In-stent restenosis with Drug eluting stent, on going research

of 5
8/19/2019 Willingness to Pay to Eliminate the Risk of Restenosis
1/8
1941-7713American Heart Association. All rights reserved. Print ISSN: 1941-7705. Online ISSN:2011Copyright ©
Greenville Avenue, Dallas, TX 72514Circulation: Cardiovascular Quality and Outcomes is published by the American Heart Association. 7272
DOI: 10.1161/CIRCOUTCOMES.109.9154212010;
2011;4;46-52; originally published online December 14,Circ Cardiovasc Qual Outcomes
Jacques LeLorier, James M. Brophy and Stéphane RinfretJason R. Guertin, Aihua Liu, Michal Abrahamowicz, David J. Cohen, Salma Ismail,
Coronary Intervention : A Contingent ValuationWillingness To Pay To Eliminate the Risk of Restenosis Following Percutaneous
http://circoutcomes.ahajournals.org/content/4/1/46.fullon the World Wide Web at:
The online version of this article, along with updated information and services, is located
http://www.lww.com/reprintsReprints: Information about reprints can be found online at
[email protected]. E-mail:Health, 351 West Camden Street, Baltimore, MD 21201-2436. Phone: 410-528-4050. Fax:Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters Kluwer http://circoutcomes.ahajournals.org/site/subscriptions/ online atSubscriptions: Information about subscribing to Circulation: Cardiovascular Quality and Outcomes is
by guest on January 20, 2011circoutcomes.ahajournals.orgDownloaded from
http://circoutcomes.ahajournals.org/content/4/1/46.fullhttp://circoutcomes.ahajournals.org/content/4/1/46.fullhttp://www.lww.com/reprintshttp://www.lww.com/reprintsmailto:[email protected]:[email protected]://circoutcomes.ahajournals.org/site/subscriptions/http://circoutcomes.ahajournals.org/site/subscriptions/http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/http://www.lww.com/reprintsmailto:[email protected]://circoutcomes.ahajournals.org/site/subscriptions/http://circoutcomes.ahajournals.org/content/4/1/46.full
8/19/2019 Willingness to Pay to Eliminate the Risk of Restenosis
2/8
Willingness To Pay To Eliminate the Risk of RestenosisFollowing Percutaneous Coronary Intervention
A Contingent Valuation
Jason R. Guertin, MSc; Aihua Liu, MSc; Michal Abrahamowicz, PhD;David J. Cohen, MD, MSc; Salma Ismail, MSc; Jacques LeLorier, MD, PhD;
James M. Brophy, MD, PhD; Stéphane Rinfret, MD, SM
Background —Percutaneous coronary intervention (PCI) remains limited by the risk of restenosis. Patients’ perceptions of
the health benefits and value of avoiding restenosis are incompletely known.
Methods and Results—We used a contingent valuation approach to assess the willingness to pay (WTP) for a hypothetical
treatment that eliminates the risk of restenosis among 270 PCI patients. Patients were provided with a scenario
describing a baseline 10% or 20% probability of restenosis in the year following the procedure, which could lead to
repeat PCI or, more rarely, bypass surgery, without any increase in mortality. Six different “take it or leave it” bids
($500, $1000, $1500, $2000, $2500, and $3000) and both risk levels were randomly assigned. Multiple logistic
regression was used to identify independent predictors of a positive response to the WTP question. Using nonparametricmethods, the median WTP to eliminate the risk of restenosis was estimated at $2802. As expected, higher income was
independently associated with a higher probability of a positive response to the WTP question (odds ratio, 2.81; 95%
CI, 1.32 to 5.97). Bids also were independently associated with the probability of being willing to pay, and this
association followed a quadratic effect. Below $1500, bid had little impact on patient answers. However, as prices
increased, the probability of being willing to pay started to decrease sharply.
Conclusion—The potential to eliminate the risk of restenosis, a benign complication, would have substantial value for
patients undergoing PCI. (Circ Cardiovasc Qual Outcomes. 2011;4:46-52.)
Key Words: restenosis stents cost-benefit analysis
Percutaneous coronary intervention (PCI) with stent implan-
tation effectively reduces angina in patients with coronary
artery disease.1 However, benefits of PCI remain limited in the
following year by restenosis, a nonfatal and relatively benign
complication that nevertheless can lead to recurrent symptoms,
repeat revascularization (RR) procedures,2,3 and a decrease in
quality of life (QOL).4 Drug-eluting stents (DES) reduce the risk
of restenosis and subsequent RR procedures by 50% to 75%
compared to bare-metal stents (BMS).5 Despite their efficacy,
there still is debate about whether the increased effectiveness of
DES compared with BMS justifies their incremental cost.6,7
Editorial see p 9
The contingent valuation approach assesses, in monetaryvalues, all benefits associated with a preferred health state. This
goal may be achieved by asking how much money an individual
would trade to avoid a given decrement in health in a hypothet-
ical market and then determining his or her maximum willing-
ness to pay (WTP) for avoiding this detrimental condition.8 By
doing so, the contingent valuation quantifies, through a single or
a series of questions, all of the benefits arising from avoiding a
detrimental health condition, whether they are gains in leisure or
work time, reduction in pain levels, or any other benefit that may
be achieved by avoiding the detrimental health condition. Al-
though this method may overestimate the value of examined
goods,9 assessing patients’ WTP for a treatment that provides a
preferred condition can produce additional information on the
impact a condition can have on patient well-being. Contingent
valuation is of particular interest for understanding treatments
that reduce restenosis because the clinical consequences of
restenosis generally are short lived.10
The goal of this projectwas to use this technique to measure how much Canadian
patients value treatments that could eliminate restenosis
post-PCI.
