
Workshop 25 Optimization of CT Urography in Hematuriaradreference.info/SAR13_files/CTU...
30
Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Downloaded from sar2013.conferencespot.org Workshop 25 Optimization of CT Urography in Hematuria Aart J. van der Molen, MD Leiden University Medical Center The Netherlands SAR Annual Meeting 2013 Wailea (Maui) HI, 26 February 2013 Downloaded from sar2013.conferencespot.org
Transcript of Workshop 25 Optimization of CT Urography in Hematuriaradreference.info/SAR13_files/CTU...

Downloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.orgDownloaded from sar2013.conferencespot.org
Workshop 25Optimization of CT Urographyin Hematuria
Aart J. van der Molen, MDLeiden University Medical Center
The Netherlands
SAR Annual Meeting 2013Wailea (Maui) HI, 26 February 2013
Downloaded from sar2013.conferencespot.org

Hematuria and Risk of UCC
• Hematuria very frequent clinical presentation• 6-8% of urological consults
• Microhematuria: 0-9% risk UCC• Macrohematuria: 10-28% risk UCC
• Hematuria causes in UK in 4020 patients> LT UCC 10,3% RCC 1,5%> Stones 8,4% UT UCC 0,3%
Edwards, BJU Int 2006Downloaded from sar2013.conferencespot.org

Urothelial Cell Carcinoma
• UCC - 10% tumors UT> Multicentricity: 2-4% UCC in LT and UT
• Synchronous tumors> 24-39% of UT pats synchronous tumors in LT> 1-2% bilateral if renal UCC> 2-9% bilateral if ureteral UCC
• Metachronous tumors> 11-13% of UT pats metachronous tumors in UT
Downloaded from sar2013.conferencespot.org

Tumor Incidence
• NL Tumor registry
• Nationwide database on 16,8 million inhabitants
• Micro: no UT-UCC in men < 50yr and women < 70yr
• Macro: no UT-UCC in patients < 50yr• Most malignancy at younger age RCC or Bladder
UCCwww.cijfersoverkanker.nl
Downloaded from sar2013.conferencespot.org

2010 Urological Tumor Incidence NL
NL Tumor Registry, 2012Downloaded from sar2013.conferencespot.org

NVU Hematuria Guideline NL 2011Risk UCC Low Medium High
HematuriaMicro< 50 yr
Macro< 50 yr
Micro> 50 yr
Macro> 50 yr
Initial RR, eGFR, U sediment, U dysmorphic erys, U protein
1st Step (US + Cys) US + Cys US + Cys CTU + Cys
2nd Step uCT or CTU uCT or CTU U cyto
3rd Step U cyto U cyto URS
4th Step URS URSVan der Molen – AJR 2012
Downloaded from sar2013.conferencespot.org

Justification CTU
In clinical picture of painless hematuria:• Use CTU as 1st line study in high-risk patients• When UT-UCC is the main question, risk
increased in macrohematuria > 50 yrs• Otherwise, CTU should be 2nd line
• In low- to medium-risk do uCT first and check> Most significant findings already seen on uCT
• When needed, complete to CTU in same examCauberg – J Endourol 2011Lokken – AJR 2012Van der Molen – AJR 2012Downloaded from sar2013.conferencespot.org
AUA Guideline AMH 2012
• Initial evaluation of AMH should include multiphasic CTU with phases for renal parenchyma and urothelium
• For patients with CTU contra-indications MRU is alternative, in combintion with RPG for upper tracts
• For patients with CTU/MRU contra-indications uCT or US combined with RPG is alternative
• Cystoscopy performed on all patients ≥ 35y with asymptomatic AMH
• Cystoscopy performed on all AMH patients with risk factors for UT malignancy, regardless of age
Downloaded from sar2013.conferencespot.org

How High is the Dose in CTU ?
• Scary radiation dose in early studies….> Values 25-35 mSv reported, highs up to 66 mSv> Some low doses down to 15 mSv
• Analysis in 3 starting centres in 2009 in NL/Spain• 2-phase CTU 16 mSv – 3-phase CTU 22 mSv
> Valid for average sized patients (E not defined for obese)
• Newer analysis CTU in 2011/2012 - per scan phase
Caoili – Radiology 2005Vritska – AJR 2009Downloaded from sar2013.conferencespot.org

