
Workforce and Organisational Development Plan
104
1 Hywel Dda University Health Board 3 Year Integrated Medium Term Plan 2016/17 – 2018/19 Enabling and Supporting Plan Annex 8 Workforce, Education and Organisational Development Strategy & Plan 31st March 2016
Transcript of Workforce and Organisational Development Plan

1
Hywel Dda University Health Board 3 Year Integrated Medium Term Plan 2016/17 – 2018/19 Enabling and Supporting Plan Annex 8 Workforce, Education and Organisational Development Strategy & Plan 31st March 2016

2
INTRODUCTION The aim of this annex is to provide the additional information regarding our workforce, give details of the actions which will be taken during 2016/17, 2017/18 and beyond to ensure we have a flexible, skilled and motivated workforce ready to support the effective delivery of quality services to our community. The actions we intend to take cover 3 areas: our workforce, our communities and our future. We outline the key drivers and expected changes in each section then provide detail of the actions we will take to address these issues. The full workforce and OD plan is then brought together at the end of the document.
Our workforce is key to the delivery of the IMTP. This section presents a detailed description of:-
current information on our workforce, including reference to key national strategies and drivers
progress in delivering the planned work described previously
current and anticipated challenges over the next 12-36 months and further where appropriate
next steps to develop the workforce.
The Workforce and Organisational Development team work with operational services and colleagues in planning & finance to enable proactive and integrated working. This enables the team to engage with the planning of new services and modernisation of workforce models to ensure that workforce planning is fully integrated and embedded at all levels. The principles of Prudent Healthcare underpin all plans, as does the investment in the development of our staff to maximise their full potential to deliver the prioritised service outcomes. The Health Board will achieve this via number of workforce initiatives and techniques which are detailed within this annex. OUR WORKFORCE Overview Hywel Dda has 9,871 (7433.09 wte) directly employed staff which equates to 43% of our budget. This excludes our Primary Care contractor workforce and social care staff across our three Local Authorities. The breakdown of the University Health Board by staff group as at 31st December 2015 and our turnover (based on the average turnover over the last 3 years), is reflected in the table below: Workforce Analysis (based on ESR data drawn at end Dec 2015 and vacancy position 11 Dec)

3
Staff Group
WTE Headcount % average turnover
over last 3 yrs
Add Prof Scientific And Technical 248.36 299 8.91%
Additional Clinical Services 1450.12 2168 7.51%
Administrative And Clerical 1307.12 1564 10.22%
Allied Health Professionals 481.67 581 8.91%
Estates And Ancillary 795.53 1281 7.71%
Healthcare Scientists 151.33 169 6.86%
Nursing And Midwifery Registered 2535.06 3209 6.54%
Medical & Dental (Excl. Drs In Training) 455.90 600 15.16%
Total 7433.09 9871
2015 has seen turnover begin to reduce having steadily increased since 2013. This is being closely monitored but is seen as a very good indicator that the Health Board is beginning to make a difference with our workforce despite the pension changes which gave rise to concern that retirements would mean our turnover would continue to rise. The figures in the graphs below present information from ESR (Electronic Staff Record) which is the electronic data base of our staff in post and inform workforce, finance and payroll systems.
Whilst ESR can provide the HB with information on our current workforce which can assist in our assessment of risks based upon age profile, gender and turnover, it does not reflect our vacancies by profession. In order to provide a workforce analysis we therefore also review vacancies across the HB currently and posts which have proved difficult to fill. This information is analysed and triangulated to identify where the risks sit within professions, services and sites. Currently the vacancy information available is based upon those known within the recruitment service information, however we recognise that there is a gap in that there will be vacancies within services being reviewed prior to recruitment and to understand the whole picture the Workforce & OD team are currently working to establish a mechanism for capturing
Turnover
0.00%
1.00%
2.00%
3.00%
4.00%
5.00%
6.00%
7.00%
8.00%
9.00%
1 2 3 4 5 6 7 8 9 10 11 12
2015
2014
2013

4
this information. The analysis is based upon the recruitment information available.
This is then mapped as a timeline to see where and when the recruitment pressure points sit to inform focussed recruitment plans and in tandem with clinical service plans the educational commissioning numbers required are submitted over the next 5 years to mitigate the risk and ensure that the HB has the right staff with the right skills to deliver the service. Our workforce is predominantly female (78%). The total workforce in post including bank and locum staff is 9871 individuals and of them 50.54% staff are full time and 49.46% p/t., this changes when bank and locum staff are excluded, it then changes to 57.91% full time and 42.09% part time.
Health Board Gender and P/T and F/T Profile (excluding bank and locum)
The age profile of the workforce is presented by professional group in this section of the annex. This information supports our assessment of risk associated with turnover related to potential retirements. The risks associated with our age profile are likely to be mitigated to an extent over the next 3 years by the changes to the pension scheme, as whilst staff may have the option to retire at 55 due to their profession, it may not be a viable option for them financially unless they have made specific provision. The HB presently has 30% of staff who retire who return to work. 34% of our total workforce are between the ages of 46 & 55. There are very few employees below the age of 20 as would be expected in a predominantly regulated workforce.
Health Board Age Profile (all staff groups)
It is key to review the age profile by the specific staff groups as the profile and the associated risk changes considerably.

5
The IMTP defines the planned service provision for our healthcare community. Our workforce is key to the delivery of our services and every one of the wide ranging staff groups have a role to play in delivery. Each face some common challenges but all equally have specific issues which can impact upon their ability to deliver their service effectively. In each section this is described with the actions which are planned over the next 2 years based upon analysis of current information, projections and predictions. Registered Nursing and Midwifery and Healthcare Support Workers (HCSW) The HB currently employs 2535.06 wte (3209 headcount) registered nurses and 1,107.81 wte (1,760 headcount) HCSW across our acute and community hospitals and in community services. The average retirement age based upon the last 3 years leavers is 59 for registered nursing and midwifery. Currently there are 159.25 wte registered nurses who are 59 yrs old or over and 720.27 who are currently over 50. The age profile for HCSW reflects that 219.7 wte are currently over 56 yrs old however they are easier to recruit, and the HB has a very well defined development programme, Skills to Care, linked with Corporate Induction to ensure all our support workers have the skills required to deliver the role under supervision from day 1 on the ward. This programme is exemplar and has underpinned the principles set within the new All Wales HCSW Framework baseline development which in future requires that all support staff will have access to a qualification within NHS Wales within the next 5 years. Registered Nursing HCSW
This age profile presents the background information to inform predicted turnover rates, which is analysed in the context of current baseline vacancies. There are currently 190.21 wte registered and 28.19 wte HCSW vacancies across the HB (known vacancies, in process and onboarding). In 2013 we had 129.46 wte leavers, 175.96 wte in 2014 (reflecting an increase of 46.5 wte leavers) and 201.52
6
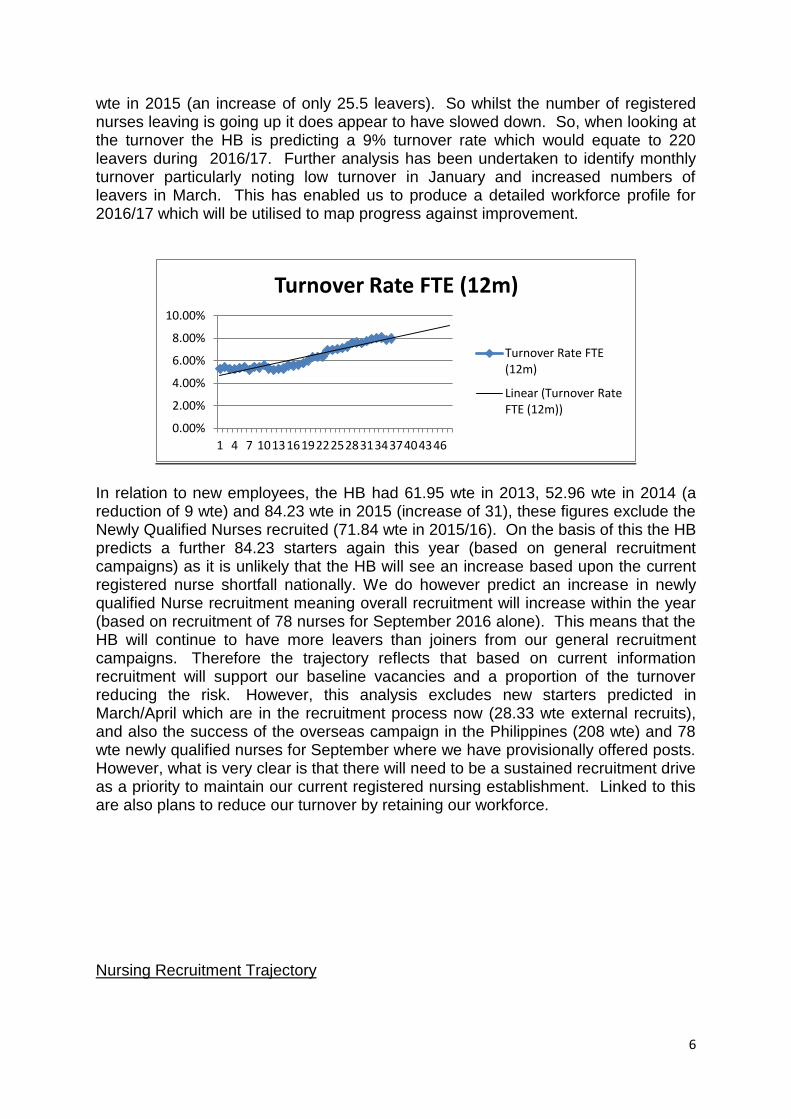
wte in 2015 (an increase of only 25.5 leavers). So whilst the number of registered nurses leaving is going up it does appear to have slowed down. So, when looking at the turnover the HB is predicting a 9% turnover rate which would equate to 220 leavers during 2016/17. Further analysis has been undertaken to identify monthly turnover particularly noting low turnover in January and increased numbers of leavers in March. This has enabled us to produce a detailed workforce profile for 2016/17 which will be utilised to map progress against improvement.
In relation to new employees, the HB had 61.95 wte in 2013, 52.96 wte in 2014 (a reduction of 9 wte) and 84.23 wte in 2015 (increase of 31), these figures exclude the Newly Qualified Nurses recruited (71.84 wte in 2015/16). On the basis of this the HB predicts a further 84.23 starters again this year (based on general recruitment campaigns) as it is unlikely that the HB will see an increase based upon the current registered nurse shortfall nationally. We do however predict an increase in newly qualified Nurse recruitment meaning overall recruitment will increase within the year (based on recruitment of 78 nurses for September 2016 alone). This means that the HB will continue to have more leavers than joiners from our general recruitment campaigns. Therefore the trajectory reflects that based on current information recruitment will support our baseline vacancies and a proportion of the turnover reducing the risk. However, this analysis excludes new starters predicted in March/April which are in the recruitment process now (28.33 wte external recruits), and also the success of the overseas campaign in the Philippines (208 wte) and 78 wte newly qualified nurses for September where we have provisionally offered posts. However, what is very clear is that there will need to be a sustained recruitment drive as a priority to maintain our current registered nursing establishment. Linked to this are also plans to reduce our turnover by retaining our workforce. Nursing Recruitment Trajectory
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
1 4 7 10 13 16 19 22 25 28 31 34 37 40 43 46
Turnover Rate FTE (12m)
Turnover Rate FTE (12m)
Linear (Turnover Rate FTE (12m))
7
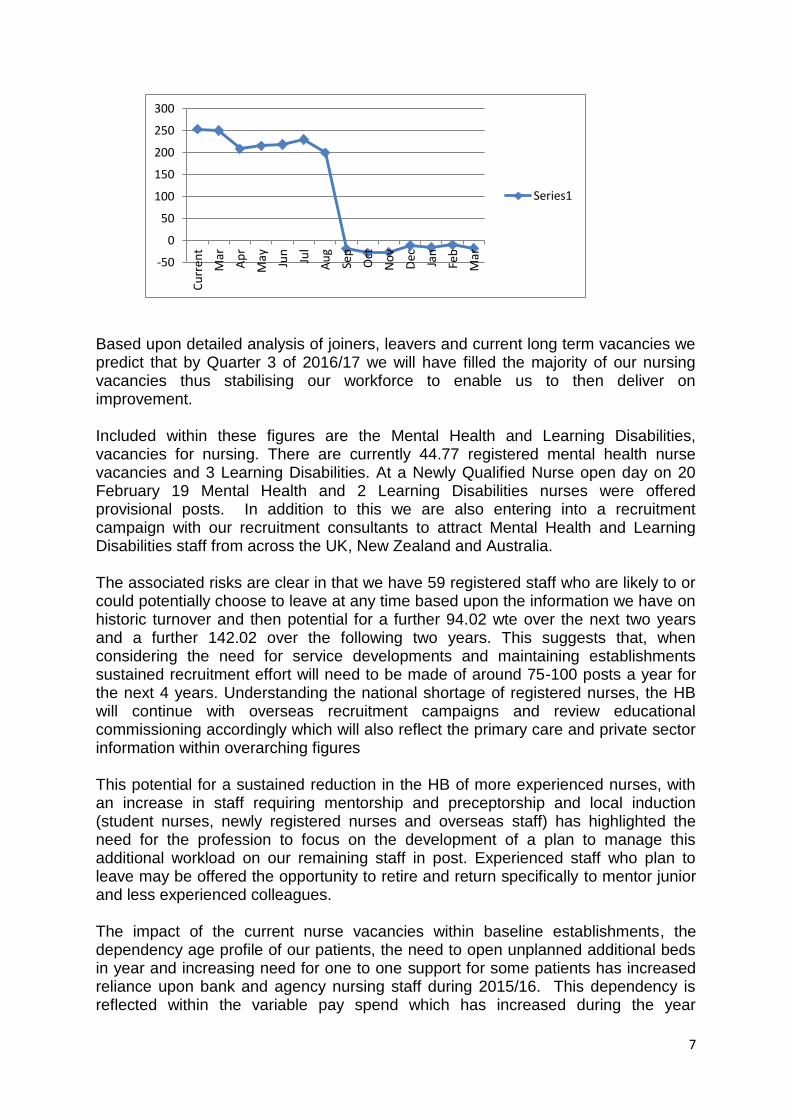
Based upon detailed analysis of joiners, leavers and current long term vacancies we predict that by Quarter 3 of 2016/17 we will have filled the majority of our nursing vacancies thus stabilising our workforce to enable us to then deliver on improvement. Included within these figures are the Mental Health and Learning Disabilities, vacancies for nursing. There are currently 44.77 registered mental health nurse vacancies and 3 Learning Disabilities. At a Newly Qualified Nurse open day on 20 February 19 Mental Health and 2 Learning Disabilities nurses were offered provisional posts. In addition to this we are also entering into a recruitment campaign with our recruitment consultants to attract Mental Health and Learning Disabilities staff from across the UK, New Zealand and Australia. The associated risks are clear in that we have 59 registered staff who are likely to or could potentially choose to leave at any time based upon the information we have on historic turnover and then potential for a further 94.02 wte over the next two years and a further 142.02 over the following two years. This suggests that, when considering the need for service developments and maintaining establishments sustained recruitment effort will need to be made of around 75-100 posts a year for the next 4 years. Understanding the national shortage of registered nurses, the HB will continue with overseas recruitment campaigns and review educational commissioning accordingly which will also reflect the primary care and private sector information within overarching figures
This potential for a sustained reduction in the HB of more experienced nurses, with an increase in staff requiring mentorship and preceptorship and local induction (student nurses, newly registered nurses and overseas staff) has highlighted the need for the profession to focus on the development of a plan to manage this additional workload on our remaining staff in post. Experienced staff who plan to leave may be offered the opportunity to retire and return specifically to mentor junior and less experienced colleagues. The impact of the current nurse vacancies within baseline establishments, the dependency age profile of our patients, the need to open unplanned additional beds in year and increasing need for one to one support for some patients has increased reliance upon bank and agency nursing staff during 2015/16. This dependency is reflected within the variable pay spend which has increased during the year
-50
0
50
100
150
200
250
300
Cu
rren
t
Mar
Ap
r
May
Jun
Jul
Au
g
Sep
Oct
No
v
Dec
Jan
Feb
Mar
Series1

8
particularly in the use of Agency staff which is represents a high cost/value ratio. Registered Nurse Variable Pay Spend
VARIABLE PAY
APR MAY JUNE JULY AUG SEPT OCT NOV DEC JAN FYE
OVERTIME 10,468.48 10,956.12 6,288.18 5,863.15 4,849 7,686.41 8,967.96 12,473.86 12,627.49 6,522.88 8,6703.53
AGENCY 542,866 571,967 602,063 572,576 901,684 953,137 865,092 868,182 933,450 938,046 7,749,075
BANK 221,754 221,385 205,291 240,191 222,312 241,698 207,963 225,022 268,537 223,295 2,277,447
HCSW Variable Pay
2013/14 2014/15 2015/16 2015/16 Current 2015/16
Average Monthly
Average Monthly
Average Monthly Monthly Cumulative
Cost Cost Cost to
Date Cost Cost
AGENCY 4,315 24,927 123,508 161,925 1,235,076
BANK 237,469 285,900 309,025 296,210 3,090,251
The resolution of this financial and potential qualitative risk is mitigated to an extent by the ongoing recruitment drives and planned increases within registered and HCSW bank staff and the introduction of a Nursing Pool on each hospital site during 2016/17. The HB is currently establishing a Variable Pay Reduction Programme with 4 key workstreams including:
Bank/ Agency
E–rostering
recruitment
medical workforce
These groups will look to add financial controls, eradicate HCSW agency by end Q2, begin and continue to reduce reliance on nursing agency by end Q3, increase use of nurse pools and targeted recruitment to specific vacancies. PADR (Appraisal) Performance Appraisal and Development Review (PADR) is key to any organisation in ensuring that the workforce is valued and supported to develop and research has proven that it improves patient outcomes (Michael West). The HB is working with nurse managers to increase the current HB compliance rates reflected below, which remain below our target (although improved during 2015/16) of 85% compliance. The low rates are to an extent a reflection of the impact of nurse vacancies/service pressures on time to undertake PADR effectively and maintain service delivery. There is a drive to specifically support registered nurses as PADR is a key requirement within the Nurse Revalidation process. Registered Nursing HCSW
9
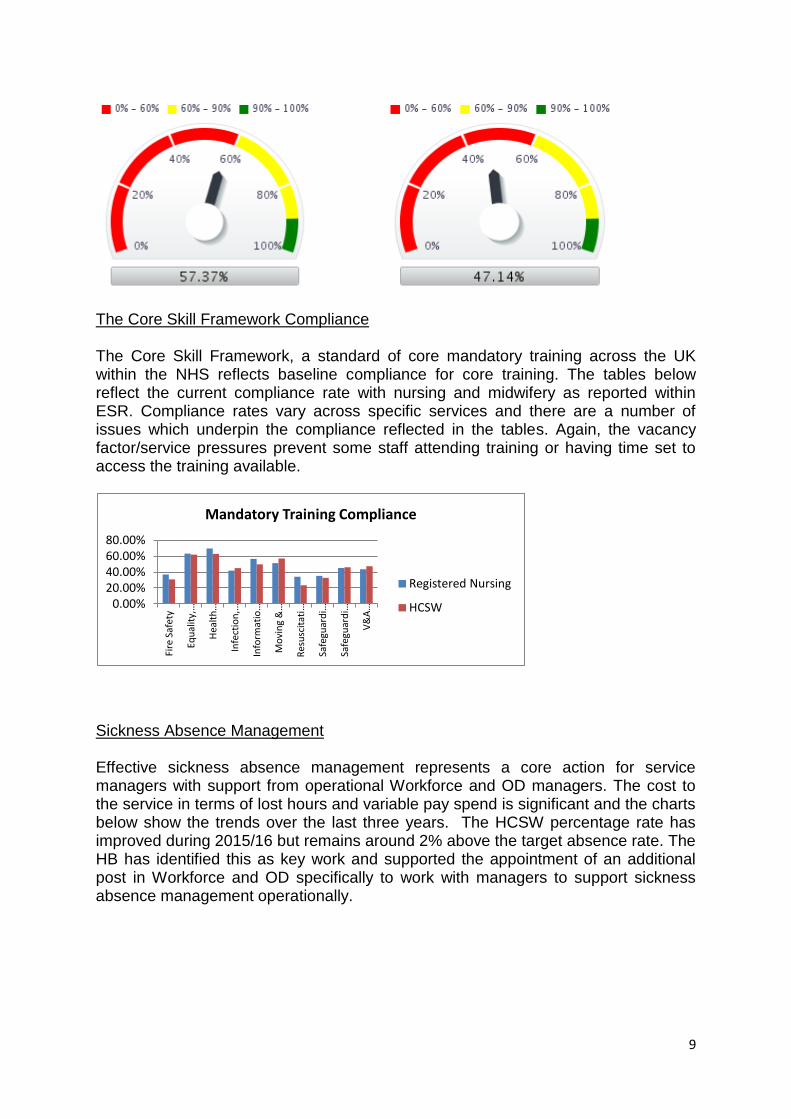
The Core Skill Framework Compliance The Core Skill Framework, a standard of core mandatory training across the UK within the NHS reflects baseline compliance for core training. The tables below reflect the current compliance rate with nursing and midwifery as reported within ESR. Compliance rates vary across specific services and there are a number of issues which underpin the compliance reflected in the tables. Again, the vacancy factor/service pressures prevent some staff attending training or having time set to access the training available.
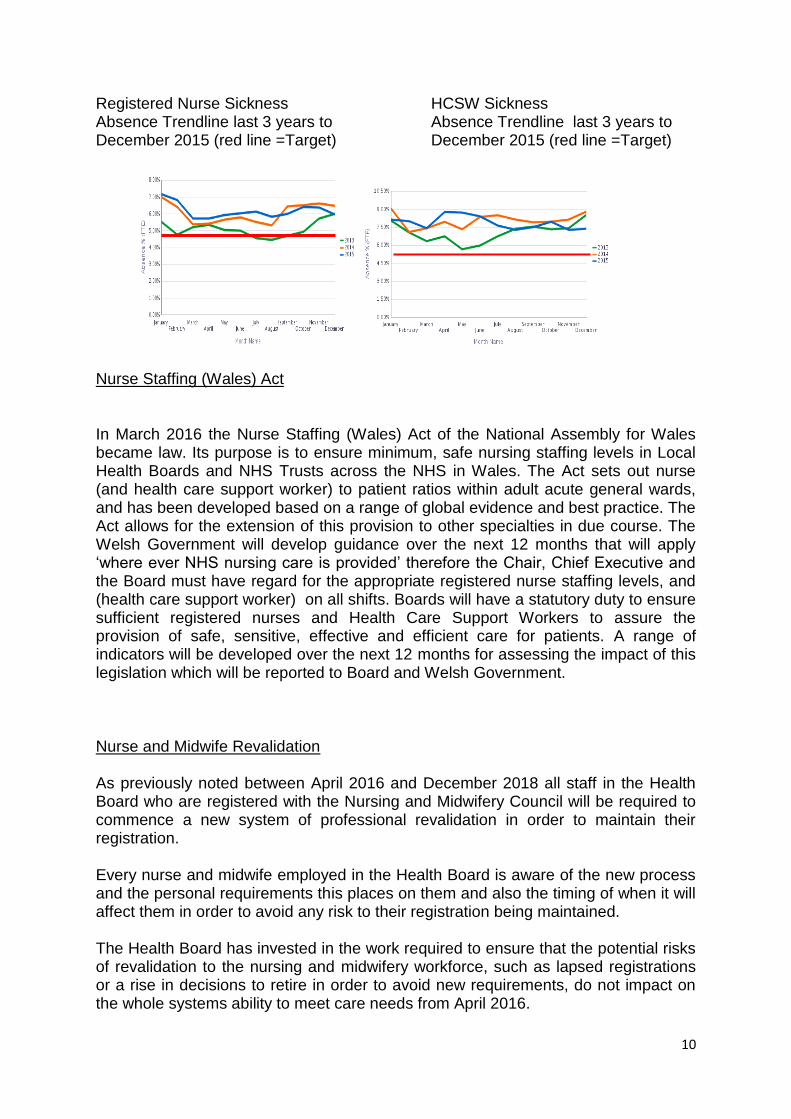
Sickness Absence Management Effective sickness absence management represents a core action for service managers with support from operational Workforce and OD managers. The cost to the service in terms of lost hours and variable pay spend is significant and the charts below show the trends over the last three years. The HCSW percentage rate has improved during 2015/16 but remains around 2% above the target absence rate. The HB has identified this as key work and supported the appointment of an additional post in Workforce and OD specifically to work with managers to support sickness absence management operationally.
0.00% 20.00% 40.00% 60.00% 80.00%
Fire
Saf
ety
Equ
alit
y, …
Hea
lth
…
Infe
ctio
n, …
Info
rmat
io…
Mo
vin
g &
…
Res
usc
itat
i…
Safe
guar
di…
Safe
guar
di…
V&
A …
Mandatory Training Compliance
Registered Nursing
HCSW
10
Registered Nurse Sickness HCSW Sickness Absence Trendline last 3 years to Absence Trendline last 3 years to December 2015 (red line =Target) December 2015 (red line =Target)
Nurse Staffing (Wales) Act
In March 2016 the Nurse Staffing (Wales) Act of the National Assembly for Wales became law. Its purpose is to ensure minimum, safe nursing staffing levels in Local Health Boards and NHS Trusts across the NHS in Wales. The Act sets out nurse (and health care support worker) to patient ratios within adult acute general wards, and has been developed based on a range of global evidence and best practice. The Act allows for the extension of this provision to other specialties in due course. The Welsh Government will develop guidance over the next 12 months that will apply ‘where ever NHS nursing care is provided’ therefore the Chair, Chief Executive and the Board must have regard for the appropriate registered nurse staffing levels, and (health care support worker) on all shifts. Boards will have a statutory duty to ensure sufficient registered nurses and Health Care Support Workers to assure the provision of safe, sensitive, effective and efficient care for patients. A range of indicators will be developed over the next 12 months for assessing the impact of this legislation which will be reported to Board and Welsh Government.
Nurse and Midwife Revalidation As previously noted between April 2016 and December 2018 all staff in the Health Board who are registered with the Nursing and Midwifery Council will be required to commence a new system of professional revalidation in order to maintain their registration. Every nurse and midwife employed in the Health Board is aware of the new process and the personal requirements this places on them and also the timing of when it will affect them in order to avoid any risk to their registration being maintained. The Health Board has invested in the work required to ensure that the potential risks of revalidation to the nursing and midwifery workforce, such as lapsed registrations or a rise in decisions to retire in order to avoid new requirements, do not impact on the whole systems ability to meet care needs from April 2016.
11
The UHB has developed a strong infrastructure locally to support registered nurses and midwives in preparing for revalidation including: ready access to up-to-date information on the HB intranet site with all the key documentation; a range of rolling workshops held across all sites which around 1200 staff attended to gain support in portfolio development; 525 trained as Confirmers; planning the alignment of PADR with revalidation dates to enable timely management and planning. During 2016/17 we anticipate 1050 nurses proceeding through the revalidation process. 2015/16 actions delivered The actions delivered to date through the Workforce and OD teams include:-
Recruitment into baseline establishment vacancies and management of turnover as projected with the national shortages of registered nurses across the UK
o Overseas recruitment has resulted in offers to 38 European nurses, 20 of whom started by 25th January 2016. A further 42 nurses from the Philippines (Skype) have been offered posts and further 166 through a visit in February 2016, totalling 246 overseas staff recruited.
o proactively linked with student nurses in training nearing completion and arranging informative recruitment days with presentations from the Board, videos reflecting local initiatives and awards achieved (nationally and locally) as well as formal interviews ending the day with presentations of ‘offer of employment’ letters. These have been very well attended and successful with 53 registered nurses recruited who started in September 2015 and a further 28 who start in March 2016. A further event was held February 2016 with 78 students receiving a conditional offer of employment.
o attended national Job fairs in London, Dublin and Birmingham. o attended and run 6 Career Fairs Withybush Hospital, Halliwell
Centre, Lampeter University, Parc-y-Scarlets Stadium, Amman Valley and Penglais Comprehensive Schools
o attended mock interviews for school pupils to prepare for employment at Ysgol Dyffryn Taf, Queen Elizabeth High School Carmarthen
o innovative advertising using videos of service leads’ on the job’ o reviewed our ‘Working for us’ internet pages by use of social
media Facebook and LinkedIn to both recruit and raise the profile of the HB
o created a dedicated role to develop our future workforce with increased focus on work experience and links with local colleges and schools
o established new vacancy and recruitment monitoring systems
the specific recruitment challenges related to specialist sub-specialties; mental health, practice nursing (who draw from our community nursing workforce),Paediatrics and Intensive Care
o as above, and