Received March 25, 2010; accepted September 13, 2010.From the Université de Montréal (J.R.G., J.L.); Centre Hospitalier de l’Université de Montréal Research Centre (J.R.G., S.I., J.L., S.R.); Department
of Epidemiology, Biostatistics and Occupational Health (A.L., M.A., J.M.B.), McGill University; and Division of Clinical Epidemiology (A.L., M.A.,J.M.B.) and Division of Cardiology (J.M.B.), McGill University Health Centre, Montreal, Canada; Saint Luke’s Mid America Heart Institute (D.J.C.),Kansas City, Mo; and Institut universitaire de cardiologie et de pneumologie de Québec (S.R.), Quebec City, Canada.
Guest Editor for this article was Brahmajee K. Nallamothu, MD.Correspondence to Stéphane Rinfret, MD, SM, Clinical and Interventional Cardiology, Multidisciplinary Cardiology Department, Institut universitaire
de cardiologie et de pneumologie de Québec 2725, Chemin Ste-Foy, Quebec City, Quebec G1V 4G5, Canada. E-mail [email protected]
© 2011 American Heart Association, Inc.Circ Cardiovasc Qual Outcomes is available at http://circoutcomes.ahajournals.org DOI: 10.1161/CIRCOUTCOMES.109.915421
46 by guest on January 20, 2011circoutcomes.ahajournals.orgDownloaded from
http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/
8/19/2019 Willingness to Pay to Eliminate the Risk of Restenosis
3/8
WHAT IS KNOWN
● Restenosis occurs in 15% of patients undergoingpercutaneous coronary intervention (PCI) with bare-metal stents.
● In a previous contingent valuation study in the United
States, patients presented with a 30% risk of restenosisfollowing PCI were willing to pay median amounts of $273, $366, and $1162 for a 10%, 20%, and 30%reduction in the risk of restenosis, respectively.
WHAT THIS STUDY ADDS
● Our study shows that patients in a public healthcaresystem would be willing to pay a median amount of $CAN 2802 for a procedure that would eliminate therisk of restenosis following PCI.
● Our study also identified that before undergoingcardiac catheterization followed by ad hoc PCI,
90.7% of patients believed that PCI could prolongtheir life span, and 92.2% of patients believed that itcould improve their quality of life.
Methods
Patient PopulationBetween November 18, 2005, and March 7, 2008, all patientsundergoing cardiac catheterization with ad hoc PCI at the CentreHospitalier de l’Université de Montréal were approached to partici-pate in the study. The only exclusion criteria were (1) patient refusal,(2) any clinical situation that does not safely allow the administrationof the questionnaire before the catheterization, and (3) inability tounderstand French or English. The study protocol was approved by
the hospital’s Scientific and Ethical Research Committees, and allpatients provided written informed consent.
Data CollectionImmediately before the planned cardiac catheterization, trainedinvestigators administered an in-person questionnaire to collectsocioeconomic data, WTP, and health-related QOL assessments.Clinical data were extracted from patients’ hospital charts. Thequestionnaire also included questions regarding patients’ perspectiveon PCI.
WTP AssessmentWe used the contingent valuation method to assess patients’ WTP fora hypothetical treatment that would eliminate the risk of restenosis(and subsequent RR) in the year following a PCI. The question was
asked following an ex post perspective. In other words, the questionwas given to patients who require or may directly benefit from theproposed program.11 We used a closed-ended dichotomous formatquestion to assess the patients’ WTP for the proposed program.12,13
With this method, patients were provided a single dichotomous “takeit or leave it” (ie, yes or no) question that asked whether they wouldbe willing to pay a proposed amount for the treatment or interventionbeing evaluated.
To assess the monetary value of a treatment that would eliminatethe risk of restenosis in the year after a PCI, each patient was askedbefore their planned cardiac catheterization the following question:
“If you undergo an angioplasty or stent procedure today,
there is a risk that the blockage in the artery will come back
in the next 6 to 12 months, a complication called restenosis,
which could lead to recurrent chest pains (or other symp-toms). Restenosis does not put your life in danger but could
result in 1 or more revascularization procedure(s) in the
future. Those procedures could be another angioplasty,
implantation of a stent, or, in rare cases, coronary artery
bypass surgery. The risk of restenosis is around X%. Let us
suppose the existence of a new treatment that reduces this
risk to 0%. Would you be willing to pay $Y for this new and
improved treatment? 1) Yes 2) No.”
