
Working_well
40
Working well Guidance on promoting health and wellbeing at work direction 09.3
-
Upload
joseacostadiaz -
Category
Documents
-
view
214 -
download
0
description
bienestar laboral
Transcript of Working_well

Working wellGuidance on promoting health and wellbeing at work
direction
09.3

IOSH publishes a two-tier
range of free technical
guidance. Our guidance
literature is designed to
support and inform members
and motivate and influence
health and safety stakeholders.
Direct infoBrief, focused information on healthand safety topics, typically operation-or sector-specific.
DirectionStrategic corporate guidance on healthand safety issues.
Working well – guidance onpromoting health and wellbeing at workThe aim of this guide is to promote aholistic, proactive approach tomanaging health and wellbeing issuesat work. It also aims to encourageoccupational safety and healthpractitioners to work with others,particularly occupational health andhuman resource specialists, to improveemployees’ work performance andreduce sickness absence through:- identifying and addressing thecauses of workplace injury and illhealth, as required by health andsafety law
- addressing the impact of health onthe capacity of employees to work,eg support those with disabilitiesand health conditions, andrehabilitation
- promoting healthier lifestyles andtherefore making a positive impacton the general health of theworkforce.
It’s not the intention of this guide toprovide in-depth guidance or advice onspecific health issues.
The guide refers to UK law, statisticsand examples. Readers from outsidethe UK who want to apply its findingsshould be aware of possible differencesand may need to use data from theirown countries.
IOSH Technical Committee

Contents
1 IOSH’s view 022 What is wellbeing? 033 Managing health conditions and disabilities at work 074 Key wellbeing issues 085 How should employers promote health? 146 Implementing a wellbeing strategy in the workplace 167 Conclusion 19References 20Training for OSH practitioners 22Links to more case studies 22
AppendicesA Some key drivers for wellbeing at work 23B Key stakeholders and the part they play 25C Supplementary wellbeing domains 28D Delivering a wellbeing event 29E Resources 32
Case studies1 BT 062 GlaxoSmithKline 093 East Sussex Council 134 Burnley Borough Council 15
Figures1 A healthy organisation 162 An example of health, safety and wellbeing events 31
Acknowledgments

Research shows that being in work isgenerally good for people’s health andwellbeing,1 and case studies indicatethat helping employees to improve ormanage their health can result inincreased attendance and performance.In addition, a review of Gallup studiesexamining links between employees’satisfaction, engagement andperformance across organisationsconcludes that workplace wellbeingand performance are complementaryand dependent parts of psychologicallyand financially healthy organisations.The review found that ‘the presence ofpositive workplace perceptions andfeelings are associated with higherbusiness-unit customer loyalty, higherprofitability, higher productivity andlower rates of [staff] turnover’.2
Because the UK has an ageingpopulation – as a result of increasedlife expectancy and low birth rates –having more people in work isimportant for the future of the nationaleconomy. And with fewer youngpeople entering employment, there willbe an increasing need for employers toattract, retrain and retain employees.Although the skills gap may beaddressed to some extent by immigrantand migrant workers (eg from EasternEurope), the future workforce is likelyto have a higher proportion of olderemployees and employees withdisabilities and chronic healthconditions.
In addition, if government, healthcareservices, other professionals, employersand employees don’t work together topromote the health and wellbeing ofindividuals, issues such as obesity,alcohol and drug abuse and mental illhealth will have a negative impact onthe workplace.
Many employers already have a widerange of professionals in theirworkplace who carry out activities thatsupport employees’ wellbeing.However, the time has come for aholistic approach in which allstakeholders work together for thecommon goal of a happy, healthy andmotivated workforce.
Employers who want to retain anddevelop their workforce will need tomake sure that they have suitablestrategies to:- continue to protect their employeesfrom work-related health and safetyrisks, as required by law
- help employees who have commonminor health conditions return to orremain in work
- encourage employees to look aftertheir own health and wellbeing andprovide opportunities that enablethem to do so.
The law requires employers to managetheir work-related health and safetyrisks. Organisations who are alsoconsidering introducing ‘wellbeingstrategies’ need to already haveeffective health and safetymanagement arrangements in place.Wellbeing strategies need tocomplement and support existingcorporate strategies, such as those forhealth and safety and humanresources.
IOSH believes that the occupationalsafety and health (OSH) communityshould play a fundamental role insupporting wellbeing in the workplace.Over 35,000 IOSH members are alreadyworking in all employment sectors(public, private and voluntary) in theUK and abroad, helping to reduce thenegative effects of work on employees’health and safety. Many have theinfluencing and communication skillsneeded to promote healthy behavioursand, through a positive approach toindividual risk assessment, can helpemployers rehabilitate those withdisabilities and health conditions backinto the workplace.
This guide seeks to help andencourage OSH practitioners to bemore effective and proactive inpreventing work-related ill health, andto play their part in promoting healthand good rehabilitation practices intheir workplaces.
1 IOSH’s view
02

Definitions of wellbeing generally relateto people’s experience of their qualityof life. For instance, Waddell & Burton1
define it as: ‘The subjective state ofbeing healthy, happy, contented,comfortable and satisfied with one’squality of life. It includes physical,material, social, emotional(“happiness”), and development andactivity dimensions.’
As a large part of an employee’s life isspent at work, employers can andshould play an important part inhelping their workers achieve a goodquality of life. The workplace can alsobe a useful arena to encourage peopleto improve their health.
The Chartered Institute of Personneland Development (CIPD) uses thefollowing definition of wellbeing, whichbalances the needs of the employeewith those of the organisation:4
‘creating an environment to promote astate of contentment which allows anemployee to flourish and achieve theirfull potential for the benefit ofthemselves and their organisation.’
This definition is strongly linked toemployee engagement and creating anorganisation that employees will wantto work for because they feel safe, arevalued by their employer and feel partof a happy and supportive workcommunity. This is part of what iscalled the ‘psychological contract’,5 theunwritten expectations that employersand employees have about each other.The psychological contract recognisesthat employees’ commitment isn’tachieved through pay alone. Employerswho pay attention to quality of lifeissues can help secure employees’commitment and motivation, and soimprove productivity and retentionrates. Changes in work practices areaffecting some aspects of thepsychological contract, such as jobsecurity, so it’s important thatemployers counter this by looking afterother areas that have an impact onemployees’ wellbeing. For instance, theCIPD notes that research shows thatthere’s an important link betweengood work–life balance and a positivepsychological contract.
The government’s strategy paper,Health, work and well-being – Caringfor our future6 is clearly focused onstrategies for preventing ill health andsupporting those with health problems
to remain in or return to work, helpingthem and their families, and alsoreducing the societal costs of sicknessabsence and incapacity for work.
So, employers and society need aworkforce that’s motivated, physicallyand psychologically well, and resilient,and a holistic approach to wellbeingcan help achieve this (see Appendix A,page 23).
This guidance document focuses on thehealth aspects of wellbeing, rather thanissues such as culture and employeeengagement, which are traditionally thedomain of human resources specialists.
Employers who invest in theiremployees’ health demonstrate thatthey care for and value their staff.Encouraging employees to plan andtake part in health-related activities atwork encourages social interaction andthe development of a positive workcommunity, which will affect the otheraspects of wellbeing and help theemployer achieve a happy, motivatedworkforce that’s more likely to stay andperform well.
“A business’s most valuable asset is, and will always be, the dedicated staff that devote
themselves to delivering the work of the organisation. Healthy and fit staff are essential to
ensuring a company remains efficient and profitable… None of us doubt that good staff
management practices ensure that our workforce delivers our aims – but many of us forget
that unless we help them manage their health, fitness, and well-being many of our workers
can and will fall ill. Surveys of our workers show that they value these aspects of their work
more than just financial rewards. People want to perform to the best of their ability.
We know that work is good for people. It provides economic stability as well as being a
valuable source of social interaction both for the individual and the community within
which they work. Fit, healthy staff deliver profitable businesses which in turn allow the UK
to remain one of the most prosperous and best places to work and live.”3
Professor Dame Carol Black, UK National Director for Health and Work
03
2 What is wellbeing?

What is the evidence of thebenefits of a holistic view ofwellbeing? The CIPD’s Absence ManagementAnnual Survey report 20087 estimatesthat, on average, UK employees areabsent from work eight days per year.For each employee, this amounts to anannual cost to the employer of £666per year. The report also found thatstress, mental illness, back pain andmusculoskeletal disorders are some ofthe largest causes of absence in bothmanual and non-manual workers.
A review by Lunt et al.8 concludes thatthe length of sickness may be as muchto do with an individual’s beliefs aboutthe cause, consequences andcontrollability of their health problemas the underlying condition. This‘biopsychosocial’ approach recognisesthat the onset and maintenance ofcommon ill health conditions is drivenby an interaction between physical,psychological, social andenvironmental factors. This includesfactors such as individualcharacteristics (eg age, gender, pastexperiences), health beliefs andbehaviours (eg smoking, drinking andexercise), the work environment,economic stability and social supportoutside work.
So, while OSH practitioners may focuson the work-related causes ofabsence, it’s unlikely that a significantimpact will be made on sicknessabsence rates unless employersattempt to understand and address (sofar as it’s in their control) other issuesthat play their part.
Lunt et al.’s review looks at whatinfluences wellbeing, and identifiesfactors such as social status, incomeand quality of life – although they’reoften linked with other externalfactors such as an individual’sperception of past experiences orambitions. Social networks also seemto have a beneficial effect onwellbeing. This is particularly true ifpeople have trust in the network.9
Lunt et al. urge that it’s necessary totake this context into account whentrying to understand and manage therisks of common health problems.Focusing on the immediate workenvironment could mean thatimportant psychosocial hazards areignored. Organisational climate andwork–life balance also need to beconsidered when assessing andmanaging common health risks suchas stress and musculoskeletalconditions.
Targeting morale is particularlyimportant, as high morale helps tocounter the effects of stress. Lunt etal. coin the term ‘well-being assets’ todescribe factors that help individualscounter stress. These include:- being realistic about their job- having a good job ‘fit’- finding work meaningful- being physically fit and eating well- having a flexible coping style- working for an organisation thathas flexible working practices
- having social support.
This supports the case for givingemployees opportunities to exercise,eat healthily and participate in anyappropriate health checks or screeningin the workplace. Suitable adjustmentsto the workplace also help employeeswho are managing health conditionsat work feel that they’re in control oftheir symptoms.
Why should OSH professionals getinvolved?OSH practitioners who wonder whythey need to consider wellbeing issuesneed only look at the parallels withthe Health and Safety Executive’s(HSE) stress management standards.10
An employer who looks after allaspects of employees’ wellbeing is lesslikely to have work-related problemsthat contribute to employees’ stress.As Lunt et al.’s review shows,improving employees’ sicknessabsence and wellbeing can’t beachieved by tackling work-relatedcauses alone. What’s also needed is to
address employees’ morale andphysical health.
OSH practitioners should already beimplementing strategies to addresswork-related health and safety risks.Wellbeing offers an opportunity for adifferent approach to getting healthand safety on the business agenda,and may be more attractive to someorganisations. For instance, it may beseen to provide a means of improvingbusiness performance by engaging andmotivating employees, improvingrecruitment and retention, andaddressing sickness absence andassociated costs.
Many OSH practitioners have to tackletheir employer’s negative view ofhealth and safety as something thathas to be done only because the lawrequires it. However, wellbeing may beseen in a more positive and proactivelight, as something a good employerwould want to do to get the best fromtheir employees. This is a greatopportunity for the OSH practitioner tobuild bridges with other professionalsemployed or contracted by theirorganisation, and to extend their owncompetence.
While OSH practitioners may worktirelessly to address the workplacecauses of accidents and ill health, thestrong influence that individualcapability, health attitudes and lifestylecan have means that it’s unlikely thatoverall sickness absence can beimproved without taking a holisticapproach to employees’ health.
The business case for wellbeingIn 2008, PricewaterhouseCooperspublished a report on the business casefor wellbeing programmes, Buildingthe case for wellness.11 The study,which included a review of availableliterature and 55 case studies, showsthat wellbeing programmes can givebusinesses benefits through costsavings or additional revenuegeneration. The prime benefits are costsavings arising from improved sickness
2 What is wellbeing?
04

absence and employee turnover, feweraccidents and injuries, and betteremployee satisfaction. Seven of the 55case studies reviewed reported thattheir investment in a wellnessprogramme had resulted in savings.One example was of a discountedphysiotherapy service at a call centre,which realised a benefit–cost ratio of34:1 over six months. Ergonomicsupport programmes yieldedbenefit–cost ratios ranging from 1:1 to 12:1.
A collaborative project betweengovernment and non-governmentagencies, Well@Work, was set up toassess the effectiveness of workplacehealth programmes in a wide range ofwork environments and to helpdevelop an evidence base of whatworks. An evaluation report of theproject12 presented the following keyfindings:- some of the initiatives aimed atencouraging employees to be moreactive (including those aimed atincreasing active travel) achievedsignificant increases in participants’physical activity levels
- employers reported increased staffmorale, and better workatmosphere, communications andinteractions between employeesand managers
- employees said that they enjoyedtaking part in health initiatives andliked the opportunity to meet newcolleagues and socialise; they alsovalued peer support and found thecompetitive element of some of theprogrammes motivating
- eight of the 11 employers takingpart in the project stated that theywanted to continue with wellnessprogrammes, indicating that theyvalued their positive impact onemployees and workplace culture.
A framework for wellbeingInvestors in People (IiP)13 is creating aframework for health and wellbeing,with the aim of developingorganisations and increasingproductivity. The IiP has run pilots inover 350 UK organisations, and mayinclude this new strand in their IiPStandard. The project encouragesorganisations to develop a ‘health andwell-being strategic plan’, focusing notjust on employees’ health but on thewider business.
The initiative is designed to improveorganisational and individualperformance through preventingharm, managing risk and maintaininghealth and wellbeing, and aims forcontinuous improvement. To supportthe initiative, IiP has a range of usefulhealth and wellbeing resources.14
The framework covers the followingareas:14
- line management andworkplace culture, eg the styleand capabilities of managers,including their ability to manageteam members and teamenvironments effectively, tackleissues of attendance andrehabilitation, identify potentialcauses of stress, and direct peopleto sources of help and support
- prevention and riskmanagement, eg going beyondminimum legal requirements tomanage risks to health, includingstress and preventing physical andmental harm
- individual role andempowerment, eg making surethe design of job roles, as well ascommunication and objective-setting in the organisation,promotes individual wellbeing
- work–life balance, eg goingbeyond minimum legalrequirements to support flexibleworking arrangements where thismeets the needs of theorganisation and individual
- enabling health improvement,eg supporting, in a proportionateway, employees who want to livehealthily.
“The achievement of personal well-being involves a number of positive decisions regarding
lifestyle. This is very different to stress avoidance with the negative connotation of being
unable to cope and falling ill prior to any action being taken. In their ideal form, well-
being initiatives are proactive and work to enable employees to achieve their full potential
– physical, mental, social, intellectual and spiritual.”4
05