12
o run specific focussed campaigns for specialty staff
the ability to support the ongoing development of staff including expansion of numbers accessing career pathways from HCSW – registration training
o worked with the local university to develop career pathway for career stage 4 support staff to have an access route to reduced registered training programme – 4 staff have had funding to date.
the control of the variable pay expenditure o established new group specifically working to reduce variable pay
spend in nursing on agency and bank o plans in train to develop locally based nurse pools on each acute
site.
retention of our experienced staff o increased support for staff to retire and return to work to retain our
experienced staff and help develop junior colleagues through succession planning
o wide range of staff benefits offered to our staff
the management of the projected overseas and newly registered nurses starting along with increased numbers of nurses in train in term of mentorship and preceptorship support
o workforce and OD leading project plan to lead on all aspects of recruitment/employment/relocation with specific nurse sub-group to plan and mitigate professional challenges.
the nursing and midwifery revalidation requirements o a range of rolling workshops held across all sites which around
1200 staff attended to gain support in portfolio development; 525 trained as Confirmers; planning the alignment of PADR with revalidation dates to enable timely management and planning.
the impact of patient dependency shift within acute, community and primary care services associated with the underlying needs of our patients (chronic conditions, frailty and dementia) increasing the need for 121 care.
o Nurse acuity modelling has been undertaken within the general medical and surgical wards on a six monthly basis and provided the HB with some indication of a shift in the dependency levels within the acute wards. The Workforce and OD team have been supporting the patient scoring activity by triangulating with workforce and financial information. The staffing configuration across the wards is flexible in order to manage additional wards/beds it is difficult to map trends to accurately inform prospective establishment requirements against a changing case-mix.
Development programmes have been designed and delivered to support the introduction of Assistant Practitioner roles. To date,
o 75 staff completed underpinning 60 credit SHS107/108 qualification since 2010 and are eligible for Trainee Assistant Practitioner Roles.
o 4 Trainee Assistant Practitioners are currently in post with a further 2 to commence shortly.
13
o 8 staff are currently employed in Assistant Practitioner Roles and have completed the second part of the qualification (additional 60 credit modules linked to the role and are fully registered as Assistant Practitioners within Hywel Dda.
o 2 previous Assistant Practitioners are currently following pre-registration nursing programmes which they entered at year 2 of the programme due to their Assistant Practitioner qualification.
o A total of 20 staff have completed the full 120 credit qualification which enables the shortened route to nurse pre-registration training. 4 of these have commenced this training in September 2015.
The Challenges/Actions Planned 2016/17 The key challenges and actions planned for nursing and midwifery are summarised below:
recruitment into baseline establishment vacancies and management of turnover as projected mitigating the risk of the national shortages of registered nurses across the UK (Q3 2016)
managing the specific recruitment challenges related to specialist sub-specialties; mental health, practice nursing (who draw from our community nursing workforce), Paediatrics and Intensive care through focussed campaigns (Q3/4 2016)
support the ongoing development of staff including expansion of numbers accessing career pathways from HCSW – registration training (Q4 2016)
control of the variable pay expenditure though the variable Pay Reduction Programme groups (Q3 2016)
focussed retention of our experienced staff through retire and return options
management of the projected overseas and newly registered nurses along with increased numbers of student nurses in training in terms of mentorship and preceptorship support (Q3 2016)
the development of nurse rotations linked with university programme development to support nurses to move from BSc- MSc through structured workplace and academic development. These rotations could be placed within specific sub-specialties, general medicine or surgery, community and primary care to intensivist allowing development whilst supporting organisational need. (Q3 2016)
deliver the required changes to workforce arising from requirements of the Nurse Staffing Levels (Wales) Bill (Q1 and Ongoing)
ensure the delivery of 2000 nursing and midwifery revalidations during 2016/17 (Q1 and Ongoing)
management of the impact of patient dependency shift within acute, community and primary care services associated with the underlying needs of our patients (chronic conditions, frailty and dementia) through focussed development programmes on frailty care (Q1 and ongoing)
further strengthening of IT infrastructure to support community and integrated teams functioning effectively (Q1 and ongoing)

14
delivery of PADR and mandatory training compliance through structured planning of PADR and facilitated use of the E- learning options combined with face to face clinical update programmes through structured full day training programmes nursing teams (Q2 and ongoing)
The detailed HB OD plan is in section 3 on page 96
Medical and Dental Workforce The HB currently employs 455.9 wte (600 staff) medical staff, excluding doctors in training. The current turnover rate based on the last three years is 15.16%. The average retirement age based upon the last 3 years is 61. Currently there are 40.96 wte who are 61 yrs old or above and a further 157.43 wte who are currently over 50. There are currently 113.9 wte vacancies (Consultants, Spec and Junior posts) across the HB.
Age profile
The average number of leavers per month has fairly static over the last three years from 10.10 wte in 2013 to 10.48 wte in 2014 to 8.73 in 2015 year to date. However, the percentages may be skewed by the number of clinical staff choosing to retire and return Since 1 March 2015 to 29 February 2016, there were 10, of these 5 (50%) returned.
Turnover
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
1 4 7 10131619222528313437404346
Turnover Rate FTE(12m)
Linear (Turnover RateFTE (12m))

15
The vacancies within acute services relate primarily to key sub-specialties where there are national shortages and the HB has experienced difficulties in attracting staff into established posts when they find work more attractive financially as Locum and Agency staff. The table below reflects those vacancies which have been advertised more than once.
SPECIALTY DOCTOR
GENERAL MED CARE OFTHE ELDERLY X2 EMERGENCY MEDICINE X2 GENERAL SURG X1 OPTHALMOLOGY X1 PSYCHIATRY GEN ADULT X1
CLINICAL FELLOW T RAUMA AND ORTHOPAEDICS X 4 GEN SURG X 4 EMERGENCY MED X 2
CONSULTANT
T RAUMA AND ORTHOPAEDICS X 3 CARE OFTHE ELDERLY X 2 RESP MED X 1 CARDIOLOGY X 1 UROLOGY X 1 GASTROENTEROLOGY X 1 EMERG ASSESS UNIT X 1 MEDICAL ASSESSMENT UNIT X 1 HAEMATOLOGY X 1 RADIOLOGIST X 7 HISTOPATHOLOGIST X 3 ORTHOGERIATRIC X 1 PAEDS X 1 OBS TETRICS AND GYNAECOLOGY X 1 PSYCHIATRY GEN ADULT X1
The HB is looking at how we attract and retain clinical staff through specific workstreams focussing on filling our established posts in particular those which link to our key strategic aims eg diagnostic services, respiratory, cardiac and reducing variable pay spend. Recruitment are working with medical agencies to support us in attracting talent and also for wider promotion of the HB when they attend recruitment fairs across the UK and overseas by providing them with information, materials and links to the HB web pages. In doing this it creates capacity for the HB to focus on;
Campaigns for difficult to fill posts with input from current clinical staff, blogs, video walks through the workplace etc
the effective management of the detailed recruitment process
development of initiatives locally such as the work undertaken within Withybush Hospital where the HB has been successful in the recruitment of Junior Medical Doctors since the loss of trainees in August 2015. The programme entailed detailed adverts being constantly advertised and job descriptions tailored specifically at Overseas doctors seeking to come to the UK to gain experience and MRCP. A robust 2 stage interview process was introduced to establish the English language skills or the individual doctors & a formal interview. If the doctors were then still interested in the programme and were successful at interview they were then offered 2 year appointments. A robust induction followed. Skills Laboratories and assessments were then conducted in order to assess and sign off competencies for F1 and F2 years. This process will now be

16
replicated in general surgical services and trauma and orthopaedic services during 2016/7 where the HB anticipate rota issues.
encouraging our current medical staff to raise the profile of the HB through their own Clinical networking acting as ambassadors of their own clinical sub-specialties.
Learning and embedding lessons learned to support overseas staff in the following areas:-
o Effective Support structures; Medical education, continuing professional development, and career development and Clinical practice.
o Mentoring for the doctors within the departments established o Facilitated Peer Support Groups which provide a means of
continuing support to help resolve individual challenges of NHS working and living. Facilitators were volunteers: local consultants, overseas doctors themselves, who had also trained as mentors. Each was faced with the challenge of fitting the role into their busy clinical schedule, as well as that of delivering the role.
Sickness Absence Trend over the last 3 years
The HB acknowledges that the sickness absence information is based upon information reflected within ESR and there is local recognition that some sickness absence may not be recorded within the system. This will therefore feature in our 2016/17 work plan. Appraisal Compliance
93% Compliance

17
The current appraisal compliance figure for the HB is 93% in terms of evidence of appraisal although the HB acknowledges that the quality of the appraisals is variable. The HB has invested in a specific post of Revalidation and Appraisal Manager to support the delivery of this work. The Medical appraisal and revalidation processes across the Health Board have continued to develop over the last year with an even greater emphasis being placed on quality assurance and information triangulation. Since the introduction of Medical Revalidation, it has become evident that across various departments of the Health Board there is a wealth of information that can be used to inform appraisal meetings, however, a lack of consistency relating to the number of Doctors who access the information available has been identified. From April 2016, a new process of providing information directly to Doctors will be rolled out across the Health Board. This information will relate to continuing professional development, individual performance activity, along with incidents, claims and complaints. The process will raise the quality of appraisal inputs and outputs and will provide added assurances to the Responsible Officer when making revalidation recommendations. The process will also help to raise the quality of the job planning process, which although is completely separate from Medical Appraisal, is inarguably interlinked, in the sense that information that informs one process can also be used to inform the other. Providing information in this way will also further encourage Doctors to ensure that any data they input into various IT systems, records etc, is as accurate as possible.
Variable Pay The variable pay spend reflected in the table below represents a significant risk fiscally and qualitatively and some directly related to the recruitment difficulties cited earlier. The Variable Pay Reduction Programme includes a specific medical workstream tasked with saving £5m by April 2017 through reduction in use of locum and agency staff, refined job planning, improved control mechanisms, standardised locum rates and improved rota management.
VARIABLE PAY
APR MAY JUNE JULY AUG SEPT OCT NOV DEC JAN FYE
AGENCY 382,859 205,008 55,708 176,532 70,994 -1,756 115,222 51,765 130,803 109,167 1,296,302
PREMIUM LOCUM 300,849 328,608 368,601 532,956 486,706 616,588 757,815 624,222 836,433 840,098 5,692,875
LOCUM 355,515 418,964 445,301 505,286 515,670 477,054 545,685 644,012 551,667 569,991 5,029,145
2015/16 Actions Delivered
Successful recruitment of Junior Medical Doctors at Withybush General Hospital since the loss of trainees in August 2015. The programme entailed detailed adverts being constantly advertised and job descriptions tailored specifically at Overseas doctors seeking to come to the UK to gain experience and MRCP. Robust 2 stage interview process was introduced to establish the English language skills or the individual doctors & the informal question and answer session. If the doctors were

18
then still interested in the programme we could offer them and passed the initial interview, and they were then offered conditional 2 year appointments immediately at the end of the interview subject to the satisfactory employment checks etc. A robust induction followed. Skills Laboratories and assessments were then conducted in order to assess and sign off competencies for F1 and F2 years
In relation to recruitment the following initiatives have been started during 2015/16
o Where posts that are hard to recruit, meetings are taking place with the service to draw up bespoke impact adverts, and job description, and all adverts for substantive Consultants posts now being advertised as a Glossy colour advert instead of lineage, as well as Services pages being drawn up, and even some with Video links from members of staff.
o Incremental Overseas credit being publicised, when doctors are appointed so that they are not being placed on the minimum point even though experienced from overseas.
o Skype Interviews are now being undertaken within the health board which is reducing non attendees, and offers are being made within 24 hours, as not to loose the candidates to another health board.
o Permanent recruitment from agencies are now in place, which is enhancing our profile in all areas.
o Links are being developed with universities in Bulgaria, Czech Republic and Hungary, as well as Sri Lanka utilising the MTI scheme.
o 3 Months free hospital accommodation being given to overseas doctors to help them to settle into the UK.
o Initiatives such as Bevan Fellows and Research from Professor Lewis’ recent Chair appointment are being promoted in adverts.
o Attendance at conferences are being undertaken – Geriatric annual National meeting being held in Ceredigion 4/3/2016, where we will have a stand to promote the HB and vacancies we have.
o Promotion of adverts and health board in practise on social media. o Relocation/Recruitment Incentives being looked including top of
the scale salary proposals at to be proposed for overseas doctors in line with other HB’s
Maintained our medical staff appraisal compliance at above 90%
BGH Consultant is the national Stroke lead
Developed a medical mentoring scheme in partnership with the Royal College of Physicians and the British Medical Association (BMA)
Delivered the Consultant Leadership Development Programme.
Hywel Dda is the first Health Board in Wales to appoint two Bevan Commission Fellows,
appointment of a respiratory chair with Swansea University – these are both important means which will help to attract and retain leading

19
clinicians into Wales, creating a dynamic learning and innovative climate in which to live and work
Consultant job planning compliance at 72%
Medical Revalidation Hywel Dda University Health Board is the Designated Body for between 750 and 800 Doctors at any one time and is a combination of both Secondary Care and Primary Care Doctors. The GMC anticipated that in:-
Year 1 (April 2013-March 2014) 20% of all Doctors involved at the outset would be revalidated
Year 2 (April 2014-March 2015) 40% of all Doctors involved at the outset would be revalidated
Year 3 (April 2015- March 2016) 40% of all Doctors involved at the outset would be revalidated
The HB met each of the GMC targets for Years 1 & 2 and are on course to meet the target set for Year 3. This means that the majority of Doctors for whom Hywel Dda is currently a Designated Body have been successfully revalidated and are currently in the second cycle of the process. The Medical Revalidation process has developed considerably over the last year and this has been mainly facilitated by the quality assurance of the appraisal process across the HB. Triangulating and reviewing information which is held by the HB with that which Doctors take to appraisal has helped to identify areas for improvement which may be directly applicable to individual Doctors (e.g. performance), and/or other services and processes across the Health Board as a whole. Years 3 & 4 of this five year revalidation cycle will see considerably less numbers of Doctors being revalidated and this will provide us with time to further improve and ensure that the process is as robust as possible. The Challenges/Actions 2016/17 The main challenges and planned actions to mitigate the medical workforce across acute and primary care services are:
The planning to manage the age profile of the workforce and mitigate risks associated with impact upon service delivery through use of alternative roles such as Advanced Practice roles, Physicians Associates, Physicians Assistants and new workforce models (Q1 and ongoing)
Minimising the recruitment challenges due to national shortages of key specialist areas by focussed overseas recruitment campaigns, new workforce models and replicating the successful recruitment work undertaken in WGH (Q1 and ongoing)
Mitigate the risks associated with the national shortfall in trainee GPs across the UK through positive recruitment emphasising the benefits of working within mid and west Wales. Working closely with the Mid and West Wales Collaborative and opportunities to establish links with students from England.
Using the National Medical Workforce training deficit information reported through the centre for Workforce intelligence to inform strategic planning
20
Manage the impact on service delivery/rotas of the deanery on withdrawing training posts and impact of the projected fill rate for Core medical Training of only 40% through innovation and use of new roles as previously described. There is a specific risk associated with the relocation of WGH anaesthetic trainees to GGH. Service managers are looking at alternative working patterns currently and potentially recruitment of further Physicians Assistants who have been used very successfully across the service.
(Q1ongoing)
in Mental Health the Deanery posts are not always filled and this has a direct impact upon service delivery- the service continues to try to secure CT LAS posts but this remains challenging (Q1ongoing)
the filling of middle grade posts recruitment continues to be after 3 cycles of advertisement and final offering posts the candidates withdrew their interest during 2016/17 we will be looking at opportunities for alternative workforce models as well as focussed recruitment overseas (Q1ongoing)
the current high locum and agency usage meaning high cost service provision which doesn’t assist in developing services or provides high quality. The variable pay workstream will focus upon reduction of spend and filling posts (Q1ongoing)
Job planning is now planned to be fully implemented and used as a means to ensure service delivery including specific activity targets mapped to sessions to enable effective delivery of the service plans and targets.
maintain current level of consultant appraisal above 90% (Q1ongoing)
the HB will be actively promoting the medical Engagement Scales survey this year to gain as much information from our medical workforce locally to inform our priorities and planning in terms of their wellbeing.
begin work to ensure Core Skills Training Framework is also delivered to our medical workforce using E-learning through joint work between Post Graduate education and training and medical recruitment team. (Q3 )
The detailed HB OD plan is in section 3 on page 96
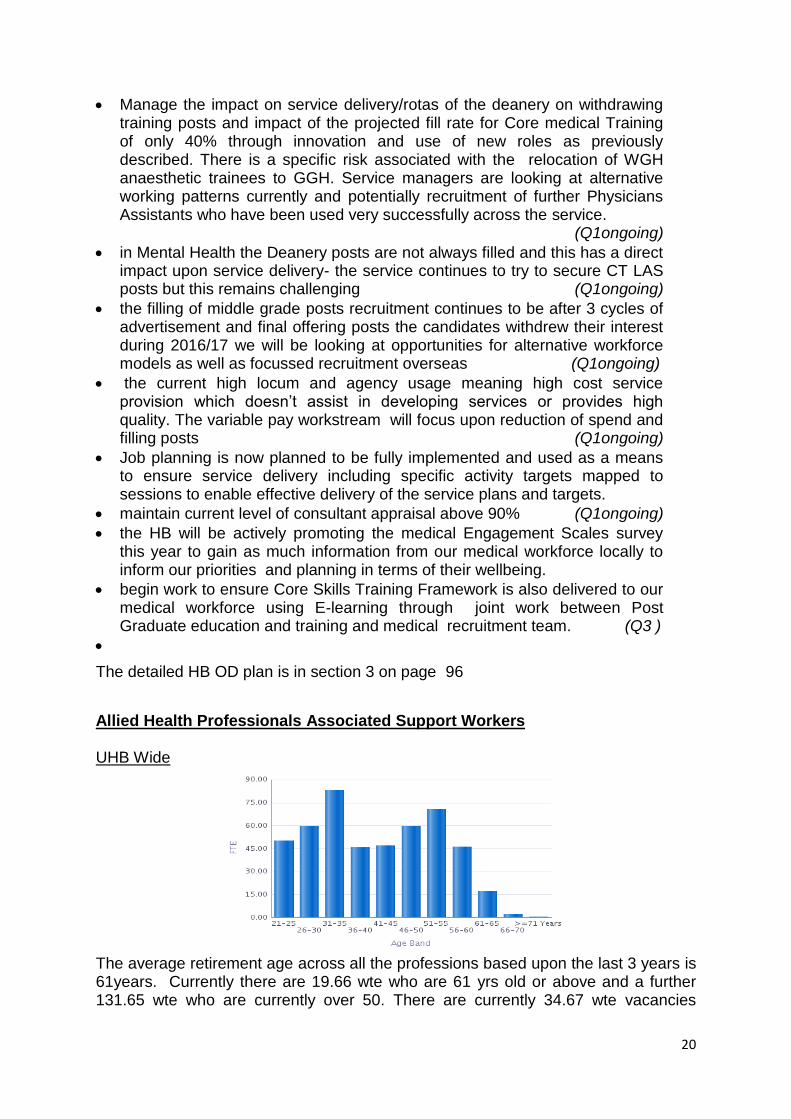
Allied Health Professionals Associated Support Workers UHB Wide
The average retirement age across all the professions based upon the last 3 years is 61years. Currently there are 19.66 wte who are 61 yrs old or above and a further 131.65 wte who are currently over 50. There are currently 34.67 wte vacancies

21
across the HB. The average number of leavers per month has been fairly static over the last three years from 2.37 wte in 2013 to 2.96 wte in 2014 to 2.93 wte in 2015 year to date.
Currently clinical services are focusing on re-ablement within community settings and the development of additional therapy roles. When there are difficulties in recruiting to vacancies within these professions, where the teams are smaller and there is less flexibility to move staff to cross cover there is a real impact upon the ability to deliver the service. The prospective recruitment plan will acknowledge the need for continued focussed recruitment campaigns and proactive recruitment of final year students in training combined with development of opportunities to ‘grow our own’ through the support worker route. The core service priorities across therapies are 7 day working, stroke re-ablement and prevention, frailty and chronic conditions management (community/acute). Physiotherapy has had a percentage increase in activity in year ranging from 3-15% across specific services and there are continued challenges associated with baseline funding of posts and ongoing funding from both ICF and CRT funding streams associated with developments identified within last years plan. Dietetics has a focus on frailty and elderly nutrition and hydration, obesity and stoke management and is seeking to undertake an establishment review as there are differentials in service provision due to historic differences in baseline workforce within each county All services have reviewed their workforce plans and workforce wte in line with any funding anomalies and developments associated with organisational and tier 1 target service delivery. Some services have not reviewed the baseline establishments since the HB was established and the workforce differentials across counties effects delivery models as previously noted. This work is now underway. Variable Pay AHPs
VARIABLE PAY
APR MAY JUNE JULY AUG SEPT OCT NOV DEC JAN FYE
AGENCY 2,628 657 1,402 13,632 7,985 -3,520 25,010 74,042 -13,96 108,734
Actions Delivered 15/16
Turnover
0.00%
1.00%
2.00%
3.00%
4.00%
5.00%
6.00%
7.00%
8.00%
9.00%
1 2 3 4 5 6 7 8 9 10 11 12
2015
2014
2013

