Workload Measurement Instrument for Cancer...
62
YOUR P EER-R EVIEWED GUIDE TO GLOBAL C LINICAL T RIALS M ANAGEMENT appliedclinicaltrialsonline.com Volume 20 Number 1 Sites APPLIED CLINICAL TRIALS January 2011 Volume 20, Number 1 January 2011 INSIDE The Future of Obesity Drug Development SITES Reducing the Challenges of Study Coordination Workload Measurement Instrument for Cancer Trials Recruitment: African Americans in Clinical Trials Also in this issue 2011: A Challenge for the Biomedical Research Community? Joint Manifesto Tries to Address Vicious Cycle Discontent with IRBs R&D Success Rate Continues to Fall Complete contents on page 6 1992–2011 ACT 20 20 Y e a r o f S e r v i c e
Transcript of Workload Measurement Instrument for Cancer...

YOUR PEER-REVIEWED GUIDE TO GLOBAL CLINICAL TRIALS MANAGEMENT appliedclinicaltrialsonline.com
Volu
me 2
0 N
um
ber 1
S
ites A
PP
LIE
D C
LIN
ICA
L T
RIA
LS
Jan
ua
ry 20
11
Volume 20, Number 1 January 2011
INSID
E
The Future
of Obesity
Drug D
evelopment
➤ SITES
Reducing the Challenges of Study Coordination
Workload Measurement Instrument for Cancer Trials
Recruitment: African Americans in Clinical Trials
Also in this issue
■ 2011: A Challenge for the Biomedical Research Community?
■ Joint Manifesto Tries to Address Vicious Cycle
■ Discontent with IRBs
■ R&D Success Rate Continues to Fall
Complete contents on page 6
1992–2011
ACT
2020Year of Servi c
e

PAREXEL International
+1 781 487 9900
www.PAREXEL.com
Right where you need usPAREXEL knows scientific drug development from
end to end. We complement your capabilities with
our strategic insight, deep scientific knowledge, and
tactical expertise—providing you support and guidance
to secure strategic advantage.
With nearly 30 years of experience and 10,000
professionals in more than 50 countries, we provide
the precise fit of expertise when, where and
how you need it.
s�2EGULATORY�EXPERTISE�ACROSS�INTERNATIONAL�BOUNDARIES
s��0HASE�)n)6�CLINICAL�SERVICES�FOR�YOUR�INDICATION��
compound, and patient population
s��4ECHNOLOGY�ALIGNED�TO�ACCELERATE�DEVELOPMENT�
AND�MAXIMIZE�2/)
s��-ARKET�ACCESS�STRATEGY�AND�COMMUNICATIONS�TO�REACH�
your markets and achieve peak revenue quickly
DIA EuroMeeting 2011
Geneva, Switzerland
-ARCH����n���������
Clinical Trial Supply Europe
Barcelona, Spain
&EBRUARY����n���������
Look for PAREXEL at:


4 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
CLINICAL TRIALSAPPLIED
CLINICAL TRIALSAPPLIED
Editorial Offices485 Route 1 South, Building F, First Floor, Iselin, NJ 08830 USA
+1 (732) 346-3080 fax: +1 (732) 596-0003, www.appliedclinicaltrialsonline.com
EDITOR-IN-CHIEF Lisa Henderson, [email protected]
MANAGING EDITOR Timothy Denman, [email protected]
ASSISTANT EDITOR Kayda Norman, [email protected]
CORPORATE ART DIRECTOR Jerry Lehman, [email protected]
ART DIRECTOR Dan Ward, [email protected]
EUROPEAN EDITOR Philip Ward, [email protected]
PO Box 114, Deeside CH5 3ZA, UK +44 1244 538 583
WASHINGTON EDITOR Jill Wechsler
+1 (301) 656-4634 fax: +1 (301) 718-4377
Sales OfficesVP & GENERAL MANAGER PHARMA/SCIENCE GROUPS David C. Esola
PUBLISHER AND EUROPEAN SALES Wayne K. Blow
485 Route 1 South, Building F, First Floor, Iselin, NJ 08830 USA
+1 (732) 346-3021 fax: +1 (732) 596-0003
UK: +44 1925 732 797 fax: +44 1925 732 798, [email protected]
ADMINISTRATIVE ASSISTANT Daisy Roman-Torres
+1 (212) 951-6794 fax: +1 (212) 951-6604 [email protected]
WESTERN SALES MANAGER John Kiesewetter
PO Box 71275, Eugene, OR 97401 USA
+1 (541) 338-0022 fax: +1 (541) 338-0044, [email protected]
EAST COAST SALES EXECUTIVE Hope Corcoran
+1 (732) 346-3043 fax: +1 (732) 596-0003, [email protected]
ADVERTISING SALES COORDINATOR Joanne Capone
+1 (732) 346-3031 fax: +1 (732) 596-0012
ACT CHESTER UK OFFICE: +44 1244 393 100
Marketing ServicesCLASSIFIED DIRECTORY SALES & EMPLOYMENT OPPORTUNITIES ADVERTISING
Christine Kazimer
+1 (440) 891-2794 or +1 (800) 225-4569, ext. 2794
fax: +1 (440) 826-2865, [email protected]
AUDIENCE DEVELOPMENT MANAGER Wendy Bong
+1 (218) 740-7244, [email protected]
DIRECT MAIL LISTS Tamara Phillips
+1 (888) RENT-LIST (736-8547) ext. 2773, [email protected]
PERMISSIONS/INTERNATIONAL LICENSING Maureen Cannon
+1 (440) 891-2742 fax: +1 (440) 891-2650, [email protected]
REPRINTS +1 (800) 290-5460 ext. 100 or [email protected]
+1 (717) 505-9701 ext. 100 (outside USA)
SUBSCRIPTIONS +1 (888) 527-7008 (toll-free within USA)
+1 (218) 740-6477 (outside USA), [email protected]
BACK OR CURRENT ISSUES +1 (800) 598-6008, +1 (218) 740-6480 (outside USA)
Production OfficesPRODUCTION MANAGER Saravanan Mylsamy
Advanstar Communications, 131 W. 1st Street, Duluth, MN 55802 USA
+1 (218) 740-7259 fax: +1 (218) 740-7223. All color separations, proofs, and
film produced by Advanstar’s Scanning and Digital Prepress Departments.
President, Chief Executive Officer Joe Loggia Executive Vice President, Finance
& Chief Financial Officer Ted Alpert Executive Vice President, Corporate
Development Eric I. Lisman Vice President, Chief Technology Officer J. Vaughn
Vice President, Electronic Media Group Mike Alic Vice President, Media Operations
Francis Heid Vice President, Human Resources Nancy Nugent Vice President,
General Counsel Ward D. Hewins Executive Vice President, Healthcare & Pharma/
Science Group Steve Morris
Applied Clinical Trials does not verify any claims or other information appearing in any of
the advertisements contained in the publication, and cannot take any responsibility for
any losses or other damages incurred by readers in reliance on such content. ACT wel-
comes unsolicited articles, manuscripts, photographs, illustrations and other materials
but cannot be held responsible for their safekeeping or return.
Advanstar Communications provides certain customer contact data (such as customers’
names, addresses, phone numbers and email addresses) to third parties who wish to pro-
mote relevant products, services, and other opportunities which may be of interest to you.
If you do not want Advanstar Communications to make your contact information available
to third parties for marketing purposes, simply call toll-free 866-529-
2922 between the hours of 7:30 am and 5 pm CT and a customer
service representative will assist you in removing your name from
Advanstar’s lists. Outside the U.S., please phone 218-740-6395.
Over 18,250* BPA-qualifi ed
clinical trial professionals
around the globe are reading
Applied Clinical Trials…
WHY? Because ACT delivers over 18 years
of editorial excellence with the current
and high-quality content that clinical trial
professionals trust. By reading ACT, industry
professionals learn eff ective and effi cient
solutions to strategic and tactical challenges
within the tightly regulated, highly
competitive pharmaceutical environment.
FREE PRINT AND ONLINE SUBSCRIPTIONS
www.AppliedClinicalTrialsOnline.com
*BPA December 2009

Generate
Web traffic.
Encourage medication compliance.
Substantiate
label claims.
Gather market research.
Prove efficacy.Identify new
markets. Monitor
patient safety.
Engage patients.
Promote health awareness.
One Tool.
Unlimited Potential.
800-572-9394 z www.QualityMetric.com/onetool
What do you want to accomplish? QualityMetric’s multi-purpose SF health
surveys can help you achieve your goals at every stage of product development
and distribution.
Measure. Compare. Prove. These versatile, scientifically-valid tools provide
precise and reliable patient-reported data you can use throughout your product’s
life cycle to demonstrate comparative effectiveness, create marketing opportunities
and secure formulary approval.
Service. Service. Service. We’ll customize a survey to match your needs, and
we’ll provide survey scoring and expert analysis that can help you get to know your
markets—and the value of your product—like never before.
To learn how you can use a QualityMetric survey to meet the ever-growing
challenges created by increased competition, healthcare reform, and soaring
costs, contact Sheila Hetu today at 1-800-572-9394, ext. 274, or send an
email to [email protected].
Unleash the power of information with QualityMetric SF health surveys

6 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
A P P L I E D C L I N I C A L T R I A L S
O U R M I S S I O N
Applied Clinical Trials is the authoritative, peer-reviewed resource and thought leader for the global community that de-signs, initiates, manages, conducts, and monitors clinical trials. Industry professionals learn effective and efficient solutions to strategic and tactical challenges within the tightly regulated, highly competitive pharma ceutical environment.
COMMENTARY
10 From the EditorIns and Outs of Being Social
Lisa Henderson
19 View from WashingtonResearch Community Faces New Challenges
Jill Wechsler
22 View from BrusselsThe New Year Brings Same Old Battles
Peter O’Donnell
26 Clinical Trial InsightsFrustration with IRB Bureaucracy & DespotismKenneth A. Getz
58 A Closing ThoughtDeteriorating Quality in Global Trials
Jean-Pierre Tassignon
CLINICAL TRIALS COMMUNITY
14 News
51 Business and People Update
54 Calendar of Events
MARKETPLACE
56 Showcase
57 Marketplace
55 Advertiser Index
VOLUME 20, NUMBER 1
SITES
36 Workload Measurement
Instrument
Mary Coffey Julie Berridge, James Lyddiard, and Jacqueline Briggs
A better understanding of the
time, staff, and financial resources
required to conduct clinical trials
is necessary.
42 Increase African
American Enrollment
Patricia Sanders
Recession and acquisitions can
compromise the efforts to recruit
hard-to-reach American minorities.
COVER STORY
30 Collaborative Staffing Model for Multiple SitesMary E. Larkin, Paul McGuigan, Denise Richards, Karen Blumenthal, Kerry Milaszewski, Laurie Higgins, Jill Schanuel, and Christen Long
Strategies that may reduce the challenges of study coordination.


8 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
A P P L I E D C L I N I C A L T R I A L SEditorial Advisory Board
The expertise of Editorial Advisory Board members is essential to the
credibility and integrity of Applied Clinical Trials. These clinical trials experts
share with the editors the wisdom gained through their experience in many
areas of drug development. EAB members review manuscripts, suggest top-
ics for coverage, and advise the editors on industry issues. All manuscripts
must first be submitted to the Editor-in-Chief, Applied Clinical Trials, 485
Route 1 South, Building F, First Floor, Iselin, NJ 08830 USA.
Kiran Avancha, PhD, RPhClinical Research PharmacistUniversity of Miami Hospital and Clinics/Sylvester Comprehensive Cancer CenterMiami, FL
Aaron F. Bartlone, MSVice President& Head of Global QualityUCBBrussels, Belgium
Maarten Beekman, MDVice President, Medical & Regulatory AffairsAstraZeneca Zoetermeer, Netherlands
Paul Bleicher, MD, PhDChief Medical OfficerHumedicaBoston, MA
Timothy Callahan, PhDChief Scientific OfficerBiomedical SystemsSaint Louis, MO
Jo Collier, MBChB, FFPMMedical DirectorClinical Science and PharmacokineticsQuotient ClinicalNottingham, UK
Francis P. CrawleyExecutive DirectorGood Clinical PracticeAlliance–EuropeKessel-Lo, Belgium
Domenico Criscuolo, MD, PhD, FFPMChief Executive OfficerGenovaxColleretto Giacosa, Italy
Edward Stewart Geary, MDVice President& Global Safety OfficerEisai Co., Ltd.Tokyo, Japan
Uwe Gudat, MDMedical DirectorOffice of Chief Medical OfficerMerck SeronoGeneva, Switzerland
Felix Khin-Maung-GyiPharmD, MBA, CIPChief Executive OfficerChesapeake Research Review, Inc.Columbia, MD
Michael R. Hamrell, PhD, RACPresidentMORIAH ConsultantsYorba Linda, CA
Erica J. Heath, CIP, MBAPresidentEthical and Independent Review Services, LLCSan Anselmo, CA
Tim M. Jaeger, MD, PhD, MBAHead of Commercial Operations EMEA & LATAMSwisslab LIS SolutionsRoche Diagnostics Ltd./Swisslab GmbHBerlin, Germany
Brian J. Koziol, PhDDirector, Project Management& Strategic OperationsAmgen Inc.Thousand Oaks, CA
Patricia E. Koziol, PhDPresidentPEK Associates, Inc.Holmdel, NJ
Jeffrey S. Litwin, MDExecutive Vice President & Chief Medical OfficerERTPhiladelphia, PA
Somesh Nigam, PhDVice PresidentHealthcare InformaticsMedical Devices & DiagnosticsJohnson & JohnsonNew Brunswick, NJ
Timothy Pratt, PhD, MBAPrincipalCRUCIAL Clinical/Business ConsultantsMinneapolis, MN
Stanley C. RogersExecutive Vice PresidentSMHW Associates, LLCLawrenceville, NJ
Richard Rubin, MDDirectorThe Vermont Clinical Study CenterBurlington, VT
Stephen Senn, PhDProfessor of StatisticsDepartment of StatisticsThe University of GlasgowGlasgow, UK
Johanna Schenk, MD, FFPMSenior Partner& Managing DirectorPharmaProjekthaus GmbH & Co. KGFrankfurt, Germany
Albert J. Siemens, PhDChairmanNovella Clinical Inc.Research Triangle Park, NC
Thomas Sudhop, MDDirector and ProfessorFederal Institute for Drugsand Medical DevicesBonn, Germany
John R. Vogel, PhDDrug Development ConsultantJohn R. Vogel Associates, Inc.Kihei, HI
Glen de VriesPresident Medidata Solutions WorldwideNew York, NY
Right job, Right now...
Jobs i n the B i o te c hno l o gy ,
Pha rmac e u t i c a l and
Hea l thc a r e Indus t r y
Are you a clinical research specialist
looking for a new challenge?
Then look no further than
emedcareers.com.
As a member of the pioneering Jobsite
network, we have thousands of constantly
updated job opportunities available
online - and one of those could be
just right for you.
www.emedcareers.com

FIRST
ANYTIME. ANYWHERE.
It’s a global thing.
Medpace is the best choice for your
next study based upon peer-reviewed
excellence (number 1 rating by
investigative sites), our strategic
integration across the globe, experience
in accelerating patient recruitment, and
our unparalleled ability to manage large
concurrent trials.
Medpace. A world of amazing
results right in your hands.
HAND EXPERTISE.
North America Europe South America Asia-Pacific Middle East Africamedpace.com/firsthand

10 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
Lisa Henderson
Editor-in-Chief
email: [email protected]
www.appliedclinicaltrialsonline.com
From the Editor
Just like any technology, big
purchase, or business need, there
has to be a benefit for you to sign on.
For better or worse, websites make it
easier for people to be out there and
have information more accessible.
The better? Humorous rants from Dr.
Grumpy’s blog spot, and movie ratings
with detailed reasons behind the PG-13.
The worse? Bullying on Facebook.
I’m what is technically termed, a
late majority technology adopter. The
iPhone was introduced January 9, 2007.
I bought my iPhone 3G in March 2010. I
love it. But I wasn’t convinced for a long
time. I prefer others to go forward and
try the technology, then let me know
what the best uses are.
Social media, the same thing. I’m
on Facebook, I understand the value,
but I keep my family life and work life
separate. I love my Mom, but the photo
of her cat isn’t really what I want under
my name and photo in all seriousness
as the editor of Applied Clinical Trials.
Others I have talked to about this
agreed and said that’s why they prefer
LinkedIn; it’s more professionally-
oriented. I have a LinkedIn account
also, but my activity level is low.
Twitter? For my personal life, no.
But for Applied Clinical Trials, the time
is right to start tweeting. The editors
are going to tweet what they read, and
what they observe. I am in the enviable
position of following and staying
abreast of the developments in a very
interesting industry. So why not share
what I find out? Find our insights
@trialsonline.
More for 2011 So while some of us struggle with the
importance of social media in general,
for our company, we are definitely
getting the hang of the best uses of this
medium for our online audiences and
how they can benefit.
The most interesting development
is a “social media” website that is
dedicated to one segment of the
industry. Don’t let the terminology fool
you. This is a very exciting project and
I don’t want to give all the details away
before it’s time. Suffice to say, bringing
together people who share a similar
interest and passion into a professional
online meeting place can provide the
true dialogue that our audiences seek.
2011 represents 20 years that Applied
Clinical Trials has been bringing people
together in the pages of the magazine.
We certainly have a successful
reputation and we think the time is right
to bring the audience closer together
in forums that will make positive
differences to your work life. We hope
you will join us.
For the socially stretched, look for real uses of social media that will make a difference to your work life.
In September, Psychology Today published an article “Revenge
of the Introvert.” The article noted that introverts and extraverts
are equally divided in the population, but introverts process
information and stimulus quite differently from extraverts. Introverts
are not shy, rather they just need more alone and quiet time. There
are millions on Facebook and maybe equally as many who could
care less about Facebook, and I wondered if this is in fact related.
Are introverts naturally—by predisposition—going to shun the
online party just like a real-life one? Social in and of itself can mean
extravert. Maybe social media is overwhelming for the introverts? The
choice is related to benefit and how best to use the information.
Ins and Outs of Being Social

Coonsoidlteadltd
Coaoiclilpereint
Proeucd coovergenct
© 2010 Perceptive Informatics, Inc. A PAREXEL® Company.iPad is a trademark of Apple Inc.
Tell us your demands!What do you demand from your
clinical trial technology solutions?
Go to www.perceptive.com and
enter your demands for a chance
to win an Apple iPad!
Ttoies
uoerdemlnys!
Meeting your demands3HUFHSWLYH¶V�H&OLQLFDO�6XLWHWhy put up with having to switch between applications, interrupting
natural user workflow?
It’s time to demand Perceptive’s eClinical Suite – we are making use of multiple technologies simpler for our end users. Our unique product convergence enables randomization and dispensation directly from within our DataLabs EDC solution without logging into IVR/IWR. All powered by proven robust eClinical platforms and deep life sciences expertise.
To discover how Perceptive can meet your demands, visit www.perceptive.com/eclinical or contact us at [email protected].