LUMC Dose in CTU: FBP 2011
• Data from all CTU in LUMC @ Aquilion 64 / ONE
Phase Range DLP EAll CTU 1020 ± 565 14,4 ± 8,0
UP 395 ± 71 260 ± 134 3,7 ± 1,9NP 266 ± 96 338 ± 203 4,3 ± 3,4Test 18 ± 2 11 ± 11 0,15 ± 0,15EP 1 374 ± 72 477 ± 264 6,7 ± 3,7EP 2 294 ± 58 312 ± 160 4,4 ± 2,3
Van der Molen, in preparationDownloaded from sar2013.conferencespot.org

LUMC Dose in CTU: AIDR3D 2012• Data from all CTU in LUMC with iterative recon• Interim analysis 6 mo ongoing study @ Aquilion
ONEPhase Range DLP EAll CTU 487 ± 300 6,9 ± 4,2
UP 514 ± 47 146 ± 106 2,1 ± 1,5NP 338 ± 60 137 ± 86 1,9 ± 1,2Test 20 ± 2 10 ± 6 0,14 ± 0,09EP 1 517 ± 37 228 ± 149 3,2 ± 2,1EP 2 447 ± 119 163 ± 42 2,3 ± 0,6
Van der Molen, in preparationDownloaded from sar2013.conferencespot.org

Old School 3-Phase CTU
Unenhanced A&P
NephrographicA
ExcretoryA&P
Downloaded from sar2013.conferencespot.org

Oral Hydration
Negative CM for bowel marking• facilitates associated findings
Water before CTU• resorbed from bowel: aids diuresis, avoids dehydration• cheap and easy• 800-1000ml within 30min before CTU • Improves complete opacification upper/lower ureter
Silverman, Radiology 2006
Jammie!
Downloaded from sar2013.conferencespot.org

Basic CTU Scanning
CTU Technique parameters • Near isotropic imaging
> Remember: resolution ≠ voxel size• Technique parameters: kV, mA, rotation
> 100-120 kV, 3D tube current modulation, rotation ∼ body size
• Acquisition parameters: collimation, pitch> High resolution – thin slice acquisition, low pitch
• Reconstruction parameters: slice thickness, rec index> High resolution – thin slice reconstruction, overlapping
• Standard MPR/curved MPR - MIP or VRT only if needed
Downloaded from sar2013.conferencespot.org

Voxel Size is NOT Resolution• Voxel size
> SFOV / Matrix (400/512 or around 0.8 mm)
> Nominal reconstructed slice thickness
• In-plane spatial resolution> Determined by PSF Kernel: 6-7 lp/mm > 0.7-0.8mm for Standard
• Through-plane spatial resolution> True effective slice thickness > Some 30% larger for thin slice
Downloaded from sar2013.conferencespot.org

Basic CTU Protocol
CTU Technique parameters – Aquilion ONE• Collimation 80 x 0.5mm – Pitch 0.812
> Ultra-Helical 160 x 0.5mm has too much overrange !• Reconstruction 1/1mm for MPR/CPR/MIP/VR• Reconstruction 5/5mm + 3/3 cor MPR for clinicians• 100 kV is sufficient
> 120 kV easier for TCM or Iterative Recon (AIDR 3D)• Tube current modulation: SD/NI 15-24 (5mm slices)• CTDIvol 4-6 mGy unenhanced phase• CTDIvol 8-12 mGy enhanced phases
Downloaded from sar2013.conferencespot.org

TCM: Adapt SD/NI to Slice Thickness
GE Lightspeed VCT
0
10
20
30
40
0 0,625 1,25 1,875 2,5 3,125 3,75 4,375 5
Slice Thickness
Nois
e In
dex
(HU)
NI2/NI1 =√ SW1/SW2
Downloaded from sar2013.conferencespot.org

Modern Contrast Injection
Single bolus – Nephrographic phase• Adapt CM volume to patient weight !• 120ml CM400 @ 3.0 ml/s in 75 kg
~ 1.6 ml/kg injected during 40s~ 640 mgI/kg injected during 40s~ Flux 0.04 ml/kg/s or 16 mgI/kg/s
• We use practical weight categories > e.g. 50-65, 65-80, 80-100, and more than
100kg
Keep TI constant
Downloaded from sar2013.conferencespot.org