Each patient was randomly assigned a single price (Y) of $500,$1000, $1500, $2000, $2500, or $3000. The price range was decidedbased on current incremental cost of DES compared to BMS, whichwas between $1500 and $2000 in most Canadian hospitals. Theinvestigators explained to the patients that in order to obtain this newtreatment, they would be required to pay out of pocket the proposedamount before the intervention. To test whether WTP would increasewith the magnitude in baseline risk, patients were randomly assignedto 1 of 2 alternative risks of restenosis (X): 10% or 20%. Thecombination of 6 different prices and 2 baseline risk values resultedin 12 alternative scenarios distributed with equal probabilities amongthe patients. To mitigate the hypothetical bias, the fact that somepatients are willing to say yes within a hypothetical context but areunwilling when presented with a real context, we added a secondWTP question in order to validate the response to the first question.9
If the patient answered yes to the proposed bid, the amount wasincreased by $500, and the patient was asked again whether he or shewould be still be willing to pay. In the event that patients refused toanswer the WTP scenario questions or gave an “I don’t know”response, they were considered to reject the proposed amount (ie,were assigned the no response). Although no consensus exists,Blumenschein et al9 suggested adding an “are you sure” question asa means to validate the patient’s answer. Adding a second WTP wasbelieved to increase patients’ reflection time on the initial questionby focusing on the economic value of avoiding restenosis. Thelowest proposed amount ($500) was selected because it was repre-sentative of the selected range of bids while remaining a marginalincrease compared to initial proposed amounts.
QOL Assessment
To assess a possible relationship between QOL and WTP, patientsalso were asked to provide mental health status information using theSymptom Checklist-90-R (SCL-90-R)14 and QOL information usingthe 36-item Medical Outcome Study Short-Form Health Survey(SF-36) questionnaire.15
Statistical AnalysesContinuous variables are described as meanSD and categoricalvariables by frequencies. Nonnormally distributed continuous vari-ables were compared with the Wilcoxon rank sum test.
To estimate the median WTP, we used the nonparametric methodproposed by Kriström.16 Assuming that the probabilities of WTPcorresponding to each bid increase monotonically with decreasingprice, a linear interpolation should provide a reasonably accurateapproximation to the true relationship. Thus, the median WTP can be
estimated as the bid at which the probability of a positive response,estimated from the linear model, is 50%. If the observed proportionsof positive responses did not follow a monotone curve, this wasinterpreted as due to sampling error or too-small increases betweenthe adjacent bids. In that case, the probabilities were recalculated bycombining the adjacent bids until all the probabilities followed amonotone sequence, and the median was reestimated using thecombined bids.
The responses to the WTP question were assessed by 2 ap-proaches. In the first approach, only the first amount assigned wasconsidered. The second, more conservative approach was used toavoid overestimation of the true WTP.17 In that approach, a patientwas considered as willing to pay the first amount only if he or shealso agreed to pay $500 more than the originally assigned price. Thissecond amount was not used when estimating the median WTP.
We used multiple logistic regression to identify patient character-istics independently associated with a higher probability of respond-
Guertin et al Willingness To Pay To Eliminate Restenosis 47
by guest on January 20, 2011circoutcomes.ahajournals.orgDownloaded from
http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/
8/19/2019 Willingness to Pay to Eliminate the Risk of Restenosis
4/8
ing by the affirmative to the WTP question. Separate analyses wereperformed for each of the 2 approaches discussed previously. Price,risk of restenosis, patient income, history of PCI, history of myo-cardial infarction (MI), and history of coronary arterial bypass graft(CABG) surgery were hypothesized a priori to influence the patients’answers to the WTP question and, therefore, were forced into themodel regardless of their statistical significance. We then usedforward and backward model selection procedures in separate
analyses to identify additional statistically significant (P0.05)determinants of the responses to the WTP question among thefollowing variables: age, sex, education, working status, chronicheart failure, history of MI, history of CABG surgery, somatizationscore, depression score, anxiety score, SF-36 mental componentscore (MCS), and SF-36 physical component score (PCS).
To investigate how increasing price affects the patients’ responsesto the WTP questions, we considered 4 alternative models for theeffect of price. All 4 models adjusted for the same a priori-selectedcovariates but represented the effect of price differently. Specifically,the models represented the effect of price using the followingfunctions: linear (model 1), logarithmic (model 2), 2-term quadraticfunction with separate linear and quadratic terms (model 3), andrestricted 1-term quadratic function without the linear term (model4). In the quadratic models, original prices were transformed to price
increment, calculated as price
$500 (ie, centered to have 0 value atthe minimum price of $500 considered in our study). In model 3, wetested the quadratic component for the nonlinearity of the effect of price. Model 4 restricts the estimated quadratic function to have themaximum value at a price of $500, which ensures a monotonicallydecreasing effect of price. In contrast, model 3 may yield anonmonotone effect of price, which would be considered clinicallyimplausible and likely to reflect overfitting. In addition, we tested thesignificance of the linear term in model 3. The lack of significanceof the linear term (P0.05) was interpreted as the evidence that themonotone effect of price, estimated in model 4, provided equallygood fit to data as the more complex, and possibly nonmonotone,function estimated in model 3. We then used the Akaike informationcriterion (AIC),18 which accounts for the difference in each model’sdegrees of freedom, to determine the best fitting among the 4alternative models.