12 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
appliedclinicaltrialsonline.com
N O T E W O R T H Y
Go to:
appliedclinicaltrialsonline.com
to access these exclusive stories
and other featured content.
Biosimilars FDA UpdateA podcast interview with William
Egan, PhD, VP, and Jeffrey
Freitag, MD, SVP, PharmaNet
Consulting, provides a first-
hand update on the FDAs public
hearing on regulations for the
approval of generic versions of
biological products and what the
sponsor community can expect
moving forward.
Lönngren on EMAWilliam Looney, Editor-in-Chief
of Pharmaceutical Executive,
provides an excerpted interview
with Thomas Lönngren, depart-
ing EMA Executive Director, in a
December blog post.
Emerging Disease PathwaysPharmaFaceoff.com features a
recorded panel discussion on the
challenges related to drugs get-
ting to market. Specifically on the
table were complex trials, includ-
ing the need for more biomarkers
and upticks in personalized medi-
cine; increased regulatory hurdles
for pharmaceutical sponsors; and
outsourcing issues. Watch the dis-
cussion and leave your comments.
Competitive PressuresA September 2010 Wall Street Journal article outlined pressures among CROs,
specifically the mid-sized ones, that are advised to find better strategies to stay
competitive. While those same CROs will unofficially admit only that they are
large CROs, our informal sampling poll found more than half of the respondents
believe that mid-size CROs are being squeezed.
Synergy Research Group (SynRG),
a Russia-based CRO, released its
SynRG Orange Paper Q3 2010, a
quarterly analytical report on the clini-
cal trial market in Russia. The follow-
ing highlights are from the report.
The RZN approved 134 new clini-
cal trials of all types including local
and bioequivalence studies in the third
quarter of 2010—a 12% decrease com-
pared to last year’s figure.
The main contribution to the to-
tal number of studies is still made by
multinational, multicenter clinical tri-
als, even though the number of these
studies decreased by one third over Q3
2009 and stood at 60 new studies in Q3
2010. The number of local clinical trials
conducted in Russia by domestic and
foreign sponsors had a 7% increase and
stood at 42 trials.
Although most clinical trials in Rus-
sia are still being sponsored by for-
eign companies (57%), the ratio be-
tween foreign and domestic companies
changed significantly: in Q3 2009 their
shares were 67% and 33% respectively,
while in Q3 2010 the share of trials
sponsored by domestic companies in-
creased to 43%.
Clinical trials initiated in Q3 2010
were sponsored by manufacturers
from 17 countries. The largest num-
ber of trials were initiated by Russian
sponsors, American sponsors took the
runner-up place, followed by German
and Swiss sponsors.
Twelve new Phase I clinical tri -
als were launched in Q3 2010; while
the number of the Phase II trials de-
creased from 47 trials in Q3 2009 to 18
in the Q3 2010. The number of Phase
III trials also decreased over last year,
down from 86 to 61 studies, while the
number of Phase IV studies remained
unchanged at 10 new trials.
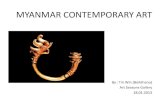
Is the mid-size CRO being squeezed by smaller specialty CROs and large CROs?
Yes54%
25%
21%
No
Not sure
Source: appliedclinicaltrialsonline.com survey, 12/06/10-12/20/10

Formerly known as PharmaLinkFHI, Novella Clinical is created from the combined strengths
of PharmaLinkFHI, Matrix Clinical and eReady Monitors.
1X^_WPa\P�3TeT[^_\T]c�����<TSXRP[�3TeXRT�3TeT[^_\T]c�����2[X]XRP[�ATb^daRX]V
6[^QP[�7TPS`dPacTab)�AC?��=2��DB0��k��?W^]T�( (�#'#� (! �
4da^_TP]�>_TaPcX^]b)�BcTeT]PVT��D:��k��?W^]T��##���� #"'�!! !!
You see beyond the clinical trial. Your ultimate goal is to give people a better quality of life and more
opportunities to enjoy those special little moments, like blowing bubbles in the backyard or catching
fireflies. We’re proud to be a part of your mission. Our promise is to give your clinical program
the individual attention it deserves, combined with therapeutic and in-country expertise to help you
achieve your goal. We are Novella Clinical. Moving Potential. Forward. www.novellaclinical.com

14 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
News
T H E R A P E U T I C C O R N E R
With New Year’s resolutions
still fresh in the mind, many
may have put “lose weight”
at the top of their list. Along with
gym enrollments, those who are very
overweight may have hoped to add
a prescription medication to their
regimen. However, what started out
in 2010 as potential new therapies
for obesity has turned into a murky
future for drug development in
this area. Sponsors with potential
therapies at the starting gate were
derailed by safety issues and even
an already approved and marketed
drug—Meridia in the United States—
has been pulled voluntarily by its
manufacturer, or forced out by global
regulatory authorities.
In January 2010, the EMA sus-
pended the marketing authorization
for sibutramine, known as Reductil,
Reduxade, and Zelium, across the
EU. This was based on the results of
a European postmarket request for a
cardiovascular outcome study due to
concerns raised in the clinical trial
data. The FDA then evaluated and
met on the SCOUT data in September,
and asked Abbott Laboratories to vol-
untarily withdrawal Meridia from the
market on October 8. In mid-Novem-
ber, India’s regulatory authority, the
Drugs Controller General of India, fol-
lowed suit and suspended formulations
related to sibutramine and r-sibutra-
mine imports and manufacturing.
Paul Aftring, VP and Global Head,
Endocrine and Metabolic Disorders at
i3, told Applied Clinical Trials that the
current climate for obesity drugs is
“difficult to say the least.” The reasons
why are directly related to these vari-
ous cardiovascular safety issues. How-
ever, when it comes to recruitment,
potential participants aren’t turning
away from clinical studies, even with
the historical cardiovascular events
related to these drugs.
“The condition is extraordinarily
prevalent,” said Aftring. “Finding sub-
jects to participate is easy.” Where the
trial becomes challenging is in subject
retention and global trials issues.
Retention and engagement“Obesity specialists are well aware
that this is a population that is hard
to keep engaged,” explained Aftring.
Much like any other weight-loss ap-
proach, if there is limited or slow suc-
cess, the person will lose interest. But
in a clinical trial, participation to the
end of the trial is required for the data
and the control group.
Aftring suggests using small re-
wards such as pedometers, which can
monitor activities even after the trial
is over, or cookbooks that can help
with diet. “You have to make sure you
aren’t creating undue influence,” said
Aftring, “but these types of things
can be used.” But outside of useful
tokens, what else can be done for the
obese subject?
Since not all investigators will be
obesity specialists, there is a need
to educate the site staff on engage-
ment and retention. Engagement can
come in the form of follow-up phone
calls, compliance to the study, and
encouragement on achievements, no
matter how small they are. There will
be weight loss achievements because
all subjects in an obesity clinical trial
will still be required to comply with the
standard of care, which is diet and ex-
ercise. Specifically, these trials call for
all subjects to limit their dietary fat to
30 percent. The difference, of course,
is some will be on placebo and others
on the experimental agent.
In order for the data to be measur-
able across a global trial in obesity,
however, is where conduct can become
complex. How does a measurement
becoming equalized when a subject is
instructed to take the agent before a
meal— members of one culture might
eat a number of small meals during
the day, and a large meal at night,
while another culture might feature
three large meals per day. “The chal-
lenge is how to get consistent results,”
said Aftring. “There are local nuances
that need to be addressed.” i3 wrote
and posted an article to its website
at www.i3global.com/spotlight/spot-
light03232010 that discusses these
global issues in detail, from variability
in diet and exercise to developing
those educational materials involved
across cultures.
With the challenges of a negative
risk-benefit ratio surrounding obesity
drugs due to increased cardiovascular
events, future development may lie
in the comorbid conditions in cardio-
vascular disease and type II diabetes.
Industry experts predict a dearth of
drugs for obesity, a similar 10-year
span that occurred with the fen-phen
safety issues in the 1990s. Aftring
notes there is much more activity on
the diabetes side of the endocrine
equation. In the end, it may be that
sponsors will focus on testing diabe-
tes drugs with better risk profiles, or
working toward obesity drugs that
have a novel mechanism. However,
trial managers can take the aforemen-
tioned advice from Aftring for cultural
nuances in a global trial. Applying
local and cultural norms in any trial is
necessary, as well as retention and en-
gagement strategies. These will not be
lost in current or future diabetes and
related trials.
Obesity Wins One, but Rest of Field Uncertain

W
W
&HWHUR�5HVHDUFK is the industry’s leading early phase CRO
specializing in full-service clinical pharmacology, bioanalytical
and scientifi c affairs. You can count on the people behind our
services. Our scientists and medical staff have unmatched
knowledge and experience to provide accurate, reliable data.
Cetero develops practical approaches specifi cally designed
to accommodate your research needs and accelerate your
drug-development process.
We have a proven track record of delivering accurate data
when you want it, in a format you want, with an unwavering
commitment to quality.
877.7CETERO [email protected] www.cetero.com/act
our therapeutic focus
Allergy
Asthma
Dermatology
Diabetes

16 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
News
G L O B A L N E W S
GCP training will come under
the spotlight at the start of
February, when the European
Forum for GCP’s annual congress
takes place in Budapest, Hungary.
The two-day meeting will bring
together experts from a range of
clinical trial disciplines to discuss the
needs of the key players. The organiz-
ers’ prime aims are to exchange na-
tional and organizational experiences
and to devise constructive proposals
for meeting GCP training needs.
“Although the European Commis-
sion has established a comprehensive
regulatory package to ensure that
GCP principles apply to the conduct
of clinical trials within Europe, it is
very apparent that the practical imple-
mentation of this regulatory package
differs between member states,” state
the organizers.
Training must be appropriate for
each partner, whether it is an industry
or academic sponsor, ethics commit-
tee, competent authority, or investiga-
tor. This training is often inadequate,
inconsistent, and too theoretical. This
has to be addressed, as does the need
to ensure that patients and the public
are more aware of the benefits and
risks of taking part in studies involv-
ing the use of rigorous standards, ac-
cording to officers from the EFGCP.
Two important initiatives being con-
sidered by EFGCP are the creation of
a common curriculum and provision
of certification and accreditation. The
keynote address from Jean-Pierre
Tassignon, MD, PhD, President of
Crossover CRI (Zug, Switzerland),
will ask whether harmonized training
standards are really necessary.
The event, called “Certified GCP
Training—Needs and Solutions,”
is being held February 1- 2, and is
supported by the
Hungarian Clinical
Trial Management
Society. Its seven
workshops will ad-
dress e-GCP train-
ing, how to teach
clinical research to
medical students,
training of experi-
enced investigators
and responsibilities
for training their
teams, the suit-
ability of SOPs
as training tools,
how to train risk-
benefit assessment
in rare diseases,
the contribution of
patients in ethics
committees, and
special training for
research involving
older people and
geriatric patients.
The conference
will also include an
update on the Pa-
tientPartner project
to be given by Cor
Oosterwijk, PhD,
from The Neth-
erlands. PatientPartner is a three-
year European Union FP7 (Seventh
Framework Program) project investi-
gating, enforcing, and advising on the
role of patient organizations in clini-
cal trials (www.patientpartner-eu-
rope.eu). Its main goals are to make
inventories of the needs of patient
organizations; to identify and realize
common points of action amongst all
stakeholders by engaging in an ac-
tive dialogue; to realize the European
Network of Patients Partnering in
Clinical Research (ENPCR); to create
a European network for interaction
with the other stakeholders in the
clinical trial field; and to create Eu-
ropean, patient-centred guiding tools
and recommendations on how to cre-
ate a successful partnership.
PatientPartner organized a training
workshop in Brussels on December
7-8, 2010, and in his Budapest presen-
tation, Oosterwijk will present details
about the results of the workshop.
—Philip Ward
EFGCP to Establish Changes in GCP Training
LIV
IO S
INIB
ALD
I/G
ET
TY
IM
AG
ES
The European Forum for GCP’s annual congress will take place in Budapest, Hungary.

2010 Good Clinical Practice:
A Question & Answer Reference GuideNEWFor CRs, investigators/sites, auditors, compliance, legal, and other clinical professionals
What’s new for 2010:
60+ pages of all-new Q&As, including questions addressing emerging topics such Zas the use of social media in clinical trials, and the implications of IRB reviews of social media content used for patient recruitment.
A new chapter featuring exclusive interviews with Leslie Ball, M.D., director Zof CDER’s Division of Scientific Investigations (DSI), and Joanne Less, M.D., director of FDA’s Good Clinical Practice Program on the priorities and direction of the FDA’s GCP enforcement programs.
Completely new and updated section featuring all the latest data and trends on the ZFDA’s clinical trial compliance inspections, inspectional findings, and common areas of GCP noncompliance.
200+ Q&As updated to reflect the very latest FDA guidances, regulations, Zcomments, and developments
While continuing with a U.S./FDA focus, this innovative reference guide has now been expanded to provide even more information on not just US GCP, but international GCP issues in such regions and countries as the European Union, India, Latin America and Russia! Find out for yourself why more and more leading pharma and biotech companies are using this reference guide to educate their clinical professionals, trial auditors, and site staff on the many emerging complexities of GCP standards.
With the completely updated and expanded 2010 guide, read how the FDA will now be focusing more intently on sponsors’ “quality systems” when significant problems are discovered at clinical study site, why the rate of significant non-compliance is being discovered at clinical trial sites, and how increasing numbers of new drug reviews are being delayed due to GCP compliance issues.
In one pocket handbook, you’ll have authoritative answers to
hundreds of common and emerging questions, in 20+ GCP-related
areas, right at your fingertips:
FDA and ICH GCP Standards for r�Clinical Research Form FDA 1572-Statement of r�Investigator Informed Consent r�Patient Recruitment r�State Standards and GCP r�Source Data/Documentation r�Investigator/Site Requirements r�Clinical Monitoring r�Clinical Study Safety Reporting r� Clinical Trial Protocols/Protocol r�Changes/Protocol Violations
Institutional Review Boards r� Quality Assurance Activities/Study r�Auditing/FDA Inspections Investigational Drug Accountability, r�Administration, and Labeling r� Now includes a new section on GCP r�in Latin America! Also provides all FDA, ICH, and EU r�GCP-related regulations and guidances in one source!
Barnett International: A division of Cambridge Healthtech Institute,
����'JSTU�"WFOVF�t�4VJUF�����t�/FFEIBN �."�������64"�t�1IPOF��������������
For more information, and
to place your pre-order
today please visit:BarnetInternational.com/Publications
Or Contact:Elizabeth Andrews
Account Manager
Barnet Educational Services
Phone: 781-972-5418
Email: [email protected]
www.barnettinternational.com

18 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
News
L E T T E R T O T H E E D I T O R
D A T A A N A LY S I S
In the November 2010 issue of
Applied Clinical Trials, Viq Pervaaz
said “the pharmaceutical industry
has been ripe with merger and
acquisition activity for the last several
years.” As a tool in this economically
challenged period, M&A transactions
can make the difference between
a positive financial year and one
that is not. Recently, a clever way to
achieve a strong end of year finish
is via growth, competitive edge, and
M&A transactions. Acquisition in this
economic environment is a great option
to explore. However, for a cohesive,
seamless merger, it will take work and
planning, before, during, and after the
deal sheet is signed. Both sides must be
guided, informed, and M&A-ready. To
achieve a successful M&A, preparation
is necessary: understanding the
transaction, strategy alignment, and
utilization of success metrics specific to
the type of M&A is a great beginning.
Recently I was approached by
pharma to assess, manage, and
implement a more centralized, M&A-
ready clinical/regulatory approach
to “a combined” pipeline. With the
addition of a promising new pipeline,
clinical/regulatory operations
expanded considerably and rapidly;
overnight, fragmentation resulted. The
fragmentation generated operational
inefficiencies, lost timelines, increased
costs, and eventually lethargic worker
performance. Management lacked a
realistic view of what was expected of
them. Pre-existing business models did
not apply, quality was lost, and deadlines
were sacrificed in the expansion.
Gaps and stumbling blocks in each
pharma company are identified and
worked through to improve operations,
process, and quality standards. Data
and documentation audits focused on
short and long-term objectives, should
outline best practices.
How can this be accomplished?
Opportunities for improvement are
assessed and changes implemented.
The implementation plan is agreed
upon by all functions, all teams,
all CROs. An implementation
project planner, “a gate-keeper”
is developed to clearly execute
prioritized recommendations.
Bridging the gap between corporate
leaders and operational staff, team,
and functions is the main key to
improvement. Communicate and
monitor progress. Manage the
issues pertaining to resource and
capacity. Lead people with clear,
concise, well communicated vision
and realistic expectations. Nothing
is insurmountable when assessed,
planned, implemented, tracked, and
monitored prior to, during, and after
the M&A transaction. Lead people,
manage issues. Communicate.
Diane L. Mauriello, PhD
President
Dante Resources, Inc.
Throughout the entire
clinical development, who
has the most interaction
with prospective and active
subjects? Who is primarily
responsible for the quality of
the source data that ultimately
decides the approvability of all
biopharmaceutical products?
Yes, the answers are identical:
the site coordinator, study
coordinator, or clinical research
coordinator, whatever title you
choose. These individuals are
the keystone, the glue that holds
the study process together.
Without them very few patients would
be randomized, informed consent
forms would not be completed, site
contracts would not be negotiated,
data would not be entered, queries
would not get resolved, and database
lock would be delayed.
Delay is the key point. Site
coordinators help a study stay on
track. Without good ones, hitting
milestones would be nearly impossible.
ISR dedicated an entire study
(The Voice of the Site Coordinator—
www.isrreports.com/reports) to
understanding site coordinator’s
experiences and perspectives on
improving the success of clinical trials.
—Industry Standard Research
Site Coordinators: An Untapped Resource
Achieving a Successful M&A
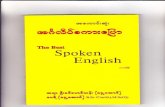
51%
28%22%
SiteCoordinators
PrincipalInvestigators
Subjects
Source: Industry Standard Research
Principal investigators were asked who satisfaction surveys should focus on during a study. Site Coordinators were named more than half the time, ahead of PIs themselves.