Split-bolus Injection
Split bolus – Nephrographic phase• Larger 1st bolus for urographic phase• Bolus 1: 75ml CM400 @ 3.0 ml/s in 75 kg• Bolus 2: 45ml CM400 @ 3.0 ml/s in 75 kg
~ 1.0 / 0.6 ml/kg injected during 25 / 15s~ 400 / 240 mgI/kg injected during 25 / 15s~ Flux 0.04 / 0.04 ml/kg/s or 16 / 16
mgI/kg/s• Individualize interbolus delay with test injection
Keep TI for both boluses constant
Downloaded from sar2013.conferencespot.org

Associated Maneuvers• 0.1mg/kg furosemide – 3-5min before CM• 3D: Dilution – Distention – Distribution• Detection of most calculi in excretory phase• Shorter scan delay EP possible : 7-8 min
> Wide variation between patients: combine with test-images
• Saline iv bolus showed mixed results in ureter opacificationand distention
• We use 200ml iv bolus by power injector when furosemide is contra-indicated or unwanted
Kemper – Invest Rad 2005; Silverman – Rad 2006; Sanyal – Eur Rad 2007Downloaded from sar2013.conferencespot.org

Low-dose Test Images
• In routine CTU• Individualize excretory phase• Avoids non-opacified ureter • 4x4 to 4x6mm sequential – adds DLP 8-12 mGy cm• First test 2min before planned time EP• Needs adequate renal function bilaterally !• Easiest with 3P single bolus protocols
Nolte-Ernsting - Eur Radiol 2006Downloaded from sar2013.conferencespot.org

