Why You Switched to the Tiger 2 Self-Advancing … You Switched to the Tiger 2 ... •...
12
EASE OF USE • Self-advancing technology minimises hands-on time for clinicians. • Requires no additional devices or costly capital equipment to facilitate placement. • Unique design helps prevent kinking and migration into the stomach. COST-EFFECTIVE • Eliminates need for expensive placement procedures (i.e., surgery, fluoroscopy, endoscopy). • Requires only one x-ray to confirm final placement in the jejunum. IMPROVED NUTRITION ADMINISTRATION • Bedside placement allows enteral feeding to be started sooner than other methods. • Small-bowel feeding results in higher intake of calories and protein for quicker achievement of patients’ nutritional goals. 1 PATIENT SAFETY • Eliminates risks to patients during transport to operating room or radiology for tube placement. Why You Switched to the Tiger 2 ™ Self-Advancing Nasal Jejunal Feeding Tube Why You Switched
Transcript of Why You Switched to the Tiger 2 Self-Advancing … You Switched to the Tiger 2 ... •...
EasE of UsE• Self-advancingtechnologyminimiseshands-ontimeforclinicians.
• Requiresnoadditionaldevicesorcostlycapitalequipmenttofacilitateplacement.
• Uniquedesignhelpspreventkinkingandmigrationintothestomach.
Cost-EffECtivE• Eliminatesneedforexpensiveplacementprocedures(i.e.,surgery,fluoroscopy,endoscopy).
• Requiresonlyonex-raytoconfirmfinalplacementinthejejunum.
improvEd NUtritioN admiNistratioN • Bedsideplacementallowsenteralfeedingtobestartedsoonerthanothermethods.
• Small-bowelfeedingresultsinhigherintakeofcaloriesandproteinforquickerachievement ofpatients’nutritionalgoals.1
patiENt safEty• Eliminatesriskstopatientsduringtransporttooperatingroomorradiologyfortubeplacement.
Why You Switched to the Tiger 2™ Self-Advancing Nasal Jejunal Feeding Tube
Why You Switched
Product Features
Product Features
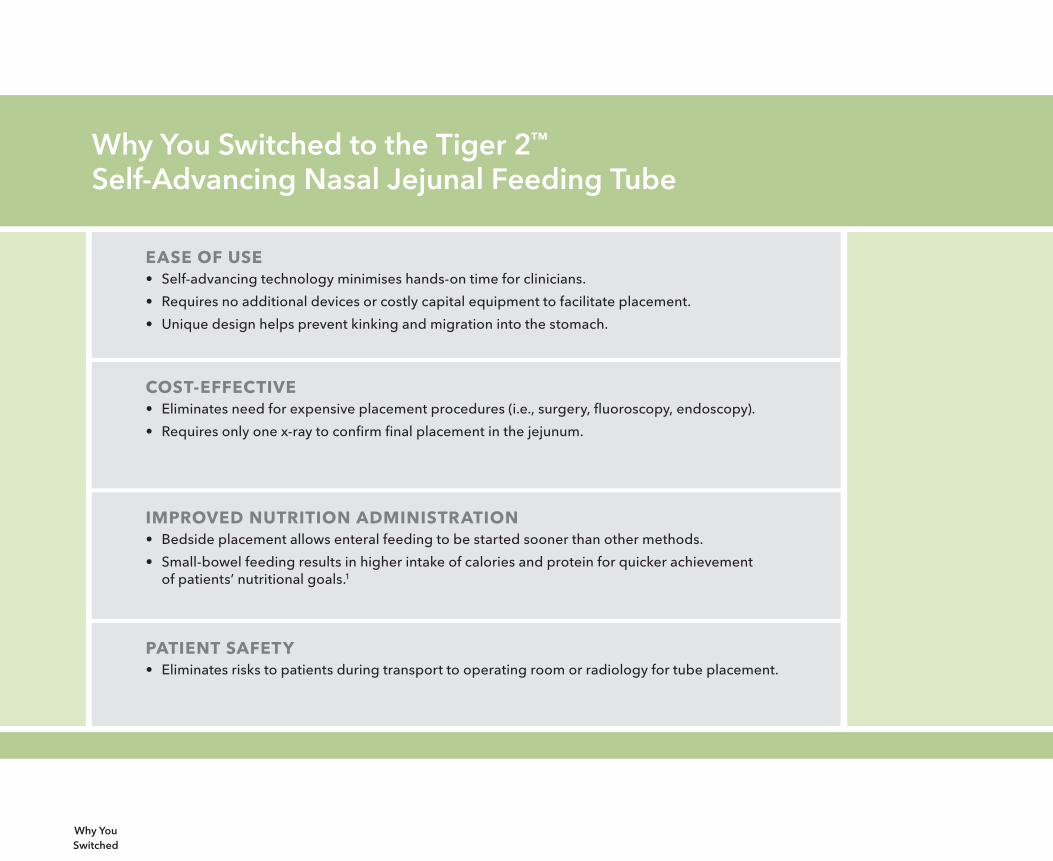
Distance markingsevery10cmfrom40-100cmprovidevisualconfirmationoftubeposition.(Tubeisradiopaquetoenhancex-rayvisualisation.)