22
Undertook focussed recruitment campaign for physiotherapists in Ireland, revisiting in April
Planned pre registration day with Cardiff University students to interview and provisionally offer posts as we are with pre registration nurses.
The Challenges/Actions 2016/17 The main challenges facing Allied Health Professionals are:
The HB will review baseline establishment and funding streams in light of the activity levels and the disparity in terms of workforce/service provision across the counties (Q1ongoing)
The management of frailty across acute, community and primary care is key to unlocking many of the operational service delivery challenges. The HB will review the HCSW Skills to Care Programme to enhance the Frailty training content in line with recent pilot work undertaken within PPH, and undertake ward based multi disciplinary staff development (Q1)
The current recruitment of registered physiotherapists due to a national shortage combined with ongoing difficulties in recruiting to West Wales will be managed through continued focussed campaigns (UK and overseas) combined with a review of the workforce model and potential to better utilise HCSW and Assistant Practitioners across acute, community and primary care. (Q1ongoing)
the impact of other local HB’s offering higher A4C bands to attract staff will be mitigated by better publicising the positive and innovative practices in the HB
support the delivery of the re-ablement agenda and increase community and primary based services with a challenge in recruiting registered workforce will be part of the establishment review agenda and also review of workforce model. (Q1ongoing)
need to expand re-ablement and frailty management and move to 7 day services to better support patient flows through prevention of admission, front of house MDT assessment of patients and community and primary care based re-ablement activity (Q2ongoing)
the podiatry service will be redesigning the vascular pathway through skills development within Primary and Community Care and increased workforce (1x B7 and 6x B6) within the podiatry team to support clinical interventions (Q3)
the AHP priority work streams align in terms of development required to support frailty as previously noted, stroke patients and cardiac/respiratory chronic conditions
PADR and Mandatory training compliance is patchy across professions and focussed planning will be undertaken to attain compliance levels. (Q1ongoing)
The detailed HB OD plan is in section 3 on page 96 Registered Physiotherapists & Associated Support Workers

23
The HB currently employs 112.41 wte (127 headcount) registered with a turnover of 9.14% in the last year, and 39.84 wte (42 headcount) support workers with a turnover of 7.32% in the last year. There are currently 15.59 wte registered and 11.5 wte support staff who are over 50 yrs of age. The average retirement age for the profession is 61 years, so there are 2.75 registered and 1.62 support staff currently over 61 who could potentially choose to retire in the near future. Physiotherapy turnover in 2015 by wte was 11.80% and when broken down by county service Carmarthenshire was 9.95%, Ceredigion was 14.96% and Pembrokeshire was 13.47%. In addition there are currently 10 wte registered physiotherapy vacancies across the HB which represents a challenge to service delivery given the proportion of the establishment and this is informing our recruitment projections and planning for the profession. Age profile Registered HCSW
Registered Sickness Absence Unregistered Sickness Absence last 3 years to December 2015 last 3 years to December 2015 (red line =Target) (red line =Target)
Age Band Headcount FTE
21-25 23 22.40
26-30 17 16.26
31-35 26 22.96
36-40 17 14.37
41-45 10 8.76
46-50 15 12.06
51-55 12 9.57
56-60 4 3.27
61-65 3 2.75
Grand Total
127 112.41
Age Band Headcount FTE
21-25 3 2.90
26-30 6 5.50
31-35 7 5.41
36-40 4 3.18
41-45 8 6.89
46-50 4 4.45
51-55 4 5.18
56-60 3 4.70
61-65 2 1.14
66-70 1 0.48
Total 42 39.84

24
The sickness absence levels for registered staff have increased across the service over the last 2 quarters of the year in comparison with previous years which could be attributed to the additional pressure of the vacancy factor on the remaining staff in post, whilst the support staff sickness absence is below the national target. PADR (Appraisal) Compliance
The appraisal compliance is currently poor, managers are under pressure to deliver clinical services which may account for the low level. Workforce and OD have provided detailed information to senior manager on compliance to inform their planning. The aim is to achieve 85% compliance and maintain this level during 2016/17.
Registered HCSW
Core Skills Training Framework Compliance
The Core Skill Framework, a standard of core mandatory training across the UK within the NHS reflects baseline compliance for core training. The tables below reflect the current compliance rate within physiotherapy as reported within ESR. Again, the vacancy factor/service pressures prevent some staff attending training or having time set to access the training available. ,

25
Variable Pay (Registered and Unregistered)
VARIABLE PAY
APR MAY JUNE JULY AUG SEPT OCT NOV DEC JAN FYE
OVERTIME 221.24 176.51 166.83 500.74 578 719.26 635.36 559.06 324.14 725.73 4606.87
The variable pay spend is attributable to baseline establishment vacancies. The focussed recruitment campaign will address this spend and the variable pay workstreams will encompass a reduction in spend during 2016/17. Occupational Therapy and Associated Support Workers The HB currently employs 65.32 wte (72 headcount) registered OT and 17.04 wte (21 headcount) support staff across the three counties. The wte turnover rate over the last 12 months has been 8.05% for registered and 1.24% for support staff The average age for retirement is 58 years , there are 7.78 wte registered and 3.69 wte currently over 55 years within the service. This number of registered staff as a proportion of the total number in post, who are also likely to be the more experienced clinical staff represent a challenge in terms of the knowledge and skills the service will potential lose over the next 2 -3 years. There are currently 2 wte registered vacancies. On the basis of historical analysis we are not overly concerned in terms of replacements with the current labour market.
0.00% 20.00% 40.00% 60.00% 80.00%
100.00%
Fire
Saf
ety
Equ
alit
y, …
Hea
lth
Saf
ety …
Infe
ctio
n, …
Info
rmat
ion
…
Mo
vin
g &
…
Res
usc
itat
ion
, …
Safe
guar
din
g …
Safe
guar
din
g …
V&
A M
od
ule
…
Mandatory Training Compliance
Physiotherapists
Support Staff

26
Age profile Registered HCSW
Registered staff Support Staff
Age Band Headcount FTE
21-25 8 8.00
26-30 6 6.00
31-35 14 13.10
36-40 8 7.03
41-45 6 5.68
46-50 11 9.22
51-55 10 8.42
56-60 5 4.27
61-65 4 3.60
Grand Total 72 65.32
Registered Sickness Absence Unregistered Sickness Absence last 3 year to December 2015 last 3 year to December 2015 (red line =Target) (red line =Target)
The registered and support staff sickness absence levels have improved during the year and are both below the national target
Age Band Headcount FTE
26-30 1 1.00
31-35 0 0.50
36-40 1 1.50
41-45 4 4.48
46-50 3 3.00
51-55 5 2.88
56-60 4 1.90
61-65 1 0.71
66-70 2 1.08
Grand Total 21 17.04

27
PADR (Appraisal) Compliance The appraisal compliance is currently poor and well below the expected 85% compliance. Managers are under pressure to deliver clinical services which may account for the low level. Workforce and OD have provided detailed information to senior manager on compliance to inform their planning. The aim is to achieve 85% compliance and maintain this level during 2016/17.
Registered HCSW
Core Skills Training Framework Compliance The Core Skill Framework, a standard of core mandatory training across the UK within the NHS reflects baseline compliance for core training. The tables below reflect the current compliance rate within physiotherapy as reported within ESR.
Variable Pay (Registered And Unregistered)
VARIABLE PAY
APR MAY JUNE JULY AUG SEPT OCT NOV DEC JAN FYE
OVERTIME 16.78 46.78 93.96 157.52
0.00% 10.00% 20.00% 30.00% 40.00% 50.00% 60.00% 70.00% 80.00% 90.00%
100.00%
Fire
Saf
ety
Equ
alit
y, D
iver
sity
&
Hu
man
Rig
hts
H
ealt
h S
afet
y &
W
elfa
re
Infe
ctio
n,
Pre
ven
tio
n &
…
Info
rmat
ion
G
ove
rnan
ce
Mo
vin
g &
H
and
ling,
…
Res
usc
itat
ion
, (L
evel
s 1
,2 a
nd
3)
Safe
guar
din
g A
du
lts,
(Le
vels
1 …
Sa
fegu
ard
ing
Ch
ildre
n, (
Leve
ls …
V
&A
Mo
du
le A
, B
and
C
Mandatory Training Compliance
OTs
Support Staff
28
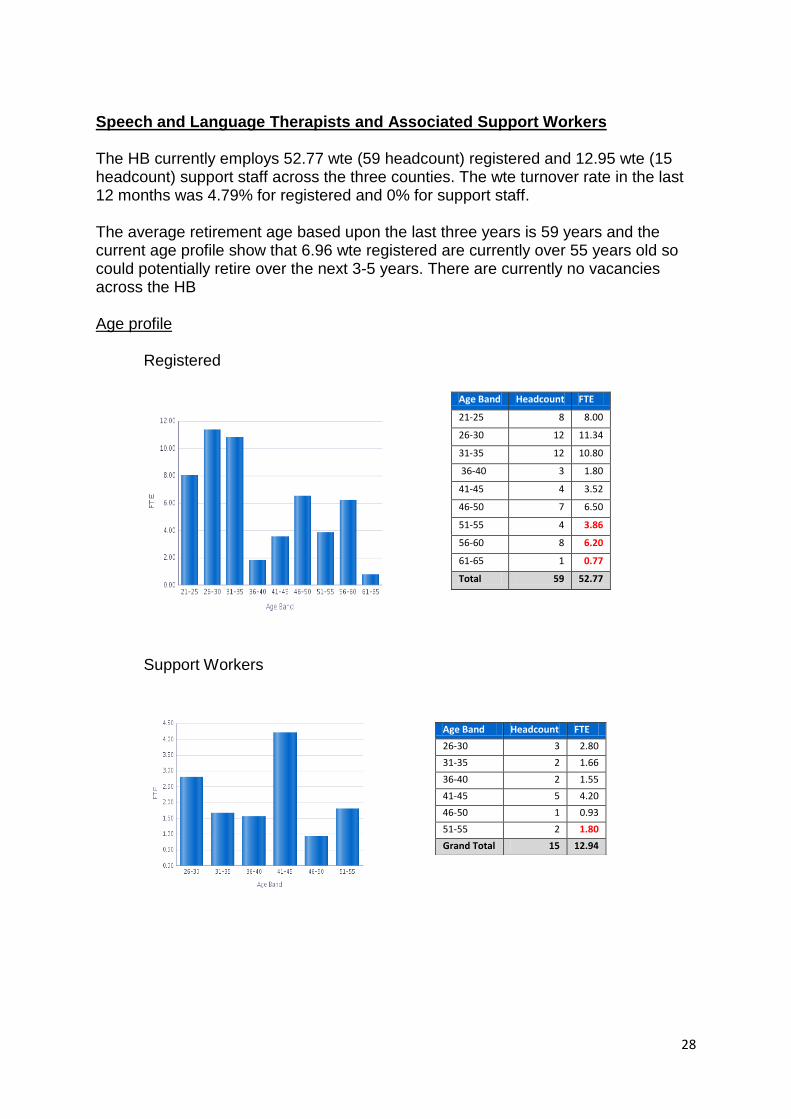
Speech and Language Therapists and Associated Support Workers The HB currently employs 52.77 wte (59 headcount) registered and 12.95 wte (15 headcount) support staff across the three counties. The wte turnover rate in the last 12 months was 4.79% for registered and 0% for support staff. The average retirement age based upon the last three years is 59 years and the current age profile show that 6.96 wte registered are currently over 55 years old so could potentially retire over the next 3-5 years. There are currently no vacancies across the HB Age profile
Registered
Support Workers
Age Band Headcount FTE
21-25 8 8.00
26-30 12 11.34
31-35 12 10.80
36-40 3 1.80
41-45 4 3.52
46-50 7 6.50
51-55 4 3.86
56-60 8 6.20
61-65 1 0.77
Total 59 52.77
Age Band Headcount FTE
26-30 3 2.80
31-35 2 1.66
36-40 2 1.55
41-45 5 4.20
46-50 1 0.93
51-55 2 1.80
Grand Total 15 12.94
29
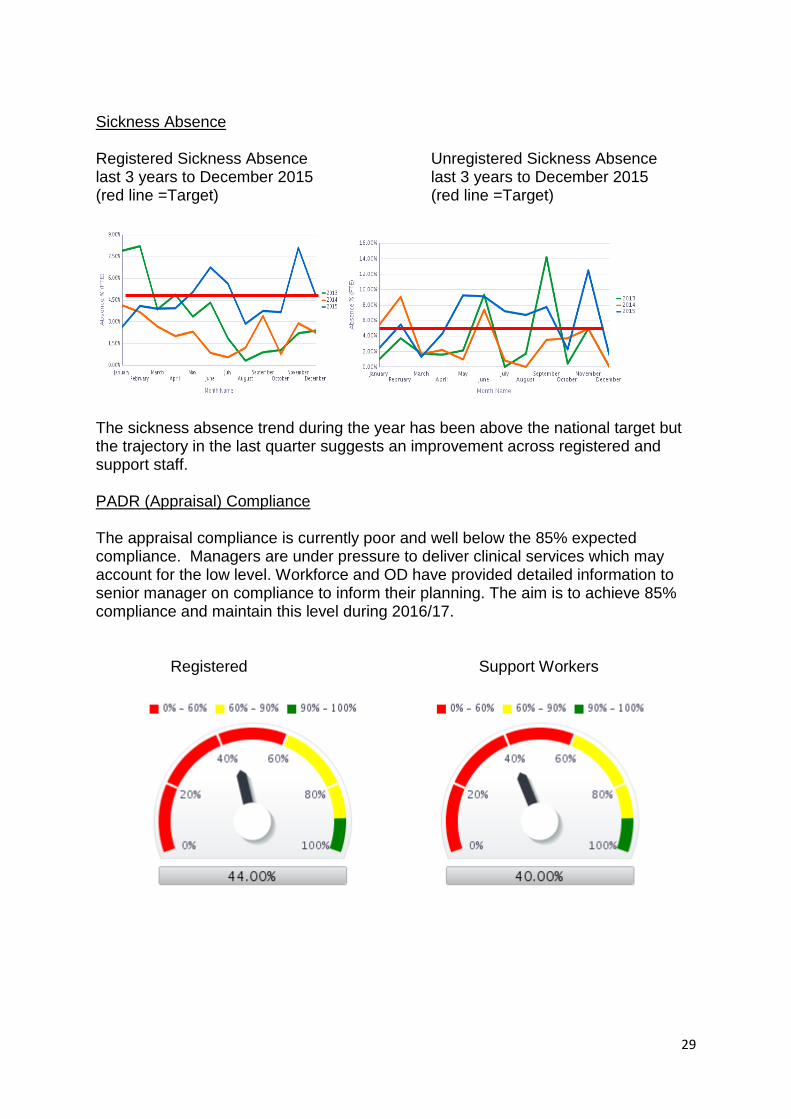
Sickness Absence Registered Sickness Absence Unregistered Sickness Absence last 3 years to December 2015 last 3 years to December 2015 (red line =Target) (red line =Target)
The sickness absence trend during the year has been above the national target but the trajectory in the last quarter suggests an improvement across registered and support staff. PADR (Appraisal) Compliance The appraisal compliance is currently poor and well below the 85% expected compliance. Managers are under pressure to deliver clinical services which may account for the low level. Workforce and OD have provided detailed information to senior manager on compliance to inform their planning. The aim is to achieve 85% compliance and maintain this level during 2016/17.
Registered Support Workers
30
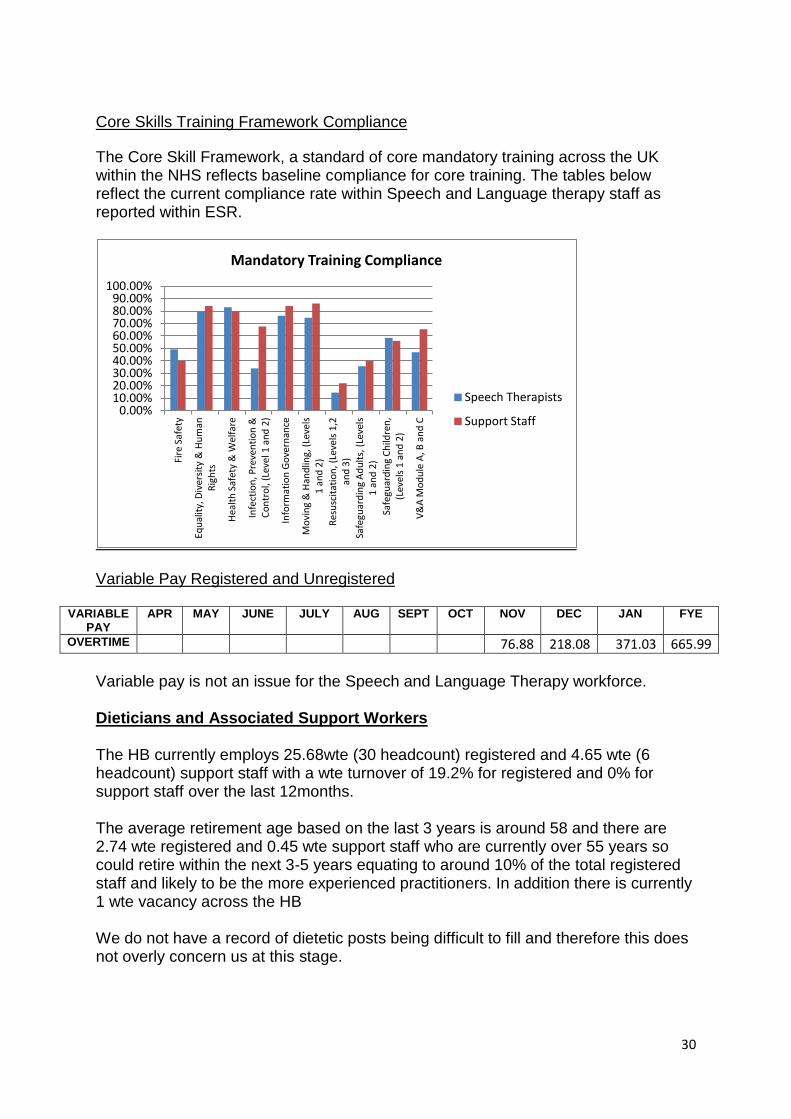
Core Skills Training Framework Compliance
The Core Skill Framework, a standard of core mandatory training across the UK within the NHS reflects baseline compliance for core training. The tables below reflect the current compliance rate within Speech and Language therapy staff as reported within ESR.
Variable Pay Registered and Unregistered
VARIABLE PAY
APR MAY JUNE JULY AUG SEPT OCT NOV DEC JAN FYE
OVERTIME 76.88 218.08 371.03 665.99
Variable pay is not an issue for the Speech and Language Therapy workforce. Dieticians and Associated Support Workers The HB currently employs 25.68wte (30 headcount) registered and 4.65 wte (6 headcount) support staff with a wte turnover of 19.2% for registered and 0% for support staff over the last 12months. The average retirement age based on the last 3 years is around 58 and there are 2.74 wte registered and 0.45 wte support staff who are currently over 55 years so could retire within the next 3-5 years equating to around 10% of the total registered staff and likely to be the more experienced practitioners. In addition there is currently 1 wte vacancy across the HB We do not have a record of dietetic posts being difficult to fill and therefore this does not overly concern us at this stage.
0.00% 10.00% 20.00% 30.00% 40.00% 50.00% 60.00% 70.00% 80.00% 90.00%
100.00%
Fire
Saf
ety
Equ
alit
y, D
iver
sity
& H
um
an
Rig
hts
Hea
lth
Saf
ety
& W
elfa
re
Infe
ctio
n, P
reve
nti
on
&
Co
ntr
ol,
(Lev
el 1
an
d 2
)
Info
rmat
ion
Go
vern
ance
Mo
vin
g &
Han
dlin
g, (
Leve
ls
1 a
nd
2)
Res
usc
itat
ion
, (Le
vels
1,2
an
d 3
)
Safe
guar
din
g A
du
lts,
(Le
vels
1
an
d 2
)
Safe
guar
din
g C
hild
ren
, (L
evel
s 1
an
d 2
)
V&
A M
od
ule
A, B
an
d C
Mandatory Training Compliance
Speech Therapists
Support Staff

31
Age profile
Registered HCSW
Sickness Absence Registered Sickness Absence Unregistered Sickness Absence last 3 year to December 2015 last 3 year to December 2015 (red line =Target) (red line =Target)
Age Band Headcount FTE
31-35 3 2.20
36-40 1 1.00
41-45 1 1.00
56-60 1 0.45
Grand Total
6 4.65
Age Band Headcount FTE
26-30 3 3.00
31-35 11 10.38
36-40 2 1.80
41-45 5 3.07
46-50 4 3.00
51-55 2 1.69
56-60 3 2.74
Grand Total 30 25.68

32
The sickness rate with registered and support staff were below the NHS Wales national target during 2015 with it exceeding the target only once during the year which it likely to reflect a single episode of sickness. PADR (Appraisal) Compliance Registered HCSW
The appraisal compliance is currently poor and significantly below the 85% expected level of compliance. Managers are under pressure to deliver clinical services which may account for the low level. Workforce and OD have provided detailed information to senior manager on compliance to inform their planning. The aim is to achieve 85% compliance and maintain this level during 2016/17. Core Skills Training Framework Compliance The Core Skill Framework, a standard of core mandatory training across the UK within the NHS reflects baseline compliance for core training. The tables below reflect the current compliance rate within Dietetics staff as reported within ESR.
Variable Pay
VARIABLE PAY
APR MAY JUNE JULY AUG SEPT OCT NOV DEC JAN FYE
OVERTIME 247.02 247.02
0.00% 10.00% 20.00% 30.00% 40.00% 50.00% 60.00% 70.00% 80.00%
Fire
Saf
ety
Equ
alit
y, …
Hea
lth
…
Infe
ctio
n, …
Info
rmat
i…
Mo
vin
g &
…
Res
usc
ita…
Safe
guar
d…
Safe
guar
d…
V&
A …
Mandatory Training Compliance
Dietitians
Support Staff

33
Podiatry The HB currently employs 29.98 wte (36 headcount) registered and 3.51wte (4 headcount) support worker podiatrists. The wte turnover in the last year has been 5.31% for registered and 0% for support workers. The average retirement age for Podiatrists over the last 3 years is 59 yrs and there are currently 5.05 wte registered and 1.8 wte support staff currently over 55 yrs old who could potentially choose to retire in the next 3-5 years. There are currently no vacancies across the HB. Age profile Registered HCSW
Age Band Headcount FTE 26-30 2 2.00 31-35 8 6.40 36-40 3 2.40 41-45 3 2.60 46-50 5 4.62 51-55 9 6.91 56-60 5 4.16 61-65 1 0.89 Grand Total
36 29.98
Age Band Headcount FTE
46-50 1 0.80
51-55 1 0.91
56-60 1 1.00
61-65 1 0.80
Grand Total
4 3.51

34
Sickness Absence Registered Sickness Absence Unregistered Sickness Absence last 3 years to December 2015 last 3 years to December 2015 (red line =Target) (red line =Target)
The sickness absence rate over 2015 has been well below the All Wales national target however for registered practitioners a peak was noted in December where rates increased above the target. PADR (Appraisal) Compliance Registered HCSW
The PADR compliance rate is well below the 85% target compliance for registered practitioners but above 60% however support worker compliance is extremely poor. Improvement is required and Workforce & OD staff are supporting managers to improve compliance within 2016/17.

35
Core Skills Training Framework Compliance The Core Skill Framework, a standard of core mandatory training across the UK within the NHS reflects baseline compliance for core training. The tables below reflect the current compliance rate within Podiatry staff as reported within ESR.
Healthcare Scientists Pathology The HB currently employs 104.55 wte (114 headcount) registered staff and 70.87 wte (91 headcount) support staff. The wte turnover rate over the last year was 4.09% for registered and 8.74% for support staff. There are currently 1.54 wte vacancies within the service. The average retirement age is 61 years and there are currently 3.07 wte registered and 4.04 wte support staff already over 60 years old and further 30.03 wte registered 15.86 wte support staff over 50 years old. Local intelligence reflects that some of the most senior clinical team are within this age bracket and this presents a risk to the service as there is a national shortage of the higher skilled specialists in Wales.
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
Fire
Saf
ety
Equ
alit
y, D
iver
sity
&
Hu
man
Rig
hts
Hea
lth
Saf
ety
& W
elfa
re
Infe
ctio
n, P
reve
nti
on
&
Co
ntr
ol,
(Lev
el 1
an
d 2
)
Info
rmat
ion
Go
vern
ance
Mo
vin
g &
Han
dlin
g,
(Lev
els
1 a
nd
2)
Res
usc
itat
ion
, (Le
vels
1,2
an
d 3
)
Safe
guar
din
g A
du
lts,
(L
evel
s 1
an
d 2
)
Safe
guar
din
g C
hild
ren
, (L
evel
s 1
an
d 2
)
V&
A M
od
ule
A, B
an
d C
Mandatory Training Compliance
Podiatrists
Support Staff

36
Age profile
Registered
Sickness Absence Registered Sickness Absence Unregistered Sickness Absence last 3 years to December 2015 last 3 years to December 2015 (red line =Target) (red line =Target)
Age Band Headcount FTE
21-25 3 3.00
26-30 10 10.00
31-35 9 8.00
36-40 22 19.44
41-45 15 14.31
46-50 18 16.69
51-55 20 19.93
56-60 11 10.10
61-65 5 2.07
66-70 1 1.00
Grand Total 114 104.55
Age Band Headcount FTE
<=20 Years 2 1.60
21-25 6 5.33
26-30 7 6.40
31-35 13 10.96
36-40 5 3.63
41-45 18 12.90
46-50 12 10.23
51-55 15 11.21
56-60 7 4.65
61-65 2 1.40
66-70 4 2.54
Grand Total 91 70.87

37
The sickness absence rate for registered staff has been compliant through the year but the support staff sickness absence has been variable although has begun to improve towards the end of 2015.
PADR (Appraisal) Compliance Appraisal compliance is currently poor and significantly below the 85% target for both registered and support staff. Workforce & OD have provided detailed information and are supporting managers to improve performance in this area.
Registered Unregistered
Core Skills Framework Compliance The Core Skill Framework, a standard of core mandatory training across the UK within the NHS reflects baseline compliance for core training. The tables below reflect the current compliance rate within Pathology staff as reported within ESR.