Unilateral Obstruction = Headache…..
• UPJ-stenosis, tumor or stone (partial) obstruction, etc.• Delay time of obstructed side much longer…..
• Good reason to perform US as initial step, even in high-risk patients: to steer CTU protocol
• 3P Single Bolus most flexibility> How to avoid high radiation-dose studies ??
• Separate protocol: 3P CTU in Unilateral Obstruction
Downloaded from sar2013.conferencespot.org
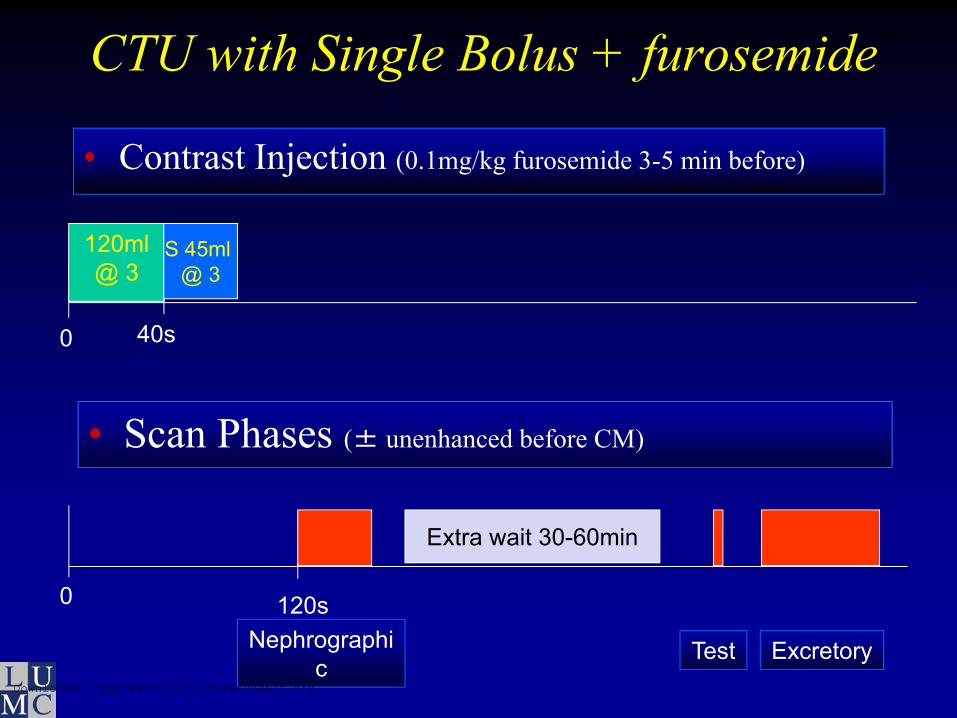
CTU with Single Bolus + furosemide
• Contrast Injection (0.1mg/kg furosemide 3-5 min before)
• Scan Phases (± unenhanced before CM)
0
0
120ml @ 3
40s
120sNephrographi
cExcretoryTest
S 45ml @ 3
Extra wait 30-60min
Downloaded from sar2013.conferencespot.org
Upper Tract UCC
• CTU appearance of UCC> Small or larger focal mass with hydroureter> Circumferential ureteric wall thickening> Luminal narrowing
• Small lesion better on EP axials with wide windows• Circumferential wall thickening better on transverse
or MPR
• Tiny upper tract UCC difficult to appreciate prospectively
Caoili AJR 2005Downloaded from sar2013.conferencespot.org
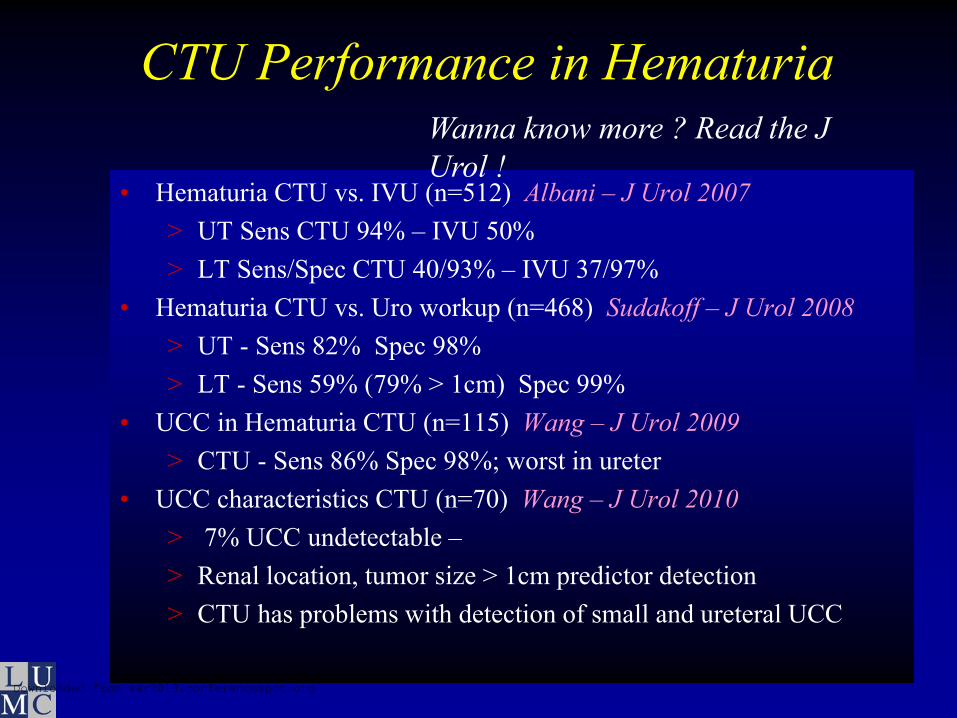
CTU Performance in Hematuria
