
WIDER Working Paper No. 2013/095
24
Copyright UNU-WIDER 2013 *University of Adelaide, Australia; emails: [email protected]; [email protected] This study has been prepared within the UNU-WIDER project ‘ReCom–Foreign Aid: Research and Communication’, directed by Tony Addison and Finn Tarp. UNU-WIDER gratefully acknowledges specific programme contributions from the governments of Denmark (Ministry of Foreign Affairs, Danida) and Sweden (Swedish International Development Cooperation Agency—Sida) for ReCom. UNU-WIDER also gratefully acknowledges core financial support to its work programme from the governments of Denmark, Finland, Sweden, and the United Kingdom. ISSN 1798-7237 ISBN 978-92-9230-672-4 WIDER Working Paper No. 2013/095 The World Bank’s health projects in Timor-Leste The political economy of effective aid Andrew Rosser and Sharna Bremner* Abstract The World Bank’s health sector projects in Timor-Leste—the Health Sector Rehabilitation and Development Project and the Second Health Sector Rehabilitation and Development Project— have been among the few successful operations it has funded in that country. This paper examines the factors underpinning their relative success and considers the wider lessons of the Bank’s experience for our understanding of the conditions that lead to effective aid in fragile contexts. Much commentary on these projects has suggested, either implicitly or explicitly, that good design and management were key factors in their success. We argue that political economy factors also played an important role, extending and revising an earlier analysis. In particular, we suggest that these rehabilitation and development projects benefitted from (i) a political economy context that was relatively conducive to aid effectiveness in general and (ii) the fact that there was relatively little elite resistance to the World Bank’s health policy agenda compared to its policy agenda in other sectors. In terms of wider lessons, we argue for a more political understanding of the determinants of aid effectiveness. Specifically we suggest that aid effectiveness needs to be seen as a function not just of the technical quality of project design and the administrative competence of project managers but also the extent to which there is congruence between donor and local elites’ agendas. Keywords: Timor-Leste, aid effectiveness, fragile contexts, health, World Bank JEL classification: I18 and O21
Transcript of WIDER Working Paper No. 2013/095

Copyright UNU-WIDER 2013
*University of Adelaide, Australia; emails: [email protected]; [email protected]
This study has been prepared within the UNU-WIDER project ‘ReCom–Foreign Aid: Research and Communication’, directed by Tony Addison and Finn Tarp.
UNU-WIDER gratefully acknowledges specific programme contributions from the governments of Denmark (Ministry of Foreign Affairs, Danida) and Sweden (Swedish International Development Cooperation Agency—Sida) for ReCom. UNU-WIDER also gratefully acknowledges core financial support to its work programme from the governments of Denmark, Finland, Sweden, and the United Kingdom.
ISSN 1798-7237 ISBN 978-92-9230-672-4
WIDER Working Paper No. 2013/095 The World Bank’s health projects in Timor-Leste The political economy of effective aid Andrew Rosser and Sharna Bremner*
Abstract
The World Bank’s health sector projects in Timor-Leste—the Health Sector Rehabilitation and Development Project and the Second Health Sector Rehabilitation and Development Project—have been among the few successful operations it has funded in that country. This paper examines the factors underpinning their relative success and considers the wider lessons of the Bank’s experience for our understanding of the conditions that lead to effective aid in fragile contexts. Much commentary on these projects has suggested, either implicitly or explicitly, that good design and management were key factors in their success. We argue that political economy factors also played an important role, extending and revising an earlier analysis. In particular, we suggest that these rehabilitation and development projects benefitted from (i) a political economy context that was relatively conducive to aid effectiveness in general and (ii) the fact that there was relatively little elite resistance to the World Bank’s health policy agenda compared to its policy agenda in other sectors. In terms of wider lessons, we argue for a more political understanding of the determinants of aid effectiveness. Specifically we suggest that aid effectiveness needs to be seen as a function not just of the technical quality of project design and the administrative competence of project managers but also the extent to which there is congruence between donor and local elites’ agendas.
Keywords: Timor-Leste, aid effectiveness, fragile contexts, health, World Bank JEL classification: I18 and O21

The World Institute for Development Economics Research (WIDER) was established by the United Nations University (UNU) as its first research and training centre and started work in Helsinki, Finland in 1985. The Institute undertakes applied research and policy analysis on structural changes affecting the developing and transitional economies, provides a forum for the advocacy of policies leading to robust, equitable and environmentally sustainable growth, and promotes capacity strengthening and training in the field of economic and social policy making. Work is carried out by staff researchers and visiting scholars in Helsinki and through networks of collaborating scholars and institutions around the world.
www.wider.unu.edu [email protected]
UNU World Institute for Development Economics Research (UNU-WIDER) Katajanokanlaituri 6 B, 00160 Helsinki, Finland Typescript prepared by Liisa Roponen at UNU-WIDER. The views expressed in this publication are those of the author(s). Publication does not imply endorsement by the Institute or the United Nations University, nor by the programme/project sponsors, of any of the views expressed.
Acronyms
ADB Asian Development Bank
ADST Timorese Social Democratic Association
AMP Parliamentary Majority Alliance
CNRT National Congress for Timorese Reconstruction
DHMT district health management team
ETHPWG East Timorese Health Professionals Working Group
F-FDTL Falintil-Timor Leste Defence Force
GNI gross national income
HDI human development index
HMIS health management information systems
HSRDP Health Sector Rehabilitation and Development Project
IBRD International Bank for Reconstruction and Development
ICG International Crisis Group
IDPs internally displaced persons
IEG Independent Evaluation Group (of the World Bank)
IHA Interim Health Authority
INTERFET International Force for East Timor
JHWG Joint Health Working Group
NGOs non-government organizations
PSD Partido Social Democrata (Social Democrat Party)
SAME Servico Autonomo de Medicamentos e Equipamentos de Saude
TFET Trust Fund for East Timor
UNTAET United Nations Transitional Administration in East Timor
WHO World Health Organization

1
1 Introduction
The World Bank has invested heavily in promoting the reconstruction and development of the Democratic Republic of (hereafter Timor-Leste) since Indonesia’s violent withdrawal from the territory1 in 1999. It was a key part of various donor missions that planned the territory’s reconstruction in 1999-2000 and it has overseen a substantial grant programme there ever since.2 Yet the returns on this investment have been modest, even according to the Bank’s own assessment. In a recent review of the Bank’s activities in Timor-Leste since 2000, the Independent Evaluation Group (IEG) (2011), the Bank’s evaluations arm, rated the vast majority of project and sector outcomes as either ‘unsatisfactory’ or ‘moderately unsatisfactory’ and the Bank’s overall performance as ‘moderately unsatisfactory’. While the Bank had made ‘some important contributions to Timor-Leste’s development’, it argued, the outcomes had fallen ‘well short of objectives’ in most areas (IEG 2011: 1). Table 1 provides a summary of the IEG’s ratings of the Bank’s performance by sector.
Table 1: IEG ratings
Sector IEG rating
Health moderately satisfactory Education moderately unsatisfactory Poverty and unemployment alleviation unsatisfactory Youth unemployment and disaffection unsatisfactory Veterans moderately satisfactory State capacity moderately unsatisfactory Fiscal and public financial management moderately unsatisfactory Legislation unsatisfactory Private sector development unsatisfactory Agriculture unsatisfactory Hydrocarbons highly satisfactory Power sector moderately unsatisfactory Overall assistance moderately unsatisfactory
Source: IEG (2011: ix-xii).
One of the sectors in which the World Bank has achieved positive results is health. Beginning in 2000, it funded a series of health projects aimed at improving access to and the quality of basic healthcare, the capacity of health service providers to provide quality healthcare, and the government’s ability to formulate, implement and monitor all aspects of health policy (IEG 2011: 30). The most important of these were the Health Sector Rehabilitation and Development Project (HSRDP I) and the Second Health Sector Rehabilitation and
1 We describe East Timor/Timor-Leste as a ‘territory’ at various points in this paper to account for its changing political/administrative status over time—i.e., Portuguese colony, Indonesian province, UN administered territory, and now independent country—as well as the fact that the UN never officially recognised East Timor’s incorporation into Indonesia.
2 Between 2000 and 2010, it was involved in 39 separate operations in Timor-Leste across a range of sectors including health, education, agriculture, power, hydrocarbons, private sector development, fiscal and public financial management, state capacity-building, legislation, poverty and unemployment alleviation, veterans, and youth unemployment and disaffection. Its investment in Timor-Leste has also been substantial in financial terms: US$24.6 million in International Development Association grants, US$5 million in International Bank for Reconstruction and Development grants, and US$316.3 million in grants from various trust funds (IEG 2011: 1).