38
The Challenges/Actions 2016/17
Pathology services along with EBME have been nationally identified as priority staff groups for career stage 2 – 4 in Modernising Scientific Careers although the priority for these 2 groups is level 4 with the additional priority that this career stage acts as a conduit to career stage 5 equal to progression into registration programmes. This work has been reflected within the HB Education Commissioning figures based on best estimates in terms of numbers.
The management of the risks associated with the age profile of the most experienced clinical leads is of concern given the national shortage of experiences staff but hoped to be mitigated through dvelopment of current workforce/succession planning and imaginative recruitment campaign planning. (Q2 and ongoing)
Further planning for improved PADR and mandatory training compliance will be underway in year
The detailed HB OD plan is in section 3 on page 96 Variable Pay
VARIABLE PAY APR MAY JUNE JULY AUG SEPT OCT NOV DEC JAN FYE
OVERTIME 266.08 560.53 826.61 AGENCY 2,442 16,781 6,071 25,836 36,311 29,314 38,329 18,808 4,365 41,156 219,413
OVERTIME SCIENTIFIC PRACTITIONERS 1296.21 1372.63 530.61 76.47 3276.92
Variable pay is not an issue within the Healthcare Scientist workforce.
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
Fire
Saf
ety
Equ
alit
y, D
iver
sity
&
Hu
man
Rig
hts
Hea
lth
Saf
ety
& W
elfa
re
Infe
ctio
n, P
reve
nti
on
&
Co
ntr
ol,
(Lev
el 1
an
d 2
)
Info
rmat
ion
Go
vern
ance
Mo
vin
g &
Han
dlin
g,
(Lev
els
1 a
nd
2)
Res
usc
itat
ion
, (Le
vels
1,2
an
d 3
)
Safe
guar
din
g A
du
lts,
(L
evel
s 1
an
d 2
)
Safe
guar
din
g C
hild
ren
, (L
evel
s 1
an
d 2
)
V&
A M
od
ule
A, B
an
d C
Mandatory Training Compliance
Pathologists
Support Staff
39
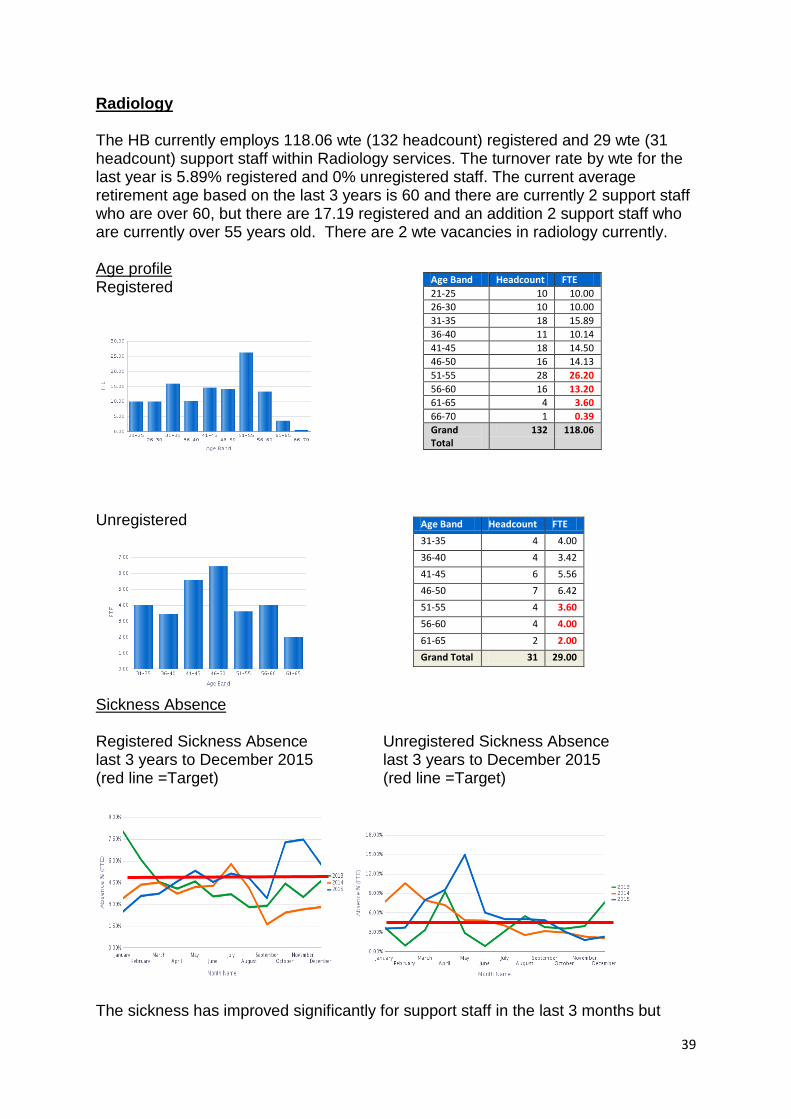
Radiology The HB currently employs 118.06 wte (132 headcount) registered and 29 wte (31 headcount) support staff within Radiology services. The turnover rate by wte for the last year is 5.89% registered and 0% unregistered staff. The current average retirement age based on the last 3 years is 60 and there are currently 2 support staff who are over 60, but there are 17.19 registered and an addition 2 support staff who are currently over 55 years old. There are 2 wte vacancies in radiology currently. Age profile Registered
Unregistered
Sickness Absence Registered Sickness Absence Unregistered Sickness Absence last 3 years to December 2015 last 3 years to December 2015 (red line =Target) (red line =Target)
The sickness has improved significantly for support staff in the last 3 months but
Age Band Headcount FTE
21-25 10 10.00
26-30 10 10.00
31-35 18 15.89
36-40 11 10.14
41-45 18 14.50
46-50 16 14.13
51-55 28 26.20
56-60 16 13.20
61-65 4 3.60
66-70 1 0.39
Grand Total
132 118.06
Age Band Headcount FTE
31-35 4 4.00
36-40 4 3.42
41-45 6 5.56
46-50 7 6.42
51-55 4 3.60
56-60 4 4.00
61-65 2 2.00
Grand Total 31 29.00

40
increased for registered staff throughout the year. PADR (Appraisal)Compliance The PADR compliance rates are excellent at over 80% compliance across registered and support staff are near the 85% target.
Registered HCSW
Core Skills Training Framework – Compliance The Core Skill Framework, a standard of core mandatory training across the UK within the NHS reflects baseline compliance for core training. The tables below reflect the current compliance rate within Radiology staff as reported within ESR.
Variable Pay
VARIABLE PAY
APR MAY JUNE JULY AUG SEPT OCT NOV DEC JAN FYE
OVERTIME 21.11 1792.24 1260.15 5742.12 1961.23 1396.23 792.56 990.25 1140.44 15096.33 AGENCY
Variable Pay will be monitored and reasons for use established to further reduce during 2016/17 Psychologists
0.00% 10.00% 20.00% 30.00% 40.00% 50.00% 60.00% 70.00% 80.00%
Fire
Saf
ety
Equ
alit
y, …
Hea
lth
Saf
ety …
Infe
ctio
n, …
Info
rmat
ion
…
Mo
vin
g &
…
Res
usc
itat
ion
…
Safe
guar
din
g …
Safe
guar
din
g …
V&
A M
od
ule
…
Mandatory Training Compliance
Radiologists
Support Staff

41
The HB currently employs 32.56 wte (36 headcount) psychologists with a wte turnover rate in the last year of 12.4%. There are currently 6.76 wte over 51 yrs old which represents around 20% of the workforce who could potentially retire over the next 5-10 years. There are currently 4 long term unfilled vacancies in Mental Health (Adult and Old Age) and 3 vacancies in Learning Disabilities. Age profile
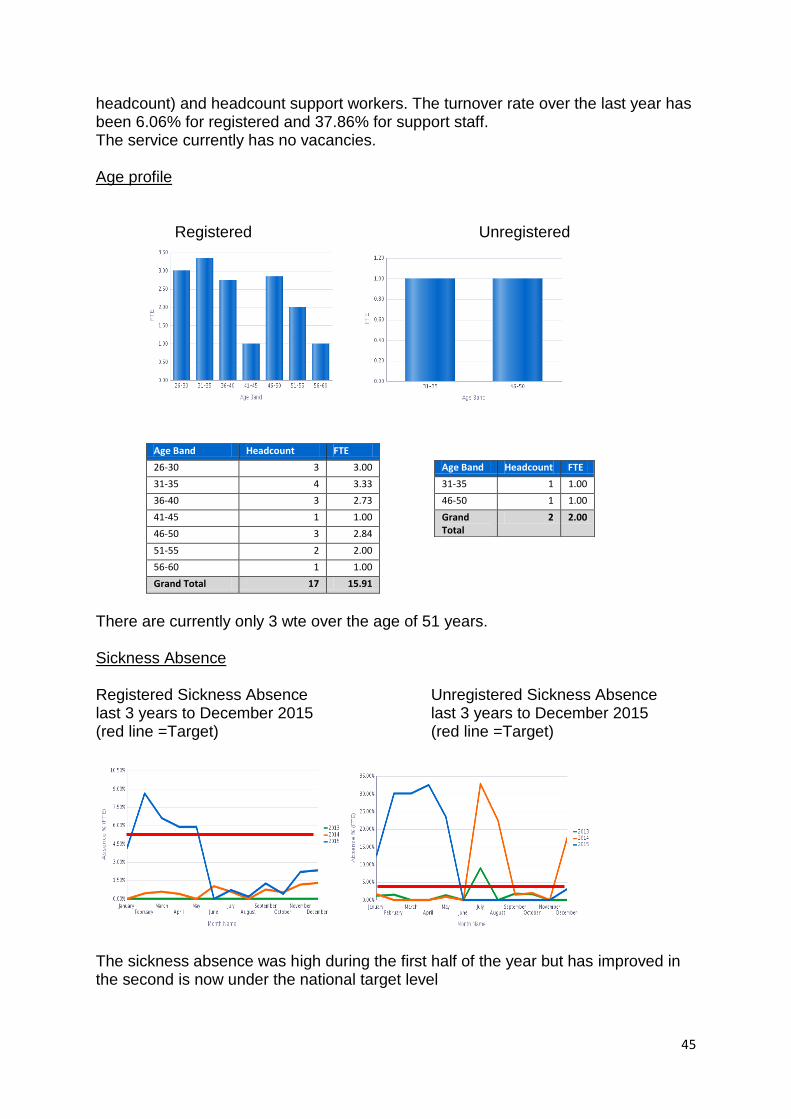
Sickness Absence last 3 years to December 2015 (red line =Target) Sickness absence has increased incrementally until September but has since reduced to the national target level.
PADR (Appraisal) Compliance Compliance rate is excellent at 82% so nearing the compliance target. Support will continue to be provided to ensure compliance remains at this or an improved level.
Age Band Headcount FTE
26-30 3 3.00
31-35 10 9.20
36-40 7 6.80
41-45 6 4.80
46-50 2 2.00
51-55 4 3.40
56-60 2 1.56
61-65 1 1.00
66-70 1 0.80
Grand Total 36 32.56

42
Core Skills Training Framework Compliance The Core Skill Framework, a standard of core mandatory training across the UK within the NHS reflects baseline compliance for core training. The tables below reflect the current compliance rate within Psychology staff as reported within ESR.
Challenges/ Action Plan 2016/17
the development of further clinical psychologists within acute services supporting chronic conditions management through in house succession planning, education commissioning and focussed recruitment
Retention and attracting psychology posts within the Mental Health Service
The detailed HB OD plan is in section 3 on page 96 Cardiology There are currently 24.06 wte (26 headcount) registered and 78.51 wte (94 headcount) support staff working within Cardiology. The wte turnover in the last 12 months is 17.02% for registered and 2.69% for support staff. The service has no current vacancies. Age profile There are currently 3.8 wte registered and 22.76 wte support staff are currently over 51yrs old.
0.00% 10.00% 20.00% 30.00% 40.00% 50.00% 60.00% 70.00% 80.00% 90.00%
Fire
Saf
ety
Equ
alit
y, D
iver
sity
&
Hu
man
Rig
hts
Hea
lth
Saf
ety
& W
elfa
re
Infe
ctio
n, P
reve
nti
on
&
Co
ntr
ol,
(Lev
el 1
an
d 2
)
Info
rmat
ion
Go
vern
ance
Mo
vin
g &
Han
dlin
g,
(Lev
els
1 a
nd
2)
Res
usc
itat
ion
, (Le
vels
1,2
an
d 3
)
Safe
guar
din
g A
du
lts,
(L
evel
s 1
an
d 2
)
Safe
guar
din
g C
hild
ren
, (L
evel
s 1
an
d 2
)
V&
A M
od
ule
A, B
an
d C
Mandatory Training Compliance
Psychologists

43
Registered
Unregistered
Sickness Absence Registered Sickness Absence Unregistered Sickness Absence last 3 years to December 2015 last 3 years to December 2015 (red line =Target) (red line =Target)
Sickness absence rates are high within both registered and unregistered staff. Workforce and OD will support the managers to apply the All Wales Policy to support staff to return to work as soon as possible and manage staff absence effectively. PADR(Appraisal) Compliance
Age Band Headcount FTE
21-25 2 2.00
26-30 5 5.00
31-35 2 1.70
36-40 4 3.41
41-45 7 6.19
46-50 2 1.96
51-55 2 2.00
56-60 1 0.80
>=71 Years 1 1.00
Grand Total 26 24.06
Age Band Headcount FTE
<=20 Years 2 2.00
21-25 5 4.03
26-30 6 5.60
31-35 10 8.29
36-40 12 9.66
41-45 16 13.29
46-50 14 11.87
51-55 7 5.60
56-60 13 11.16
61-65 8 6.60
66-70 1 0.40
Grand Total 94 78.51

44
Registered Unregistered
PADR compliance is below the target 85%, support staff have higher compliance rate than registered staff work is underway to increase compliance rate. Core Skills Framework Training Compliance The Core Skill Framework, a standard of core mandatory training across the UK within the NHS reflects baseline compliance for core training. The tables below reflect the current compliance rate within cardiology staff as reported within ESR.
Challenges/Actions 2016/7,
Workforce and OD are working with service managers on the development of a Cardiac Catheter Laboratory Development in terms of the workforce requirements for the model for the future service and also the development needs.
Planning to increase and attain PADR and Core Skill Framework compliance will be underway
The detailed HB OD plan is in section 3 on page 96 Audiology The HB currently employs 15.91 wte (17 headcount) registered and 2 wte (2
0.00% 10.00% 20.00% 30.00% 40.00% 50.00% 60.00% 70.00%
Fire
Saf
ety
Equ
alit
y, D
iver
sity
&
Hu
man
Rig
hts
Hea
lth
Saf
ety
&
Wel
fare
Infe
ctio
n, P
reve
nti
on
&
Co
ntr
ol,
(Lev
el 1
…
Info
rmat
ion
G
ove
rnan
ce
Mo
vin
g &
Han
dlin
g,
(Lev
els
1 a
nd
2)
Res
usc
itat
ion
, (Le
vels
1
,2 a
nd
3)
Safe
guar
din
g A
du
lts,
(L
evel
s 1
an
d 2
)
Safe
guar
din
g C
hild
ren
, (Le
vels
1 …
V&
A M
od
ule
A, B
an
d
C
Mandatory Training Compliance
Cardiology
Support Staff
45
headcount) and headcount support workers. The turnover rate over the last year has been 6.06% for registered and 37.86% for support staff. The service currently has no vacancies. Age profile
Registered Unregistered
Age Band Headcount FTE
26-30 3 3.00
31-35 4 3.33
36-40 3 2.73
41-45 1 1.00
46-50 3 2.84
51-55 2 2.00
56-60 1 1.00
Grand Total 17 15.91
There are currently only 3 wte over the age of 51 years. Sickness Absence Registered Sickness Absence Unregistered Sickness Absence last 3 years to December 2015 last 3 years to December 2015 (red line =Target) (red line =Target)
The sickness absence was high during the first half of the year but has improved in the second is now under the national target level
Age Band Headcount FTE
31-35 1 1.00
46-50 1 1.00
Grand Total
2 2.00

46
PADR (Appraisal) Compliance PADR compliance is excellent and over the 85% target.
Registered Unregistered
Core Skills Framework Training Compliance The Core Skill Framework, a standard of core mandatory training across the UK within the NHS reflects baseline compliance for core training. The tables below reflect the current compliance rate within audiology staff as reported within ESR.
Challenges/Actions 2016/17
Maintain current PADR compliance and Core Skills Framework compliance rate
The detailed HB OD plan is in section 3 on page 96 Neurophysiology The HB currently employs 3.81 registered staff (4 headcount) and 2 wte (2 headcount) are currently over 50 years old. There has been no turnover over the last year and there are no vacancies currently.
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
Fire
Saf
ety
Equ
alit
y, D
iver
sity
…
Hea
lth
Saf
ety
& …
Infe
ctio
n, …
Info
rmat
ion
…
Mo
vin
g &
…
Res
usc
itat
ion
, …
Safe
guar
din
g …
Safe
guar
din
g …
V&
A M
od
ule
A, B
…
Mandatory Training Compliance
Audiology
Support Staff
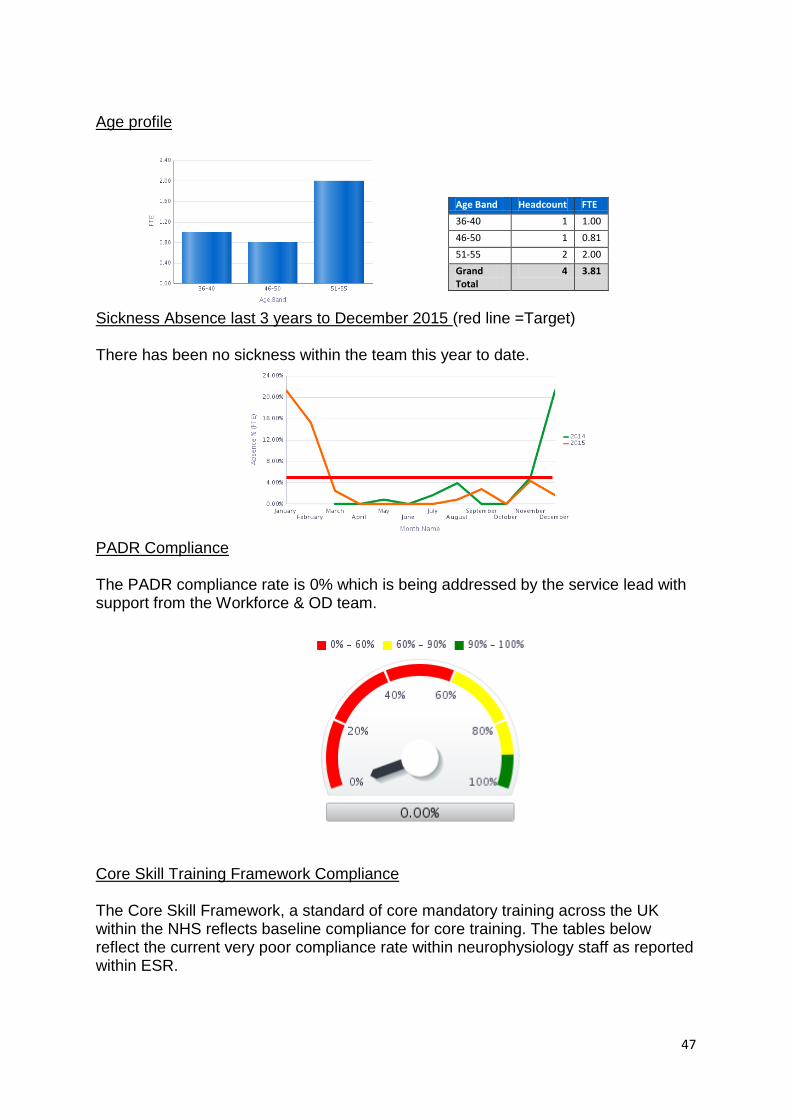
47
Age profile
Sickness Absence last 3 years to December 2015 (red line =Target) There has been no sickness within the team this year to date.
PADR Compliance The PADR compliance rate is 0% which is being addressed by the service lead with support from the Workforce & OD team.
Core Skill Training Framework Compliance The Core Skill Framework, a standard of core mandatory training across the UK within the NHS reflects baseline compliance for core training. The tables below reflect the current very poor compliance rate within neurophysiology staff as reported within ESR.
Age Band Headcount FTE
36-40 1 1.00
46-50 1 0.81
51-55 2 2.00
Grand Total
4 3.81
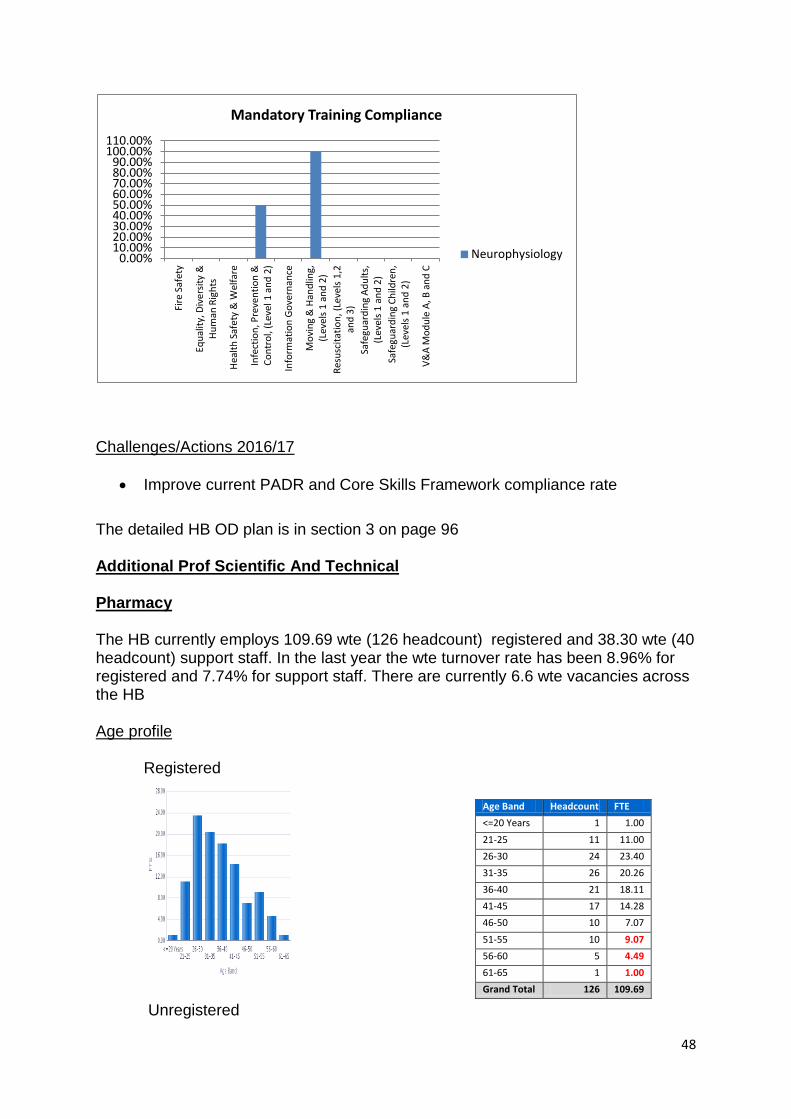
48
Challenges/Actions 2016/17
Improve current PADR and Core Skills Framework compliance rate
The detailed HB OD plan is in section 3 on page 96 Additional Prof Scientific And Technical Pharmacy The HB currently employs 109.69 wte (126 headcount) registered and 38.30 wte (40 headcount) support staff. In the last year the wte turnover rate has been 8.96% for registered and 7.74% for support staff. There are currently 6.6 wte vacancies across the HB Age profile
Registered
Unregistered
0.00% 10.00% 20.00% 30.00% 40.00% 50.00% 60.00% 70.00% 80.00% 90.00%
100.00% 110.00%
Fire
Saf
ety
Equ
alit
y, D
iver
sity
&
Hu
man
Rig
hts
Hea
lth
Saf
ety
& W
elfa
re
Infe
ctio
n, P
reve
nti
on
&
Co
ntr
ol,
(Lev
el 1
an
d 2
)
Info
rmat
ion
Go
vern
ance
Mo
vin
g &
Han
dlin
g,
(Lev
els
1 a
nd
2)
Res
usc
itat
ion
, (Le
vels
1,2
an
d 3
)
Safe
guar
din
g A
du
lts,
(L
evel
s 1
an
d 2
)
Safe
guar
din
g C
hild
ren
, (L
evel
s 1
an
d 2
)
V&
A M
od
ule
A, B
an
d C
Mandatory Training Compliance
Neurophysiology
Age Band Headcount FTE
<=20 Years 1 1.00
21-25 11 11.00
26-30 24 23.40
31-35 26 20.26
36-40 21 18.11
41-45 17 14.28
46-50 10 7.07
51-55 10 9.07
56-60 5 4.49
61-65 1 1.00
Grand Total 126 109.69