A 2-tailed P0.05 for the Wald test was considered statisticallysignificant for all tests. Analyses were performed using SAS version9.1.3 (SAS Institute; Cary, NC) statistical software.
Results
Patient SampleA total of 312 patients were approached to participate in our
study. Of these, 270 (87%) completed both parts of the WTP
questionnaire and were included in our analysis. Three
patients gave protest answers (eg, patients refused to answer
the WTP question due to ideological convictions), and 7
patients responded with an “I don’t know” answer; all were
assumed to have given a negative response to the WTP offer.Socioeconomic and clinical characteristics of the study pop-
ulation are presented in Table 1.
Patient Perceptions on the Role of PCIThe majority of patients initially believed that PCI could
prolong their life span and improve their QOL (90.7% and
92.2%, respectively).
WTPMost (68.9%) patients were willing to pay the amount
proposed in the first question. Among those who were willing
to pay the first amount, the majority (85.9%) also were
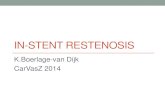
willing to pay $500 more. Therefore, 59.2% of study patientswere willing to pay both proposed amounts. Figure 1 shows
the percentage of patients who gave a positive response to theWTP questions as a function of the price being asked.
Because 50% of the patients responded positively to the
$3000 price, we can assume that the median WTP amount,
using only the response to the first question, is at least $3000.
Based on linear extrapolation, the median WTP was esti-
Table 1. Demographic Characteristics of the Study Population
Variable Total
Age, y (meanSD) 64.110.9
Male sex 198 (73.3)
Marital status
Married or living as married 175 (65.5)
Divorced or separated 41 (15.4)
Widowed 25 (9.4)
Never married 26 (9.7)
Employment status
Employed 91 (34.2)
Retired or unemployed 175 (65.8)
Gross family annual income
$60 000 and missing 213 (78.9)
$60 000 57 (21.1)
Education level
Grade school 42 (15.6)
High school 121 (44.8)
College 52 (19.3)
University 55 (20.4)
Clinical characteristics
Stable angina and inducible ischemia 132 (49.8)
Diabetes 64 (23.9)
History of MI 104 (40.8)
History of PCI 76 (28.9)
History of CABG surgery 38 (14.2)
Data are presented as no. (%), unless otherwise indicated.
Figure 1. Percentage of patients positively responding to WTPquestions in relation to the amount asked. The solid curverepresents the proportion of patients positively responding tothe first WTP question only. The dashed curve represents thelinear extrapolation of the first scenario question. The f curve
represents the proportion of patients positively responding toboth the first and the second WTP question.
48 Circ Cardiovasc Qual Outcomes January 2011
by guest on January 20, 2011circoutcomes.ahajournals.orgDownloaded from
http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/
8/19/2019 Willingness to Pay to Eliminate the Risk of Restenosis
5/8
mated to be as high as $3784. When using the second, more
conservative approach, based on the willingness to accept the
price $500 higher than the originally stated price, the median
WTP was estimated at $2802. When we reestimated the
median using all the original percentages of positive answers
to the WTP questions (without aggregation), we obtained the
value of $2806, which is very close to the median of $2802
(relative difference of 0.2%) calculated based on the com-
bined bids.
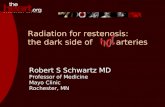
Scale TestTo test the construct validity of our study, we also examined
the probability of positively responding to the WTP question
as the function of the risk of restenosis (10% or 20%), which
could be defined as a scale test (Figure 2).19 We expected the
2 curves to show that the proportion of positive response
would be lower in the patients presented with the 10% risk of
restenosis scenario and that it would decrease when the
amounts asked increased. Although the 2 curves were gener-
ally consistent with these assumptions, they did not com-
pletely follow them (Figure 2). Because capacity to pay couldgreatly influence the probability of positively responding to
the WTP, we hypothesized that these discrepancies may be
due to residual confounding by the differences in individual
patient income. Therefore, we conducted a multivariable
regression analysis to examine how the probability of being
willing to pay was related to the risk of restenosis (20%
versus 10%) after having adjusted for patients’ income and
the amount asked. Results of the multivariable analysis
indicated that among patients with the same income and
assigned the same price, those presented with a greater risk of
restenosis would be significantly more likely to respond
positively to the WTP question (odds ratio [OR], 1.78, 95%CI, 1.07 to 2.97). These results tend to support the idea that
patients were indeed able to discriminate between the levels
of restenosis risk assumed in the 2 scenarios.
QOL
Mean scores of several dimensions of QOL assessed with theSCL-90-R and SF-36 questionnaires are presented in Table 2.
Patients who were willing to pay had similar anxiety, depres-
sion, and somatization scores as assessed by the SCL-90-R
questionnaires as those who refused. The SF-36 MCS and
SF-36 PCS were also similar in patients who were and were
not willing to pay the proposed amount.
