’s objectives and design were reasonable yet unquestionably ambitious in terms of the institutional capacity requirements for implementation. The PAD mentioned specifically that the “institutional capacity of the CCSS continues to be satisfactory while that of the MOH is less so”, and “the MOH has not produced satisfactory results, including substantial delays in implementation of its Action Plan”. The Project’s implementation arrangements were by and large the same that were in place for the HRP, and the same unit within the CCSS was to be responsible for overall coordination of the Project. The activities under the components were designed to achieve expected results, and the PAS and the corresponding Project Actions Matrix that fed into it provided a detailed “roadmap”, from activities through to objectives. 38. A design issue that in retrospect made little sense relates why the preparation team opted for contracting an external agency to design and implement the Project’s monitoring and evaluation system. As discussed below, the contracting of this agency ended up being very problematic and in the end, the PIU designed and implemented this system internally, with several activities (such as monitoring and evaluation of management agreements -Compromisos de Gestión-, equity-based resource allocation to health units, and others) internalized by CCSS operating departments. This revision made more sense: the unit that was responsible for implementation of the Project, and its coordination with other units in CCSS was made responsible for its monitoring and follow-up. The institution-building achieved, as well as coordination with the PIU and other CCSS units, would have been difficult had an external agency been entrusted with the Project’s monitoring. 39. There were several issues with respect to the Project’s preparation and timing that could have been addressed more systematically. The Project was not fully prepared at the time of approval, especially by current Bank standards that require completion of all

12
institutional arrangements and readiness of the project management unit to perform at the time the project is approved. In addition, recognizing the time required for approval of external funding by the country’s National Assembly, the Project’s schedule and timetable were overly optimistic—(five years with expected closing on December 31, 2006), especially considering that national elections were scheduled for early 2002 in Costa Rica. The project was under preparation in 2001, and it should have been foreseen that the 2002 elections would very likely affect eventual approval of the Project by the Assembly. 40. Finally, although potential problems with procurement had been identified up-front as a substantial risk that could affect implementation, in the end the Project’s design involved around 225 different procurement processes, of which only three involved goods or services costing over the equivalent of $1 million. 41. Government Commitment and Stakeholder Involvement. The Government’s commitment to the Project (and to its own process of health reform) was strong. Recognizing that the then upcoming national elections could lead to implementation delays, the Project’s preparation involved a broad process of consultation across political parties that indicated that the main themes of the reform would be adopted regardless of the outcome of the elections. Authorities of the CCSS held more than ten broad consultation meetings with key members of the main political parties involved in the healthcare sector. The PAS was discussed with these groups, and recommendations were built into the Project’s design. Specific consultations were also held with aspiring presidential candidates and key congressmen. 42. Consensus-building had been a critical element of Costa Rica’s health reform process from its very start. The first phase of the country’s health reform had built several mechanisms into the functioning of the health system that served to incorporate beneficiary input and feedback that guided the Project’s design. These include mechanisms to incorporate community participation in the primary care model, including specific activities where the community and stakeholders could be involved in planning and evaluation of health care services, and also in the establishment and implementation of the health care boards (Juntas de Salud). The Juntas were auxiliary entities designed to enhance the use of citizenship rights by making individuals co-participants in the definition, implementation, and monitoring of CCSS priorities. 43. Assessment of Risks. The Project’s risk matrix underestimated the number of risks, their ratings, as well as the risk the Project in its entirety, which received a modest risk rating. In the end, two identified risks, both rated as substantial in the PAD, impacted the Project from the beginning. The first identified risk was described as the “Government’s commitment and institutional stability” and the second was described as the “National contracting law procedures related to procurement will slow implementation”. Risks assessed during preparation did not include the risk of staffing changes, which as described below were a serious issue during the Project’s early years. Nor did preparation activities consider the risk that institutional agreements required for implementation (e.g., with IMAS), and that had not been secured during preparation,

13
would never materialize. The preparation process also failed to identify the potential risk of a major scandal that affected the main implementing agency’s credibility, although this would have been extremely difficult to foresee, especially in Costa Rica.
2.2 Implementation 44. The US$17 million loan for the Health Sector Strengthening and Modernization Project was approved by the Bank’s Board on July 12, 2001 and signed on August 23, 2001. The approval of the loan by Costa Rica’s National Assembly took significantly longer than originally expected, in part because approval was affected by the national elections in early 2002 and subsequent change in Government administration. Then, however, with Congressional approval secured on May 15, 2002, it took the Borrower almost an additional eight months to comply with conditions of effectiveness. The loan only became effective on January 9, 2003, almost eighteen months after approval by the Bank’s Board. 45. With a difficult and significantly delayed start, the Project faced important challenges that, together with weaknesses in preparation, affected performance throughout the implementation period. From December 2004 through October 2006, one or more of the ratings covering the Project’s Implementation Progress, Development Objectives, component and other issues were either unsatisfactory or moderately unsatisfactory. Even with the $3 million cancellation in June 2005, disbursements lagged until almost the last two years of the Project. In late 2006 and early 2007, with new leadership in the CCSS at all levels, implementation began to turn around. The Project was able to accomplish in its last three years a range of objectives that it had been unable to even start in its first four years of implementation. 46. Incomplete Preparation. There were several aspects of the Project’s preparation that were not in place when it was approved. These included the Operational Manual (including the definition of management procedures for subprojects in line with the Loan and Project Agreements), the first year’s Annual Action Plans and Procurement Plans, the Institutional Agreement between CCSS and the IMAS, and the Terms-of-Reference (TORs) for contracting of the agency that would handle external monitoring of the Project. Inter-institutional agreements to formalize the Project’s implementation arrangements had not been drafted, much less formalized. Internally, the Bank still had issues with arrangements for procurement, for example, to the point that although it was not a formal condition of effectiveness, the Bank requested a revision of a supplementary legal opinion (which had been issued on September 11, 2002 and considered insufficient by the Bank) dealing with certain applications of the Bank’s Guidelines for contracting consultants. 47. These arrangements and documents that were not formalized could have caused delays in and of themselves, but the reality was that there was no agreement internally in Costa Rica on what was required to ensure successful project implementation, nor was there documentation that confirms a joint vision between the Bank and the Government on what was required in terms of fiduciary and institutional arrangements to ensure satisfactory performance of the project. As a result, the back and forth on reaching

14
agreement on several issues (such as the MOH’s first year Action Plan, the Terms of Reference for contracting an M&E agency, and the criteria for selecting, evaluating and implementing subprojects) resulted in additional delays. The case of the Institutional Agreement between CCSS and IMAS was by far the most extreme example of lack of up-front preparation that should have been carried out. When discussions regarding this Agreement began in Costa Rica, the Contraloria General de la República issued legal opinions against its signing. For a couple of years the subject was under discussion at the highest levels of Government until finally, on June 13, 2005, the MOF decided to request cancellation of funds allocated to IMAS for the strengthening of the SIPO. Obviously, without an Institutional Agreement in place, funding for carrying out scheduled activities was not provided (and CCSS came up with alternative mechanisms to replace the information the SIPO was to provide). Similarly, on June, 25, 2005 the Contraloria General de la Republica decided that a formal agreement was needed between the MOH and CCSS, and funding was delayed pending signature of that agreement. 48. Changes in Administration, Staffing and Reporting Arrangements for the PIU. From the beginning of implementation, the Project was affected by changes in government and government-appointed staff that were responsible for various roles and activities. Both the Minister of Health and the President of the CCSS were changed as well as the Executive Director responsible for the PIU in the CCSS. Annex 12 presents a table summarizing the various changes at all levels that affected the environment within which the Project was implemented. In all, during implementation, there were three different government administrations (following electoral processes in February 2002 and February 2006), five Presidents of the CCSS (following changes in government administrations and the allegations of corruption described below) and six Executive Directors of the project’s implementation unit (following changes in the Presidents of the CCSS).
49. In addition, the reporting arrangements and focus of the unit responsible for the Project’s management in the CCSS were modified on several occasions. These changes left the implementing responsibility of the project management unit poorly defined. Originally, this unit reported directly to the CCSS Executive President. Project activities related to planning, contracting and monitoring were implemented through the CCSS Directorates under the overall coordination of this unit. In 2006, what had essentially been a Project Coordination Unit responsible for coordinating the Project’s overall implementation was transformed into a Project Implementation Unit (PIU) under the Operational Directorate5. The PIU became more active in project decisions relating to planning, contracting and monitoring, and took the leadership and responsibility for the project’s successes and failures. In addition the PIU worked in a coordinated fashion with all of the CCSS’ Directorates, using the institution’s established processes and procedures, while ensuring their compatibility with the Bank’s requirements.
5 CCSS’ Operational Directorate was split in 2006, and from that time, the PIU reported to the new Directorate of Infrastructure and Technology.

15
50. CCSS Allegations of Corruption. In early 2004, the media in Costa Rica announced several cases of alleged corruption, involving several former presidents of Costa Rica as well as a former President of the CCSS. The first case that was made public involved a loan to the CCSS for the procurement of medical equipment, of which about 20 percent had allegedly been diverted for other purposes. High level CCSS authorities were prosecuted and placed under arrest. The internal and external credibility of the CCSS’ management immediately came into question and clearly affected the management decisions within the CCSS related to purchases of goods and services. Managers in the CCSS delayed or postponed decisions related to purchases and contracts, since many CCSS procurement actions started to be intensively reviewed by the National Controller’s Office and Internal Auditing Unit. 51. In response, the President of Costa Rica appointed a Special Committee to investigate CCSS management, and requested extensive information regarding the implementation of both the prior HRP and the current Project. The results of this investigation showed the allegations to be more political than technical. With respect to both of the Bank-financed projects, the investigation revealed only minor questions about contracting of one staff as well as more extensive questioning about what the Committee felt were excessively high expenses for consultancies. 52. This overall situation impacted the Project and its implementation adversely in several ways: (i) the new CCSS Board of Directors recentralized all project-related decisions; (ii) internal administrative and legal reviews of project-related procurement decisions began to be scrutinized, increasing substantially the already excessive steps and time involved in what should have been normal reviews; (iii) all externally-financed projects started to be viewed with extreme distrust, especially regarding the financing of consultancies. In addition, there was a major change in staffing of the CCSS from its President, Directing Board, and Legal Department down through other levels. 53. Procurement. Despite the up-front agreement that Bank procurement guidelines would take precedence over local legislation for all project procurement, ambiguity regarding the appropriate procedures to follow, and the increased scrutiny that the CCSS faced after the allegations of corruption, created a situation in which the procurement of works, goods and service under the Project became extremely complex and time-consuming. When implementation improved and procurement got underway in earnest, procurement was carried out in a manner that followed both local legislation and Bank guidelines. Even so, this required an enormous effort on the part of the PIU to ensure appropriate follow-up and adherence to schedules. In addition, procurement decisions were also delayed by a critical factor that had not been identified during the Project’s preparation: the time it took for internal approvals of large procurements under the CCSS internal procedures. Under those procedures, the Junta Directiva was required to provide ex-ante approval of contract awards of more than US$1 million. Composed of nine members (divided evenly among organized labor, the private sector and government) the Junta is an ad-hoc group that meets periodically on dates scheduled in advance. Therefore, if the Junta raised any questions regarding a proposed award that required
16
research or investigation, resolution would not happen until the next scheduled meeting of the Junta.
54. The problems that the Project faced with procurement caused important delays in the contracting of goods, works and services. These delays were eventually addressed by the PIU, which in the end was able to recover previous slippages and implement most of the Project’s activities in its final years. However, by that point, the mentioned problems had driven the CCSS to finance several of the activities that were to be financed by the Bank with its own internal resources. The activities that the CCSS self-financed included small works, rehabilitation of health facilities, and other purchases of goods that the PIU considered difficult to implement in a reasonable time period using the Bank’s procedures. A major factor why this happened was because some Units within the CCSS were not fully engaged with the procurement process and execution of the Bank’s Project. 55. Actions Taken in Response to Problems. Starting in 2005, CCSS and the Bank’s supervision team intensified efforts towards getting the Project’s implementation back on track. This was accomplished in part through the preparation of a very detailed Action Plan setting out a critical path of activities and procurement actions that would be necessary to bring implementation to a successful conclusion. This Action Plan was monitored closely by staff of the PIU and the Bank.
2.3 Monitoring and Evaluation (M&E) Design, Implementation and Utilization 56. Monitoring and Evaluation Design. A comprehensive monitoring and evaluation system was to be developed during the first six months of the Project. The system was to be managed by a third party to ensure transparency and lack of bias in the evaluation process. The M&E system was to be used to carry out bi-annual evaluations with the Bank; these evaluations were to be an integral part of the planning process to guarantee that the proposed investment plans were directly related to the social development objectives. The evaluations were to include all key performance indicators, in addition to other indicators that the CCSS and the Bank would agree to include for M&E purposes. The Project was to be monitored according to compliance with the PAS and the Project Actions Matrix (Annex 11). Some of the defined indicators were complex, and depended on several variables. Beneficiary assessments and surveys on user satisfaction that had been conducted during the previous Health Reform Project and that had been used as an instrument for performance and evaluation would be updated under the Project. 57. With assistance under the Project subcomponent “Financing and resource allocation”, CCSS planned to improve its allocation of resources by improving the then existing algorithm and introducing a formula-based system that took population and health risk into account. The targeting system used by SIPO was to be improved in order to allocate public subsidies in a more equitable manner. 58. Monitoring and Evaluation Implementation. The contracting of a third party to design and maintain the Project’s M&E system was continuously delayed due to problems in contracting. In a first attempt, there was a conflict of interest in one of the

17
firms selected to implement this task. In a later attempt, there were no qualified bidders. The MOF provided software they had developed for project monitoring, but the PIU felt that the system did not meet the Project’s needs. The PIU then developed a very detailed system for monitoring implementation and progress toward the Project’s development objectives. Starting in early 2007, the PIU developed and/or relied upon systems to monitor several key elements and activities: (i) the Project’s monitoring indicators and the PAS; (ii) critical procurements and other actions needed to keep the Project on track; (iii) progress in implementation of the sub-projects; (iv) the CCSS’ existing internal control systems; (v) internal auditing by the CCSS; and (vi) external auditing by the Contraloria General de la República. The last three included financial management and monitoring the use and application of resources and internal control systems. 59. Monitoring and Evaluation Utilization. Baseline data for the Project’s monitoring indicators only became available in 2006, and was only used as an instrument to monitor progress since that time. Starting in mid-2007, project monitoring became a priority to the PIU, which assigned high importance to getting the Project on track and overcoming the previous delays in implementation. The PIU adopted strict measures to monitor project activities, including progress toward objectives. Together with the Bank, the Project’s procurement and activity monitoring system was updated and reviewed weekly, with follow-up actions identified to ensure compliance with strict deadlines that were designed to bring the Project and the activities it financed to a satisfactory completion. 60. Several monitoring activities included in the Project’s design were carried out by the CCSS operational directorates and monitored for purposes of the Project’s objectives by the PIU. These activities include the allocation of resources to health regions on the basis of equity considerations (by the CCSS Administrative Management Directorate); the establishment, agreement, monitoring and follow-up to the Compromisos de Gestión (by the CCSS Administrative Management Directorate); and the efforts to increase efficiency in the procurement and distribution of pharmaceuticals and other medical supplies (by CCSS Medical Management Directorate). Because of the issues with signing the Inter-Agency Agreement with IMAS, the Project’s activities related to the strengthening of the IMAS database were never implemented. As an alternative, CCSS opted to establish a new system of identifying poor households, Ficha Familiar, that will provide more extensive, broader, information on all CCSS beneficiaries across the country, through a census, that gathers important vital statistics, health information, information on living conditions and consumption. The Bank provided hands-on technical assistance to the establishment of this system that is being utilized on a pilot basis to prioritize the allocation of resources, thereby furthering the Project’s equity objectives.
2.4 Safeguard and Fiduciary Compliance 61. Safeguard. None of the Bank’s Safeguard policies were triggered by the Project. While the Project was to deal mostly with institutional and organizational issues in the health sector, there were activities to be financed that would enhance the ability of the CCSS to increase ambulatory surgery in order to rationalize hospitalization use when appropriate, and for this reason an environmental assessment was prepared. The
18
preparation team analyzed all environmental legislation in Costa Rica and the procedures used in hospitals for waste collection, disposal and/or storage, related issues with transportation of waste, etc. The team, in consultation with the CCSS, the MOH and environmental health specialists, concluded that the Project should not include special environmental measures beyond those already being followed by the CCSS, and the regulatory efforts by the MOH. 62. The vast majority of sub-projects and activities carried out under the Project incorporated the country’s indigenous areas. In such areas, equity was interpreted as ease of access. To this end, activities included the improvement of information systems with the introduction of the automated Ficha Familiar, the Geographic Information System for Epidemiology, the incorporation of GPS (Global Positioning System) for location of homes, and the Integrated Pharmacy system. In addition, access to primary care technicians was improved through the provision of all-terrain vehicles and the ‘floating hospital’, and service delivery was strengthened by improving the cold chain for more effective vaccination delivery as well as equipment to enhance problem-solving in health services. The impact of these and other cross-cutting efforts has contributed to the reduction of infant mortality. 63. Procurement. The Project’s procurement capacity assessment had concluded that based on the experience under the ongoing Health Reform Project, the PCU had adequate coordinating and operational arrangements for the new Project. However, the assessment identified the following issues: (i) difficult national procurement environment in light of the conflicts between the Bank’s guidelines and national contracting law, as well as controversies resulting from the ex-post review by the Contraloria General de la República (CGO) of signed contracts, which often required conformity with national law; (ii) added responsibilities of the PCU in responding timely and effectively to the delays in project Procurement and Contracting Plans, and following up of frequent bidder disputes; and (iii) capacity of the PCU to coordinate and advise the health units in the procurement of inputs included in their sub-projects. An Action Plan to strengthen and enhance the procurement capacity of the PCU was agreed with the Bank during preparation. As described in Section 2.2 above, procurement was one of the biggest challenges the Project faced during implementation. 64. Financial Management. The Project’s financial management assessment similarly concluded that the PCU had in place adequate financial management arrangements for the then ongoing Health Reform Project, and an Action Plan for enhancing those arrangements and adapting them to the new Project was agreed. The signing of a contract with the Project’s external auditors was complied as a Condition of Effectiveness. Despite a few comments on the Project’s external audits that were addressed by the PCU, financial management arrangements proceeded rather smoothly and there were no significant issues with the external auditors’ opinions.
2.5 Post-completion Operation/Next Phase 65. Since completion, the Project has become a program maintained and managed by the Government. While a next phase Bank project is not currently being prepared, a