Case study 1 – BT‘Work fit’ is BT’s vehicle for health promotion. It’s a jointinitiative with the BT unions. It aims to promote smallbehavioural changes which, if sustained, will have a long-term impact on health and wellbeing. Each campaignfocuses on a specific health issue and uses a modularapproach to ‘drip feed’ messages to employees. Partnersfrom the voluntary sector are engaged to provideresource material and support for those who want it. Thephilosophy of the ‘Work fit’ programme is ‘helping you tohelp yourself’.
Campaigns have included:- nutrition and exercise – this involved 16,500employees, 75 per cent of whom had maintainedlifestyle improvements six months later
- smoking-cessation – 1,000 employees took part and athird managed to kick the habit
- cancer awareness – aimed at informing employeesabout ways of reducing cancer risks and how toidentify early signs. It included website-basedinformation with external links, a series of stories instaff newsletters, and roadshows across the UK andglobally.
BT’s approach to stress and mental health focuses onthree areas: prevention, protection and intervention. Thestrategy has resulted in a 30 per cent reduction in mentalhealth-related sickness and a return-to-work rate of 75per cent for people absent for more than six months withmental health problems.
Prevention is a combination of good management practicesand education. ‘Positive mentality’ was a 16-week
2 What is wellbeing?
06
campaign that aimed to promote resilience, improveunderstanding of mental health issues and reduce the stigmaof mental illness. The campaign was run in conjunction withthe Sainsbury Centre for Mental Health and MIND. Itconsisted of website information and roadshows coveringthe link between physical and mental health, lifestyle issues,support and relationships. Quizzes were used to testparticipants’ understanding of the material. A session onpositive thinking completed the campaign. An evaluationshowed that more than 50 per cent of those engaged hadbeen influenced to make lifestyle changes. Success wasmeasured by hits on the website (28,932 in total), thenumber of quiz entries and accuracy of responses, and afollow-up survey three months later.
Protection is aimed at early identification of those at riskand actively building resilience. BT uses an online stress riskassessment tool called STREAM, which was developed withHR, line management and union involvement. The 30-itemquestionnaire – based on the HSE stress managementstandards – gives a red, amber or green rating to responses.Following amber or red ratings, line managers must holdone-to-one meetings within a specific time period toresolve issues. The tool is also used across divisions toidentify hot spots.
Where there are mental health problems, a suite ofproportionate interventions is used to resolve them and tohelp keep people in work or return them to work as soonas appropriate. BT is also currently developing ‘mentalhealth first aid’ training.
Case study provided by Catherine Kilfedder, BT Group Health Adviser.

An important aspect of wellbeing issupporting employees with healthconditions to remain in work or toreturn to work following an absence.There’s a common belief that peoplewho have problems with their healthshould not return to work until they’refully fit. However, evidence shows that,provided the right modifications aremade, managing an ill health conditionat work is often better for theindividual than prolonged absence.
Waddell & Burton1 highlight thebenefits of work in providing theeconomic stability, social networkingand self-esteem that’s important forpeople’s physical and mental wellbeing.There’s also an increasing consensusthat many common health conditionscan be managed effectively in theworkplace, leading to better healthoutcomes than prolonged periods ofsickness absence. Clearly this isdependent on workplace hazards(physical and psychosocial) beingcontrolled and appropriate support(including work adaptations) beingprovided.
Where rehabilitation forms part of anattendance management policy, itshould be made clear that it’s for themutual benefit of employees and theemployer. Employees should not bepressurised into returning to workbefore they’re ready. However, asdiscussed earlier, there will be a mix ofbiopsychosocial issues that affect theabsent employee, which the employermay need to take into account. Forexample, the beliefs the employeeholds about their illness may be abarrier to rehabilitation.
Fennell15 found that individuals with achronic illness go through variousstages – crisis, stabilisation, resolutionand integration. Employees in theresolution stage begin to accept thelimitations imposed by their illness andthen, at the integration stage, maybecome ready to return to employmentand rejoin their social networks. Whenconsidering a rehabilitationintervention, the employer should takeaccount of the stage an employee is atand be prepared to accommodate theemployee’s changing beliefs about theiremployment. The employer should alsoexplore any barriers that the employeeperceives are preventing them fromreturning to work. Besides treating theunderlying condition, work or socio-economic factors may need to beaddressed too. The employer may beable to deal with the work-relatedissues, and point the employee tosources of help for other problems.
Many people are prevented fromworking because of misconceptionsand stigma about their ill healthcondition, which often lead todiscrimination. Creating a culturewhere working with a health conditionis considered the norm, and providingaccess to a range of support choices,will help employers recruit theseskilled people, enable them to managetheir condition while continuing towork and, if employees do have totake time off work, get them back towork quickly.
Work-based activities that promotewellbeing and help employees developpositive coping behaviours areimportant in overcoming some of thepsychosocial issues that may affecthealth. There are several ways in whichan employer can assist an employeewith recovery and long-termmanagement of their health conditionat work. These include:- education programmes formanagers that addressmisconceptions and stigma aboutconditions such as mental illness
- providing employees withinformation about self-managingcommon health conditions, as wellas details of support groups
- encouraging employees to set uptheir own in-house support groups
- providing flexible workingarrangements that allow employeesto take time off for treatment ormore frequent rest breaks
- providing employees with access tointerventions – psychological (egcounselling or cognitive behaviouraltherapy) or physical (egphysiotherapy or back care classes)– where the employee’s GP hasagreed this would be beneficial.
There’s more information onsupporting employees with specifichealth conditions in the next section.The IOSH publication A healthy return16
gives more guidance on goodrehabilitation practice.
07
3 Managing health conditions and disabilities at work
“A mental well-being strategy implemented by BT led to a 30 per cent reduction in mental
health-related sickness absence and a return to work rate of 75 per cent for people absent
for more than 6 months with mental health problems.”17

This section outlines some of the keywellbeing issues. Sections 5 and 6 showhow they affect employers and whatemployers can do.
Mental wellbeingStatistics from the Sainsbury’s Centre18
provide clear evidence of theconsiderable costs associated withmental health in the workplace.
At any one time, nearly one in sixpeople in the UK workforce is affectedby a mental health condition such asstress, depression or anxiety. This risesto one in five if alcohol or drugdependence is included. Mental healthproblems account for around 40 percent of sickness absence, whichequates to around 2.8 days per personper year, while stress and mental healthmay account for up to 5 per cent oftotal staff turnover.
An effective strategy should take aholistic view of mental wellbeing,including:- the basic legal requirement toprevent work-related mental healthproblems, by providing good workingconditions and practices. The HSE’sstress management standards10 andthe CIPD/HSE/IiP stress competencyframework19,20 provide usefulguidance on this
- regularly assessing how well theorganisation is performing againstthe stress management standards, sothat areas for improvement can beidentified and addressed. Someorganisations can help with runningsurveys or ‘stress audits ofemployees’. Also, the HSE21 andEngineering Employers’ Federation(EEF)22 offer free assessment tools
- good recruitment practices, to makesure applicants with a history ofmental health problems aren’tdiscriminated against
- training for managers to increasetheir understanding of mental healthand their ability to supportemployees who have problems.Managers need to understand howwork can have a negative impact on
mental wellbeing, how to identifyand tackle the early signs of mentaldistress, and how best to supportthose with ongoing mental healthproblems
- encouraging employees to look aftertheir mental wellbeing. Healthychoices such as a balanced diet andexercising are good for mental (andphysical) wellbeing, helping to buildmental and emotional resilience
- providing access to help and supportfor affected employees. This mayinclude helping employees findsupport, or supplying services such ascounselling or cognitive behaviouraltherapy
- introducing rehabilitationprogrammes for those who havetaken time off work. Once anemployee is off sick with a mentalhealth problem, a lack of contact andsupport from the employer is often amajor barrier to their return towork.17
Unfortunately, people with mentalhealth conditions can experience stigmaand discrimination, ranging from beingignored or excluded to verbal or physicalharassment. The Department of Healthis funding an initiative called ‘Shift’23 totackle these issues in England. Theequivalent in Scotland is called ‘Seeme’.23 The Shift website offersemployers and line managers practicalguidance on managing and supportingpeople with mental health problems inthe workplace. For more information on‘Shift’ and ‘See me’, see Appendix E,page 34.
Physical wellbeing: musculoskeletalhealth Musculoskeletal disorders (MSDs) such asback pain are very common. Accordingto a survey published in 2000, almosthalf (49 per cent) of the UK’s adultpopulation report low back pain lastingfor at least 24 hours at some time in theyear, and it’s estimated that four out ofevery five adults (80 per cent) willexperience back pain at some stage intheir life.24
As well as back pain, some work taskscan lead to employees experiencingproblems with their upper limbs andneck. These may be caused byprolonged, repetitive tasks, such aswhen using computers or working on aproduction line. Working inuncomfortable work conditions or poorenvironmental conditions (eg cold orpoor lighting), or using work tools thatcause vibration, can also contribute toMSDs. Discomfort from poorly designedwork activities can affect employees’work performance. If the causes are nottackled, they can lead to permanentharm.
HSE statistics25 show that in Britain in2007/08, there were more cases of self-reported work-related MSDs than stress.In total, 539,000 people reportedsymptoms of MSDs, of which 45 percent related to backs and 39 per cent toupper limbs and necks.
4 Key wellbeing issues
08
Tips for staying happy
1. Keep physically active 2. Eat well 3. Only drink alcohol in
moderation 4. Value yourself and others 5. Talk about your feelings 6. Keep in touch with friends and
family 7. Care for others 8. Get involved, make a
contribution 9. Learn a new skill 10. Do something creative 11. Take a break 12. Ask for help
Source: Making it possible: improvingmental health and well-being in England.www.shift.org.uk/employers/lmr/wellbeing/index.html.

It’s often difficult to identify a singlecause of back pain. However, thefollowing are often contributory factors:- having had back pain in the past- smoking and obesity - physical factors such as heavyphysical work; frequent bending,twisting, lifting, pulling and pushing;repetitive work; a static posture;vibration
- psychosocial factors such as stress,anxiety, depression and poor jobsatisfaction.
The NHS advises that back pain isn’tnormally serious, and in most cases thebest treatment is to stay active, withsensible levels of movement and usingover-the-counter painkillers if needed.26
An HSE report evaluating 19 projects inthe ‘Back in work’27 initiative identifiedsome key messages, including: - keep active, both to prevent andtreat back pain
- seek early treatment.
The report also highlights the benefits ofgood posture, using lifting aids andadjustable work equipment, andproviding employees with regular breaksfrom prolonged or repetitive tasks, aswell as back care information.
Employers should adopt an approach tophysical wellbeing that includes:- the basic legal requirement toprevent work-related MSDs throughrisk assessment, good workplaceergonomics, advice on safe computeruse and involving employees infinding solutions
- encouraging employees to keep activeand fit by promoting physical activity.Those with back pain may need toavoid work and sporting activities thatinvolve lifting, twisting, pulling andpushing and excessive loading of theback muscles, although yoga-typeexercise, and exercises to increaseendurance of the abdominal and backmuscles, can be helpful
- providing employees with informationand support, such as through backcare programmes
- adopting rehabilitation programmesthat, where appropriate, encourageemployees to keep active throughworking, rather than resting at home.
For more guidance sources on MSDs,have a look at Appendix E on pages 32–36.
09
steering group. Solutions are shared across the business,so that others can learn from them. The programme hasresulted in over 100 improvements and workplace injurieshave fallen by 40 per cent.
A musculoskeletal impact team was also set up to focuson non-work-related MSDs. This initiative resulted inproviding advice and support to improve employees’understanding of back problems and how to handlethem, and the setting up of a back care programme(called ‘Back school’) for chronic back pain sufferers. GSKalso makes sure that its managers and employees arebetter informed about back pain, so that they understandthat it’s possible for an employee to return to work, aspart of a suitable rehabilitation programme, before they’refully fit.
Case study adapted from Thomson I D S. HR Studies Update, No. 823, June 2006.
Case study 2 – GlaxoSmithKlineGlaxoSmithKline (GSK) has an employment healthmanagement (EHM) team that provides a holistic approachto managing the overall health of employees, covering theareas of mental health, musculoskeletal health, materialhandling and attendance management. The team includeshealth and resilience project leaders, whose role is todesign and implement healthcare programmes.
One such programme was the participatory workplaceergonomics programme. Local ergonomic improvementteams were established at each GSK site, comprisingemployees representing different functions, includingengineers, office support, staff and onsite EHM andhealth and safety professionals. Team members are givenbasic ergonomics training, a toolkit and access to adedicated ergonomics website to support them. Theteams meet regularly to discuss issues that have beenbrought to their attention by employees and considersolutions. Complex issues are often referred to a UK
Other physical health issuesThere are many other physical healthissues which can be addressed in awellbeing strategy. Projects shouldcombine controlling work-related risksand appropriate health surveillance(both legal requirements) withpromotion campaigns to encourageemployees to look after themselves.Issues include:- respiratory conditions: awarenessand control of work-related causes;smoking-cessation programmes
- skin safety: awareness and control ofwork-related risks; advice on handcare or sun safety
- noise and vibration: awareness andcontrol of work-related risks
- infection control: hand hygiene;vaccination policies.
You can get more information on someof these issues in Appendix E on pages32–36.
Healthy eating and obesityAccording to a recent research review,obesity has more than trebled in the UKduring the past 25 years.28 Being obeseor overweight is associated with ahigher likelihood of suffering numerouschronic illnesses, including cardiovasculardisease, diabetes, joint disorders andcertain types of cancer. Obesity costsEngland 18 million sick days and 30,000deaths every year. The increase inobesity appears to be due largely to adecrease in physical activity (calorieintake has changed little since 1980, butthe UK now travels 25 per cent less onfoot or by bicycle, and watches twice asmuch TV).
Healthy eating isn’t just aboutmaintaining a healthy weight. Abalanced diet can help to preventdigestive disorders (eg constipation),iron deficiency (which can makepeople feel tired, irritable and less ableto concentrate), bone conditions suchas osteoporosis, cancers of thegastrointestinal tract, as well as somehormone-related cancers (eg breast).Some also suggest that deficiencies insome vitamins and minerals can
increase the chance of feelingdepressed.29
Employees with balanced diets andgood eating habits may have lessdigestive-related absence and betterenergy, concentration and performancelevels.
Obesity can have an impact on healthand safety at work, for instance byaffecting employees’ fitness forphysically active tasks and their ability tocarry out tasks safely, such as manualhandling. Even for sedentary work, theremay be ergonomic impacts, eg standardoffice chairs may not be suitable forobese people.
Health promotion activities in this areashould focus on maintaining a healthy,balanced diet and physical fitness. It’sbetter to encourage people to loseweight slowly and maintain the loss,rather than diet intensively – peoplewho get into a cycle of loss-regain-loss(or ‘yo-yo’ dieting) can end with a poorbody image and a negative attitudetowards food. Employers shouldencourage obese employees who wantto lose weight to seek medical advice onhow best to do this.
There are several ways employers canhelp employees lose weight and eathealthily, eg making a range of healthyoptions available in staff canteens,promoting increased physical activity,and providing advice on healthy eatingin staff newsletters.
Employers should also consider howwork pressures can have a negativeimpact on employees’ diet. Manyemployees, for example, say that,because of work pressures, they:- don’t have the time to preparehealthy meals
- skip breakfast or lunch during theworking week
- have to work at their desk throughtheir lunch break.
For more information on healthy eating,see Appendix E on pages 32–36.
SmokingThe impact of smoking on health is welldocumented. It’s one of the biggestcauses of death and illness in the UK,resulting in 114,000 deaths a year.Smoking increases the risk of at least 50medical conditions, some of which canbe fatal. Others can cause irreversible,chronic damage to health. Theseinclude:- cancers of the lung, mouth, throat,larynx, oesophagus, bladder, kidney,pancreas and stomach
- coronary heart disease- stroke- chronic bronchitis and emphysema - impotence and reduced fertility - dementia- digestive problems.
Smoking also makes some work-relatedhealth conditions worse, eg asbestos-related disease, vibration white fingerand asthma.30
By law, all workplaces in the UK mustnow be smoke-free. Employers shouldhave smoke-free policies and considerhow they can support employees to quitsmoking. IOSH’s guide on smoke-freeworkplaces, A breath of fresh air,31 givesmore advice on this area. Some usefullinks are also included in Appendix E onpages 32–36.
Alcohol and drugsThere are clearly work-related safetyissues associated with allowingemployees to work while under theinfluence of alcohol or drugs. Employerswho knowingly allow employees towork under the influence of alcohol ordrugs, where this affects the safety ofthemselves and others, could beprosecuted under the Health and Safetyat Work Act. Transport system operatorsmay also be prosecuted under theTransport and Works Act 1992 if theydon’t show due diligence in trying toprevent employees working under theirinfluence. Employees affected by alcoholand drugs are likely to have increased
4 Key wellbeing issues
10