• Hematuria CTU vs. IVU (n=512) Albani – J Urol 2007> UT Sens CTU 94% – IVU 50%> LT Sens/Spec CTU 40/93% – IVU 37/97%
• Hematuria CTU vs. Uro workup (n=468) Sudakoff – J Urol 2008> UT - Sens 82% Spec 98%> LT - Sens 59% (79% > 1cm) Spec 99%
• UCC in Hematuria CTU (n=115) Wang – J Urol 2009> CTU - Sens 86% Spec 98%; worst in ureter
• UCC characteristics CTU (n=70) Wang – J Urol 2010> 7% UCC undetectable –> Renal location, tumor size > 1cm predictor detection> CTU has problems with detection of small and ureteral UCC
Wanna know more ? Read the J Urol !
Downloaded from sar2013.conferencespot.org
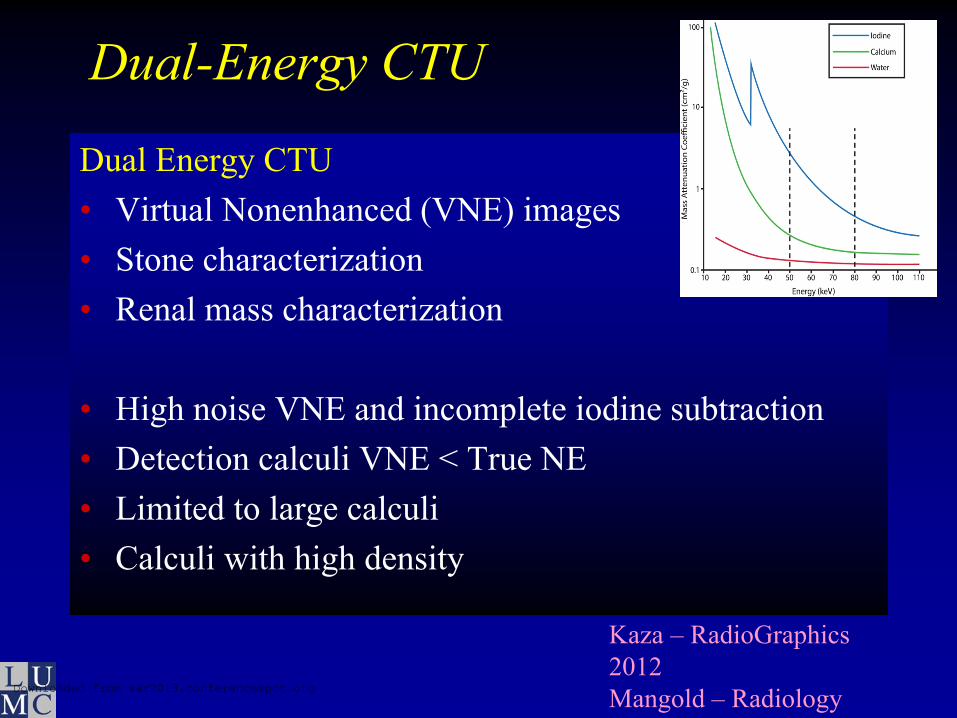
Dual-Energy CTU
Dual Energy CTU• Virtual Nonenhanced (VNE) images• Stone characterization• Renal mass characterization
• High noise VNE and incomplete iodine subtraction• Detection calculi VNE < True NE• Limited to large calculi• Calculi with high density
Kaza – RadioGraphics 2012Mangold – Radiology Downloaded from sar2013.conferencespot.org
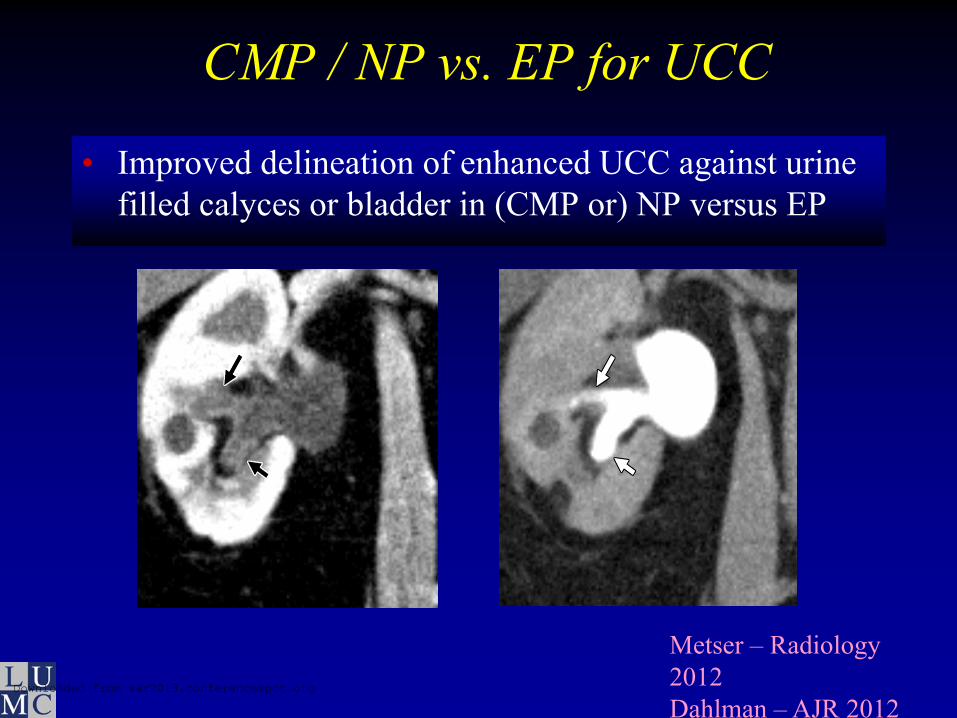
CMP / NP vs. EP for UCC
• Improved delineation of enhanced UCC against urine filled calyces or bladder in (CMP or) NP versus EP