19
furthering of the Project’s objectives is fully incorporated in the current operational plans of both the Government and the CCSS. The Project was carried out by CCSS and MOH staff, and these institutions remain responsible for continuing to pursue the reforms, activities and other objectives with their own financial and staff resources. 66. Costa Rica has recently gone through a national electoral process, and a new Government administration took office in May 2010. While specific details of the new Government’s program were not available at the time of ICR preparation, some themes are already apparent. The new President’s Program, Plan de Gobierno 2010-2014,recognizes Costa Rica’s achievements in health, especially vis-à-vis other countries of similar income levels, and prioritizes programs to improve coverage, quality and service delivery within an overall framework of greater efficiency in resource usage. Specifically, the Plan de Gobierno 2010-2014 maintains and aims to improve the health service delivery model supported by the Project. Specifically, the Plan calls for creating 150 new EBAIS, improving another 100 EBAIS in lower income areas of the country, and promoting even more ambulatory solutions as a means of making services more responsive, timely and efficient. It also prioritizes a further strengthening of the CCSS, to be achieved through more financing, staffing and through greater use of information and technology to strengthen its internal managerial and external service provision functions. 67. For its part, the CCSS Strategic Plan 2007-2012 emphasizes the objectives that were supported under the Project while reaffirming the institution’s objectives to reduce disparities in health service delivery through a sustained effort to improve physical, technological, human resource and process improvements in the primary and secondary health service networks. At the same time, CCSS will continue to pursue more efficient service provision at its hospitals through increased incorporation into the primary and secondary health networks, and through greater ambulatory and other work process improvements. The CCSS strategic plan identifies five challenges moving towards 2025: (i) Costa Rica’s demographic transition which means an aging population and its consequent implications for contributions and demand for health care; (ii) the country’s epidemiological transition, whereby the leading causes of death will become similar to those of a developed county, resulting in higher costs to the system as a whole; (iii) changes in the structure of the labor market, with a reduction of employment in agriculture in favor of services, that will require efforts for the CCSS to incorporate a greater number of independent workers, often under temporary contracts; (iv) a steady flow of immigrants, and the need to address their needs to maintain internal cohesion in the country; and (v) the Government’s ability to regulate effectively the provision of complementary areas and/or sectors such as the quality of water resources, protection of the environment, public transport, education and culture, all of which ultimately have an impact on the health status of Costa Rica’s citizens.
3. Assessment of Outcomes
3.1 Relevance of Objectives, Design and Implementation

20
68. The Project’s objectives were and continue to be extremely relevant to Costa Rica’s health sector strategy. The project spanned and was consistent with two CASs. As described in Section 2.5 above, the objectives are fully aligned with the country’s and the CCSS’ current development priorities. Bank assistance, especially starting in 2006, was responsive to helping the Borrower make up for initial delays in the Project’s implementation and ensuring progress towards its development objective (Section 5.1 (b)). The PDOs were ambitious, but as they were and continue to be aligned with those of the Government; they in fact represented the Government’s own goals. Perhaps more than the PDOs themselves, individual targets in the PAS were ambitious, and given delays and other implementation problems described in Section 2.2, were in some cases only partially achieved.
3.2 Achievement of Project Development Objectives 69. The Project’s progress towards the achievement of its Development Objectives is presented below, according to the indicators and targets set out in the PAS. Overall, the Project met most of its expected objectives, only falling short in the extent of achievement of those objectives as a result of initial implementation delays. There is every reason to believe that with continued priority assigned to the health care delivery model that the Project supported, full achievement of the objectives and targets will be achieved in the near term. (a) To align the organizational and functional structure of the CCSS with recent changes separating financing, purchasing and provision of health services at all levels; 70. The Project accomplished this objective with only minor shortcomings. Costa Rica’s health care delivery system is composed of three integrated layers of health institutions: at the top, seven large general and/or specialized national hospitals that deliver services to the entire population based on need; three large health networks or redes (Red Noroeste, Red Este, Red Sur) each divided into regions by population (8 in total, including the metropolitan San Jose region) that include regional hospitals; and then Equipos Básicos de Atención Integral de Salud (EBAIS) which are composed of a general medical practitioner, a nurse auxiliary, a pharmacy auxiliary and a primary health technical assistant, and are also created or identified based on population. At present, there are 962 EBAIS functioning in Costa Rica, each composed of a team of at least a medical practitioner, a nursing assistant and a technical assistant in primary care. Some EBAIS also have a pharmaceutical assistant and an assistant for health statistics. All of these health units, general or specialized hospitals, regional hospitals or EBAIS are currently operating under management agreements (Compromisos de Gestión) with the CCSS’ Dirección de Compra de Servicios de Salud. This arrangement has resulted in health services coverage of 100% throughout the country.
Objective Indicator Achieved

21
Objective Indicator Achieved
Indicators in the PAS New organizational structure of the CCSS-based on separation of financing, purchasing and provision and according to decentralization process approved by CCSS Board and implemented
Achieved. Norms on the separation of financing, purchasing and provision executed with counterpart funds. Diagnostic of the supply side carried out.
Introduce the organizational changes that required to prepare the CCSS for increasing decentralization and other changes related to the separation of financing and provision
New strategy for human resource management approved and implemented
Achieved. (with CCSS resources)
Continued strengthening and consolidation of the Dirección de Compras in the CCSS
At least 60% of contracts with CCSS health care providers include outcome indicators operating under performance contracts
Achieved. (with CCSS resources) All contracts with health care providers operate under performance contracts.
40% increase in quality adjusted coverage rates in primary health care
Achieved. Children under one year:06/30/2001 – 54% 2005/2006 – 70.1% 11/01/2009 – 92%
% increase in lower income patients’ satisfaction with CCSS health care providers
2002:83.91% 2004:86.7% 2009 N/A
Other Indicators Design and validation of the CCSS’ strategic plan (Plan Estratégico) through 2025, with targets for 2006-2011.
Achieved. CCSS Strategic Plan 2007-2012 designed and validated (December 2006)
Training workshop on the Strategic Plan (Plan Estratégico)
Achieved.
Number of health administrators trained in accordance with strategy prepared by CENDEISSS that come from the Health Areas with the lowest levels of efficiency
Achieved.20 health administrators and 73 medical directors trained, (2009)
(b) To promote improvements in quality and fulfillment of consumer rights, as well as the efficiency and effectiveness of the Ministry of Health (MOH) as a regulatory agency, by strengthening the institutional and regulatory framework.

22
71. The Project achieved this objective with minor shortcomings. Because of delays in implementation, activities designed to achieve this objective began later than anticipated, with the result that while the overall framework for strengthening the MOH in its new regulatory role is in place, progress towards expected targets was slower than originally envisaged. 72. The MOH designed and published its Plan Strategic 2008-2010 following a participatory course designed and delivered to all of the institution’s managers at the central, regional and area levels. The course focused on public negotiation and leadership of and strategic planning in public institutions, and culminated with the preparation of its strategic plan. The strategico Plan clearly identifies the MOH’s regulatory role in the health sector under one broad strategic area, with five specific objectives: (i) strengthen and maintain health surveillance activities; (ii) formulate the National Health Policy and strategic plans in health; (iii) oversee the use of financing for public health to guarantee equitable access to health services and protection of the environment; (iv) develop, maintain and promote the national system of scientific and technological development in health; and (v) develop and monitor the system for impact evaluation of health programs. The Plan also contains institutional actions and requirements for accomplishing these objectives, and detailed indicators and time-bound targets for the three-year period, and is available to the public on MOH’s website. Those requirements include, among other things, the modernization of the MOH’s information technology platform, which the Project supported through purchase of equipment, software, training and systems design. At the same time, it was considered important that the general public understand the MOH’s new regulatory role, and a Communications Plan was prepared and is currently being implemented. 73. With technical assistance supported by the Project, the MOH developed standards for hospitals; designed a sustainable accreditation process that emphasizes the evaluation of hospital processes and results to be rolled out country-wide; trained interdisciplinary and inter-institutional teams in carrying out the accreditation process; designed a system for analyzing the resulting information; and created, defined and strengthen the institutional structure needed to ensure its sustainability. The new hospital standards cover the following areas: (i) attention to patients; (ii) emergencies; (iii) obstetrics; (iv) operating facilities; (v) human resources; (vi) information management; (vii) environmental management; (viii) leadership; and (ix) training and internships (for hospitals with medical training programs). Four pilot hospitals (a national, a regional, a local and a private hospital) were selected for rolling out the accreditation process. Twenty-two external evaluators and six evaluators from the MOH’s Dirección de Servicios de Salud, Unidad de Acreditación responsible for accreditation received training on the evaluation process, and the respective coordinators in each of the four hospitals received training on preparing a self-evaluation to start the process. Following the self-evaluation, the accreditation process was continued through the visit of the external evaluators (in teams of two, including an external evaluator and one from the MOH) and the preparation of the evaluation report, including requirement for follow-up by the hospital to receive accreditation. Recommendations from the pilot experience include: (i) MOH should establish a continuous program of training in hospital
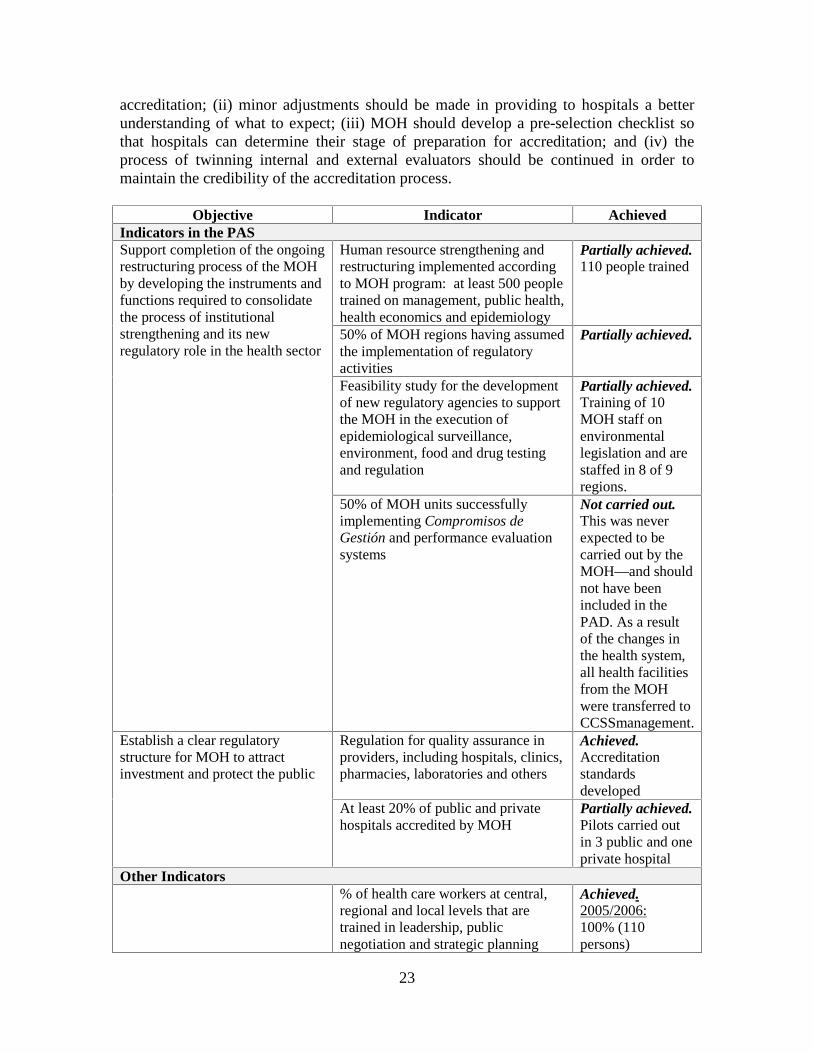
23
accreditation; (ii) minor adjustments should be made in providing to hospitals a better understanding of what to expect; (iii) MOH should develop a pre-selection checklist so that hospitals can determine their stage of preparation for accreditation; and (iv) the process of twinning internal and external evaluators should be continued in order to maintain the credibility of the accreditation process.
Objective Indicator Achieved Indicators in the PAS
Human resource strengthening and restructuring implemented according to MOH program: at least 500 people trained on management, public health, health economics and epidemiology
Partially achieved. 110 people trained
50% of MOH regions having assumed the implementation of regulatory activities
Partially achieved.
Feasibility study for the development of new regulatory agencies to support the MOH in the execution of epidemiological surveillance, environment, food and drug testing and regulation
Partially achieved. Training of 10 MOH staff on environmental legislation and are staffed in 8 of 9 regions.
Support completion of the ongoing restructuring process of the MOH by developing the instruments and functions required to consolidate the process of institutional strengthening and its new regulatory role in the health sector
50% of MOH units successfully implementing Compromisos de Gestión and performance evaluation systems
Not carried out. This was never expected to be carried out by the MOH—and should not have been included in the PAD. As a result of the changes in the health system, all health facilities from the MOH were transferred to CCSSmanagement.
Regulation for quality assurance in providers, including hospitals, clinics, pharmacies, laboratories and others
Achieved. Accreditation standards developed
Establish a clear regulatory structure for MOH to attract investment and protect the public
At least 20% of public and private hospitals accredited by MOH
Partially achieved. Pilots carried out in 3 public and one private hospital
Other Indicators % of health care workers at central, regional and local levels that are trained in leadership, public negotiation and strategic planning
Achieved.2005/2006:100% (110 persons)

24
Objective Indicator Achieved Number of professionals at the central and regional level trained in environmental legislation
Achieved. 10 persons
Design the MOH Strategic Institutional Plan for 2007-2009
Achieved.
Implement communication plan on the MOH’s regulatory functions
Partially achieved. Plan designed and in process of being implemented.
(c) To improve the quality and efficiency of CCSS’ health delivery system by supporting decentralization of decision-making, consolidation of the primary care delivery network based on a population-based system, and introduction of performance-based incentives for providers; 74. The Project achieved the above objective with minor shortcomings. As described under the first objective in this Section and in the table below, CCSS made significant progress in decentralizing decision-making, consolidating the primary health care delivery networks and introducing performance-based incentives to providers. CCSS reports that in 2008, 70 percent of the targets set in the aggregate of its management agreements (Compromisos de Gestión) were met. The CCSS was able to improve the overall quality and efficiency of health services delivered through several efforts: (i) a significant expansion in the number of operating EBAIS; (ii) performance agreements with health care providers; (iii) the development of guidelines for ambulatory surgeries; (iv) extensive training efforts for both hospital administrators and staff of health units in decentralized management (on normative and legal aspects of health networks, planning, health care delivery models, human resource management, among other topics), supported by subprojects that financed medical equipment, information technology equipment and software; and (v) technical assistance for process improvements in health units. In all, 60 subprojects financed some combination of the above inputs for 17 health areas, 6 peripheral hospitals, 13 regional hospitals, and 7 national hospitals, for a total value of US$6.2 millions 75. A pilot plan for ambulatory surgery was introduced in two national hospitals and one regional hospital, and has since been expanded to another national hospital. In all, ambulatory services have increased, and now represent about 40 percent of all hospital discharges, more than double the initial target. In its 2008 Annual Report, CCSS reports that as a result of this plan, the waiting list for surgery at the national level has dropped for the first time in five years. In addition, the first three hospitals to participate in the pilot plan reported that their surgery waiting lists have dropped by about 30 percent, on average.
Objective Indicator Achieved Indicators in the PAS

25
Objective Indicator Achieved At least 70 percent of all healthcare providers (including at least 20 hospitals) have been included in the Regulation on Deconcentration and are operating in accordance with the Law and the Addendum to the Compromisos de Gestión
Achieved. 100% of all health providers have been included, including 21 hospitals
Approval by the CCSS Board of strategies and investment plan to increase and to improve ambulatory solutions
Achieved. Approved and implemented.
To improve efficiency, quality and client/patient focus through the mechanisms in the Law on Desconcentration
At least 10 CCSS hospitals with a professional manager as CEO and working under rules and procedures of the Reglamento de Desconcentración
Substantially achieved. All hospitals have either professional manager or a medical doctor with training in hospital administration as CEO
To promote the development of outpatient and home care solutions to improve efficiency and patient focus
Ambulatory surgery to be 20% of total hospital discharges
Achieved. 2009 –40%
Continuation of the EBAIS model by consolidating all EBAIS opened until 2001 and by opening 100 more EBAIS and consolidating all EBAIS in the territory
Achieved.962 EBAIS exist in the country (2008)
Other Indicators % of decentralized health centers that receive financing under subprojects
2005/2006:79% (27 out of 34 decentralized health centers)
% of decentralized health centers that receive financing under component I
Achieved 2009: 100% of the 34 decentralized centers
% of first level health centers that have been trained in decentralized health management
2005/2006:55%
(d) reduce inefficiencies in the pharmaceutical sub-sector and promote rational drug use by introducing changes in the planning, purchasing and distribution of pharmaceuticals and supplies; 76. This objective was achieved with only minor shortcomings. A key activity was the introduction of an integrated pharmaceutical information system, Sistema Integrado en Farmacia (SIFA) that monitors and follows pharmaceuticals through purchasing,