This vaccine is being developed to help
patients on the other side of the world.
How do you plan on getting it there?
Over 30 years of experience differentiates
Marken as a leading Life Science Logistics
Specialist.
t� 96 Scientists
t� 524 Researchers
t� 2689 Patients
t� 4 years in development
t� Over $600 million invested

Marken delivers decades of experience
and regional expertise in extending
the reach of Life Science.
LATIN AMERICA
MARKEN ARGENTINA
Tel: +54 11 4509 6070
Fax: +54 11 4942 9752
Email:[email protected]
MARKEN MEXICO
Tel: +52 55-2643-7893
Fax: +52 55-2643-7892
Email: [email protected]
MARKEN BRAZIL
Tel/Fax: +55 115584-6203
Email: [email protected]
ASIA
MARKEN BEIJING
Tel: +86 10 6462 6318
Fax: +86 10 8448 9768
Email: [email protected]
MARKEN HONG KONG
Tel: +852 2237 0323
Fax: +852 2237 0662
Email: [email protected]
MARKEN JAPAN
Tel: +81 (0) 3 5640 3056
Fax: +81 (0) 3 5460 3059
Email: [email protected]
MARKEN SINGAPORE
Tel: +65 6545 2636
Fax: +65 6743 8343
Email: [email protected]
MARKEN MUMBAI
Tel: +91 22 4236 5800
Fax: +91 22 2857 7905
Email: [email protected]
NORTH AMERICA
MARKEN LOS ANGELES
Tel: +1 310 641 8393
Fax: +1 310 641 8396
Email: [email protected]
MARKEN NEW YORK
Toll Free: +1 800 932 6755
Direct Dial: +1 516 307 3287
Fax: +1 516 307 3284
Email: [email protected]
MARKEN MIAMI
Tel: +1 305 500 9288
Fax: +1 305 500 9117
Email: [email protected]
MARKEN SAN FRANCISCO
Tel: +1 650 266 9950
Fax: +1 650.583.8952
Email: [email protected]
AFRICAMARKEN JOHANNESBURG
Tel: +27 11 974 9798
Fax: +27 11 974 3268
Email: [email protected]
EUROPE
MARKEN BRUSSELS
Tel: +32 2 718 0820
Fax: +32 2 718 0825
Email: [email protected]
MARKEN FRANKFURT
Tel.: +49 6102 798 75-0
Fax: +49 6102 798 75-10
Email: [email protected]
MARKEN MILAN
Tel: +39 02 2695 0198
Fax: +39 02 2695 3471
Email: [email protected]
MARKEN STOCKHOLM
Tel: +46 8 594 41420
Fax: +46 8 594 41426
Email: [email protected]
MARKEN EDINBURGH
Tel: +44 131 333 4012
Fax: +44 131 335 6847
Email: [email protected]
MARKEN HAMBURG
Tel: +49 40 8405800
Fax: +49 40 84058014
Email: [email protected]
MARKEN LONDON
Tel: +44 208 388 8555
Fax: +44 208 388 8666
Email: [email protected]
MARKEN PARIS
Tel: +33 1 5697 5697
Fax: +33 1 5697 5699
Email: [email protected]
MARKEN ZURICH
Tel: +41 43 816 58 11
Fax: +41 43 816 58 66
Email: [email protected]
OCEANIA
MARKEN SYDNEY
Tel: +61 (0)2 9318 1777
Fax: +61 (0)2 9319 1700
Toll free: +1 800 627 533
Email: [email protected]

appliedclinicaltrialsonline.com APPLIED CLINICAL TRIALS 19January 2011
To see more View from Washington articles, visit
appliedclinicaltrialsonline.com
View from Washington
Jill Wechsler
is the Washington editor
of Applied Clinical Trials,
(301) 656-4634
Research Community Faces New ChallengesNew user fees, health initiatives, and FDA compliance concerns are top issues for 2011.
The tension is mounting on
Capitol Hill, as Republicans
seek to cut the federal deficit by
squeezing resources for govern-
ment agencies, including the Food and
Drug Administration and the National
Institutes of Health. They’re looking for
opportunities to criticize lax regulatory
oversight that compromises product
and patient safety. Challenges to the
Obama administration’s health reform
program will create uncertainties for
biopharmaceutical companies about
whether new fees and policies will be
implemented as planned, or if industry
will have to pay stiffer rebates and
taxes without gaining the millions of
additional customers promised cover-
age under a reformed health insurance
system. Pressure on federal agencies to
obtain additional revenues, moreover,
will intensify government efforts to hit
violative companies with stiff fines and
to ratchet up user fees from industry.
Fees firstThe Prescription Drug User Fee Act
(PDUFA) has to be reauthorized by
October 1, 2012, for FDA to continue
collecting nearly $700 million in fees to
support the review process for drugs
and biologics. Although that legisla-
tive deadline may seem far away, FDA
wants to have a PDUFA V plan ready
for public review by fall in order to
transmit it to Congress early 2012;
failure to reauthorize user fees by next
summer theoretically would force FDA
to lay off hundreds of staffers and shut
down its drug review process.
Last April, FDA’s Center for Drug
Evaluation and Research (CDER)
launched a two-year process for revising
PDUFA. CDER Director Janet Wood-
cock noted that 65 percent of human
drug review funding comes from user
fees, a situation that some critics claim
makes the agency overly dependent on
industry. Yet, despite such qualms, no
one suggests that FDA curtail any activi-
ties or cancel the fee program.
Pharma and biotech companies of-
fered general support for user fees,
while pointing out that multiple post-
marketing requirements are slowing
down the drug review process and
undermining approval time frames.
Patient advocates, pharmacists, and
doctors agreed that the proliferation of
risk evaluation and mitigation strategies
(REMS) made drug development more
costly and complicated prescribing and
dispensing. Consumer groups focused
more on direct-to-consumer drug adver-
tising, seeking user fee support for man-
datory pre-review of DTC ads, clearer
prescribing information, better protec-
tion of patients in clinical trials, and full
disclosure of clinical trial results.
FDA has been discussing these and
other issues at meetings with manufac-
turers, patient and consumer groups,
and healthcare professionals and
academic experts, as part of a broad,
transparent consultative process re-
quired by the FDA Amendments Act
(FDAAA) of 2007. A main FDA goal
for PDUFA V is to gain more flexibility
in meeting review time frames and re-
sponding to sponsor meeting requests.
The agency has proposed to extend the
review clock for more complex applica-
tions, such as those with REMS, that
require advisory committee meetings,
or that involve inspections of foreign
manufacturing facilities—but that ap-
pears to cover most NDAs.
The overarching issue is to what
extent industry fees should fund FDA
initiatives to improve drug development
and regulatory science. FDA proposes
to tap fee revenues to increase staff
consultations on innovative clinical trial
designs, on utilizing biomarkers in drug
development, on complex manufacturing
issues, and to standardize electronic sub-
missions. The agency also seeks added
resources to support the Sentinel Active
Surveillance System, standards for meta-
analysis, rare disease programs, and
improved dose selection and safety as-
sessments. But this year’s fee to process
a new drug application (NDA) with clini-
cal data already exceeds $1.5 million, up
from $1.17 million in 2008, and sponsors
are wary that expanding the pool of
activities supported by PDUFA would
boost fees disproportionately.
Congress will address many of these
issues as it crafts a broader FDA re-
form bill to carry the PDUFA reautho-
rization. As with FDAAA, this “must-
pass” legislation is a prime candidate
to establish a host of new FDA policies
and programs: curbs on drug advertis-
ing, expanded drug reimportation,
refining the REMS program, requiring
new drugs to demonstrate compara-
tive superiority, and enhancing FDA
authority to pull drugs off the market
and to issue subpoenas, to name a few.
An FDA reform bill also may authorize
the collection of user fees for generic
drugs, an issue that has been discussed
for years and now has industry support.

View from Washington
Biosimilars and CER
Another important FDA initiative is to
establish standards and policies govern-
ing the development and approval of
“similar” versions of biotech therapies.
Patient and consumer groups and health
plans and payers are pressing for a clear
biosimilar development pathway to fa-
cilitate access to less costly therapies, a
goal that will be increasingly important
as more biologics come on the market.
FDA held a two-day public meeting in
November to launch the process for
establishing a framework for developing
biosimilars, as stipulated by the Afford-
able Care Act enacted last March 2010.
A long list of brand and generic drug
manufacturers testified on the scope
and size of preclinical and clinical tests
and data needed to document the safety
and efficacy of such products, and FDA
will be digesting these and other com-
ments over the coming months. FDA
officials appeared interested in identify-
ing a middle ground between ensuring
product safety and efficacy, and making
affordable new treatments available to
patients. However, Commissioner Ham-
burg indicated at a later meeting that a
complete approval pathway for biosimi-
lars may be elusive, as the science and
products will evolve continuously.
The health reform legislation also
expanded federal support for compara-
tive effectiveness research (CER), and
that initiative will begin to take shape
in the coming year. The governing
board for the Patient-Centered Out-
comes Research Institute (PCORI)
held its first meeting in November
where it adopted bylaws and explored
operating procedures. Its first tasks
are to hire an executive director and
staff, develop a communications plan,
and map how the strategy will work
with its Methodology Committee.
Before PCORI awards grants for
new CER projects, the Board wants
to assess what research and analysis
already is going on in this field and
where there are information gaps to fill.
The Department for Health and Human
Services (HHS), NIH, and the Agency
for Healthcare Research and Quality
have dispersed $1.1 billion for CER
projects over the last two years, and
most of these initiatives are up and run-
ning. PCORI’s “environmental scan”
could benefit from a planned HHS
initiative to establish an online CER
Healthcare fraud and abuse is a prime target as authorities look hard at all opportunities to save money and generate revenues.
© 2010 Perceptive Informatics, Inc. A PAREXEL® Company.
PsssssHave you discovered DataLabs, the
More top 20 global pharmaceutical
companies have used DataLabs than you think!
To find out what you’re missing, visit www.perceptive.com/edc

catalog, and from a database of feder-
ally funded CER projects being created
by the Partnership to Improve Patient
Care. The Board also would like to
review state and private CER initiatives
to better identify early projects that can
increase general understanding of CER
and further illuminate PCORI’s role.
Costs drive complianceBy steering patients and providers to
the most effective treatments, CER
advocates hope to improve healthcare
quality, while also reducing spending
on medical services and products. With
healthcare consuming an ever-growing
portion of federal and state budgets,
authorities are looking hard at all op-
portunities to save money and generate
revenues, and healthcare fraud and
abuse is a prime target. The Justice
Department announced in November
that it recouped $3 billion in civil settle-
ments and judgments last year, much
of it from pharmaceutical companies.
At the top of the list is Pfizer’s $2.3
billion settlement for promoting unap-
proved drug uses; Astra Zeneca agreed
to a $302 million civil settlement and
Novartis paid $193 million. FDA also
has been stepping up actions against in-
vestigators and research organizations
that violate the rules.
There’s no sign of any letup as
extensive pharma layoffs promise to
encourage more dismissed workers to
blow the whistle on corporate malfea-
sance. In October, GlaxoSmithKline
agreed to a $750 million settlement,
and Merck negotiated a $950 million
deal with the Justice Department to
settle marketing violations related to
Vioxx (on top of the $5.6 billion the
company has paid out to settle various
Vioxx lawsuits and claims).
Because stiff fines don’t seem to
compel some companies to toe the
line, the regulators and prosecutors
are weighing even harsher penalties.
One threat is to bring criminal charges
against corporate executives consid-
ered responsible for serious violations.
A former Glaxo executive is headed for
trial for making false statements and
blocking an FDA investigation; convic-
tion could bring a jail term as well as
fines. If that doesn’t compel companies
to clean up their acts, the feds also
are looking to ban companies commit-
ting fraud from doing business with
Medicare and Medicaid under a stiffer
federal exclusion policy.
In addition to waving the enforce-
ment stick, FDA leaders talk of more
guidance and assistance to help
companies meet quality and safety
standards and to bring high quality
drugs more quickly to patients. Efforts
by industry and regulators to find the
resources and appropriate policies to
achieve this objective will be in the
spotlight in the coming year. ❏
sssst! best kept secret in EDC?
The DataLabs EDC solution is the proven solution from Perceptive
Informatics built on a powerful platform to provide cutting-edge
EDC functionality. Optimal for all types and sizes of clinical trials,
the DataLabs solution means total flexibility and ease of use for
sponsors and sites.
Contact us today at [email protected] to learn more about the
best kept secret in EDC.

22 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
To see more View from Brussels articles, visit
appliedclinicaltrialsonline.com
View from Brussels
Peter O’Donnell
is a freelance journalist
who specializes in
European health affairs
and is based in Brussels,
Belgium.
The New Year Brings Same Old BattlesAn alliance between two European leaders gives hope for unison but falls short on solutions.
As the glitz and warm
goodwill of the festive season
evaporate, drug firms and
drug regulators are once
again faced with the chilly reality of
their differences of view, still largely
unresolved as we move into the second
decade of the 21st century. The
clinical trial community is one of the
principal victims of these differences,
pincered between ever-increasing
demands for demonstration of value
and ever-tighter budgetary constraints
from cash-strapped sponsors.
The problem is depressingly fa-
miliar: growing healthcare demand,
rising healthcare costs, tougher
drug-launch criteria, squeezed com-
pany revenues, and pressure on R&D
budgets—at the same time, drug
development becomes harder and
more expensive. What makes it all the
harsher in this unhappy new year is
that the economic downturn is biting
severely into both public expenditure
and private-enterprise profits.
Two luminaries of the European
pharmaceutical scene—one from each
side of that traditional divide—made
an attempt to forge a new approach as
the old year came to an end. Andrew
Witty, the CEO of GlaxoSmithKline
and President of the European Federa-
tion of Pharmaceutical Industries and
Associations, and one of Europe’s top
regulators, John Dalli, the European
Union’s Commissioner for Health, is-
sued a sort of joint manifesto that tried
to square the classic vicious circle.
Their starting point was that policy-
makers and the pharmaceutical indus-
try across the European Union share
the goal that all citizens and patients
in Europe should enjoy equal access
to the right medicines and vaccines.
They offered a vision of the phar-
maceutical industry, policy makers,
health insurers, patients, and others,
working together to achieve that ob-
jective. Success, they claimed, would
result in healthier citizens, enhanced
competitiveness, more balanced bud-
gets, and fair reward for innovation.
“Valuable innovation can transform
lives,” they agreed.
A noble aspiration. At the broadest
level, the need for greater equality is
clear—as Dalli and Whitty remarked.
They pointed to the beneficial impact
of earlier diagnosis and new treat-
ments on cancer, where incidence is
increasing in the EU, but mortality is
decreasing. “There is significant vari-
ability in patient access and in relative
survival rates,” they went on to note.
“Similarly, we see wide variability
between member states in the speed
with which valuable innovative medi-
cines become available to patients,
and then further variability in uptake
between member states and between
disease areas.”
Aspiration is one thing. Delivery
is another. As the two European
pharma champions acknowledge,
the task of delivering equality across
Europe is not easy. “Health services
everywhere face enormous chal-
lenges. Governments are understand-
ably struggling to cope with rapid
demographic change, the pace of
technological change, and unbridled
demand for healthcare. The current
financial crisis exacerbates the dif-
ficulty of balancing desire for health-
care equality with the need for finan-
cial management.”
Against this background, they go
on, “governments need to maximize
public health outcome for a given bud-
get, and to make choices.”
This is the difficult bit—for pharma
companies struggling to get new
products onto the market, and equally
for health authorities harangued by
their publics.
European governments are focus-
sing on value for money, and rely
increasingly on processes like health
technology assessment for decision-
making. Dalli and Witty both say that
this is appropriate, but there are reser-
vations and hesitations.
“HTA requirements in different
member states vary considerably,
which causes complexity for industry.
The ongoing fragmentation of health-
care delivery in Europe introduces
further challenges,” they remark, in a
bold display of diplomatic harmony.
But as they advance in their argu-
ment, the underlying tensions inevita-
bly emerge.
Making it all the harsher in this unhappy new year is the economic downturn biting severly into both public expenditure and private-enterprise profits.

PharmaNet has spent years honing scientific skills and refining expertise in our clinical
development and bioanalytical laboratory operations. Dedicated therapeutic experts
specialize in oncology, cardiovascular, neurosciences, infectious diseases, and other key
areas. Our project teams integrate innovative science and quality into each project.
From small to large programs, in a clinical environment or laboratory, this is just one
more reason why PharmaNet works for you.
Bioanalytical and Phase I-IV, Proven Therapeutic Expertise.
1 609 951 6800 www.pharmanet.comWorks For You
Phase I - IV B ioanalytical B ioequivalence Consult ing Staf f ing
Please visit us at:
• The 1st Regulated Bioanalysis Workshop
(Asia Pacific), Shanghai, China
• ISCR Conference, New Delhi, India
• Paediatric Drug Development Conference,
London, United Kingdom
• DIA Annual EuroMeeting, Geneva, Switzerland
• World Pharma Trials/Clinical Trials Supply
(Biopharm Asia), Singapore, China

24 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
View from Brussels
“In this challenging climate, it is
vital to achieve the best results for
patients across the European Union,
for public budgets and for industry,”
they say. They speak of “an equilib-
rium” between the needs of these
different players—but in the same
sentence they add: “with patients put
first”—immediately suggesting some
disequilibrium in the priority to be
allocated to each player. Reading this,
it is impossible to resist the thought
that all players are equal, but some
are more equal than others.
From that point onwards, their
joint manifesto starts to fray, with its
separate threads stitched tenuously
together only by the deployment of
well-meaning generalizations that
studiously avoid confrontation on the
difficult details.
“All stakeholders need to change
the way they think and act, with
‘health for all’ achieved collabora-
tively at local, national, and European
level,” they chorus blithely—and
innocuously, since the appeal is so
vague as to be meaningless.
“‘All for health’ should be the key
enabler—the more institutions work
in a trusting environment, the more
likely the right approaches can be de-
veloped,” they warble happily, allow-
ing sound to triumph over sense.
Where the manifesto addresses the
distinct needs of each “stakeholder,”
it does so in the same well-meaning
and inoffensive terms. “Industry must
be a genuine partner to governments
and their agencies,” it trills. Who
could take exception to its brotherly
expressions of mutual understand-
ing? Industry “must deliver new
medicines and vaccines that address
unmet patient need and have demon-
strable value.” Well yes, of course.
And how? “This means getting R&D
right—reversing the decline in pro-
ductivity and delivering medicines
that match the health needs of the
population.” Not wrong, of course,
but not sufficiently right either to
bring any illumination into the dark
realities of this debate. Similarly,
“industry must increase the transpar-
ency of what it does and be a source
of ideas to governments, including
on increasing funding and more ef-
ficient use of budgets.” Insofar as
this highly-nuanced and carefully se-
lected language conveys anything at
all, it seems to amount to little more
than an offer to industry to connive
with governments in engineering its
own downfall.
As a concession, as it were, to in-
dustry sensibilities, the passage con-
cludes: “The pharmaceutical industry
is hugely innovative. If governments
work to support innovation, the indus-
try will deliver the next era of revolu-
tionary medicine.”
That blandly optimistic formula-
tion is followed by another: “Govern-
ments have the key responsibility for
delivering equitable healthcare. It is
possible for them to encourage and
reward therapeutic progress, while
maintaining core characteristics
like equity, public funding, and strict
regulation.” It may indeed be pos-
sible. What would be more interest-
ing would be to know more about how
it is to be done.
The recipes proposed for success
remain largely at the same level of
pious exhortation and comfortable
banality. “We must create in Eu-
rope the right policy and regulatory
framework.” OK, what’s next? “This
requires that effective prevention
and wellness programs are in place.”
Safe, but vague. “We must shift focus
from cost to value, and set a strategic
agenda that addresses unmet needs.”
Difficult to fault, but difficult to deci-
pher, too.
There is some attempt to grapple
with the difficulties in establishing
a sense of value—but again, without
much real commitment to a discern-
ible course of action. There is talk of
“allowing industry to understand the
type of added value that matters to
patients and will be funded by pay-
ers,” and of “a shared understanding
of value” through “high quality dia-
logue between industry and authori-
ties.” Dalli and Witty (a coupling of
names that faintly suggests a comic
duo from the age of music hall, even
if their routine often seems short of a
punch line) see an important role for
health technology assessment in en-
suring that “the government does not
pay for medicines that do not work
but that equally, patients get access
to medicines that may help them.”
But how it should play this role is less
clear. “Closer cooperation” is one rec-
ommendation, immediately countered
by the remark that “a single approach
in the EU is undesirable, since mem-
ber states will want to make decisions
according to their own priorities.”
At the same time, “the current di-
versity and overlap leads to unequal
access for patients, complexity for
industry, duplication of work, and
unnecessary red tape.” This tangled
series of observations is hardly clari-
fied by the conclusion that “While the
final decision has to remain national,
in particular on price and reimburse-
ment, we should explore a common
methodology on the clinical aspects
of health technologies in Europe
which might then be used for assess-
ments of relative efficacy and effec-
tiveness at European level.”
So if clinical trial and pharmaceuti-
cal professionals were hoping that
this unusual outburst of ecumenism
in Brussels was going to make things
easier—or even just clearer—in the
new year, well, I’m very sorry. But
happy new year anyway. ❏
Reading their manifesto, it is impossible to resist the thought that all players are equal, but some are more equal than others.