2
Development Project (HSRDP II). In its 2011 country programme review, the IEG (2011) rated these projects ‘satisfactory’ and ‘moderately satisfactory’ respectively. Although both projects experienced significant delays and failed to achieve results in certain areas, they are widely credited with having made a substantial contribution to the rehabilitation of Timor-Leste’s health system, improved governance within the sector, and improvements in a range of health indicators including immunization rates and health service utilization rates.
The purpose of this paper is to explore the factors that have shaped the World Bank’s relative success in Timor-Leste’s health sector and, in particular, the relative successes of HSRDP I and II. It also considers the wider lessons of the Bank’s experience for our understanding of the conditions that lead to effective aid in fragile contexts. Much commentary on the HSRDPs has suggested, either implicitly or explicitly, that good design and management were key factors in their success (Tulloch et al. 2003; Rosser 2007; World Bank 2009; IEG 2011: 29-33). We argue that political economy factors also played an important role, extending and revising the brief analysis of these factors provided by Rosser (2007). In particular, we suggest that the HSRDPs benefitted from (i) a political economy context that was relatively conducive to aid effectiveness in general and (ii) the fact that there was relatively little elite resistance to the World Bank’s policy agenda in the health sector compared to its policy agenda in other sectors. In terms of wider lessons, the paper thus reinforces arguments, expressed by a number of scholars, for a more political understanding of the determinants of aid effectiveness (see, for instance, van de Walle 2005; Rosser 2006; Manor 2007).
In presenting this analysis, we begin by examining the country context in which the two projects were established, focusing in particular on Timor-Leste’s health situation following Indonesia’s withdrawal in 1999. We then examine the nature of the two projects and the results they achieved before moving on to our explanation of their relative successes, bringing in comparative analysis of the World Bank’s performance in the education sector to illustrate the important role of political economy factors. The final part of the paper assesses the lessons of the Bank’s experience in Timor-Leste for our understanding of aid effectiveness.
2 The country context
When the World Bank began operating in East Timor in 1999—as Timor-Leste was known during the years of Indonesian occupation (1975-99) and UN transitional administration (1999-2002)—the territory was amongst the least developed in the world, reflecting centuries of oppressive and violent rule, underinvestment in the territory’s economic development, and the widespread destruction that accompanied Indonesia’s withdrawal. Under Portuguese colonial rule, the Timorese suffered over two centuries of wilful neglect. Under Indonesian occupation they suffered gross human rights violations that included random massacres, torture, starvation, extra-judicial killings, forced migration, and the systematic raping of women as a form of ethnic cleansing (Mason 2005: 744-5; Beck and Araujo 2013: 161). An estimated 60,000 to 100,000 Timorese were killed in the twelve months following Indonesia’s invasion in 1975 alone. Estimates of the total death toll from the invasion and subsequent occupation are between 180,000 to over 200,000 (Molnar 2010: 46-50). While the Indonesian government transferred substantial resources to East Timor during its occupation, much of these went into funding Indonesian military forces and a bureaucracy staffed largely, at least at the most senior levels, by Indonesians (Patrick 2001: 50). Development outcomes were poor. Timor’s human development index (HDI) was just 0.395 in 1999, placing it in

3
152nd place out of the 162 countries for which HDIs were calculated that year. Poverty indicators were high, with 41 per cent of the population living below the national poverty line of US$0.55 per person per day, over half the population were illiterate, and maternal mortality rates were extremely high with 420 women dying for every 100,000 live births (UNDP 2002: 1).
In August 1999, the Indonesian government, under international pressure, organized a plebiscite on the territory’s future. A resounding 78.5 per cent of voters decided in favour of independence. In its wake, pro-Indonesian militias backed by the Armed Forces orchestrated a wave of violence throughout the territory that resulted in the destruction of approximately 70 per cent of public infrastructure (including electricity, communication and water supply systems) and numerous buildings and homes. It is estimated that around 250,000 people, almost a third of the population, fled across the border into West Timor and other areas of Indonesia (Gorjão 2002: 315; Ingram 2012: 4; UNHCR 2004: 12). In this context, troops from the International Force for East Timor (INTERFET) arrived in East Timor to restore security and address the intensifying humanitarian crisis. A team of experts known as the Joint Assessment Mission to East Timor visited the nation shortly after the arrival of INTERFET troops to examine the existing situation and identify short-term relief and reconstruction priorities, as well as longer-term development requirements. It noted that there was severe psycho-social stress, food insecurity, population displacement and that water and sanitation systems had collapsed (World Bank 1999b).
The territory’s health situation was particularly precarious. During their occupation, the Indonesians had assembled a territory-wide health system, comprised of Indonesian government-run hospitals and clinics, and district-based health centres that were operated by approximately 160 doctors and 2000 nurses and midwives. In 1999, most doctors, many of whom were Indonesian, fled the territory, leaving just 30 behind. Most senior health administrators left as well (World Bank 1999a: 1). At the same time, healthcare facilities were intentionally targeted during the 1999 violence, with a third being severely damaged or destroyed entirely. An assessment conducted in January 2000 found that two-thirds of Timor’s health facilities were without mains electricity or essential medical equipment, while almost half were without mains water (Morris 2001: 873). Finally, the crisis displaced huge numbers of people from their homes: between 520,000 and 620,000 people, roughly 65–80 per cent of the total population, ended up residing in internally displaced persons (IPD) camps in East Timor or West Timor (WHO 2000).3 The result was that the majority of the population was without access to adequate medical care, food, shelter, clean water and sanitation for some time. There was strong concern that such conditions would lead to high levels of malnutrition, escalated risks of disease outbreaks and increases in mortality due to diarrhoeal disease, vaccine preventable diseases, malaria, upper respiratory diseases and mental health problems (ibid.).
3 Prior to independence, population data for East Timor were unreliable. A census had been conducted under Portuguese colonial rule in 1970. However the next one was not carried out until 1990, when the nation was under Indonesian rule. It would not be until 2004 that a full census was again conducted. The United Nations Development Programme Human Development Report (2002: 13) used data from the 1970 and 1990 census’, in conjunction with growth projections to estimate that Timor’s population was approximately 779,567 in the first half of 1999.
4
In the immediate aftermath of the Indonesian withdrawal, civil society organizations played the key role in health service delivery in the territory. The Catholic Church and religion-based charities had provided health services throughout the years of Indonesian occupation, operating small hospitals and local clinics (McGregor, Skeaff and Bevan 2012: 1135; Patrick 2001: 58). Following the Indonesian withdrawal, they were joined by a flood of international non-government organizations (NGOs) that arrived to provide emergency services. These NGOs included the International Committee of the Red Cross, World Vision International, and Médecins Sans Frontières. The efforts of the Catholic Church and other NGOs combined saw 71 health facilities established by February 2000, in comparison to the 96 facilities that were operating prior to the violence. These facilities operated at a sub-district level or higher, meaning that health services for many Timorese were limited, particularly those residing in rural villages (World Bank 2000: 5; Rosser 2007: 127).
The Joint Health Working Group (JHWG), a team of representatives from UN agencies, the NGO community and Timorese health professionals from the East Timorese Health Professionals Working Group (ETHPWG) provided an initial means of coordination. Following the establishment of the United Nations Transitional Administration in East Timor (UNTAET) in October 1999, the JHWG developed plans to establish a local health authority to rebuild and administer the health system in Timor and agreed to a minimum set of standards at a workshop in February 2000. After this workshop, an Interim Health Authority (IHA) was established as part of UNTAET. The IHA was a joint international-Timorese body—something that made it distinct from most other parts of UNTAET—and became the de facto ‘ministry of health’ (La’o Hamutuk 2000). Led by Jim Tulloch, the head of the UNTAET Office of Health, and Sergio Lobo, a founding member of the ETHPWG and East Timor’s only qualified surgeon, it consisted of 16 East Timorese health professionals at the central level, an additional 13 at the district level, and six UNTAET health staff (Tulloch et al. 2003: 8).
3 The HSRDPs
3.1 Overview of projects
To address the burgeoning health crisis, the IHA and foreign donors agreed that two health projects should be funded through the Trust Fund for East Timor (TFET), a multi-donor facility established under World Bank and Asian Development Bank auspices to fund grants for projects in key sectors such as energy infrastructure, health, education, and governance.4 The first, HSRDP I began in mid-2000 while HSRDP II began in mid-2001. Both were supported by grants from the World Bank while the latter was also supported by a grant from the European Union (Tulloch et al. 2003: 2). Rather than being stand-alone initiatives, these projects formed part of a sector-wide approach focused on constructing a new health system, rather than rebuilding the previous system. The World Bank notes that this approach:
4 While the World Bank was the trustee, the ADB was responsible for managing TFET projects aimed rehabilitating roads, ports, water utilities, telecommunications and power, and had joint responsibility with the World Bank and ADB for community development projects such as microfinance. The World Bank had primary carriage of TFET projects in the sectors of health, education, agriculture, private sector development and economic capacity-building (World Bank 2001a).