26
distribution, inventory management and dispensing to patients. Approximately 86 percent of CCSS’ health units were linked to the system in January 2010, and plans are in place to cover the remainder by the end of the year. Survey results show that waiting times for pharmaceuticals have dropped by as much as 50 percent, while around 98 percent of needed pharmaceuticals are on hand at any given time. Further, SIFA has delivered other important results: (i) errors in dispensing medications and prescriptions have been reduced, especially for patients that are treated in different health units; (ii) users’ prescription history is recorded, feeding into the system for purchasing and distribution; (iii) inventory costs have been reduced; (iv) SIFA facilitates purchasing and distribution based on epidemiological characteristics of beneficiaries by health unit; (v) SIFA permits improved budget planning based on better estimates of purchasing requirements, not only at the national level but at the level of health units as well; and (vi) SIFA reduces wastage of unutilized pharmaceuticals. 77. CCSS also reviewed and introduced improvements in pharmaceutical and medical equipment procurement arrangements looking carefully at local legislation, costs, and services offered by providers, process control and packaging quantities. CCSS also implemented measures to reduce storage costs for pharmaceuticals. By redesigning its arrangements for storage of pharmaceuticals, relying to a greater extent on its own storage facilities as opposed to contracted facilities, CCSS estimates from April 2008 (when it introduced these arrangements) through December 2008 it was able to reduce storage costs by about C. 265 million (US$511,7216). The decrease was approximately 20 percent in December 2008. Finally, the Project financed a technical, legal and financial feasibility study of a new model of inventory control for CCSS and later the development and implementation of a bar code system, with the goal of more precise identification of the products that CCSS produces and purchases, in order to have better control of the institution’s physical inventory.
78. A Technical, Legal and Financial Feasibility Study for a New Model of Management for CCSS Pharmaceutical and Medical Supplies Inventory aimed to analyze and evaluate the policies, standards, criteria and variables that existed within CCSS; and to assess the efficiency of the theoretical and practical procedures used for the planning and programming of the pharmaceutical supply cycle. The study measured the impact of the pharmaceutical inventory purchased under the legal, financial and technical criteria established by the CCSS, its terms and conditions, and the entire process of the institution’s supply chain, both at the central and the local level. In addition, the study was designed to define operating financial, and other costs, as well as current centralized methods for procuring goods. Finally, the study developed a situational analysis on the status and condition of the infrastructure of the Central Warehouse, the Puntarenas Warehouse, pharmacy warehouses, suppliers for hospitals and health areas, and the infrastructure of warehouses of the production plants. The analysis was designed to establish their current capacity to meet their obligations: receiving, storage, control, rotation and distribution, among others. It would also determine the impact on the
6 Exchange rate of 2008: 517.86CRC = US$1 (accessed from http://www.gocurrency.com/v2/historic-exchange-rates.php?ccode2=USD&ccode=CRC&frMonth=5&frDay=2&frYear=2008 on June 2, 2010)

27
Central Store of receiving and storing raw materials from the production centers of the Directorate of Industrial Production and its other regular supplies.
Objective Indicator Achieved Indicators in the PAS
40% decrease of time between initial bid and delivery of pharmaceuticals
Achieved. Decreased by 50%
To improve efficiency in the acquisition and distribution of pharmaceuticals to health care providers and ultimately to patients
75% decrease of total pharmaceutical budget spent on warehouse storage costs
N/A
Other Indicators % pharmaceutical budget that is managed under the automated pharmacy system
Achieved. 2009:100%
Design and implementation of an information system for accounting and inventory control in CCSS
Achieved. System operating centrally and in all health centers
(e) Develop financial mechanisms that will improve the equitable distribution of resources, improve efficiency in the provider payment mechanisms and strengthen CCSS’ capacity to collect payroll contributions. 79. Progress towards the above objective was achieved, with some shortcomings, in the implementation of programmed activities. Equity, as defined by the indicator selected to measure progress, improved under the Project. The gap between the average per capita spending in the Brunca Region and the National Average was reduced from 46 percent in 2002 to 13.1 percent in 2009, an overall reduction of about 72 percent 80. The Project financed the purchase of software, as well as continued training for users on how to utilize the software to establish a system of 25 Diagnostic Related Groups. The information for the Diagnostic Related Groups that has been compiled is being used for decision making in regards to resource distribution and will be incorporated in the payment mechanisms for hospitals in the future. As explained in Section 2.2, the IMAS component was never implemented. As an alternative, CCSS opted to utilize and update an internal beneficiary registry, the Ficha Familiar, that contains extensive socio-economic information and information on usage of the health system for all beneficiaries in a given region. The Project financed the design of the Ficha Familiar system and the purchase of small laptops for surveyors, as well as a pilot survey in one region of the country. The information currently exists for other regions, but needs to be updated through household surveys and incorporated in the information system. Further efforts to expand the system will require additional staff, training, and computer equipment for surveyors. Costa Rica’s centralized collection system (Sistema Centralizado de Recaudación - SICERE) was consolidated and expanded, through training and through development of improved reporting methods (i.e., web-based) and other systems improvements. These efforts produced impressive results. From November 2007 to November 2008, collections increased by 68 percent among employers (number of employers) and 71 percent among workers (number of workers).
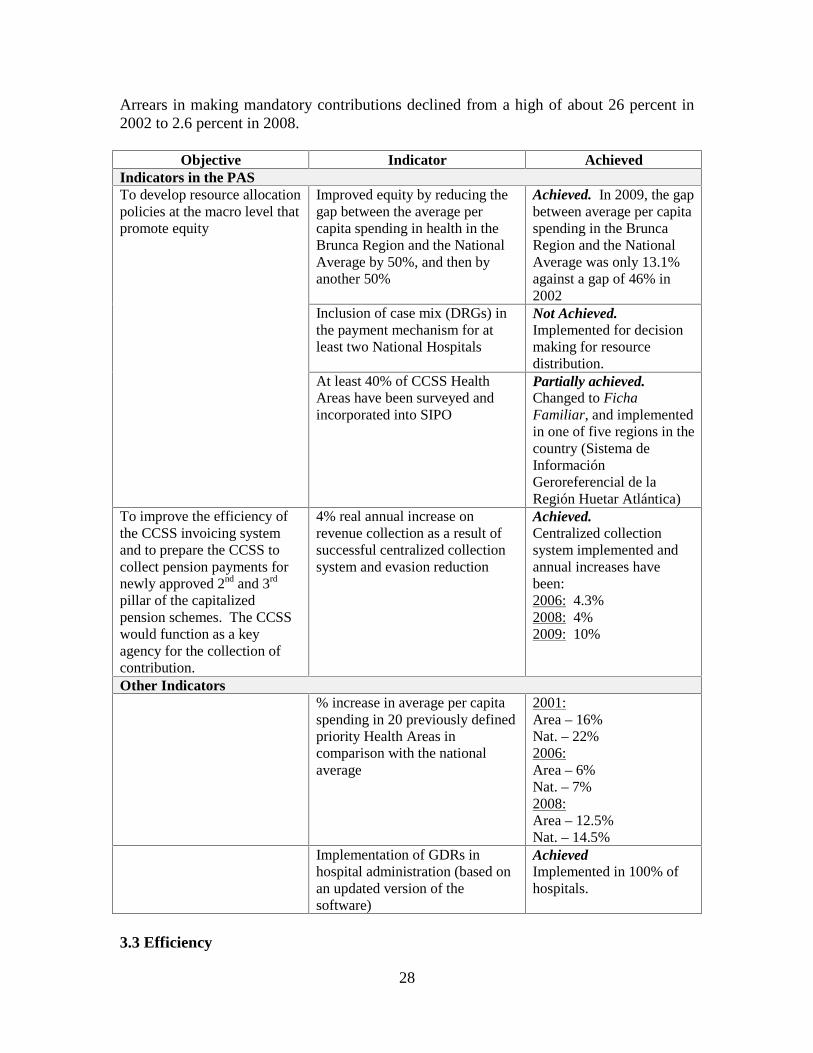
28
Arrears in making mandatory contributions declined from a high of about 26 percent in 2002 to 2.6 percent in 2008.
Objective Indicator Achieved Indicators in the PAS
Improved equity by reducing the gap between the average per capita spending in health in the Brunca Region and the National Average by 50%, and then by another 50%
Achieved. In 2009, the gap between average per capita spending in the Brunca Region and the National Average was only 13.1% against a gap of 46% in 2002
Inclusion of case mix (DRGs) in the payment mechanism for at least two National Hospitals
Not Achieved. Implemented for decision making for resource distribution.
To develop resource allocation policies at the macro level that promote equity
At least 40% of CCSS Health Areas have been surveyed and incorporated into SIPO
Partially achieved. Changed to Ficha Familiar, and implemented in one of five regions in the country (Sistema de Información Geroreferencial de la Región Huetar Atlántica)
To improve the efficiency of the CCSS invoicing system and to prepare the CCSS to collect pension payments for newly approved 2nd and 3rd pillar of the capitalized pension schemes. The CCSS would function as a key agency for the collection of contribution.
4% real annual increase on revenue collection as a result of successful centralized collection system and evasion reduction
Achieved. Centralized collection system implemented and annual increases have been: 2006: 4.3% 2008: 4% 2009: 10%
Other Indicators % increase in average per capita spending in 20 previously defined priority Health Areas in comparison with the national average
2001:Area – 16% Nat. – 22% 2006:Area – 6% Nat. – 7% 2008:Area – 12.5% Nat. – 14.5%
Implementation of GDRs in hospital administration (based on an updated version of the software)
Achieved Implemented in 100% of hospitals.
3.3 Efficiency

29
81. An ex-post economic analysis was not prepared. However, the Project’s impact on the overall efficiency of CCSS health services provision can be inferred from the assumptions in the Project’s economic analysis carried out during preparation. The analysis forecast that, at completion, the Project would produce substantial savings for the sector, primarily through reductions in hospitalization costs resulting from ambulatory surgery. Another area of savings (the economic analysis considered direct benefits only) was to be derived from improvements in the management of the pharmaceutical supply chain. The long and complex bidding process for pharmaceuticals that led to the need to keep excess inventory, which caused problems in the storage and distribution of drugs, was causing sizable losses to the CCSS. Finally, the Project was expected to lead to reductions in overhead from increasing decentralization, specifically administrative savings that would be produced by reorganization and improved management information systems in the MOH and CCSS. 82. At the time of Project completion, 40 percent of all hospital discharges in Costa Rica were the result of ambulatory surgeries, as opposed to a target of 20 percent upon which the Project’s ex-ante economic analysis had been based. Similarly, the entirety of the CCSS pharmaceutical budget is now managed under the integrated pharmaceutical information and distribution system, Sistema Integrado en Farmacia (SIFA), developed by the CCSS under the Project. In addition to these benefits, the time interval between bids and delivery of pharmaceuticals has been reduced by an average of about 50 percent. All pharmacies within the CCSS are connected to SIFA, which has resulted in improved inventory control, reduced wastage, and reduced waiting times for patients to have prescriptions filled as well as greater standardization across different levels of health centers.
3.4 Justification of Overall Outcome Rating Rating: Moderately Satisfactory 83. The Project’s Overall Outcome Rating is rated Moderately Satisfactory. This rating is based on the Project’s continued high relevance, the increased efficiency that it brought to the CCSS, and the progress toward achievement of its objectives, as presented in Section 3.2. On balance, the Project achieved most of its objectives with only minor shortcomings. There were significant shortcomings in the achievement of improving the equitable distribution of resources, or at least in the ability to substantiate this achievement. This issue undoubtedly in part resulted from cancellation of the activities that were to be implemented by IMAS, as well as the resulting late start of activities to update and expand the Ficha Familiar that would have been instrumental in providing the information required for achieving greater equity in resource allocation.
3.5 Overarching Themes, Other Outcomes and Impacts (a) Poverty Impacts, Gender Aspects, and Social Development

30
84. As mentioned above, it is difficult to measure the Project’s impact on poverty since the updating of the SIPO was never carried out, and the Ficha Familiar was only implemented on a pilot basis in three Health Areas (Talamanca, Alajuelita, y Puntarenas). The Project did have some direct impacts on indigenous groups, through implementation of a subproject which aimed to create a real-time mobile census of all families in an indigenous area. The census was designed to analyze 250 variables covering information on the health, economic, social, environment and cultural status of each family, which would allow improved decision making and better targeting of the real needs of indigenous communities. (b) Institutional Change/Strengthening 85. The Project was by and large and institutional development project that, despite the delays that it encountered, had an important role in strengthening the CCSS and MOH in several areas described in Section 3.2. The most important institutional development results include: (i) the separation of financing and service provision functions within a decentralized framework; (ii) the strengthening of the MOH regulatory capacity; (iii) strengthened capacity of CCSS for delivering health care services through decentralized networks, the purchasing of those services under performance contracts, and for planning and distributing pharmaceuticals; and (iv) the development and piloting of the Ficha Familiar in three health areas as the basis for improving regional equity through formula-based allocations based on population, risk-adjustment and poverty. (c) Other Unintended Outcomes and Impacts (positive or negative)
No applicable
3.6 Summary of Findings of Beneficiary Survey and/or Stakeholder Workshops No applicable
4. Assessment of Risk to Development Outcome Rating: Low to Negligible
86. The Risk to Development Outcome is considered Low to Negligible. The Project’s main contribution was in supporting the restructuring of the CCSS and MOH and developing institutional capacity to carry out their newly-defined functions under the health reform. CCSS’ Strategic Plan 2007-2012 sets out the institution’s policies, priorities, institutional plans and proposed investments that envisage the continued pursuit of the Project’s objectives. Similarly, the MOH’s current Strategic Plan reinforces the institution’s regulatory function within the overall framework of the Government’s vision of the health sector. The functional changes in the national health system count on strong support from across the political spectrum, and also from the beneficiaries who count on more equitable, quality health care since health service delivery is seen as a key pillar of Costa Rica’s public social services. Change is slow in Costa Rica, mostly because of the country’s strong democratic tradition that relies on a system of gradual consensus building and institutional accountability during any reform process. But these
31
very same issues that affected project implementation by causing multiple delays almost guarantee the long-term political and social sustainability of the Project’s outcomes. As the backbone of the country’s social insurance, CCSS counts on the necessary funding from workers’ and employers’ contributions to continue its pursuit of delivering high-quality, efficient and equitable health services to its beneficiaries.
5. Assessment of Bank and Borrower Performance
5.1 Bank Performance (a) Bank Performance in Ensuring Quality at Entry Rating: Moderately Satisfactory
87. Bank Performance in Ensuring Quality at Entry is rated Moderately Satisfactory based on the factors mentioned below.
88. Strategic Relevance. The strongest element of the Bank’s performance in ensuring quality at entry related to the Project’s strategic relevance, which was very high. The Project represented a continuation of support that the Bank had provided in an earlier operation and was the next logical step in the country’s health reform, a high priority for the Government. Project design incorporated lessons learned under the previous Bank-financed project, including findings and recommendation of technical studies and evaluations of the experience with the reform process on the primary health care model (EBAIS), the management contracts through the annual reports, an assessment of the pharmaceutical sector and policy options, a public expenditure review and patient satisfaction surveys. 89. State of Project Preparation. As mentioned in Sections 2.1 and 2.2, there were several aspects of preparation that, in retrospect, were not sufficiently advanced or completed at the time of approval/effectiveness. These aspects later affected the Project’s implementation. Although approval of external financing by Costa Rica’s Assembly normally involves a period of time after approval during which preparation could be advanced, it is not clear that even preliminary agreements had been reached on the content of what would be required. Thus, finalizing initial agreements and documents continued through the stages of early implementation. 90. Fiduciary Aspects. The Bank’s preparation team rightly addressed the possibility of issues with procurement that could affect implementation. Unfortunately, the solution that was pursued did little to resolve delays in procurement, and, furthermore, did not address the issue that delays were caused not only through the requirement of ex-ante approval by the Contraloria, but also through the requirement of ex-ante approval by the CCSS Junta Directiva for larger contracts.
91. Monitoring and Evaluation Arrangements. A very detailed monitoring and evaluation framework, supported by a detailed Policy Action Schedule, was in place at approval. As mentioned in Section 2.1, however, it is not clear why the Bank opted to

32
support the contracting out of the Project’s M&E, under a contract to be financed with loan funds. As the Project supported basically the strengthening of institutions capacity to deliver health services under the Government’s health reform, monitoring and evaluation of those institutions and the programs and activities that they financed should have been seen as an integral element in their institutional capacity strengthening. 92. Risk Assessment. As described in Section 2.1, the Project’s Risk Framework underestimated or did not make explicit several risks that emerged, although in retrospect since this was the follow-up to an operation that was rated Highly Satisfactory, these risks might have been difficult to envisage at the time of preparation. One of these risks includes the fact that, while the institutional capacity of the CCSS was rated satisfactory based on the rating of the previous HPR project, the Project was unable to foresee that additional internal supervision procedures put in place, which stemmed from corruption allegations made to the CCSS, exacerbated the already cumbersome procurement procedures, rendering the CCSS unable to perform at its potential capacity.
(b) Quality of Supervision Rating: Moderately Satisfactory
93. The Quality of Supervision is rated Moderately Satisfactory. Bank supervision can be separated in two phases: from approval through 2006 and then from 2006 until loan closing. 94. From Approval through 2006. The Bank’s supervision from approval, through an extended period until effectiveness was focused almost exclusively on getting the Project ready for implementation. In part because of the issues with the quality of preparation described above, early implementation had to address many tasks that should have been completed before project effectiveness. These include such issues as agreeing upon drafts of operations manuals, interagency agreements, procurement plans, other effectiveness conditions, etc. Because of this, during early implementation Bank supervision was unable to focus its supervision around development impact. In retrospect, the Project likely received less supervision inputs than would have been justified for a project that was facing such important implementation issues. At the same time, early supervision was slow to take action to downgrade project ratings, almost seeming to take the position that there was little that the Bank could do to contribute to resolving Costa Rica’s internal issues. During this period, Bank Supervision is rated Moderately Unsatisfactory. 95. From 2006 through Project Completion and Loan Closing. Supervision changed dramatically starting in 2007. This change was precipitated in part by the Project’s continued unsatisfactory implementation performance, the perception that unless implementation improved dramatically, the Project would not have a chance of meeting its development objectives and that project restructuring should be discussed as an option to improve performance. A detailed Action Plan was agreed with CCSS, and was updated with progress reports and submitted monthly to the Bank. Supervision became more intensive with focus on fiduciary aspects of the project and technical assistance, in