49
There are currently 14.56 wte registered staff (of which 5.49 are over 56 yrs) and 7.5 wte currently over 50 years old. Local knowledge reflects that the most senior and experienced team members are likely to be planning their retirement over the next 3-5 years which will impact on the service significantly in each county at a time when the impact of changes to pharmacy education will be impacting upon acute services in terms of student placement changes. Workforce and OD have established a group with the Head of pharmacy Services to evaluate the impact of the change, identify the risk and develop a plan to mitigate. Sickness Absence Registered Sickness Absence Unregistered Sickness Absence last 3 years to December 2015 last 3 years to December 2015 (red line =Target) (red line =Target)
Sickness absence rates within registered and support staff have been below the national target level for most of the year.
Age Band Headcount FTE
21-25 12 11.40
26-30 4 3.90
31-35 7 6.70
36-40 4 4.00
41-45 3 2.80
46-50 2 2.00
51-55 4 4.00
56-60 4 3.50
Grand Total 40 38.30
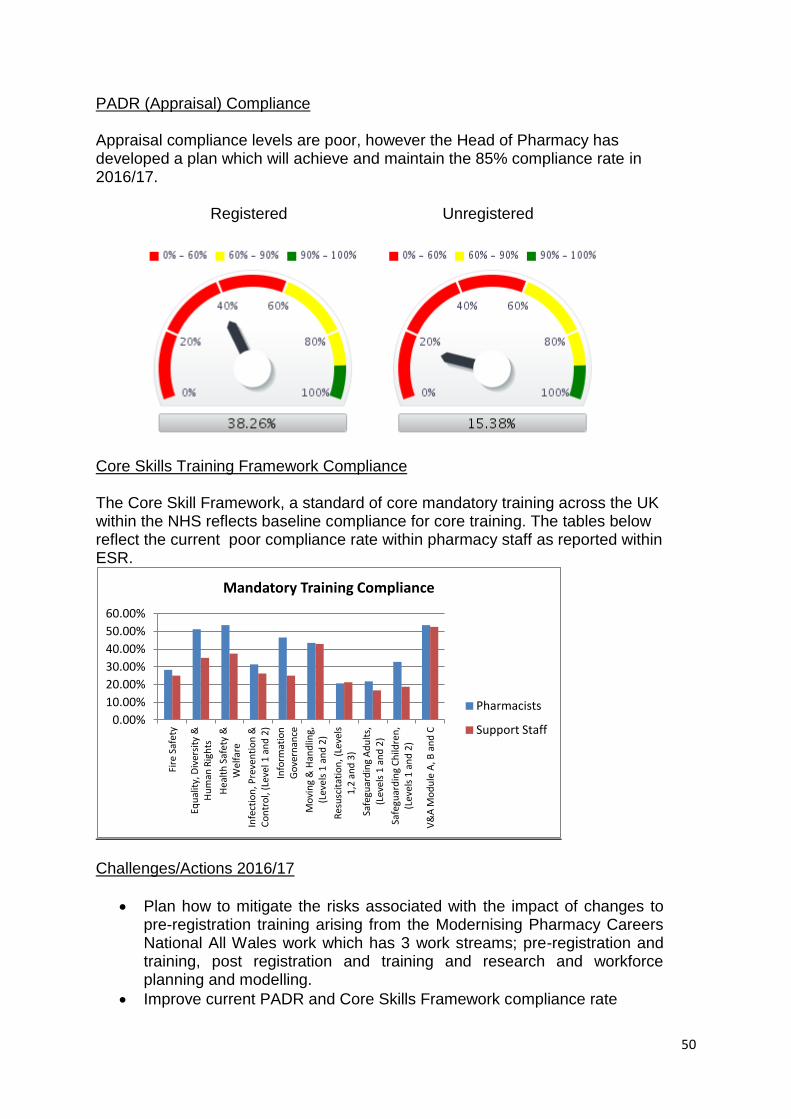
50
PADR (Appraisal) Compliance Appraisal compliance levels are poor, however the Head of Pharmacy has developed a plan which will achieve and maintain the 85% compliance rate in 2016/17.
Registered Unregistered
Core Skills Training Framework Compliance The Core Skill Framework, a standard of core mandatory training across the UK within the NHS reflects baseline compliance for core training. The tables below reflect the current poor compliance rate within pharmacy staff as reported within ESR.
Challenges/Actions 2016/17
Plan how to mitigate the risks associated with the impact of changes to pre-registration training arising from the Modernising Pharmacy Careers National All Wales work which has 3 work streams; pre-registration and training, post registration and training and research and workforce planning and modelling.
Improve current PADR and Core Skills Framework compliance rate
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
Fire
Saf
ety
Equ
alit
y, D
iver
sity
&
Hu
man
Rig
hts
Hea
lth
Saf
ety
&
Wel
fare
Infe
ctio
n, P
reve
nti
on
&
Co
ntr
ol,
(Lev
el 1
an
d 2
)
Info
rmat
ion
G
ove
rnan
ce
Mo
vin
g &
Han
dlin
g,
(Lev
els
1 a
nd
2)
Res
usc
itat
ion
, (Le
vels
1
,2 a
nd
3)
Safe
guar
din
g A
du
lts,
(L
evel
s 1
an
d 2
)
Safe
guar
din
g C
hild
ren
, (L
evel
s 1
an
d 2
)
V&
A M
od
ule
A, B
an
d C
Mandatory Training Compliance
Pharmacists
Support Staff

51
Support primary care cluster management teams with additional pilots.
Align with new national Pharmacists in Practice Programme to be launched April 16
The detailed HB OD plan is in section 3 on page 96
Variable Pay
VARIABLE PAY
APR MAY JUNE JULY AUG SEPT OCT NOV DEC JAN FYE
OVERTIME 202.73 0 202.73
Variable pay is not a concern at this time. Operating Department Practitioners (ODP) and Assistant (ODA) The HB currently employs 52 wte (52 headcount) ODP and 3.08 wte (4 headcount) ODA. The wte turnover rate in the last year was 9.58% (ODP) and 0% (ODA). There are currently 0 vacancies across the HB. Age profile
ODP ODA
Age Band Headcount FTE
26-30 5 4.85
31-35 7 6.85
36-40 11 10.80
41-45 5 4.72
46-50 14 13.85
51-55 6 6.00
56-60 3 3.00
61-65 3 1.92
Grand Total 54 52.00
Age Band Headcount FTE
26-30 1 1.00
36-40 1 0.75
46-50 1 0.80
51-55 1 0.53
Grand Total
4 3.08

52
The age profile represents 10.92 wte ODP are over 51 years and local intelligence informs the HB that there will be a number of these staff who are planning to retire over the next 3 years which represents 20% of the current ODP team. The risks have been mitigated by increasing our education commissioning figure this year to 10 places.
Sickness Absence ODP Sickness Absence ODA Sickness Absence last 3 years to December 2015 last 3 year to December 2015 (red line =Target) (red line =Target)
ODP sickness rates were above the national target level until November 2015 but then improved to below the required level. ODA sickness has remained constantly low. PADR Compliance
ODP ODA
The PADR compliance rates are very poor and the manager is developing a plan to work towards achieving the 85% target. Significant focus will be given to this during 2016/17.

53
Core Skills Training Framework Compliance The Core Skill Framework, a standard of core mandatory training across the UK within the NHS reflects baseline compliance for core training. The tables below reflect the current poor compliance rate within ODP/ODA staff as reported within ESR. Considering PADR activity appears to be very low it is pleasing to see training is in a much stronger position.
The Challenges/Actions 2016/17
the age profile of the team along with the service trend for specialised ODP according to clinical surgical subspecialties will impact upon service delivery and this is mitigated by the education commissioning figures and also in need for increased workplace development.
Improve current PADR and Core Skills Framework compliance rate
The detailed HB OD plan is in section 3 on page 96 Orthopaedic Technical Staff (OTS)
The HB currently employs 15.34 wte (16 headcount) OTS had no turnover during 2015/16. There are currently 7.81 wte currently over 51 years old which represents 50.9% of the workforce who could choose to retire over the 5 years so there will be a need for focussed succession planning . There are no vacancies currently.
0.00% 10.00% 20.00% 30.00% 40.00% 50.00% 60.00% 70.00% 80.00% 90.00%
Fire
Saf
ety
Equ
alit
y, D
iver
sity
&
Hu
man
Rig
hts
Hea
lth
Saf
ety
& W
elfa
re
Infe
ctio
n, P
reve
nti
on
&
Co
ntr
ol,
(Lev
el 1
an
d 2
)
Info
rmat
ion
Go
vern
ance
Mo
vin
g &
Han
dlin
g,
(Lev
els
1 a
nd
2)
Res
usc
itat
ion
, (Le
vels
1,2
an
d 3
)
Safe
guar
din
g A
du
lts,
(L
evel
s 1
an
d 2
)
Safe
guar
din
g C
hild
ren
, (L
evel
s 1
an
d 2
)
V&
A M
od
ule
A, B
an
d C
Mandatory Training Compliance
ODPs
ODAs

54
Age profile
Sickness Absence last 3 years to December 2015 (red line =Target)
Sickness absence levels have reduced throughout the year and are close to the national target level.
PADR (Appraisal) Compliance PADR compliance is below the 85% target and effort is required to ensure compliance. Support is being provided to the service.
Age Band Headcount FTE
26-30 2 2.00
41-45 1 1.00
46-50 5 4.53
51-55 3 3.00
56-60 3 2.81
61-65 2 2.00
Grand Total 16 15.34

55
Core Skills Training Framework Compliance The Core Skill Framework, a standard of core mandatory training across the UK within the NHS reflects baseline compliance for core training. The tables below reflect the current poor compliance rate within Orthopaedic Technical staff as reported within ESR.
Challenges/Actions 2016/17
Improve current PADR and Core Skills Framework compliance rate
The detailed HB OD plan is in section 3 on page 96 Chaplains The HB currently employs 4.09 wte (19 headcount) 17 of the 19 individuals over 51 yrs and 14 individuals over 61 yrs currently.
Age profile
This is not an unexpected profile for this workforce.
0.00%
10.00%
20.00%
Fire
Saf
ety
Equ
alit
y, D
iver
sity
& …
Hea
lth
Saf
ety
& …
Infe
ctio
n, …
Info
rmat
ion
…
Mo
vin
g &
Han
dlin
g, …
Res
usc
itat
ion
, …
Safe
guar
din
g …
Safe
guar
din
g …
V&
A M
od
ule
A, B
…
Mandatory Training Compliance
Orthopaedic Technicians
Age Band Headcount FTE
31-35 1 0.19
46-50 1 0.04
51-55 2 0.14
56-60 2 1.10
61-65 5 1.40
66-70 6 0.56
>=71 Years 2 0.64
Grand Total
19 4.09

56
Sickness Absence last 3 years to December 2015 (red line =Target) There is no sickness absence recorded for 2015.
PADR Compliance
The PADR compliance rate is zero and Workforce and OD will follow up to see where within the organisation the line management sits and support a broad PADR discussion with the team of Chaplains as supporting the spiritual wellbeing of our patients and staff is a priority. Core Skills Training Framework Compliance
0.00%
10.00%
Fire
Saf
ety
Equ
alit
y, D
iver
sity
& …
Hea
lth
Saf
ety
& …
Infe
ctio
n, …
Info
rmat
ion
…
Mo
vin
g &
Han
dlin
g, …
Res
usc
itat
ion
, …
Safe
guar
din
g A
du
lts,
…
Safe
guar
din
g …
V&
A M
od
ule
A, B
…
Mandatory Training Compliance
Chaplains

57
Challenges/Actions 2016/17
Ensure management line accountability clarified and ensure supported to achieve PADR and mandatory training
Improve current PADR and Core Skills Framework compliance rate
The detailed HB OD plan is in section 3 on page 96 Estates and Hotel Services The HB currently employs 617.71 (801 headcount) ancillary staff with a wte turnover rate of 5.68% over the last 12 months and 136.08 (137 headcount) estates staff with a wte turnover of 2.95 %over the year. Age Profile
The average retirement age based upon the last 3 years is 65 for estates and ancillary staff, currently there are 36.99 wte who are 65 yrs old or above and a further 346.62 wte who are currently over 50. There are currently 3 wte Estates and 3.42 wte Hotel services vacancies across the HB. The average number of leavers per month is fairly static over the last three years from 3.12 wte in 2013 to 4.21 wte in 2014 to 3.4 wte in 2015 year to date. The information, when reviewed in detail reflects that some managers and heads of services are within the group likely to be potentially retiring at the same time with a number of senior and experienced technical leads. The service has been actively succession planning and developing staff within the service to mitigate these risks. Turnover has significantly reduced during 2015.
Turnover
0.00%
1.00%
2.00%
3.00%
4.00%
5.00%
6.00%
7.00%
8.00%
1 2 3 4 5 6 7 8 9 10 11 12
2015
2014
2013

58
Age profile Hotel Services Estates
Sickness Absence Trend line over last 3 years (red line = target) Hotel Services Estates
Age Band Headcount FTE
<=20 Years 1 1.00
21-25 1 1.00
26-30 7 7.00
31-35 15 14.80
36-40 9 9.00
41-45 16 15.28
46-50 20 20.00
51-55 37 37.00
56-60 18 18.00
61-65 12 12.00
66-70 1 1.00
Grand Total 137 136.08
Age Band Headcount FTE
<=20 Years 27 13.85
21-25 44 28.89
26-30 77 58.34
31-35 62 49.73
36-40 60 50.23
41-45 69 52.77
46-50 116 92.77
51-55 122 98.11
56-60 114 91.69
61-65 75 57.36
66-70 25 17.57
>=71 Years 10 6.37
Grand Total 801 617.70

59
Sickness absence in hotel service has risen significantly in 2015/6 in Hotel services compared with Estates who have managed to control their rates in 2015 to below the all Wales target. PADR Compliance Hotel Services Estates
The PADR compliance within Hotel Services is poor and work is underway to significantly improve compared to Estates where the target of 85% has almost been achieved. Core Skills Training Framework Compliance The Core Skill Framework, a standard of core mandatory training across the UK within the NHS reflects baseline compliance for core training. The tables below reflect the current poor compliance rate within estates and ancillary staff as reported within ESR. It is disappointing to see training compliance so low compared to PADR performance in Estates and this will be addressed in 2016/17.
Variable Pay Hotel Services
VARIABLE PAY
APR MAY JUNE JULY AUG SEPT OCT NOV DEC JAN FYE
OVERTIME 3712.6 4049.48 4545.08 5772.44 6909.64 7576.16 6955.49 2920.62 5814.3 4323.85 52579.66
0.00% 10.00% 20.00% 30.00% 40.00% 50.00% 60.00%
Fire
Saf
ety
Equ
alit
y, D
iver
sity
…
Hea
lth
Saf
ety
& …
Infe
ctio
n, …
Info
rmat
ion
…
Mo
vin
g &
…
Res
usc
itat
ion
, …
Safe
guar
din
g …
Safe
guar
din
g …
V&
A M
od
ule
A, B
…
Mandatory Training Compliance
Hotel Services
Estates

60
Estates
VARIABLE PAY
APR MAY JUNE JULY AUG SEPT OCT NOV DEC JAN FYE
OVERTIME MAINT & WORKS 1377.39 781.31 343.46 1184.29 1327.64 1402.99 1104.02 2734.14 1552.44 11807.68 OVERTIME 582.57 655.44 1228.38 1247.62 1604.81 2040.42 1104.24 622.93 571.76 290.25 9948.42 AGENCY 915 2,347 -4,695
Variable pay will be reviewed as part of the variable pay programme to ensure it is not being used as an alternative to recruitment. Challenges/Actions 2016/17
the workforce and OD team will work with the Hotel Services team to raise the profile of PADR in deriving better outcomes from staff and work with them to see whether the investment will also reduce the high sickness rates over the last 3 years.
The need to grow our own future workforce, utilising opportunities of apprenticeships in both estates and facilities to mitigate the risks associated with the age profile, and loss of skilled trades.
The detailed HB OD plan is in section 3 on page 96
Administrative and Clerical The HB currently employs 1307.15 wte (1492 headcount) administrative and clerical staff and the wte turnover rate in the last year was 6.09%. This staff group encompasses many corporate services teams and managers such as Finance, Planning, IT, Workforce and OD and the senior managers who support the Executive Directors as well as the administrative support for all the clinical services. There are currently 20.6 wte vacancies currently across the HB.
Age Profile
The age profile information reflects that there are 520.88 wte who are currently over 51 yrs, however the impact of these figures is really only realised when drilled down
Age Band Headcount FTE
<=20 Years 6 5.76
21-25 43 39.89
26-30 103 93.68
31-35 125 105.11
36-40 125 109.32
41-45 212 187.39
46-50 275 245.89
51-55 266 235.80
56-60 211 183.21
61-65 95 77.56
66-70 27 21.38
>=71 Years 4 2.93
Grand Total
1,492 1,307.92

61
within specific service teams. All are undertaking succession planning and requested retirement/return numbers have increased as noted within the plan. Average retirement age mirrors statutory retirement ages.
Sickness and Absence Trendline over last 3 years (red line= target)
Sickness absence is below the national target. PADR Compliance
PADR compliance is poor and compliance is well below the 85% target expected. Support is being provided to managers to achieve and maintain compliance in 2016/17. Core Skills Training Framework Compliance
0.00% 10.00% 20.00% 30.00% 40.00% 50.00%
Fire
Saf
ety
Equ
alit
y, …
Hea
lth
…
Infe
ctio
n, …
Info
rmat
io…
Mo
vin
g &
…
Res
usc
itat
i…
Safe
guar
di…
Safe
guar
di…
V&
A …
Mandatory Training Compliance
Admin & Clerical

62
The Core Skill Framework, a standard of core mandatory training across the UK within the NHS reflects baseline compliance for core training. The tables below reflect the current poor compliance rate within administrative staff as reported within ESR. Challenges/Actions 2016/17
The need to grow our own future workforce, utilising opportunities of apprenticeships in A&C to mitigate the risks associated with the age profile, and loss experienced staff.
To ensure that CPD is supported within specialist corporate service teams; Finance, W&OD and IT
The detailed HB OD plan is in section 3 on page 96
Primary Care The Health Board is currently developing focused workforce plans for each of the clusters in line with the WG ‘A Planned Primary Care Workforce for Wales’ These plans will focus on the four main areas outlined in this document which are:
Putting in place the foundations for a more robust approach to workforce planning securing the long-term sustainability of the right sized workforce with the right skills to meet the expectations set out in the plan for a primary care service for Wales can only be achieved through a planned approach which takes a whole system view of healthcare. At present there are gaps in data and knowledge of the existing workforce and further clarity about the services which will increasingly be delivered in the community is needed if we are to understand the type of workforce required in the long term.
Supporting the continuing development of primary care clusters and the sharing of best practice. The Welsh Government is committed to the role of clusters as a means of transforming primary care. The maturity of clusters and the development of new roles and ways of working for the primary care workforce are inextricably linked. This document therefore sets out action to support cluster development in the immediate and medium term. These actions complement those in the primary care plan.
Investing in the development of the wider primary care workforce. The long-term sustainability of primary care in Wales will also depend on making the most of the widest possible range of professions and using their skills and abilities, according to the prudent healthcare principles. As part of this, the way in which the primary care workforce is educated and trained needs to be reconsidered in light of a new focus on inter-professional and multi-disciplinary working. e.g. Development of Prescribing Pharmacist Model for GMS creating a pathway into GMS

63
work will support the diversification of the workforce and of Physician Associates to support doctors in the diagnosis and management of patients. The training takes 2 years and current discussion within the region in relation to a consistent approach to supporting individuals through the programme is ongoing.
Stabilising key sections of the current workforce. GPs and the nursing profession are central to primary care and will remain so in the future. It is recognised that both of these groups are currently under considerable pressure. This document sets out actions to be taken in the next year to address a range of issues we face today ahead of new models of working being embedded across Wales
Hywel Dda has 7 Primary Care clusters:-
Taf/Tywi Locality (2Ts)
Amman Gwendraeth
Llanelli
North Ceredigion
South Ceredigion
North Pembrokeshire
South Pembrokeshire Each cluster has developed an evolving ‘live’ Cluster Network Action Plan which complements the individual practice development plans, and aims to tackle issues that cannot be managed at an individual practice level, or challenges that can be more effectively and efficiently delivered through collaborative action. This approach both contributes to the consistency of approach and also to enable more effective management of the impact of increasing workforce challenges. The Workforce The quality and detail of the Primary Care workforce data has proved to be challenging to collect to anywhere near the level of information available to the HB via ESR. Every year the HB primary care managers have worked hard to try and improve the information year on year. However, variation exists in terms of the quality of the data which has been raised at a national level, and work to improve the collation and quality of the data is being progressed nationally as well as locally. Hywel Dda is not unique in this respect. For example, data has been extracted from the Medical Performers list combined with the Exeter system and information submitted for annual returns to Welsh Government. Hywel Dda does not appear to have provided a return since 2013. The data presented, unless otherwise referenced, is sourced from the 2015 annual General Medical Services (GMS) return but as previously stated we have limited confidence in its accuracy. Some steps have been taken to improve as part of the latest iteration of the cluster reports which are due to be submitted by end April 2016. The workforce plan is a live document which informs our Workforce & OD priorities during the year and improving this data to inform priorities will be key.

64
The Workforce Profile The charts below are present headcount rather than wte
GPs make up 24% of the total workforce, with nurses making up 17%. Other roles including health care assistants, phlebotomists and AHPs account for 11%. 48% of the total headcount relates to non-clinical roles. Of these, there are 54 Practice Managers in Hywel Dda, 57 Medical Secretaries and 376 Receptionists. Our current primary care clinical workforce is below (headcount) but the proportion differs significantly in the individual clusters. GPs account for 46% of the total headcount, with nurses 33% and Health Care Assistants including Phlebotomists accounting for 18%.
GPs 24%
Nurse Practitioners 2%
Practice Nurses 15%
Advanced Paramedic
Practitioners
Specialist Practice Nurses
Nurse Prescribers
Health Care Assistants 7%
Phlebotomists 2%
Dispensers 2%
Pharmacists
Receptionists 34%
Practice Managers 5%
Medical Secretaries 5%
Other 4%

65
PRIMARY CARE CLINCIAL WORKFORCE PROFILE BY LOCALITY
GP 46%
Nurse Practitioner 4%
Practice Nurse 28%
Specialist Nurse Practitioner
1%
Advanced Paramedic Practitioner
Nurse Prescriber
Health Care Assistant
13%
Phlebotomist 5%
Dispenser 3%
Pharmacist
PRIMARY CARE CLINICAL WORKFORCE - HYWEL DDA
GP52%
Nurse Practitioner
Practice Nurse26%
Specialist Nurse Practitioner
Advanced Paramedic
Practitioner
Nurse Prescriber
Health Care Assistant
11%
Phlebotomist4%
Dispenser7%
Pharmacist
Taf/Tywi Locality
GP49%
Nurse Practitioner
4%
Practice Nurse33%
Specialist Nurse Practitioner
4%
Health Care Assistant
10%
Llanelli
GP45%
Nurse Practitioner
7%
Practice Nurse28%
Nurse Prescriber1%
Health Care Assistant
12%
Phlebotomist5% Dispenser
1%
Pharmacist1%Amman Gwendraeth
GP43%
Nurse Practitioner
1%
Practice Nurse24%
Specialist Nurse Practitioner
3%
Health Care Assistant
18%
Phlebotomist10%
Dispenser1%North Ceredigion

66
The information presented in these charts is challenging to analyse without knowledge of functionally how they are used as teams to deliver a service overall within each practice. For example some have phlebotomists, others don’t but do their HCSW undertake phlebotomy? During 2016/17 part of the work required within individual clusters is to review how the practices utilise their resource base and share best practice, so that when there are opportunities to modernise their workforce model they can be planning future workforce now, and where appropriate begin to develop their skills. Turnover GPs and nursing roles are central to primary care and will remain so in the future. There is however a growing recognition, that other professional groups such as Pharmacists, Therapists, Advanced Practitioners and Physicians Associates will form a substantial part of the solution. Workforce by Cluster– contractor teams (GMS database information 2015) (*5 year planned
retirements as described/known by the contractors)
Locality (no of practices)
GP NP PN SNP APP N presc
HCA Phleb Dispen Pharm
2T (8 ) 48 0 24 0 0 0 10 4 7 0
GP44%
Nurse Practitioner
4%
Practice Nurse32%
Health Care Assistant
18%
Phlebotomist2%South Ceredigion
GP52%
Nurse Practitioner
3%
Practice Nurse25%
Advanced Paramedic
Practitioner
1%
Health Care Assistant
12%
Phlebotomist6%
Dispenser1%North Pembrokeshire
GP38%
NP7%
PN27%
N presc1%
HCA13%
Phleb5%
Dispen8%
Pharm1%
South Pembrokeshire

67
*9 *1 *6
Amman Gwendraeth (8)
37 *11.5
6 *2
23 *3
0 0 1 10 4 1 1
Llanelli (9) 36 *17
3 *2
24 *5
3 0 0 7 0 0 0
N Ceredigion (7) 32 *10.5
1 *0
18 *3
2 0 0 13 7 1 0
S Ceredigion (7) 34 *21
3 *1
25 *2
0 0 0 14 2 0 0
N Pembrokeshire (9)
50 *17.25
3 *2
24 *7
0 1 0 12 6 1 0
S Pembrokeshire (6)
34 *18
6 (8)*
24 *3
0 0 1 12 4 7 1
KEY: GP General Practitioner (N.B this includes partners and salaried GPs) NP Nurse Practitioner, PN Practice Nurse, SNP Specialist Nurse Practitoner, APP Advanced Paramedic Practitioner, N Presc Nurse Prescriber, HCA Health Care Assistant, Phle Phlebotomist, Dispen Dispenser, Pharm Pharmacist
GP NP PN SNP APP N Presc HCA Phle Dispen Pharm
Total
271
22
162
5
1
2
78
27
17
2
Predicted Retirements 2015-2020
104.25 (38%)
14* 63%
29 18%
Predicted GP Retirement Turnover and retirement data is not robust so the retirement dates reflected here are those known to the GP Practices, however the annual return 2015 predicts that within 5 years, 38% of current GPs are likely to retire. To mitigate this risk the HB continues to explore innovative approaches to GP recruitment and creation of capacity through new roles. Local experience indicates that up to 50% of retiring GPs may retire and return on a salaried basis, given that anecdotally many are retiring due to partnership pressures and pension changes. In addition, we currently have three GP Training Schemes in Hywel Dda. The national workforce information suggests that for 2016/2017 and beyond these schemes are going to be difficult to recruitment into across both Wales and the UK as a whole. Predicted Nursing Retirement The annual return suggests that 63% nurse practitioners and 18% of practice nurses are likely to retire within the next 5 years. It is suggested that the nursing team data presented here does not reflect an entirely accurate picture due to the constraints/interpretation of the data collection for the GMS annual return. This includes clarity around the titles and roles of the nursing team and whether the data refers to WTE or a headcount.