14 Fr diameteroptimizesdeliveryofmedicationsandthicker,fiber-containingformulas.
Five large sideports helppreventthetubefromclogging.
Blunt, closed tipisatraumatictointernalstructuresandtissue.
Polyurethane material issoft,pliantand“memoryfree,”whichpreventskinkingandallowstubetotravelsmoothlythroughthegastrointestinaltractwithoutdamaginginternalstructures.
Universal adapterallowsconnectiontoavarietyofenteralfeedingsystems.
Cilia-like flapshelpfeedingtubeself-advance,aidinreducingtheriskofdislodgementandeliminatetheneedtorepositionthepatient.
Indications/Contraindications
Indications:Tiger 2 is intended to provide short-term enteral access for delivery of nutrition and/or medications to the small bowel.
Contraindications:• Oesophagealorgastricvarices
• Internationalnormalisedratio>1.3(attimeofinsertion and/or expected at time of removal)
• Anticoagulatedpatients(anticoagulatedattimeofinsertionand/orexpectedtobeanticoagulatedattimeofremoval)
• Pathologiccoagulopathies
• Historyofbleedingdisorders
• Small-orlarge-bowelobstruction
• Ischemicbowel
• Peritonitis
• Oesophagealstrictureorobstruction
• Gastricobstruction
• Recentnasal,oral,oesophagealorgastricsurgeryortrauma
• Deviatedseptum
• Inabilitytopassthefeedingtubethroughthenares
• Uncooperativepatient
Indications/ Contraindications
Insertion Checklist
The following items may be helpful during the Tiger 2 insertion process. Refertohospitalprotocolforthespecificmixofitemsrecommendedbyyourinstitution.
● Torque cable
● Stethoscope
● Water-soluble lubricant
● Lidocaine gel
● Non-Luerlockirrigationsyringe,60mLorlarger
● Towel
● Gloves
● Sterilewater
● 4 x 4 inch gauze
● Skinprep
● Prokineticagent(asrecommendedbyyourhospital)
● pHpaperinhalfstripsorCO2 detector
● Emesis basin
● HypoallergenictapeorNGstriptosecuretube
Insertion Checklist
Precautions
• Tiger2shouldonlybeusedbyorunderthesupervisionofpersonneltrained in standard gastric tube placement procedure.
• Proceedveryslowlywhenremovingthetubethroughthenoseormouth.
• ThefeedingadapterismanufacturedfromPVC(polyvinylchloride),which containsDEHP. The catheter itself does not contain DEHP.
• Thetubeisnotintendedforusebeyond30days.
• Thetorquecable(suppliedseparately)shouldbeusedonlytofacilitate placement of the Tiger 2 through the nose or mouth and into the stomach. Thetubeshouldbeadvancedonly50-70cmintothestomach.
• DonotinsertthetorquecableintoaTiger2thatisalreadyinsitu.Doingso may cause damage to internal tissues/structures.
Precautions

Instructions for Use (Abbreviated)*
1. Visuallyinspectthetubetocheckforkinks,bendsorbreaks that would inhibit proper working condition.
2.Applylubricanttothedistaltip.
3.Advance50-70cmofthefeedingtubenasallyororallyintothe stomach(dependingonpatient’sanatomicalmeasurements).Use insufflation and auscultation to confirm placement in the stomach.
4.Leavetubeinplaceat50-70cmfor30minutesto1hour.
5.Thereafter,manuallyadvancethetube10cmevery30minutes to1houruntilthe100cmmarkisreached.
6.Atthe100cmmark,takeanabdominalx-raytoconfirmposition in the small intestine.
7. Securethefeedingtubeusinghypoallergenictape.
*RefertotheTiger2IFUforcompleteinstructionsforuse.
Instructions for Use
Important Information
Torque CableAtorquecable(suppliedseparately)willprovideadditionalsupportinsideTiger2foradvancementindifficultcases.Itshouldbeusedonlytofacilitateplacement50-70cm intothestomach.Donotinsertthetorquecableintoatubethatisalreadyinsitu,as doing so may cause damage to internal tissues/structures.
Prokinetic AgentsProkineticagentsmaybeusedtoincreaseperistalsisinaccordancewith institutional protocol.
Placement Time Finalplacementinthesmallintestineusuallyoccurswithin3-4hours;however,itmaytake12-24hoursinthecaseofdecreasedperistalsis.Iffinalplacementisnotachievedwithin24hours,alternativemethodsofprovidingnutritionalsupportmayneedtobeconsidered.
FlushingA.S.P.E.Nrecommendsflushingfeedingtubeswith30mLofwaterevery4hoursduringcontinuousfeedingorbeforeandafterintermittentfeedingsinadultpatients.Sterilewater should be used for immunocompromised or critically ill patients.2Refertoyourhospital protocol for more information on flushing. The inner diameter of the Tiger 2 is3.3mm.RemembertocompareTiger2measurementswithyourexistingfeedingtubein case an adjusted flush volume is warranted.