sickness absence and poorerperformance. A wellbeing approachshould consider the effect of alcohol anddrugs on the workplace. It’s also goodpractice for employers to offerinformation on their impact on healthand wellbeing, and provide those whoare dependent, or have family memberswho are dependent, with occupationalhealth support and the contact details oforganisations that can help them.
AlcoholMore than 90 per cent of people in theUK drink alcohol. In moderation,drinking alcohol isn’t likely to be aproblem, but drinking too much or atthe wrong time can be harmful.
Over the past 30 years, alcohol hasbecome cheaper and more widelyavailable. People are now drinking moreand starting to drink at a younger age.About one in three men and one in sixwomen have a health problem causedby alcohol, and according to the RoyalCollege of Psychiatrists,32 around one in15 men are physically addicted toalcohol.
Alcohol is the cause of many hospitaladmissions for physical illnesses andaccidents. Many of us are familiar withsome of the short-term effects ofalcohol. Alcohol also leads to long-termphysical health problems such as liverdisease and an increased risk of somecancers, as well as mental healthproblems such as depression, memoryloss and brain damage. Alcohol-relateddeaths increased by 19 per cent from2001 to 2006. NHS hospital admissionsin England with a primary or secondarydiagnosis specifically related to alcoholhave more than doubled over the past10 years.33
In the UK, up to 17 million working daysare lost annually due to alcohol-relatedabsence, and absenteeism from workthrough alcohol misuse has beenestimated to cost the economy about£1.5 billion.34
Alcohol can affect work performance infour main ways:- working while under its influenceincreases the likelihood of mistakes,errors of judgment and increasedaccidents. It can also lead toinappropriate behaviour
- the after-effects of drinking canimpair both work attendance andperformance. Many people take sickleave, but those who go to workmay have difficulty concentrating orworking at their normal pace
- persistent heavy drinking can lead toa range of social, psychological andmedical problems, includingdependence
- employees with family members whoare alcohol-dependent may find theimpact of dealing with the problemaffects their work performance.
DrugsIt’s an offence, under the Misuse ofDrugs Act 1971, to produce, supply andpossess most controlled drugs except incertain specified circumstances, eg whenprescribed by a doctor. Those whoknowingly permit the production orsupply of controlled drugs, or the takingof drugs on their premises, could also becommitting an offence.
People can also misuse certain solvents,which may be available at work.Possessing solvents isn’t illegal, andmany are often present in theworkplace.
The 2007/08 British Crime Surveyestimates that 35.8 per cent of 16 to59-year-olds have used one or moreillicit drugs in their lifetime, and 9.3 percent used one or more illicit drugs inthe previous year. The survey alsoestimates that 13.9 per cent of thoseaged 16 to 59 have used a Class Adrug at least once in their lifetime, and3 per cent have used at least one ClassA drug in the previous year. (Class Adrugs are the most harmful andinclude ecstasy, cocaine and heroin.)Cannabis (a Class B drug35) is the drugmost likely to be used.36
An HSE report on the scale and impactof illegal drug use by workers foundthat:37
- in a survey of workers, 13 per centof respondents reported drug use inthe previous year. The rate variedconsiderably with age, from 3 percent of those over 50 to 29 per centof those under 30
- drug use is associated strongly withsmoking and heavy drinking
- drug use has a negative impact onperformance and is associated withan increase in minor injuries
- recreational drug use may affectsafety at work.
The Home Office website, Tacklingdrugs: changing lives,38 includesinformation for employers. Through thesite, employers can link to trainers whocan:- train employees in alcohol and drugissues
- advise and review alcohol and drugpolicies
- assess and advise individualemployees for treatment
- advise organisations how to promotesensible drinking.
Solvents are not physically addictive, butusers may develop a psychologicaladdiction to ‘sniffing’ solvents inresponse to underlying problems orworries. Between 1971 and 2005, justover half the deaths from solvent abusewere aged 14 to 18. However, in 2006and 2007 over two-thirds of those whodied from solvents were over 25.39
Employers often have solvents in theworkplace and so should be aware oftheir potential to be misused, particularlyif young people, eg those on workexperience, can get access to them.
For more guidance on the kind ofsolvents that can be misused, visit theRe-solv website.40
11

Alcohol and drug policiesEmployers should produce andimplement alcohol and drug policies inconsultation with their staff. The policiesshould seek to:- inform employees of the problemsassociated with alcohol and drugs,and how to identify if they have aproblem and where to get advice
- provide guidance to managers onhow to recognise employees withpotential alcohol and drug problemsand what to do about them
- provide employees with confidentialaccess to help and advice if theythink that they have an alcohol ordrug problem and are consideringseeking help voluntarily at an earlystage
- provide confidential help toemployees who have an alcohol ordrug problem that comes to lightthrough observation or normaldisciplinary procedures, for examplethrough poor work performance,absenteeism or misconduct. Fordrugs, employers need to considerthe legal requirements under theMisuse of Drugs Act
- tackle safety-related issues, eg byredeploying or dismissing those whohave put themselves and others atserious risk of harm through themisuse of alcohol or drugs at work.Policies on safety, performance ormisconduct should make clear whendismissal will be necessary
- identify where there’s a risk thatemployees could obtain drugs (egmedication and some solvents) in theworkplace and make sure thatsystems are in place to control access.
Some employers carry out screening foralcohol and drugs. Screening needs tobe implemented with care and can neverbe the complete answer to problemscaused by alcohol and/or drug misuse.
For more advice on alcohol policies andscreening, see the HSE’s Don’t mix it! Aguide for employers on alcohol at work.41
See the HSE’s Drug misuse at work: aguide for employers42 for guidance ondrug misuse.
For general guidance on both alcoholand drugs at work, visit the HSEwebsite.43
The ageing workforceA report produced by the HSE’s Healthand Safety Laboratory44 shows thatmany beliefs about the deterioratingwork ability of older people are myths.In reality, older workers vary greatly intheir physical and mental capabilitiesand so any adaptations to their workshould be based on their individualneeds and capabilities, not their age.
Musculoskeletal changes result in adecrease in muscular strength and spinalflexibility, so ageing workers may needto be given physically lighter work tasks.However, physical capacity can bemaintained by regular physical exercise.As with other employees, older workersbenefit from good working conditions,varied work and a healthy lifestyle.
Factors such as lifestyle, exercise,nutrition and smoking are likely to begreater determinants of health than age,so health promotion initiatives in theworkplace would benefit all employees,whatever their age. (The recommendedactivity levels for adults, given belowunder the heading ‘How much physicalactivity is good for you?’, are alsoappropriate for older people.) It’sparticularly important that older peopleretain their mobility through daily activityand take part in activities that promoteimproved strength, co-ordination andbalance. However, research indicatesthat there’s a greater risk of physicalinjury among older people, so theyshould avoid carrying out high intensityactivities, or activities that involvesudden or complicated movement,unless they are already used to this typeof exercise.
Physical activity In At least five a week, the ChiefMedical Officer45 states that ‘Physicalactivity not only contributes towellbeing, but is also essential for goodhealth’. Physical activity:- reduces the risk of developing majorchronic diseases (such as coronaryheart disease, stroke and type 2diabetes) by up to 50 per cent, andthe risk of premature death by about20 to 30 per cent
- helps to reduce obesity. (Obesitydoubles the risk of death, coronaryheart disease, stroke and type 2diabetes, and increases the risk ofsome cancers and musculoskeletalproblems.) People who use acombination of a low-calorie dietand physical activity to lose weightlose greater fat mass and conservemore lean tissue, which is likely to beimportant to long-term sustainedweight loss
- is effective as a treatment for mild,moderate and severe clinicaldepression, and may also helppeople with other mental illnesses.Regular moderate exercise helpspeople feel better by improving theirmood, reducing anxiety andimproving their self-perception. It canalso help reduce stress and improvesleep
- increases bone mineral density inadolescents, maintains it in youngadults, and slows its decline in oldage. In addition, aerobics-typeexercise programmes can also helpprevent recurrence of low back pain
- low to moderate intensity activity canproduce health benefits for olderpeople and help prevent age-relatedweight gain.
4 Key wellbeing issues
12
Why promote physical activity at work?In general, working adults spend asignificant proportion of their wakinghours at work, with many in sedentaryoccupations. Even though work isoften less physically demanding than inthe past, it still takes up a largeamount of people’s time. This cancause a dual disadvantage of longwork hours requiring little physicalactivity, and little free time or energy toexercise. It can therefore make goodsense to provide opportunities forphysical activity at work.
How much physical activity is good foryou?At least five a week45 recommends atotal of at least 30 minutes a day ofmoderately intense physical activity onfive or more days of the week isneeded to reduce the risk of ill healththrough inactivity. Many people need
45 to 60 minutes of such physicalactivity each day to prevent obesity.Physical activity can be built up inbouts of 10 minutes or more, egwalking to and from work, taking alunchtime walk or climbing stairsinstead of using the lift.
A person who engages in moderatelyintense activity on a regular basisshould be able to continue that activityfor many minutes without exhaustion,and will usually experience:- an increase in breathing rate- an increase in heart rate, to thelevel where the pulse can be felt
- a feeling of increased warmth,possibly accompanied by sweatingon hot or humid days.
The amount of activity a person needsto do to achieve moderate intensityvaries from one individual to another.
A person who is unfit or overweightmay only have to walk up a slope toexperience these feelings, whereas avery fit athlete may be able to continuephysical activity for some time beforethe feelings become noticeable.The good news for employers is that ifthey create opportunities foremployees to have short bouts ofmoderate physical activity, this will helpthose who are unfit or have busylifestyles – and who take advantage ofthe opportunities – reach therecommended level. This level ofactivity includes:- commuting by foot or bike- having a job that includes regularphysical tasks (delivering post,decorating)
- carrying out regular household orgarden activities
- taking part in regular recreation orsocial sport at moderate intensity.
East Sussex Council employs more than 15,000 staff.Three years ago, the absence rate was relatively high –over nine days per person each year. This cost the councilapproximately £7.5 million a year. At one point there were250 staff signed off on long-term sick leave. East Sussexwanted to tackle their high absence rate and to promotethemselves as a caring employer that looks afteremployees’ health and wellbeing.
The first step was to increase the size of the occupationalhealth team. The council created two-and-a-half full-timeoccupational health adviser posts, and gave staff moreopportunity to access a doctor. Tough measures werebrought in to reduce the absence rates, balanced by aseries of wellbeing-related schemes.
New members of staff are not entitled to sick pay untilthey’ve reached a year’s service and those who are off sickfor longer than four weeks, or more than twice in sixmonths, are automatically referred to an occupationalhealth physician. However, employees now have access to: - free smoking-cessation clinics - sessions on reflexology, slimming, massage and pilates(all at around £15 a session)
- a tailored personal training programme, ‘Fit bug’ - a once-yearly image consultancy workshop, ‘Colour me beautiful’
- a network of 150 local counsellors, with the councilproviding the first five sessions free.
All these services are made available to staff at reducedrates. The council is also considering offering staff access tophysiotherapy to help alleviate musculoskeletal problems.
The impact of the changes has been immediate. Sicknessrates dropped to eight days per year, saving the council £1 million (which more than compensates for the£100,000-a-year cost of extra occupational health advisersand increased doctor time). Staff surveys indicate thatemployee morale has also improved, as 73 per cent ofstaff enjoy working for the council, up 6 per cent on theprevious year.
Communication has been one of the key reasons for thesuccess of the approach. Changes and new schemes havebeen promoted on TV screens in the staff canteen, atteam briefings and on the intranet.
Case study provided by Leatham Green, Assistant Director forPersonnel and Training, East Sussex Council. A fuller version of thecase study is on the Improvement and Development Agency forLocal Government website, under the organisational good practicelibrary, at www.idea.gov.uk/idk/core/page.do?pageId=7355969.
13
Case study 3 – East Sussex Council