33
general more hands-on, and for the first time focused on development impact and monitoring progress towards the PAS and Action Matrix. The Bank provided support for procurement, through training and several special missions; although in the end it is not clear whether these actions had significant impact on shortening the delays in procurement actions. During this period, Bank Supervision is rated as Satisfactory. 96. Taking into consideration the Bank Supervision ratings for both periods as described above, and the fact that supervision during the final period was able to turn implementation around in an important manner, on balance Bank Supervision is rated Moderately Satisfactory.
(c) Justification of Rating for Overall Bank Performance Rating: Moderately Satisfactory
97. Overall Bank Performance is rated Moderately Satisfactory. This is based on a Moderately Satisfactory rating for Quality at Entry and an overall rating of Moderately Satisfactory for Supervision.
5.2 Borrower Performance (a) Government Performance Rating: Moderately Satisfactory
98. Government Performance is taken to mean the broader government, i.e., the Ministry of Finance (MOF) and other central government institutions. In this sense, Government Performance is rated Moderately Satisfactory. Throughout implementation, the Government demonstrated commitment to achieving the Project’s development objectives which also supported social outcomes that the Government has consistently prioritized in national policy. During preparation, the Government supported the CCSS objectives, and made significant efforts to structure a project that responded to these objectives. In spite of these positive efforts, the Project’s implementation was affected by several broader factors that were beyond the control of the implementing agencies, but that were generally well-understood at the time of preparation. Costa Rica’s internal democratic and fiduciary framework is well-established, with well-defined mandates and procedures. In many instances, these existing procedures influenced the pace and timing of key decisions with respect to project preparation and implementation, especially when Government’s procedures (e.g., procurement) were not fully compatible with those of the Bank. On the other hand, the cancellation of the loan resources allocated to IMAS was justified since it was not possible to reach consensus on formalizing an agreement to support implementation of the SIPO. 99. The allegations of corruption in the CCSS resulted in increased scrutiny not only on the activities of the implementing agency, but also in increased questioning of financing technical assistance and consultancy contracts with external borrowing. Despite its concerns regarding delays in implementation and efficient use of external borrowing, the MOF agreed not to request cancellation of loan funding. Beyond that, the Borrower provided an overall environment of stability, both institutional and otherwise,

34
and an established process of continuous consultation and involvement that bodes well for the sustainability of the Project’s accomplishments.
(b) Implementing Agency or Agencies Performance Rating: Moderately Satisfactory
100. Implementing Agencies’ Performance is taken to mean that of CCSS, and the MOH, the two agencies responsible for implementing project activities. 101. The CCSS continuously demonstrated commitment to the Project’s development objectives, which were fully congruent with its own objectives. As discussed in the section covering Bank Performance for Supervision above, however, it is relevant to disaggregate CCSS’ performance by phases, done below. 102. Project preparation flowed immediately from the final phases of the HRP’s implementation. The Project’s design and implementation arrangements also followed those of the HRP. When loan effectiveness was delayed, the CCSS continued implementing the logical next steps in their reform with internal resources, and began implementation of certain activities under the Project that were considered inherent to CCSS’ internal program. Unfortunately, the delays in implementation, coupled with the allegations against the CCSS’ former Executive President, and the HRP’s former Project Manager, had a noticeable impact on the pace with which all CCSS programs, including the Project, were implemented. With an internal investigation ongoing, CCSS planned activities slowed, as did any efforts to decentralize activities. The increased scrutiny invariably affected staffing decisions as well as individual staff’s disposition to make decisions that might later be challenged. During early implementation, CCSS’ performance would be rated Moderately Unsatisfactory. Although efforts towards the PAS continued, they did so at a very slow pace. 103. With new leadership starting in mid-2006, CCSS performance improved dramatically. The entire institution remained not only committed to the Project’s objectives, but also to improve its implementation and recover some of the time that had been lost during its first four years. One of the first decisions made by the institution’s leadership was to modify what had been the Project Coordinating Unit’s (PCU) reporting relationship. The PCU was moved to an operational directorate -- first the Directorate of Operations and then the Directorate of Infrastructure and Technology -- and was transformed into a Project Implementing Unit (PIU) that worked in coordination with other CCSS Directorates. An increased focus on the Project and its financing resulted in the appointment of highly qualified and experienced staff to the PIU. The new staff had the knowledge and authority necessary to make decisions, as well as a “can-do” attitude that put plans into action. During this phase, the PIU put into place an ambitious Action Plan which was supported the Bank with a stronger and more intense supervision. The PIU monitored the Action Plan regularly and followed up on compliance when necessary. As a result of these efforts, the Project succeeded in accomplishing in a little over two years what it had been unable to accomplish during the previous four or five. CCSS performance during this period would be rated Highly Satisfactory.

35
104. The MOH’s performance was more stable, albeit from the start it had a smaller, though no less important role in the country’s health reform. The MOH had also been perceived as having weaker implementation capacity than CCSS. However, the MOH was able to carry out most of the planned activities under the Project, and therefore the MOH is now in a stronger position to carry out its regulatory functions. Overall, its performance would be rated Moderately Satisfactory. 105. Overall, the Implementing Agencies’ performance is rated Moderately Satisfactory, in view of the serious problems during early implementation, that were in the end compensated for by a strong, reinvigorated effort towards the accomplishment of the Project’s objectives in the later years. (c) Justification of Rating for Overall Borrower Performance Rating: Moderately Satisfactory
106. Overall Borrower Performance is rated Moderately Satisfactory in view of similar ratings for both Borrower and Implementing Agencies’ Performance, as described above.
6. Lessons Learned 107. There are several Lessons Learned from the Project, with respect to its design and implementation experience, that are relevant not only to similar projects, but also to the design of projects in Costa Rica, or countries with similar environments. Project Design 108. Procurement. Procurement delays, due to complex processes, or lack of understanding of or incompatibility with Bank procurement procedures, are often cited as a cause of delays in project implementation. In the case of this Project, the possibility of issues with procurement had been identified up front, and actions expected to mitigate potential delays had been prepared. In spite of this, the Project as implemented involved a total of around 225 procurement processes, of which only three involved goods or services costing over the equivalent of US$1 million. While the Bank’s procurement guidelines and processes are efficiency-enhancing, and the Bank should continue to work with its clients to streamline their own internal processes and procedures (both in the context of the projects it finances and on a broader basis), it is possible to design projects that minimize potential procurement delays while supporting broader public sector objectives. For example, it should be possible to design an investment project for eventual Bank financing around the procurement of a small number of large contracts, for which bidding specifications and documents could be detailed during preparation, or that involves the financing of smaller, often called “non-procurable” items. 109. Effectiveness Delays. Effectiveness delays, taken here to mean delays of more than six months in loan effectiveness following approval, are increasingly commonplace in countries that require legislative approval of external financing. Although the Bank has recently sought to minimize the number of effectiveness conditions as a means of

36
ensuring timely project start-up, the reality is that there is often a long lag in effectiveness pending legislative approval. This fact should be considered in the project’s timetable as one in which selected activities could be finalized, thereby permitting earlier loan approval. Such a plan would require careful definition of what type of activity could be “left” to be completed during this “waiting” period. Obviously, any activity requiring up-front decision by the Government should be agreed in advance (e.g., in the case of the Project, the agreement with IMAS), with specific arrangements and details further elaborated after approval. Such an arrangement would also involve a change in how the Bank addresses supervision during a project’s early stages, shifting from waiting for a government to comply to having the Bank actively engaged in supporting compliance, similar to what is now done in the final phases of project preparation. 110. Monitoring and Evaluation. Monitoring and evaluation should be an integral part of project implementation. This is especially true in projects which focus on institutional capacity strengthening, in support of what in the case of the Project was a much broader government program. Monitoring should not be contracted out in most instances. If the institutional capacity for monitoring is appraised as being weak, project design should incorporate activities aimed at strengthening that capacity, which should be viewed in the context of being part and parcel of strengthening an institution’s overall project management and implementation capacity. Implementation 111. Reporting relationships of project units. The reporting relationship of a project unit can have an important impact on project implementation. Under the Project, the change in location of the PCU/PIU from the Office of the Executive President to an operating directorate in the institution had an important impact in improving the efficiency and pace of implementation. The change also resulted in a detailed Action Plan that played an important role in turning the Project around (in addition to other changes in the Project’s operating environment). In this case, the Office of the Executive President did not have capacity for project management or implementation, and the mere fact that the unit reported to the Executive President did not result in greater Government commitment to implementation. It is clear that in the case of the Project, the relocation of its implementation responsibilities to the CCSS departments responsible for project management, staffed with specialized managers and staff, resulted in a major improvement.
7. Comments on Issues Raised by Borrower/Implementing Agencies/Partners (a) Borrower/implementing agencies
(b) Cofinanciers Not Applicable (c) Other partners and stakeholders Not Applicable

37
Annex 1. Project Costs and Financing
(a) Project Cost by Component (in USD Million equivalent)
Components Appraisal Estimate (USD millions)
Actual/Latest Estimate (USD millions)
Percentage of Appraisal
POLICY DESIGN AND IMPLEMENTATION
20.75 15.00
MONITORING & EVALUATION & PROJECT MGMT.
2.75 2.00
Total Baseline Cost 0.00 17.00 Physical Contingencies 0.00 0.00 Price Contingencies 0.00 0.00 Total Project Costs 23.5 17.00 Front-end fee PPF 0.00 0.00
Front-end fee IBRD 0.00 0.00
Total Financing Required 23.5 17.00
(b) Financing
Source of Funds Type of Cofinancing
Appraisal Estimate
(USD millions)
Actual/Latest Estimate
(USD millions)
Percentage of Appraisal
Borrower 6.50 6.8 .00 International Bank for Reconstruction and Development 17.00 13.3 .00

38
Annex 2. Outputs by Component The following table outlines the activities by component during the Project. Activity Description Start Date
(D-M-Y) End Date (D-M-Y)
Amount (US$)
Component I – Policy Design and Implementation
1. Health Services Supply
1.1 Development of a methodology for the monitoring of EBAIS
30/09/2002 31/12/2002 $ 2,400.00
1.2 Epidemiologic diagnosis for adults 03/09/2003 03/04/2004 $ 40,000.00
1.3 PC03-22. Management of the quality improvement process at Dr. Moreno Cañas Clinic.
06/10/2003 06/12/2003 $ 15,000.00
1.4 Training in Pharma-Economics 13/10/2003 17/10/2003 $ 3,670.00
1.5 Training in Pharma-Economics 17/11/2003 21/11/2003 $ 4,727.00
1.6 Autoclave Table 28/11/2003 23/03/2004 $ 80,360.00
1.7 PC03-05. Improvement in the distribution of medical supplies and IV - Escalante Pradilla Hospital and EBAIS in the Area of Pérez Zeledón. PC03-09. Strengthening the current system of the warehousing and distribution of materials and supplies.
10/06/2004
08/07/2004
31/08/2004
10/04/2006
$ 31,249.00
$3,765.00
1.8 Technical Assistance for bid processes of Goods Subprojects
10/05/2004 09/11/2004 $ 7,666.00
1.9 Technical Assistance for the preparation of clinical guides
12/02/2004 11/01/2005 $ 15,980.00
1.10 Technical Assistance in Architecture for the Program of Sub-Projects
09/03/2004 16/04/2005 $ 15,960.00
1.11 PC03-14. Purchase of a dental ambulatory unit for the Buenos Aires Canton, Buenos Aires Health Area. PC03-15. Improvement of the processes of care for users, through the automation of resources in informatics. Health Area in Naranjo.
13/02/2004
05/03/2003
13/05/2005
19/07/2006
$8,285.00
$ 27,462.00
1.12 PC03-15 Improvement of the processes of health care to users, through the automation of resources in informatics. Health Area in Naranjo.
05/03/2003 19/07/2006 $ 5,900.00
1.13 Analysis of key processes and preparation of a proposal for improvement of the functioning of NHSRA.
19/05/2005 31/03/2006 $ 80,000.00

39
Activity Description Start Date (D-M-Y)
End Date (D-M-Y)
Amount (US$)
1.14 Training in in Pharma-Economics for professionals
07/06/2004 11/06/2004 $ 4,353.00
1.15 Ultrasound 10/06/2004 06/05/2005 $ 55,000.00
1.16 PC03-11 Program of instrumentation for cervical, spinal and dorso-lumbar spinal cord. Hospital Enrique Baltodano
10/06/2004 21/04/2005 $ 99,514.00
1.17 Training for Professionals in Pharmacy about Pharmaco-epidemiology
28/05/2005 12/10/2007 $ 4,588.23
1.18 PC03-14. Purchase of an ambulatory dental unit for the Buenos Aires Canton, Buenos Aires Health Area
18/02/2004 13/05/2005 $ 8,285.00
1.19 PC03-27. Improvement in performing ultrasound tests in the Los Santos Health Area. P03-28. Improvement in detecting gastric pathology through a bid for a gastroscope –Health Area in Los Santos
10/06/2004
10/06/2004
06/05/2005
12/09/2005
$55,000.00
$ 61,800.00
1.20 Technical Assistance for procurement of goods
01/01/2005 10/05/2005 $ 4,333.00
1.21 PC03-01. Program of ambulatory surgery - Dr. Solón Núñez Frutos Clinic.
07/03/2007 07/06/2007 $ 538.75
1.22 PC03-01. Program of ambulatory surgery in Dr. Solón Núñez Frutos Clinic.
07/03/2007 07/06/2007 $ 15,018.38
1.23 PC03-01. Program of ambulatory surgery in Dr. Solón Núñez Frutos Clinic.
10/06/2004 07/06/2007 $ 349.06
1.24 PC03-01. Program of ambulatory surgery in Dr. Solón Núñez Frutos Clinic.
10/06/2004 07/06/2007 $ 440.00
1.25 PC03-17. Initiating dental services in the EBAIS of Fray Casiano and San Luis. Health Area Chacarita. PC03-24. Equipment for the clinical laboratory, C.A.I.S. in Buenos Aires.
10/06/2004
10/06/2004
27/05/2005
07/07/2006
$ 5,147.00
1.26 PC03-17 – Opening dental services for the EBAIS in Fray Casiano and San Luis. Health Area Chacarita. PC03-24. Equipment for the clinical laboratory C.A.I.S. de Buenos Aires.
10/06/2004
10/06/2004
27/05/2005
07/07/2006
$ 270.00
1.27 PC03-17. Opening dental services for the EBAIS in Fray Casiano and San Luis. Health Area Chacarita. PC03-24. Equipment for the clinical laboratory C.A.I.S. de Buenos Aires
10/06/2004
10/06/2004
27/05/2005
07/07/2006
$ 932.00
1.28 PC03-17. Opening dental services for the EBAIS in EBAIS de Fray Casiano y San Luis. Health Area Chacarita.
10/06/2004
10/06/2004
27/05/2005
07/07/2006
$ 2,000.00

40
Activity Description Start Date (D-M-Y)
End Date (D-M-Y)
Amount (US$)
PC03-24. Equipment for the clinical laboratory C.A.I.S. de Buenos Aires
1.29 PC03-30. Improvement of case resolution capacity – Clinical Laboratory - Health Area Cariari. PC03-24. Equipment for the clinical laboratory C.A.I.S. de Buenos Aires.
22/12/2006 07/03/2007 $ 22,780.00
1.30 PC03-30. Improvement of case resolution capacity of the Clinical Laboratory - Health Area Cariari. PC03-24. Equipment for the clinical laboratory C.A.I.S. de Buenos Aires.
10/062004
10/06/2004
05/10/2007
07/04/2006
$ 32,875.00
1.31 PC03-30. Improvement of the resolution capacity of Clinical Laboratory- Health Area in Cariari. PC03-24. Equipment for the clinical laboratory C.A.I.S. in Buenos Aires.
10/062004
10/06/2004
05/10/2007
07/04/2006
$ 1,800.00
1.32 PC03-12. Strengthening of the ambulatory surgery program, Hospital of Guapiles.
15/04/2005 30/07/2005 $ 13,667.00
1.33 PC03-21. Remodeling of bathrooms in Sala No 1 and No 2 - National Rehabilitation Center
04/05/2005 15/08/2005 $ 23,750.00
1.34 PC03-09. Strengthening the current system of storing and distributing supplies and materials. Health Area of Cariari. PC03-30. Improvement of the case resolution capacity - Clinical Laboratory - Health Area of Cariari.
24/10/2005 28/02/2006 $ 212,949.70
1.35 Technical Assistance in architecture for the Project Programs.
17/04/2005 10/04/2006 $ 14,040.00
1.36 Technical Assistance in fundamentals and methodological principals EFQM
29/07/2005 29/11/2005 $ 9,800.00
1.37 Technical Assistance for purchase of goods 11/05/2005 10/05/2006 $ 12,000.00
1.38 Technical Assistance for the execution of subprojects.
10/06/2005 09/06/2006 $ 18,000.00
1.39 PC03-02. Initiation of mammogram imaging in Dr. Solón Núñez Frutos Clinic. PC03-07. Design of bathroom area in Medicine and Surgery for both men and women. PC03-08. Remodeling of the Pharmacy, Hospital William Allen. PC03-26. Remodeling of sampling area in Clinical Laboratory William Allen.
28/11/2005 30/03/2006 $ 26,720.00

41
Activity Description Start Date (D-M-Y)
End Date (D-M-Y)
Amount (US$)
1.40 Design for expanding services for mammogram imaging in Solón Núñez Clinic
28/11/2005 30/03/2006 $ 4,950.00
1.41 Projector for Liberia Hospital 08/10/2004 08/12/2005 $ 1,450.00
1.42 PC03-16. Automation of Pharmacy services (Implementation of SIFA). Health Area Chacarita.
12/03/2007 31/07/2007 $ 2,890.00
1.43 PC03-16. Automation of Pharmacy services (Implementation of SIFA). Health Area Chacarita.
12/03/2007 31/07/2007 $ 6,480.00
1.45 PC03-12. Strengthening the ambulatory surgery program, Hospital of Guápiles.
28/02/2006 16/03/2006 $ 6,500.00
1.46 Technical Assistance for strengthening and development of ambulatory surgery
02/06/2006 02/01/2007 $ 25,000.00
1.47 PC03-08. Remodeling of Pharmacy in William Allen Hospital. PC03-09. Strengthening the current system of storing and distributing supplies and materials. Health Area of Cariari. PC03-15. Improvement of processes of Primary Health Care for users through the automation of informatics resources. Health Area of Naranjo. PC03-16. Automation of Pharmacy services (Implementation of SIFA). Health Area of Chacarita. PC03-17. Initiation of dental services in the EBAIS of Fray Casiano and San Luis. Health Area Chacarita. PC03-18. Modernization of computer equipment at the Pharmacy (Implementation of SIFA). Hospital Max Peralta de Cartago. PC03-19. Implementation of system to make appointments in Dr. Enrique Baltodano Briceño Hospital. PC03-19. PC03-20. Automation of the pharmacy services in the Health Area of Esparza. PC04-12. Implementation of Automated Pharmacy System at San Vicente de Paul Hospital.
12/03/2007 31/07/2007 $ 136,245.00
1.48 PC03-08 Remodeling of Pharmacy at the William Allen Hospital. PC03-09. Strengthening and distribution of materials and supplies. Health Area of
12/03/2007 31/07/2007 $ 7,580.00