5
was designed to work at two inter-related levels: (i) to permit the definition of needs across the board: service delivery, rehabilitation of the health infrastructure, health systems and health policy development; and (ii) to coordinate donor financing of the sector…... (World Bank 2001b: 39).
HSRDP I sought to provide immediate, short-term health services and prepare long-term services, frameworks and policies that were appropriate to the conditions of East Timor (World Bank 2005: 2). To this end, it consisted of two main components: (i) restoring access to basic health services; and (ii) health policies and health systems development. The first of these components was designed to address immediate health needs and had a budget of US$10.0 million. It had a short-term focus and involved a number of subcomponents, namely:
(i) A transitional strategy for service provision centred on the contracting of NGOs to provide the delivery of high priority programmes (e.g., immunization, malaria control, and nutrition and health promotion) at the district level.
(ii) The establishment of a pharmaceutical logistics system to ensure the timely availability of drugs and medical supplies, including the construction of a central warehouse and the development and adoption of an essential drug list and standard guidelines.
(iii) The rehabilitation and equipping of a number of health facilities.
(iv) The establishment of a referral system and facilities through ambulance and radio supply;
(v) Capacity strengthening within the health system through training on service delivery, administration and management responsibilities.
(vi) A small grants scheme designed to enable community organizations and professional associations to carry our health promotion activities, as a means of promoting community participation (World Bank 2005: 2-3).
The second component of the HSRDP I had a longer-term focus, and was allocated a budget of just US$1.8 million. It aimed to develop a functioning health system and sound health policies, and also comprised a number of subcomponents: (i) policy development to provide input into the role of the government and financing of the health sector, while supporting the development of a health policy framework; (ii) designing a health system, including a baseline demographic and health survey to assist future development, designing a logistics system for pharmaceuticals and the construction of health legislation and regulations; and c) a strategy to develop human resources based on the profile of existing health staff (World Bank 2005: 3).
In mid-2001, the successor to the IHA, the Division of Health Services and donors agreed that a second project should be funded to continue and expand the progress made under HSRDP I. Where HSRDP I focused on the provision of basic health services and the establishment of public health initiatives such as immunization programmes, the Second Health Sector Rehabilitation and Development Project (HSRDP II) aimed to increase the utilization of health services and increase the quality of available care. It had three components: (i) supporting on-going service delivery that was established during HSRDP I through the provision of technical assistance to health sector managers, particularly at a district level, as well via the supply of pharmaceuticals to health facilities; (ii) improving the
6
range and quality of available services and implementing support systems, with a particular emphasis on re-equipping hospitals, standardizing service delivery and strengthening referral systems and creating an effective autonomous medical supply entity; and (iii) the development and implementation of health sector policies and management systems, including through the development and implementation of a Human Resource Management Strategy and financial management capacity-building activities (World Bank 2009: 1-3).
HSRDP II was financed via the multi-donor TFET, with an allocated budget of US$12.6 million that was administered by the World Bank, and via a European Trust Fund grant of US$20.36 million. The bulk of the financing was allocated to the second component, which reflected the high cost of hospital equipment and the purchasing of medications and supplies to be stocked at the Autonomous Medical Supply entity, which came to be named Servico Autonomo de Medicamentos e Equipamentos de Saude, or SAMES (World Bank 2009: Annex 1).
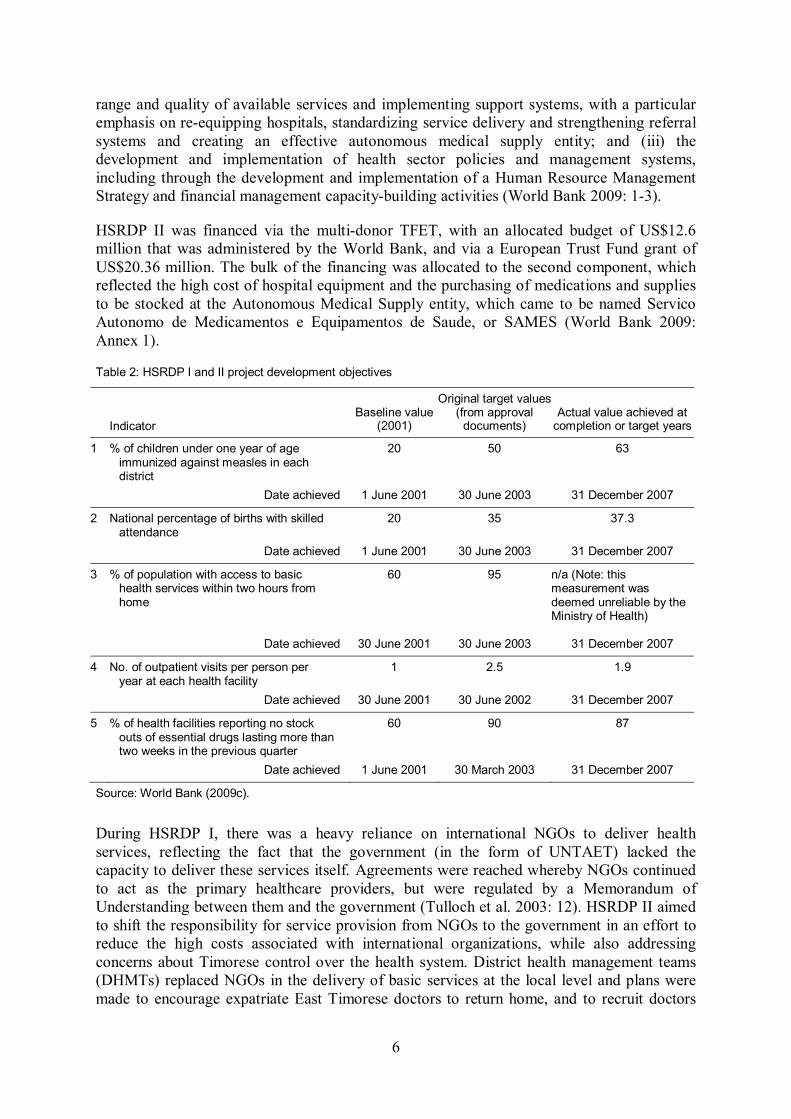
Table 2: HSRDP I and II project development objectives
Indicator Baseline value
(2001)
Original target values (from approval
documents) Actual value achieved at
completion or target years
1 % of children under one year of age immunized against measles in each district
20 50 63
Date achieved 1 June 2001 30 June 2003 31 December 2007
2 National percentage of births with skilled attendance
20 35 37.3
Date achieved 1 June 2001 30 June 2003 31 December 2007
3 % of population with access to basic health services within two hours from home
60 95 n/a (Note: this measurement was deemed unreliable by the Ministry of Health)
Date achieved 30 June 2001 30 June 2003 31 December 2007
4 No. of outpatient visits per person per year at each health facility
1 2.5 1.9
Date achieved 30 June 2001 30 June 2002 31 December 2007
5 % of health facilities reporting no stock outs of essential drugs lasting more than two weeks in the previous quarter
60 90 87
Date achieved 1 June 2001 30 March 2003 31 December 2007
Source: World Bank (2009c).
During HSRDP I, there was a heavy reliance on international NGOs to deliver health services, reflecting the fact that the government (in the form of UNTAET) lacked the capacity to deliver these services itself. Agreements were reached whereby NGOs continued to act as the primary healthcare providers, but were regulated by a Memorandum of Understanding between them and the government (Tulloch et al. 2003: 12). HSRDP II aimed to shift the responsibility for service provision from NGOs to the government in an effort to reduce the high costs associated with international organizations, while also addressing concerns about Timorese control over the health system. District health management teams (DHMTs) replaced NGOs in the delivery of basic services at the local level and plans were made to encourage expatriate East Timorese doctors to return home, and to recruit doctors