At its simplest, employers need toprovide employees with informationand create opportunities for them toengage in a healthy lifestyle.
When promoting physical activity, themain focus should be to encourageemployees to engage in short bouts ofmoderate activity on most days. Thiswill be of particular benefit to thosewho are not currently sufficientlyphysically active. Employers could:- have a flexible working policy thatallows employees to exercise beforework or during their lunch break
- encourage employees to walk orcycle to work, which also promotesthe wider benefits of energy efficiencyand reduced transport costs
- encourage the use of stairs ratherthan lifts
- provide healthy eating options incanteens and offer healthyalternatives, such as fresh fruit andvegetables, at meetings andworking lunches
- hold ‘healthy cooking’demonstrations and include healthyrecipes in staff newsletters
- provide health promotioninformation on their staff intranet,notice boards and in newsletters
- arrange discounts for staff at localleisure centres and health clubs
- provide information on walks nearwork (local authorities may be ableto help with this and may also run‘health walk’ schemes)
- provide support to employees whowant to quit smoking or break theiralcohol or drug dependency
- encourage employees to set up andattend support groups, eg weightloss or walking clubs
- if resources permit, provide cyclingstorage, shower facilities, orsubsidise some low impact activitiessuch as yoga or t’ai chi
- promote fitness as part of otherroutine training programmes, eghow to use machinery, tools orequipment.
The case studies in this guide and thelinks to more case studies (see page22) will help stimulate more ideas.
The most successful health promotionprojects are likely to be those that areflexible, positive and fun. The aimshould be to provide a range ofdifferent activities that are accessible tomost staff, whatever their fitness level.Here, employers need to considerequality and diversity issues and becareful not to discriminate. For instance,physical activities may need to includethose that are accessible to employeeswith disabilities. There may be culturalreasons why people in some ethnicgroups may not join in (eg dress codes),so employers, particularly those with anethnically diverse workforce, need tounderstand cultural barriers and explorehow they can be overcome.
Employees should be involved inplanning and designing activities.Communicating the availability ofactivities and their success is veryimportant. Setting pedometer or stairclimb challenges can help to getemployees thinking about their health.A wellbeing event is also a good wayof engaging employees (see AppendixD, page 29). The Well@Workevaluation report12 is a good source ofinformation on what makes healthpromotion projects successful.
As highlighted by social marketingtechniques, employees are more likely toengage in activities if they can see thebenefits for themselves.46 It’s also usefulto link to national health initiatives andcampaigns such as ‘Race for life’ (seepage 36), and to make the most of themedia. For example, dancingcompetitions are popular televisionprogrammes, so perhaps now’s the timefor lunchtime salsa lessons!
There are small risks that employeescarrying out physical activities at workwill be injured and employers may beworried about liability. These risks areminimal if activity is limited tomoderate intensity and if people are
advised to progress gradually from onelevel of intensity to the next. It’ssensible to produce a statement thatadvises employees that they’reresponsible for making sure they’rewell enough to do physical activities,and that they may need to take advicefrom their GP.
If an employer wants to hold sportsevents, especially higher impactactivities, they should be organised bypeople who are competent in thatsport (sporting professional bodieswill help you identify the appropriatequalification). A competent sportsprofessional will be able to check thehealth status of employees takingpart in the activity, advise theemployer on the suitability of theirvenue, and will often be trained infirst aid. The employer should makesure the sports professional has publicliability insurance, and check thattheir own insurance takes suchactivities into consideration.
Employers who are concerned thatincreased physical activity may lead tomore injuries, and hence sicknessabsence, may be reassured by studieswhich suggest that introducingphysical activity initiatives at workreduces work injuries.47
Employers sometimes promote the useof ‘therapies’ such as massage oraromatherapy. There’s little, if any,evidence that some popular therapiesimprove physical or mental health, butthey may have their place inimproving employees’ sense ofwellbeing and of being valued by theiremployer. Care should be taken asthere may be health risks associatedwith some therapies, so it’s best tostick to well established treatments,where the provider is able todemonstrate competence throughrecognised qualifications. These canbe identified by contacting therelevant professional body. Some localauthority adult education centres areable to run ‘taster sessions’ or shortcourses in the workplace.
5 How should employers promote health?
14

Burnley has some of the worst health indicators inEngland. Burnley Borough Council works with otherpartners to develop and deliver the East Lancashire Healthand Well-Being Strategy, with the aim of improving thehealth of its citizens. A large proportion of councilemployees live in Burnley, so it made sense to have awellbeing strategy aimed at employees too. The councilalso recognised that good staff attendance is vital ifimproved performance is to be maintained. A majorcontribution to achieving this is to have a safe, happy andhealthy workforce.
Against this background, the council’s people anddevelopment team (which includes human resources andhealth and safety professionals) sought to implement aholistic approach to employee wellbeing that wouldinform policy development, reduce the number of days’absence per employee, including absence due to stress-related illness, and improve the effectiveness of theworkforce.
A wellbeing group was formed (sponsored by the leaddirector for health and safety), bringing togetheremployees from:- people and development- equalities and access- planning and environment- healthy lifestyles- communications- UNISON, the trade union.
The group has carried out several initiatives as part of awellbeing strategy. The strategy has senior managersupport. Employees were encouraged to complete aquestionnaire, which has been used to inform eventplanning. The group’s success comes from the commitmentof all the professionals involved.
Projects to date have included:- developing a ‘Be well’ handbook, which givesemployees lifestyle tips, provides information on thecouncil’s family-friendly policies and how to access itswellbeing initiatives (eg gym classes, smoking-cessationsessions), and gives signposts to help from externalorganisations
- running several events during a stress awareness weekto give people a taste of different wellbeing initiatives,including free swimming, yoga and other exerciseclasses, as well as presentations on neuro-linguisticprogramming,acupressure and reflexology
- discounted membership of the council’s leisure facilitiesand a weekly yoga class
- a ‘know your numbers’ blood pressure day - smoking-cessation classes, which employees couldattend in work time
- monthly wellbeing bulletins published on the intranet- revising or introducing several policies, including thoseon managing attendance, stress, infection control,performance management and flexible retirement
- providing managers with risk assessment training - running stress management workshops- developing policies on breastfeeding and domesticviolence
- holding workplace events for employees who needsupport to change health-related behaviours
- introducing a ‘cycle-powered smoothie maker’ atvarious council offices.
One of the measures of their strategy’s success has been afall in the number of days lost to stress per employee, from3.35 in 2006/07 to 2.55 in 2007/08.
The council plans to continue to run wellbeing eventsthroughout the year to coincide with national and localinitiatives, eg walk to work, men’s health week and obesityawareness, and to implement a buy-a-bike scheme. It alsointends to introduce a supportive friends network, as wellas continue to provide counselling and cognitivebehavioural therapy to employees, and revise or producewellbeing-related policies that cover issues such as alcoholand drugs, bullying and harassment.
Case study provided by Heather Brennan, People and DevelopmentManager, and Simon Astin, Assistant Health and Safety Adviser,Burnley Borough Council.
15
Case study 4 – Burnley Borough Council

A recent study11 outlines some keyelements that make a wellbeinginitiative successful. These include:- programmes designed to meetemployees’ needs and values
- senior management buy-in – thisgoes beyond mere endorsement toactive and visible participation
- programmes aligned to the overallaims and goals of the business
- good communication, both in termsof employees being informed andupdated on initiatives, and beingconsulted on their needs and viewson future programmes
- a means of measuring theoutcomes and business benefits.
Who should lead a wellbeingstrategy?Human resources, occupational healthand OSH practitioners all have a keyrole in planning and delivering awellbeing strategy. However, for thestrategy to be successful, it needs to beled by a senior manager who candemonstrate commitment to wellbeingand act as a champion and role model.It’s also important that line managerssupport the strategy.
Who should play a part in thestrategy?The relative contribution made byhuman resources, occupational healthand OSH practitioners depends on theorganisation’s priorities. However, keyto the success of the strategy will beemployees’ support. It’s important,therefore, that trade union, safety oremployee representatives are involved.As already explained, managers play akey role in implementing the strategyand so need to be on board. Employersmay also be able to get support fromorganisations that offer healthpromotion services, for example somelocal councils and NHS trusts. Appendix B (page 25) shows the keystakeholders in a wellbeing strategyand the roles that they can play. Therelationship is also shown in Figure 1.
To implement the strategy, a teamshould be set up, led by a seniormanager and include representatives ofall the key stakeholders.
6 Implementing a wellbeing strategy in the workplace
16
Figure 1: A healthy organisation
Identifying parameters andprioritiesIt can be helpful to consider wellbeingunder the general headings of:- promoting health and wellbeing(helping people to stay fit and healthy)
- the effect of work on health(continuing to make sure peoplearen’t injured or made ill by theirwork)
- the effect of health and wellbeing onwork (helping people with healthconditions and impairments toremain in or return to work).
Appendix B (page 25) shows the areasthat wellbeing covers.
Your wellbeing strategy team shouldstart by carrying out an analysis toidentify:- what your organisation does now- what your organisation needs to do- what your gaps and priorities are.
When deciding your priorities, you’llneed to consider what’s likely to havethe greatest impact, taking account ofyour organisational culture (sometimesreferred to as ‘the way we do thingsaround here’).48,49 For instance,investing in a large health promotionprogramme may not result in sustainedimprovement in health, unless yourorganisation has a positiveunderpinning health and safety culture.Without a positive health and safetyculture, it will probably have littleimpact. A greater impact is likely to beachieved through a resourcedrehabilitation programme, as evidencesuggests that such programmes canpay for themselves by reducing thecost of sickness absence.10 As forhealth promotion, there are manyactivities that employers can encourageto promote health at minimal cost andwhich may gradually engageemployees.
The views of employees are veryimportant. Wellbeing programmes arelikely to be more successful ifemployees are asked what theyconsider is important and whether thisis taken into account.
Implementing the strategyIn general, it’s better to implementwellbeing-related initiatives as a seriesof discrete, sustainable projects,communicating and building on thesuccess of each project. Each projectshould have clear, measurableoutcomes and be part of an overallprogramme. The team set up to deliverthe wellbeing strategy will need to helpreview the effect of wellbeinginitiatives and the process for comingup with new ideas to excite andmotivate employees. Some suggestedstrategies and programmes to improvemental and physical wellbeing aregiven in this guide, as well as guidanceon delivering wellbeing events inAppendix D (pages 29–31) and links toresources in Appendix E (pages 32–36).The case studies in this guide andthose referenced on page 22 shouldalso help to generate ideas.
Measuring your successSenior managers will expect to see thebusiness case for a wellbeing strategyto include measures of success, such asreduced sickness absence rates andpositive outcomes from employeesurveys. Important survey measures arewhether the employee feels valued andenjoys working for the organisation.The success of individual healthpromotion programmes can bemeasured in terms of short-termoutcomes (eg weight loss through adiet club) or sustained engagement inthe activities set up by the employer.However, obtaining an objectivemeasure of sustained improvements inemployees’ health and lifestylebehaviour could be challenging.
Financial benefits can be calculatedfrom associated cost savings (minus thecost of interventions), through reducedsickness absence, staff turnover, injuryclaims or health insurance. There mayalso be other financial benefits.Building the case for wellness11 is auseful source of information onevaluating wellbeing programmes froma financial perspective.
To help you assess the impact ofwellbeing programmes on costs, andthe cost of ill health to yourorganisation, use the Health, Work andWellbeing business healthcheckevaluation tool50 and the HSE’s illhealth costs calculator.51
Health checks Health checks as part of a wellbeingstrategy are usually voluntary, and areoften popular and well taken up byemployees. A health check can rangefrom expensive ‘executive medicals’ toIT-based questionnaires with pointersto sources of health and advice. Datacan be stored anonymously from suchsources, and organisations can usethem to produce an overview of thehealth of their workforce and targetprogrammes where there is thegreatest need. For example, if you havea significant number of workers whoare obese and want to lose weight, orsmokers who want to kick the habit, itcan make good business sense totarget programmes at these groups.
As part of an overall strategy, voluntaryhealth screening can be beneficial inearly detection of disease in a smallnumber of cases, but is probably morebeneficial to most in giving anopportunity to have a health-baseddiscussion and to steer people intomore healthy lifestyles. However,careful thought needs to be given as tothe purpose, objectives and outputs ofsuch health checks and also to theroles of the professionals involved.
17

Under the Data Protection Act 1998,health data is sensitive information, soemployers should not collect it unlessit’s necessary. If an employer doescollect it, they should keep itconfidential. Most employees wouldprobably find it unacceptable to givethis kind of information directly totheir employer. However, if they knowthat healthcare professionals have aduty of confidentiality, employees maybe happy to give it to an occupationalhealth professional, including one whoworks in their organisation.
The organisation also needs to givesome thought to how it will respond ifinformal health checks identify thatsomeone who works in a safetycritical occupation has a healthproblem, for instance if someonewhose work involves driving is foundto be alcohol-dependent. If afterundergoing voluntary health checksemployees find that it leads to threatsto their employment, it mayundermine the wellbeing approach.The Faculty of Occupational Medicineoffers guidance for occupationalphysicians on the ethical principlesgoverning occupational medicine andissues such as the status ofoccupational health records.52
In safety critical work such as drivingtrains or flying planes, employers oftenrequire employees to undergo alcoholand drug testing. Such testing shouldnot be confused with general healthchecks designed to promote healthand wellbeing at work, although thisaim can be fulfilled by such checks,depending on their nature and if donepositively. Alcohol testing in safetycritical areas, for example, is obviouslyvery different to providing ‘voluntaryhealth checks’. Such specialist workneeds a chain of custody* andmedico-legally driven processes.53 It’salso important not to confuse healthchecks with health surveillance, wherethe law requires that employeesexposed to certain work-related healthhazards are monitored for early signsof any problems.
Wellbeing eventsA useful way of encouragingemployees to take an interest in theirhealth and get a taste of activities thatcan improve their wellbeing can be tohold a wellbeing event.
All events should have at least thefollowing key stages:- planning and preparation- build-up - event delivery- breakdown- wash-up and evaluation- appreciation and acknowledgment.
For more information on these stages,as well as a real-life example of twoevents held by an organisation, seeAppendix D, pages 29–31.
6 Implementing a wellbeing strategy in the workplace
18
* Chain of custody records should be maintained throughout the life of the evidence and must document every instance of contact with theevidence and the action performed on it.