42
Activity Description Start Date (D-M-Y)
End Date (D-M-Y)
Amount (US$)
Cariari. PC03-15. Improvement of the processes of Primary Health Care, through the automation of services in informatics. Health Area of Naranjo. PC03-16 Automation of Pharmacy services (Implementation of SIFA). Health Area Chacarita. PC03-17. Initiation of dental services in the EBAIS of Fray Casiano and San Luis. Health Area Chacarita. PC03-18. Update and modernization of computer equipment in pharmacy services (Implementation of SIFA). Hospital Max Peralta de Cartago. PC03-19. Implementation of the automated appointment system in the Dr. Enrique Baltodano Briceño Hospital. PC03-20. Automation of the pharmacy in Esparza Health Area. San Vicente de Paul.
1.49 Pharmacy Integrated System. PC04-12 Implementation of the Pharmacy Automated System San Vicente de Paul Hospital.
12/03/2007 31/07/2007 $ 109,145.00
1.50 PC03-02. Opening of mammogram imaging services in Dr. Solón Núñez Frutos Clinic. PC03-04. Opening of a diagnosis center for breast pathology in San Carlos Hospital. PC03-06. Quality Improvement of MRI diagnosis for hospitalized patients at Dr. Escalante Pradilla Hospital.
10/06/2004
05/05/2003
09/10/2006
10/08/2006
$82,200.00
$ 79,400.00
1.51 Purchase of a Holter System Device 16/07/2004 $ 15,195.83
1.52 Design of plans and inspection for minor civil works – Dental and Social Work. Clorito Picado Clinic.
18/05/2006 16/08/2006 $ 13,162.50
1.53 TR05-05. Strengthening of Administrative management through improvement of inventory management and strengthening of the maintenance management. Coronado Area. TR05-06. Strengthening of the delivery of medical supplies. Improvement of the conditions for environmental management. Health Area in Coronado. TR05-16. Strengthening of ambulatory solutions through the strategy of group health care and training. Coronado Clinic.
07/08/2006 30/09/2008 $ 99,377.00

43
Activity Description Start Date (D-M-Y)
End Date (D-M-Y)
Amount (US$)
1.54 PC04-03. Strengthening of surgical major services, Enrique Baltodano Hospital (Ophthalmological).
13/01/2006 06/01/2006 $ 79,000.00
1.55 Strengthening of ambulatory services, HCG. 02/01/2007 30/09/2008 $ 76,690.00
1.56 Design for remodeling Pharmacy services at San Juan de Dios Hospital.
30/10/2006 30/09/2008 $ 31,500.00
1.57 TR05-11. Strengthening of ambulatory services, Dr. Rafael A. Calderón Guardia Hospital.
22/01/2007 30/09/2008 $ 60,000.00
1.58 TR05-09. Ambulatory program for heart rehabilitation at the Hospital Dr. Rafael A. Calderón Guardia
08/01/2007 30/09/2008 $ 64,000.00
1.59 PC03-24. Equipment for the clinical laboratory C.A.I.S. de Buenos Aires.
10/06/2004 07/07/2006 $ 11,100.00
1.60 PC04-10. External and internal signage for the National Psychiatric Hospital
18/01/2007 10/07/2007 $ 11,247.62
1.61 PC03-24. Equipment for the clinical laboratory C.A.I.S. de Buenos Aires.
10/06/2004 07/07/2006 $ 11,600.00
1.62 UVA 07/03/2007 07/05/2007 $ 12,500.00
1.63 UVA 07/03/2007 07/05/2007 $ 9,000.00
1.64 TR05-02. Administrative system for medical records
13/02/2007 30/04/2007 $ 43,999.77
1.65 TR05-11. Strengthening of ambulatory services, Dr. Rafael A. Calderon Guardia Hospital. TR05-13. Strengthening of ambulatory services through the construction of a national ambulatory service model at Mexico Hospital. Preparation of basic studies for the design of plans and inspection, expansion and remodeling of Emergency Services. Cl. Clorito Picado Hospital.
22/03/2007 30/11/2007 $ 125,000.00
1.66 Supply and installation of transformers. Cl. Cubujuquí, Heredia
09/05/2007 09/09/2007 $ 115,000.00
1.67 PC04-04. Strengthening of the transportation area in Buenos Aires, Second round (Deconcentration). TR05-10. Program for domiciliary care for oxygen-dependant patients. Dr. Rafael A. Calderon Guardia Hospital. TR05-11. Strengthening of ambulatory services. Dr. Rafael A. Calderon Guardia Hospital.
13/01/06
13/01/2006
13/01/2006
24/12/2007
13/12/2007
14/07/2007
$ 22,500.00

44
Activity Description Start Date (D-M-Y)
End Date (D-M-Y)
Amount (US$)
TR05-12 Program for domiciliary primary health care for children with respiratory dysfunction. Metropolitan Area of the National Children’s Hospital
1.68 Design of plans, permits and inspections. Goicoechea Health Area.
19/03/2007 30/09/2008 $ 19,750,00
1.69 TR05-14. Strengthening of ambulatory services with specialized equipment to diminish long waiting lists for surgery. San Carlos Hospital
02/06/2007 17/07/2007 $ 75,400.00
1.70 Expansion of Surgery Area. Golfito Hospital. 03/07/2007 15/02/2008 $ 191,191.94
1.71 Technical assistance for training and use of medicines, investment strategy for Prescription Quality Improvement.
28/05/2007 12/10/2007 $ 14,502.00
1.72 PC04-12. Implementation of automated pharmacy system. San Vicente de Paul Hospital. TR05-17. Strengthening of the surgery program of Golfito Hospital and support to service network.
13/06/2007 24/08/2007 $ 96,232.57
1.73 Vehicles: 02/06/2007 17/09/2007 $ 67,500.00
1.74 Purchase of equipment for the local level. TR05-11 Strengthening of the ambulatory service area, Dr. Rafael A. Calderón Guardia Hospital
30/08/2007 26/11/2007 $ 92,560.00
1.75 Purchase of equipment for the local level. TR05-11. Strengthening of ambulatory services, Dr. Rafael A. Calderón Guardia Hospital
30/08/2007 26/11/2007 $ 138,460.00
1.76 Purchase of equipment for the Local level: solar refrigerators.
06/06/2007 05/10/2007 $ 112,430.00
1.77 TR05-03. Strengthening and improvement of dental services of first and second level of Primary Health Care and Social Work. Clorito Picado Clinic.
11/09/2007 20/02/2008 $ 192,091.16
1.78 Endobronchial Ultrasound for the México Hospital
15/09/2007 01/11/2007 $ 122,600.00
1.79 PC04-01. Implementation of laparoscopic surgery, Hospital William Allen Second round. (ambulatory solutions). TR05-14. Strengthening of the ambulatory service equipment, specialized to diminish long waiting lists. San Carlos Hospital. TR05-15 14 Strengthening of ambulatory
13/01/2006
13/01/2006
13/01/2006
18/12/2007
19/12/2007
19/12/2007
$ 435,494.08

45
Activity Description Start Date (D-M-Y)
End Date (D-M-Y)
Amount (US$)
services via strategy of group attention and training. Coronado Clinic. TR05-18. Strengthening of ambulatory services network. Runca Region, Escalante Pradilla Hospital. TR05-19. Strengthening of the Ambulatory Laparoscopic Surgery, México Hospital. Strengthening of ambulatory services. HCG
13/01/2006
13/01/2006
19/12/2007
19/12/2007
1.81 PC03-08. Remodeling of the pharmacy, Hospital William Allen. TR05-0.7 Opening of the Dental Services and increase of coverage and quality in primary health care in Ipís and Zetillal., Health Area of Coronado
13/01/2006
26/01/2006
03/04/2008
30/01/2008
$ 74,250.00
1.82 Argon Plasma 16/10/2007 14/03/2008 $ 84,440.00
1.83 TR05-12. Program for in-house assistance for children with respiratory problems. National Children Hospital.
15/11/2007 30/06/2009 $ 19,584.00
1.84 Remodeling and inspection of rooms for hospitalized patients. William Allem Hospital
18/02/2008 30/08/2008 $ 363,000.00
1.85 TR05-23. Strengthening of the Emergency Service Network. Dr. Marcial Fallas Clinic
29/04/2008 30/08/2008 $ 313,858.00
1.86 Construction and inspection of EBAIS. Mata de Plátano
27/03/2008 27/08/2008 $ 554,554.00
1.87 PC04-08. Improvement of management and patient care during external consultation through implementation of services in the CENARE.
31/07/2007 20/10/2007 $ 73,465.00
1.88 TR05-11. Strengthening of ambulatory emergency services, Dr. Rafael A. Calderón Guardia Hospital. TR05-14. Strengthening of ambulatory services with equipment specialized to diminish long waiting lists for surgery in San Carlos Hospital. TR05-18. Strengthening of ambulatory services, Region Brunca, Escalante Pradilla Area.
13/01/2006
13/01/2006
13/01/2006
13/12/2007
19/12/2007
196/12/2007
$ 75,696.00
1.89 TR05-11. Strengthening of ambulatory services at Dr. Rafael A. Calderon Guardia Hospital. TR05-14. Strengthening of emergency services with specialized equipment to reduce long waiting lists for surgery. San Carlos
13/01/2006
13/01/2006
13/01/2006
13/12/2007
19/12/2007
196/12/2007
$ 5,693.00

46
Activity Description Start Date (D-M-Y)
End Date (D-M-Y)
Amount (US$)
Hospital. TR05-18. Strengthening of ambulatory services, Brunca, Escalante Pradilla
1.90 Supply of Dental Unit – Primary Health Care 20/06/2008 30/09/2008 $ 641,466.00
1.91 Supply of Dental Units- Primary Health Care (Dental Rays X )
22/02/2007 24/12/2007 $ 74,403.00
1.92 Information system for the support of decision-making - Huetar Atlántica Region
05/09/2008 30/11/2008 $ 38,100.00
1.93 Licences ARC-VIEW 9.2 for the Geographic Information System for the Huetar Atlántica Region.
05/09/2008 30/11/2008 $ 61,900.00
1.94 Ultrasound - Endobronchial for the Dr. Calderón Guardia Hospital
03/09/2008 24/11/2008 $ 147,840.00
1.95 Technical assistance for the economic feasibility study to increase coverage of the technological services used for videoconferencing
03/11/2008 03/12/2008 $ 17,500.00
1.96 Technical assistance for the national oncology network in the development and operations of network services in cancer.
02/02/2009 02/11/2009 $ 3,300.00
1.97 Cardiology and peripheral Vascular. San Juan de Dios. Hospital Angiograph
28/02/2009 30/07/2009 $ 1,231,036.00
1.98 Pulmonary ventilators and O.N monitor 19/06/2009 30/08/2009 $ 100,000.00
1.99 Purchase of ultrasound for gyno-obstetric services in HSJD
19/06/2009 30/08/2009 $ 109,500.00
1.100 Purchase of hysteroscopy for gyno-obstetric services in H S.J.D
08/06/2009 30/07/2009 $ 116,000.00
1.101 Autoclaves for the Health Area in Santo Domingo Heredia
30/05/2009 30/07/2009 $ 63,485.00
1.103 All-terrain vehicle for the Huetar Atlántica Region
26/06/2009 30/08/2009 $ 23,200.00
1.104 Purchase of Electrocautery Equipment with Argon Plasma (Scalpel)
19/06/2009 14/08/2009 $ 53,000.00
1.105 Non-Mydriatic Retinal Camera 12/06/2009 30/07/2009 $ 77,550.00
1.106 Pulmonary ventilators for adults 19/06/2009 30/07/2009 $ 377,671.10
1.107 Purchase of vital signs monitors 12/06/2009 30/07/2009 $ 100,000.00
1.108 Ambulance Boat (Huetar Atlántica Region) 19/06/2009 14/08/2009 $ 60,646.00
1.109 Computer equipment for the Ministry of Health
13/04/2009 30/07/2009 $ 10,585.00
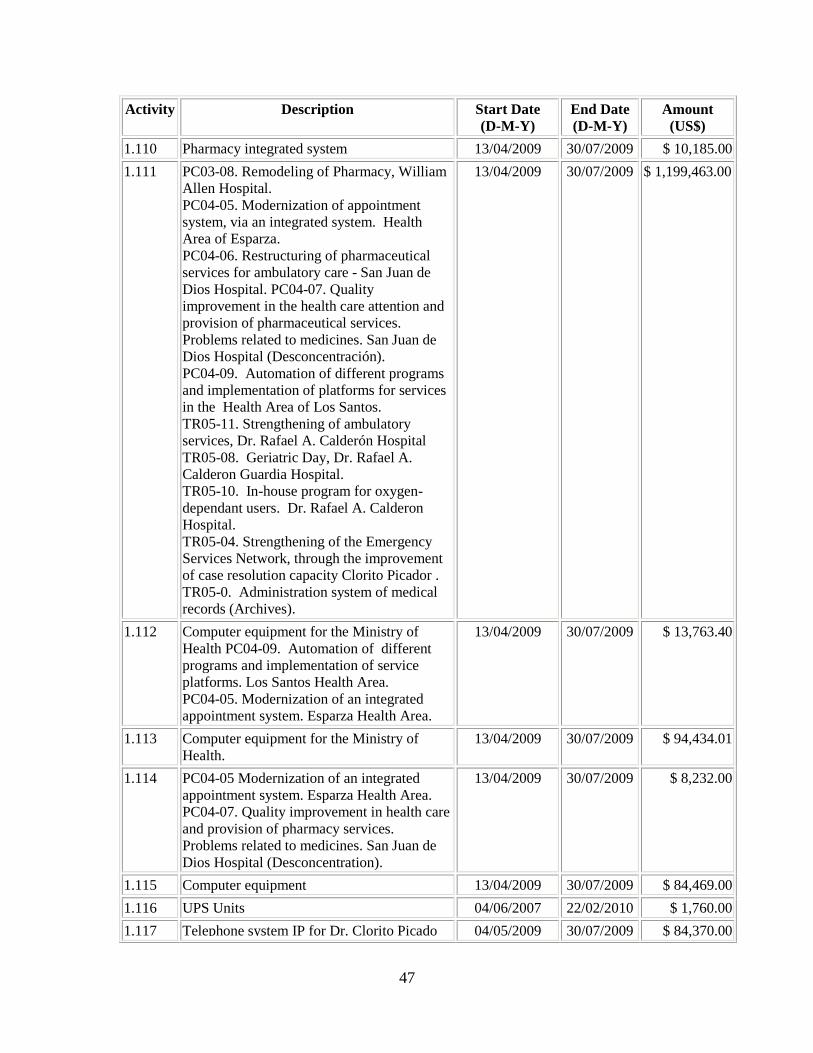
47
Activity Description Start Date (D-M-Y)
End Date (D-M-Y)
Amount (US$)
1.110 Pharmacy integrated system 13/04/2009 30/07/2009 $ 10,185.00
1.111 PC03-08. Remodeling of Pharmacy, William Allen Hospital. PC04-05. Modernization of appointment system, via an integrated system. Health Area of Esparza. PC04-06. Restructuring of pharmaceutical services for ambulatory care - San Juan de Dios Hospital. PC04-07. Quality improvement in the health care attention and provision of pharmaceutical services. Problems related to medicines. San Juan de Dios Hospital (Desconcentración). PC04-09. Automation of different programs and implementation of platforms for services in the Health Area of Los Santos. TR05-11. Strengthening of ambulatory services, Dr. Rafael A. Calderón Hospital TR05-08. Geriatric Day, Dr. Rafael A. Calderon Guardia Hospital. TR05-10. In-house program for oxygen-dependant users. Dr. Rafael A. Calderon Hospital. TR05-04. Strengthening of the Emergency Services Network, through the improvement of case resolution capacity Clorito Picador . TR05-0. Administration system of medical records (Archives).
13/04/2009 30/07/2009 $ 1,199,463.00
1.112 Computer equipment for the Ministry of Health PC04-09. Automation of different programs and implementation of service platforms. Los Santos Health Area. PC04-05. Modernization of an integrated appointment system. Esparza Health Area.
13/04/2009 30/07/2009 $ 13,763.40
1.113 Computer equipment for the Ministry of Health.
13/04/2009 30/07/2009 $ 94,434.01
1.114 PC04-05 Modernization of an integrated appointment system. Esparza Health Area. PC04-07. Quality improvement in health care and provision of pharmacy services. Problems related to medicines. San Juan de Dios Hospital (Desconcentration).
13/04/2009 30/07/2009 $ 8,232.00
1.115 Computer equipment 13/04/2009 30/07/2009 $ 84,469.00
1.116 UPS Units 04/06/2007 22/02/2010 $ 1,760.00
1.117 Telephone system IP for Dr. Clorito Picado 04/05/2009 30/07/2009 $ 84,370.00