7
from other developing countries to take the place of Western doctors who had been employed by the NGOs (World Bank 2001b: 8). Both the HSRDP I and HSRDP II contained a set of key performance indicators that were used to measure project performance as well as that of the overall health system (see Table 2) (World Bank 2005: 1, 2009: i).
3.2 Outcomes
Both projects experienced significant difficulties. There were substantial delays in the construction and rehabilitation of health centres as a result of a number of factors including changes in design details, a limited number of experienced supervisors, and a lack of understanding of the World Bank’s procurement procedures (Tulloch et al. 2003: 19; World Bank 2005: 6-7). Slow procurement also plagued the rehabilitation of regional hospitals, the main hospital in Dili and the Central Lab. The process for identifying hospital equipment needs began in 2004 but procurement was not launched until 2006. The Ministry of Health was without a full-time procurement officer or biomedical equipment specialist for the majority of the second project’s duration (World Bank 2009: 10-11). SAMES experienced problems as a result of underqualified staff—from 2000 until 2005 the country lacked even a single university-trained Timorese pharmacist—and language differences, the latter proving to a serious obstacle to knowledge and skill transfers from expatriate to local staff (Huff-Rousselle 2009: 20). Another problem was the low quality of health information data. For instance, weak forecasting of demand, a process reliant on good quality health data, was partially responsible for US$2.66 million in overstocked and expired drugs at the facility in early 2004 (Huff-Rousselle 2009: 21). Finally, neither project addressed Timor-Leste’s shortage of qualified medical personnel. Both included components aimed at increasing the capacity of the Timorese workforce but these were focused on administrative and bureaucratic activities rather than the supply of medical personnel (IEG 2011: 31).5
Nevertheless, the HSRDPs made a positive contribution to the rehabilitation and development of Timor-Leste’s health sector in two respects. First, they helped to transform the country’s health system from a state of almost total devastation following the violence in 1999 into a functioning health service. The immediate basic health needs of the population were met due to the rehabilitation of healthcare facilities and other infrastructure, the procurement and distribution of essential medications and supplies, and strengthened planning and implementation of health services at the district level. Monitoring and evaluation showed increases in immunization rates and the number of births that were attended by a skilled health worker, while the average travel time from one’s home to a health facility decreased for a large portion of the population following the implementation of the projects (World Bank 2009: 15-6). The poor quality of baseline data makes it difficult to judge the precise extent of improvement in these respects.6 But the overall trend is fairly clear.
5 In the end, the President of Timor-Leste, Xanana Gusmão, struck a deal with the President of Cuba, Fidel Castro, that saw a large contingent of Cuban doctors sent to Timor to service national, regional and rural hospitals and health clinics. By 2008 there were almost 300 Cuban health workers in Timor-Leste and around 700 Timorese students studying medicine in Cuba (Anderson 2008: 53). In 2005, a Faculty of Medicine was opened at the National University and students were no longer sent to Cuba, but were enrolled in the new Cuban-operated Faculty (Anderson 2010: 185).
6 Census data collected following the implementation of HSRDP I showed that the population of Timor-Leste was larger than previously thought and the crude birth rate had been underestimated (World Bank 2005: 5). This, however, is to be expected in post-conflict situations and efforts were made to improve the quality of

8
Second, the HSRDPs contributed to improved health sector governance. A major contribution of the first project was the preparation of district health plans for the 12 districts outside of Dili. This was a task that was considered to be ‘beyond the capacity of the IHA alone’, and was the first step towards the IHA being viewed as a legitimate government body (Tulloch et al. 2003: 10). In late 2001, just over 18 months after the devastation that followed the independence vote, a Timorese-run Ministry of Health had been established and over 800 health staff had been recruited (ibid.: 16). The implementation of the HSRDPs also saw the production of the health policy framework which outlined the strategic policy direction of the Ministry of Health (2002: 26), based upon its Mission Statement:
the Mission of the Ministry of Health is to strive to ensure the availability, accessibility and affordability of health services to all East Timorese people, to regulate the health sector and to promote community and stakeholders participation…
Finally, despite SAMES’s difficulties, its establishment provided a mechanism for the distribution of medical supplies. From a state of almost total disarray, both during the Indonesian occupation, and following the violence in 1999, the formation of a public-sector pharmaceutical supply in Timor passed several milestones by 2005. The essential drugs list addressed the most pressing health needs and financial limitations, whilst also demonstrating a level of bureaucratic efficiency via clear, consistent and rational guidelines for product procurement (Huff-Rousselle 2009: 22). The central warehouse facility was constructed from scratch and the distribution system functioned relatively well, under the circumstances.
Overall, it is probably fair to say that the two projects’ achievements were modest. Timor-Leste remains a country beset by serious health problems: for instance, high child and maternal mortality rates and comparatively high incidence rates of tuberculosis and malaria.7 But compared to most other World Bank interventions in Timor-Leste, their contribution to the country’s development has been relatively positive.
In this respect, a comparison with the Bank’s projects in Timor-Leste’s education sector, also implemented through TFET, is informative. Remarkable progress was made in both sectors in terms of reconstructing and rehabilitating facilities and making them operational again. Huge numbers of schools and health facilities were rebuilt, large numbers of teachers and medical personnel were recruited, and school enrolment rates and health facility usage rates increased. But there was a marked difference in the quality of the services that were delivered. Whereas the delivery of basic health services led to significant improvements in immunization coverage rates and some improvement in the number of people with access to clean water (World Bank 2006: 1), for instance, there is little evidence to suggest that the delivery of basic education services improved school students’ skills and abilities. For instance, the
available data under HSRDP II, with the implementation of a Health Management Information System (HMIS) and the Timor-Leste Standards of Living Survey (World Bank 2009: 12).
7 The World Health Organization’s 2011 Timor-Leste Health Indicators show that under-5 mortality rates are 54 per 1000 live births, compared with a global average of 51 per 1000 live births. Maternal mortality rates are much higher than the global average of 210, with 300 deaths per 100,000 live births. The prevalence of tuberculosis was 701 per 100,000 people, much higher than the global average of 170, whilst the incidence of malaria is 10,376 per 100,000 people, compared with a global average of 4082 per 100,000 people (WHO 2013: 2).

9
government’s Primary School Achievement Survey (PSAS) conducted in 2003 found overall low levels of achievement among Grade 3 and 4 students in mathematics, the discipline on which it focused. Results for Grade 3 students were ‘only marginally better than if students had guessed throughout the test’ (World Bank 2004a: 37). Results for Grade 4 students were slightly better (World Bank 2004a: 37).
4 Explaining the HSRDPs’ effectiveness
What explains this relatively positive outcome? As noted earlier, much commentary on the HSRDPs has suggested, either implicitly or explicitly, that the projects benefitted from good design and management (Tulloch et al. 2003; Rosser 2007; World Bank 2009; IEG 2011: 29-33). Specifically, it has been suggested that:
(i) The projects were designed on the basis of a sound understanding of Timor-Leste’s health problems as a result of extensive analytical work carried out by the Joint Assessment Mission, the ETHPWG, and the IHA in the months following the Indonesian withdrawal.
(ii) The projects’ design allowed considerable flexibility in implementation, making it possible for project managers to respond to rapidly changing circumstances.
(iii) There was good donor coordination in the health sector by virtue of the use of a sector-wide approach.
(iv) There was strong country ownership of the HSRDPs, reflecting the fact that ETHPWG members, many of whom went on to hold senior positions in the IHA and subsequently the Ministry of Health, were involved in their design.
(v) The fact that the projects developed health sector policy and institutions at the same time as carrying out rehabilitation work reduced the risk that the latter would ‘lock in’ inappropriate infrastructure and delivery mechanisms—a common problem in post-conflict environments (Macrae 2001).
In interviews, World Bank staff suggested that the HSRDPs were different in these respects from World Bank projects that were less successful in achieving their objectives, especially with regards to factors (iii), (iv) and (v) above.8 As such, it seems reasonable to conclude that part of the two projects’ success story is related to the quality of their design and implementation.
In an earlier paper researched and written in 2004-05, Rosser (2007) argues that the HSRDPs also benefitted from a relatively favourable political economy context, reflecting five aspects of Timor-Leste’s political economy. First, donor funding for Timor-Leste was relatively generous in the years immediately following Indonesia’s withdrawal and for health in particular because of the ‘political attractiveness of emergencies and the undeniable health needs in such situations’ (Tulloch et al. 2003: 29) and public pressure on many Western governments to make amends for having effectively abandoned East Timor after the Indonesian invasion in 1975. Second, Timor-Leste’s dependence on aid income and vulnerability in security terms meant that the government had a strong incentive to cooperate
8 Interviews with Elisabeth Huybens, Dili, August 2004 and March 2006, and Ian Morris, Dili, August 2004.

10
closely with donors and make a concerted effort to achieve development results. To do otherwise would have jeopardized relationships crucial to the new nation’s survival. Third, the country’s health minister during the Fretilin government (2002-2007), Rui Maria de Araujo, had strong technical, leadership and administrative skills. Fourth, decision-making authority both in general and in relation to health policy in particular was concentred in the hands of the Council of Ministers (i.e., the cabinet), reflecting the ruling party Fretilin’s dominance of the national parliament. This made the HSRDP’s policy and institutional development work much easier politically than it would have been had the political system been more fragmented and parliament had exercised strong oversight of the executive’s activities. Finally, between 2000 and 2005, the country was relatively politically stable, allowing its political leaders to focus on promoting economic and social development and reducing the risk that renewed violent conflict would result in the destruction of rehabilitated health infrastructure.
Most of these conditions changed somewhat after 2005. Most notably, the country’s political stability was brought to a dramatic end by the crisis that followed the government’s dismissal of roughly one-third of the country’s armed forces in early 2006. The dismissal triggered widespread violence, the displacement of tens of thousands of people, an Australian-led intervention to restore stability, the resignation of then Prime Minister Mari Alkatiri, an
Figure 1: Net ODA, 2000–11
Source: Authors’ computations.