Break Through to Success at the BIO Exhibition
Join us June 27-30 for the 2011 BIO International Convention—
the industry’s most dynamic event—where leading-edge providers display
their latest technologies, services and solutions at the bustling BIO Exhibition.
Find the breakthrough solutions you need from among 1,700 companies
strategically organized into Product Focus Zones, regional and country
Pavilions, and engaging Interactive Theaters to expedite your search.
Encounter 15,000+ biotech leaders, innovators and decision makers from 65
countries, face to face—
O� in the BIO Exhibition—with new Exhibition Power Hours
O� during thought-provoking sessions and Keynotes
O� at exclusive receptions and special events
O� through participating in the BIO Business Forum
Leadership. Partnerships. Breakthroughs.
June 27-30, 2011Monday-Thursday
Walter E. Washington Convention CenterWashington DC USA
Follow us:
Register Today and Save 40%
Early-bird deadline:May 19, 2011
convention.bio.org

26 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
Clinical Trial Insights
Kenneth A. Getz
MBA, is a Senior Research
Fellow at the Tufts CSDD
and Chairman of CISCRP,
both in Boston, MA, email:
To see more Clinical Trial Insights articles, visit
appliedclinicaltrialsonline.com
Frustration with IRB Bureaucracy & DespotismDoing more harm than good will ultimately force human subject protection system reform.
My personal frustration
with institutional review
boards reached a boiling
point several months ago.
A dozen IRBs had each reviewed a
general educational brochure prepared
by the Center for Information and
Study on Clinical Research Participa-
tion (CISCRP). The brochure was not
specific to any clinical studies and its
focus was on explaining the risks and
benefits of clinical trial participation.
All IRBs had suggested revisions to
the educational language. But only one
of the 12 IRBs rejected it. The reason
for rejecting the brochure: Educational
material “…should not include the word
hope because the term is coercive.”
My deep frustration was felt on many
levels. The concept of “hope” is central
to patients and their families wanting
to consider and evaluate clinical trials
among their options. Just as risks can
be discussed openly and in a language
that the lay public understands, gen-
eral educational information must also
openly and honestly acknowledge the
potential benefits of participation. Why,
you might ask, were IRBs even review-
ing a general educational brochure
when it falls outside their jurisdic-
tion?1 As an independent non-profit,
CISCRP’s mission is to provide public
education to promote greater, more
balanced and informed understanding
and awareness of the clinical research
process. This is also part of the overall
mission of all human subject protection
programs. By rejecting CISCRP’s edu-
cational materials, was this IRB doing a
disservice to the very population that it
strives to protect?
I’m clearly not alone in my frustra-
tion. A large and growing number of
government and private-sector clini-
cal research professionals are voicing
their concerns and suggesting that
our current human subject protection
system is ripe for radical reform to
change its antiquated, fragmented, bu-
reaucratic, and over-reaching ways. A
number of peer-reviewed articles have
sounded the alarm including: Salim
Yusuf’s “Randomized Clinical trials:
Slow Death by a Thousand Unneces-
sary Policies?”2 and Christine Grady’s
“Do IRBs Protect Human Research
Participants?”3 This past year the Insti-
tute of Medicine has singled out IRBs
as one of the top barriers to achieving
efficiencies in clinical research. At a
meeting that I attended in October,
serious concerns were raised by aca-
demic and government leaders that
failures of the IRB system are actually
hindering the ethical protection of
study volunteers.
Too many cooksWhat’s wrong with the system? Or,
as some have rephrased the question,
what’s not wrong with it? Our nation’s
system of human subject protection
programs has evolved into a complex
regulatory and legal environment with
19 agencies in addition to the Food and
Drug Administration (FDA) sharing
oversight for protection of study par-
ticipants. These agencies include the
Social Security Administration and the
Department of Homeland Security. Af-
ter protracted debate, various agencies
adopted the Common Rule in 1991 to
harmonize human subject protection
policies. Many agencies subsequently
have added regulations while others
have adopted inconsistent guidance
on how to interpret the rule. The FDA
chose not to even adopt the Common
Rule, but did change its IRB and in-
formed consent regulations to more
closely correspond to federal policy.
Adding to the confusion is the fact that
IRBs must follow federal privacy re-
quirements and state laws. Some IRBs
must also balance compliance with
International Conference on Harmoni-
zation (ICH) guidelines for studies out-
side the United States. This complex
and crowded array of organizations
have burdened IRBs with substantial
inconsistencies in ethics regulations
and the challenge of complying with
many different and potentially conflict-
ing requirements.
Unnecessarily wastefulManaging that burden would be
enough. But there is the added weight
on research sponsors to reconcile
and coordinate wide and inconsistent
variation in ethical review decisions
across multiple IRBs. Current regula-
tions require that each institution and
investigative site involved in clinical
research receive IRB approval. An
ethical review of a single protocol for
a multicenter trial requires that many
IRBs conduct their own independent
reviews. Reviews of the same protocol
are not coordinated, they result in
contradictory recommendations and
outcomes, and they cost the research
sponsor and study staff substantial
time and resources.

lab results you can trust
Head Office: Bayerstr. 53, D-80335 Munich, Germany
INFO-PHONE: +49 89 741 393 0 – E-MAIL: [email protected] – HOMEPAGE: www.INTERLAB.de
Europe – The Americas – Asia/India/China – Australia – South Africa – Near/Middle East
Project Managers = key to INTERLAB’s success
s�PROJECT�TEAMS�IN�53!�AND�'ERMANY
s�DEDICATED��FLEXIBLE�AND�PRO ACTIVE�SCIENTISTS
s�IDENTICAL�QUALITY�STANDARDS�IN�ALL�LOCATIONS�WORLDWIDE
High Quality and Strong Expertise
s�OVER��������SAMPLES�DAY�IN�%UROPE��ECONOMIES OF SCALE
s�SINCE�������ESTABLISHED�INFRASTRUCTURE�FOR�GLOBAL�STUDIES
s�SINCE�������GLOBAL�)4�PLATFORM�COMPLIANT�WITH���#&2��
s�COUNTRY SPECIFIC�FLAT�FEES�FOR�TRANSPORTATION��NO�SURPRISES�
s�UNLESS�YOUR�BUDGET�IS�UNLIMITED� WHY�PAY�MORE�ELSEWHERE�
Range of Services: incl. genetics
s�BIO ANALYTICAL�SERVICES
s�ASSAY�DEVELOPMENT
s�EXTENDED�SAMPLE�STORAGE
s�WORLDWIDE�SHIPPING
s�VISIT KITS��AUTOMATIC�RE SUPPLIES
s�SMALL��REGIONAL�STUDIES��0HASE�) ))
s�INTERNATIONAL�TRIALS��0HASES�)) )6
s�ONE�GLOBAL�1!�SYSTEM��)3/�����
Customized
central lab services
with global reach
for over 16 years:
since 1994
MIT
G
Customized
central lab services with global reach
for
our sponsors’ satisfaction

28 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
Clinical Trial Insights
Clinical research professionals in
both the public and private sectors
widely agree that our current multiple
IRB system is wasteful and causes
unnecessary delays. In a recent New
England Journal of Medicine edito-
rial, OHRP Director Jerry Menikoff,
said that duplicative reviews not only
provide “relatively few benefits,” but
the current structure actually might
lead to “less-than-optimal protection”
of those who volunteer to participate
in research.
Menikoff points out that the system
results in individual IRBs feeling
powerless to change the protocol
when risks are identified. If one IRB
has serious concerns about the study
design, it usually results in that IRB
leaving the study—either of its own
accord or after being dropped by the
sponsor—rather than resulting in a
change to the protocol.
Overreaching, overwhelmingA growing number of research
sponsors and investigative site staff
have expressed frustration and concern
about IRBs overseeing more than
their jurisdiction dictates. During the
past two decades, IRBs have asserted
themselves as gatekeepers of all
interactions with patients and the public
and the protectors of every possible
potential or imagined harm that might
occur during research. As such, IRBs
often impose burdensome, impractical,
unnecessary requirements in order to
err on the side of extreme caution.
Researchers and institutions com-
plain that IRBs are overly expansive in
interpreting regulatory requirements
and that they focus on inconsequen-
tial details during reviews. Others
complain that IRBs have been over-
whelmed with obligations that have
little to do with protection of research
participants, and IRB members tend
to focus more on procedures and
documentation than on difficult ethical
questions and serving patients’ and the
public’s best interests.
As clinical research has become
more complex and demanding, the
scope of IRB responsibilities has ex-
panded to include compliance with
privacy regulations, checking for poten-
tial financial conflicts of interest, and
reviewing the methodological sound-
ness and scientific merit of a study. Yet
as IRBs are asked to take on more re-
sponsibilities, they have been criticized
for becoming less effective and more
susceptible to questionable practices.
The now famous sting operation carried
out by the General Accounting Office
(GAO) in 2008 exposed a national hu-
man subject protection system vulner-
able to unethical manipulation.
IRB jurisdiction and authority is also
virtually never challenged or evaluated.
Few sponsors and investigative sites are
willing to question an IRB’s decisions
out of fear that the IRB might scrutinize
their proposal more closely or won’t
approve their research. The IRB’s deci-
sion is the gospel—taken without ques-
tion—despite the fact that nowhere in
the regulations is an appeal prohibited.
There is no data measuring whether
IRBs are doing their job in protecting
study volunteers from unnecessary
risk of harm. The IRB system, which
evolved from an institution-based struc-
ture with little accountability or data
collection, lacks even rudimentary met-
rics for measuring its own success.
Eventual reformThere’s no question that frustration
among all stakeholders is intensify-
ing and will eventually drive reform.
But structural and procedural re-
forms are likely a long way off given
such a complex, crowded, and heavily
regulated system.
Many ideas for IRB reform center
around streamlining and creating a
better, harmonized review process.
One approach would be for sponsors
to require the use of a central IRB as
a condition for sites to participate in a
study. Another proposal would change
the system to impose more demands on
early trials with new interventions while
simplifying the oversight of commonly
used interventions. Academic and gov-
ernment leaders have recommended
collecting more data in order to mea-
sure IRB performance.
The FDA and OHRP both support
the use of a single, central IRB for mul-
ticenter research. Drug sponsors have
increasingly contracted with central
IRBs to review studies conducted by
community-based investigative sites.
Most universities and hospitals still opt
to use their own internal IRBs when
conducting both privately and federally
funded research. OHRP is leading an
effort to coordinate guidelines across
various agencies, and plans to propose
the creation of a single new agency to
oversee all human subject research in
the United States.
As criticism and dissatisfaction
grows, our national IRB system has
been losing credibility and respect
among regulatory agencies, clinical re-
search professionals, patients, and the
public. Extreme frustration may drive
reform even sooner. After all, we owe it
to patients and the public to get this IRB
system, or a new one, working right. ❏
References1. Code of Federal Regulations, Title 21, Part
56, Section 102, 109 (US Government
Printing Office, Washington, DC).
2. S. Yusuf, “Randomized Clinical Trials:
Slow Death by a Thousand Unnecessary
Policies?” Canadian Medical Association
Journal, 171 (8) 889-892 (2204).
3. C. Grady, “Do IRBs Protect Human
Research Participants?” Journal of the
American Medicial Association, 304 (10)
1122-1123 (2010).
Clinical research professionals in the public and private sectors agree that our current multiple IRB system is wasteful and causes unnecessary delays.

THEABOUT
IT’S ALL
SERVICEOur customers have much to say about the service they can count on from Aptuit’s Clinical Packaging & Logistics.
They tell us it’s all about reliability. They recognize that we consistently deliver at maximum effectiveness, supported
by efficient systems. They say it’s all about the exemplary service of a designated Project Manager on every project,
making sure that all work is done right the first time, every time. They are impressed with the attentive service they
receive from primary and secondary packaging experts and packaging designers. They acknowledge the value our
global service from sites in North America, Europe and Asia, citing our regulatory expertise and our network of global
depots. And repeatedly, they say that they know they can depend on our ability to work with controlled substances,
relying on our refrigerated, frozen, controlled drug and stem cell storage and distribution capabilities.
And we have a message for our customers, and for those who are thinking about partnering with us: at Aptuit, it’s all
about continuing to provide the highest level of service, at every level of our organization.
CLINICAL PACKAGING & LOGISTICS
For more information, please call +1 816-767-3900 North America, +44 131-451-2451 Europe
or visit www.aptuit.com/Services/Clinical Operations.aspx

30 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
Sites
Collaborative Staffing Model for Multiple SitesReducing the challenges of study coordination in complex, multi-site clinical trials.
Mary E. Larkin, Paul McGuigan, Denise Richards, Karen Blumenthal,
Kerry Milaszewski, Laurie Higgins, Jill Schanuel, and Christen Long*
The implementation of complex,
multi-site clinical trials pres-
ents challenges that make re-
cruitment efforts, participant
follow-up, and organization of
staff critical to the success of the overall
outcome. This article describes a unique
staffing model utilized by the TODAY
(Treatment Options for type 2 Diabetes in Ado-
lescents and Youth) study, an NIH (National
Institutes of Health) sponsored trial designed
to explore treatment options for type 2 diabetes
in youth. At each study center, the program
coordinator (PC) and diabetes educator (DE)
work together to implement the study protocol.
A staffing model that provides this type of mu-
tual support for two key members of the study
team may decrease the burden customarily
encountered solely by the PC in complex trials,
and furthermore allows for cross-coverage and
flexibility. To determine the degree of overlap
and task sharing between the PC and DE across
study sites, a self-administered survey was dis-
tributed to all PCs and DEs. Survey results
as well as specif ic examples demonstrating
an effective collaborative approach by front-
line study personnel in managing various chal-
lenges encountered in study implementation
are included.
BackgroundThe TODAY study, which randomized its first
participant in 2004, aims to identify optimal
treatment regimens for type 2 diabetes specifi-
cally for adolescents and youth, as incidence
has dramatically increased.1-4 The study follows
an ethnically diverse group of 704 overweight
youth (aged 10-17 at enrollment) with new on-
set type 2 diabetes (less than two years
duration) for a minimum of two to six
years at 15 clinical centers across the
United States. The goal is to compare
the efficacy of three treatment arms (two
medication-only arms and one intensive
lifestyle intervention combined with med-
ication arm) on glycemic control.3 Study
participants have routine medical visits
every two months for the first year and quarterly
thereafter. Interim medical visits are scheduled
as needed for management of comorbidities or
reinvigoration of diabetes management.
The study participants are adolescents and
their families who are coping with a new diagno-
sis of type 2 diabetes, and are also typically deal-
ing with extreme socioeconomic challenges, psy-
chiatric problems, and/or other chronic health
concerns. Many of them have life circumstances
that are inherently unstable; the recent diag-
nosis of a chronic illness creates additional dis-
ruptions in their lifestyles. It is not unusual for
them to present a number of pressing issues at
each study visit requiring extensive interaction
with personnel with two distinct protocol-driven
roles: PCs and DEs.
Unlike the typical staffing model in large clini-
cal trials where the designated PC assumes most
of the responsibility for the daily work of imple-
menting the protocol,5 in the TODAY study, the
PEERREVIEWED

appliedclinicaltrialsonline.com APPLIED CLINICAL TRIALS 31January 2011
PC and DE at each study center work together to sched-
ule and conduct visits, as well as collect outcome data.
Although the study design and roles are protocol-driven,
placing specific expectations on the PC and DE, the real-
ity of carrying out each visit requires flexibility and task-
sharing; the demands often lead to overlap in these roles at
each study site.
In order for this type of staffing model to be effectively
implemented, teamwork and cross-training are essential
and are supported by weekly conference calls and periodic
study group meetings among all PCs, DEs, and staff of
the Data Coordinating Center (DCC). The calls allow the
opportunity to offer thoughts and perspectives on current
study issues, as well as the opportunity to explore specific
questions or challenges of protocol implementation. Both
PCs and DEs attend study trainings that emphasize imple-
mentation of the trial and care of the enrolled population.
This cross-training assures that the DE or PC can each
help with the other’s tasks where necessary, in order to
facilitate timely completion of the study visits.
There are limited published reports regarding effective
staffing models of large clinical trials, and although the
typical tasks performed by a research nurse6,7 and/or clini-
cal research coordinator8,9 have been described, the roles
remain poorly defined. Little is known about workload dis-
tribution and job satisfaction, and many of the reports are
anecdotal in nature.
In the Diabetes Control and Complication Trial (DCCT),
the PC role was filled almost exclusively by nurses. Dur-
ing the planning phase of the DCCT, the anticipated scope
of duties of the research trial coordinator was unclear. In
1984, the second year of the trial, 21 trial coordinators (19
nurses, one physician’s assistant, one dietician) were sur-
veyed about their job activities, and subsequently reported
diverse duties, including spending almost 50 percent of
their time in medical management and 30 percent in ad-
ministrative activities. 10
In the 1990s, there were few resources available for in-
experienced PCs and the expectations of the role remained
vague. It was not uncommon for studies to employ a model
of hiring a PC with no clinical background, but who ex-
In the 1990s, there were few resources available for inexperienced PCs and the role remained vague.
ICON Clinical Research
24 hours in the life of ICON
ICON Development Solutions
Scientific Research Manager,
Elizabeth, conducts a neuropathic pain
study in a pharmacodynamic testing suite.
When it’s 3.15pm at our Clinical Pharmacology
Unit in Manchester, it’s 9.15am at our units
in Omaha and San Antonio, where our
pharmacodynamic specialists are conducting
complex models to identify early efficacy
signals for candidate compounds. This is
just one example of how ICON Development
Solutions provides global expertise to expedite
early drug development.
No matter the hour of the day, there’s an
ICON expert somewhere around the world
working to deliver results for informed,
timely decision-making.
ICON Development Solutions:
www.iconplc.com/translational
9.15amSan Antonio, U.S.

32 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
Sites
celled in other skills such as problem solving, communica-
tion, and organization.5 In some studies, dieticians were
selected for the PC role due to the necessity of delivering
nutrition education as part of the study protocol.11
In 2004, a survey of the standard tasks performed by 41
oncology clinical trial research coordinators showed that
they all participated in activities such as recruitment, data
collection, adverse event reporting, and audit preparation.8
Those with a nursing background had significantly greater
involvement than non-nurse coordinators in clinical care,
such as assessment of response to therapy, adverse effects,
and query resolution. In 2007, a report of survey results
from 205 PCs (50 percent registered nurses) examined
factors related to PC turnover. The findings revealed three
major themes: the need for formal training, lack of promo-
tion opportunities, and poor allocation of workload.9
In the TODAY study, a combination of clinical manage-
ment and administrative tasks are required at each study
visit. In general, the PC is primarily responsible for adminis-
trative aspects of study implementation, such as IRB corre-
spondence, budget preparation, supply ordering, equipment
maintenance, data entry, and shipping of lab specimens.
The DE’s central responsibilities focus on medication ad-
herence and adjustment, patient and family education, and
clinical management of diabetes and its comorbidities.
However, scheduled participant visits do not necessarily fall
into discrete components solely requiring the skills of one
type of staff member (clinical) or another (administrative).
In addition, many study visit appointments occur during
non-routine work hours in order to accommodate the par-
ticipants’ work and school schedules. It is neither practical
nor feasible, within the constraints of staffing limitations,
to always have both staff members available for each visit,
especially when visits occur after hours and on weekends.
To determine if the degree of overlap between the roles
of the PCs and DEs across all sites was consistent with
our expectations, given the complexity of the study visits,
a questionnaire was developed and administered to all eli-
gible PCs and DEs.
MethodsParticipants. The sample consisted of 31 TODAY staff mem-
bers (n=15 PCs; n=16 DEs). The authors, who represent
DEs and PCs, were not included in the sample to avoid bias
of the results.
Measures. The authors developed a questionnaire de-
signed to examine specific responsibilities related to con-
ducting study visits and participant follow-up. It included a
demographic section (i.e., role assignment as a PC or DE,
years of experience working on the TODAY study, years
of experience working in diabetes care/research prior to
TODAY, education level, and employment status with the
TODAY study—part-time or full-time), and an 18-item list
of the tasks expected to be most frequently performed by
PCs or DEs as described in the TODAY study manual of
operations and through author consensus.
Procedures. The survey was administered during a na-
tional study group meeting in June 2008. To preserve ano-
nymity of the respondents, the survey was distributed and
collected by a DCC representative. To be sure that all PCs
and DEs had the opportunity to participate, the DCC also
distributed the survey via e-mail following the meeting.
Responses to the electronic survey were sent directly to the
DCC, where results for all of the surveys were tallied and
categorized according to role group (PC/DE).
ResultsThirty-one responses were received out of a total possible
sample of 43 representing a response rate of 72%. Demo-
graphic information regarding the sample is summarized
in Figure 1. Most respondents (65%) held a bachelor’s de-
gree, and close to one-third had a master’s level education.
Of the 31 respondents, the majority came from a nursing
background (54%), while the remainder was evenly divided
between dietetics (22%) and other disciplines (22%). Before
working in the TODAY study, 45% had less than one year of
research experience, while 13% had greater than 10 years.
The most common previous research experiences included
roles as a research coordinator (55%), recruiter (42%), and re-
search nurse (39%). About 50% of those who responded were
working part-time on the study, while 50% reported working
full-time. Approximately half of the respondents had been
with the study since its inception and half had started after
the beginning of the trial. The majority (65%) had greater
than five years of experience in diabetes-related patient care.
PCs and DEs Background and Professional Affiliation
70%
60%
50%
40%
30%
% o
f R
esp
on
de
nts
Education
Previous
Research Experience
Previous
Roles Experience
PC
DE
20%
10%
0%
BA BSRN RD NP
MS
<1yr
1-5 yr
6-10
yr
>10yr
Resea
rch A
ssist
ant
Resea
rch C
oordin
ator
Resea
rch N
urse
Co-Inve
stig
ator
Recru
iter
Adm
inist
rato
r
Resea
rch D
itician
Source: Mary E. Larkin et al.
Figure 1. Research coordinator and recruiter
were the two most common roles among PCs and
DEs prior to joining TODAY.