We know that being in work can beone of the best things for health, aslong as the work is ‘good’.1,54,55
Employers should help keep theirworkers well and healthy by makingsure that work isn’t carried out inconditions that lead to stress, MSDs orother health problems. In addition,employers who want theirorganisations and employees to be‘working well’ will need to:
- Ensure a good employee-to-job ‘fit’,ie matching employees’ skills andexperience to their job requirements.
- Take account of organisationalvalues, the ‘reality’ of the job andthe employees’ expectations. Atperformance appraisals, it’s usefulto review how the reality of anemployee’s job may contrast withtheir expectations and values.
- Regard wellbeing as a jointresponsibility of management andemployees, and make sure yourorganisation’s policy reflects this.Point out the benefits of preservingwellbeing for both the employer(such as efficiency and increasedmorale) and employee (eg improvedhealth and resilience).
- Regard working with a healthcondition as the norm, as long asappropriate modifications can bemade to the workplace and suitablesupport is put in place. An ageingworkforce means this will becomemore important in the future.
- Promote a positive organisational‘climate’. This is about howemployees perceive the organisationthrough its managerial practices,leadership behaviours, how itinvolves employees and also thereward systems. ‘Climate’ is alsoused to describe the tangibleoutputs of an organisation’s healthand safety culture, as perceived byemployees at a point in time. It canbe measured using surveys,supplemented by observations,workshops and focus groups.
- Make sure that managers reflectthe wellbeing policy in their actions.This consistency will lead to anincrease in employees’ trust in theorganisation. It’s possible to auditthis by examining consistency inareas such as selection andrecruitment, communication in theorganisation, sickness management,performance measurement andflexible working practices.
- Monitor holistic wellbeing. Thisinvolves measuring quality of lifejudgments,* physiological healthindicators and health beliefs, as wellas standard stress indicators, suchas those described in the HSE’sstress management standards. So,include wellbeing factors in yourstress risk assessment. A tableproduced by Lunt,7 whichsummarises these, is included inAppendix C, page 28.
As part of a multi-professionalapproach, OSH practitioners can helpemployers make appropriate changesto the work environment, the job orthe working arrangements, to supportemployees with health problems andimprove workers’ health and wellbeing.They can help educate and raiseawareness among employers,employees and fellow professionalsabout the benefits of healthyorganisations, what makes work‘good’, and how to develop ‘wellbeingassets’ in the workplace.
19
7 Conclusion
* Debate still continues on definitions for quality of life; collectively they highlight that it’s a subjective state encompassing physical, psychologicaland social functioning, and a key feature is its basis on the perceived gap between actual and desired living standards.7
1. Waddell G and Burton K. Is workgood for your health and well-being? London: The StationeryOffice, 2006.
2. Harter J K, Schmidt F L and KeyesC L M. Well-being in the workplaceand its relationship to businessoutcomes: a review of the Gallupstudies. 2002. media.gallup.com/DOCUMENTS/whitePaper--Well-BeingInTheWorkplace.pdf.
3. Institute of Directors. Well-being atwork: how to manage workplacewellness to boost your staff andbusiness performance. London:IOD, 2006.
4. Chartered Institute of Personneland Development. What’shappening with well-being atwork? London: CIPD, 2007.www.cipd.co.uk/NR/rdonlyres/DCCE94D7-781A-485A-A702-6DAAB5EA7B27/0/whthapwbwrk.pdf.
5. Chartered Institute of Personneland Development. Thepsychological contract. Factsheet.January 2009. www.cipd.co.uk/subjects/empreltns/psycntrct/psycontr.htm?IsSrchRes=1.
6. Department for Work andPensions, Department of Health,Health and Safety Executive.Health, work and well-being –Caring for our future: a strategy forthe health and well-being ofworking age people. 2005.www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_4121757.pdf.
7. Chartered Institute of Personneland Development. Annual surveyreport 2008: absencemanagement. London: CIPD, 2008.www.cipd.co.uk/NR/rdonlyres/6D0CC654-1622-4445-8178-4A5E071B63EF/0/absencemanagementsurveyreport2008.pdf.
8. Lunt J, Fox D, Bowen J, Higgs G,Crozier S and Carter L. Applyingthe biopsychosocial approach tomanaging risks of contemporaryoccupational health conditions:
scoping review. HSL/2007/24.Buxton: HSL, 2007.www.hse.gov.uk/research/hsl_pdf/2007/hsl0724.pdf.
9. Helliwell J F and Putnam R D. Thesocial context of well-being.Philosophical Transactions of theRoyal Society, London B 2004; 359:1435–1446 doi:10.1098/rstb.2004.1522.www.pubmedcentral.nih.gov/picrender.fcgi?artid=1693420&blobtype=pdf.
10. Health and Safety Executive.Management standards for work-related stress. www.hse.gov.uk/stress/standards/index.htm.
11. PricewaterhouseCoopers. Buildingthe case for wellness. 2008.www.workingforhealth.gov.uk/documents/dwp-wellness-report-public.pdf.
12. British Heart Foundation.Well@Work programme.www.bhfactive.org.uk/evaluation/previousprojects.html.
13. Investors in People. Health andwellbeing at work.www.investorsinpeople.co.uk/MEDIARESEARCH/TOOLS/Pages/HealthAndWellbeingatWork.aspx.
14. Investors in People. Health &wellbeing at work. 2009.www.investorsinpeople.co.uk/Documents/Health%20and%20Wellbeing/2009/HealthWellbeing_ResourcePack_March09.pdf.
15. Fennell P A. A four-phase approachto understanding chronic fatigue.In: Jason L A, Fennell P A andTaylor R (eds). Handbook of chronicfatigue. Hoboken, N J: John Wiley &Sons Inc, 2003: 155–175.
16. IOSH. A healthy return – Goodpractice guide to rehabilitatingpeople at work. Wigston: IOSH,2008. www.iosh.co.uk/files/technical/A%20HEALTHY%20RETURN121208%2Epdf.
17. Wilson A. The commercial case forhealth and wellbeing.www.scmh.org.uk/pdfs/nehin_july07_alexwilson.pdf.
18. The Sainsbury Centre for MentalHealth. Mental health at work –developing a business case. Policypaper 8. December 2007.www.scmh.org.uk/pdfs/mental_health_at_work.pdf.
19. CIPD. Line management behaviourand stress at work.www.cipd.co.uk/subjects/health/stress/_lnstrswrk.htm?IsSrchRes=1.
20. HSE. Stress managementcompetency indicator tool.www.hse.gov.uk/stress/mcit.htm.
21. HSE. Management standardsindicator tool. www.hse.gov.uk/stress/standards/pdfs/indicatortool.pdf.
22. EEF. Work organisation assessment.www.workorganisation.org.uk.
23. www.shift.org.uk; www.seemescotland.org.uk.
24. BackCare. Back facts.www.backcare.org.uk/335/Facts-and-figures.html.
25. Health and Safety Executive. Healthand safety statistics 2007/08. 2008.www.hse.gov.uk/statistics/overall/hssh0708.pdf.
26. NHS Choices. Back pain at work.www.nhs.uk/Livewell/workplacehealth/Pages/Backpainatwork.aspx.
27. Brown D. Corporate solutionsconsulting UK for HSE. Initiativeevaluation report: Back in work.CRR 441/2002. Sudbury: HSEBooks, 2002. www.hse.gov.uk/research/crr_htm/2002/crr02441.htm.
28. Butland B, Jebb S, Kopelman P,McPherson K, Thomas S, Mardell Jand Parry V. Trends and drivers ofobesity: a literature review for theForesight project on obesity. 2007.www.foresight.gov.uk/Obesity/Literature_Review.pdf.
29. Ahrens U. Food facts: food andmood. The British DieteticAssociation. 2006.www.wellnessdevon.co.uk/HTML/resources/food%20facts%20food%20and%20mood.pdf.
References
20
30. NHS. What are the health risks ofsmoking? www.nhs.uk/chq/pages/2344.aspx?CategoryID=53&SubCategoryID=53&r=1&rtitle=http%3a%2f%2fwww.nhs.uk%2fchq++2344%3fCategoryID%3d53%26SubCategoryID%3d53.
31. IOSH. A breath of fresh air:managing a smoke-free workplace.WIgston: IOSH, 2008.www.iosh.co.uk/files/technical/A%20BREATH%20OF%20FRESH%20AIR%201%2Epdf.
32. The Royal College of Psychiatrists.Alcohol and depression.www.rcpsych.ac.uk/mentalhealthinformation/mentalhealthproblems/alcoholanddrugs/alcoholdepression.aspx.
33. The NHS Information Centre.Lifestyles statistics. NHS data onalcohol admissions. 2008.www.ic.nhs.uk/webfiles/publications/alcoholeng2008/Statistics%20on%20Alcohol-%20England%202008%20final%20format%20v7.pdf.
34. The Institute of Alcohol Studies.Alcohol and the workplace. 2008.www.ias.org.uk/resources/factsheets/workplace.pdf.
35. Home Office. Advisory Council onthe Misuse of Drugs. Cannabis:classification and public health.2008. drugs.homeoffice.gov.uk/publication-search/acmd/acmd-cannabis-report-2008?view=Binary; drugs.homeoffice.gov.uk/publication-search/cannabis/acmd-cannabisreclassification?view=Binary.
36. Home Office. Drug misusedeclared: findings from the2007/08 British Crime Survey.drugs.homeoffice.gov.uk/news-events/latest-news/drug-misuse-declared?version=1.
37. Smith A, Wadsworth E, Moss S andSimpson S. The scale and impact ofillegal drug use by workers.Sudbury: HSE Books, 2004.www.hse.gov.uk/research/rrpdf/rr193.pdf.
38. Home Office. Tackling drugs,changing lives: Drugs strategy –National workplace initiative.drugs.homeoffice.gov.uk/drug-strategy/drugs-in-workplace/national-workplace-initiative.
39. Field-Smith M E, Butland B K,Ramsey J D and Anderson H R.Trends in death associated withabuse of volatile substances1971–2007. Report 22. London: StGeorge’s, University of London,2009. www.sgul.ac.uk/about-st-georges/divisions/faculty-of-medicine-and-biomedical-sciences/mental-health/icdp/our-work-programmes/volatile-substance-abuse-mortality-study/volatile-substance-abuse-mortality-reports-1/vsa-report-22.pdf.
40. www.re-solv.org. 41. Health and Safety Executive. Don’t
mix it! A guide for employers onalcohol at work. www.hse.gov.uk/pubns/indg240.htm.
42. Health and Safety Executive. Drugmisuse at work: a guide foremployers. Sudbury: HSE Books,1998. www.hse.gov.uk/pubns/indg91.pdf.
43. Health and Safety Executive.Alcohol and drugs at work.www.hse.gov.uk/alcoholdrugs.
44. Benjamin K and Wilson S. Factsand misconceptions about age,health status and employability.HSL/2005/20. Buxton: Health andSafety Laboratory, 2005.www.hse.gov.uk/research/hsl_pdf/2005/hsl0520.pdf.
45. Department of Health. At least fivea week: evidence on the impact ofphysical activity and its relationshipto health. London: DOH, 2004.www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4080994.
46. Weinreich N K. What is socialmarketing? www.social-marketing.com/Whatis.html.
47. Scottish Executive. Let’s makeScotland more active: a strategy for
physical activity. Edinburgh:Scottish Executive, 2003.www.scotland.gov.uk/Resource/Doc/47032/0017726.pdf.
48. Guldenmund F W. The nature ofsafety culture: a review of theoryand research. Safety Science 2000;34 (1–3): 225.
49. IOSH. Promoting a positive culture.Wigston: IOSH, 2004.www.iosh.co.uk/files/technical/PromotingAPosCulture%2Epdf.
50. Health, Work and Wellbeing,PricewaterhouseCoopers andBusiness in the Community. Thebusiness healthcheck.www.workingforhealth.gov.uk/Initiatives/business-healthcheck-tool/Default.aspx.
51. Health and Safety Executive. Ill-health costs introduction.www.hse.gov.uk/costs/ill_health_costs/ill_health_costs_intro.asp.
52. Harling K and Hunt S (eds).Guidance on ethics foroccupational physicians. 6th ed.London: Faculty of OccupationalMedicine, 2006.
53. A working group of the Faculty ofOccupational Medicine. Guidanceon alcohol and drug misuse in theworkplace. London: Faculty ofOccupational Medicine, 2006.
54. Cross-government Health, Workand Well-being Programme. DameCarol Black’s review of the healthof Britain’s working agepopulation. Summary of evidencesubmitted. London: The StationeryOffice, 2008.www.workingforhealth.gov.uk/documents/summary-of-the-evidence.pdf.
55. The Royal College of Psychiatrists.Mental health and work. London:RCP, 2008.www.workingforhealth.gov.uk/documents/mental-health-and-work.pdf.
56. HSE. Securing health together.www.hse.gov.uk/sh2.
57. Department of Health. Choosinghealth: making healthy choiceseasier. Public Health White Paper.
21
http://drugs.homeoffice.gov.uk/publication-search/cannabis/acmd-cannabisreclassification?view=Binary
London: Stationery Office, 2004.www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4094550.
58. Cross-government Health, Workand Well-being Programme.Working for a healthier tomorrow:Dame Carol Black’s review of thehealth of Britain’s working agepopulation. London: The StationeryOffice, 2008.www.workingforhealth.gov.uk/documents/working-for-a-healthier-tomorrow-tagged.pdf.
59. The Employment and SupportAllowance Regulations 2008. www.opsi.gov.uk/si/si2008/uksi_20080794_en_1.
60. Department of Health. Healthyweight, healthy lives: a cross-government strategy for England2008. www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_082378.
61. Department of Health, HomeOffice. Safe. Sensible. Social. Thegovernment’s alcohol strategy.www.dh.gov.uk/en/Publichealth/Healthimprovement/Alcoholmisuse/DH_085386.
62. Health and Safety Executive. Stress-related and psychological disorders.www.hse.gov.uk/statistics/causdis/stress/index.htm.
63. Health and Safety Executive.Musculoskeletal disorders.www.hse.gov.uk/statistics/causdis/musculoskeletal/index.htm.
64. Health and Safety Executive. Healthand safety statistics 2007/08.Overall picture for Britain.www.hse.gov.uk/statistics/overpic.htm.
65. Department for Work andPensions, Department of Health.Improving health and work:changing lives. The government’sresponse to Dame Carol Black’sreview of the health of Britain’sworking-age population. London:The Stationery Office, 2008.www.workingforhealth.gov.uk/documents/improving-health-and-work-changing-lives.pdf.
References
Training for OSH practitioners
Links to more case studies
22
It’s important that OSH practitionersknow the extent of their competenceand their limitations. The followingcourses may be useful for increasingcompetence in occupational healthissues. Appendix E (pages 32–36) alsogives links to organisations that canprovide occupational health advice.
IOSH offers a range of ContinuingProfessional Development courses forOSH practitioners, covering topics suchas MSDs, work-related stress, basicpsychology, rehabilitation andergonomics. For a full list of coursesand more details, visitwww.iosh.co.uk/index.cfm?go=courses.cpd_brochure.
The University of Nottingham offers anMSc course in workplace health thatmeets the needs of the OSHpractitioner – seewww.nottingham.ac.uk/iwho/workplacehealth.
You can get more case studies on thefollowing websites:
British Heart Foundationwww.bhf.org.uk/healthatwork andwww.bhf.org.uk/HealthAtWork/success_stories.aspx
Health, work and wellbeingwww.workingforhealth.gov.uk/Case-Studies/Default.aspx
NHS Pluswww.nhsplus.nhs.uk/public/casestudies.asp
Securing health togetherwww.hse.gov.uk/sh2/casestudies.htm
Staff Wellbeing – creating successthrough wellbeing in higher education www.wellbeing.ac.uk/casestudies.php