Effect of Price on the Probability of a PositiveResponse to the WTP QuestionAmong the 3 alternative models (see Statistical Analysis
section) that yielded clinically plausible, monotonically de-
creasing effects of price, the restricted quadratic model 4 fit
the data much better than the 2 other models (AIC, 300.9 formodel 4, 304.0 for model 1, and 307.3 for model 2). Model 4
fit was also marginally better than the implausible nonmono-
tone function estimated with the unrestricted 2-term quadratic
model 3 (AIC, 301.1). Moreover, in model 3, the linear term
was statistically nonsignificant (P0.18). The latter finding
corroborates our expectation that the highest probability of a
positive answer corresponds to a price, which is not signifi-
cantly different from the minimum price of $500 considered
in our study and, thus, provides further support for the
clinically plausible model 4.
Predictors of a Positive Answer to theWTP QuestionResults of simple logistic regression analyses for predicting
the probability of being willing to pay the proposed amount
(conservative approach) are presented in Table 3. As ex-
pected, patients with a gross family income of $60 000 and
those assigned to a greater risk of restenosis in the following
year (20% versus 10%) were more likely to be willing to pay
the proposed amount. Using the restricted quadratic function,
corresponding to the best-fitting model (model 4) for the
effect of price, an increase in price was associated with a
significant decrease in patient WTP (P0.014).
Table 4 summarizes the results of the final multivariable
logistic regression model selected by both the forward and thebackward procedures. The model identified 2 variables as
Figure 2. Percentage of patients positively responding to theWTP question as a function of the presented risk of restenosisfollowing PCI. Positive response to the WTP question is basedon the conservative approach assumption. The ■ curve repre-sents the percentage of patients positively responding to the
WTP question when presented with a 20% risk of restenosisfollowing PCI. The curve represents the percentage ofpatients positively responding to the WTP question when pre-sented with a 10% risk of restenosis following PCI.
Table 2. Patient QOL and Mental Health Status According to
WTP the Proposed Amount
Willing To Pay Unwilling To Pay Mean P
SCL-90-R*
Anxiety 0.40 (0.10–0.60) 0.45 (0.10–0.60) 0.83
Depression 0.56 (0.15–0.77) 0.60 (0.15–0.85) 0.71
Somatization 0.77 (0.33–1.00) 0.82 (0.33–1.17) 0.75
SF-36†
MCS 51.33 (46.59–58.32) 50.65 (45.65–57.09) 0.41
PCS 38.24 (29.67–46.84) 38.45 (30.43–47.42) 0.82
Data are presented as mean (interquartile range).
*SCL-90-R score ranges from 0 to 4, where 4 is the worst possible score.
†SF-36 score ranges from 0 to 100, where 100 is the best possible score.
Guertin et al Willingness To Pay To Eliminate Restenosis 49
by guest on January 20, 2011circoutcomes.ahajournals.orgDownloaded from
http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/
8/19/2019 Willingness to Pay to Eliminate the Risk of Restenosis
6/8
independent, statistically significant predictors of the proba-
bility of answering positively to the WTP question (Table 4).
Patients with gross family income $60 000 were more than
twice as likely to respond positively to WTP questions thanthose with a lower income (OR, 2.81; 95% CI, 1.32 to 5.97).
An increase in price was shown to have a significant
quadratic relation to patient response to the WTP question
(P0.001). In general, below $1500, price had little impact
on patient response to the WTP question. In contrast, as the
prices increased from $1500 to $3000, the probability of
positively responding to the WTP question started to decrease
sharply. For example, for patients with a gross family income
$60 000; risk of restenosis 20%; and a history of PCI, MI,
and CABG surgery, the estimated probabilities of their
answering yes to the WTP question were 0.81, 0.80, and 0.77
for the original bids of $500, $1000, and $1500, respectively.
However, for the patients with the same characteristics, the
estimated probability decreased to 0.72 at $2000 and 0.64 at
$2500 and was as low as 0.53 for the maximum price of
$3000. None of the other sociodemographic variables or
clinical characteristics was independently associated with the
probability of being willing to pay the proposed amount
(Table 4).
DiscussionPatients waiting for a coronary angiography with ad hoc PCI
would be willing to pay a median amount of $2802 for a
treatment that would eliminate their risk of restenosis follow-
ing PCI. Considering that patients who refused to answer the
WTP question and those who responded with an “I don’t
know” response were considered to reject the proposed
amount, the actual median WTP amount might be evenhigher. As expected, higher income and lower prices favored
answering positively to the WTP question, upholding the
internal validity of the method we used.17 Although higher
prices were shown to decrease the patients’ probability of
positively responding to the WTP question, the relation
seemed to follow a quadratic relationship, mainly beyond
$1500. Such results seem to indicate that the ability to pay
(and not the price of the treatment eliminating the risk of
restenosis) would be the only parameter of importance at
prices below $1500. This finding could imply that patients
consider that such a therapy is worth at least $1500. Alter-
natively, this finding may indicate that patients do not
consider the budgetary impact of the increase as beingconstant. For example, increasing the price from $500 to
$1000 may not have the same impact for patients as increas-
ing the price from $2000 to $2500.
To the best of our knowledge, this study is the first to
estimate patients’ WTP for the elimination of a risk of
restenosis in a publicly funded healthcare system setting.