appliedclinicaltrialsonline.com APPLIED CLINICAL TRIALS 33January 2011
Consistent with our cross-training goals, a high degree
of overlap is confirmed by the answers to the self-report
survey. As shown in Figure 2, the respondents share (de-
fined as over 50% of both PCs and DEs report performing
on a regular basis) close to half (8 out of 18) of the typical
study-related tasks, such as: scheduling visits, maintain-
ing phone correspondence, attending meetings, setting up
study visit charts, allocating medication from the central
dispensing center, assessing medication compliance, and
obtaining anthropometrics. In addition, DEs obtain lab
samples slightly more often than PCs.
Discussion Results from the current study are consistent with the
hypothesis that coordination of the TODAY study involves
cross-training and task-sharing between two roles, the
PCs and DEs, across all sites. An example of the benefits of
cross-training can be seen in scheduling appointments and
maintaining communication with the participants. These
are typically two of the most time-demanding tasks for the
PCs, as participants frequently reschedule multiple times
due to conflicting plans. In addition, because of the chal-
lenges that many study families face which include other
health issues and socioeconomic and language barriers,
Tasks Performed on a Regular Basis by PCs and DEs
% o
f R
esp
on
den
ts
Tasks
100
90
80
70
60
50
40
30
20
10
Sch
ed
ulin
g
Vis
it S
et-
up
Ph
on
e C
alls
Sta
ff M
eeti
ng
s
Main
tain
eq
uip
men
t
IRB
Co
mm
itte
e c
alls
Su
pp
ly o
rderi
ng
Ob
tain
an
thro
po
metr
ics
Bu
dg
et/
gra
nt
mg
mt
Dru
g a
llo
cati
on
Data
en
try
Sh
ipp
ing
Ass
ess
med
co
mp
lian
ce
Ob
tain
/pro
cess
lab
sam
ple
s
Med
icati
on
ad
just
men
t
Ru
n-i
n less
ion
s/fo
llo
w-u
p e
du
cati
on
PC
DE
Inte
rpre
t la
b r
esu
lts
& d
ete
rmin
ein
terv
en
tio
ns
0
Source: Mary E. Larkin et al.
Figure 2. Program coordinators and diabetes educators shared close to half of the typical study-
related tasks.
Data manager, Todashi,
processes data from an
oncology study.
10.14amTokyo, Japan.
ICON Clinical Research
24 hours in the life of ICONWhen it’s 7.14pm in our Nashville office,
it’s 10.14am in Tokyo, where a data manager
is reviewing EDC data within our integrated
reporting system and providing comprehensive
information for a global clinical trial. ICON’s
data managers are trained to employ the most
efficient technology solutions and standards.
Our experience and understanding of eClinical
processes and systems, such as EDC &
ePRO, enable us to provide the optimum
solution for each project.
No matter the hour of the day, there’s an
ICON expert somewhere around the world
working to deliver results for informed,
timely decision-making.
ICON Clinical Research:
www.iconplc.com/datamanagement

34 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
Sites
contact information may change frequently, making it dif-
ficult to stay in contact. During some phases of the study,
frequent contact by phone may be required between the DE
and the family, for example, when it is necessary to adjust
insulin doses and review blood sugar levels. Because of the
frequency of phone contact utilized in this activity, the DE
can also assume the administrative task of scheduling ap-
pointments, thus alleviating the burden on the PC.
Another benefit of having staff members from both groups
(PC and DE) working closely with the participants is that
different information may be reported to each individual. For
example, the PC collects general information from the par-
ticipant and/or the family during check-in. This information
is often very important and related to diabetes self-manage-
ment and may not always be shared with the DE. It is impor-
tant for the DE and the PC to communicate throughout the
visit to make sure that all relevant information gathered by
the PC is provided to the DE for review and clinical interpre-
tation. For instance, if the participant has exceeded a certain
threshold of weight gain or an elevated blood pressure prior
to the last visit, the results will be brought to the attention of
the DE so that he/she can intervene by reinforcing education
or evaluating whether a study MD should be consulted.
Study visits, which involve gathering anthropometric
data, administering questionnaires, assessing medica-
tion compliance, downloading blood glucose meters, and
providing medication and monitoring supplies, can range
from 1-7 hours in length and are often complicated by
unanticipated difficulties in schedule flow. Managing new
comorbid conditions such as hypertension, hyperlipidemia,
or poor glycemic control may necessitate unexpected time
spent for teaching insulin injections, low-fat meal planning,
or instructing the family in the use and side effects of new
medications. As a result, PCs may need to re-prioritize
the goals of the visit, allowing more time with the DE than
planned, without disrupting the schedule of data collection
or jeopardizing adherence to the protocol.
Conclusions The PCs and DEs in the TODAY study collaborate to fa-
cilitate study visits, track participant progress, and nurture
relationships with participants and their families. As de-
scribed previously, the PCs and DEs have a working knowl-
edge of each others’ roles, which fosters team cohesion,
especially during subject appointments. Task-sharing pro-
vides opportunities for preemptive problem solving among
the front-line study staff. Depending on staffing, each site
may function slightly differently, but it is essential for the
DE and the PC to work together as a team throughout the
study visit to ensure complete data collection and efficient
time management.
This staffing model provides mutual support for the PC
and DE at each study center, decreases the challenges cus-
tomarily encountered solely by the study coordinator in a
complex trial, and allows for cross-coverage and flexibility.
While the roles retain their specific responsibilities and
specialties as dictated by the study protocol and design,
there is significant overlap, redundancy, and cross-training
between the two groups, allowing flexibility of participant
scheduling and the ability to respond to unanticipated
needs of participants as they may arise.
The limitations of this staffing model include the added
resources which may be necessary to train and support
both role groups as well as the need for continued commu-
nication between staff members in order to facilitate this
level of collaboration.
This type of collaborative staffing model (where the spe-
cific job responsibilities and procedural protocol are clearly
laid out while allowing for the burden to be shared for some
of the most time-consuming and tedious elements of study
coordination) could potentially increase job satisfaction
and reduce staff turnover in long-term trials. For example,
research conducted in community mental health settings
suggests that the implementation of manualized protocols
such as those utilized to guide the implementation of the
TODAY study can enhance staff satisfaction and decrease
staff turnover.12 While this effect was not measured or
reported in this article, future research may be aimed at
describing the relationship between staffing models, staff
attrition, and subject retention.
Editors’ note: Funding information and a list of TODAY
Study Group members can be found in the online edition of
the article, www.appliedclinicaltrialsonline.com.
References 1. American Diabetes Association, “Type 2 Diabetes in Children
and Adolescents Consensus Statement,” Diabetes Care, 23 (3)
381-389 (2000).
2. A.L. Rosenbloom, J.R. Je, R.S. Young, and W.E. Winter, “Emerg-
ing Epidemic of Type 2 Diabetes in Youth,” Diabetes Care, 22 (2)
345-354 (1999).
3. G. Alberti, P. Zimmet, J. Shaw, Z. Bloomgarden, F. Kaufman,
and M. Slink, “Type 2 Diabetes and the Young: The Evolving
Epidemic,” Diabetes Care, 27 (7) 1798-1811 (2004).
4. The TODAY Study Group, “Treatment Options for Type 2 Dia-
betes in Adolescents and Youth: A Study of the Comparative
Efficacy of Metformin Alone or in Combination with Rosigli-
tazone or Lifestyle Intervention in Adolescents with Type 2 Dia-
betes,” Pediatric Diabetes, 8 (2) 74-87 (2007).
Future research may be aimed at describing the relationship between staffing models, staff attrition, and subject retention.

appliedclinicaltrialsonline.com APPLIED CLINICAL TRIALS 35January 2011
12. G.A. Aarons, D.H. Sommerfeld, D.B. Hecht, J.F. Silovsky, and
M.J. Chaffin, “The Impact of Evidence-Based Practice Imple
mentation and Fidelity Monitoring on Staff Turnover: Evidence
for a Protective Effect,” Journal of Consulting and Clinical Psychol-
ogy, 77 (2) 270-280 (2009).
Mary E. Larkin** MS, RN, CDE, is the Manager of Clinical
Research and Chair of the TODAY Study Diabetes Educator
Committee, e-mail: [email protected], Karen Blumenthal,
BA, is a Research Assistant, and Denise Richards, MSN, FNP,
CDE, is a Nurse Practitioner and Diabetes Educator, at the
Massachusetts General Hospital Diabetes Center 50 Staniford
Street, Ste. 340, Boston, MA 02114. Paul McGuigan, BSN,
RN, CDE, is the Program Coordinator at Rainbow Babies and
Children’s Hospital CASE Medical Center. Kerry Milaszewski,
BSN, RN, CDE, is a Diabetes Educator and Laurie Higgins,
MS, RD, LDN, CDE, is a Diabetes Educator at Joslin Clinic,
Boston, MA. Jill Schanuel, M.Ed, is the Program Coordinator
at University of Oklahoma Health Sciences Center. Christen
Long, BA, is a Senior Research Assistant at George
Washington University Biostatistics Center.
* For the TODAY Study Group.
** To whom all correspondence should be addressed.
5. S. Pelke and D. Easa, “The Role of the Clinical Research Coordi-
nator in Multicenter Clinical Trials,” Journal of Obstetric, Gyne-
cologic, and Neonatal Nursing, 26 (3) 279-285 (1997).
6. M. Offenhartz, K. McClary, and C. Hastings, “Nursing and New
Realities of Clinical Research,” Nursing Management, 39 (11)
34-39 (2008).
7. H. Ehrenberger and L. Lillington, “Development of a Measure
to Delineate the Clinical Trials Nursing Role,” Oncology Nursing
Forum, 31 (3) 64-68 (2004).
8. F. Rico-Villademoros, T. Hernando, J. Sanz, A. Lopez-Alonso, O.
Salamanca, C. Camps, and R. Rosell, “The Role of the Clinical
Research Coordinator-Data-Manager-in Oncology Clinical Tri-
als,” BMC Medical Research Methodology, 4 (6) 2004.
9. C. Duane, M.A. Granda, D. Munz, and J.C. Cannon, “Study
Coordinators’ Perceptions of their Work Experiences,” The
Monitor, September 2007, 39-42.
10. J. Ahern, N. Grove, T. Strand, J. Wesche, C. Seibert, A.
Brenneman, and W. Tamborlane, “The Impact of the Trial
Coordinator in the Diabetes Control and Complications Trial
(DCCT),” The Diabetes Educator, 19 (6) 509-512 (1993).
11. A. Frydrych, J. Burrowes, J. Leung, S. McLeroy, D. Cock-
ram, L. Uhlin, S. Marjoram, B. Weiss, and J. Dwyer, “Dieti-
cians as Study Coordinators,” Applied Clinical Trials, March
2003, 60 -68.
ICON Medical Imaging
24 hours in the life of ICON
Project Director, Daniel, ensures that
the medical images and the patient’s
eCRF are ready for review by a
cardiologist for a type 2 diabetes trial.
3.28pmZurich, Switzerland.
When it’s 9.28am in Philadelphia, it’s 3.28pm in
our medical imaging core laboratory in Zurich,
where medical images, lab summaries, ECGs,
patient profiles and the eCRF are electronically
hosted for review by Clinical Endpoint
Committee (CEC) members located around
the globe. Our MIRATM CEC module provides
endpoint data to committee members in an
electronic auditable environment, regardless
of the location of the committee member.
No matter the hour of the day, there’s an
ICON expert somewhere around the world
working to deliver results for informed,
timely decision-making.
ICON Medical Imaging:www.iconplc.com/imaging

36 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
Sites
Workload
Measurement
Instrument
It is necessary to understand the time, staff, and financial resources required to conduct clinical trials.
Mary Coffey, Julie Berridge, James Lyddiard, and Jacqueline Briggs
CHAD BAKER/GETTY IMAGES
It is increasingly evident to all par-
ties involved in the sponsorship and
management of clinical trials that
a better understanding of the time,
staff, and f inancial resources re-
quired to conduct clinical trials is neces-
sary. The increasing use and complexity
of multi-modality treatment regimes, the rising
costs of clinical trials, the emphasis on the ef-
ficient use of available resources and adherence
to Good Clinical Practice (GCP), and increas-
ing regulatory requirements and demands for
quality assurance/control, have resulted in an
increased focus on workload issues. Failure to
address these issues has resulted in research
staff using unproven methods or a simple esti-
mation for determining workload, leading, in
some cases, to unrealistic expectations, exces-
sive workload, or inefficient use of resources.
The EORTC Clinical Research Coordinators
Group recognized the importance of address-
ing this problem based on understanding the
tasks involved, the time requirements, and the
resources necessary to effectively and efficiently
conduct clinical research. The development of a
workload measurement instrument (WMI) was
seen as a means of providing a tool by which
individuals could estimate more accurately the
time and resources required to participate in
clinical trials. The initial project was supported
by the EORTC and funded by a grant from Fonds
Cancer (FOCA).
The WMI was developed in seven
stages and the first stages: development,
validation and revision of a draft check-
list of trial related activities, drafting of
the WMI, a feasibility pilot study, and
analysis and revision of the trial related
tasks incorporated into the four modules
previously outlined in an Applied Clinical
Trials article that appeared in June 2008,
titled “Workload Measurement.”1 Coincidental to
the development of the WMI, Jacqueline Briggs
had developed a complexity tool for assessing
the complexity of a study prospectively.2 It was
agreed that, in the longer term, a joint workload
and complexity project would aim to indepen-
dently validate and link together the WMI and
the complexity tools.
This article describes the seventh stage of
development of the WMI; a prospective study
using the WMI to collect data for the purpose of
validating the four WMI modules.
Materials and methodsThe preparatory phase identified the specific
actions necessary and the financial and staff
resources required to complete the prospective
study. The Steering Committee members pre-
sented the prospective study outline to a meet-
PEERREVIEWED

appliedclinicaltrialsonline.com APPLIED CLINICAL TRIALS 37January 2011
ing of National Cancer Research Network Managers and
identified the networks that would be willing to collaborate.
Expression of interest questionnaires were sent out to all
UK network managers and to research staff in several Eu-
ropean centers to identify research staff and potential trials
for inclusion in the prospective study. Fifteen UK networks
and a center in Ireland initially agreed to participate in the
study and, of these, 12 networks returned completed mod-
ules as part of the prospective study.
The prospective study focused only on research related
activity and not on what would be considered routine care.
Workload was only recorded for research staff working on
the trials and excluded investigators, pharmacists, day care
staff, etc. These staff members were excluded as it was felt
that it would be difficult to collect accurate workload data
from such a wide range of staff and this was accepted as a
limitation for the purposes of this study.
As the joint project had been extended to include
complexity the four WMI modules (Module 1: planning
stage; Module 2: implementation stage; Module 3: trial
data management stage; Module 4: closure/final stage)
were reviewed. In order to facilitate the validation of the
complexity tool and create the necessary links between
the two tools, it was agreed to divide Module 2 into two
modules: 2a recruitment and treatment and 2b treatment
and follow-up.
A data collection period of six months was agreed and
the time frame for completion of data collection was Oc-
tober 2005 to May 2006. Prior to the commencement of
the data collection period, three training days were held
in Newcastle, London, Nottingham, and Wales to roll
out the study to the interested participants. Forty-three
Modules Returned
Module Title
Number
returned
1 Planning 17
2a Implementation—treatment 268
2b Implementation—follow-up 88
3 Trial data management 41
4 Closure/final 0
Source: Mary Coffey et al.
Table 1. A total of 414 completed modules were returned from collaborators from 27 hospitals covering 12 UK Cancer Research Networks.
ICON Central Laboratories
24 hours in the life of ICON
4.45pm
Laboratory Technician, Laila, prepares samples
for a Phase II study assessing the feasibility and
safety of a new drug in subjects with heart failure.
Tianjin, China.
When it’s 8.45am at our central laboratory in
Dublin, it’s 4.45pm at our central laboratory
in Tianjin, where chemistry samples for a
cardiovascular study are being tested. This
is just one example of how ICON Central
Laboratories provides global support for
clinical trials.
No matter the hour of the day, there’s an
ICON expert somewhere around the world
working to deliver results for informed,
timely decision-making.
ICON Central Laboratories:
www.iconplc.com/centrallabs

38 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
Sites
research staff attended these training days. Information
was provided individually for staff unable to attend the
training days.
From the training days and returned questionnaires, a
number of trials were selected on which the prospective
study would focus. For modules 1 and 4 it was agreed that
any trial in set up or at the closure stage could be included
due to the small number of trials likely to be at these
phases during the six month time frame. For modules
2 and 3, trials covering as many tumor types, treatment
modalities, and study types were selected to ensure as in-
clusive a range of activities as possible. A total of 36 studies
were identified and included in the prospective study.
Guidelines for the completion of each module were de-
veloped and circulated, together with the four modules and
the list of identified trials, to 70 collaborators, covering 15
networks that had agreed to participate. Collaborators were
asked to record the time taken, in minutes, for each indi-
vidual task or subtask undertaken as identified within the
modules. A subsection—other—was included for recording
any additional activities not identified within the modules.
A separate section recorded the hospital name, trial name
and number, the date for data collection commencement
and completion, the reason why data collection was ended,
and whether more than one form had been completed. This
allowed us to identify the total period
of data collection and subsequent anal-
ysis of workload for a single trial visit
or over the course of a trial period.
Data was entered into a database
developed in conjunction with the
NCRN IT department based on all the
identified tasks and subtasks of the
WMI modules. The NCRN agreed to
provide staff in order to complete the
data input and carry out some pre-
liminary data analysis and a system
for quality assurance of the data was
agreed upon.
The Steering Group met regularly
to review the progress of the prospec-
tive study, and as returned modules
were received, to carry out the initial
quality assurance procedures. All re-
turned modules were double-checked
to ensure accuracy, and when tasks
or subtasks were entered in an in-
correct section these were noted and
revised prior to entry onto the da-
tabase. Incorrect or unclear entries
were deleted. Regular contact and
feedback was maintained with the
collaborators throughout the study
by e-mail, newsletters including answers to frequently
asked questions, and presentations at Cancer Research
Network Managers’ meetings.
ResultsA total of 414 completed modules were returned from col-
laborators from 27 hospitals covering 12 UK Cancer Re-
search Networks. Three networks or centers did not return
Summary of the Changes Made
Number of subtasks
on which changes
were made
Number of times a
change was made to
the same subtask
57 1
11 2
2 3
1 5
1 9
1 15
1 16
Source: Mary Coffey et al.
Table 2. Cumulatively, 130 changes were made.
Subtask Completion per Module
Number of times
a subtask was
completed
Modules
1 2a 2b 3
> 10 10 2 4 11
11-20 3 3 2
21-30 3 2 1 1
31-40 4 1
41-50 4 3 1
51-60 4
61-70 2 2 2 1
71-80 3
81-90 3 1
91-100 1
101-200 14 1
200+ 16 1 1
Source: Mary Coffey et al.
Table 3. For Module 2b and 3, the most frequently completed subtasks related to case report form completion, photocopying and sending trial documents, and the preparation and submission of trial amendments.

www.PRAinternational.com / +1 (919) 786-8200 US / +44 (0) 118 918 1000 EU
the global reach you need with THE PERSONAL ELEMENT you expect
PRA’s therapeutic expertise, experienced project teams and our differentiating
PERSONAL ELEMENT enable us to deliver for our clients. This unique
PRA philosophy –THE PERSONAL ELEMENT– recognizes that true, quality
service comes from trained, empowered and dedicated employees using
innovation and personal commitment to accelerate the development life cycle.
Isn’t it time you experienced THE PERSONAL ELEMENT?
Your Full Service
Clinical Research Partner
Meet Paola:
Located in
Victoria, Canada–
one of PRA’s 38
offices worldwide