68
There is no information regarding the large percentage relating to nurse practitioners, although these are relatively small in number. Given the increase in the number of nurses undertaking the Advanced Practice MSc course locally and the attractive career path and demand for Advanced Nurse Practitioners in Primary Care, we will be looking to these roles to enhance the number of NPs, to both offset the planned retirements, and support some of the GP deficit within the system. The Primary Care Nursing Practice Development Team are undertaking a baseline nursing assessment with all practices across the HB which will include information relating to contracted hours, age profiles and expected years to retirement. This is due to be completed by May 2016 and will provide better, up to date data on our current nursing workforce and profile in primary care and compliment the data collected for the GMS annual return Action to improve the quality of workforce information is being progressed. The GMS annual return is being clarified and the returned data will be updated and amended for next year to address these issues. The retirement dates are also those known to the GP Practices. This is invariably difficult to predict reliably as it is based on what information is known and is subject to change. This information differs from the data gathered with support from the Local Medical Committee two years ago and the GMS Annual Contract Return will be updated to enable further information to be consistently received. Some of the clusters have recruited staff to assist with the workload and to embrace new ways of working. These are outlined later in this document, and further development of these roles and plans will be supported by the new Workforce and OD project officer which has been created for 8 months to support the primary care workforce development agenda. A key consideration which has been factored within the education commissioning is that the practice nurses are generally recruited from the community nurses working within the local service delivery team which is a constant drain upon their more experienced staff. Medical Appraisal And Revalidation The information relating to GP appraisal and revalidation has been obtained from the ‘MARS’ system and the practice information has been included by the Doctors themselves. This information is cross checked with the General Medical Council and the Medical Performers List. First Cycle Revalidation rates across Hywel Dda is 94.9%.
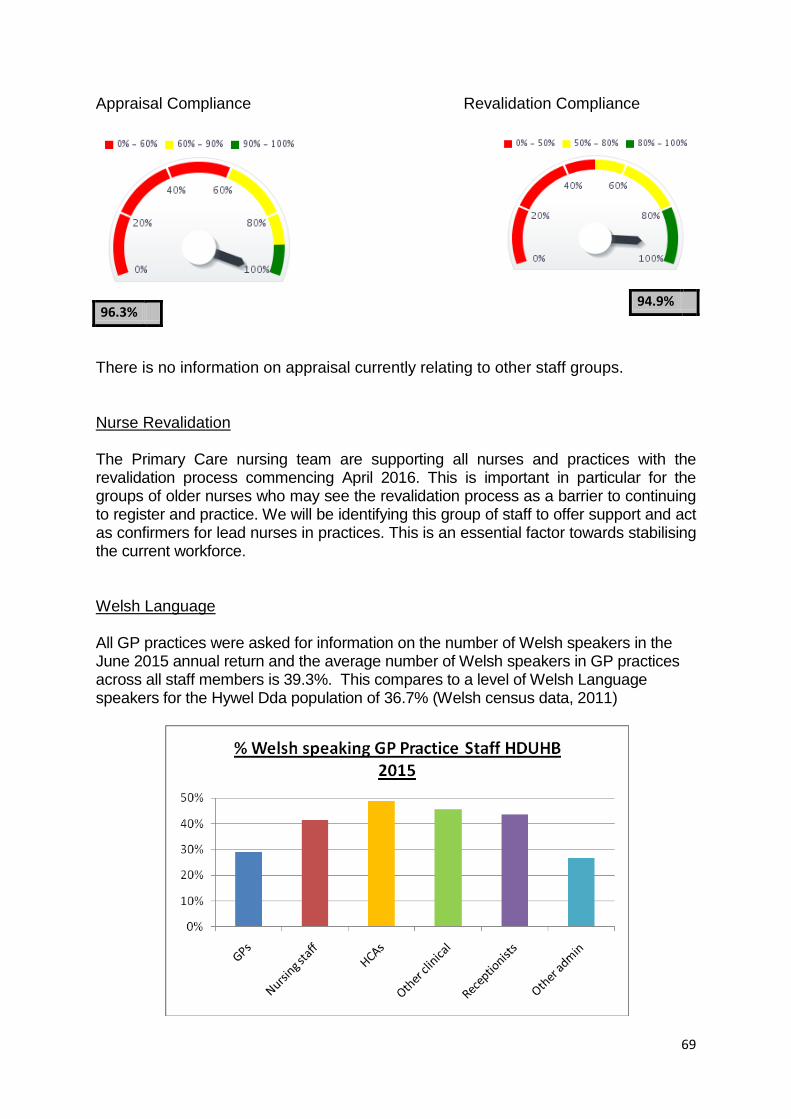
69
Appraisal Compliance Revalidation Compliance
There is no information on appraisal currently relating to other staff groups. Nurse Revalidation The Primary Care nursing team are supporting all nurses and practices with the revalidation process commencing April 2016. This is important in particular for the groups of older nurses who may see the revalidation process as a barrier to continuing to register and practice. We will be identifying this group of staff to offer support and act as confirmers for lead nurses in practices. This is an essential factor towards stabilising the current workforce. Welsh Language All GP practices were asked for information on the number of Welsh speakers in the June 2015 annual return and the average number of Welsh speakers in GP practices across all staff members is 39.3%. This compares to a level of Welsh Language speakers for the Hywel Dda population of 36.7% (Welsh census data, 2011)
94.9% 96.3%

70
The All Wales Data reflects the following
The gender breakdown is 51% female and 49% male
Over 40% of the workforce is over 50 years old, The average leaving age for GPs across Wales is 54 for male and 45 for female. Based on this data, of the 370 GPs identified in the All Wales report, (Hywel Dda information reflects 271 in the GMS return 2015) 44% of male and 45% of female GPs are at or above this leaving age.
Hywel Dda has 6.33 wte GPs per 10,000 head of population (Wales average = 6.5) compared to the highest of 7.38 and lowest of 5.76.
Hywel Dda has the highest number of nurses per 10,000 population at 5.08 (ave=4.04) and the highest percentage of extended role and specialist nurses at 24.6%.
We employ extended role, specialist and advanced nurses to a greater extent than other organisations. It is acknowledged that this may be due to the difficulties in recruiting GPs, so potentially the increased use of nurses could be a method of providing some more capacity in the system. Challenges
Lack of access to/and quality of data
Potential impact of retirements/leavers – GPs/Nurses
Pension changes which may impact on the numbers of staff retiring
Nurse Revalidation
Recruitment to GPs
Shortage of GP trainees
The decrease in GP and Nurse Practitioner (NP) capacity Actions 2015/16 Some of the clusters have recruited staff to assist with the workload and to embrace new ways of working. These are outlined below, and further development of these roles and plans will be supported by the new Workforce and OD role as part of this plan.
South Ceredigion
successfully appointed 2 part time Cluster Frailty and Chronic Disease Pharmacists and 1 WTE Cluster Frailty and Chronic Disease Nurse.
The Cluster Pharmacists commenced in post in the first and second week of November and Cluster Nurse commenced in mid December. Their initial work programmes are concentrating on care homes. Once this work is completed they will be targeting the ‘at risk’ patients as identified in the MSDi software by the practices.
cluster paramedic will also be commencing employment on 14 March 2016 to assist with the nursing home visits and assist GP workload.
71
Taf/Tywi (2Ts)
Generic Technician has been successfully recruited by the cluster. The OT Tech receives direct referrals for assessments. Outcomes from assessments undertaken include: Home exercise plans, utilisation of 3rd sector organisations e.g red cross for wheelchair hire, provision of equipment such as zimmer frames, commodes and grab rails. The majority of these patients are being seen within two weeks (one patient was assessed the day after referral) whereas if they had been referred for assessment via the normal referral route the current waiting time is 13 weeks. Already the post is also positively impacting on the waiting list as patients are now coming off the list as they have been assessed by the Generic Technician.
Amman Gwendraeth
GP Led frailty service – the cluster have attempted to recruit 2 or 3 Part time GPs but have been unsuccessful due to no applicants. One of the cluster practices have offered to provide the service using their GP workforce and this has been combined with the recruitment of an Advanced Nurse Practitioner (Commences in post 7 March 2016)
South Pembrokeshire
Community Heart Failure Nurse - 0.5WTE for the south of the County to improve community cardiac services within South Pembrokeshire.
Cluster Pharmacist – successfully recruited and commences 4 April 2016 to work as part of the GP practices within nursing and residential homes to undertake medication reviews; Prudent Prescribing Principles.
North Pembrokeshire
Paul Sartori Advance Care Planning Nurses - appointment of 1 WTE (2 part-time posts linked to specific practices) Advance Care Planning (ACP) Nurse Facilitators to the Paul Sartori Foundation.
The actions for 2016/17 articulated below assume the following:
A 30% retire and return rate for GP partners into salaried posts (reducing the retirement deficit to 75.25)
A 30% success rate in direct one for one GP recruitment (deficit 46.25)
The remaining 46.25 deficit to be met by a variety of substituted roles utilising a combination of existing and new roles within other professional groups, as well as changes to non medical skill sets (e.g. non medical prescribing)
Not all elements of the GP role (e.g. higher level clinical reasoning and decision making skills) are susceptible to skill mix changes. However enhancing skill mix will have the added benefit of enhancing GP practice by allowing them to focus on higher level practice and wider professional activities, thus increasing job satisfaction

72
The use of other professionals does not, however, provide one for one replacement for GPs, and additionally, some GP time will be required to educate and supervise elements of the GP role that have been delegated.
A dedicated Workforce and OD role will support each cluster in further assessing its workforce needs and linking these to the broader strategy and support that the Health Board can offer to address these. It is important to note that the clusters continue to evolve and the collaboration discussions also support this, the Health Board can at this point only support and provide expertise to assist with workforce planning. Actions 2016/17 All of the actions within the list will be delivered (Q1 and ongoing) as part of ongoing OD programme with Primary Care The core actions will be:
Work with clusters to gather and analyse data to provide robust information to inform workforce and service plans and development – particularly in relation to retirement and turnover.
Working with the clusters to evaluate their service models and consequently workforce models
Provide OD support to clusters and OD skills development
Develop the Primary Care Support Team (as part of the Pacesetter funding) including increasing the GP component of the team by at least 1 per cluster
Development of a ‘pallet’ of new, extended and expanded roles, initially to support the practice support team but to then roll out, work within to build sustainable solutions for specific practices or to provide critical support if required to practices finding themselves in specific difficulties. These roles include advanced practice, prescribing pharmacists and other non-medical prescribers, physician associates
Continue to support clusters to achieve high revalidation and appraisal compliance rates – working with the small number of practices who are not yet at 100%.
Develop Physicians Associates – 2 trainees currently in recruitment via Mid Wales Collaborative. A further 7 are identified for primary care within IMTP – and Swansea University course is anticipated to commence Sept 16.
Aim to recruit 12 nurse practitioners in each year for next 3 years (36 in total)
Support 9 pharmacists to become independent prescribers (1 per cluster plus 2 for the Primary Care Support Team)
Support an additional 4 pharmacists for 2017/18 and 7 during 2018/19 to become independent prescribers.
Increase the number of extended nurse roles – eg nurse prescribers/specialists
Appoint an additional 17 Advanced Practice posts– including non-medical prescribing over the 3 year period to ensure a coverage of 4 Advanced Practitioners per cluster.
Develop 14 practice based pharmacists by 2019.
Review the skills of the HCSW within practices – potential development for Assistant Practice
Return to Practice support for practice nurses
Encouragement of retire and return through salaried options

73
Develop Primary Care ‘nurse bank’ – recruit 12 RNs and 12 HCSW during 2016/17.
Provide OD and Leadership Development Support through existing HD teams and All Wales initiatives
Improve the quality of the data to ensure robust evidence on which to base decisions relating to the primary care workforce.
Clarify and amend the GMS annual return is data to address data issues
Primary Care Nursing Practice Development Team are undertaking a baseline nursing assessment
Develop a model in partnership with WAST to second APs on a rolling programme to Primary Care to enable this work to be carried forward and provide additional support across more practices. It is anticipated that the recruited APs will be released to this programme from February 2016.
Establish a non-acute hospital workforce development group. This will include membership of primary care, community, WAST and third sector to enable cross sector working
Commence Development of 9 PA training roles across each by 2019
Develop and Recruit Advanced Practitioner Roles
Spread the successful models of OT support
Integrate the working of the CMATs service
Increase the Practice Support Team
Develop Pharmacy through the PiP programme developed through Public Health Wales.
core Skills/capacity needs assessment audit
Development of leadership and organisational development capacity
The development of the leadership and OD skills of the workforce will be essential in order to deliver the likely new workforce models in primary care require effective organisational development support and strong leadership skills. While some of this will be supported at a national level, there is a need to ensure that locally, clusters are appropriately supported to develop and implement this. This includes access to the development of facilitation skills to support the clusters in developing their collaborative models. Establishing a wider and more distributed model of leadership will require the development of new career structures, succession planning and talent management. It is not possible to separate the workforce challenges from the rising demand for more complex care closer to home, and the aim is to develop an environment where the patient is seen prudently, at the right time and by the right person, laying the foundation for effective and appropriate use of a broader skill mix. General Workforce Issues In addition to addressing profession specific issues the HB also needs to ensure other key areas are developed. A series of strategies act as enablers to support workforce sustainability and development actions which will work within our workforce assumptions, these include:

74
The 10 year Workforce Plan for Wales is being developed and this will underpin future work streams. Other staff management tools include:- Organisational Change Policy (OCP) is applied to the operational delivery of all service changes impacting upon the workforce. In addition to this a number of policies and strategies exist to support modernisation and these include:
Voluntary Early Release Scheme (VER) - designed to assist staff in taking a personal decision regarding their future employment and enable staff who may wish to leave their employment with NHS Wales to do so with an appropriate compensatory payment. It is a scheme under which an individual employee, in agreement with their employer, chooses to leave employment in return for a severance payment. VER is not a contractual entitlement and is not redundancy.
Deployment Policy - This policy sets out the principles and processes to support the flexible movement of staff between services and teams to support service delivery.
Welsh Language The Health Board takes its responsibility to provide bilingual services to our patients very seriously and to support this has developed and begun to implement its bilingual skills strategy. The first part of the strategy for all service areas was to identify our welsh speakers and below is our progress to date based upon the feedback from our staff. There was 60% return from staff used to collate the data on welsh language skills, 19% of our staff are proficient in using basic Welsh Language skills in the workplace and have achieved level 3 (intermediate), 4(higher) or 5 (proficient).
The Health Board developed in 2014 its national award winning ‘Welsh Language Bi-lingual Skills Strategy’. This strategy is built on four stages:
4980, 36%
3080, 22%
2271, 17%
764, 6%
755, 5%
694, 5% 1167,
9%
HDUHB Welsh Language Competencies as at 31st December 2015
Unknown
0 - No Skills / Dim Sgiliau
1 - Entry/ Mynediad
2 - Foundation / Sylfaen
3 - Intermediate / Canolradd
4 - Higher / Uwch
5 - Proficiency / Hyfedredd
75
1. Identifying local service need through analysis of census data relating to
the Welsh language within the population of Hywel Dda 2. Audits of staff’s current Welsh Language Skills to find out where our
current Welsh speakers are based 3. Identification of the current skills gaps between the population and
workforce Welsh language data. 4. Bridging the gap – ensuring our staff are able to deliver the service bi-
lingually where appropriate. This includes staff confidence and language development opportunities, and assessing vacant posts to establish whether the ability to speak Welsh is essential or desirable.
In addition the Workforce and OD team are currently working with the Welsh Language officers to evaluate the impact of the anticipated implications of the revised measure, and identify actions locally and those better placed to be managed nationally. Actions 2016/17
continue to send out monitoring forms for data collection and input to ESR (Q1 and ongoing)
gain information from social care colleagues and assess potential risks for HB on basis of likely change to standards (Q1 and ongoing)
Identify work which could be supported at a national level
report and identify cost / risks to inform Exec team
The detailed HB OD plan is in section 3 on page 96 Retention
The Health Board continues to work towards being the Employer of Choice not only within the local community, but also to retain existing staff, therefore reducing turnover for non retirement related reasons and in doing so attracting a highly skilled workforce to join the organisation from across the UK. To achieve this there are a range of initiatives currently in place as well as new work to strengthen our position. This includes staff benefits, health and well-being support and thank you events. We are supporting our staff with education and development including leadership development programmes for our medical staff and a consultant mentoring scheme. Good staff health, well-being and sustainable engagement is proven to impact on organisational performance and is therefore vital for ensuring that the Health Board can meet the challenges of delivering comprehensive and consistent high-quality patient care, continuing to improve services within resource and financial restraints, reinforcing and supporting public health promotion and prevention initiatives, attracting and retaining staff. Recognising the importance of retaining current staff and undertaking effective succession planning is key to sustaining our workforce.

76
Actions 2016/17 (Q1 and ongoing)
continue work to publicise good practice and raise the profile of HB using social media and clinical networks to reflect best practices /service developments
establishing a mechanism to follow up all staff appointed a year after induction to get feedback on their experience over their 12 months in the HB to inform local induction, culture, development opportunities etc
Actively inviting experienced staff to retire and return as appropriate to support key work , where identified e.g. supporting mentorship of new starters
Maintain and actively seek to expand staff benefits available to staff
Develop staff to access career pathways
Actively support CPD for all professionals
Encourage innovation and encourage staff to contribute to development of teams and services
The detailed HB OD plan is in section 3 on page 96
Staff Engagement The Health Board recognises that the plan can only be delivered through strong and honest partnerships with staff and their representatives as well as through our engagement with individuals and openness through a variety of communication methods responding to ‘queries and myths’. Partnership working is imperative if we wish to ensure a locality perspective to healthcare delivery. The Health Board works in partnership with Trade Union representatives through the Local Partnership Forum, which is supported by three County-based Partnership Forum Groups and an Organisational Change Sub-Group. There are also three Local Medical Staff Committees and also a Local Negotiating Committee (LNC) which is a specific forum established to discuss and agree policies, and terms and conditions relating to medical staff.
The ‘Hywel Dda Manager’s Standard’ was developed in 2012, which sets out the behaviours expected of all Hywel Dda Managers. A supporting manager’s passport development programme supports managers to achieve the competencies and behaviours required of the manager’s standard and over 400 staff have now completed the programme. Hywel Dda also adopted the Aston ‘Team Based Working’ approach which is an evidence base which demonstrates the clear link between workforce practice (including team working, engagement) and improved patient outcomes. To measure our improvement, and provide evidence on which to develop future actions, we will be taking part in the Medical Engagement Scale survey during spring 2016. It is increasingly recognised that encouraging and facilitating greater medical engagement is crucial to the successful design and sustained delivery of new and changing NHS services. We will also be progressing the NHS Staff Survey during

77
June 2016, and aim to improve our completion rate from 20% for the 2013 survey. Actions 2016/17
support and actively encourage successful returns and local engagement by effectively operationally managing national NHS Staff Survey and the medical Engagement Scale (Q 2)
Strengthen management competence by Increase numbers accessing management passport by 20 places (Q1 and ongoing)
Ensure representation on key developments and workforce working groups
The detailed HB OD plan is in section 3 on page 96 Health & Wellbeing The Health Board has undergone a period of significant change with more to come and this inevitably has an impact on employee well-being and the services and functions in place which are designed to support staff. The challenge lies in managing change in ways which promote and support employee well-being, line managers having the skills and support to effectively manage the human element of change processes and the various support teams having the capacity to provide timely and appropriate advice and support to staff where that is needed. Our on-going workforce challenges are directly related to continuing service developments whilst there remain baseline establishment vacancies within core services. The resultant dilution of core staff across new service areas places them under additional pressure which the UHB is fully aware of and supporting through professional leads and psychological wellbeing initiatives. Increasing work demands and ongoing change processes are known to increase the risk of work related stress, which in turn can lead to increased absenteeism with decreased productivity, increased interpersonal conflict and an impact on the quality of patient care. The challenge is around the ongoing promotion of employee well-being, taking effective systemic measures to prevent and reduce work related stress and having cost effective and evidence based support services in place to address staff well-being issues in a timely way when they do arise. The Health Board recognises that we need to think more broadly about health and well-being. Instead of focusing solely at the level of the individual employee, we will pay attention to the range of complex, inter-related factors that influence individual well-being (such as organisational culture, leadership, environment and engagement). We also will support our staff via a comprehensive occupational health and wellbeing service. We will scope and deliver a number of wellbeing initiatives to promote staff health which includes:-
weight loss support
78
alcohol reduction
exercise programmes
smoking cessation
cardiovascular screening
enhancing wellbeing benefits to allow gym membership and activity days out
We are planning the introduction of multi-professional tele-medicine between our staff and a multi-disciplinary team for more effective consultation and also using technology for 1-2-1. Plan to develop the service to enable ward visits to speak to staff in the workplace. The HB is working to embed Health & Wellbeing within the work based culture of the organisation from planning and decision making, leadership and management style, performance review, change management, work life balance, absence management, physical and mental health emotional intelligence through to the working environment. Platinum Corporate Health Standard Hywel Dda Health Board was the first NHS organisation in Wales to achieve the platinum level of the Corporate Health Standard. Our achievement has been widely recognised, and we are due to revalidate in 2016. This will be against the new standard, and work is currently progressing to ensure that we are able to maintain this prestigious award which demonstrates the excellent work that we do to support our staff in health and well-being, as well as wider in our corporate social responsibility. (Q3) Sickness and Absence Management Historically the Health Board has achieved the WG target and returned rates amongst the very lowest in Wales. Hywel Dda was ‘best in class’ between 2012 to 2014 of all of the larger Health Boards. At the end of the last financial year (2014/15) our performance began to deteriorate. This has largely been due to the severe recruitment difficulties experienced and also the extent of organisational change implemented during this period. The Health Board has recognised the deterioration in rates and are determined that performance will improve in the year ahead. Sickness is very firmly one of the major priorities for all Health Board managers and is measured and monitored regularly at Board and sub Board meetings. The Health Board has also provided additional and dedicated resources to the Workforce team in order to help drive improvement. Early signs are very positive and encouraging. There is increased focus on sickness auditing ie to ensure that managers are adhering to the All Wales policy requirements and also in terms of support, help and training for line managers involved in the process. The Health Board is particularly focussed on improving mental wellbeing and has signed the employer pledge for Time to Change Wales. We will enhance our staff plan and drive improvement via our Workforce & OD Sub Committee and work with
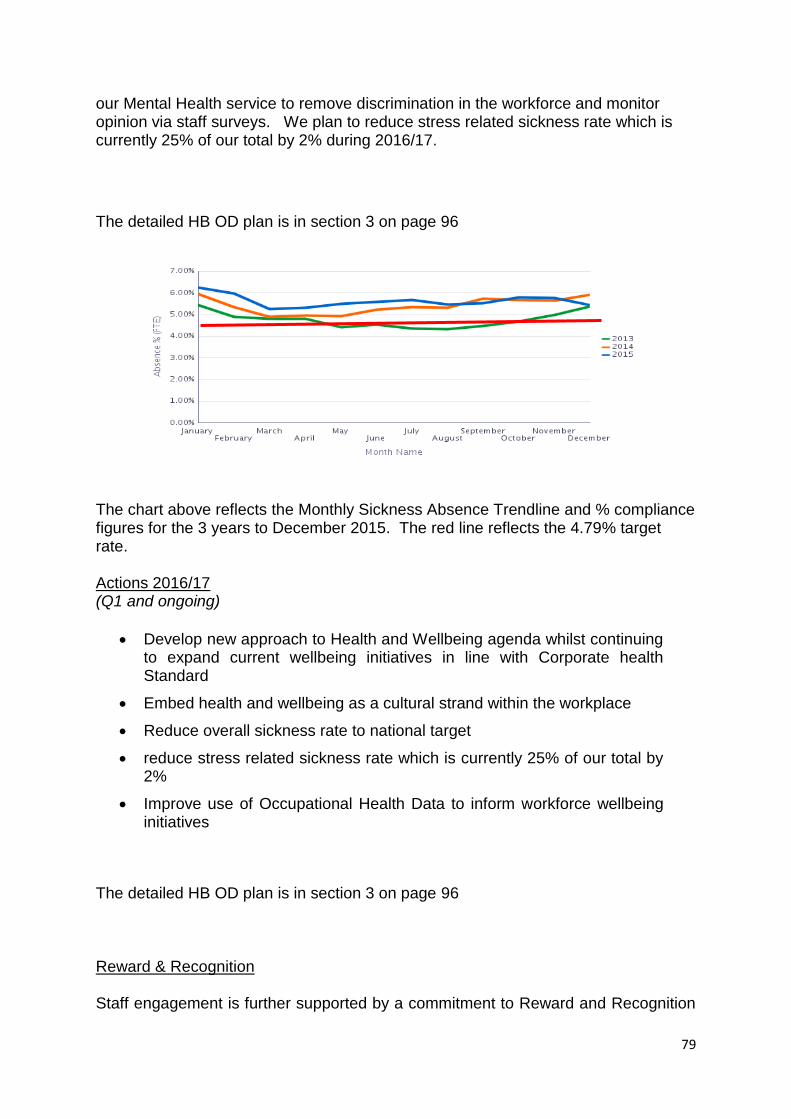
79
our Mental Health service to remove discrimination in the workforce and monitor opinion via staff surveys. We plan to reduce stress related sickness rate which is currently 25% of our total by 2% during 2016/17.
The detailed HB OD plan is in section 3 on page 96
The chart above reflects the Monthly Sickness Absence Trendline and % compliance figures for the 3 years to December 2015. The red line reflects the 4.79% target rate. Actions 2016/17 (Q1 and ongoing)
Develop new approach to Health and Wellbeing agenda whilst continuing to expand current wellbeing initiatives in line with Corporate health Standard
Embed health and wellbeing as a cultural strand within the workplace
Reduce overall sickness rate to national target
reduce stress related sickness rate which is currently 25% of our total by 2%
Improve use of Occupational Health Data to inform workforce wellbeing initiatives
The detailed HB OD plan is in section 3 on page 96 Reward & Recognition Staff engagement is further supported by a commitment to Reward and Recognition