11
assassination attempt on then President Jose Ramos Horta, and ultimately a change of government at the 2007 elections (ICG 2006; Shoesmith 2007). The subsequent Parliamentary Majority Alliance (AMP) government, a multi-party coalition, has lacked the coherence and discipline of the previous government, being characterized by a number of public stoushes (Shoesmith 2013: 126). This did not prevent the government’s re-election in 2012 with a slightly different configuration of political parties. But it has meant that policy-making has been more contested than the Fretilin period.
Finally, since 2002 aid to Timor-Leste has declined significantly, falling particularly sharply as a proportion of gross national income (GNI) (see Figure 1), reflecting the growing importance of oil to Timor-Leste’s economy as a result of the exploitation of Timor Sea oil reserves. With the government less reliant on aid, donors have exercised less leverage over policy than previously, something that is evident, for instance, in the AMP government’s prioritization of spending on infrastructure rather than health and education and its decision to breach Petroleum Fund saving rules to fund the new infrastructure investments (Anderson 2013: 229-37; Shoesmith 2013: 138-40). It is also evident in growing disquiet about corruption, much of which is centred on procurement processes (de Jesus Soares 2013; ICG 2013: 35-7). The main line of continuity with the pre-2006 period has been in relation to leadership of the Health Ministry. As under the Fretilin government, this ministry has continued to be led by figures with relatively strong technical, leadership and administrative skills, although the standing of the current Minister has been undermined by a recent scandal related to domestic violence (Judicial System Monitoring Programme 2001).
Despite the changes since 2006, however, it is still fair to say that Timor-Leste has offered a relatively favourable political economy context to donors engaged in reconstruction efforts. The country has not descended into civil war, experienced a major economic crisis (in fact, it has progressed from low-income to lower middle-income country status in the World Bank’s classifications, thanks largely to increased oil revenues), or suffered a military coup (although it came close to one in 2006). In this respect, it has been different to many other post-conflict societies: for instance, as Lakhdar Brahimi (2007), a former special adviser to the UN Secretary General has observed, ‘about half of the countries where [UN] peace operations were said to have ended in success, actually fell back into conflict within five years’.
Noting that the broad political economy context has been relatively conducive to aid effectiveness does not explain, however, why the World Bank’s experience in Timor-Leste has differed so dramatically across sectors (or indeed why its performance overall has been so poor). To explain this, we need to understand the politics of each of these sectors and the extent to which this politics constrained the World Bank’s ability to promote its development agenda. The point, as we will show below, is that the World Bank’s agenda encountered much less resistance from domestic political elites in the health sector than in other sectors. In the health sector, domestic political elites offered broad support to the Bank or, at least, were able to engineer an accommodation between the Bank’s policy agenda and alternative policy agendas.
Despite the changes since 2006, however, it is still fair to say that Timor-Leste has offered a relatively favourable political economy context to donors engaged in reconstruction efforts. The country has not descended into civil war, experienced a major economic crisis (in fact, it has progressed from low-income to lower middle-income country status in the World Bank’s classifications, thanks largely to increased oil revenues), or suffered a military coup (although it came close to one in 2006). In this respect, it has been different to many other post-conflict societies: for instance, as Lakhdar Brahimi (2007), a former special adviser to the UN

12
Secretary General has observed, ‘about half of the countries where [UN] peace operations were said to have ended in success, actually fell back into conflict within five years’.
Noting that the broad political economy context has been relatively conducive to aid effectiveness does not explain, however, why the World Bank’s experience in Timor-Leste has differed so dramatically across sectors (or indeed why its performance overall has been so poor). To explain this, we need to understand the politics of each of these sectors and the extent to which this politics constrained the World Bank’s ability to promote its development agenda. The point, as we will show below, is that the World Bank’s agenda encountered much less resistance from domestic political elites in the health sector than in other sectors. In the health sector, domestic political elites offered broad support to the Bank or, at least, were able to engineer an accommodation between the Bank’s policy agenda and alternative policy agendas.
5 The political economy of relative success
Donor representatives have generally explained differences in development outcomes across sectors in Timor-Leste in terms of two factors: (i) the relative personal abilities of government ministers and other senior officials in these sectors and (ii) the extent to which government departments and agencies have applied ‘best practice’ in public administration. In interviews, several representatives contrasted the abilities of the former health minister, Rui Maria de Araujo, with those of the education minister at the time, and pointed to this difference as a key determinant of the contrasting outcomes in these sectors.9 In official publications, donors have focused more on the second factor. In a 2004 discussion paper on governance issues in Timor-Leste, for instance, the World Bank (2004: 11) notes that, in contrast to many other ministries, the Ministry of Health had ‘succeeded in empowering and instilling accountability in its staff’ by developing relatively clear policies, implementing strong planning and budgeting systems, and devising effective systems for assessing performance (Rosser 2009).
There can be no doubt that human resource, administrative and institutional factors have played a significant role in shaping development outcomes in Timor-Leste. But these outcomes have also reflected different levels of contestation over the nature of state policy in each sector.10 To illustrate this point, we begin by identifying the main actors involved in struggles over development policy in Timor-Leste since 1999 and then examine the way in which their interests, agendas and forms of leverage over the policy-making process shaped policy outcomes in the health and education sectors, both sectors in which the World Bank was active.
9 Interviews with officials at the World Bank and AusAID and consultants employed by these organizations, Dili, 2004 and 2006.
10 An interesting question for further research is whether health policy is inherently less political than education policy regardless of country context. It is possible that the World Bank's relative success in Timor-Leste’s health sector compared to its education sector reflects a wider political economy of health and education reform in which the forces opposed to neoliberalism are stronger and more organized in the education sector compared to the health sector.

13
5.1 The contending actors
From the end of Indonesian occupation in Timor-Leste in 1999 until the mid-2000s political and social power in that territory was concentrated in the hands of western donors: i.e., the various Western governments that have had bilateral aid programmes in the territory and the multilateral organizations (the UN and the World Bank in particular) over which these governments exercise enormous influence. Their power was arguably at its height in the 2-3 years immediately following the Indonesian withdrawal when the United Nations Transitional Administration in East Timor (UNTAET), the body established to govern the territory until independence, was formally the sovereign power (Suhrke 2001: 3; Chesterman 2002: 46). But they remained powerful after the territory gained independence in May 2002 because their importance as a source of funding and their role as the ultimate guarantors of Timor-Leste’s security gave them enormous structural leverage over the Timorese state.11 Their influence has declined somewhat since the government of Timor-Leste started to receive substantial income from the oil and gas sector in the mid-2000s. With alternative investment resources at its disposal, the government has been less dependent on donors and consequently had far greater autonomy in devising policy than in the period before the mid-2000s.
In broad terms, donors’ agenda has been to promote policy and institutional reforms aimed at ensuring the emergence and proper functioning of a liberal market economy and liberal democratic political system (Rosser 2009). In particular, it has promoted fiscal rectitude and accountability, the liberalization of trade and foreign investment regimes, the rule of law, reduced corruption, and the delivery of quality public services on an affordable basis.
A second set of actors that has shaped development policy in Timor-Leste since 1999 is the leadership of Fretilin, the political party most clearly associated with Timorese resistance to Indonesian occupation and, in the period between 2002 and 2007, the dominant political party. The Fretilin leadership’s power stemmed from two main sources: its control of parliament between 2002 and 2007 and party members’ occupation of key positions in the state apparatus. In the 2001 national elections Fretilin won 57 per cent of the vote, less than expected but enough for it to secure 55 out of a total 88 seats in the national parliament. With the support of the Timorese Social Democratic Party (ASDT), which won six seats in parliament, it held enough votes to pass a national constitution in 2001 that, in establishing a semi-presidential rather than the presidential political system,12 ensured that the party in control of parliament played the central role in policy-making. After the election, the Fretilin leadership installed party members in key positions in the state apparatus, giving it further influence over policy formulation as well as influence over the implementation of policy. Since losing the 2007 election, however, its influence through both mechanisms has declined considerably.
In broad terms, the Fretilin leadership has supported much of the donor development agenda. Originally committed to Marxism-Leninism as its official ideology (Shoesmith 2003: 238-41), Fretilin changed its ideological orientation dramatically after 1999, as its leaders sought
11 See Winters (1996) for a discussion of the notion of structural leverage.
12 See Shoesmith (2003) for an explanation of the difference between these two systems within an East Timorese context.