Political driversIn July 2000, the UK governmentpublished Securing health together,56 a10-year occupational health strategy. Itsets out a vision to tackle high levelsof work-related ill health and toreduce the personal suffering, familyhardship and costs to individuals,employers and society.
In November 2004, the Department ofHealth published its public health whitepaper, Choosing health: makinghealthier choices easier.57 The paperoutlines key principles for helping thepublic make healthier and moreinformed choices about their health. Itwas followed in 2005 by thegovernment’s strategy for the healthand wellbeing of working age people,Health, work and well-being – Caringfor our future.6 The aim of the strategyis to create workplaces where thehealth and wellbeing of employees isprotected, and to give employees everyopportunity to improve their healthand wellbeing.
The strategy states that success shouldlead to:- an improvement in the health andwellbeing of people of working age
- increased employment – with morepeople able to work than everbefore
- optimal performance andattendance – with people absentfrom work less
- people and their employers beingempowered to promote and protecttheir own health
- increased productivity – so thatpeople are more effective whenthey’re at work
- a reduction in health inequalitiesand social exclusion, resulting inbenefits for individuals, families,communities and society
- people being able to work to a laterage if they wish
- people with health problems ordisabilities being able to optimisetheir work opportunities.
For some time, concern had beenexpressed in government circles andbeyond about the large numbers ofworking age people claiming incapacitybenefit, in particular the number ofclaimants suffering from a mental healthcondition. Unlike other conditions, theirnumber failed to reduce, remaining ataround 200,000 per year since 1996.58
In 2008, the government replacedincapacity benefit with the employmentand support allowance, with the aim ofhelping people return to and remain inwork. The assessment for support isnow based on identifying what theclaimant can do, rather than focusingon their disability.59
The government strategy, Healthyweight, healthy lives,60 identifies fiveareas for tackling excess weight:- preventing weight problems inchildren to avoid the ‘conveyor belt’effect into adulthood
- promoting healthier food choices –reducing the consumption of foodsthat are high in fat, sugar and salt,and increasing the consumption offruit and vegetables
- building physical activity into dailylife – getting people moving as anormal part of their day
- creating incentives for better health– increasing the understanding andvalue that people place on thelong-term impact of decisions
- personalised advice and support –complementing preventive carewith treatment for those whoalready have weight problems.
The strategy includes a focus on howemployers can be encouraged topromote wellness among their staff,and make healthy workplaces part oftheir core business model.
The government’s alcohol strategy61
aims to improve understanding ofwhat acceptable drinking behaviour isand reduce alcohol-related harm. Itexplains the role of police, localcommunities, local authorities, theNHS, voluntary organisations, thealcohol industry and others in helpingto change drinking culture.
The national drug strategy, Drugs:protecting families and communities, isa cross-government programme ofpolicies and interventions thatconcentrate on the most dangerousdrugs, the most damaged communitiesand problematic drug users. The HomeOffice website, Tackling drugs:changing lives,38 gives moreinformation on the government’salcohol and drugs strategies.
The high cost of employee absenceand worklessnessIn 2008, Dame Carol Black, the firstNational Director for Health and Work,published a review of the health ofBritain’s working age population. InWorking for a healthier tomorrow,58
Black notes that around 175 millionworking days were lost due to illness in2006. This cost the nation over £100billion, greater than the annual budgetfor the NHS and equivalent to theentire gross domestic product ofPortugal. Black also notes that around7 per cent of the UK workforce wereon incapacity benefit, with an extra 3per cent off work due to illness at anyone time.58
Nationally, in 2007/08, there were563,000 new cases of workplace illhealth. Of these, 42 per cent(237,000)62 were due to work-relatedstress, depression or anxiety, and178,000 (31.6 per cent)63 to MSDs.This was out of a total of 2.1 millionnew and existing cases. In the sameperiod, 28 million working days werelost due to work-related ill health and6 million to workplace injury,representing 1.4 days per worker.64
23
Appendix A – Some drivers for wellbeing at work

It’s been estimated that, compared tosickness absence, 1.5 times moreworking time is lost through sub-optimal performance at work due tomental ill health. At any one time,nearly one worker in six in the UK isaffected by a clinically diagnosablemental health condition such asdepression or anxiety, or problemsrelating to stress.16
Improving health and work:changing livesDame Carol Black’s review58 outlinesthe important role of the workplace inpromoting health and wellbeing andthe need to change perceptions aboutfitness to work, and to address thehigh level of sickness absence andnumber of people on incapacitybenefit. As part of the review,PricewaterhouseCoopers wascommissioned to consider the widerbusiness case. Their study11 found thatwellbeing programmes can havesignificant positive financial benefitsfor business.
In November 2008, the governmentpublished a positive and potentially far-reaching response65 to Dame CarolBlack’s report, which should herald anew approach to the management ofhealth and wellbeing in the UK. Key initiatives forming part of this newapproach include:
- an electronic ‘fit note’ (capability-based medical certificates) focusingon what people can do rather thanwhat they can’t do
- a national education programmefor GPs to help them advise peopleon how to return or remain in work
- appointing co-ordinators to leadaction on health, work andwellbeing in their local areas,including support for smallbusinesses
- a national centre for working agehealth and wellbeing, which willidentify and monitor trends,evaluate interventions and initiatives,identify evidence gaps andencourage research to close them
- a business healthcheck tool to helpbusinesses estimate the costs of illhealth and identify savings theycould make by introducing healthand wellbeing programmes
- a national strategy for mentalhealth and employment, aiming tobring employment and healthservices closer together and tackleissue such as stigma anddiscrimination
- extending the NHS Plus programmeto include more testing ofinnovative ways of offering cost-effective occupational healthservices to SMEs
- an occupational health helplinepilot for small businesses, providing
access to professional occupationalhealth advice for individualemployees’ health issues, includingmental health
- a challenge fund to encourage localinitiatives in small businesses toimprove health and wellbeingthrough worker engagement
- a review of the health andwellbeing of the NHS workforce, toprioritise whole-systemimprovement and recommendaction for local delivery
- a pilot of early intervention services,including the ‘Fit for work’ servicepilots, which will provide case-managed, multidisciplinary support
- extending the ‘Access to work’programme, providing governmentadvice and support with extra fundsto meet the needs of employeeswhose health or disability affectsthe way they do their jobs
- a pilot programme to help healthand safety practitioners play a moreactive role in managing andpromoting health in theirworkplaces
- creating a council for occupationalhealth to explore methods of jointworking and to develop evidence-based guidelines and standards.
IOSH will be working closely with thegovernment to deliver this joined-upapproach to work and wellbeing.
Appendix A – Some drivers for wellbeing at work
24

25
Appendix B – Key stakeholders and the part they play
Promoting health and wellbeing (helping people to stay fit and healthy)
All employees(includingrepresentatives)
Managers Human resources Occupationalhealth
OSH practitioners Senior managers
Help to plan andprioritise thewellbeing at workstrategy
Consult withemployees andtheirrepresentatives andappropriateprofessionals
Provide appropriate advice and input to the consultation Initiate or lead onstrategydevelopment
Look after ownhealth andwellbeing
Promote, support and act as role model
Participate inactivities toimprove health andwellbeing
Encourageemployees toparticipate inactivities thatimprove theirhealth andwellbeing
Run health promotion activities
Provide information on what can be done, eg usingresources provided by the British Heart Foundation
Provide resourcesor facilities to helpimprove health, egshowers,pedometers
Organise orchampion teamactivities
Encourage orsupport employeesto organiseactivities
Communicate positive wellbeing messages
Co-ordinate communication of health-related activitiesorganised by others
Act as championfor organisation
Suggest ideas
Tell everyone what you’ve done
Co-ordinate communication of success stories and ideas Monitor and review
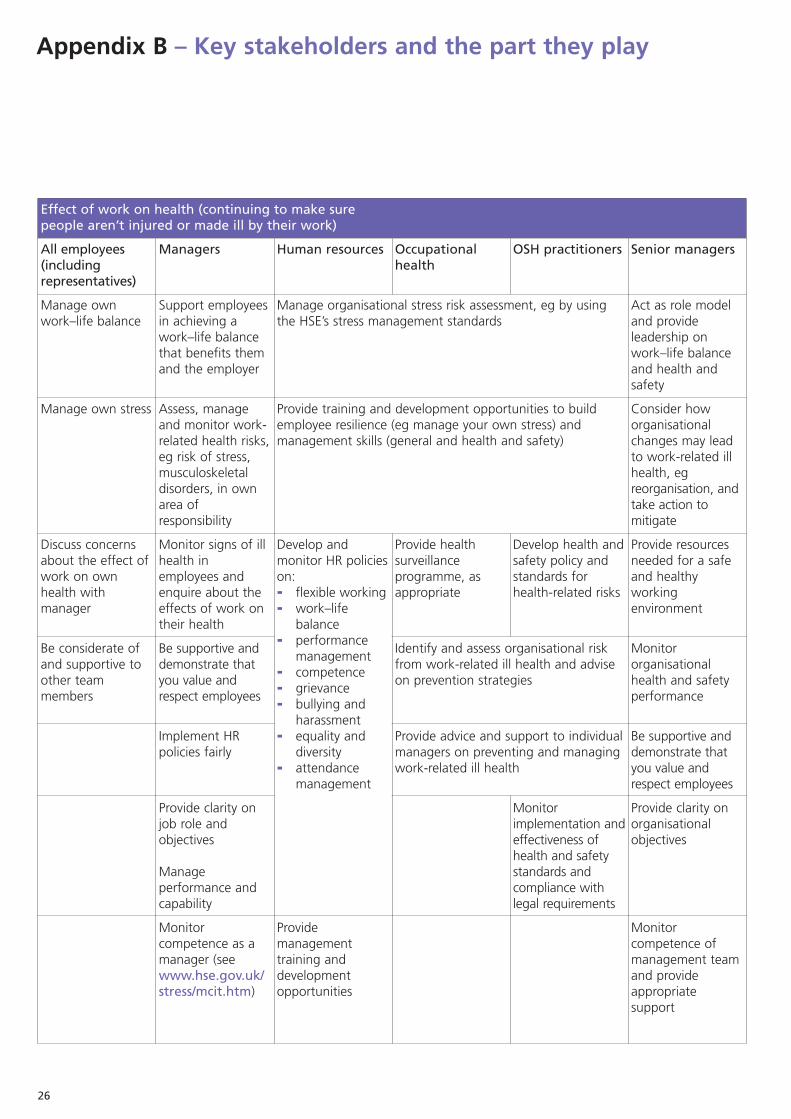
Appendix B – Key stakeholders and the part they play
26
Effect of work on health (continuing to make sure people aren’t injured or made ill by their work)
All employees(includingrepresentatives)
Managers Human resources Occupationalhealth
OSH practitioners Senior managers
Manage ownwork–life balance
Support employeesin achieving awork–life balancethat benefits themand the employer
Manage organisational stress risk assessment, eg by usingthe HSE’s stress management standards
Act as role modeland provideleadership onwork–life balanceand health andsafety
Manage own stress Assess, manageand monitor work-related health risks,eg risk of stress,musculoskeletaldisorders, in ownarea ofresponsibility
Provide training and development opportunities to buildemployee resilience (eg manage your own stress) andmanagement skills (general and health and safety)
Consider howorganisationalchanges may leadto work-related illhealth, egreorganisation, andtake action tomitigate
Discuss concernsabout the effect ofwork on ownhealth withmanager
Monitor signs of illhealth inemployees andenquire about theeffects of work ontheir health
Develop andmonitor HR policieson:- flexible working- work–lifebalance
- performancemanagement
- competence - grievance - bullying andharassment
- equality anddiversity
- attendancemanagement
Provide healthsurveillanceprogramme, asappropriate
Develop health andsafety policy andstandards forhealth-related risks
Provide resourcesneeded for a safeand healthyworkingenvironment
Be considerate ofand supportive toother teammembers
Be supportive anddemonstrate thatyou value andrespect employees
Identify and assess organisational riskfrom work-related ill health and adviseon prevention strategies
Monitororganisationalhealth and safetyperformance
Implement HRpolicies fairly
Provide advice and support to individualmanagers on preventing and managingwork-related ill health
Be supportive anddemonstrate thatyou value andrespect employees
Provide clarity onjob role andobjectives
Manageperformance andcapability
Monitorimplementation andeffectiveness ofhealth and safetystandards andcompliance withlegal requirements
Provide clarity onorganisationalobjectives
Monitorcompetence as amanager (seewww.hse.gov.uk/stress/mcit.htm)
Providemanagementtraining anddevelopmentopportunities
Monitorcompetence ofmanagement teamand provideappropriatesupport
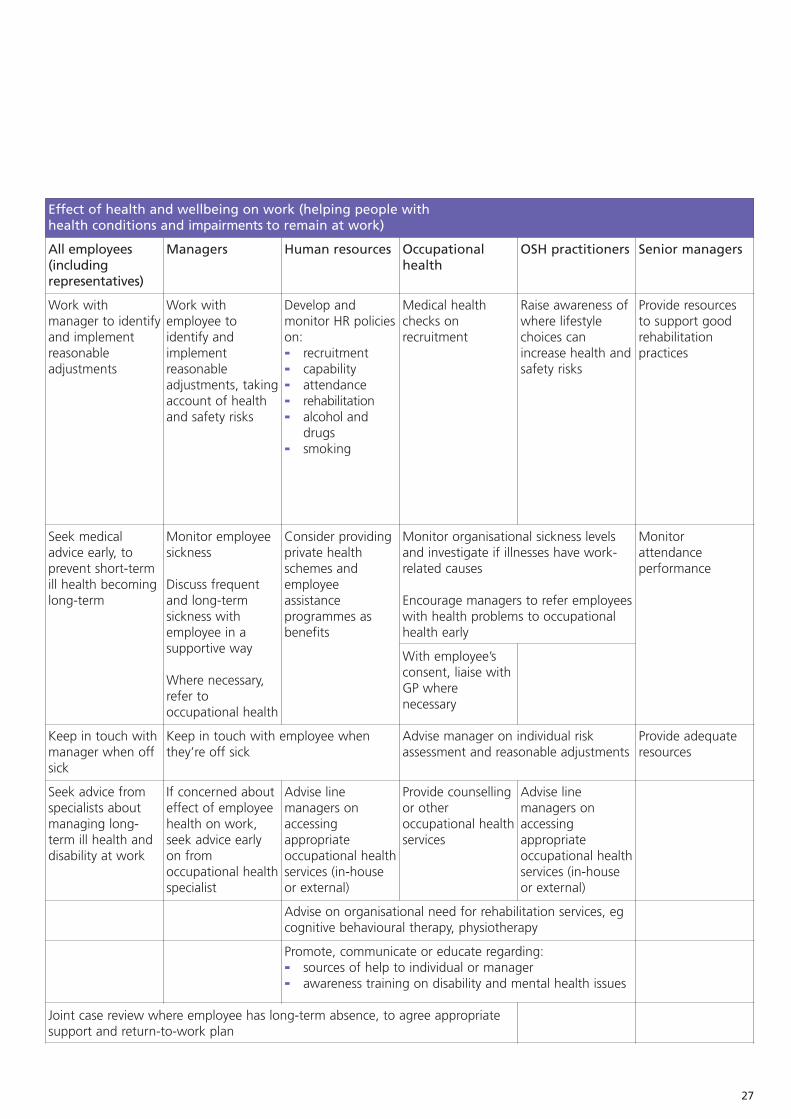
27
Effect of health and wellbeing on work (helping people with health conditions and impairments to remain at work)
All employees(includingrepresentatives)
Managers Human resources Occupationalhealth
OSH practitioners Senior managers
Work withmanager to identifyand implementreasonableadjustments
Work withemployee toidentify andimplementreasonableadjustments, takingaccount of healthand safety risks
Develop andmonitor HR policieson:- recruitment- capability- attendance- rehabilitation- alcohol anddrugs
- smoking
Medical healthchecks onrecruitment
Raise awareness ofwhere lifestylechoices canincrease health andsafety risks
Provide resourcesto support goodrehabilitationpractices
Seek medicaladvice early, toprevent short-termill health becominglong-term
Monitor employeesickness
Discuss frequentand long-termsickness withemployee in asupportive way
Where necessary,refer tooccupational health
Consider providingprivate healthschemes andemployeeassistanceprogrammes asbenefits
Monitor organisational sickness levelsand investigate if illnesses have work-related causes
Encourage managers to refer employeeswith health problems to occupationalhealth early
Monitorattendanceperformance
With employee’sconsent, liaise withGP wherenecessary
Keep in touch withmanager when offsick
Keep in touch with employee whenthey’re off sick
Advise manager on individual riskassessment and reasonable adjustments
Provide adequateresources
Seek advice fromspecialists aboutmanaging long-term ill health anddisability at work
If concerned abouteffect of employeehealth on work,seek advice earlyon fromoccupational healthspecialist
Advise linemanagers onaccessingappropriateoccupational healthservices (in-houseor external)
Provide counsellingor otheroccupational healthservices
Advise linemanagers onaccessingappropriateoccupational healthservices (in-houseor external)
Advise on organisational need for rehabilitation services, egcognitive behavioural therapy, physiotherapy
Promote, communicate or educate regarding:- sources of help to individual or manager- awareness training on disability and mental health issues
Joint case review where employee has long-term absence, to agree appropriatesupport and return-to-work plan
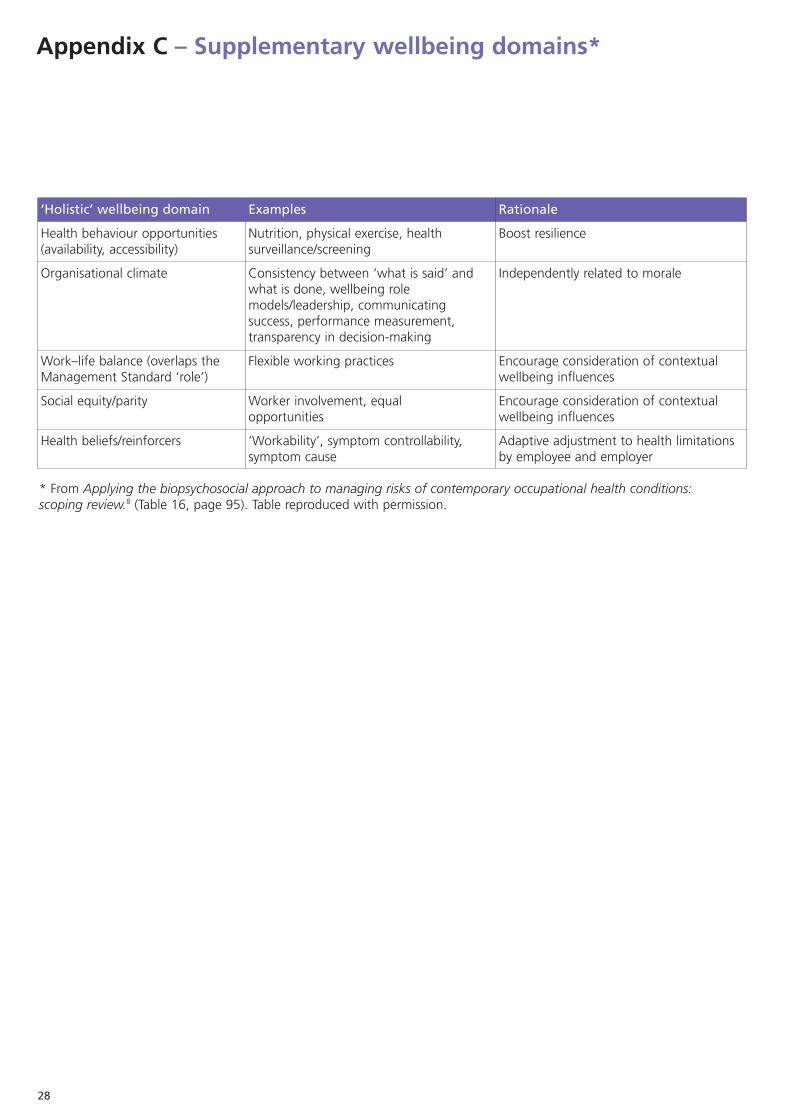
Appendix C – Supplementary wellbeing domains*
28
‘Holistic’ wellbeing domain Examples Rationale
Health behaviour opportunities(availability, accessibility)
Nutrition, physical exercise, healthsurveillance/screening
Boost resilience
Organisational climate Consistency between ‘what is said’ andwhat is done, wellbeing rolemodels/leadership, communicatingsuccess, performance measurement,transparency in decision-making
Independently related to morale
Work–life balance (overlaps theManagement Standard ‘role’)
Flexible working practices Encourage consideration of contextualwellbeing influences
Social equity/parity Worker involvement, equalopportunities
Encourage consideration of contextualwellbeing influences
Health beliefs/reinforcers ‘Workability’, symptom controllability,symptom cause
Adaptive adjustment to health limitationsby employee and employer
* From Applying the biopsychosocial approach to managing risks of contemporary occupational health conditions:scoping review.8 (Table 16, page 95). Table reproduced with permission.