Greenberg et al20 previously reported that US patients were
willing to pay no more than $US 273 and $US 366 for a
similar 10% and 20% reduction of the risk of restenosis.
Several reasons may explain the differences in observed WTP
between both studies. First, both risk scenarios in our study
assessed patients’ WTP for the complete elimination of the
risk of restenosis. Although our observed median WTP is
much higher than those observed in the American study,
patients in the latter study were willing to pay a much higher
amount ($1162) for the complete elimination of the risk of
restenosis. Second, given that patient healthcare costs are
already covered by taxes in Canada, it is possible that patients
would be willing to pay a much higher out-of-pocket amount
because they are only directly paying for the treatment that
eliminates the risk of restenosis compared to US patients who
would be required to pay for the whole procedure as well as
the hypothetical treatment.
Our analysis does not refer to a specific technology aimed
at reducing the risk of restenosis, such as DES, but to ahypothetical treatment that can completely eliminate resteno-
Table 3. Unadjusted Associations Between Several Variables
and WTP Based on a Positive Answer to Both Questions
(Second Approach)
Variable Unadjusted OR 95% CI P
Price asked in $1000* . . . . . . 0.014
Gross family income ($60 000 vs
$60 000 or missing)
1.89 1.01–3.55 0.05
Risk of restenosis in the following year
(20% vs 10%)
1.66 1.01–2.72 0.05
History of PCI 1.31 0.76–2.27 0.33
History of MI 1.00 0.60–1.67 1.00
History of a CABG surgery 0.97 0.48–1.94 0.93
Age, y 0.99 0.96–1.01 0.22
Female vs male sex 0.85 0.49–1.46 0.55
College and higher vs lower 1.62 0.97–2.67 0.06
The respondent is currently employed 0.87 0.52–1.45 0.59
Somatization† 0.85 0.56–1.30 0.46
Depression† 0.87 0.56–1.37 0.55
Anxiety† 0.78 0.46–1.32 0.35
SF-36 MCS† 1.01 0.98–1.03 0.54
SF-36 PCS† 1.00 0.98–1.02 0.88
*Price asked (per $1000 increment) has a quadratic relation with patient
WTP (see text for details). Price asked was calculated as initial price$500 (ie,
centered to have 0 value at the minimum price of $500 considered in our
study).
†Per 1-point increase.
Table 4. Independent Predictors of WTP
Independent Variable OR* 95% CI P
Price asked in $1000† . . . . . . 0.001Gross family income ($60 000 vs
$60 000 or missing)‡
2.81 1.32–5.97 0.01
Risk of restenosis in the following
year (20% vs 10%)‡
1.61 0.90–2.90 0.11
History of PCI‡ 1.59 0.82–3.06 0.17
History of MI‡ 0.87 0.48–1.59 0.65
History of a CABG surgery‡ 1.34 0.55–3.28 0.52
*Adjusted for all other variables listed in the table.
†Price asked (per $1000 increment) has a quadratic relation with patient
WTP (see text for details). Price asked was calculated as initial price$500 (ie,
centered to have 0 value at the minimum price of $500 considered in our
study).
‡Variable was forced into the model based on a priori considerationregardless of its statistical significance.
50 Circ Cardiovasc Qual Outcomes January 2011
by guest on January 20, 2011circoutcomes.ahajournals.orgDownloaded from
http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/
8/19/2019 Willingness to Pay to Eliminate the Risk of Restenosis
7/8
sis. No treatment currently can achieve such a health benefit.
Most cost-effectiveness analyses have indicated that the best
“bang for the buck” with DES may be limited to patients with
higher risk profiles, although the widespread implantation of
DES in the unselected population may not be cost-effec-
tive.6,21–23 Such evaluations usually were based on a disease-
specific cost-effectiveness ratio: cost per RR avoided.21–25
Although this metric has intuitive appeal and is straightfor-
ward to calculate, the proper threshold value to declare that an
intervention is cost-effective was derived from available
literature and believed to be $10 000 per RR avoided.20–22
Compared with societal thresholds in cost-effectiveness anal-
yses, the amount patients are willing to pay to attain a
preferred health state may substantially differ from society’s
WTP for the same outcome. Therefore, our results should not
be used to set a threshold to declare a treatment as cost-
effective when using the cost per RR avoided metric. We can
only conclude that patients would be willing to pay a
substantial amount ($2802 out of their pocket), which
amounts to close to 3 times the incremental cost of a DESover a BMS (currently $1000), for a treatment that com-
pletely abolishes the risk of this detrimental health condition
(a goal that has yet to be realized with current therapies).
Our study has limitations that we need to acknowledge.