14
to build a strong relationship with donors in order to ensure the survival of the independent Timorese state and their party’s own political future. It is now officially committed to a free market economy and liberal democracy (Symonds 2006; Aditjondro 2001: 6-7; Saldhana 2006). This liberal orientation has translated into a broad commitment to regulate the economy along neoliberal lines, deliver basic health and education services to citizens in order to produce voters and workers, and maintain internal and external security in order to create political and social conditions that are conducive to capitalist investment. But its support for a neoliberal democratic agenda has been tempered by nationalist concerns to define a distinct East Timorese national identity and promote national strength and resilience (Rosser 2009).
A third set of actors that has shaped development policy in Timor-Leste is the leadership of Falintil, the armed wing of the resistance movement during Indonesian occupation, and associated organizations. In 2001, Falintil was dissolved as its members were either decommissioned or recruited into the armed forces (Falintil-FDTL or, for short, F-FDTL). The power of the Falintil leadership has stemmed in part from its control over the F-FDTL and its consequent ability to use violence, legitimately or illegitimately, in pursuit of its objectives;13 its ability to influence popular opinion and mobilize large numbers of people for demonstrations and other forms of collective action, reflecting the fact that Falintil leaders are widely regarded as national heroes; and its control over key parts of the state apparatus, especially the presidency and from 2007 the national parliament. Within this group, Xanana Gusmão has been the dominant figure. He was the head of Falintil during the Indonesian occupation and, following a landslide election victory in early 2002, became President of Timor-Leste from 2002 to 2007 (Shoesmith 2003: 244). In the run-up to the 2007 elections, he vacated the presidency in an attempt to seize control of parliament away from Fretilin, establishing the National Congress for Timorese Reconstruction (CNRT) as an electoral vehicle. The CNRT won 24 per cent of the vote, enough to allow it to form government in coalition with a diverse group of other parties and deliver Gusmão the prime ministership (a more powerful position than the presidency). As noted above, the AMP government was re-elected in 2012. At the same time, another Falintil leader, Taur Matan Ruak was elected president.
In terms of policy, the CNRT has lacked a clear platform (Shoesmith 2013: 132). In public statements, Gusmão has been broadly supportive of the liberal market economic policies that donors have promoted in Timor-Leste since 1999 (Gusmão 2005: 162-9) and in government CNRT has overseen an overall shift in development policy towards a more market-based approach (Anderson 2013). But, like the Fretilin leadership, Gusmão and the CNRT’s support for neoliberal reform has been tempered by a concern to promote national strength and resilience. It has also been tempered by a desire to ensure that the F-FDTL has adequate access to financial resources (Rosser 2009: 178-9). Finally, the government’s burgeoning oil wealth has enabled Gusmão and other AMP leaders to encourage a form of patronage politics that one observer has characterized as ‘runaway state-building’ (Shoesmith 2013: 138-40).
A number of other actors have also sought to shape development policy in Timor-Leste post-1999 but, in general, had much less impact than the aforementioned three sets of actors. These include the Catholic Church, the minor political parties, local NGOs, and martial arts, veterans, and extremist groups. During the Indonesian occupation, the Catholic Church
13 As Rees (2004: 5) notes, the F-FDTL is ‘the only body with control of overwhelming coercive force’.

15
became a lightning rod for Timorese grievances against the Indonesian government and military, reflecting the fact that Timor-Leste is predominantly Catholic while Indonesia is predominantly Moslem and the fact that military rule meant that few other institutions existed in Indonesian East Timor that might perform this role. But since 1999, its role as a lightning rod for grievances has declined as the major cleavages in Timorese politics have become ones within the Timorese community, rather than between this community and Moslem outsiders. At the same time, senior church figures were excluded from the Fretilin government, as the Fretilin leadership sought to reserve formal political authority for itself, although they did exercise influence over some issues, particularly ones of religious significance: in 2004, for instance, they persuaded the Fretilin government to endorse natural methods of family planning alongside the use of contraception as part of its family planning policy. The AMP government has ‘adopted a much more engaged approach to the church’, steering significant resources its ways for anti-violence programmes, church buildings and renovations and accommodating church concerns on issues such as the criminalization of prostitution and abortion (McGregor, Skeaff and Bevan 2013: 1139). But its role in policy-making has been minor compared to the actors mentioned above, reflecting the fact that there has remained a clear separation between church and state in Timor-Leste throughout the post-independence period.
The role of the minor political parties has similarly increased over time but remained modest compared to the aforementioned three sets of actors. During Fretilin’s term in government, these parties had too few seats in the national parliament to influence legislation and the Fretilin leadership completely excluded them from the cabinet. Since the formation of the AMP government in 2007, some minor political parties have exercised greater influence over policy by virtue of their membership of the governing coalition, most notably the Democratic Party (which grew out of the student and youth movements under Indonesian occupation), the Social Democrat Party (Partido Social Democrata, PSD) and the Timorese Social Democratic Association (ADST). Yet none of these parties have had clear ideological and policy agendas, being more focused on the distribution of political office (Shoesmith 2013: 132; Saldhana 2006). At the same time, the AMP government has been so dominated by Gusmão that their role has remained minor. Gusmão reportedly tends to act ‘on his own initiative’ rather than in consultation with members of his own party and coalition partners and see ‘his role as a leader, not as a member of a team of ministers representing their own political parties’ (Shoesmith 2013: 132)
For their part, local NGOs and martial arts, veterans and extremist groups have had almost no role in the formal political process (Holloway 2004; Smith 2004: 285-7). In general, the only way in which these actors have been able to influence policy has been to organize demonstrations, engage in violence, or otherwise cause disruption. When their attempts to cause disruption have intersected with attempts by elements such as soldiers from the F-FDTL to do the same thing, they have had some effect. But otherwise, they have exercised limited influence.
In the following subsection, we examine the way in which contests between these sets of actors—particularly the first there—have shaped the nature of government policy in the health and education sectors and, in so doing, the extent to which the World Bank has been able to use its aid effectively.

16
5.2 The political economy of aid effectiveness in health and education
Donors’ development policy agenda in Timor-Leste’s health and education sectors has focused on building the capacity of the state to deliver basic health and education services in order: (i) to ensure that Timor-Leste’s poor are equipped with the skills and abilities to enable them to compete in the international labour market; and (ii) to build the foundations for a functioning procedural democracy. For instance, the World Bank (2003: 1) argued that its education projects would provide ‘a foundation for democratic discourse through literacy,’ help to ‘increase productivity’, and provide ‘skills and abilities for an increased formal workforce.’ Similarly, it (2005: 21) envisaged that its health sector projects would ‘contribute to an increase in labour supply and productivity, as well as to improved educational outcomes’ in that country. In interview, Bank officials also stressed the importance of ensuring that basic education and health services were affordable.14 All of these elements reflected the neoliberal and liberal democratic orientation of donors’ development agenda and, in particular, a concern to, as Cammack (2004; 2006) has put it, ‘proletarianize’ the poor.
The Fretilin and Falintil leaderships have supported this approach much more strongly in the health sector than the education sector. At the beginning of the government’s 2002 health sector policy framework, Gusmão declared: ‘Let us not be tempted to build and develop modern hospitals that are costly and in which only half a dozen people benefit from good treatment. Let us concentrate above all on planning intensive campaigns of sanitation, prevention, and the treatment of epidemics and endemics for the whole population’ (Ministry of Health 2002). This statement can be seen as reflecting concern within Timor-Leste about the way in which the health system and in particular the hospital system during the Indonesian occupation primarily served the interests of Indonesian military and bureaucratic officials rather than ordinary Timorese. But it also resonates with donors’ concerns about the cost effectiveness of the government’s health and education programmes. Anderson (2010) has suggested that the government’s deal with Cuba for the training of Timorese doctors reflected a commitment by the country’s political leadership to progressive Latin American notions of ‘social medicine’. Likewise the government’s accommodation of the Catholic Church in relation to issues such as abortion and contraception indicates a willingness to back away from technocratic approaches to health on religiously sensitive issues. But, in broad terms, donors, the Fretilin leadership and the Falintil leadership have all been on the same page in relation to health policy issues. The Cuban deal arguably complemented rather than challenged the HSRDPs by addressing an acknowledged gap in these projects’ activities—namely, insufficient attention to manpower issues (IEG 2011: 31). And the influence of the Catholic Church has only extended to a specific set of issues rather than health policy in general.
But while the Fretilin leadership and the Falintil leadership broadly supported the donor development agenda in health, their support in relation to the education part of this agenda was tempered by their simultaneous commitment to building a particular national identity. In public speeches, Gusmão has echoed donor concerns that the education system should focus on producing job-ready graduates in order to enhance national economic competitiveness and reduce unemployment (see, for instance, Gusmão 2005: 29-30). But the Fretilin and Falintil
14 Interviews with Ian Morris and Elizabeth Huybens, World Bank, Dili, August 2004 and March 2006. See also La’o Hamutuk (2000).