48
Activity Description Start Date (D-M-Y)
End Date (D-M-Y)
Amount (US$)
Clinic.
1.118 Oxygen tanks (liquid) HCG;HNN 04/04/2007 14/06/2007$ 56,712.50
1.119 TR05-10. In-house care services for oxygen- dependant patients - Dr. Rafael A. Calderon Guardia Hospital. TR05-12. Program for the integrated in-house pediatric care children with respiratory problems. National Children’s Hospital. TR05-18. Strengthening of ambulatory services, Brunca Region. Escalante Pradilla.
30/05/2007 31/07/2007 $ 4,985.00
1.120 TR05-10. In-house care services for oxygen- dependant patients. Dr. Rafael A. Calderón Guardia Hospital. TR05-12. National Children’s Hospital TR05-18. Strengthening of ambulatory care services. Brunca Region, Escalante Pradilla Hospital.
30/05/2007 31/07/2007 $ 15,240.00
1.121 TR05-10. In-house care services for oxygen- dependant patients. Dr. Rafael A. Calderón Guardia Hospital. TR05-12. Program for in-house care for children with respiratory problems. National Children’s Hospital. TR05-18. Strengthening of ambulatory services in the Brunca Region. Escalante Pradilla.
30/05/2007 31/07/2007 $ 11,240.00
1.122 TR05-10. In-house care services for oxygen- dependant patients. Dr. Rafael A. Calderón Guardia Hospital. TR05-12. Program for in-house care for children with respiratory problems in the metropolitan area. National Children’s Hospital. TR05-18. Strengthening ambulatory care services. Escalante Pradilla.
30/05/2007 31/07/2007 $ 2,500.00
1.123 TR05-10. Dr. Rafael A. Calderón Guardia Hospital. TR05-12 In-house care services for oxygen dependant patients - Dr. Rafael A. Calderon Guardia Hospital TR05-18. Strengthening of ambulatory care services. Brunca, Escalante Pradilla.
30/05/2007 31/07/2007 $ 8,900.00
1.124 TR05-10. Dr. Rafael A. Calderón Guardia Hospital.
30/05/2007 31/07/2007 $ 7,500.00

49
Activity Description Start Date (D-M-Y)
End Date (D-M-Y)
Amount (US$)
TR05-12. In-house care services for oxygen-dependant patients. Dr. Rafael A. Calderón Guardia Hospital, National Children’s Hospital. TR05-18. Strengthening of network services, Escalante Pradilla
1.125 TR05-10. Dr. Rafael A. Calderón Guardia Hospital. TR05-12. National Children’s Hospital. TR05-18. Strengthening of ambulatory services Program. Brunca Region, Escalante Pradilla
30/05/2007 31/07/2007 $ 9,035.96
1.126 Non-Mydriatic Retinal Camera 30/01/2008 03/03/2008 $ 29,380.00
1.127 Air conditioning for the Ministry of Health 17/09/2007 27/11/2007 $ 5,880.00
1.128 TR05-12 Program for an in-house integrated health care for children with respiratory problems. Metropolitan Area. Children’s Hospital. TR05-13. Strengthening of ambulatory services through the construction of a national ambulatory service at the México Hospital.
09/03/2009 30/06/2009 $ 187,207.19
1.129 Purchase of laparoscopic tower for the Blanco C Hospital.
12/06/2009 30/07/2009 $ 100,000.00
Component I – Implementation and Policy Design
1. Financing and Reallocation of resources
1.1 Professor in Health Economics (Graduate level )
28/10/2002 01/11/2002 $ 5,232.25
1.2 Professor in Health Economics 21/10/2002 26/10/2002 $ 5,232.25
1.3 Professor in Health Economics 25/11/2002 29/11/2002 $ 5,232.25
1.4 Professor in Health Economics 14/01/2003 18/01/2003 $ 5,232.25
1.5 Professor in Health Economics 08/03/2004 12/03/2004 $ 4,852.91
1.6 Professor in Health Economics 10/05/2004 14/05/2004 $ 5,226.37
1.7 Professor in Health Economics 12/07/2004 16/07/2004 $ 5,232.25
1.8 Professor in Health Economics 19/07/2004 23/07/2004 $ 5,040.25
1.9 Professor in Health Economics 26/07/2004 30/07/2004 $ 5,232.25
1.10 Feasibility study. Technical, legal and financial. New Administration Model for inventory of medical supplies at the CCSS
30/05/2005 03/11/2005 $ 114,705.32
1.11 Professor in Health Economics 30/08/2004 03/09/2004 $ 5,232.25
1.12 Professor in Health Economics 11/10/2004 15/10/2004 $ 5,232.25

50
Activity Description Start Date (D-M-Y)
End Date (D-M-Y)
Amount (US$)
1.13 Professor in Health Economics 25/10/2004 29/10/2004$ 5,232.25
1.14 Professor in Health Economics 08/11/2004 12/11/2004$ 5,232.25
1.15 Professor in Health Economics 06/12/2004 10/12/2004$ 5,232.25
1.16 Professor in Health Economics 20/07/2005 20/03/2006$ 150,000.00
1.17 Purchase of Software licenses for Hospital Administration. AP-GDR
10/05/2006 19/06/2008 $ 514,348.00
Component I – Policy Design and Implementation
1. Strengthening of the Ministry of Health
1.1 Technical Assistance for Formalizing the Archives System – MS
12/05/2004 12/12/2004 $ 2,637.36
1.2 Technical Assistance for the Communications Plan at Ministry of Health
20/02/2006 20/06/2006 $ 16,000.00
1.3 Technical Assistance for analysis of the needs to elaborate TDRs for information systems at the Ministry of Health
08/02/2006 10/05/2006 $ 30,926.00
1.4 PC03-08. Remodeling of the Pharmacy, Hospital William Allen. PC03-09. Strengthening of the current system for storing and distribution of supplies and materials. Cariari Health Area PC03-15. Improvement of health care services to users, via the automation of IT resources. Health Area of Naranjo. PC03-16. Automation of the pharmacy services (Implementation of SIFA). Health Area Chacarita. PC03-17. Initiation of dental services in the EBAIS of Fray Casiano.
13/01/2006
08/07/2004
March 2003
10/06/200410/06/2004
03/04/2008
April 2006
19/07/2006
19/07/2006 27/05/2005
$ 90,558.01
1.5 PC03-08. Remodeling of the Pharmacy, William Allen Hospital. PC03-09. Strengthening the current system of storing and distributing supplies and materials, Health Area of Cariari. PC03-15. Improvement of the processes of care to users, through the automation of computing resources. Health Area of Naranjo. PC03-16. Automation of pharmacy services (Implementation of SIFA). Health Area of Chacarita. PC03-17. Initiation of dental services in the EBAIS of Fray Casiano and San Luis. Health Area of Chacarita. PC03-18. Updating and modernization of
13/01/2006
08/07/2004
05/03/2003
10/06/2004
10/06/2004
10/06/2004
10/06/2004
03/04/2008
22/02/2010
19/07/2006
19/07/2006
27/05/2005
19/07/2006
19/07/2006
$ 187,915.00

51
Activity Description Start Date (D-M-Y)
End Date (D-M-Y)
Amount (US$)
computer equipment in the pharmacy service (Implementation of SIFA). Max Peralta Hospital of Cartago. PC03-19. Implementation of automated appointments system at the Hospital Dr. Enrique Baltodano Briceño. PC03-20. Automation of the pharmacy services of the Health Area of Esparza. PC04-12. Implementation of Pharmacy Automated System of Hospital San Vicente de Paul.
10/06/200410/06/200413/01/2006
19/07/2006 19/07/2006 22/02/2010
1.6 Technical Assistance, accreditation development process.
13/12/2007 13/12/2009 $ 355,151.00
1.7 Senior Management Program for the Ministry of Health
30/11/2006 30/03/2007 $ 85,000.00
1.8 Master of Environmental Law 17/06/2006 09/02/2008 $ 29,000.00
1.9 Strengthen the regulatory framework for Qualification Norms of Type A Health Facilities in the MOH
26/09/2008 31/07/2009 $ 68,688.00
1.10 Project Management Program 19/06/2009 16/10/2009 $ 43,800.00
1.11 MS Computer Equipment 15/05/2009 22/06/2009 $ 56,400.00
1.12 Update software licenses and technical support for Oracle database MS
16/10/2009 06/11/2009 $ 41,331.80
Component I – Policy Design and Implementation
1. Regulation and Institutional Strengthening
1.1 System Reform Technical Assistance for Disability, Old Age and Death and FRE
02/12/2002 01/12/2003 $ 26,400.00
1.2 Exhibition "Current Trends in Public Hospital Management and Strategic Areas”
08/08/2003 08/08/2003 $ 1,500.00
1.3 Integral Assessment of the effectiveness of instruments applied in the process of deconcenration and alignment of Medical Management
27/08/2003 27/08/2004 $ 2,000.00
1.4 Strategic Planning Liaison between Executive Presidency and PFMSS
23/08/2004 22/02/2005 $ 15,000.00
1.5 Liaison officer for Strategic Planning between the Executive Presidency and PFMSS
17/03/2005 16/09/2005 $ 51,000.00
1.6 Technical Assistance for Management Group
22/08/2005 22/02/2006 $ 15,700.00

52
Activity Description Start Date (D-M-Y)
End Date (D-M-Y)
Amount (US$)
1.7 Technical Assistance from a specialist in network optimization
06/04/2008 10/10/2006 $ 14,400.00
1.8 Technical Assistance Executive Presidency Priority Action Items
07/08/207 16/06/2008 $ 9,000.00
1.9 Consulting to model the business model of Accounting and Inventory Control; the analysis, design, construction and Implementation of Information System and its interfaces with others
17/03/2007 17/03/2008 $ 395,416.14
1.10 Technical Assistance to coordinate the preparation of a feasibility study on the reasonableness of outsourcing services for comprehensive health care
19/03/2007 23/10/2007 $ 25,000.00
1.11 Training Program: Modern Management and Change Management of Health
01/08/2007 30/06/2008 $ 183,657.00
1.12 Technical Assistance: Development of Implementation Plan Priority Action Lines
07/08/2007 16/06/2008 $ 27,000.00
1.13 Development of a module of the Integrated Health Information (SIFF)
30/06/2008 23/01//2009 $ 361,020.00
1.14 Extension for SIFF automation 18/05/2009 06/11/2009 $ 114,000.00
1.15 Purchase of telemedicine equipment for tele-health program
28/02/2009 31/08/2009 $ 531,242.46
1.16 Purchase of telemedicine equipment for the tele-health program
28/02/2009 31/08/2009 $ 427,681.58
1.17 Technical Assistance to establish correlation between the health and the demographic profiles of the population covered by networks and sub-networks
13/04/2009 13/07/2009 $ 17,500.00
1.18 Technical Assistance for institutional network design, unified communication training in health care management
09/06/2009 09/11/2009 $ 46,500.00
1.19 Training in health care management 14/07/200914/10/2009 $ 35,000.00
1.20 Organizational structure Implementation of comprehensive care
17/07/2009 17/11/2009 $ 40,000.00
1.21 Advanced management training in health services for Directors of Metropolitan Hospitals and Clinics
03/08/2009 03/11/2009 $ 223,500.00

53
Activity Description Start Date (D-M-Y)
End Date (D-M-Y)
Amount (US$)
Component II - Monitoring and Evaluation and Project Management
2 Administrative Financial Management
2.1 External Audit for implementation up to 12/31/2002 and Addendum for 12/31/2003.
17/05/2002 31/12/2002 $ 12,000.00
2.2 Communication Link in Executive Presidency
13/05/2002 13/11/2002 $ 18,000.00
2.3 Technical Assistance in the Area of Informatics -Office of the President CCSS
13/05/2002 13/11/2002 $ 9,000.00
2.4 Deconcentration Strategic Area Coordinator
01/09/2002 01/09/2003 $ 36,000.00
2.5 Selection of UCP technical personnel 05/12/200220/12/2002 $ 15,000.00
2.6 External Audit for the periods 2004 and 2005.
01/06/2005 31/03/2006 $ 43,200.00
2.7 External Audit of the Project 2008-2009 09/03/200931/03/2010 $ 18,200.00

54
Annex 3. Economic and Financial Analysis Not Applicable

55
Annex 4. Bank Lending and Implementation Support/Supervision Processes
(a) Task Team members Names Title Unit
Lending Maria-Luisa Escobar Task Manager, Sr. HNP Economist LCSHD Eduardo Brito Sr. Counsel LEGLA Manuel Vargas Financial Management Officer LCOAA Maria Valeria Pena Lead Sociologist LCSEO Monica Rojas de Arnez Disbursement Officer LOAEL
Rosa Estrada Procurement and Implementation Analyst
LCSHD
Ruth Levine Sr. HNP Economist LCSHD Sonia Levere Language Program Assistant LCSHD Suzana de Campos Abbott Principal Operations Officer LCC2C
Supervision/ICR
Rafael Cortez Task Team Leader, Sr. Economist(Health)
LCSHD
C. Izquierdo-Gonzalez Finance Assistant CTRDM Carlos E. Sobrado Senior Economist LCSPP Carlos Marcelo Bortman Sr. Public Health Specialist LCSHH Evelyn Villatoro Senior Procurement Specialist EAPPR Fabienne Mroczka Financial Management Specialist LCSFM Fernando Montenegro Torres Sr. Economist (Health) LCSHH Gustavo Castro F. Raposo Finance Analyst CTRDM Irani G. Escolano Consultant LCSPT Jesus María Fernández Díaz Sr. Public Health Specialist LCSHH Julia B. Nannucci Temporary LCSHH Laura B. Rawlings Lead Social Protection Specialist HDNSP Luis R. Prada Villalobos Senior Procurement Specialist MNAPR Manuel Salazar Sr. Social Protection Specialist AFTSP
Rocio Schmunis ET Consultant LCSHD Rolande Simone Pryce Country Officer LCC3C Solange A. Alliali Sr. Counsel LEGLA Sonia M. Levere Language Program Assistant LCSHH
Suzana de Campos Abbott ICR Primary Author LCSHD Viviana A. Gonzalez E T Temporary LCSHE