First, our selected range of value underestimated patients’
WTP for the intervention, and as such, we needed to linearly
extrapolate our population’s median WTP. Although the
selected range was based on the incremental cost of DES over
BMS, a wider or higher range of bids would have yielded a
more-precise answer. Additionally, WTP using an out-of-
pocket amount already has been shown to overestimate
patients’ real WTP.9 Despite attempting to palliate this issue,
patients may still have stated an increased WTP due to thevirtual exercise of the survey. Second, we used an ex post
approach that involved asking a sample population of patients
undergoing cardiac catheterization with ad hoc PCI about
their WTP for a treatment that would eliminate the risk of
restenosis. The ex post approach estimates the amount a user
would be willing to pay for the treatment at the point of
consumption.11 In contrast, the ex ante approach estimates the
amount an individual would be willing to pay, through
increased taxes or insurances fees, for the treatment to be
covered by an insurance plan.11 Although the ex post ap-
proach is more commonly used in contingent valuations,
some have argued that the ex ante approach should be favored
due to its theoretical foundation.26 However, the ex post
approach offers several advantages, including better under-
standing by actual patients of risk and benefits associated
with the proposed treatment.27,28 Third, we used a closed-
ended format to elicit our patients’ WTP. Evidence shows
that different formats can yield different estimates of WTP;
however, there is no consensus on which format should be
used.12 There is at least some concern that closed-ended
formats can overestimate the real WTP.29,30 Fourth, our study
was performed in a single large teaching hospital. Although
this center provides services to patients in and beyond the
greater Montreal region, our study sample comprised essen-
tially French-Canadians whose values may possibly differfrom patients outside our province or country. Finally, as
acknowledged earlier, we attempted to assess patients’ WTP
for a hypothetical treatment that would completely eliminate
restenosis with no additional risk. This assumption diverges
from the current outcome of DES, which remains limited by
a residual risk of restenosis, although the residual risk appears
lower than 5% to 7% in most cases.5 Therefore, the WTP we
assessed cannot be considered equivalent to the WTP for the
incremental cost of DES versus BMS, and determining such
a WTP would require an additional contingent valuation
specifically comparing the benefits of DES to BMS. Further-
more, conventional decision theory would suggest that the
probability of a positive answer to the WTP question should
be proportional to the baseline risk.31,32 Accordingly, in our
study, the group presented with the 20% risk of restenosis
should have a twice-higher probability of a positive answer
than the 10% group. Our point estimate of the adjusted OR
for the higher (20%) versus lower (10%) baseline risk (OR,
1.78; 95% CI, 1.07 to 2.97) is slightly below the expected
value of 2.0, but the latter value is well within the estimated
95% CI, suggesting that the discrepancy may be due tosampling error. Whereas our questionnaire was designed to
assess WTP for only a 10% or 20% risk of restenosis, it
would be interesting to estimate the WTP corresponding to
other risk levels. Finally, it is possible that the actual increase
in the probability of the patient willing to pay in the situation
with the higher baseline risk of restenosis is lower than
expected because of concerns about the incremental risk of
other associated complications.
In conclusion, despite being informed that restenosis is a
non-life-threatening condition, our results indicate that pa-
tients would be willing to pay a substantial amount to
eliminate the risk of this complication after PCI. Although
our results provide additional information on the benefits
provided by technologies that reduce restenosis rates, a
complete cost-benefit analysis specifically examining DES
would be required to assess the entire benefits provided by
DES over BMS.
Sources of FundingThis study was funded by the Fonds de la recherche en Santé duQuébec (FRSQ). Drs Rinfret and Brophy are clinician-scientists of the FRSQ. Dr Abrahamowicz is a James McGill Professor of Biostatistics at McGill University.
DisclosuresDr Cohen has received grant support from Cordis and BostonScientific and consulting fees from Medtronic. Dr Rinfret hasreceived grant support from Cordis Canada and consulting fees fromCordis and Abbott Vascular Canada. No other potential conflict of interest relevant to this article was reported.
References1. Bucher HC, Hengstler P, Schindler C, Guyatt GH. Percutaneous trans-
luminal coronary angioplasty versus medical treatment for non-acute
coronary heart disease: meta-analysis of randomised controlled trials.
BMJ . 2000;321:73–77.
2. Brophy JM, Belisle P, Joseph L. Evidence for use of coronary stents. A
hierarchical Bayesian meta-analysis. Ann Intern Med . 2003;138:777–786.
3. Baim DS. New devices for percutaneous coronary intervention are rapidly
making bypass surgery obsolete. Curr Opin Cardiol. 2004;19:593–597.
4. Rinfret S, Grines CL, Cosgrove RS, Ho KK, Cox DA, Brodie BR, MoriceMC, Stone GW, Cohen DJ. Quality of life after balloon angioplasty or
Guertin et al Willingness To Pay To Eliminate Restenosis 51
by guest on January 20, 2011circoutcomes.ahajournals.orgDownloaded from
http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/
8/19/2019 Willingness to Pay to Eliminate the Risk of Restenosis
8/8
stenting for acute myocardial infarction. One-year results from the
Stent-PAMI trial. J Am Coll Cardiol. 2001;38:1614–1621.
5. Babapulle MN, Joseph L, Belisle P, Brophy JM, Eisenberg MJ. A hier-
archical Bayesian meta-analysis of randomised clinical trials of drug-
eluting stents. Lancet . 2004;364:583–591.
6. Eisenberg MJ. Drug-eluting stents: the price is not right. Circulation.
2006;114:1745–1754, discussion 1754.