80
through a range initiatives acknowledging that our staff are not only our most important asset, they are our population and our patients and we must develop our commitment to them as much as possible. The Health Board has a well developed and established Staff Benefits Scheme which covers a wide range of benefits including:
Employee of the month to be introduced in 2016
NHS Discounts encompassing entertainment, finance, health, shopping, travel, communication and IT,
access to local fitness clubs,
cycle to work schemes
Technology schemes
Car purchase scheme – first year of the scheme
Leave Purchase Scheme which allows staff to have a greater work life balance.
Our Best of Health Staff Awards is an award scheme to recognise and reward the abundance of innovative and good practice in delivery of health services across the Health Board. It aims to encourage and highlight best practice and support quality initiatives at all levels of the organisation and awards can be won by anyone who has achieved or demonstrated measurable or clearly visible improvements in patient care or service delivery. Nominations are received from individual staff members, teams, directorates, departments and members of the public, patients, carers and service users. All nominations are judged against set criteria by a panel including representation from the Executive Team, Independent Board Members, the Health Board’s Partnership Forum, Hywel Dda Community Health Council and sponsors of the awards. Actions 2016/17 (Q1 and ongoing)
Maintain HB position as best in Wales in terms of the scope and range benefits available to our workforce
maintain and publicise the range of benefits available increase by 2 new schemes within year
The detailed HB OD plan is in section 3 on page 96 NHS Pension Scheme It must be recognised that The NHS Pensions Scheme is still a tremendous advantage to working within the NHS and therefore attractive to our future workforce. The scheme changed in 2015 and introduced new pension arrangements to members. These are:
A Career Average Re-valued Earnings (CARE) scheme, with benefits based on a proportion of pensionable earnings during a career.
An accrual rate of 1/54th of each year’s pensionable earnings with no limit on pensionable service.

81
A normal pension age at which benefits can be claimed without reduction for early payment, linked to the same age as you are entitled to claim your state pension.
Pensions in payment to increase in line with inflation(currently CPI)
During 2016 the HB will be looking to support staff to understand the implications of these changes. Actions 2016/17 (Q1 and ongoing)
Ensure all staff aware of changes to pensions and potential personal impact on retirement plans
Ensure managers use the information on pension changes to inform their workforce analysis in terms of impact
The detailed HB OD plan is in section 3 on page 96 Values & Behaviours
During 2014/15 Hywel Dda University Health Board carried out a large scale exercise to develop its values. Over 3000 staff actively engaged in the process to contribute to the development of values they believe are core to them so that the values are present in all staff and everyone can expect to be treated in accordance with those values. Going forward, all staff will be recruited and trained against these core values. To ensure the Health Board makes a difference and performs to its optimum three Organisational values wrap around the individual values. These being:-
To always put people at the heart of everything we do
To work together, work as one to be the best we can be

82
Strive to deliver & develop excellent services One way in which we aim to achieve this is by developing a core culture where all staff act as if they are the ‘first point of contact’ for our patients or their relatives, using a key strap line to focus attitudes and behaviours:
‘Remember, they could be you or your family’ This will be embedded within all developmental programmes and induction during the year.
Staff, volunteers and any providers working on our behalf are required to work towards the 3 organisational values As previously noted we have begun to introduce values-based recruitment and during 2015 have used values-based exercises as part of our HCSW Bank, Student Nursing, Overseas Nursing and Executive Director recruitment process. Actions 2016/17
Use a communication campaign to ensure the organisational values are embedded across the HB (Q3)
Continue to widen used of values based recruitment practices (Q2)
Embedding the ‘Remember, they could be you or your family’ focussed culture (Q1 and ongoing)
The detailed HB OD plan is in section 3 on page 96 Culture To achieve our organisational vision, we have been developing a culture of engagement, openness and honesty and in which all elements of the workforce are encouraged to be innovative. Central to this is the need for clear and supportive leadership, including robust and empowering clinical leadership and staff engagement. Actions 2016/17
Embed the culture and values within all leadership, management and supervisory development programmes (Q1 and ongoing)
The detailed HB OD plan is in section 3 on page 96
2. OUR COMMUNITIES

83
The Health Board is just part of a wider community and workforce and OD have strong links across the community to support common initiatives.
LIFT The Health Board LIFT Hub Team is based in Llanelli as this is the region within the Health Board geographical spread identified as requiring focussed work. The Health Board has an identified lead on this work who is the link with the local LINK Hub team to plan local strategies. The Health Board team is enhancing and strengthening the work placement infra-structure currently in place to be able to provide prospective LIFT candidates with the widest possible range of placements across our services as possible. The team have developed with service leads a directory of non-clinical work placements across Carmarthenshire primarily in view of the Llanelli focus. This encompasses a range of opportunities including administrative and clerical services, hotel services (cleaning, catering, portering, driving, laundry) and Estates (engineering, carpentry, painting, gardening). We are excluding clinical service based placements currently as the services have huge pressures to support the staff in training posts or needing placements in order to access University programmes. We have received 18 applications of which 14 were offered placements across Portering, Catering, Estates, Medical Electronics and Amman Valley Hospital. 5 withdrew after offer.1 is currently under offer and 3 were assessed as unsuitable at interview. We also held an information session for LIFT eligible individuals at the end of January to raise awareness of the scheme.
Actions 2016/17
Increase placements offered 20-25 during the year
Run 10 additional sessions supporting LIFT candidates with job interview skills or access to programmes available in house.
The detailed HB OD plan is in section 3 on page 96
Work Experience The Health Board has established links with local schools and colleges and is committed to working with them to provide students and any individual interested in working within the NHS, not only with work placement but also with an understanding of the wide range of professions required to support the NHS. The team ensure that they are aware of access to apprenticeships, in house development programmes as we want all our staff to achieve their full potential. In the past year, the Health Board have provided 294 placements across all services. We are increasing our opportunities through working with education providers to ensure we contribute to the education of our local population at each stage of the curriculum.
84
Actions 2016/17
Increase the number of work experience opportunities and schools/colleges liaison both by at least 10% during 2016/17.
(Q1 and ongoing) The detailed HB OD plan is in section 3 on page 96 Volunteers and Volunteering The use of volunteers within the Health care setting can be often overlooked and misunderstood. Volunteers pose tremendous benefits to patients from having someone to sit with them for a chat when they are alone, to helping with nutrition needs. The Health Board currently has over 200 volunteers through our ‘Volunteering for Health’ scheme and will look to widen the scope of use of volunteers acknowledging the value of them to the organization. ‘Volunteering for Health’ recruits volunteers for a variety of roles to support patients and enhance their experience of hospitals within the University Health Board including ward befriending, peer support roles and department ‘meet and greeters’ which are very popular with the local community. In 2015, 24 volunteers went onto paid employment, 10 with Hywel Dda University Health Board. 23 volunteers went onto university, 20 into nursing or medicine. The plan in 2016/17 is to increase the number of volunteers into employment with the HB by 10%. As part of this work the HB will also engage with our current workforce to enable them to explore opportunities to support our communities. This could be via school governors, charity work, carers programme, participation in local volunteering clubs and also by supporting staff volunteering through the Wales for Africa programme. Hywel Dda University Health Board (HDUHB) and Trieste Mental Health Services are working together with the formal signing of the first Mental Health International Twinning Agreement in Wales. Trieste is recognised by the World Health organisation as a centre of excellence for the delivery of mental health services and the MPHG hope to use the twinning agreement as an opportunity to inform a new model care. A core aspect of the Trieste twinning agreement is a staff exchange programme has been agreed between Trieste and Hywel Dda Health Board. At present a total of 3 exchange visits have taken place from Hywel Dda. In November 2014 a total of 8 representatives from Hywel Dda (5 Health Board staff, 2 Local Authority staff and 1 member of Dyfed Powys Police) undertook the first visit to form a senior management perspective on the transferability of services and to make links with management in Trieste. In 2015 expressions of interest were sought for a second exchange visit and a total of 11 HDUHB members of staffs, from a wide range of disciplines, were short listed to take part. Further, 2 carer representatives were also shortlisted by West Wales Action for Mental Health, to be part of the exchange. In December 2015 three from this group had the opportunity to visit Trieste to get firsthand experience of the services and health centre environments, as well as speak to the staff. The visiting staff also attended an international mental health conference occurring in Trieste at the time. A presentation was given by the Health

85
Board staff at the conference on the twinning agreement and the experiences of using learning sets to reflect on and improve practice. The remaining of 10 shortlisted staff and carers visited Trieste in February 2016, for an in depth visit to the services provided and to speak with staff working within these. It is hoped that the knowledge gained on these exchanges will be used to develop and deliver Mental Health service improvement projects within Hywel Dda. Further, a number of Health Board-wide presentations will be undertaken by those involved in the exchange, in order that the learning experiences are widely shared and championed. A second visit for Hywel Dda is currently being planned for October 2016, which will be inclusive of health board staff, carers, service users, police and social care representatives. Expressions of interest will be sought nearer the time. Trieste are planning on visiting Hywel Dda in April and are particularly interested in visiting Older Adult Mental Health and Child and Adolescent services. This visit is currently being planned to coincide with the Learning Sets taking place over the next few months, in order that Trieste staff can contribute within these. Further, the possibilities of a trainee psychiatrist from Trieste undertaking a secondment in HDUHB are currently being pursued. Learning Sets The running of learning sets, in conjunction with Trieste and the International Mental Health Collaborating Network, are also a key aspect of the twinning agreement. The learning sets provide staff and stakeholders in Hywel Dda and Trieste an opportunity to reflect on current practices and ideas for service improvement are encouraged and developed within the meetings.
To date two learning sets have now taken place in Hywel Dda in which a total of 23 health board, local authority, and carer and service user representatives have signed up to be part of. Trieste have been unable to join the learning sets thus far via video link, but are planning on running their Learning Sets in parallel with Hywel Dda. Further, as mentioned above staff exchange visits will be arranged around learning set dates, so as to maximise the opportunities for the sharing of learning and knowledge. Actions 2016/17 (Q1 and ongoing)
plan to increase numbers by 10%
investigate opportunities to use the Trieste model of twinning across other areas
The detailed HB OD plan is in section 3 on page 96 3. OUR FUTURE Developing Our Workforce to Fulfil Current Roles and Prepare for New Roles in The Future

86
The key to our future is the development of a future proof, robust Education Strategy to ensure our staff are supported and developed to undertake their current roles effectively and are ready to embrace new roles for the future. Development of this education strategy will commence during the spring of 2016, when an initial vision will be created to deliver a 21st century approach to bring together a range of partners – both public and private sectors, to develop an innovative approach to education and training, which seeks to:
Develop our local children, young people and the wider population through effective career identification and subsequent planning of development opportunity
Create a menu of opportunities to translate their learning into practical experience regardless of age.
Create opportunities for our staff to link with education providers and create ‘guest lecturer’ opportunities
Work to provide opportunities within streams of work to provide a holistic approach to the subject. This would differ from the traditional way in which healthcare is viewed. For example, a nutrition programme may currently involve sessions being provided by a nutrition nurse or dietician whereas this model would also involve sessions delivered by our chefs and even grounds staff where appropriate.)
Creating a range of innovative career pathways alongside our traditional health care professional routes
Develop the option for portfolio careers to allow our local population excellent career opportunities to allow them to be able to live and work in the area they grew up in if they so wish.
The strategy will bring together the partners to share existing resources including experts and accommodation, so that education is delivered in appropriate environments, that are both attractive to staff and students, to demonstrate Hywel Dda’s commitment to development of it’s workforce – and support our overall aim to be an employer of choice. Alongside all of the above, the Education Strategy will identify the training and development required for all staff at all levels of the organisation and from that will plan training interventions for the next 3 years. Through this we will also define the education investment and revenue budget required to adequately support the required development needs. The Strategy will also link to the Estates strategy as investment in training environments to support modern apprentice training delivery is required. To deliver the UHB’s plans, it is critical that staff are appropriately skilled to enable them to fulfil their current roles and develop to enable them to progress in their roles, and to meet the challenges of future roles. The Learning and Development function co-ordinates all non-medical education and

87
development activity and provides a wide-ranging staff development function to support our service priorities. Internal training and development officers provide a training and specialist advisory service for
Induction
Mandatory training programmes
Clinical Skills and Patient Safety related training programmes
Resuscitation and Simulation Programmes
Health Care Support Worker ‘Skills to Care’ Programmes
Moving and Handling
Prevention and management of violence and aggression
Leadership Development Programmes
Management Development Programmes
Coaching and Mentoring
Where possible these programmes are delivered to a multi disciplinary audience, and utilise a team based working approach to encompass the human factor elements which assist in improving patient safety and outcomes. We have national award winning programmes, and where appropriate, accreditation is available through our registered centre status for Institute of Leadership and Management (ILM) and Agored Cymru. There is a centralised education budget, and a post-registration nursing contract with Swansea University. The co-ordination of all study leave is managed centrally. We have excellent relationships with our partner organisations, and work with other local public service organisations to deliver leadership and management development as well skills training such as dementia, safeguarding and are currently piloting a health and social care worker new role initiative, identifying and delivering the training required. We are rapidly increasing our ability to access development through technology – but again this is dependent on our capability to deliver as well as staff capability to use. We have invested in laptops which are able to be used as ‘library loans’ in wards and departments, to allow staff to complete e-learning where access to computers is difficult. We are also able to provide access to our learning from home. New roles We will continue to develop our extended and advanced roles to support service development and to meet the needs of the population where traditional roles are hard to recruit or require modernisation. Where new and modernised roles are being developed, the required education timescales will need to be included in the plan. This is particularly of note for Assistant Practice, Advanced Practice and Physician Associate roles. A range of initiatives have been noted previously. However, specialists, enhanced roles, extended scope practitioners and advanced and assistant practitioners have a huge role in supporting the HB to modernise workforce models. It is key that staff maximise the use of their knowledge and skills and that we use every opportunity to

88
support staff through career pathways to ‘grow our own’ staff for the future. It is recognised that these posts along with Physicians Associates and new support worker roles will play a key role in supporting new service models within the overarching service model. The Health Board has a robust governance framework (EAGLE) to allow us to develop extended, expanded and new roles in the absence of statutory regulation and issues of concern have been resolved through the introduction of the EAGLE Governance Framework. All new, expanded and extended roles are subject to EAGLE scrutiny process to ensure that the appropriate scope of the role, delegation and accountability arrangements and qualifications/skills and knowledge are identified. The EAGLE governance framework continues to be expanded and meets the requirement of each situation tested in providing a robust system to develop and introduce new roles and expand existing roles. There are 16 Advanced Practice Roles and 13 Assistant Practice Roles registered within the Health Board, all meet the requirements of both the All Wales Advanced Practice Framework and our internal regulation/registration system – the EAGLE Governance Framework. Continuous Innovation and Improvement The Health Board has taken an organisational development approach to improvement, through the delivery of the Improving Quality Together programme. This All-Wales development brings a coherent approach to service and process improvement, utilising a methodology which is designed to empower staff to make changes within their own environment. It starts from the principle that all NHS staff have a duty not only to perform to their job description, but to continuously suggest and make improvements in their working practices and that of their teams. Elements of the IQT programme are included in the consultant leadership programme and our consultant leaders are progressing improvement work as part of the programme, supported by the quality improvement team. Effective Leadership - Developing Leaders and Managers The Health Board recognises that high quality leadership is crucial to the achievement of organisational objectives and to ensure sustainability and future development. The Health Board has a strong commitment to leadership development and acknowledges its role to increase capability of current leaders and develop future leaders. The UHB has worked to achieve this through a number of internal programmes, and access to a range of external programmes including those delivered through Academi Wales, the Kings Fund and Universities. In addition to creating bespoke solutions for individuals, a range of internal offerings support leadership development at all levels. Many of these programmes offer formal accreditation.
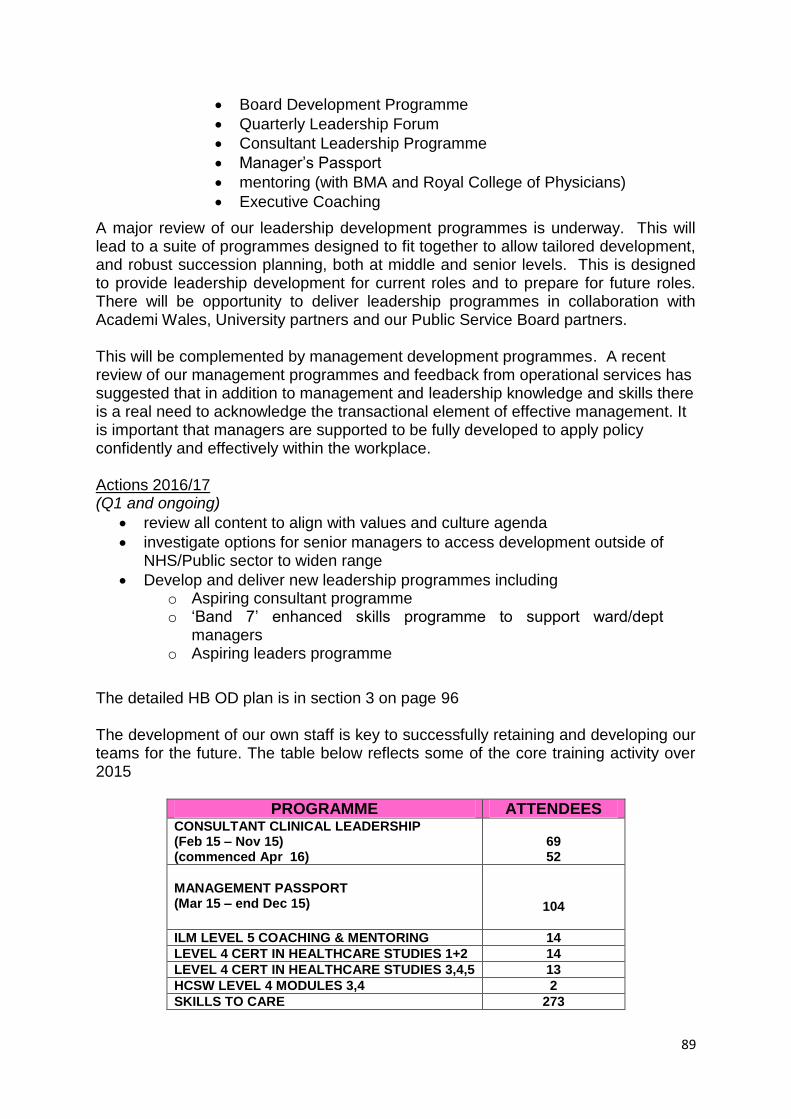
89
Board Development Programme
Quarterly Leadership Forum
Consultant Leadership Programme
Manager’s Passport
mentoring (with BMA and Royal College of Physicians)
Executive Coaching
A major review of our leadership development programmes is underway. This will lead to a suite of programmes designed to fit together to allow tailored development, and robust succession planning, both at middle and senior levels. This is designed to provide leadership development for current roles and to prepare for future roles. There will be opportunity to deliver leadership programmes in collaboration with Academi Wales, University partners and our Public Service Board partners. This will be complemented by management development programmes. A recent review of our management programmes and feedback from operational services has suggested that in addition to management and leadership knowledge and skills there is a real need to acknowledge the transactional element of effective management. It is important that managers are supported to be fully developed to apply policy confidently and effectively within the workplace. Actions 2016/17 (Q1 and ongoing)
review all content to align with values and culture agenda
investigate options for senior managers to access development outside of NHS/Public sector to widen range
Develop and deliver new leadership programmes including o Aspiring consultant programme o ‘Band 7’ enhanced skills programme to support ward/dept
managers o Aspiring leaders programme
The detailed HB OD plan is in section 3 on page 96 The development of our own staff is key to successfully retaining and developing our teams for the future. The table below reflects some of the core training activity over 2015
PROGRAMME ATTENDEES CONSULTANT CLINICAL LEADERSHIP (Feb 15 – Nov 15) (commenced Apr 16)
69 52
MANAGEMENT PASSPORT (Mar 15 – end Dec 15)
104
ILM LEVEL 5 COACHING & MENTORING 14
LEVEL 4 CERT IN HEALTHCARE STUDIES 1+2 14
LEVEL 4 CERT IN HEALTHCARE STUDIES 3,4,5 13
HCSW LEVEL 4 MODULES 3,4 2
SKILLS TO CARE 273

90
(Apr 15 – end Jan 16)
INDUCTION (Apr 15 – end Jan 16)
802
IQT BRONZE (Apr 15 – end Jan 16)
145
HIGHER AWARD/CPD 161
As could be seen earlier staff release to attend training is an ongoing challenge. This includes both the ability to ensure mandatory and essential training is delivered, the additional activity associated with increased numbers through corporate induction as well as ongoing continuing professional and personal development (CPD). Where new and modernised roles are being developed, the required education delivery/attainment timescales are being included in the planning stage. This is particularly of note for Assistant Practice, Advanced Practice and Physician Associate roles. There will also be a requirement for backfill to support development of staff for these posts. We have reviewed all roles with ‘Advanced’ in the title, to ascertain whether some of these can be converted to Advanced Practice roles in line with NHS Wales Advanced Practice Framework, to support service developments and new initiatives with minimal development interventions. There are current challenges relating to the high levels of recruitment of overseas and newly qualified nurses and implications of education commissioning in terms of the student placements and mentorship required. We have assessed the ability to successfully support the mentorship of educational placements of students and have undertaken an analysis of current mentors by department and county in order to map new starters and projected trainees commissioned to identify the risk and plan for development of further current staff as mentors. The Workforce and OD Directorate structure has been reviewed and refined. The new lead for Leadership, Education and Development team has reviewed the current service and developed a plan which aims to re-focus our current programmes to support the core strategic operational priorities, simplify delivery, maximise access and make best use of the resources available to the service. This includes process mapping all activities, realigning them to ensure they are mapped to make best use of staff and the level of skills available and reviewing all job descriptions. Actions 2016/17 (Q1 and ongoing)
improve in mandatory training (UK Core Skills) training compliance to 50% level one compliance by December 2016 and 85% as soon as possible thereafter.
manage the volume of new staff requiring induction and Skills to Care Programmes
review skills to care content to align with frailty agenda
To expand the band 4 development to create opportunities for more staff to access registration through this route across professions not only nursing
Plan deliver the national requirements to deliver the HCSW Framework