56
(b) Staff Time and Cost Staff Time and Cost (Bank Budget Only)
Stage of Project Cycle No. of staff weeks USD Thousands (including
travel and consultant costs)Lending
FY01 8 37.03 FY02 3 13.71 FY03 9 39.52 FY04 0.00 FY05 0.00 FY06 2 7.41 FY07 1.32 FY08 0.00
Total: 22 98.99 Supervision/ICR
FY03 3 22.74 FY04 18 83.73 FY05 12 55.24 FY06 19 88.98 FY07 29 169.21 FY08 20 111.00 FY09 12 87.47 FY10 13 66.46
Total: 126 684.83
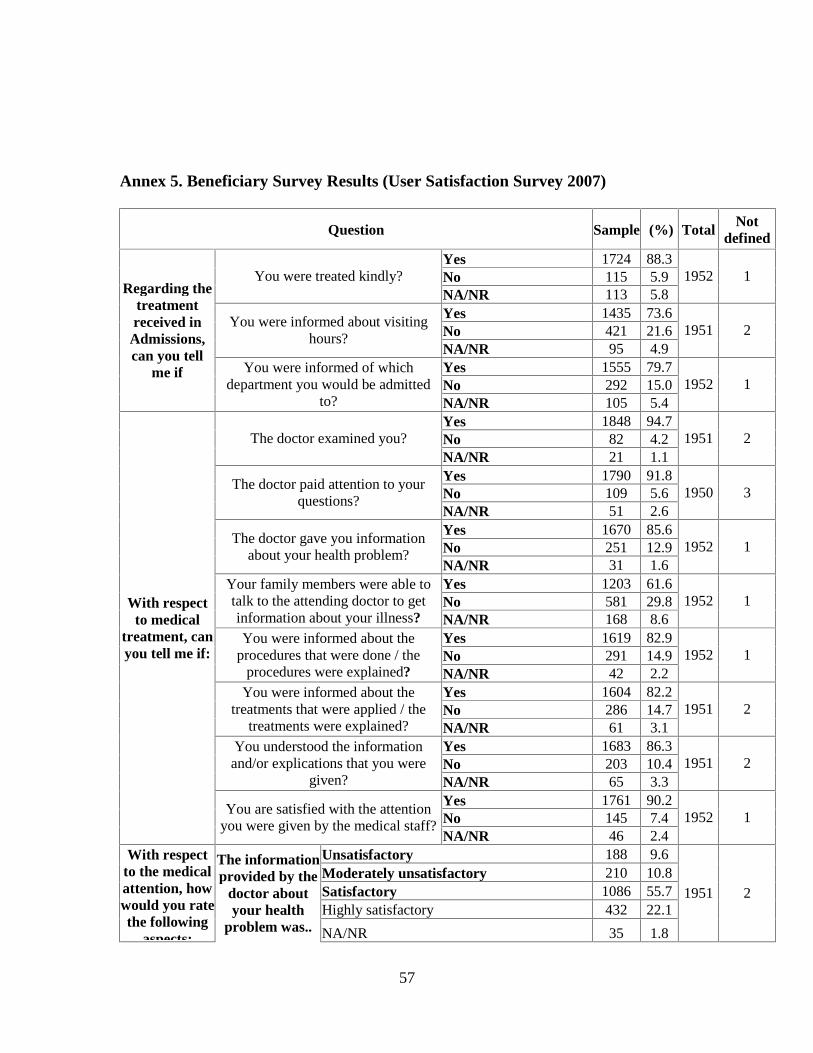
57
Annex 5. Beneficiary Survey Results (User Satisfaction Survey 2007)
Question Sample (%) Total Not defined
Yes 1724 88.3No 115 5.9 You were treated kindly? NA/NR 113 5.8
1952 1
Yes 1435 73.6No 421 21.6
You were informed about visiting hours?
NA/NR 95 4.9 1951 2
Yes 1555 79.7No 292 15.0
Regarding the treatment received in Admissions, can you tell
me if You were informed of which department you would be admitted
to? NA/NR 105 5.4 1952 1
Yes 1848 94.7No 82 4.2 The doctor examined you? NA/NR 21 1.1
1951 2
Yes 1790 91.8No 109 5.6
The doctor paid attention to your questions?
NA/NR 51 2.6 1950 3
Yes 1670 85.6No 251 12.9
The doctor gave you information about your health problem?
NA/NR 31 1.6 1952 1
Yes 1203 61.6No 581 29.8
Your family members were able to talk to the attending doctor to get information about your illness? NA/NR 168 8.6
1952 1
Yes 1619 82.9No 291 14.9
You were informed about the procedures that were done / the
procedures were explained? NA/NR 42 2.2 1952 1
Yes 1604 82.2No 286 14.7
You were informed about the treatments that were applied / the
treatments were explained? NA/NR 61 3.1 1951 2
Yes 1683 86.3No 203 10.4
You understood the information and/or explications that you were
given? NA/NR 65 3.3 1951 2
Yes 1761 90.2No 145 7.4
With respect to medical
treatment, can you tell me if:
You are satisfied with the attention you were given by the medical staff?
NA/NR 46 2.4 1952 1
Unsatisfactory 188 9.6 Moderately unsatisfactory 210 10.8Satisfactory 1086 55.7Highly satisfactory 432 22.1
With respect to the medical attention, how would you rate the following
aspects:
The information provided by the
doctor about your health
problem was.. NA/NR 35 1.8
1951 2
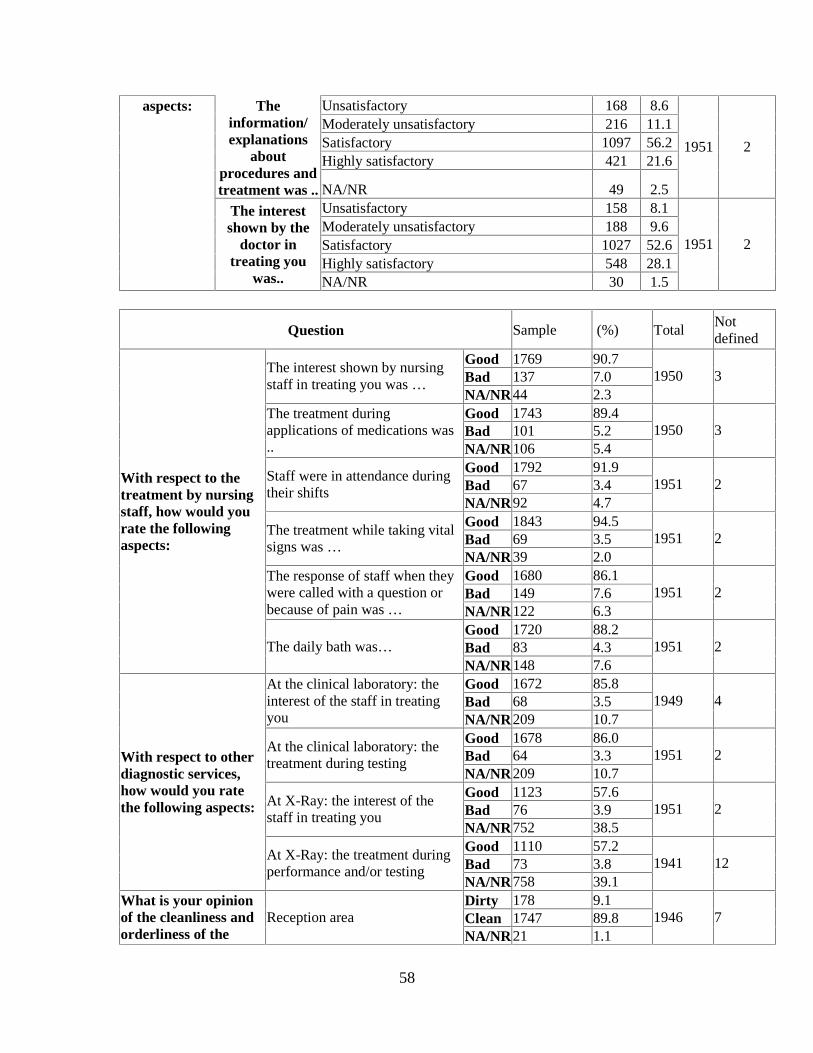
58
Unsatisfactory 168 8.6 Moderately unsatisfactory 216 11.1Satisfactory 1097 56.2Highly satisfactory 421 21.6
The information/ explanations
about procedures and treatment was ..NA/NR 49 2.5
1951 2
Unsatisfactory 158 8.1 Moderately unsatisfactory 188 9.6 Satisfactory 1027 52.6Highly satisfactory 548 28.1
aspects:
The interest shown by the
doctor in treating you
was.. NA/NR 30 1.5
1951 2
Question Sample (%) Total Not defined
Good 1769 90.7 Bad 137 7.0
The interest shown by nursing staff in treating you was …
NA/NR 44 2.3 1950 3
Good 1743 89.4 Bad 101 5.2
The treatment during applications of medications was .. NA/NR 106 5.4
1950 3
Good 1792 91.9 Bad 67 3.4
Staff were in attendance during their shifts
NA/NR 92 4.7 1951 2
Good 1843 94.5 Bad 69 3.5
The treatment while taking vital signs was …
NA/NR 39 2.0 1951 2
Good 1680 86.1 Bad 149 7.6
The response of staff when they were called with a question or because of pain was … NA/NR 122 6.3
1951 2
Good 1720 88.2 Bad 83 4.3
With respect to the treatment by nursing staff, how would you rate the following aspects:
The daily bath was… NA/NR 148 7.6
1951 2
Good 1672 85.8 Bad 68 3.5
At the clinical laboratory: the interest of the staff in treating you NA/NR 209 10.7
1949 4
Good 1678 86.0 Bad 64 3.3
At the clinical laboratory: the treatment during testing
NA/NR 209 10.7 1951 2
Good 1123 57.6 Bad 76 3.9
At X-Ray: the interest of the staff in treating you
NA/NR 752 38.5 1951 2
Good 1110 57.2 Bad 73 3.8
With respect to other diagnostic services, how would you rate the following aspects:
At X-Ray: the treatment during performance and/or testing
NA/NR 758 39.1 1941 12
Dirty 178 9.1 Clean 1747 89.8
What is your opinion of the cleanliness and orderliness of the
Reception area NA/NR 21 1.1
1946 7

59
Question Sample (%) Total Not defined
Dirty 392 20.1 Clean 1474 75.7 Bathroom NA/NR 82 4.2
1948 5
Dirty 298 15.3 Clean 1528 78.4 Bathrooms or showers NA/NR 124 6.4
1950 3
Dirty 174 8.9 Clean 1712 87.7 Hallways NA/NR 65 3.3
1951 2
Dirty 159 8.2 Clean 1769 90.7
following areas and furniture?
Bed NA/NR 22 1.1
1950 3
Inadequate 243 12.5 Adequate 1634 83.8 Visiting hours NA/NR 73 3.7
1950 3
Inadequate 174 8.9 Adequate 1588 81.4
The rules governing family members who are taking care of the sick NA/NR 188 9.6
1950 3
Inadequate 124 6.4 Adequate 1784 91.4
Regarding your stay in the hospital, what is your option of:
The attention received during the hospital stay
NA/NR 43 2.2 1951 2
Question Sample (%)e Total Not defined
From 0 to 15 minutes 1329 20.14 From 15 mins to half hour
1781 26.99
From half to 1 hour 1869 28.33 From 1 to 2 hours 1079 16.35 More than 2 hours 425 6.44 One day or more 21 0.32
On the day of your appointment, to be seen by the doctor
N/A 94 1.42
6598 8
From 0 to 15 minutes 2654 40.25 From 15 mins to half hour
1624 24.63
From half to 1 hour 820 12.44 From 1 to 2 hours 465 7.05 More than 2 hours 424 6.43 One day or more 340 5.16
On the day that you made the appointment, to be given an appointment time
N/A 266 4.03
6593 13
From 0 to 15 minutes 4896 74.23
Cho
osin
gfr
omam
ong
the
follo
win
gop
tion
s,w
hat
have
been
the
wai
ting
tim
es:
To fill out the forms From 15 mins to half hour
1142 17.31
6596 10

60
Question Sample (%)e Total Not defined
From half to 1 hour 313 4.75 From 1 to 2 hours 62 0.94 More than 2 hours 25 0.38 One day or more 20 0.30 N/A 138 2.09
From 0 to 15 minutes 3454 52.36 From 15 mins to half hour
1374 20.83
From half to 1 hour 885 13.42 From 1 to 2 hours 333 5.05 More than 2 hours 197 2.99 One day or more 49 0.74
To submit the prescription to the pharmacy
N/A 305 4.62
6597 9
From 0 to 15 minutes 909 13.78 From 15 mins to half hour
867 13.15
From half to 1 hour 1169 17.73 From 1 to 2 hours 1327 20.12 More than 2 hours 1678 25.44 One day or more 333 5.05
For the medications to be dispensed
N/A 312 4.73
6595 11
From 0 to 15 minutes 2216 33.65 From 15 mins to half
hour 1847 28.04
From half to 1 hour 1153 17.51 From 1 to 2 hours 497 7.55 More than 2 hours 133 2.02 One day or more 88 1.34
Cho
osin
gfr
omam
ong
the
follo
win
gop
tion
s,w
hat
have
been
the
wai
ting
tim
es: For the clinical laboratory to
take or receive your samples
N/A 652 9.90
6586 20
Less than 1 week 487 7.42 From 1 to 2 weeks 335 5.11 From 2 weeks to 1
month 394 6.01
From 1 to 3 months 773 11.78 More than 3 months 1210 18.45
To get access to x-ray services
N/A 3361 51.23
6560 46
Less than 1 week 224 3.41 From 1 to 2 weeks 223 3.39 From 2 weeks to 1
month 401 6.10
From 1 to 3 months 530 8.07 More than 3 months 1139 17.33
To have an ultrasound
N/A 4054 61.70
6571 35
Less than 1 week 258 3.93
Cho
osin
gfr
omam
ong
the
follo
win
gop
tion
s,w
hat
have
been
the
wai
ting
tim
es:
To get access to an appointment with a specialist From 1 to 2 weeks 255 3.89
6559 47
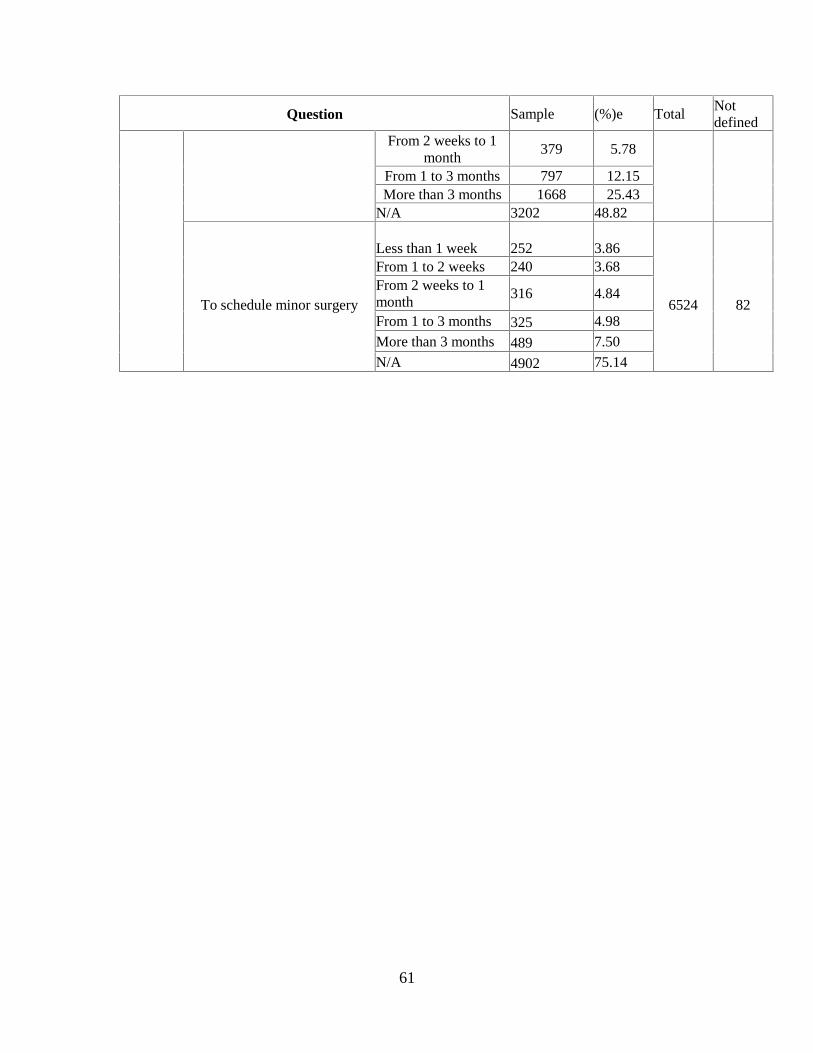
61
Question Sample (%)e Total Not defined
From 2 weeks to 1 month
379 5.78
From 1 to 3 months 797 12.15 More than 3 months 1668 25.43
N/A 3202 48.82
Less than 1 week 252
3.86
From 1 to 2 weeks 240 3.68 From 2 weeks to 1 month
316 4.84
From 1 to 3 months 325 4.98 More than 3 months 489 7.50
To schedule minor surgery
N/A 4902 75.14
6524
82

62
Annex 6. Stakeholder Workshop Report and Results Not applicable

63
Annex 7. Summary of Borrower’s ICR and/or Comments on Draft ICR The Borrower submitted its Project Completion Report on March 25, 2010. The report is in the Project files. The Borrower also submitted official comments on this ICR on June 16, 2010. These comments support the conclusions and findings of the report. The Borrower also acknowledged the lessons learned included in the report that would be helpful to design future projects in Costa Rica. All recommendation provided by the Borrower have been incorporated in the document. Informal translation of Borrower’s comments (letter dated June 16, 2010) The ICR highlights the objectives and accomplishments of the project and it describes the goals that were met during the implementation period. The ICR also describes the factors that affected project execution, which the Government considers very valuable for the CCSS and also for the Bank in its role as a financial institution. The Government requests the Bank to correct the total amount disbursed mentioned in the document. PCU records shows a total amount disbursed of US$13,306.049.34. Once this amount is corrected in the report, the Government endorses the contents of the ICR and agrees to make the document public.
Signed by
Juan Carlos Pacheco Romero Director Public Credit Ministry of Finance Costa Rica

64

65

66
Annex 8. Comments of Co-financiers and Other Partners/Stakeholders
Not applicable

67
Annex 9. List of Supporting Documents Project Appraisal Document, Health Sector Strengthening and Modernization Project, Report No. 22170 dated June 22, 2001. Implementation Completion Report, Health Sector Reform Project, Report No. 25713 dated May 14, 2003. CAS Costa Rica Country Assistance Strategy, Report No. R-93-57 dated March 10, 1993. Draft Borrower Project Completion Report dated May 2010. El País, “Caja Asegura que mayor controles de medicamentos en sus farmacias”. January 8, 2010. “CCSS eleva rigurosidad en controles de medicamentos” CCSS, Memoria Institucional 2008. CCSS, Una CCSS Renovada Hacia el 2025, Políticas Institucionales 2007-2012, Planeamiento Estratégico Institucional y Programación de Inversiones. Ministerio de Salud, Plan Estratégico 2008-2010, May 2007.

68
Annex 10. Policy Activity Schedule (PAS) Area Objectives Issue First Evaluation
(December 2002) Second Evaluation (December 2004)
Project Completion
I. INSTITUTIONAL STENGTHENING AND REGULATION Institutional Strengthening of the CCSS
To introduce the organizational changes that are required to prepare the CCSS for increasing decentralization and other changes related to the separation of financing and provision The continued strengthening and consolidation of the Dirección de Compra in the CCSS will remain a critical issue with regard to the overall success of the reforms
The CCSS continues with a centralized organizational structure that is incompatible with the new decentralized functions and the separation of financing from provision of health services The implementation of management contracts, and the development of public/private partnerships, requires strengthening of the capacity to formulate outcome-based indicators and to evaluate these indicators
New organizational structure of the CCSS-based separation of financing, purchasing and provision and according to decentralization process approved by CCSS At least 20% of contracts with CCSS health care providers include outcome indicators operating under performance contracts 15% increase in quality adjusted coverage rates in primary health care
New strategy for human resource management approved and implemented Implementation of new organizational structure of the CCSS-based separation of financing, purchasing and provision and according to decentralization process as defined during the first evaluation At least 60% of contracts with CCSS health care providers include outcome indicators under performance contracts 40% increase in quality adjusted coverage rates in primary health care % increase in lower income patients’ satisfaction with CCSS service providers
Institutional Strengthening of the MOH
To support completion of the ongoing restructuring process of the MOH by developing the instruments and functions required to consolidate the process of
The institutional strengthening of the MOH stated with a transformation of its role in the sector from being mainly a provider to become the
Human resource strengthening and restructuring implemented according to MOH program: At least 500 people trained on management, public health, health economics
50% of MOH regions having assumed the implementation of regulatory activities Feasibility study for the development of new regulatory agencies to support the MOH in the execution of epidemiological surveillance,
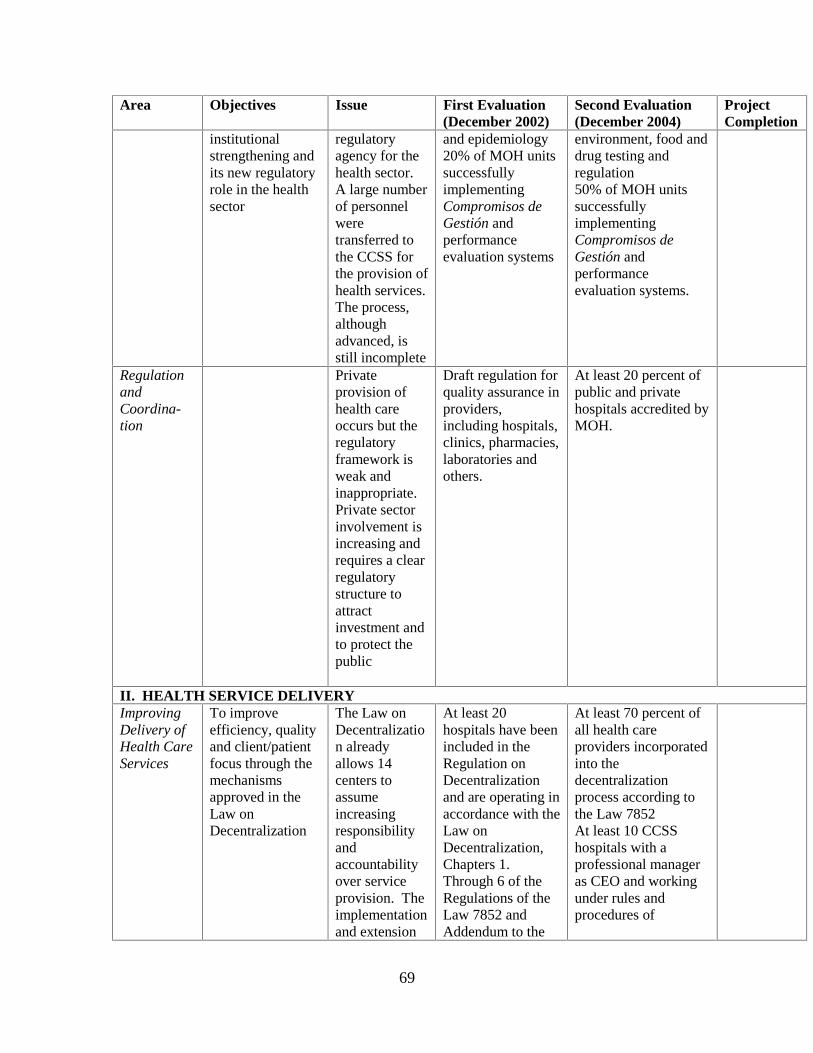
69
Area Objectives Issue First Evaluation (December 2002)
Second Evaluation (December 2004)
Project Completion
institutional strengthening and its new regulatory role in the health sector
regulatory agency for the health sector. A large number of personnel were transferred to the CCSS for the provision of health services. The process, although advanced, is still incomplete
and epidemiology 20% of MOH units successfully implementing Compromisos de Gestión and performance evaluation systems
environment, food and drug testing and regulation 50% of MOH units successfully implementing Compromisos de Gestión and performance evaluation systems.
Regulation and Coordina-tion
Private provision of health care occurs but the regulatory framework is weak and inappropriate. Private sector involvement is increasing and requires a clear regulatory structure to attract investment and to protect the public
Draft regulation for quality assurance in providers, including hospitals, clinics, pharmacies, laboratories and others.
At least 20 percent of public and private hospitals accredited by MOH.
II. HEALTH SERVICE DELIVERY Improving Delivery of Health Care Services
To improve efficiency, quality and client/patient focus through the mechanisms approved in the Law on Decentralization
The Law on Decentralization already allows 14 centers to assume increasing responsibility and accountability over service provision. The implementation and extension
At least 20 hospitals have been included in the Regulation on Decentralization and are operating in accordance with the Law on Decentralization, Chapters 1. Through 6 of the Regulations of the Law 7852 and Addendum to the
At least 70 percent of all health care providers incorporated into the decentralization process according to the Law 7852 At least 10 CCSS hospitals with a professional manager as CEO and working under rules and procedures of