7. Ligthart S, Vlemmix F, Dendukuri N, Brophy JM. The cost-effectiveness
of drug-eluting stents: a systematic review. CMAJ . 2007;176:199 –205.8. Smith RD. Construction of the contingent valuation market in health care:
a critical assessment. Health Econ. 2003;12:609–628.
9. Blumenschein K, Johannesson M, Yokoyama KK, Freeman PR. Hypo-
thetical versus real willingness to pay in the health care sector: results
from a field experiment. J Health Econ. 2001;20:441– 457.
10. O’Brien B, Gafni A. When do the “dollars” make sense? Toward a
conceptual framework for contingent valuation studies in health care.
Med Decis Making. 1996;16:288–299.
11. Johannesson M. A note on the relationship between ex ante and expected
willingness to pay for health care. Soc Sci Med . 1996;42:305–311.
12. Smith RD. The discrete-choice willingness-to-pay question format in
health economics: should we adopt environmental guidelines? Med Decis
Making. 2000;20:194–206.
13. Johannesson M, Jonsson B, Karlsson G. Outcome measurement in
economic evaluation. Health Econ. 1996;5:279–296.
14. Derogatis LR. Symptom Checklist-90-R Administration, Scoring, and
Procedures Manual—Third Edition. Minneapolis, MN: NCS Pearson;
1994.
15. Stewart AL, Hays RD, Ware JE Jr. The MOS short-form general health
survey. Reliability and validity in a patient population. Med Care. 1988;
26:724–735.
16. Kriström B. A non-parametric approach to the estimation of welfare
measures in discrete response valuation studies. Land Econ. 1990;66:
135–139.
17. Klose T. The contingent valuation method in health care. Health Policy.
1999;47:97–123.
18. Akaike H. A new look at the statistical model identification. IEEE
Transactions on Automatic Control. 1974;AC-19:716–723.
19. Norinder A, Hjalte K, Persson U. Scope and scale insensitivities in a
contingent valuation study of risk reductions. Health Policy. 2001;57:
141–153.
20. Greenberg D, Bakhai A, Neumann PJ, Cohen DJ. Willingness to pay foravoiding coronary restenosis and repeat revascularization: results from acontingent valuation study. Health Policy. 2004;70:207–216.
21. Rinfret S, Cohen DJ, Tahami Monfared AA, Lelorier J, Mireault J,Schampaert E. Cost effectiveness of the sirolimus-eluting stent inhigh-risk patients in Canada: an analysis from the C-SIRIUS trial. Am J Cardiovasc Drugs. 2006;6:159–168.
22. Brophy JM, Erickson LJ. Cost-effectiveness of drug-eluting coronarystents in Quebec, Canada. Int J Technol Assess Health Care. 2005;21:
326–333.23. Shrive FM, Manns BJ, Galbraith PD, Knudtson ML, Ghali WA.
Economic evaluation of sirolimus-eluting stents. CMAJ . 2005;172:345–351.
24. Cohen DJ, Bakhai A, Shi C, Githiora L, Lavelle T, Berezin RH, LeonMB, Moses JW, Carrozza JP Jr, Zidar JP, Kuntz RE. Cost-effectivenessof sirolimus-eluting stents for treatment of complex coronary stenoses:results from the Sirolimus-Eluting Balloon Expandable Stent in theTreatment of Patients With De Novo Native Coronary Artery Lesions(SIRIUS) trial. Circulation. 2004;110:508–514.
25. Ong AT, Daemen J, van Hout BA, Lemos PA, Bosch JL, van DomburgRT, Serruys PW. Cost-effectiveness of the unrestricted use of sirolimus-eluting stents vs. bare metal stents at 1 and 2-year follow-up: results fromthe RESEARCH Registry. Eur Heart J . 2006;27:2996 –3003.
26. Gafni A. Willingness-to-pay as a measure of benefits. Relevant questionsin the context of public decisionmaking about health care programs. Med Care. 1991;29:1246 –1252.
27. Neumann PJ, Johannesson M. The willingness to pay for in vitro fertil-ization: a pilot study using contingent valuation. Med Care. 1994;32:686–699.
28. O’Brien B, Viramontes JL. Willingness to pay: a valid and reliablemeasure of health state preference? Med Decis Making. 1994;14:289–297.
29. Frew EJ, Whynes DK, Wolstenholme JL. Eliciting willingness to pay:comparing closed-ended with open-ended and payment scale formats.
Med Decis Making. 2003;23:150–159.30. Whynes DK, Frew E, Wolstenholme JL. A comparison of two methods
for eliciting contingent valuations of colorectal cancer screening. J Health Econ. 2003;22:555–574.
31. Jones-Lee M. The Value of changes in the probability of death or injury. J Polit Econ. 1974;82:835.
32. Weinstein MC, Shepard DS, Pliskin JS. The economic value of changingmortality probabilities: a decision-theoretic approach. Q J Econ. 1980;
94:373–396.
52 Circ Cardiovasc Qual Outcomes January 2011
by guest on January 20, 2011circoutcomes.ahajournals.orgDownloaded from
http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/http://circoutcomes.ahajournals.org/