40 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
Sites
completed modules due to merger of networks, shortage of
staff, or excessive workload issues. Data was returned on
35 of the 36 studies identified for inclusion in the prospec-
tive study. Table 1 shows the modules returned.
As part of the analysis process a series of assumptions
were made. These included: research staff were experi-
enced and trained and not involved in the actual delivery
of treatment, research activity was additional to standard
treatment, and hospital support services and standard
equipment were available and accessible to research staff.
Cumulatively, 130 changes were made in the 74 sub-
tasks (Table 2). These changes included transfer from one
subtask to another where an entry was incorrect, deleting
investigators, and separating out multiple patient visits into
individual visits. The highest numbers of recording errors
(9, 15, and 16) necessitating transfer related to the record-
ing of administration activities in other subtasks rather
than administration activities.
Following extensive quality assurance procedures all
tasks and subtasks within Modules 1, 2, and 3 were vali-
dated as relevant and appropriate with no tasks or subtasks
removed. All subtasks were recorded at least once with a
very wide range within each module. For Module 1, the
most frequently completed subtasks were those relating to
the preparation and submission of documentation to Ethics
and Research and Development departments. Conversely
the lowest recorded tasks related to organizing and attend-
ing meetings other than in-house meetings for information,
training, and trial activation.
For Module 2a, the most frequently completed subtasks
related to screening for eligibility, informed consent, and
sample preparation. This was consistent with the expecta-
tions and personal experience of the project group. The
least completed subtasks in Module 2a related to liaising
and verifying radiotherapy dose reductions and missed
treatment which was anticipated given the very low num-
bers of radiotherapy related trials included in the study.
For Module 2b and 3, the most frequently completed sub-
tasks related to case report form completion, photocopying
and sending trial documents, the preparation and submis-
sion of trial amendments, and updating study documents
following amendments (Table 3).
Two major revisions were identified as necessary. The
first change related to the recognition of the importance
given to administration and communication by the collabo-
rators. The section “other” consistently included additional
administration and communication and it was agreed that
these two activities should be included as subtasks for all
main tasks in the final modules. In total, 110 transfers were
made to administration main tasks and 230 to administra-
tion subtask activities; 38 to communications main task,
with 100 to communication subtask activities. The second
change was the recombination of Module 2a and 2b with
specific sections relating to consent, treatment, and follow-
up incorporated—confusion had arisen in completion of
these as two separate modules.
RecommendationsModules 1, 2, and 3 of the workload measurement instru-
ment have been validated and are now complete. These
modules are available in their entirety online in PDF format
at appliedclinicaltrialsonline.com as part of the online ver-
sion of this article. Module 4 has been revised in accor-
dance but would benefit from validation as part of a specific
prospective study as trials reach closure stage.
It is acknowledged that there were limitations to the
prospective study that included the short data collection
window of six months, the exclusion of principal investiga-
tors and other associated staff from the data collection
exercise, compounded by the difficulty associated with
specific local hospital issues all had potential to confound
the data collected. It was accepted that these factors would
contribute to workload but would not necessarily alter the
tasks and subtasks identified for inclusion in the modules
and, therefore, such confounders were not considered sig-
nificant for the purpose of the WMI validation. For hospi-
tals or departments undertaking a workload analysis in the
future it would be appropriate to take these confounders
into account.
This WMI was developed to be a generic tool and can be
used locally, nationally, or internationally to review the trial
workload of an individual researcher, team, hospital, or
network of centers. It should inform discussions at all levels
and allow centers considering implementing new or ad-
ditional clinical trials to accurately evaluate the associated
workload and to allocate staff and resources accordingly.
References1. Julie Berridge and Mary Coffey, “Workload Measurement,”
Applied Clinical Trials, June 2008, 98-101.
2. Jacqueline Briggs, “Real World Workload Needs: Developing a
process and management tool for scoring complexity in cancer
clinical trials,” Applied Clinical Trials: Oncology & Clinical Trials
in the 21st Century, supplement, May 2008, 22-24.
Mary Coffey* is Head of Discipline at Division of
Radiation Therapy, School of Medicine, Trinity Centre for
Health Science, St. James’ Hospital, Dublin 8, Ireland,
e-mail: [email protected]. Julie Berridge is Clinical Trials
Team Manager at Mid Trent Cancer Research Network,
Nottingham City Hospital, United Kingdom. James Lyddiard
is Head of Cancer Trials at University College London
Hospitals, NHS Foundation Trust. Jacqueline Briggs is Stroke
Research Network Manager at Peninsula Stroke Research
Network, Royal Devon and Exeter Foundation NHS Trust,
Exeter, United Kingdom.

performance is a virtue{ }
1-888-345-2567 DaVitaClinicalResearch.com
The DaVita Clinical Research (DCR) Central Lab features the latest in analytical methodology and technology. Our investments in both equipment and our over 47,000-square-foot facility allow us to generate a daily test volume of approximately 144,000 tests on 60,000 samples per day. Each and every clinical project has a project manager to ensure that client-specific requirements are met and communication is maintained. Our convenient data access system allows fully compliant order entry and reporting anytime, anywhere.
DCR is always striving for innovation, and our latest milestone at the Central Lab is green packaging for samples. The unique green packaging features IATA-compliant, storage-friendly design that results in significant shipping cost reduction.
At the DaVita Clinical Research Central Lab, we
are dedicated to conducting each project on time.
High Throughput and Customer Service
Timeliness is a Virtue with the
DaVita Clinical Reseach Central Lab.

42 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
Sites
Increase African American Enrollment
Recession and acquisitions make recruiting America’s second-largest minority even harder.
Patricia R. Sanders
ANDERSEN ROSS/GETTY IMAGES
Recruitment of African Ameri-
cans into clinical tråials is go-
ing through another evolution.
With global patient outreach
far from peaking, the unchar-
tered growth of outsourcing overseas for
patient recruitment is beginning to raise
genetic issues at home.1 As American pharma-
ceutical and biotech companies rapidly expand
to other parts of the world, recession and acquisi-
tions compromise efforts to recruit hard-to-reach
American minority patients for clinical trials.
African Americans make up the second larg-
est minority group in the United States—in-
creased by 13 percent between 2005 and 2006.
More than 45 percent of America’s population is
non-white or classified non-Caucasian. In some
states, African Americans can make up as much
as 30 percent to 60 percent of the residents.2
Yet, too many clinical study results, related to
diseases critical to African Americans, show as
few as 2 percent recruitment of African Ameri-
cans, or vaguely stated as 9 percent “other” or
“non Caucasian.”
Illnesses such as asthma, diabetes, hyperten-
sion, HIV-AIDS, and certain kinds of cancer af-
fect African Americans more than other people.
Little is known about the ways African Ameri-
cans respond to treatment for these and other
conditions. Despite government regulations that
require minorities to be included in federally
funded research projects, African Americans re-
main underrepresented in these critical projects.3
Most clinical research sponsors are
aware of this shortfall, and admit there
is a problem. Yet many don’t specify or
request even 10 percent to 15 percent of
African Americans in studies unless there
is a special protocol, or unless it relates to
HIV-AIDS, sickle cell anemia, and certain
cancers. Setting minimum requirements
with your team is the first step in the complex
chain to reach African American participants.
With the 2010 US Census expected to assert-
ively focus on hard-to-reach minorities and un-
derserved populations,4 the results are predicted
to reveal even higher numbers of minorities than
in the past. If so, the omission of mandatory
clinical recruitment policies regarding African
Americans and minorities will be somewhat like
playing Russian roulette with an entire popula-
tion. Though efforts such as EDICT5 (Eliminat-
ing Disparities in Clinical Trials) has begun to
recommend new policies, changing the present
scenario requires due-diligence and creative
partnerships, both within and outside of this
clinical trial and cultural void.
In a recent health disparities symposium on
cancer, David Satcher, MD, PhD, Director of
the Satcher Health Leadership Institute, More-
PEERREVIEWED

It’s a matter of the heart.
The scientific evidence is clear:
Elevated central blood pressure is superior to brachial pressure as a predictor of cardiovascular events.
Central pressure cannot be determined through cuff pressures taken at the arm.
Drugs affect central and brachial pressures differently.
In clinical trials, it is vitally important to measure the pressure the heart, brain and kidneys actually experience.
We provide SphygmoCor®, the gold standard in noninvasive central pressure and pulse wave velocity technology, site training and real-time quality assurance with the AtCor WISDOM system.
Why Measure Central Blood Pressure?
www.atcormedical.com T 630.228.8871
VISIT US AT THE ASH ANNUAL MEETING BOOTH 1106
SphygmoCor measures ascending aortic pressure noninvasively, at the radial artery.

44 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
Sites
house School of Medicine in Atlanta, GA, spoke on “A
Right to Care.” He outlined significant barriers to health-
care of African Americans in the United States that he
calls the “UNs:” uninsured, underinsured, underserved,
and underrepresented.5
Satcher stated that 40 million Americans are uninsured;
25 million underinsured. “Doctors tend to clump together
where it’s comfortable and usually it’s not near the under-
served,” he said.
“Over the past 10 years, black doctors (and nurses) are
underrepresented in our healthcare system, and we are not
making significant progress in that area.” When seeking
healthcare or in clinical trials, it is important that a person
see themselves represented in the healthcare system.
Minority educationEliminating racial disparities in clinical trials begins and
ends at the top, with education. Educating the doctors and
medical providers is a start, but it ’s
not enough. It is critical to begin the
educational process with sponsors of
clinical trials. They could set the bar
higher by first requesting, and then
requiring larger numbers of African
Americans pre-screened for all trials
for diseases critical to this population.
The problem with recruiting and
retaining African Americans in clini-
cal trials should be viewed as the
“problem with us”—those respon-
sible for clinical recruitment, rather
than the “problem with them.” Find-
ing solutions should be a multi-level,
multi-tasking function of the sponsor;
recruitment team; clinical research or-
ganization’s or patient research orga-
nization’s vendors; project managers;
and local site investigators, all working
in concert toward this goal.
With new drug discoveries in the
pipeline, many offering hope for Af-
rican Americans,6 recruit ing them
requires new strategies that provide
ground-zero opportunities across the
board, and with the highest ROI—one
that will bridge cultural gaps.
Outreach strategies The investment return for expanding
minority outreach can dramatically
increase if that expansion includes
strategies for a closer, personal, and
more trusted outreach to venues such
as black churches and community health partnerships.
This outreach could logically make the difference be-
tween 2 percent or 10 percent recruitment of minorities in
that community.
If sponsors of trials want to build and sustain trust for
future trials, they should tap into community health net-
works that already provide local health education about
diseases. Look into trial outreach through black profes-
sional newsletters, flyer distribution to partnered church
health initiatives, and community organizations. Use site
investigators as resources. This will make a trial more
important to the community than other trials trying to re-
cruit from a distance.
Sometimes, for example, local site investigators are
already involved with these organizations. A community-
involved site investigator means there is already an impor-
tant trust factor present. Something as simple as a brief site
investigator survey could produce a treasure of resources.
C.E.D.R.I.C.T Quick Facts
C.E.D.R.I.C.T. (pronounced ced’rick) (Coalition to Eliminate Disparities and to Research
Inclusion in Clinical Trials) is a national, three-year pilot field research study on how to
increase clinical participation and retention through the education of African Americans
in clinical and medical trials.
C.E.D.R.I.C.T., a National Physician and Family Referral (NPFR) Project, began in June
2009, collaborating with National Black Leadership Initiative on Cancer (NBLIC III),
Morehouse School of Medicine, Center for Information and Study of Clinical Research
Participation (CISCRP), National Medical Association (NMA) Project IMPACT , and
National Human Genome Center at Howard University.
Through this field research study, a model for African Americans in Clinical Trials
(AACT)—pronounced ACT—a coalition pilot will be developed in key cities. The
intervention will serve as a community model for ongoing recruitment and retention of
African American and minority participants.
C.E.D.R.I.C.T. will reach over 10 million African Americans and survey over 20,000 during
the three-year period. The field research will both validate and define previous data
about fears or apprehensions about participating in medical research. It will also bring
new data on ways to eliminate the health disparities of African Americans in clinical trials.
The potential impact: C.E.D.R.I.C.T. responds to the missing pieces of the puzzle
that identifies barriers, as seen by African Americans themselves, and creates access
to networks of coalitions to assist them in becoming more educated about clinical
trials. With access to these coalitions, disease therapy education and clinical research
recruitment becomes easier as it expands into target populations.
C.E.D.R.I.C.T. is not a scientific, academic or medical research. It is conducted by
nonprofit companies with years of successful work in patient education, clinical trials
outreach, and recruitment of African Americans; utilizing dozens of community-based
and medical networks around the country.
Source: Patricia R. Sanders
Table 1. C.E.D.R.I.C.T. evolved to gather face-to-face data on African
Americans nationally.


46 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
Sites
Where site investigators are involved in the commu-
nity, there will be a greater access to African American
patients. Likewise, patient recruitment of this population
could increase dramatically in key states7 if project man-
agement is focused upon identifying, training, and funding
African American physician investigators already involved
in the community.
A new ground-zero field research, called C.E.D.R.I.C.T.,
pronounced CED’ rick, [Table 1] (Coalition to Eliminate
Disparities and to Research Inclusion in Clinical Tri-
als) has evolved to gather face-to-face data on African
Americans nationally. The initial surveys observed three
obstacles that must be tackled for better patient recruit-
ment. It also has observed three keys to addressing these
obstacles. The obstacles are trust, interest, and opt-in op-
portunities. The keys are disease, patient, and community
education.
Developing an outreach to recruit minorities for clinical
trials, while at the same time creating trust often relies on
media data that does not provide a true picture of potential
African American clinical trials participants. So we take
the standard shortcut when looking for minorities: Adver-
tise in black media.
Advertising is a proven outreach strategy and it works
on many fronts. However, the obstacle of trust cannot be
overcome solely by talking to African Americans about a
clinical trial between R&B songs. Trust involves an “in-
your-face” approach to such an intimate undertaking as
participating in a clinical trial. And for many minorities this
is not an option.8
Elise D. Cook, MD, Chair, Minority and Medically Un-
derserved Subcommittee, for SELECT trials9 was part of
the team that developed focus groups to get input from
men in target population(s). During the study, ways to
enhance minority recruitment were explored and three
one-day minority recruitment workshops were developed,
along with community partnerships with NBLIC II and
others [see sidebars]. They found that trust was built
among participants where open and ongoing communica-
tions evolved, and continued with participants even after
the trials ended.
Developing ethnic-focused communication toolsTools for developing ethnic-focused, community-based
project management could be as simple as creating a selec-
tion of educational trials flyers, posters, brochures, or pam-
phlets for distribution by your “community-involved” site
investigators in their communities.
Familiar, face-to-face exchange and distribution of cul-
turally-sensitive information, both in doctor’s offices and
the community, presents huge recruitment opportunities
toward establishing trust among African Americans for
multiple diseases.
Support project management by providing what is known
as an 800 ERN (Educational Referral Number) to buttress
the unfamiliar pre-screening interview. The ERN allows
participants to ask questions and allows for smoother tran-
sition into pre-screening. Utilizing an 800 ERN throughout
the recruitment campaign could be a positive, escalating
educational tool.
Appropriate city and site selection is critical. Unfortu-
nately, it’s often easier and quicker to stick with the famil-
iar sites. If you are looking to recruit African Americans,
selecting a site in the suburbs, as opposed to one with a
heavy concentration of African Americans, can present
Focus Groups
■ Input from men in the target population
■ 78 men participated: 16 African American and 32
from the Veteran’s Administration Hospitals system
■ Recommendations regarding communications
– Highlight personal incentives
– Explain why the study supplements were chosen
– Provide frequent study updates
– Include family members, especially spouses
– Special strategies for recruitment of minority,
low literacy, low income, and medically under-
served men
Partnership with NBLIC II
■ Minority outreach initiative of the NCI
■ Innovative outreach strategies partnering with the
local SELECT sites
– For Men Only retreats, Wellness on Wheels, and
Taking it to the Top,
■ Promotional items for events
– T-shirts, squeeze water bottles, and caps with the
SELECT logo
Minority Recruitment Workshops
■ Three 1-day workshops
– Round table discussions
• Share strategies, develop mentoring relation-
ships, and discuss problems
– Panel discussions with local community leaders
and SELECT Investigators
• Share recruitment ideas
– Disseminated workshop proceedings to all SELECT
staff at the semi-annual SWOG/SELECT Workshops

20
To Register for the 2011 program and place your nomination
for the Hall of Fame Awards, visit us online at
www.clinicaltrialpartnerhsips.com
NOMINATION CATEGORIES
Announcing the
1st Annual Partnerships Hall of Fame Awards
Partnerships in Clinical Trials event will host it’s
1st Annual Partnerships Hall of Fame Awards
ceremony to honor and celebrate the Partnerships
MVPs throughout the past 20 years.
Technology and Innovation
Lifetime Achievement
Operational Excellence
Change Management
Most Valuable Attendee
-ARCH��� !PRIL���������s�0HOENIX�#ONVENTION�#ENTER�s�!RIZONA

48 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
Sites
obstacles for participation. Finding sites that are within a
comfortable distance from African American communities
could be a matter of finding African American site doctors
and then helping them to outreach for your trial.
Sponsors could increase their chances for successful
minority recruitment by making mandatory a percentage
of investigators who are both African American doctors as
well as non-minority physicians in areas with large African
American patient bases. Applied Clinical Trials’ Editor-in-
Chief Lisa Henderson, aptly noted in May 2008 that “trial
availability in that community; physician participation in
the trial; and finally, being able to meet the criteria,” were
elements in successful recruitment of African Americans
in an oncology trial.10
Sparking interest is an elusive obstacle that is best fa-
cilitated through site community partnerships. The ques-
tion arises, “If 30% to 70% of (minority subjects) say they’d
be willing to be in a clinical trial...why do so few actually
enroll?”11 Of the African Americans surveyed, over 40%
stand firm on willingness to participate in clinical trials if
someone asked them. However, 92% are firm about their
willingness to participate if they had more information
(education) before they are called to pre-screen. Clearly,
this is an important key.
Creating an interest in clinical trials participation among
African Americans requires face-to-face exchange for
maximum effectiveness. It then becomes the question of
how to develop techniques that impact African Americans
targeted for inclusion. The residual benefits of shifting a
small percentage of the site project management resources
to a community ethnic-focused campaign will translate to
a greater ROI on current and future trials. As FDA guide-
lines become more inclusive, this shift will also avoid wast-
ing time and money backtracking later in order to recoup
minority participants for final drug approval.
With the new Health Insurance Portability and Account-
ability Act (HIPPA) regulations, outreaching to gain minor-
ity interest in clinical trials without perks and incentives
requires building strong community partnerships. Often
this is done directly at the project management and site
investigator levels.
The most profitable investmentThe third obstacle, creating opt-in opportunities, directly
impacts patient recruitment vendors and site investiga-
tors. Inf luencing African Americans to opt-in to a da-
tabase or referral list for trial participation can be site-
based, event-based, web-based, or via sponsor’s patient
recruitment vendors.
When trial sponsors outsource to clinical and patient re-
cruitment organizations, they are hoping these vendors are
able to pull their trials across the invisible line of “minimum
requirements” for African Americans and minorities. For
some trials (and a few diseases), this happens. Taking re-
sponsibility for minority patient recruitment at the beginning
helps sponsors and project management teams take control.
Clinical trial participant databases identif ied as ex-
clusively African Americans are rare. However, one re-
cent educational outreach that evolved from the 2009
C.E.D.R.I.C.T. field research is, “African American Health
Matters.” African American Health Matters is an opt-in
mobile health text message program that sends health re-
minders and tips to over 25,000 subscribers about selected
health matters. Fifty-eight percent of this audience is not
on the Internet, but 84 percent have cell phones.
Text messages also offer toll-free numbers and websites
to find disease educational materials, clinical trials remind-
ers, and positive reinforcement messages designed to help
participants maintain a positive mental attitude, an impor-
tant element of good health.
Planned involvementSponsors and recruitment organizations should adhere
to quality checks of their minority patients and physician
databases. Vendors should keep updated information about
targeted African American participants and doctors for
referral to trials. Look at track records. Whether perfor-
mance-based plus community advocacy or advertisement-
based recruitment, the yardstick for a vendor’s ability to
recruit for multiple racial populations is database develop-
ment of specialized audiences.
Sponsors should require “minimum goals” for recruit-
ing African Americans in all US-based trials. The national
average population of African Americans is around 12%,
and over 100 cities have more than 30%. With these num-
bers, recruiters should consider requiring at least 10%
participation for diseases with high mortality rates in this
population. This requirement will present new recruitment
opportunities and offer increased education for critical dis-
eases such as diabetes, hypertension, cholesterol, asthma,
arthritis, obesity, and tobacco use.
In C.E.D.R.I.C.T.’s initial field surveys, other diseases
were found to be of interest: orthopedic, cardiovascular,
prostate related, breast, lung and colon cancers, gastric,
menopausal, post menopausal, addiction, and depression
trials. The point is to reach out initially with multiple dis-
eases in multiple cities in order to identify your new patient
populations. You’ll then find the community hierarchy that
offers access for future trials.
Creating interest in clinical trial participation among African Americans requires face-to-face exchange.