17
leaderships have both been willing to compromise on this objective in order to promote nation-building objectives. The Fretilin and Falintil leaderships consist largely of individuals who were educated during the Portuguese colonial era and, in the case of the Fretilin leadership, spent most of the Indonesian occupation in the former Portuguese colony of Mozambique. Reflecting this background, they have promoted a particular brand of nationalism in the post-1999 period in Timor-Leste that has emphasized Portuguese cultural values and the use of Portuguese language as a marker of national identity. This reduced their commitment to the donor development agenda in so far as they prioritized the use of Portuguese in the education system—a language that only 5 per cent of the population speaks—over the effectiveness of the education system in providing the skills and abilities needed to produce a labour force and voters. The Portuguese and Brazilian governments made it possible for the government to carry out its attempts to promote use of Portuguese through the education system by funding Portuguese language training programmes for teachers. Other (especially Anglophone) donors, however, were highly critical of the language policy, arguing that educational considerations dictated use of Bahasa Indonesia, the national language of Indonesia, or Tetun, an indigenous lingua franca, as the primary language of use in school classrooms because both are much more widely spoken in Timor-Leste than Portuguese.
Notwithstanding the position of the Portuguese and Brazilian governments, then, it is clear that a contradiction emerged between donors, on the one hand, and the Fretilin leadership and F-FDTL, on the other hand, over which state capacities should be prioritized in the education sector. While all actors agreed that they should seek to build the state’s capacity to deliver basic education services and, in so doing, its capacity to produce educated workers who could compete in the international labour market, the Fretilin leadership and the Falintil leadership sought to subordinate this agenda to their particular nation-building objectives. For them, it became more important that the state develop the capacity to promote a particular national identity and concept of citizenship than the capacity to deliver basic education services effectively. While the country needed to produce skilled and educated workers, their position implied, it needed to produce citizens—or, at least, particular types of citizens—first. The result of this political situation was to make realization of donor agenda—and the projects associated with it—much more difficult in the education sector than the health sector.
6 Conclusion and implications
This paper has examined the factors underlying the World Bank’s relative success in Timor-Leste’s health sector and, in particular, the relative successes of HSRDP I and HSRDP II. We have argued that these projects were relatively effective, not simply for reasons related to their design and implementation, but also because (i) they were implemented within a political economy context that was conducive to aid effectiveness in general and (ii) there was relatively little elite resistance to the World Bank’s policy agenda in the health sector compared to other sectors. Whereas the Bank’s education projects ran aground in the face of elite efforts to use the education system to promote a particular national identity, its health projects were advantaged by the fact that donors and elites shared the same health policy objectives. The results for the Bank were consequently stronger in the health sector than in education sector.
In terms of wider lessons, this finding suggests that we need a more political understanding of the determinants of aid effectiveness than is offered in much of the aid effectiveness literature. Specifically it suggests that aid effectiveness needs to be seen as a function not just

18
of the technical quality of project design and the administrative competence of project managers but also the extent to which the agendas of donors and developing country elites align with one another—that is, there is a congruence, rather than a contradiction, between these agendas. In a recent analysis of the performance of its own projects, the Asian Development Bank (ADB) (2008) attributed most failures to variables such as (i) inadequate technical analysis or inappropriate project design; (ii) insufficient or deficient supervision by ADB during project implementation; (iii) insufficient capacity; (iv) questionable relevance and selection of the original project proposal; (v) the use of the wrong modality; and (vi) inappropriate or unclear implementation arrangements. By contrast, our analysis suggests that such matters of design and management are only part of the story (see also van de Walle 2005; Rosser 2006; Manor 2007). Donor projects can fail because the political economy context throws up obstacles to the realization of their objectives. Alternatively, they can succeed because the political economy context facilitates their objectives.
In recent years, donors have increasingly argued that aid effectiveness is a function of the extent of country ownership. For instance, the Paris Declaration on Aid Effectiveness, identifies country ownership as the first and most important of five broad principles of effective aid. It formally defines country ownership as recipient countries exercising leadership over the development process and, accordingly, calls on recipient countries to ‘exercise leadership in developing and implementing their national development strategies’ and take the lead in coordinating aid activities at all levels. However, it also proposes that this principle be realized primarily through the development of a national development strategy and a shift away from project‐based to programme‐based forms of aid such as general budget support, sector budget support and sector‐wide approaches. The sections of Paris Declaration that deal with alignment explicitly require donors to make increased use of recipient country public financial management and procurement systems and to assess development performance against targets established in national strategies rather than donor strategies and objectives.
Our argument, however, is consistent with a different—and more explicitly political—understanding of country ownership. Specifically, it suggests that country ownership is a function of political and social relationships rather than aid management structures and aid modalities. Where the interests and agendas of donors and powerful domestic political and social groups within recipient countries are well-aligned, the political commitment required to create ownership will emerge; where it does not, the situation will be characterized by resistance to the donor agenda and aid ineffectiveness. Such ownership may be activity or sector specific: that is, it may exist in relation to certain activities or sectors within a country but not others.
This idea has important implications for the way in which the international development community seeks to enhance aid effectiveness. First, it suggests that in making decisions about how to allocate aid, both between countries and within countries between competing sectors and activities, donors need to (i) make assessments about the likelihood their agendas will encounter resistance from powerful domestic groups; and (ii) decide whether it is thus feasible to proceed with an intervention. If the likelihood of resistance from powerful domestic groups is judged to be minor, then donors should proceed. If it judged to be major, then they have three choices: not proceed, make concessions to powerful domestic groups, or explore strategies for reducing resistance to their agenda. The latter might include: (i) redesigning aid interventions to make them more palatable to powerful domestic groups—that is, in effect, seeking to broker a compromise with these groups about the use of aid; and

19
(ii) seeking to change the political landscape in aid recipient countries so as to shift power from groups that are opposed to their agenda to ones that support it. Second, donors accordingly need to develop a better understanding of the political and social environments of the countries/sectors/activity areas in which they operate. Many donors are responding in this respect (World Bank 2009b; AusAID 2013) but in general their commitment to political and social analysis had been inconsistent and half-hearted (Unsworth 2009; Carothers and de Gramont 2013) Finally, it is extremely important for progressive civil society organizations to contest and monitor donor aid policies. One cannot assume that the donor agenda will necessarily be pro‐poor, notwithstanding the fact that popular support for aid programmes in donor countries rests partly on claims about their effectiveness in promoting poverty reduction.
If the World Bank had employed a more politically-informed approach in designing its programme in Timor-Leste, its results would have depended on the quality of its political analysis and the appropriateness and effectiveness of its response to elite resistance. These are difficult things to get right. However, the World Bank arguably would have given itself a much greater chance of producing successful results than by employing a traditional technocratic approach.
References
Aditjondro, G. (2001). Timor Lorosa’e on the Crossroads: Timor Lorosa’e’s Transformation from Jakarta’s Colony to a Global Capitalist Outpost. Jakarta: Center for Democracy and Social Justice Studies.
Anderson, T. (2008). ‘Solidarity Aid: The Cuba-Timor-Leste Heath Programme’. Paper presented to the Asian Studies Association of Australia Conference, 1-3 July. Melbourne.
Anderson, T. (2010). ‘Social Medicine in Timor-Leste’. Social Medicine, 5(4): 182–91.
Anderson, T. (2013). ‘Development Strategy’. In M. Leach and D. Kingsbury (eds), The Politics of Timor-Leste: Democratic Consolidation after Intervention. Ithaca: Cornell Southeast Asia Programme Publications, pp. 215–38.
AusAID (2013). Thinking and Working Politically: an Evaluation of Policy Dialogue in AusAID. Canberra: Office of Development Effectiveness.
Beck, M., and S. Araujo (2013). ‘Timor-Leste: The Now in the Not Yet of School Leadership’ In S. R. P Clarke and T. A. O’Donoghue (eds), School Level Leadership in Post-conflict Societies: The Importance of Context. Oxon: Routledge.
Brahimi, L. (2007). ‘State Building in Crisis and Post-Conflict Countries’. Paper presented at the 7th Global Forum on Reinventing Government: Building Trust in Government, 26-29 June. Vienna.
Cammack, P. (2004). ‘What the World Bank Means by Poverty Reduction, and Why it Matters’. New Political Economy, 9(2): 189–211.
Cammack, P. (2006). ‘UN Imperialism: Unleashing Entrepreneurship in the Developing World’. Papers in the Politics of Global Competitiveness No. 2. Manchester: Manchester Metropolitan University.
Carothers, T., and D. de Gramont (2013). Development Aid Confronts Politics: The Almost Revolution. Washington DC: Carnegie Endowment for International Peace.