70
Area Objectives Issue First Evaluation (December 2002)
Second Evaluation (December 2004)
Project Completion
To promote the development of outpatient and home care solutions to improve efficiency and patient focus
of the Law will require considerable investment and support.
Presently fewer than 25 percent of all surgeries are performed on an ambulatory basis, even thought international standards indicate that this could be increased to 50 percent. Home care and non-hospital solutions are extremely limited in the CCSS delivery network The establishment of EBAIS has led to important improvements in access and coverage. Systematic reviews of the current status of the initiative are required to consolidate implementation
Compromisos de Gestión. Approval by the CCSS Board of strategies and investment plan to increase and to improve ambulatory solutions as described in the health sector concept note. Ambulatory surgery as 8% of total hospital discharges
Continuation of the EBAIS model by consolidating all EBAIS opened until 2001, and by opening 50 more EBAIS
Ambulatory surgery to be 20% of total hospital discharges
Continuation of the EBAIS model by opening 100 more EBAIS and consolidating all EBAIS in the territory

71
Area Objectives Issue First Evaluation (December 2002)
Second Evaluation (December 2004)
Project Completion
of the model.
Planning, Purchasing and Acquisition of Medical Inputs and Pharmaceu-ticals
To improve efficiency in the acquisition and distribution of pharmaceuticals to health care providers and ultimately to patients.
The CCSS is the largest purchaser. Purchases are centralized, there are large inefficiencies in the purchase and delivery of pharmaceuticals.
25% decrease of time between initial bid and delivery of pharmaceuticals 30% decrease of total pharmaceutical budget spent on warehouse storage costs.
40% decrease of time between initial bid and delivery of pharmaceuticals 75% decrease of total pharmaceutical budget spent on warehouse storage costs.
III. FINANCING AND RESOURCE ALLOCATION Resource Allocation
To develop resource allocation policies at the macro level that promote equity
Specific resource allocation policies are required to make the transition to a more equitable distribution of resources following a population-based resource allocation model
An information system (SIPO) has been developed by IMAS to improve targeting of social sector resources, however, limited implementation in line ministries has been carried out.
Improve equity by reducing the gap between average per capita spending in the Brunca Region and the National Average by 50% Inclusion of case mix (DRGs) in the payment mechanism for at least two National Hospitals At least 20% of CCSS Health Areas have been surveyed and incorporated into SIPO.
Improved equity by reducing the gap between average per capita spending in the Brunca Region and the National Average by 50% beyond the rates attained in the second evaluation At least 40% of CCSS Health Areas have been surveyed and incorporated into SIPO.
Revenue Collection
To improve the efficiency of the CCSS invoicing system and to prepare the CCSS to collect pension payments for newly approved 2nd and 3rd pillar of the capitalized pension
The approval of the Ley de Protección al Trabajador stipulates that the CCSS will act as the central collection agency for the pension system. This new
4% real annual increase on revenue collection as a result of successful centralized collection system and evasion reduction.
4% real annual increase on revenue collection as a result of successful centralized collection system and evasion reduction.
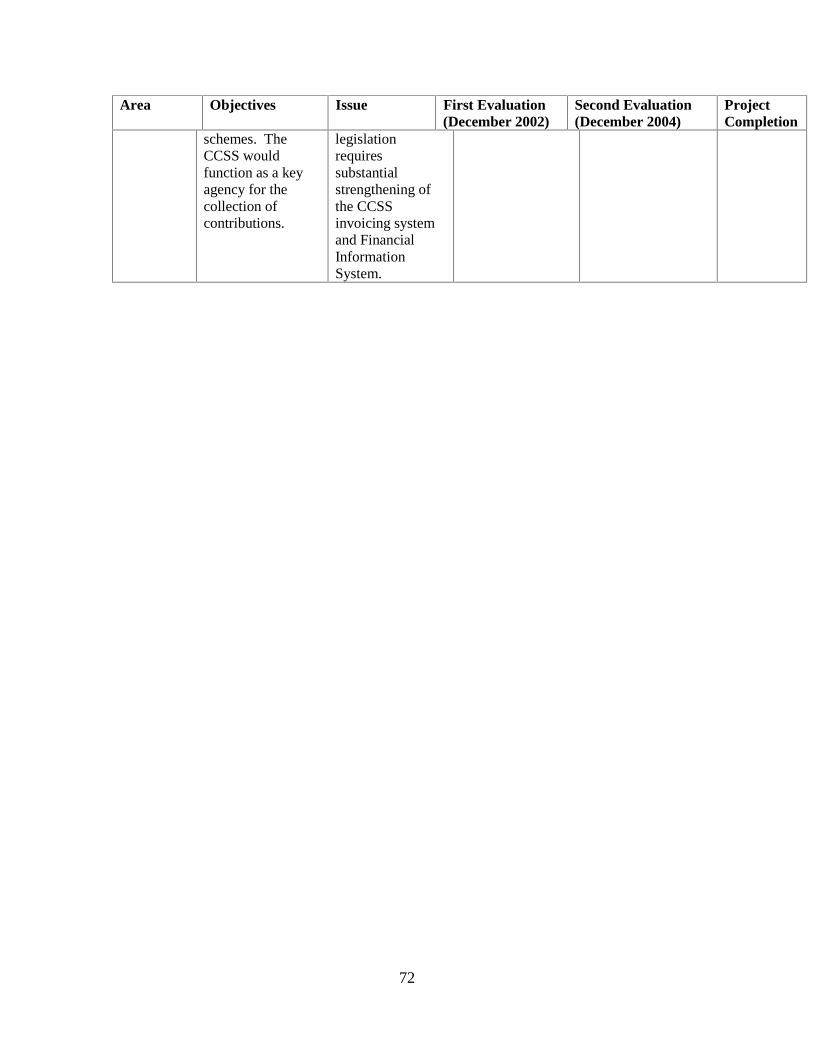
72
Area Objectives Issue First Evaluation (December 2002)
Second Evaluation (December 2004)
Project Completion
schemes. The CCSS would function as a key agency for the collection of contributions.
legislation requires substantial strengthening of the CCSS invoicing system and Financial Information System.

73
Annex 11: Project Actions Matrix
Area/Activity under
PAS Actions Supported by
Project Observations Status at
Completion I.A INSTITUTIONAL STRENGTHENING CCSS CCSS Board approval of the improved evaluation framework and implementation strategy, including: (i) evaluation process; (ii) timing; and (iii) information systems
Strengthening sectoral coordination
Assist with implementation of software to manage purchasing and evaluation process Implementation, monitoring and evaluation of compliance with National Health Plan (Plan de Atención a las Personas-PASP) and Health Services Planning Strategy (PESS) Training of staff from Purchasing (Dirección de Compra) and other management units (Gerencias) on issues related to purchasing Support to IMAS and other social sector institutions involved in social sector planning and priority setting
I.B INSTITUTIONAL STRENGTHENING MINISTY OF HEALTH Restructuring plan for the MOH executed
Consultancies and training to support the implementation of restructuring plan in the MOH Assist MOH with the implementation of management information systems and other instruments required to improve stewardship
Draft regulation for private provision and insurance, submitted to the IBRD including: (i) minimum quality standards; (ii) licensing and credentialing for
Consultancies to provide local and international technical assistance for the preparation of draft regulations on quality assurance and other core regulator issues facing the MOH.
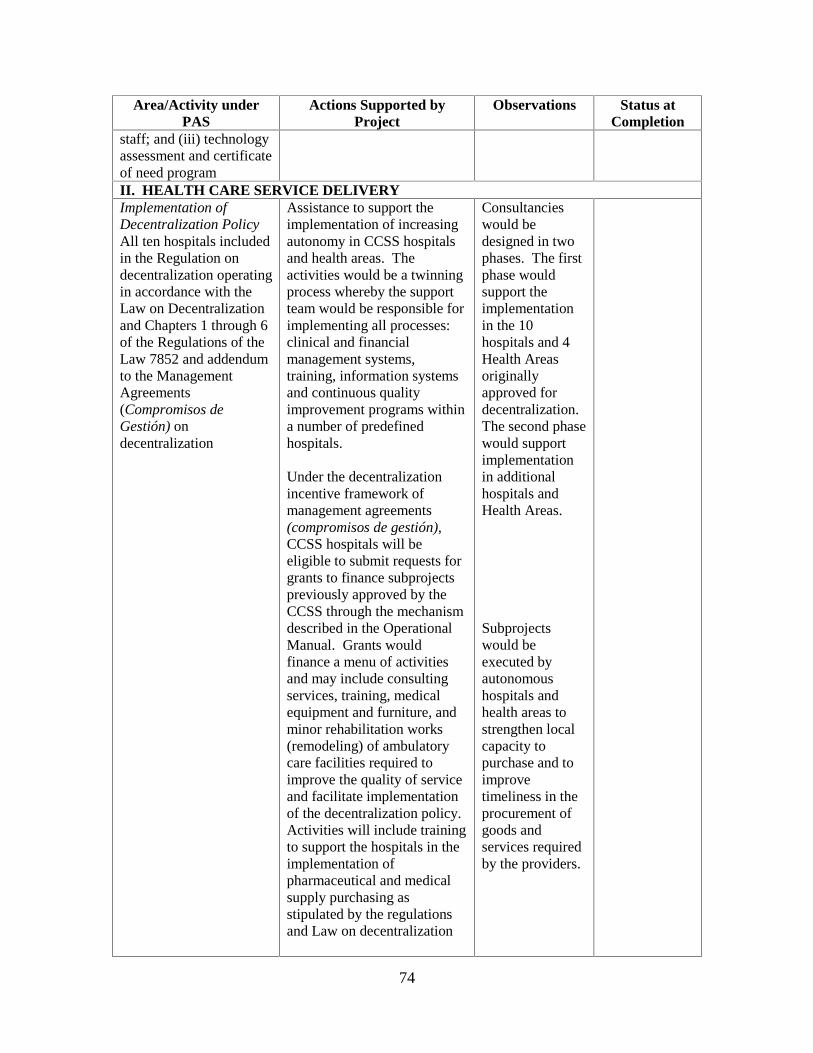
74
Area/Activity under PAS
Actions Supported by Project
Observations Status at Completion
staff; and (iii) technology assessment and certificate of need program II. HEALTH CARE SERVICE DELIVERY Implementation of Decentralization Policy All ten hospitals included in the Regulation on decentralization operating in accordance with the Law on Decentralization and Chapters 1 through 6 of the Regulations of the Law 7852 and addendum to the Management Agreements (Compromisos de Gestión) ondecentralization
Assistance to support the implementation of increasing autonomy in CCSS hospitals and health areas. The activities would be a twinning process whereby the support team would be responsible for implementing all processes: clinical and financial management systems, training, information systems and continuous quality improvement programs within a number of predefined hospitals. Under the decentralization incentive framework of management agreements (compromisos de gestión),CCSS hospitals will be eligible to submit requests for grants to finance subprojects previously approved by the CCSS through the mechanism described in the Operational Manual. Grants would finance a menu of activities and may include consulting services, training, medical equipment and furniture, and minor rehabilitation works (remodeling) of ambulatory care facilities required to improve the quality of service and facilitate implementation of the decentralization policy. Activities will include training to support the hospitals in the implementation of pharmaceutical and medical supply purchasing as stipulated by the regulations and Law on decentralization
Consultancies would be designed in two phases. The first phase would support the implementation in the 10 hospitals and 4 Health Areas originally approved for decentralization. The second phase would support implementation in additional hospitals and Health Areas.
Subprojects would be executed by autonomous hospitals and health areas to strengthen local capacity to purchase and to improve timeliness in the procurement of goods and services required by the providers.

75
Area/Activity under PAS
Actions Supported by Project
Observations Status at Completion
At least ten centers functioning with a professional hospital manager with general management oversight
Provide autonomous hospitals with resources required to hire professional managers to support the implementation of the decentralization process.
At least 40 percent of all hospitals (including the national hospitals) carrying out their own purchasing of pharmaceuticals and supplies as stipulated in the regulations to the Law.
Consultancy to support implementation of a pharmacy benefit management system that will allow for more rational pharmaceutical prescribing and use.
Increasing ambulatory care solutions To promote the development of outpatient and home care solutions to improve efficiency and patient focus
Consultancy to define strategic plan and investment strategy to increase the percentage of ambulatory surgeries to 20 percent. Subproject investments in facility rehabilitation, equipment, technology, training and supervision required to enable CCSS hospitals to increase ambulatory surgery.
Product would identify strategic areas based on the PESS and then propose the needed changes in equipment, training and infrastructure. Once the strategic plan is identified and agreed with providers, the providers would execute required investments on a decentralized basis, via the submission of subprojects.
Consolidation of the primary care model (EBAIS)
Participate with national consultants and MOH/CCCSS staff in evaluation of the Modelo de Atención.Prepare recommendations for improvement/consolidation. Strengthening and expansion of the EBAIS model to uncovered populations or to improve the quality of care in existing areas. Investments

76
Area/Activity under PAS
Actions Supported by Project
Observations Status at Completion
would include equipment, medical and non-medical training, and consultancies, including those necessary for consultation with minority groups (indigenous populations and those of African descent).
III. FINANCING AND RESOURCE ALLOCATION Resource Allocation CCSS Board approval of allocation formula to improve equity
Technical assistance to design and implement changes in the capitation formula to allow for risk adjustment. Consultancy to implement the information system to improve targeting (SIPO) of social sector expenditures, in coordination with IMAS. Implementation of SIPO in the CCSS, including training, equipment and maintenance of the system, in coordination with IMAS. Assistance to support implementation of National Health Accounts.
Evidence of improvement in resource allocation by the introduction of case mix (DRGs) in the reimbursement mechanism for at least two National Hospitals
Consultancy to support continued implementation of case mix related payment systems in CCSS hospitals, including continuation of software licenses required for management of the DRG system.
Revenue collections Equipment purchases for computer hardware and telecommunications equipment approved to ensure implementation
Integral solution to implement the MIS system (SICERE).
IV. EVALUATION AND MONITORING Project Management, Evaluation and
Assistance to support the evaluation and monitoring of

77
Area/Activity under PAS
Actions Supported by Project
Observations Status at Completion
Monitoring the Project. Timely execution of project administration functions, including delivery of project inputs: consultancies, training, equipment and travel. Assistance to support the modernization process with information, education and communication campaign.

78
Annex 12: Changes in Administration, CCSS Leadership, Project Management, and Reporting Relationships
Executive Leadership – Health Sector Strengthening and Modernization Project
President of Costa Rica
Executive President CCSS
Executive Director of the Project
Executive Director reported to
Dr. Miguel Angel Rodríguez Echeverría
(1998-2002)
Dr. Rodolfo Piza Rocafort
(1998-2002)
Dr. Juan Carlos Sánchez Arguedas
(1998-2003)
Executive President CCSS
Dr. Eliseo Vargas (2002-2003)
Lic. Norma Montero Guzmán
(2003- May 2004)
Executive President CCSS
Dr. Horacio Solano (2003-October 2004)
Dra. María Eugenia Villalta
(May – October 2004)
Executive President CCSS
Executive President CCSS
Dr. Abel Pacheco de la Espriella (2002-2006)
Dr. Alberto Saénz (October 2004-May
2006)
Dr. Zeirith Rojas Cerna
(October 2004-December 2006)
Directorate of Operations
Lic. Gerardo Marín Barrantes
(January-April, 2007)
Directorate of Infrastructure and
Technologies7
Dr. Oscar Arias Sánchez
(2006-2010)
Dr. Eduardo Doryan (May 2006- May
2010)
Dra. Daisy Corrales Díaz
(May 2007–Present)
Directorate of Infrastructure and
Technologies
7 The functions of the Directorate of Operations were later divided into two new Directorates: the Directorate of Logistics and the Directorate of Infrastructure and Technologies.

79


