“A highly informative and educational forum for anybody wanting to learn about, or keep up with, rapidly emerging global clinical trials disclosure requirements.”
— Previous Attendee, Penny Clarke, Head of Integrated Systems Support, GlaxoSmithKline
A global evolution of
transparency and
disclosure…
Organized by: Lead Media Partner: Sponsors:
A subsidiary of
Register at www.cbinet.com/ctrreu
Clinical Trial Registries and Results Databases
CBI’s 3rd Annual Forum on
CBI’s 6th
Forum on
“Excellent, comprehensive conference discussing U.S. and international requirements and updates regarding registration and result disclosure of clinical trials.”
— Previous Attendee, Shalini Jain, Associate Director, Gilead Sciences, Inc.
Register at www.cbinet.com/ctrr
From the U.S. to the UK, we’ve got you covered!

50 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
Sites
Disease, patient, and community educationThe obstacles are not insurmountable to recruiting Afri-
can Americans into clinical trials. However, the obstacles
must be overcome to avoid playing Russian roulette with
this population. How? By initiating proven market strate-
gies that work on many levels. When a company is willing
to give minority recruitment more than a cursory glance,
there are keys that will help them move forward:
Key one. Start with disease education related to the trial.
African American churches with health ministries score
big points for trust and openness. For a trial targeted to
grass-roots participation, a study flyer with trial and dis-
ease facts, and ERN numbers for pre-screening consulta-
tion is extremely valuable information at African American
churches or local health fairs.
Key two. Follow up with more patient education about
the clinical trial being conducted. This can be done with
various clinical trials recruitment outreach tools such as
trial information on black websites and community media
that cater to African American audiences, phone surveys,
web, or e-mail announcements and mobile messaging. Paid
advertisements can support this effort, but should never be
used as the primary recruitment mechanism. Also, recog-
nize the many community levels for event ads and outreach.
Key three. Keep your community network open and ac-
tive. Once you’ve established a community partnership
within selected African American communities, follow
through with each disease trial. Success depends not just
on the clinical trial, but also upon your community relation-
ship. From the relationship comes trust; from trust comes
word-of-mouth, which equals interest. From the right selec-
tion of sites and site investigators comes a cost-efficient, fo-
cused outreach support that the sponsor or patient recruit-
ment vendor can provide its sites.
ConclusionIn summary, recruiting African Americans into clinical
trials is not rocket science. However, it takes focus, commit-
ment, and a plan to develop your minority outreach around
your existing site resources by:
• Outlining ways to include African Americans, look for
strategies for inclusion and retention in your key cit-
ies by site project managers and patient recruitment
organizations.
• Developing the networks you may already have in place
in the communities with people who “talk their lan-
guage,” and with an outreach that focuses upon disease
education and health support resources.
• Supporting ground-zero opportunities in your site com-
munities with custom, IRB approved trial information
and disease education materials. Most importantly, en-
courage site outreach programs and offer bonuses and
incentives for qualifying African American doctors and
for outreach to new participants.
References 1. Tom Watkins, “Growth of Clinical Trial Outsourcing Raises
Issues,” CNN Health.com, February 18, 2009.
2. United States Census, 2000.
3. Center for Information and Study on Clinical Research Partici-
pants (CISCRP), Participant Newsletter, February 2008.
4. Associated Press, March 23, 2009.
5. David Satcher, “A Right to Care” (speech, Health Disparities Sym-
posium on Cancer: Addressing the Issues, September 21, 2009).
6. “Medicines in Development for Major Diseases Affecting Afri-
can Americans,” APC Report, 2007.
7. United States Census, 2000.
8. NPFR and C.E.D.R.I.C.T. Field Research 2010, http://www.
npfrproject.org.
9. Elise D. Cook, “Recruiting African American Men to a Cancer
Prevention Trial” (lecture, University of Texas, June 15, 2009)
10. Lisa Henderson, “Trials Where they Make Sense,” Applied
Clinical Trials Online, May 1, 2008, http://appliedclinical-
trialsonline.f indpharma.com/appliedclinicaltrials/News/
Trials -Where-They-Make-Sense/ArticleStandard/Article/
detail/513696.
11. Mark Hochhauser, “Self Deception Syndrome,” Applied
Clinical Trials Online, Nov 1, 2004, http://appliedclini-
ca lt r ia lsonl ine. f indpharma .com/appl iedcl in ica lt r ia ls/
Patient%2fSubject+Recruitment/The-Self-Deception-Syn-
drome/ArticleStandard/Article/detail/131504
Patricia R. Sanders, APR, Senior Consultant, P&E Associates,
14902 Preston Road, #404-744, Dallas, TX, 75254 e-mail:
Recruiting African Americans into clinical trials takes focus, commitment, and a plan to develop minority outreach.

appliedclinicaltrialsonline.com APPLIED CLINICAL TRIALS 51January 2011
Community
BUSINESS AND PEOPLE UPDATE People ◗ Biomedical Research Al-
liance of New York (New
York, NY) has made sev-
eral new hires including
Carmela Houston-Henry
as Business Development
Director and Rich Green as
Central IRB Business De-
velopment Director.
◗ Pamela Pannier has joined
Clinical Trials of America (Eu-
gene, OR) as Clinical Opera-
tions Director and Donald
Dickerson has joined as the
company’s new President.
◗ With over 20 years of
sales, marketing, and busi-
ness development experi-
ence within the pharmaceu-
tical arena, Rick Coulon has
been appointed Director of
Business Development at
PharmOptima (Portage, MI).
◗ Previously Chief Operat-
ing Officer of Clinigene, A.
S. Arvind, MD, has been ap-
pointed as Strategic Advisor
of Ecron Acunova (Banga-
lore, India).
◗ Making several additions
to its team, AAIPharma
Services (Wilmington, NC)
has appointed Tim Martin as
Executive Vice President of
Sales and Marketing, and
Rob Goshert as Vice Presi-
dent of Corporate Accounts.
◗ To streamline the recruit-
ment “pull-through” process
and help study sites and
sponsors succeed with their
patient recruitment efforts,
MediciGlobal (Philadelphia,
PA) has opened the Study
Resource Center and hired
Pat Patterson as its Director.
◗ Pharma Tech Industries
(Royston, GA) has ap-
pointed Bryan J. Cox as
Staff Engineer.
◗ James W. Lovett, General
Counsel of Covance, has
been appointed to BioCli-
nica’s (Newtown, PA) Board
of Directors.
◗ Edward Masterson has
joined Alliance Life Sciences
Consulting Group (Bridge-
water, NJ) as Senior Vice
President of Consulting
Operations where he will
oversee all aspects of
ALSCG consulting ser-
vices, including solution
development and service
delivery to clients.
◗ Bringing with her over
18 years of strategy experi-
ence, Rosemarie Truman
has been hired as Advanced
Clinical‘s (Deerfield, IL)
Executive Vice President
of Solutions.
◗ The Society for Clinical
Data Management (Mil-
waukee, WI) has appointed
Nimita Limaye and Ludo
Reynders, PhD, as Chairs for
its Board of Trustees.
◗ CTI Clinical Trial and
Consulting Services
(Cincinnati, OH) has made
several changes to its
team. Meredith Boley and
Robert McRae have joined
as Research Associates
and Bill Aronstein has
been promoted to Senior
Medical Director.
◗ Ricerca Biosciences (Con-
cord, OH) has appointed
William DeMaio, PhD, as
Senior Director of the Drug
Metabolism and Pharma-
cokinetics Department and
has appointed Douglas K.
Fuhrer, PhD, as Senior Di-
rector of Drug Safety.
◗ Ludo Reynders, PhD,
has joined the team at
Premier Research Group
(Philadelphia, PA) as Chief
Executive Officer.
◗ ClinPharm Consulting (Re-
search Triangle Park, NC)
has hired Giulia Ghibellini,
PhD, to implement a new
population pharmacokinet-
ics service.
◗ David Evans, Chief Infor-
mation Officer at Octagon
Research Solutions (Wayne,
PA) was appointed as
Chair to the CDISC Ad-
visory Board and Monica
Garrett, Vice President,
Global Marketing, Octa-
gon, was elected to the
position of North America
Representative on the
Board of Directors.
Alliances• Covance (Princeton, NJ)
has signed definitive agree-
ments with sanofi-aventis
(Paris, France) for Covance
to become sanofi-aventis’
R&D partner.
• Covance (Princeton, NJ)
and INphoton (Indianapolis,
IN) have entered into an alli-
ance that will grant Covance
exclusive global access to
INphoton’s intravital micros-
copy imaging technology
and expertise.
• BioClinica (Newtown, PA)
has signed a three-year,
multi-million dollar agree-
ment for enterprise-wide
EDC technology and data
management services with a
top 10 pharmaceutical com-
pany in which BioClinica
Express will support nearly
200 studies annually for this
organization.
• Cato Research (Durham,
NC) has selected Bio-
Clinica’s (Newtown, PA)
clinical trial management
system platform to help
A.S. Arvind, MDRick CoulonPamela PannierCarmela Houston-Henry

52 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
Community
streamline workflow and
facilitate the clinical study
processes.
• Richmond Pharmacology
(London, UK), Community
Research (Cincinnati, OH),
and Fundación de Investig-
ación de Diego Puerto Rico
(San Juan, Puerto Rico)
have selected Logos Tech-
nologies’ (London, UK)
ALPHADAS’ early phase, e-
source data capture system,
and site automation soft-
ware suite to accelerate and
streamline their clinical trial
operations and services.
• Charles River Laboratories
International (Wilmington,
MA) has entered into an
exclusive, long-term mar-
keting and distribution
agreement with Transposa-
gen Biopharmaceuticals
(Lexington, KY).
• PPD (Wilmington, NC)
has established an agree-
ment with the Himalayan
Institute and Hospital Trust
(Uttarakhand, India) to
expand its network of inves-
tigators in the region.
• PPD (Wilmington, NC)
and VirtualScopics (Roch-
ester, NY), have formed a
strategic alliance to deliver
a comprehensive set of clini-
cal and medical imaging
services that will enable
biopharmaceutical compa-
nies to make faster, more
confident decisions on the
development of their oncol-
ogy compounds.
• Dako (Glostrup,
Denmark) and Quintiles
(Durham, NC) have
formed a strategic alliance
to advance personalized
medicine by collaborating
on the co-development
of targeted therapies and
companion diagnostics.
Awards• Rabinder Buttar, PhD,
President and CEO of
ClinTec International
(Glasgow, Scotland), was
named Female Business
Leader of the Year at the
2010 Scottish Leadership
Awards held in Glasgow.
• Mid*Lands IRB (Overland
Park, KS) has been awarded
accreditation by the Asso-
ciation for the Accreditation
of Human Research Protec-
tion Program.
• Almac’s (Souderton, PA)
Clinical Technologies busi-
ness unit, a part of Almac
Group, has been named one
of the Best Places to Work
in PA for 2010.
Company News• The European Medicine
Agency (London, England)
and the European Network
of Centers for Pharmacoepi-
demiology and Pharmaco-
vigilance (London, England)
have awarded the first EN-
CePP study seal to an obser-
vational study researching
hospitalized patients with
Chronic Obstructive Pulmo-
nary Disease.
• A Phase III trial for Ae-
gerion Pharmaceuticals
(Bridgewater, NJ) that was
conducted by ACR Image
Metrix (Philadelphia, PA)
was published as an ab-
stract in the online supple-
ment of Atherosclerosis
and presented at the 78th
European Atherosclerosis
Society Congress.
• The former management
team for Addrenex Phar-
maceuticals has launched
a new company, Neuronex
Inc. (Morrisville, NC), a
specialty pharmaceutical
company that develops and
commercializes drugs to
treat central nervous system
diseases and disorders.
• US Oncology (The Wood-
lands, TX) has enrolled the
1,000th patient in a Phase I
clinical trial through its US
Oncology Research Network.
• Galderma (Fort Worth,
TX) has standardized on the
Medidata (New York, NY)
Rave electronic data capture
and clinical data manage-
ment platform.
• Almac’s Clinical Technolo-
gies Division has moved into
the Almac Group’s new
North American Headquar-
ters in Souderton, PA. The
company has also success-
fully completed an inspec-
tion of its Clinical Services
UK facility, located in
Craigavon, by the Medicines
and Healthcare products
Regulatory Agency.
• Perceptive Informatics
(Boston, MA) has incor-
porated IBM’s WebSphere
portal and Tivoli Access
Manager into its eClinical
platform, which provides
support for its eClinical
Suite.
New Facilities• Partnering with Sun Labs
(Menlo Park, CA), Oracle
(Redwood Shores, CA) has
created the Oracle Health
Sciences Institute in order
to focus on research that
will accelerate IT innovation
to advance personalized
medicine and drug delivery.
• PPD (Wilmington, NC)
has opened an office in No-
vosibirsk, Russia in order
to strengthen its presence
in the region. The company
has also consolidated its
clinical development opera-
tions in Beijing, China, in a
new, larger office to support
its growing client base in
the country and throughout
Asia Pacific.
• Clinical Research Ad-
vantage (Tempe, AZ) has
expanded into the Omaha/
Council Bluffs market with
the opening of three local
area offices in Omaha, Bel-
levue, and Council Bluffs.
Products• Trianz Solutions (Herndon,
VA) has released Version
6.1 of the Acceliant eClini-
cal Suite for web-based
clinical trial management
and data collection. The
new version of Acceliant
provides trial builders the
ability to define and import
CRF metadata in commonly
available formats.
• Oracle Health Sciences
(Redwood Shores, CA)
released Oracle Clinical De-
velopment Analytics 2.0 and
Oracle Life Sciences Data
Hub 2.1.4
• BioClinica (Newtown, PA)
has released its new IVR/
IWR platform, Trident IWR,
whose interface provides
clinical operations person-
nel with a way to directly set
up, monitor, and maintain
randomization and supplies
for clinical trials.
• PharmaVigilant (Westbor-
ough, MA) has enhanced
its InSpire electronic data
capture system to support
multiple languages for the
management of complex,
large-scale global trials.
• Pegasystems (Cambridge,
MA) released its Adverse
Event Case Processing
solution that collects, man-
ages, and analyzes adverse
events both during and af-
ter clinical trials.

20
To Register for the 2011 program and place your nomination
for the Hall of Fame Awards, visit us online at
www.clinicaltrialpartnerhsips.com
NOMINATION CATEGORIES
Announcing the
1st Annual Partnerships Hall of Fame Awards
Partnerships in Clinical Trials event will host it’s
1st Annual Partnerships Hall of Fame Awards
ceremony to honor and celebrate the Partnerships
MVPs throughout the past 20 years.
Technology and Innovation
Lifetime Achievement
Operational Excellence
Change Management
Most Valuable Attendee
-ARCH��� !PRIL���������s�0HOENIX�#ONVENTION�#ENTER�s�!RIZONA

54 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
To have your event considered, contact Kayda Norman at [email protected] or (732) 346-3035.
>> For a comprehensive calendar of events see appliedclinicaltrialsonline.com
Calendar of Events
February15-16: Clinical Trial Material
CMC, Fast Track to Proof of
Concept, Frankfurt, Germany.
Contact: SMi
15-17: Electronic Document
Management 2011: The Inter-
section of Data, Documents
and Submissions, National
Harbor, MD. Contact: DIA
16-17: Writing in the Regulated
Environment When English is
your Second Language, King of
Prussia, PA. Contact: CfPIE
17-18: Standard Operating
Procedures (SOPs) Develop-
ment and Implementation,
Las Vegas, NV. Contact: SoCRA
17-18: Pharmaceutical Regula-
tory Affairs in the Middle East,
London, UK. Contact: Manage-
ment Forum
17-19: 2011 Genitourinary
Cancers Symposium, Orlando,
FL. Contact: ASCO
18: Clinical Research Profes-
sional Certification Prepara-
tion and Review Course, Las
Vegas, NV. Contact: SoCRA
21-23: Marketing Pharma-
ceuticals 2011: Workshop for
Regulatory Professionals and
Promotional Review Teams,
Washington, DC. Contact: DIA
21-24: 2011 ISPE Tampa Confer-
ence, Tampa, FL. Contact: ISPE
21-25: Training Course on
Excellence in Pharmaco-
vigilance: Clinical Trials and
Post Marketing, London, UK.
Contact: DIA
23: Preclinical and Clinical
Imaging for Drug Develop-
ment—A Virtual Conference,
9:30 a.m. to 6 p.m. Contact: CBI
23: Understanding the Impact
of Statistics on the Design,
Conduct, and Reporting of
Clinical Trials Webinar, 12:00
p.m. to 1:30 p.m. Contact: ACDM
23-24: 7th Annual Forum on
Late Phase Research, London,
UK. Contact: CBI
23-25: Training Course on
Clinical Project Management,
Basel, Switzerland. Contact: DIA
23-25: Strategies for Clinical
Oncology Drug Development,
San Francisco, CA. Contact: CHI
23-25: Translational Science,
San Francisco, CA. Contact: CHI
23-25: Validaiton and GMP
Compliance Week: Achieve
Manufacturing Excellence
through Optimal Quality
Practice, TBD. Contact: IVR
24-25: Coordinating a Clinical
Trial, Coral Springs, FL. Contact:
MRM
24-25: INDs/NDAs/CTDs, New
Brunswick, NJ. Contact: CfPA
28-March 1: Adverse Drug
Effects—Reporting and
Regulatory Requirements,
Berlin, Germany. Contact: CfPIE
March2-3: FDA Clinical Trial Require-
ments Regulations, Compli-
ance, and GCP Conference, San
Francisco, CA. Contact: SoCRA
2-3: An Overview of Pharma-
coepidemiology, Arlington, VA.
Contact: PERI
2-3: IQ, OQ, PQ, Amsterdam, The
Netherlands. Contact: CfPA
2-4: Drug Development
Process-From Discovery
to Communication, Berlin,
Germany, Contact: CfPIE
3-4: Preparation of FDA
Submissions (INDs, NDAs,
BLAs, ANDAs, Post-Approval
Supplements) and Communi-
cating with the FDA, King of
Prussia, PA. Contact: CfPIE
6-9: SGO’s 2011 Annual
Meeting on Women’s Cancer,
Orlando, FL. Contact: ASCO
6-11: 46th Annual Arden
Conference: Pharmaceutical
Development of Biologics,
West Point, NY. Contact: AAPS
7: Medical Devices: Demystify-
ing Regulation and Guidance,
Arlington, VA. Contact: PERI
7-8: Clinical Document
Management—A Trial-by-Trial
Approach to Compliance, Los
Angeles, CA. Contact: CfPIE
7-9: Good Clinical Practices
(GCPs), Berlin, Germany.
Contact: CfPIE
8-9: Applying Pharmacokinet-
ics and Pharmacodynamics
for Regulatory Submissions,
Arlington, VA. Contact: PERI
9-11: EudraVigilance Train-
ing—Electronic Reporting of
ICSRs in the EEA, London, UK.
Contact: DIA
10-11: DIA/ FDA Practices
for Regulatory Information
Synthesis of Randomized
Trials for Product Safety
Evaluation, Bethesda, MD.
Contact: DIA
14-15: Clinical Trial Design
for Medical Devices, King of
Prussia, PA. Contact: CfPIE
14-15: Basic Drug Develop-
ment, Arlington, VA. Contact:
PERI
14-15: Developing Specifica-
tions for Drug Substances and
Drug Products, Amsterdam, The
Netherlands. Contact: CfPA
14-16: EudraVigilance Train-
ing—Electronic Reporting of
ICSRs in the EEA, London, UK.
14-16: BIO-Europe Spring 2011,
Milan, Italy. Contact: BIO
14-18: Clinical Science Courses,
Philadelphia, PA. Contact:
SoCRA.
AAPS: American Association
of Pharmaceutical Scientists,
(703) 243-2800,
www.aapspharmaceutica.com
ACDM: Association for
Clinical Data Management,
+44 1727 896080
ASCO: American Society of
Clinical Oncology,
(571) 483-1300, www.asco.org
BARQA: British Association
of Research Quality
Assurance, +44 1473 221411,
www.barqa.com
BIO: Biotechnology Industry
Organization, (202) 962-9200,
www.bio.org
CBI: Center for Business Intel-
ligence, (781) 939-2400,
www.cbinet.com
CfPIE: Center for Professional
Innovation and Education,
(610) 688-1708, www.cfpie.com
CfPA: Center for Professional
Advancement, (732) 238-1600,
www.cfpa.com
CHI: Cambridge Health Insti-
tute, (781) 972-5400,
www.healthtec.com
DIA: Drug Information
Association, (215) 442-6100,
www.diahome.org
ExL Pharma: (212) 400-6240,
www.exlpharma.com
ICR: Institute of Clinical
Research, +44 1628 899755,
www.instituteofclinical
research.com
IIR: Institute for International
Research, (888) 670-8200,
www.iirusa.com
ISPE: International Society of
Pharmaceutical Engineering,
(813) 960-2105, www.ispe.org
Management Forum:+44 (0) 1483 0570099,
www.management-forum.co.uk
MRM: Medical Research
Management, (877) 633-3322,
www.cra-training.com
NextLevel Pharma: +421 232
662 621, www.nextlevelpharma.
com
PDA: Parenteral Drug
Association, (301) 656-5900,
www.pda.org
SMi: +44 20 7827 6000.
www.smi-online.co.uk
SoCRA: Society of Clinical
Research Associates, (800)
SoCRA92 or (215) 822-8644,
www.socra.org