Metser – Radiology 2012Dahlman – AJR 2012
Downloaded from sar2013.conferencespot.org
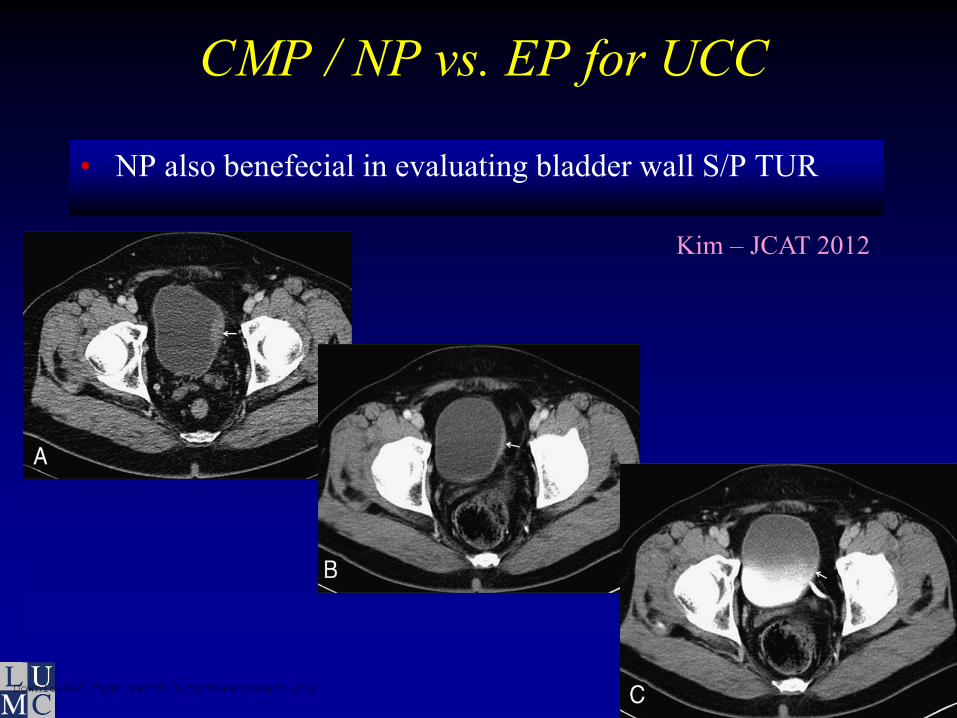
CMP / NP vs. EP for UCC
• NP also benefecial in evaluating bladder wall S/P TUR
Kim – JCAT 2012
Downloaded from sar2013.conferencespot.org

Incidental Findings CTU
• High rate incidental findings – up to 56%• Clinically important findings in 6.8%• Significant economic impact
• Look well for:> Inflammation GI tract> Inflammation pancreaticobiliary tract> AAA> Lung nodules
• Beneficial to have imaging of abdomen & pelvis in NP
Song - AJR 2012Bromage – BJR 2012
Downloaded from sar2013.conferencespot.org
New School 3-PhaseProtocol suggestion for high-risk hematuria:• Oral water & single-bolus CM 120ml (+ furosemide?)• TCM and Iterative Reconstruction• Unenhanced Phase – A
> More than 60% stones in renal locations• Nephrographic Phase – A & P
> Detection UCC and help & staging of LN and metspossible
• Excretory Phase – A & P> Optimised biphasic UT diagnosis UCC
• Optional: Delayed Excretory Phase 2 – P Prone> Optimised LT diagnosis UCC
Cowan, ECR 2012Downloaded from sar2013.conferencespot.org


