All of the stages below have a vital rolein the delivery of a safe and successfulwellbeing event. As each event isunique, it’s not possible to providecomprehensive information about allelements for each stage, so only someexamples of the types of issue that youshould consider are provided here.
Planning and preparationThis could start with a brainstormingexercise to determine:- required outcomes – to make staffaware of different types of therapy;health and fitness programmes;general health and safety;occupational health provisions andso on
- the scope of the project – forexample, one event on several sitesor one main event at a single site;running the event for staff only orothers too, eg customers, membersof the public and suppliers; thenumber of people expected toattend and the need for specialprovisions, such as access for peoplewith disabilities
- risk assessment – general andhealth and safety risk assessmentsshould be carried out on thecompetence of event suppliers(including checks on their publicliability insurance cover), fire, use ofelectricity, and the venue. Forphysical activities, it may also benecessary to consider the fitness ofpotential participants. Other risksthat may affect the programmeshould also be considered, eg if themain supplier is unable to attend
- resources needed – for example thecost of running the event; publicityfor the event and that generatedfrom the event (internal andexternal); exhibitors and serviceproviders (paid or unpaid); someoneto lead the project (event team andother paid or unpaid helpers); extrasecurity staff, first-aiders or firemarshals, or additional times whenyou need their services; insurancecover; space requirements
- emergency and contingencymeasures – for example what to doif someone is unable to fulfil theirresponsibilities, or if there’s anemergency on the day of the event(either related or unrelated to theevent). You also need to decidewho will make key decisions andthe knock-on effects decisionscould have, eg immediateunscheduled closure of an eventcould lead to congestion, andtherefore have health and safetyimplications
- event document – the informationfrom the planning stage should beused to start developing an eventdocument. The document shouldinclude information aboutoutcomes, scope, resources, anoverview risk assessment for theevent, and emergency contactnumbers and arrangements. Thefinal version of the documentshould include information from allstages of the event
- timeline – set a date for the eventand work backwards to develop aschedule for the project. Make surethat each agreed element of theevent is completed on time. You’llneed to consider the time neededfor the build-up; ordering andconfirming service providers andexhibitors; ordering equipment (egPA systems; goods and leaflets tobe included in event bags); timelags needed to cover for any delays;room bookings; team meetings andallocating responsibilities; ongoingliaison with potential and confirmedexhibitors, making sure that they’resufficiently committed to attending,and then keeping them involved inthe run-up to the event; bookingspecial guests, eg someone to openthe event, business partners. Thetimeline should be included in theevent document and be producedin line with the set agreements.
Build-upThis stage includes safely preparingareas for setting up event stands,equipment, stages and so on. This maymean that some areas need to beclosed off for the duration of the set-up. It may also require extra securitymeasures, eg early in the morning orduring the night. The build-up stagewill need to be covered by theoverview risk assessment and,depending on the activity, may alsorequire specific risk assessments. Thoseinvolved at this stage need to be fullybriefed about associated risks and anyemergency arrangements. There maybe a need for a final briefing onspecific roles and responsibilitiesimmediately before the start of theevent. There should also be a fullydetailed briefing sheet for exhibitors,even if there’s a verbal briefing.
Event deliveryThe publicised event times should beadhered to as far as possible, and ifsafe to do so. Any changes must beagreed and documented by relevantmembers of the event team and clearlycommunicated to the helpers,exhibitors and service providers and, ifnecessary, the visitors. The event teammust monitor progress of the eventagainst schedules set out in the eventdocument and intervene as and whenrequired – particularly if any health andsafety concerns arise.
BreakdownThis stage of the event must also becarefully managed, as exhibitors andservice providers are often eager topack up as soon as the event hasfinished. Depending on the scale of theactivity, it may or may not be safe toallow an early breakdown. The eventteam should decide whether to grantpermission for an earlier breakdown forany part of the event.
29
Appendix D – Delivering a wellbeing event

Wash-up and evaluationThis enables those involved in theorganisation or delivery of the event toreport on what went well and whetherthere were any elements that failed tomeet expectations or provided causefor concern. Feedback should also havebeen gathered from attendees andparticipants about the event. All suchinformation should be recorded andused for developing and improvingfuture events.
Appreciation and acknowledgmentAll exhibitors, staff and volunteersshould be thanked in writing as well asverbally.
General adviceStart off on a small scale, build on yoursuccesses, and learn from things thatdidn’t go as well as you’d expected.This will help to make future eventsmore interesting and relevant for thoseattending and participating.
Figure 2 (opposite) outlines the rangeof activities and services provided by anorganisation for their health, safetyand wellbeing events. They arrangedtwo different scale events to suit theavailability of space on each of theirsites. This enabled all staff, customersand invited members of the localcommunity to attend and participate inat least some of the activities andservices on offer.
Appendix D – Delivering a wellbeing event
30

31
The Atrium
Room 1
TherapiesHead massage HypnotherapyAromatherapyAcupunctureOsteopathyPhysiotherapyPodiatry
Room 2
Training DVDs andexercises
DVDsNAPO (animation)Fire safetyManual handling
Exercise classesHula-hoopingYoga
Room 3
Exhibition Health and Safety ExecutiveIT workstationsOccupational healthand safety unit(OHSU)OY bikes (bike hirescheme)Health checksExercisersErgonomic seating(ES)Welcome stand
Room 1 (30 seat)
Therapies 1Head massage HypnotherapyAromatherapy
Room 2 (30 seat)
Training DVDsNAPO (animation)Fire safetyManual handling
Room 3
Exhibitors’storage area
Room 4 (80 seat)
Therapies 2ReflexologySleep coachAcupuncturePhysiotherapyOsteopathy
A1
Registration
A2
Relaxation
A3
ES
A4
OHSU
A5
IT workstations
A6
OY bikes
A7
Helplines
A8
Exercisers
A9
Health checks
A10
First aid
Room 5 (100 seat)
Exercise activities
Room 6 (100 seat)
Hazard alley
Room 7 (90 seat)
Pre-event briefing09.00–10.00
Small scale event
Large scale event
Figure 2: An example of health, safety and wellbeing events

This isn’t a comprehensive list andinclusion of an organisation, exceptIOSH, doesn’t imply any endorsementby us.
Workplace health risk managementInstitution of Occupational Safetyand Health (IOSH)
Free guidance includes:
- IOSH Occupational HealthToolkit Brings together information,guidance, factsheets, case studies,training materials, presentationsand more to help OSH professionalsand employers tackle occupationalhealth problems. It covers stress,MSDs, skin disorders and inhalationdisorders. www.ohtoolkit.co.uk
- A healthy return: good practiceguide to rehabilitating people atworkThis introductory text for OSHprofessionals and others gives anoverview of rehabilitation; workadjustment assessment; casestudies; and sources of informationand training.www.iosh.co.uk/files/technical/A%20HEALTHY%20RETURN121208%2Epdf
- Out of ‘site’, out of mind?Managing office teleworking in the21st centuryThis publication includes guidanceon health-related issues affectingteleworkers, such as stress andmusculoskeletal disorders.www.iosh.co.uk/index.cfm?go=technical.details&scid=12
IOSH also provides other free guides,covering topics such as health andsafety management systems, positiveculture and behavioural safety atwww.iosh.co.uk/techguide
Health and Safety Executive (HSE)Guidance on prevention of work-related health riskswww.hse.gov.uk
Securing health togetherWeb resource that includes summariesof good occupational health practicesand case study material.www.hse.gov.uk/sh2
Occupational Health AdvisoryCommittee report and recommendationson improving access to occupationalhealth support.www.hse.gov.uk/aboutus/meetings/iacs/ohac/access.htm
The following HSE publications includeadvice on occupational health issues(HSE Books, Sudbury, Suffolk, t +44 (0)1787 313995,www.hsebooks.co.uk):
- Essentials of health and safety atwork
- Successful health and safetymanagement, HSG65 Covers occupational health as wellas safety issues
- Health risk management: a practicalguide for managers in small andmedium-sized enterprises, HSG137
The HSE publishes guidance on a rangeof workplace health-related issues.These can be accessed via the healthand safety topics link on its homepage.Examples include:
- Alcohol and drugswww.hse.gov.uk/alcoholdrugs
- Asthma www.hse.gov.uk/asthma
- Construction health riskswww.hse.gov.uk/construction/healthrisks
- Hand–arm and whole bodyvibrationwww.hse.gov.uk/vibration
- Hazardous substanceswww.hse.gov.uk/coshh
- Musculoskeletal conditionswww.hse.gov.uk/msd/index.htm
- New and expectant motherswww.hse.gov.uk/mothers
- Noise at workwww.hse.gov.uk/noise
- Sickness absence and return toworkwww.hse.gov.uk/sicknessabsence
- Skin www.hse.gov.uk/skin
- Stresswww.hse.gov.uk/stress
- Work-related diseases (skin,respiratory and cancer) www.hse.gov.uk/drp
- Young people at workwww.hse.gov.uk/youngpeople
Other organisationsAssociation of Occupational HealthNurse Practitioners (UK)www.aohnp.co.uk
British Occupational HygieneSocietywww.bohs.org
Equality and Human RightsCommissionwww.equalityhumanrights.com/en/Pages/default.aspx
Ergonomics Societywww.ergonomics.org.uk
European Agency for Safety andHealth at Work osha.europa.eu
Appendix E – Resources
32