91
Develop a new leadership development pathway including succession planning framework at middle and senior levels
Work with Swansea University , Mid and West Wales Collaborative and other partners to develop Physicians Associate roles
Develop 5 further clinical academic roles subject to service plans
Support development of cluster team leads in workforce planning skills
strengthen the workforce and OD specialist role in working with services to consider new/modernised ways of working, specifically:
o Acute service developments o The Mental Health and Learning Disability Plan o Continued work with Community and Integrated services o Building on initiatives in Primary Care – Pharmacists working
within practices to create capacity
The detailed HB OD plan is in section 3 on page 96
The Bevan Commission
Bevan Innovators The Health Board is currently supporting three Bevan Innovator schemes, two Health Board and the third is a shared project with Public Health Wales. These schemes cover patient experience, joint health and social care worker role in a care home and microbiology services. In relation to patient experience, we want to explore whether an Appreciative Inquiry (AI), an ethos that shifts attention away from the traditional problem focus to a strength base approach, can support positive change by focusing on strengths rather than the weaknesses. AI holds at its core the assumption that there is always something that works well in every organisation, we want to identify this and positively encourage more to improve end of life care experiences. We believe all staff come to work to provide good care. We believe AI can help us to explore a nurturing rather than a critical approach to support staff and ensure positive patient and family experiences. The second project has been based on a pilot project in Llanelli. The idea is to transfer healthcare related tasks to social care workers in care homes for older people. There is experience of this in the situation of non-complex wound care (NCWC). Essentially, 10 care home staff were trained in NCWC by the Tissue Viability Nurse (TVN). The trained staff utilised these skills in NCWC through the Agored Cymru accreditation framework. During the course of the project, governance issues were central factors. We utilised the EAGLE framework utilised Hywel Dda’s EAGLE (Excellence, Assurance and Governance in a Learning Environment) Governance Framework, ensuring the project was developed in a safe and effective way. The EAGLE Framework provides assurance to all staff, clients/patients and their families that the care is delivered by
92
competent and confident staff. In July 2015, a rapid evaluation of the project was undertaken. There were several elements to the rapid evaluation, essentially focussing on non-financial and financial benefits. A joint innovator project, looks at using the principles of complexity science, engage multiple audiences, including public, press, politicians and professionals, to gain personal ownership of issues relating to infection prevention and management. Bevan Innovation Hub The Health Board has recently confirmed its intention to host the innovation hub for rural health. This is currently being developed and will progress during 2016/17. Bevan Fellowships Hywel Dda was the first Health Board in Wales to appoint Bevan Clinical Fellows. Three Doctors have been appointed as Clinical Fellows. The Bevan Fellowship programme is a very important initiative which aims to help engage and capture the enthusiasm and commitment of our up and coming clinicians in Wales in addressing the Prudent Healthcare agenda. This as an important means by which we may help to attract and retain leading clinicians into Wales, creating a dynamic learning and innovative climate in which to live and work. We hope to expand this to include the use of Bevan Fellowship as an enabler for the development of a Community Pharmacist Consultant post role to enable the Primary Care Clusters require an optimisation of the services provided by community pharmacy. The roles of community pharmacists are rapidly developing with the services are gaining a greater profile through the optimisation of care to patients requires the key features of a consultant pharmacist role: expert practice, leadership, teaching and research & development. Actions 2016/17
Continue and Strengthen Bevan Fellowship interface
Identify and progress further opportunities for the Bevan Fellowships within Hywel Dda
The detailed HB OD plan is in section 3 on page 96 ARCH We are actively progressing key projects as part of our relationship with ARCH. In relation to workforce development this includes:-
Development of HCSW
Development of Physician’s Associates
Integrated Professional roles
Scientific Careers (including modernising scientific careers)

93
Leadership development
Mid Wales Collaborative The Mid Wales Health Collaborative (MWHC) has been established and a key component of this collaborative is the development of the workforce of mid Wales. This includes the development of
Centre for Excellence in rural healthcare
Development of Physician’s Associates
Future workforce models
Mid and West Wales Regional Workforce Development Group This group’s current primary focus is the delivery of the Social Care and Well-Being Act 2014. Following this initial work, the group’s remit will widen to include more health and social care workforce development and in particular, opportunities for closer working and education. Rural Academic Fellowship Newly-qualified GPs and doctors in training in other specialties will be invited to apply for a Rural Academic Fellowship, based at Swansea University’s College of Medicine. These fellowships will each be three years long. Successful applicants will work as supernumerary GPs or specialists in approved, allocated rural practices or hospitals for 3 days a week. The fellows will complete several different placements in various practices/hospitals during the course of the scheme. We propose to appoint 2 fellows each year, totalling a maximum of 6 fellows on the programme at any one time, once it is fully established. In keeping with retention data from the Cardiff University Academic Fellowships, we would hope that over 50% of the Rural Academic Fellows would remain in rural practice in Wales on completion of the scheme, and that all our fellows would have additional post-graduate qualifications. Fellows’ placements in rural hospitals or practices for the duration of the programme is pivotal to the potential successful retention of the fellows, as it allows time for fellows to explore the common preconceptions and misconceptions in and around living and working in rural Wales. These include questions and concerns about quality of life, travelling distances to and from work, accessibility clincial and diagnostic services, language barriers, rural demographics and clinical skills development. Actions 2016/17

94
Develop the programme to recruit 2 fellows per year, totalling a maximum of 6 fellows on the programme at any one time
The detailed HB OD plan is in section 3 on page 96 University and Further Education links As previously noted within the plan, University status provides the Health Board with research networks/research and development activity, and access to work closely with the academic community to support the delivery of the plan through a range of opportunities to up-skill staff as well as access to an ever growing range of development programmes. A University Partnership Board is in place, and a range of workstreams are associated with it. It acts as a creative hub to drive joint developments and monitor activity to ensure that maximum benefits are delivered for the organisations and for the health and well being of our population. We have very positive relationships with our university and further education providers who deliver much of the education to support our assistant practice and advanced and specialist practice roles. Further links have been made with our university partners, to identify additional opportunities, including offering work placements to students from Trinity St David’s University to provide work experience for their diploma pre-nursing students. We will continue to review training provision by enhancing relationships to make better use of resources available and enabling innovation and modernisation of both individual staff as well as researching and developing new workforce models focused on patient outcomes/care pathways. In order to support delivery the Health Board is working with the University to establish ‘clinical tutor’ roles to support not only the mentorship of the newly registered staff (as the numbers we will be employing may place additional pressure on the current workforce but also any overseas staff to support their professional orientation to the Health Board. Joint Clinical Academic posts are being developed with the appropriate Universities. A Respiratory Chair has been created, and development of a non-medical consultant role is currently being progressed. This will assist in our efforts to attract medical staff to the area. The current excellent partnership with Swansea, Aberystwyth and Trinity St. David’s Universities will be key in terms of the need to be creative in relation to sourcing our initial workforce locally as well as developing our own staff within local environments across the three counties. The opportunities afforded through our involvement in the ARCH project. This will be essential for development of specialist skills and there will be a need for flexibility to support the likely service needs. Where possible the Health Board is aiming to develop bespoke programmes with the Universities to meet the specific local challenges, such as movement of staff who are accustomed to acute based

95
working to a community driven service.
The Health Board is also working with Further Education colleges to strengthen apprenticeships in none core NHS professions e.g. hospitality, media, estates, business studies etc. We will also support our education providers by providing input to course content and delivery.
Future Workforce And Education Commissioning Rationale There are a number of themes emerging from the initial service plans: New working practices with a move to focused 7 day working for some
services/staff groups Development of our current workforce to’ grow our own’, including HCSW staff
supported to access registration programmes and specific focus on Frailty development programmes
The use of expanded/advanced practice roles using modular development Career stage 2-4 Modernising Scientific Careers in Pathology and EBME Need to ensure clinical staff (not solely medical, but all clinical staff groups) are
utilising their knowledge and skills to the maximum in daily applied practice and undertaking appropriate activities and maximise benefits
Focused assessment of specialist roles across all professions Utilising Pharmacists within GP practices to create capacity for GP’s Working more closely with IT specialists to prioritise where IT infrastructure will
be essential to modernising working practice and better use of workforce time Development of Surgical Assistants, Physicians Assistants and Associate roles.
Specialist ODP, Assistant Practitioners, Health and Social Care Support workers
The education commissioning figures have been defined on the basis of the workforce risks within the Health Board associated with the age profile and rurality, service plans and new roles planned as well as the implications of national professional strategies The Health Board will be working to blur the current boundaries between the medical roles within Primary and Secondary care using portfolio GP, Consultants, Physicians Associates and Advanced practice roles, (nursing and therapy) and independent prescribers to develop more imaginative workforce models. In secondary care the Health Board is moving towards a more consultant delivered model in the future with less reliance upon training grades and would be seeking to increase each year within prioritised clinical sub-specialties to support service plans, the details of priorities sub-specialties yet to be defined.. This is a high level assessment as we are currently undertaking the detailed modelling of service provision.
There will be a focus on HCSW development and career pathways, Associate Physicians, Physicians Assistants, Surgical Assistants, Advanced Practitioner and Assistant Practitioner roles along with cross sectoral HCSW development including

96
the Pathology /EBME career stage 2-4 work. The Medical Director has and will continue to actively campaign for medical education to consider training doctors of the future who can attend to the needs of rural populations with general skills as well as aiming to provide excellent training in sub specialist areas. In Nursing the pre registration education commissioning figures will present challenges and an All Wales debate is required in respect of the profession’s ability to support proactively the student placements and impact of mentorship of overseas staff recruited. As an integrated provider, we work with other public services and third sector partners to provide the commissioning figures and also access where appropriate to education and development opportunities. The opportunities to build new roles – some of which cross sectors, utilising a skills based approach become increasingly important. CONCLUSION The plans in 2016/17 as described above and detailed in the OD action Plan below will still present challenges to both Workforce and OD and the operational organisational service delivery teams. Whilst nursing recruitment into baseline vacancy projections suggests that by the 3rd quarter the HB hopes to be in a position of managing turnover, the profession will be under significant pressure supporting increased numbers of students in training, newly registered nurses and overseas nurses whilst delivering services. The medical workforce vacancies and variable pay spend are not easy to resolve and there is a need to review workforce models and challenge historic working practice. The review of baseline therapy workforce is essential if the re-ablement and frailty agenda is to be met thereby better supporting patient flow, reduction of admissions and a more primary and community based service. The organisation will be embedding new values and culture as well as driving change in services, so it will be key to have strong engagement with our staff and a strong sense of understanding the impact of change upon their wellbeing and supporting them through what will clearly be a priority. We hope this gives you a flavour of the work that is being progressed to develop our workforce. The action plan identifies what we will do to deliver this. If you would like to discuss this further please contact. [email protected] [email protected] [email protected]

97
WORKFORCE, EDUCATION & OD PLAN 2016/17 – 2018/19 This action plan covers our employed, contractor and third sector workforce. OUR WORKFORCE
THEME ACTION BY WHO
M
2016/17 2017/ 2018
2018/ 2019
ALIGNED WITH
ORGANISATIONAL
OBJECTIVES
Q1 Q2 Q3 Q4
Values and behaviours
Further develop our behaviours framework to underpin all other work
SODM √ 9
Redesign the PADR / appraisal process to enable a conversation based on values
HOWM
√ 9
Roll out Values Based Recruitment
HOSR √ √ 9
Review induction to ensure its content is appropriate, reflects organisational and personal values and gives all new staff a full understanding of HB core priorities.
HOWM
√ √ √ 9,10
Ensure all staff are offered support throughout workforce management processes and that their wellbeing is considered at all stages.
ADW √ √ √ √ √ √ 9,10
Staff Health and Wellbeing
Reduce stress related sickness absence by 2%
ADW √ 7
Reduce general sickness absence to bring back into line with All Wales target
ADW √ 1, 2, 3, 5, 6, 9, 10
Manage Time to Change Wales employer plan
ADW √ 7
Survey workforce to monitor mental health attitude & experience
ADW √ √ √ 7
Develop & deliver staff health and well being monitoring programme
ADW √ √ √ 1, 2, 3, 5, 6, 9

98
THEME ACTION BY WHO
M
2016/17 2017/ 2018
2018/ 2019
ALIGNED WITH
ORGANISATIONAL
OBJECTIVES
Q1 Q2 Q3 Q4
Revalidate platinum Corporate Health Standard
ADOD √ 9
Develop guidance for managers and staff to deal with managing chronic condition absences.
ADW √ 1, 2, 3, 4, 5, 6, 7, 8, 9
Develop staff engagement dashboard to include wellbeing measures
SODM √ 1, 2, 3, 4, 5, 6, 7, 8, 9
Draft of Self Care and Wellbeing at Work
ADW √ 1
Culture Carry out 10 pulse surveys and 10 follow up surveys per year to assess management competence and staff engagement.
HOWM
√ √ √ √ 9, 10
Deliver the All Wales Staff Survey and achieve a 5% increase on previous completion rate
HOWM
√ 9, 10
Deliver the medical engagement scale survey tool
HOWM/MD
√ 9, 10
Develop action plans to address findings from national and pulse surveys and monitor progress
HOWM
√ 9, 10
Encourage staff feedback HOWM
√ √ √ √ √ √ 9, 10
Hear 1 staff story per quarter at W&OD Sub Committee
ADOD/ADW
√ √ √ √ √ √ 9
Staff Experience
Continue to provide and enhance Staff benefits schemes by 2 per year
SODM √ √ √ √ √ 9,10
Support staff to undertake volunteering within our local communities
ADW √ √ √ √ 9, 10
Performance Management
support managers to introduce PADR
ADW √ √ √ √ √ √ 9,10
Manage pay progression in line with new policy
HWM √ √ √ √ √ 9,10
Develop new PADR template to include core objectives for all.
HWM √ 9,10
Improve our PADR compliance to maintain 85% recorded on ESR
HWM √ √ √ √ 9,10
Maintain medical appraisal compliance
HOWM
√ √ √ √ √ √ 9,10

99
THEME ACTION BY WHO
M
2016/17 2017/ 2018
2018/ 2019
ALIGNED WITH
ORGANISATIONAL
OBJECTIVES
Q1 Q2 Q3 Q4
>90%
Develop new ways to deliver mandatory training across HB to achieve 50% compliance by Q3 16 and 85% as soon as possible thereafter including career medical workforce
√ √ √ √ √ 9,10
Staff Development
Manage delivery of the All Wales HCSW Careers framework
HWM √ √ √ √ 9, 10
Undertake establishment reviews within therapy services
ADOD √ √ √ √ √
Review recruitment training to support the roll out of values based recruitment
ADOD √ √ √ √ √ √ 9,10
Develop and further enhance clinical skills programmes including focus on frailty/dementia
ADOD √ √ √ √ 8,9,10
Develop cross sector training programmes
HSCS √ √ √ √ √ 9,10
Develop rotation programme for nurses in workplaces aligned to University education
HWM √ √ √ √ 9,10
Recruitment
Recruit to baseline establishment levels in accordance with individual health professional plans
ADOD √ √ √ √ √ √ 9, 10
Where appropriate and suitable support retire and return applications
ADOD √ √ √ √ 9,10
Manage overseas recruitment programme for nursing posts
ADOD √ √ √ √ √ √ 9,10
develop innovative recruitment solutions as appropriate
ADOD √ √ √ √ √ √ 9,10
Ensure induction programme support new recruits identified in recruitment plan
ADOD √ 9,10
Continue to simplify transactional processes for recruitment
ADOD √
9,10
Variable Pay Reduction
Initiate project
D W&OD
√
9,10
Develop workstreams to reduce and where
ADW/ADOD
√
9,10
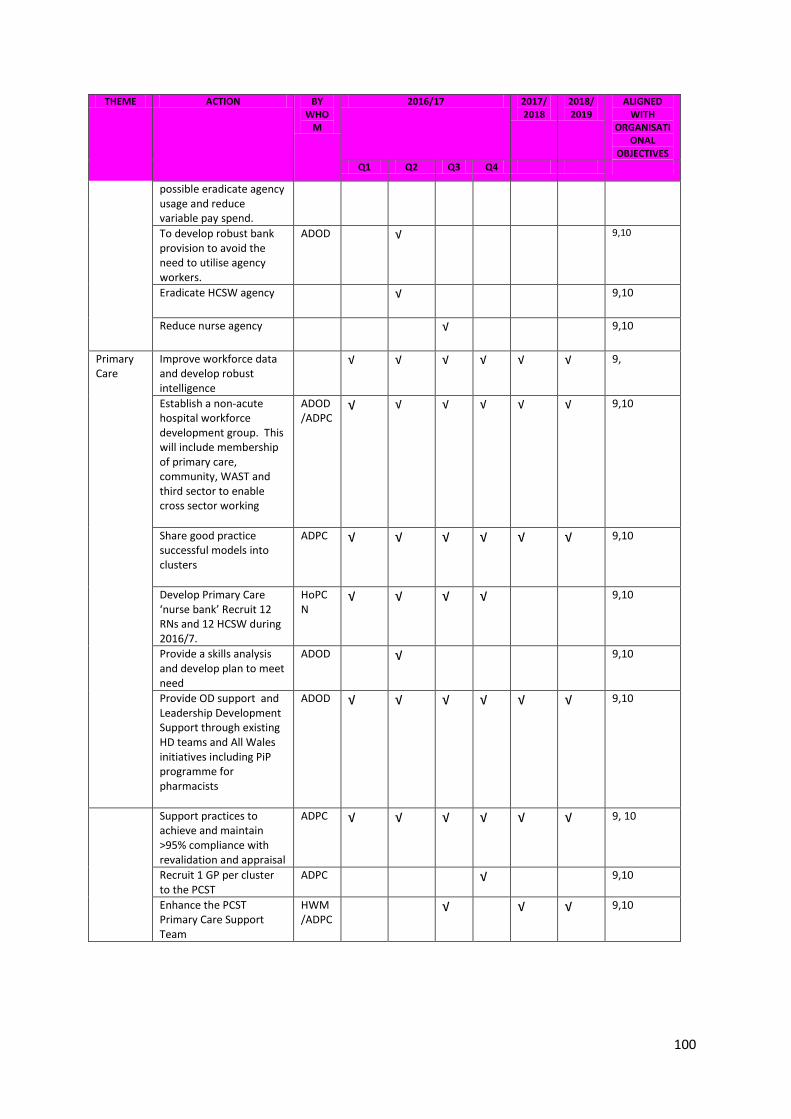
100
THEME ACTION BY WHO
M
2016/17 2017/ 2018
2018/ 2019
ALIGNED WITH
ORGANISATIONAL
OBJECTIVES
Q1 Q2 Q3 Q4
possible eradicate agency usage and reduce variable pay spend.
To develop robust bank provision to avoid the need to utilise agency workers.
ADOD √ 9,10
Eradicate HCSW agency √
9,10
Reduce nurse agency √
9,10
Primary Care
Improve workforce data and develop robust intelligence
√ √ √ √ √ √ 9,
Establish a non-acute hospital workforce development group. This will include membership of primary care, community, WAST and third sector to enable cross sector working
ADOD/ADPC
√ √ √ √ √ √ 9,10
Share good practice successful models into clusters
ADPC √ √ √ √ √ √ 9,10
Develop Primary Care ‘nurse bank’ Recruit 12 RNs and 12 HCSW during 2016/7.
HoPCN
√ √ √ √ 9,10
Provide a skills analysis and develop plan to meet need
ADOD √ 9,10
Provide OD support and Leadership Development Support through existing HD teams and All Wales initiatives including PiP programme for pharmacists
ADOD √ √ √ √ √ √ 9,10
Support practices to achieve and maintain >95% compliance with revalidation and appraisal
ADPC √ √ √ √ √ √ 9, 10
Recruit 1 GP per cluster to the PCST
ADPC √ 9,10
Enhance the PCST Primary Care Support Team
HWM/ADPC
√ √ √ 9,10

101
OUR COMMUNITIES (includes actions identified in workforce section above)
THEME ACTION BY WHOM
2016/17 2017/ 2018
2018/ 2019
ALIGNED WITH
ORGANISATIONAL
OBJECTIVES
Q1 Q2 Q3 Q4
Future Workforce
Recruit 20 additional volunteers per year
√ 9,10
Increase LIFT placements offered to 20 – 25. Run 10 additional sessions supporting LIIFT candidates with job interview skills
√ √ √ 9,10
Develop links with local FE institutions and Universities to provide development opportunities in partnership
√ 9,10
Increase work experience opportunities by 10% and support to secondary schools & further education institutions throughout the 3 counties.
√ √ √ √ √ √ 9,10
OUR FUTURE (includes actions identified in workforce section above)
THEME ACTION BY WHOM
2016/17 2017/ 2018
2018/ 2019
ALIGNED WITH
ORGANISATIONAL
OBJECTIVES
Q1 Q2 Q3 Q4
Organisational Change
Develop a robust and consistent approach to considering service integration, which will challenge norms and overcome barriers
ADW √ √ √ √ √ √ 9, 10
Developing new workforce models
Create an Advanced, Extended and new roles at all levels
ADOD √ √ √ √ √ 1 to 10
Extend opportunities for HCSW Band 4 Career Pathway (nursing , therapy, Pathology,EMBE)

102
THEME ACTION BY WHOM
2016/17 2017/ 2018
2018/ 2019
ALIGNED WITH
ORGANISATIONAL
OBJECTIVES
Q1 Q2 Q3 Q4
Investigate potential opportunities to work with University partners and FE Colleges to develop employment and career pathways
ADOD √ √ 1 to 10
Continue work to develop 7 day working across services
√ √ √ √ √
Develop new and innovative roles in primary care
ADPC √ √ √ √ √ √ 1 to 10
Equality Agenda
Implement bilingual skills strategy with all workforce.
HOWM √ √ √ √ 9, 10
Undertake annual equality report for workforce
HOWM √ √ √ 10
Take full and participator roles within ARCH, Bevan, Mid Wales Collaborative, Mid Wales Regional Workforce Development and University Partners
ADOD √ √ √ √ √ √ 9, 10
Collaboration Introduce 3 more clinical fellows
ADOD √ 9, 10
Bevan Commission
Oversee implementation of Bevan innovators
ADOD √ 9
Establish rural health hub
ADOD √ 9
Leadership
Improve succession planning/talent management strategies
HWM √ √ √ √ 1,9,10
Scope out and cost implications of current skills gap
ADOD √ √ √ √ √ 9, 10
Refine leadership programmes
HWM √ 9, 10
Expand managers passport and increase capacity by 20 managers/supervisors each year
HWM √ √ √ √ √ √ 9, 10
Develop and ADOD √ √ √ √ √ √ 9, 10

103
THEME ACTION BY WHOM
2016/17 2017/ 2018
2018/ 2019
ALIGNED WITH
ORGANISATIONAL
OBJECTIVES
Q1 Q2 Q3 Q4
implement clinical leadership programmes
Support 8 staff to attend Academi Wales Summer School
ADOD √ 9, 10
Developing our leaders and managers
Deliver Consultant Leadership Programme
ADOD √ √ √ 9, 10
Deliver 10 management passport (200 staff) programmes per year to
HWM √ √ √ √ √ √ 9,10
Develop and deliver an ‘aspiring consultant’ programme for middle grades and locums for 20 staff (each)
ADOD √ √ 9,
Develop and deliver a ‘Band 7’ programme to support 40 clinical leaders
ADOD √ √ √ 9
Develop and deliver bespoke team improvement programme (2 per year x 50 spaces)
ADOD √ √ √ √ 9
Developing a Coaching Culture
Provide access to coaching for senior staff collaboration with other public sector partners
HWM √ √ √ √ √ √ 9
Develop a coaching network within Hywel Dda
HWM √ √ √ 9
Train 20 staff at level 5 coaching
HWM √ √ 9
Train 2 staff per year at level 7 coaching (executive coaching)
ADOD √ √ 9
Mentoring Scheme
Create 15 consultant Mentors per year
ADOD √ √ √ 9
Strengthen the newly created peer support network for consultant mentors
ADOD √ √ 9
Increase number of nurse mentors to support NQN and
ADOD √ √ √ 9,10

104
THEME ACTION BY WHOM
2016/17 2017/ 2018
2018/ 2019
ALIGNED WITH
ORGANISATIONAL
OBJECTIVES
Q1 Q2 Q3 Q4
overseas recruitment
Develop a non-medical mentoring scheme
ADOD √ 9,10
Skills development
Develop a robust Education Strategy to encompass all education and training
ADOD √ 9, 10
Offer apprenticeship training programmes to all staff who fall within the 18-25 age range
ADOD √ 9, 10
Deliver 5 apprenticeship places in estates/hotel facilities areas
ADE&F √ 9, 10
Deliver psychological well being programmes to 100 staff (eg ‘you matter development programme).
HPWB √ √ √ √ √ √ 7
Develop and deliver “Great customer experience” training
HWM √ 9, 10
Develop a robust education strategy to link with our UHB Partners, ARCH, Local Schools and Colleges
√ 9,10


