20
Chesterman, S. (2002). ‘East Timor in Transition: Self-determination, State-building and the United Nations’. International Peacekeeping, 9(1): 45–76.
de Jesus Soares, A. (2013). ‘Combating Corruption: Avoiding “Institutional Ritualism” ’. In M. Leach and D. Kingsbury (eds), The Politics of Timor-Leste: Democratic Consolidation after Intervention. Ithaca: Cornell Southeast Asia Programme Publications, pp. 85–98.
Gusmão, X. (2005). Timor Lives! Speeches of Freedom and Independence. Alexandria: Longueville Books.
Gorjão, P. (2002). ‘The Legacy and Lessons of the United Nations Transitional Administration in East Timor’. Contemporary Southeast Asia, 24(2): 313–36.
Holloway, R. (2004). ‘NGO Advocacy in Timor-Leste—What is Possible’. In Catholic Relief Services (ed.), Aspects of Democracy in Timor-Leste—NGOs Advocating for Social Change. Dili: Catholic Relief Services, pp.7-16.
Huff-Rousselle, M. (2009). ‘Starting from Scratch in Timor-Leste: Establishing a Pharmaceutical and Medical Supplies System in a Post-Conflict Context’. Washington, DC: IBRD and the World Bank Group.
IEG-World Bank (Independent Evaluation Group) (2011). Timor-Leste Country Programme Evaluation, 2000–2010. Washington, DC: Independent Evaluation Group, World Bank Group.
Ingram, S. (2012). ‘Building the Wrong Peace: Reviewing the United Nations Transitional Administration in East Timor (UNTAET) through a Political Settlement Lens’. Political Science, 64(1): 3–20.
ICG (International Crisis Group) (2006). Resolving Timor Leste’s Crisis. Jakarta: International Crisis Group.
ICG (2013). Timor-Leste: Stability at What Cost? Brussels: International Crisis Group.
Judicial System Monitoring Programme (2001). ‘JSMP Comments to the Sergio Lobo Interlocutory Appeal’. Available at: www.members.pcug.org.au/~wildwood /01julappeal .htm.
La’o Hamutuk (2000). ‘Building a National Health System for East Timor’. La’o Hamutuk Bulletin, November. Dili: La’o Hamutuk.
Macrae, J. (2001). Aiding Recovery? The Crisis of Aid in Chronic Political Emergencies. London: Zed Books.
Manor, J. (ed.) (2007). Aid that Works: Successful Development in Fragile States. Washington, DC: World Bank.
Mason, C. (2005). ‘Women, Violence and Nonviolent Resistance in East Timor’. Journal of Peace Research, (42)6: 737–49.
McGregor, A., L. Skeaff, and M. Bevan (2012). ‘Overcoming Secularism? Catholic Development Geographies in Timor-Leste. Third World Quarterly, (33)6: 1129–46.
Ministry of Health (2002). ‘East Timor’s Ministry of Health: Health Policy Framework’. Dili: Ministry of Health.
Molnar, A. (2010). Timor-Leste: Politics, History and Culture. Abingdon, Oxon: Routledge.

21
Morris, K. (2001). ‘Growing Pains of East Timor: Health of an Infant Nation’. The Lancet, 357: 873–7.
Patrick, I. (2001). ‘East Timor Emerging from Conflict: The Role of Local NGOs and International Assistance’. Disasters, (25)1: 48–66.
Rees, E. (2004). ‘Under Pressure: Falintil—Forcas de Defesa de Timor-Leste: Three Decades of Defence Force Development in Timor-Leste 1975—2004’. Geneva Centre for the Democratic Control of Armed Forces Working Paper 139. Geneva.
Rosser, A. (ed.) (2006). Achieving Turnaround in Fragile States. IDS Bulletin. Brighton: Institute of Development Studies.
Rosser, A. (2007). ‘The First and Second Health Sector Rehabilitation and Development Projects in Timor-Leste’. In J. Manor (ed.), Aid That Works: Successful Development in Fragile States. Washington, DC: World Bank, pp. 123–43.
Rosser, A. (2009). ‘Rebuilding Governance in Fragile States: The Case of Timor-Leste’. In W. Hout and R. Robison (eds), Governance and the Depoliticization of Development. London: Routledge, pp.169–82.
Saldhana, J. (2006). ‘Anatomy of Political Parties in Timor-Leste’.
Shoesmith, D. (2003). ‘Timor-Leste: Divided Leadership in a Semi-Presidential System’. Asian Survey, 43(2): 231–52.
Shoesmith, D. (ed.) (2007). The Crisis in Timor-Leste: Understanding the Past, Imagining the Future. Darwin: Charles Darwin University Press.
Shoesmith, D. (2013). ‘Political Parties’. In M. Leach and D. Kingsbury (eds), The Politics of Timor-Leste: Democratic Consolidation after Intervention. Ithaca: Cornell Southeast Asia Programme Publications, pp.121–43.
Smith, A. (2004). ‘Timor-Leste: Strong Government, Weak State’. Southeast Asian Affairs, 280–94.
Suhrke, A. (2001). ‘Peacekeepers as Nation-Builders: Dilemmas of the UN in East Timor’. International Peacekeeping, 8(4): 1–20.
Symonds, P. (2006). ‘How Australia Orchestrated “Regime Change” in Timor-Leste’. Available at www.wsws.org/articles/2006/jul2006/tim1-j27.shtml (accessed 22 August 2007).
Tulloch, J., F. Saadah, R. M. de Araujo, R. P. de Jesus, et al. (2003). Initial Steps in Rebuilding the Health Sector in East Timor. Washington, DC: The National Academies Press.
UNDP (United Nations Development Programme) (2002). East Timor Human Development Report 2002. Dili: UNDP.
UNHCR (United Nations High Commissioner for Refugees) (2004). Evaluation of UNHCR’s Repatriation and Reintegration Programme in East Timor 1999–2003. Geneva: UNHCR.
Unsworth, S. (2009). ‘What’s Politics Got to do with it? Why Donors Find it so Hard to Come to Terms with Politics, and Why this Matters’. Journal of International Development, 21(6): 883–94.
van de Walle, N. (2005). Overcoming Stagnation in Aid Dependent Countries. Washington, DC: Center for Global Development.

22
Winters, J. (1996). Power in Motion: Capital Mobility and the Indonesian State. Ithaca: Cornell University Press.
World Bank (1999a). ‘Joint Assessment Mission: Health and Education Background Paper’. Washington, DC: World Bank.
World Bank (1999b). ‘Building a Nation, a Framework for Reconstruction and Development: Annex 1’. Report of the Joint Assessment Mission to East Timor. Washington, DC: World Bank.
World Bank (2000). ‘Project Appraisal Document on a Proposed Grant in the Amount of US$12.7 Million Equivalent to East Timor for a Health Sector Rehabilitation and Development Project, 24 May 2000’. Washington, DC: World Bank, Human Development Sector Unit.
World Bank (2001a). TFET Update No. 9. Dili. Available at: http://documents.worldbank.org/curated/en/2001/05/7500972/trust-fund-east-timor-update-no-9, downloaded 28 July 2013.
World Bank (2001b). ‘Project Appraisal Document on a Proposed Grant in the Amount of US$12.6 million Equivalent to East Timor for a Second Health Sector Rehabilitation and Development Project, 29 June 2001’. Washington, DC: World Bank, Human Development Sector Unit.
World Bank (2003). ‘Timor-Leste Education: The Way Forward’. Dili: World Bank. Available at: www.documents.worldbank.org/curated/en/2003/12/8469483/timor-leste-education-way-forward
World Bank (2004). ‘Timor-Leste: Key Issues in Governance’. Dili: World Bank.
World Bank (2004a). ‘Timor-Leste Education since Independence: From Reconstruction to Sustainable Improvement’. Dili: World Bank
World Bank (2005). ‘Implementation Completion Report (TF-23768) on a Grant from the Trust Fund for Timor-Leste in the Amount of US$12.7 million to the Democratic Republic of Timor-Leste for a Health Sector Rehabilitation and Development Project’. Dili: World Bank.
World Bank (2006). Background paper for the Timor Leste and Development Partners Meeting, 3-4 April. Dili: World Bank.
World Bank (2009). Project completion report HSRDP II
World Bank (2009b). ‘Problem Driven Governance and Political Economy Analysis: Good Practice Framework. Washington DC: IBRD/World Bank.
World Bank (2009c). ‘Implementation Completion and Results Report on Grants in the Amount of US$12.6 Million (TF-51363) and Euro 16.2 Million (TF-51363) to Timor-Leste for A Second Health Sector Rehabilitation and Development Project, pp. Iii-iv).
WHO (World Health Organization) (2000). ‘Plan of Action for Humanitarian Health Assistance and Public Health Action in Response to the Crisis in Timor, September 1999-February 2000’. Geneva: WHO.
WHO (2013). ‘Timor-Leste: Health Profile’. Geneva: WHO. Available at www.who.int/gho/countries/tls.pdf (accessed 30 May 2013).


