Faculty of Occupational Medicinewww.facoccmed.ac.uk
Health Protection AgencyOffers advice on public health,including infectious diseases,chemicals, poisons and radiation.www.hpa.org.uk
Institute of Acousticswww.ioa.org.uk
Institute of Occupational Healthwww.bham.ac.uk/IOH
Society of Occupational HealthNursing www.rcn.org.uk/development/communities/specialisms/occupational_health
Society of Occupational Medicinewww.som.org.uk
Further readingCox R A F, Edwards F C and Palmer K(eds). Fitness for work: the medicalaspects. 3rd edition. New York: OxfordUniversity Press, 2000.
Dorward A L. Managers’ perceptions ofthe role and continuing educationneeds of occupational health nurses.HSE Research Paper No. 34. London:HMSO, 1993.
Fingret A and Smith A. Occupationalhealth: a practical guide for managers.London: Routledge, 1995.
Mearns K J and Fenn C E. Diet, healthand the offshore worker – a pilotstudy. Sudbury: HSE Books, 1993.www.hse.gov.uk/research/othpdf/200-399/oth399.pdf
National Social Marketing Centre.Business success and employeewellbeing – The case for a new cross-government approach. London: NSMC,2008. www.nsms.org.uk/images/CoreFiles/NSMC_HealthSafe_Report.pdf
Promoting health and wellbeingBe happy be healthyProvides support, help, advice andinformation designed to make lifehappier and healthier.www.behappybehealthy.co.uk
British Heart FoundationUses public information campaigns,advertising and the media to informpeople about how to improve thehealth of their heart. Their ‘Health atwork’ webpages cover eating well,getting active, and wellbeing at work,providing online resources and ideas forhealth promotion and a range of ‘Thinkfit’ packs.www.bhf.org.uk/healthatwork
Health ScotlandWorks to improve health and reducehealth inequalities in Scotland. www.healthscotland.com
Health, Work and WellbeingGovernment-led initiative to improvethe health and wellbeing of workingage people. Includes case studies andresources.www.workingforhealth.gov.uk
National Institute for Health andClinical Excellence (NICE) NICE produces evidence-basedguidance on public health interventionsand programmes. - Workplace health promotion: how
to encourage employees to bephysically activewww.nice.org.uk/PH013
- Promoting mental wellbeing atwork (due to be published late in2009)guidance.nice.org.uk/PHG/Wave12/82
- Management of long-term sicknessand incapacity for work guidanceguidance.nice.org.uk/PH19
Scottish Centre for Healthy WorkingLives Runs a free national award programmefor promoting health in the workplace.www.healthyworkinglives.com/home/index.aspx
Take life on, one step at a timeInformation, resources and support onhealthy eating and physical activity, andhow small changes can lead to bigbenefits. It’s a joint collaborationbetween the Scottish Executive andNHS Health Scotland.www.takelifeon.co.uk
Further readingCreating a healthy workplace: a guidefor occupational safety and healthprofessionals and employers TheOccupational Health Working Group ofthe Faculty of Public Health and theFaculty of Occupational Medicine.London: FPH and FOM, 2006.
Aimed at OSH professionals andemployers, the guide and supportingleaflet:- outline why healthy workplacesmake good sense
- set out legal requirements- list resources and sources ofpractical help.
Guidewww.fph.org.uk/resources/AtoZ/r%20_healthy_workplaces.pdf
Leafletwww.fph.org.uk/resources/AtoZ/l_healthy_workplaces.pdf
How to manage health & wellbeing. Employee Benefits magazine, 2007.www.employeebenefits.co.uk/download/749/How-to-manage-healthcare.pdf
33
Mental healthAssociation for Counselling at WorkThe specialist workplace division of theBritish Association for Counselling andPsychotherapy (BACP). It aims topromote best practice in counselling atwork and other employee supportinterventions, including coaching,mediation, stress auditing, stressmanagement, trauma management andinformation services.www.counsellingatwork.org.uk
Association for Counselling at Work.Guidelines for counselling in theworkplace. ACW, 2007.www.counsellingatwork.org.uk/acw_guidelines_web.pdf
EEF Work organisation assessment tool www.workorganisation.org.uk
Mindful employerEmployer-led initiative aimed atincreasing awareness of mental healthat work and providing support forbusinesses in recruiting and retainingstaff. www.mindfulemployer.net
Royal College of PsychiatristsProfessional and educational body forpsychiatrists in the UK and Republic ofIreland. Their site includes advice onmental ill health, alcohol and drugs.www.rcpsych.ac.uk/mentalhealthinformation.aspx
Sainsbury Centre for Mental HealthPromotes new ways of helping peoplewith mental health problems get andkeep work. www.scmh.org.uk
See meA Scottish government-funded allianceof five mental health organisations thataims to tackle the stigma anddiscrimination associated with mentalill health.www.seemescotland.org.uk
Shaw Trust‘Tackling the last workplace taboo’ is aweb resource to help manage mentalill health at work.www.tacklementalhealth.org.uk
ShiftPart of the National Mental HealthDevelopment Unit, a government-funded organisation advising on bestpractice improvements.www.shift.org.uk
Further readingLayard R. Happiness. Lessons from anew science. London: Penguin Books,2006.
Musculoskeletal healthBackCareAn independent national charity thathelps people manage and prevent backpain. www.backcare.org.uk
Further readingAching arms or RSI in small businesseswww.hse.gov.uk/pubns/indg171.pdf
Early management of persistent non-specific low back painguidance.nice.org.uk/CG88
Upper limb disorders in the workplacewww.hse.gov.uk/msd/campaigns/uldchecklist.pdf
Work-related neck and upper limbdisordersosha.europa.eu/en/publications/factsheets/72
Physical activityAbout.comAbout.com is network of around 750freelance authors, who providepractical solutions to everydayproblems across thousands of topics.The following sites are relevant:www.about.com/health andwww.walking.about.com
Disability Sport EventsCreates opportunities for participationin sport for people with disabilities.www.disabilitysport.org.uk
Sport EnglandAdvises, invests in and promotescommunity sport to create an activenation and encourages people to getinvolved in sport and physical activity.www.sportengland.org
SustransThe UK’s leading sustainable transportcharity. Its vision is a world in whichpeople can choose to travel in waysthat benefit their health and theenvironment. The site providespractical, innovative ways of dealingwith the transport challenges. www.sustrans.org.uk
Walking the way to healthThe largest national body promotingand setting the standards for led healthwalks. It’s a joint initiative betweenNatural England and the British HeartFoundation, supporting health walkschemes. www.whi.org.uk
Walking-RoutesLinks to UK webpages which detailthousands of walking routes, hikingtrails, route directions, route maps andso on.www.walking-routes.co.uk
Walkit.comCalculates walking routes in majorcities in the UK, so that employeesworking in or visiting them can walk totheir destination rather than drive oruse public transport. www.walkit.com
Further readingScottish Executive. Let’s make Scotlandmore active: a strategy for physicalactivity. Edinburgh: Scottish Executive,2003. www.scotland.gov.uk/Resource/Doc/47032/0017726.pdf
Appendix E – Resources
34

Healthy eatingBritish Dietetic Association‘Food facts’ series of downloadablefactsheets on food issues.www.bda.uk.com/foodfacts/index.html
British Nutrition FoundationA registered charity seeking to promotewellbeing through science-basedknowledge and advice on diet, physicalactivity and health. It also provideshealthy eating information andresources for schools.www.nutrition.org.uk
EatwellFood Standards Agency advice onhealthy eating.www.eatwell.gov.uk/healthydiet/
Food Standards AgencyAn independent governmentdepartment set up to protect thepublic’s health and consumer interestsin relation to food. www.food.gov.uk
Weight ConcernA registered charity dedicated tofighting the UK’s obesity epidemic.Includes advice on losing weight,healthy eating and exercise.www.weightconcern.org.uk
World Health OrganizationDiet and physical activity: a publichealth prioritywww.who.int/dietphysicalactivity/en/index.html
SmokingIOSHA breath of fresh air – Managing asmoke-free workplaceIOSH guidance on smoke-free policies.www.iosh.co.uk/files/technical/A%20BREATH%20OF%20FRESH%20AIR%201%2Epdf
HSEAdvice on smoking at work.www.hse.gov.uk/contact/faqs/smoking.htm
Action on Smoking and HealthA campaigning public health charitythat works to eliminate the harmcaused by tobacco. www.ash.org.uk andwww.ashscotland.org.uk
Clearing the Air ScotlandAdvice on Scotland’s smoke-freelegislation. www.clearingtheairscotland.com/index.html
NICEInformation for employers – what youcan do to encourage your employeesto stop smokingwww.nice.org.uk/nicemedia/pdf/PHI005leaflet.pdf
Smoke Free EnglandInformation about smoke-freelegislation in England and links tosupport on quitting smoking.www.smokefreeengland.co.uk
Smoking Ban WalesAdvice on smoke-free legislation inWales. www.smokingbanwales.co.uk
Space to BreatheAdvice on smoke-free legislation inNorthern Ireland.www.spacetobreathe.org.uk
Alcohol and drugsHSEOnline information and downloadableleaflets providing advice and guidanceon alcohol and drugs at work.www.hse.gov.uk/alcoholdrugs
AdfamProvides support to people workingwith family members who are affectedby alcohol and drugs.www.adfam.org.uk
Alcohol ConcernProvides information, fact sheets andarticles on a range of topicssurrounding alcoholism.www.alcoholconcern.org.uk
Alcohol Focus ScotlandA volunteer organisation for alcoholissues in Scotland. Provides informationabout alcohol, including legal matters,frequently asked questions, and tips forsafe drinking. www.alcohol-focus-scotland.org.uk
Alcoholics AnonymousAn informal society of recoveredalcoholics that provides support forthose who want to stop drinking.www.alcoholics-anonymous.org.uk
Down your drinkA web tool designed to help peoplework out whether they’re drinking toomuch and, if so, what to do about it. www.downyourdrink.org.uk
DrugScopeAims to advise on policy developmentand reduce drug-related risk. www.drugscope.org.uk
FRANKA national helpline set up by the HomeOffice that offers free confidential helpand information about drugs 24 hoursa day. t +44 (0)800 77 66 00.www.talktofrank.com
35
Institute of Alcohol Studies A charity aimed at improving educationabout alcohol in the UK. Includes factsheets dealing with all aspects ofalcohol in society, complete with factsand figures. www.ias.org.uk
ReleaseA confidential helpline offering help ondrug use and legal issues. t +44 (0)845 450 0215www.release.org.uk
Re-SolvA national charity dedicated topreventing solvent and volatilesubstance abuse. www.re-solv.org
Royal College of PsychiatristsThe main professional body forpsychiatrists in the UK. Provides arange of information on alcohol anddrugs, including some documents invarious languages, and pricedpublications for the public andprofessionals. www.rcpsych.ac.uk/mentalhealthinformation.aspx
Tackling drugs: changing livesPart of the government’s drug strategy,these national workplace initiativewebpages offer guidance foremployers and includes access toexperienced business trainers.drugs.homeoffice.gov.uk/drug-strategy/drugs-in-workplace/national-workplace-initiative
United Kingdom AccreditationService (UKAS)The only government-recognisedaccreditation body for assessing thestandard of drug-testing laboratories inthe UK. www.ukas.com
Further readingFaculty of Occupational Medicine.Guidance on alcohol and drug misusein the workplace. London: Faculty ofOccupational Medicine, 2006.www.facoccmed.ac.uk/pubspol/pubs.jsp
Institute of Alcohol Studies. Alcoholand the workplace. St Ives: IAS, 2008.www.ias.org.uk/resources/factsheets/workplace.pdf
Men’s healthMen’s health is generally poorer thanwomen’s, and men are generally lesslikely to use GP services. The workplaceis therefore a good arena to reachthem with health messages. Thefollowing websites provide usefulinformation and resources on men’shealth issues:www.malehealth.co.ukwww.menshealthforum.org.uk
Women’s healthRace for LifeThe biggest women-only fundraisingevent in the UK. Women can walk, jogor run 5km to raise money for CancerResearch UK. The event not onlysupports a good cause, but encourageswomen to get engaged in physicalactivity. www.raceforlife.org
Women’s Health ConcernProvides an independent service toadvise, reassure and educate womenabout their health concerns. The siteincludes factsheets on a range ofwomen’s health issues.www.womens-health-concern.org
Appendix E – Resources
36

Our thanks to Claire Saunders forproducing this guide, and to everyonewho contributed to it, particularlyProfessor Kevin Holland-Elliot andDel Basi.
We welcome all comments aimed atimproving the quality of our guidance,including details of non-UK referencesand good practices. Please send yourfeedback to the Policy and TechnicalDirector, at [email protected].
Acknowledgments

WE/RJ/030909/P
This document is printed on chlorine-free paper produced from managed, sustained forests.
IOSHThe GrangeHighfield DriveWigstonLeicestershireLE18 1NNUK
t +44 (0)116 257 3100f +44 (0)116 257 3101www.iosh.co.uk
IOSH is the Chartered body for health and safetyprofessionals. With more than 35,000 membersin 85 countries, we’re the world’s biggestprofessional health and safety organisation.
We set standards, and support, develop andconnect our members with resources, guidance,events and training. We’re the voice of theprofession, and campaign on issues that affectmillions of working people.
IOSH was founded in 1945 and is a registeredcharity with international NGO status.
Institution of Occupational Safety and HealthFounded 1945Incorporated by Royal Charter 2003Registered charity 1096790


