appliedclinicaltrialsonline.com APPLIED CLINICAL TRIALS 55January 2011
APPLIED CLINICAL TRIALS (ISSN 1064-8542) is pub-lished monthly by Advanstar Communications Inc., 131 West 1st Street, Duluth, MN 55802-2065. Subscription rates: $70 for 1 year (12 issues), $120 for 2 years (24 issues) in the United States and possessions; $90 for 1 year, $140 for 2 years in Canada and Mexico; all other countries $130 for 1 year, $235 for 2 years. Single copies (prepaid only): $9 in the United States and possessions; $11 in all other countries. Add $6.50 per order for ship-ping and handling. Periodicals postage paid at Duluth, MN 55806 and additional mailing offices. POSTMAS-TER: Please send address changes to APPLIED CLINICAL
TRIALS, P.O. Box 6115, Duluth, MN 55806-6115. Canadian G.S.T. number: R-124213133RT001, Publica-tions Mail Agreement Number 40612608. Return all undeliverable Canadian addresses to: Pitney Bowes,P. O. Box 25542, London, ON N6C 6B2, CANADA.
©2011 Advanstar Communications Inc. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical including by photocopy, recording, or infor-mation storage and retrieval without permission in writ-ing from the publisher. Authorization to photocopy items for internal/educational or personal use, or the internal/educational or personal use of specific clients is granted by Advanstar Communications Inc. for libraries and other users registered with the Copyright Clearance Center, 222 Rosewood Dr. Danvers, MA 01923, 978-750-8400 fax 978-646-8700. For uses beyond those listed above, please direct your written request to Permission Dept. fax 440-891-2650 or email: [email protected].
ICSRs in the EEA, London, UK.
Contact: DIA
7-8: SoCRA Clinical Site
Coordinator/Manager
Program for Coordinators,
Research Associates, Study
Nurses, and Site Managers
Registration, Toronto, Ontario.
Contact: SoCRA
7-8: 2011 RAPS Horizons:
Regulatory and Beyond,
Vancouver, Canada.
Contact: RAPS
11-13: EudraVigilance Train-
ing—Electronic Reporting of
ICSRs in the EEA, London, UK.
Contact: DIA
11-14: ISPE Frankfurt Confer-
ence, Frankfurt, Germany.
Contact: ISPE
11-15: 2011 PDA Annual
Meeting, San Antonio, TX.
Contact: PDA
12-14: Bio-IT World Conference
and Expo, Boston, MA.
Contact: CHI
13: Biosimilars and Follow-
on Biologics, Arlington, VA.
Contact: PERI
14-18: Clinical Science Courses,
San Francisco, CA. Contact:
SoCRA
15-16: IQ, OQ, PQ, Burlingame,
CA. Contact: CfPA
16-17: Clinical Data Quality
Summit, Arlington, VA.
Contact: DIA
21-22: The EU Clinical Trial
Directive, King of Prussia, PA.
Contact: CfPIE
21-22: INDs/NDAs/CTDs,
Amsterdam, The Netherlands.
Contact: CfPA
21-22: 3rd Annual Bio/Pharma-
ceutical Drug Safety Forum,
Philadelphia, PA. Contact: CBI
21-22: The Institute of Clinical
Research 32nd Annual Confer-
ence and Exhibition, Brighton,
UK. Contact: ICR
21-23: Analytical Methods
Validation for FDA Compli-
ance, New Brunswick, NJ.
Contact: CfPA
22-23: Implementing Good
Clinical Laboratory Practice,
Cambridge, UK. Contact: BARQA
24-25: Advanced Site Manage-
ment: Finance and Produc-
tivity Enhanced Business
Practices for Clinical Research
Programs, Jersey City, NJ.
Contact: SoCRA
24-25: 3rd Annual Forum
on Payers on Personalized
Medicine, Washington DC.
Contact: CBI
24-25: 4th Annual Clinical Trial
Management Systems (CTMS),
Philadelphia, PA. Contact: CBI
24-25: Advanced Cancer
Course “International Clinical
trials Workshop” (FLASCA),
Punta del Eeste, Uruguay.
Contact: ASCO
28-29: The 3rd Annual Digital
Pharma Europe, Ingelheim,
Germany. Contact: ExL Pharma
28-29: Cardiovascular Drug
and Device Development,
Arlington, VA. Contact: PERI
28-30: 23rd Annual EuroMeet-
ing, Geneva, Switzerland.
Contact: DIA
28-30: Pharmaceutical Process
Development, Amsterdam, The
Netherlands. Contact: CfPA
30-31: Prescription Drug
Labeling Regulations: US,
Canada and EU, Arlington, VA.
Contact: PERI
30-April 1: 20th Annual
Partnerships in Clinical Trials,
Phoenix, AZ. Contact: IIR
April4-5: Good Laboratory
Practices (GLP) for Pre-Clinical
Testing, King of Prussia, PA.
Contact: CfPIE
4-5: Global Regulatory Affairs:
An Overview of Drugs and
Biologics (incl. EU Clinical
Trial Directive), Arlington, VA.
Contact: PERI
4-6: 2nd Annual Proactive
GCP Compliance, Westin
Arlington Gateway, VA.
Contact: ExL Pharma
5-6: Research Quality Assur-
ance for Good Laboratory
Practice, Cambridge, UK.
Contact: BARQA
5-7: Medical Device Regula-
tory Affairs, Denham, UK.
Contact: TOPRA
6-8: EudraVigilance Train-
ing—Electronic Reporting of
ALMAC Group . . . . . . . . . . . . . . . . . . . . . . 7
Aptuit Inc . . . . . . . . . . . . . . . . . . . . . . . . 29
AtCor Medical . . . . . . . . . . . . . . . . . . . . . 43
Barnett Educational Services. . . . . . . . . 17
BIO International . . . . . . . . . . . . . . . . . . 25
Biomedical Systems . . . . . . . . . . . . . . . . . 3
Cetero Research . . . . . . . . . . . . . . . . . . . 15
DaVita Clinical Research . . . . . . . . . . . . 41
ERT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
Emedcareers . . . . . . . . . . . . . . . . . . . . . . . 8
IRB Services . . . . . . . . . . . . . . . . . . . . . . 45
ICON Medical Imaging . . . . . 31, 33, 35, 37
IIR Partnerships . . . . . . . . . . . . . . . . .47, 53
INTERLAB Central Lab Services
—Worldwide . . . . . . . . . . . . . . . . . . . . 27
Marken . . . . . . . . . . . . . . . . . . . . . . . . 18ab
Medpace Inc . . . . . . . . . . . . . . . . . . . . . . . 9
Novella Clinical . . . . . . . . . . . . . . . . . . . . 13
Oracle Health Sciences . . . . . . . . . . . . . . 59
PRA International . . . . . . . . . . . . . . . . . . 39
PAREXEL International . . . . . . . . . . . . . . . 2
Perceptive Informatics . . . . . . . . . 11, 20-21
PharmaNet . . . . . . . . . . . . . . . . . . . . . . . 23
QualityMetric . . . . . . . . . . . . . . . . . . . . . . 5
Ad Index

56 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
Products & Services Showcase
EQUIPMENT RENTAL
ROCKWELL COMPOUNDING ASSOCIATES, INC
� e Specialist in Pharmaceutical Compounding for Clinical Trials
• Customized Dosages & Over-Encapsulation
• Placebo Controlled Blinded Studies
• Sterile and Non-Sterile Services Available
• Small Medium and Large Multi-site Trials
• Multiple Dosage Forms Available
Capsules, Eye/Ear Drops, Nasal Sprays, Enemas, Suppositories, and Topical Creams, Ointments, Lotions & Transdermals
350 Theodore Fremd Avenue
Rye, New York 10580 • (800) 829-1493
CONTRACT SERVICES MEDICAL EQUIPMENT
MESMmaking the industry’s heart beat
www.mesm.co.uk • [email protected]
tel. +44 (0)1257 225776 fax. +44 (0) 1257 225539
Providing a Cost Effective Cure for all
your Clinical Trial Equipment
Sourcing and Supplying
ECG Machines
Refrigerated Centrifuges
-80 °c Freezers
Temperature monitoring.
PP
PP
Centrifuges
ECG machinesBalances
Spirometers
Defibrilators
Storage
between
studies
Sourcing and
Logistics
Equipment
tracking through
product life
Equipment
Maintenance
Collection
from sites
worldwide
Calibration
and Repair
End of life
Recyling
MESMManagement
System

appliedclinicaltrialsonline.com APPLIED CLINICAL TRIALS 57January 2011
Who will you trust to source &
manage Commercial Drugs for your next Clinical Trial?
Global Drug Sourcing for Clinical Trials
+1.610.233.3300 • [email protected] • www.myoderm.com
PACKAGING SERVICES
CONTRACT MANUFACTURING/PACKAGING SERVICES
Laboratories
LaboratoriesPK Kits/Material and Logistics Services
Lab Operations Manual Time Point Specific Kits
Pre-printed Specimen Labels Specimen Shipment Logs
Domestic/International
Shipment Tracking/Logistics
Tel: 512.303.1265 Fax: 512.303.1390www.tcgsupplies.com
CLINICAL SUPPLIES
Clinical and Wholesale SuppliesClinical Test Material Services Wholesale SuppliesPatient-Specific Distribution Single Lots for All OrdersLabel Design and Labeling Long Expiration DatingMedical Supplies Storage/DistributionDomestic/International Diagnostic KitsCentral Randomization www.irxsc.comAvailable 24/7www.tcgsupplies.com
Tel: 512.303.1265 Fax: 512.303.1390
PLACE YOUR AD TODAY!
Have you been featured in Applied Clinical Trials? For instant credibility, put a reprint into your prospect’s hands.
Now, that’s smart.THE YGS GROUP | 800-290-5460 x100 | [email protected] YGS Group is the authorized provider of custom reprints for Applied Clinical Trials.
Smart editorial. Smart marketing.
Standard of Care in Study BudgetingSurvey reveals industry practices
surrounding standard of care and
insurance claims data.
Harold e. Glass
Pharmaceutical executives readily acknowledge that
their industry faces a number of broad challenges,
not the least of which are the escalating costs of de-
veloping new drugs and a weak public image.1 Both
issues intersect in one area of drug development:
clinical grants. Based upon an industry survey of people
working in clinical operations, and an analysis of grant pay-
ments from the perspective of standard of care (SOC), this
article argues that cost management and fair market value
can be far more effectively addressed than has been the prac-
tice to date.Clinical grants represent a major and growing cost of
developing new drugs. These rapidly increasing costs have
been extensively documented and analyzed, 2 and the re-
search suggests that clinical trials are the largest single area
of R&D operating expenses, with clinical investigator grants
representing the bulk of these costs. Many drug develop-
ment managers appreciate the need to control clinical trial
costs. One important, if underappreciated, approach involves
avoiding double payments for activities that would be nor-
mally covered by third-party payers (including Medicare and
Medicaid in the United States) as part of the standard care
that any patient would receive at that clinical research site,
whether or not that patient is part of a clinical trial. While
sites are ethically prohibited from enrolling a patient in a
clinical trial if that patient would not otherwise be treated
for the illness being studied, many of these patients would
be partially covered by third-party payers as part of the stan-
dard of medical care.Understanding the standard of medical care, however,
can be particularly dif f icult when studies involve mul-
tiple countries. At one end of the health continuum some
countries are moving toward national medical
treatment protocols—the UK’s National Health
Service is one example. While health care in
many countries has one dominant payer, few
countries have just one agency delivering almost
all their health care, as is the case in the UK. In
sharp contrast, the United States has multiple
payers and health care delivery organizations.
Such differences challenge clinical development
teams as they seek to establish medical standard
of care guidelines for clinical trial grant pay-
ments. In the United States, however, it is easier
to establish what constitutes standard of care
through the payment practices of third-party
payers.A second pharmaceutical industry challenge is
the changing relationship with physicians. After
intense scrutiny from both within and outside
the industry, pharmaceutical companies have
now developed more stringent guidelines about
what they can give to prescribing doctors. For
instance, new guidelines prohibit gifts of any sort,
restrict meals to those associated with actual
medical education, and prohibit industry em-
ployees from giving any other objects to medical
professionals. Some pharmaceutical industry observers are
also concerned about the financial relationship be-
tween investigators participating in clinical trials
and the companies sponsoring the trials. These
observers have questioned whether the grant
amount for a clinical trial reflects payment only for
work performed or whether the payment might be
an attempt to influence investigator behavior. In
these instances, the foremost concern is whether
investigators are being paid at fair market rates or
at inflated rates that might influence their behav-
ior. 3 While some published research links relative
grant payment levels with subsequent investigator
Sites
Your Peer-reviewed Guide to Global CliniCal trials ManaGeMent appliedclinicaltrialsonline.com
1992–2010
ACT
Year of Servi ce
Volume 19, Number 7 July 2010
InsId
e
Protecting Subjects:
The IRBs Next Steps
➤ SiteS
incorporating Standard
of Care in Study Budgets
Benefits of CtMS
at the investigative Site
Also in this issue
■ FDA Transparency Efforts to Impact Research
■ Survey Assesses Europe’s Clinical Trials Directive
■ Tapping into the Potential of Pharmacists
■ Biosimilars Make Headway in the U.S.
Complete contents on pages 6 & 8
EU LEGAL SERVICES
EU Legal Representative. All 27 EU countries
require an EU based legal entity for clinical trials.
Our UK based Chartered Accountants form a UK
legal entity in 48hrs. Low fees – prompt service.
www.TopazClinical.com

58 APPLIED CLINICAL TRIALS appliedclinicaltrialsonline.com January 2011
To see more A Closing Thought articles,
visit appliedclinicaltrialsonline.com
A Closing Thought
We can postulate that suitable dose-effect
relationships were demonstrated in Phase
II clinical trials for these failed drug proj-
ects. Rather than infer that preclinical
research through Phase II has suddenly
become error-prone, there is merit in as-
sessing the validity of Phase III clinical
trials today.
Until the late 80s, Phase III trials were
conducted essentially in North America
and/or Europe. The drug pipeline deliv-
ered twice as many innovative medicinal
products annually. Clinical research
globalized over the last two decades by
following the path of diminishing GDP per
capita. The evidence comes from plotting
the year of the first FDA inspection in any
particular country versus GDP per capita
in that country.
Our research evaluated the clinical trial
participation of sites in North America
and in Europe in Phase II and III industry
trials in the period 2004-2006 compared
with 2007-2009. North America partici-
pated in 60% of Phase II trials worldwide
in both periods, twice more than Europe.
The complexity of trial protocols is grow-
ing fast in Phase II, driving up the costs
of procedures and labs. According to a
Tufts Center for the Study of Drug Devel-
opment news item from May 5, 2010 the
high medical technology content of Phase
II studies may explain the dominance of
North American sites in Phase II trials.
The same report notes that Phase III
protocols are less likely to increase in
complexity. Hence, the position of North
America in Phase III is seriously under-
mined by globalization: North American
sites participate only in 30% of Phase III
trials worldwide. In 2007-2009, North
American and European sites have seen
their respective shares in Phase III trials
decline in favor of the rest of the world.
We can assume that the diminishing
participation of North American and Euro-
pean sites in Phase III trials is even worse
in terms of patients enrolled. Understand-
ably, it is cost effective for sponsors to in-
clude sites from low-cost countries in large
Phase III studies, where, in addition, par-
ticipants are potentially more incentivized.
Indeed, the lower the local standard of care
compared to that offered in the trial, the
greater the incentive for patients to take
part. To make matters worse for sites in
North America and Europe, recruitment
periods are being closed prematurely as a
function of global sample size completion.
The quality of Phase III trials is weak-
ened further by massive differences be-
tween sites. Biostatisticians do not censor
data for these conditions. Just one exam-
ple regarding concomitant medications:
WHO puts a ceiling of 1% of market value
on the amount of medicinal products in
North America and most of Europe which
are counterfeit, but the estimate is at least
10% with no ceiling for other regions of
the world. The most puzzling paradox is
that health authorities in North America
and Europe accept evidence from coun-
tries from which they do not recognize
the diplomas of doctors and other health-
care personnel who produce the data.
In conclusion, as addressed in this
space in April 2010, data from healthcare
systems with health outcomes signifi-
cantly worse than in North America and
Europe comes cheaper, but may jeopar-
dize the overall success rate of new drug
projects coming out of Phase II. ❏
A recent study (2010 Pharmaceutical R&D Factbook) indicates that
the decade-long drop in the overall success rate of pharmaceutical
R&D continued in 2009. The authors found that “the number
of experimental drug projects terminated at the final Phase III stage of
development had doubled in 2007-2009 compared with 2004-2006.”
Until the late 80’s, Phase III trials were
conducted essentially in North America
and Europe.
Jean-Pierre Tassignon, MD, PhD, President and CEOCrossover CRI [email protected]
Deteriorating Quality in Global Trials

20 of the 20 Top Pharmas
Copyright © 2008, Oracle. All rights reserved. Oracle is a registered trademark of Oracle Corporation and/or its affiliates.Other names may be trademarks of their respective owners.
oracle.com/lifesciences
or call 1.800.ORACLE.1
Oracle Health Sciences
Get Better Results With Oracle