Working to Improve the Performance of Emergency and Acute Care by Keith Kocher
17
Keith Kocher working to improve the performance of emergency and acute care
-
Upload
university-of-michigan-department-of-emergency-medicine -
Category
Health & Medicine
-
view
139 -
download
0
Transcript of Working to Improve the Performance of Emergency and Acute Care by Keith Kocher

Keith Kocherworking to improve the performance of
emergency and acute care

Why?
Health
Advancing
Promoting
Supporting
Cultivating
(not health care)

How?
Health care
Culture
Science
Economics
Politics

How?performance varies

How?
𝑉𝑎𝑙𝑢𝑒=𝑄𝑢𝑎𝑙𝑖𝑡𝑦𝐶𝑜𝑠𝑡
TimelinessFunctional status MortalityRelief of suffering Communication
Provider work Ancillary staff work
Tests TreatmentsFacility

𝑉𝑎𝑙𝑢𝑒=𝑄𝑢𝑎𝑙𝑖𝑡𝑦𝐶𝑜𝑠𝑡
How?
What value did the patient
derive from the ED visit?
What value did the system (society)
derive from the ED visit?

How?
* Doesn’t mean
we can’tdo better
performance varies*

What?2 major research projects:
• Michigan Emergency Department Improvement Collaborative (MEDIC)
• Funded by Blue Cross Blue Shield of Michigan and Blue Care Network
• Started January 2015• www.medicqi.org
• Career Development Award (K08)• Funded by the Agency for Healthcare Research
and Quality (AHRQ)• Started August 2015

UM BEA
CWM HF CHM
HFHH
MM
MidMichigan Medical CenterMidlandJeff Allen, MD
MNM
McLaren Northern MichiganPetoskeyBrian Gelb, MD
Holland HospitalHollandBrian Holt, DO
University of Michigan HospitalAnn ArborBenjamin Bassin, MDDavid Somand, MD
UM
CW Mott Children’s HospitalAnn ArborNicole Sroufe, MD
CWM
Beaumont HospitalRoyal OakBlaine Dennis, MD
BEA
Children’s Hospital of MichiganDetroitPrashant Mahajan, MD, MPH, MBA
CHM
Henry Ford HospitalDetroitSeth Krupp, MDMichelle Slezak, MD
HF
Detroit Receiving HospitalDetroitBrian O’Neil, MD
DR
M EDI CMICHIGAN EMERGENCY DEPARTMENT
IMPROVEMENT COLLABORATIVE
&PARTICIPATING SITESCLINICAL CHAMPIONS
Adult Pediatric Both

MEDIC Coordinating Center Team
Keith KocherDirector
Executive Committee Chair
Michele NypaverCo-DirectorPediatric
Committee Chair
Brad UrenSite Relations Lead
Jim PribbleQuality Initiatives LeadData and Publications
Committee Chair
Jason HamAdult QI Consultant
Michelle MacyPediatric QI Consultant
Greg LevineProgram Manager
Sarah BellData Analyst
April ProudlockData Auditor
Andrew Livingston
Administrative Assistant
ArborMetrixData Registry
Vendor

MEDIC Vision & Values Advance Emergency Care
Work together to advance the delivery of emergency care
Learn & Collaborate Provide tools to help providers help each other get better
Improve Patient Outcomes Evaluate current patterns of care, guide quality
improvement efforts
Drive Performance Deliver accurate, statistically rigorous performance
feedback

MEDIC Quality Initiatives
1) CT use for minor head injuries in adults and children
2) CT use to evaluate for pulmonary embolism in adults
3) Chest x-rays use for the evaluation of bronchiolitis, croup, and asthma in children
4) Developing outpatient alternative pathways to hospitalization from the ED in adults and children

What?
1) To determine patient clinical and hospital factors associated with variability in ED hospitalizations
“Understanding the Causes and Consequences of Variation in Emergency Department Hospitalization
Practices Across the United States”
2) To determine how patient non-clinical factors influence variability in ED hospitalizations
3) To evaluate the effect of ED hospitalization patterns on outcomes and costs
Career Development Award:

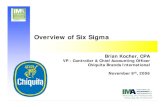
Sepsis [2]
Acute myocardial infarction [100]
Acute renal failure [157]
Stroke [109]
Congestive heart failure [108]
Pneumonia [122]
Diabetes with complications [50]
Cardiac dysrhythmias [106]
Biliary tract disease [149]
Fluid and electrolyte disorders [55]
Urinary tract infection [159]
Chronic obstructive pulmonary disease [127]
Asthma [128]
Soft tissue infections [197]
Chest pain [102]
0 10 20 30 40 50 60 70 80 90 100
Admission Rate, %
Observed Variation for the Top 15 Most Commonly Admitted Medical and Surgical Conditions
Notes: Unadjusted admission rates presented. Conditions shown with their associated clinical classification software (CCS) code. Boxes correspond to interquartile range, with median marked. Whiskers denote 10th and 90th percentiles.
from: Sabbatini AK, Nallamothu BK, Kocher KE. Reducing variation in
hospital admissions from the emergency department for low-
mortality conditions may produce savings. Health Affairs, 2014;
33(9):1655-1663.

Questions?

MEDIC: Infrastructure
Participating EDs
MEDIC Coordinating
CenterBCBSM & BCN
• Offer neutral ground for collaboration• Program funding and incentive payment design• Clinical and administrative support to
Coordinating Centers
CQI
• Clinical Leadership – develop and executes the QI agenda• Project Management• Data transfer and collection• Explore links between process and outcomes• Analytic and QI support
Data Analysis
Data Reporting
Develop Best
Practices
Data collection
Continuous Quality
Improvement
Collaborative
• Contribute to All-Payer registry
• Share and learn best practices
• Implement quality Improvement opportunities
Arbor Metrix
• Centralized database• Support chart
abstraction process• Performance reporting

Sabbatini AK, Nallamothu BK, Kocher KE. Reducing variation in hospital admissions from the emergency department for low-mortality conditions may produce savings. Health Affairs, 2014; 33(9):1655-1663.