Removal WhenremovingTiger2,proceedcautiouslyinaslow,controlledmanner.Thetubeismade from a soft and pliant polyurethane material to reduce the likelihood of tissue or structural damage during placement and removal.
Important Information
Tiger 2 Guarantee Program
IfyourTiger2feedingtubekinks,clogs,doesnotadvance,migratesbackintothestomachorispulledoutbythepatientwithin30daysofplacement,CookMedicalwillprovideanewtubefreeofcharge.
ContactyourlocalCookrepresentativeformoreinformation.
Guarantee Program
Appendix 1: A.S.P.E.N. Guidelines for Selection of Feeding Route3
Standard 9: Selection of RouteTherouteselectedtoprovidespecializednutritionsupport(SNS)shallbeappropriatetothepatient’smedicalcondition.
9.1Enteralnutrition(EN)shouldbeusedinpreferencetoparenteralnutrition(PN)tothegreatestextentpossible.
9.2PNshouldbeusedwhenthegastrointestinaltractisnotfunctionalorcannotbeaccessed,orthepatient’s nutrientneedsaregreaterthanthosethatcanbemetthroughthegastrointestinaltract.
9.3TherouteofSNSadministrationshouldbeperiodicallyreassessedforadequacyandappropriateness.
Appendices
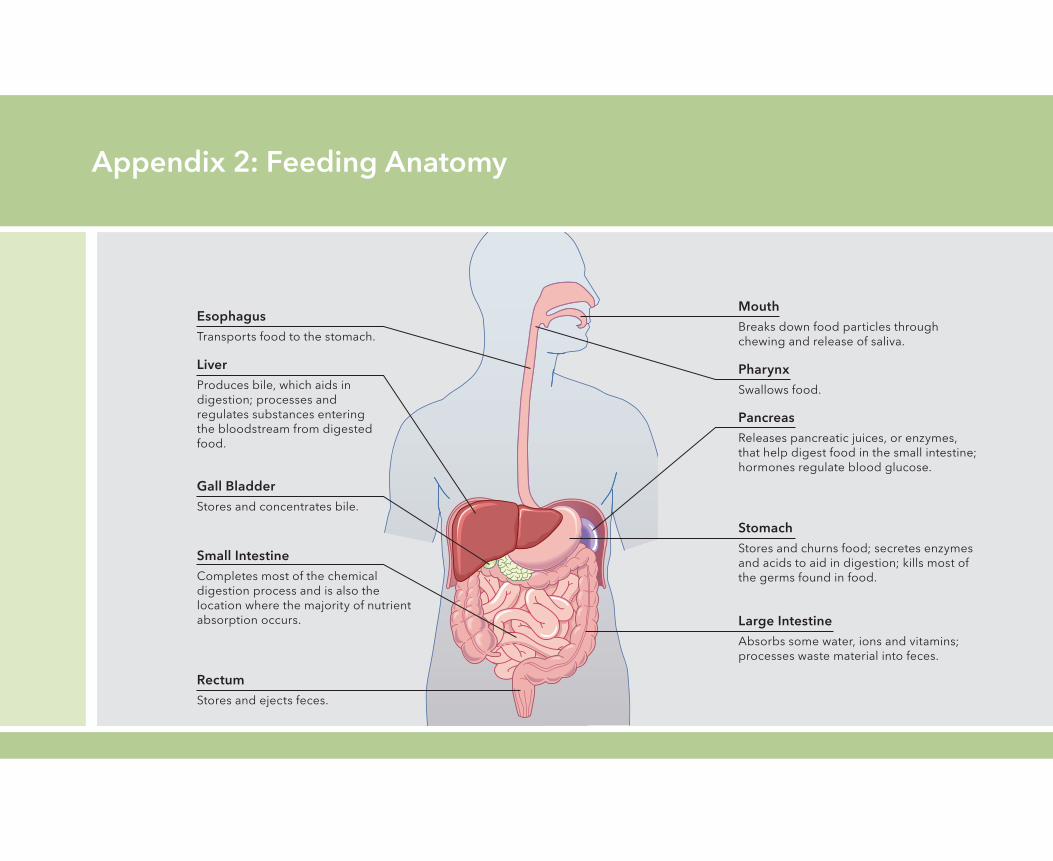
Appendix 2: Feeding Anatomy
MouthBreaks down food particles through chewing and release of saliva.
Large IntestineAbsorbssomewater,ionsandvitamins;processes waste material into feces.
PharynxSwallowsfood.
StomachStoresandchurnsfood;secretesenzymesandacidstoaidindigestion;killsmostofthe germs found in food.
Small IntestineCompletesmostofthechemicaldigestion process and is also the location where the majority of nutrient absorption occurs.
PancreasReleasespancreaticjuices,orenzymes,thathelpdigestfoodinthesmallintestine;hormones regulate blood glucose.
LiverProducesbile,whichaidsin digestion;processesand regulates substances entering the bloodstream from digested food.
EsophagusTransports food to the stomach.
Gall BladderStoresandconcentratesbile.
RectumStoresandejectsfeces.
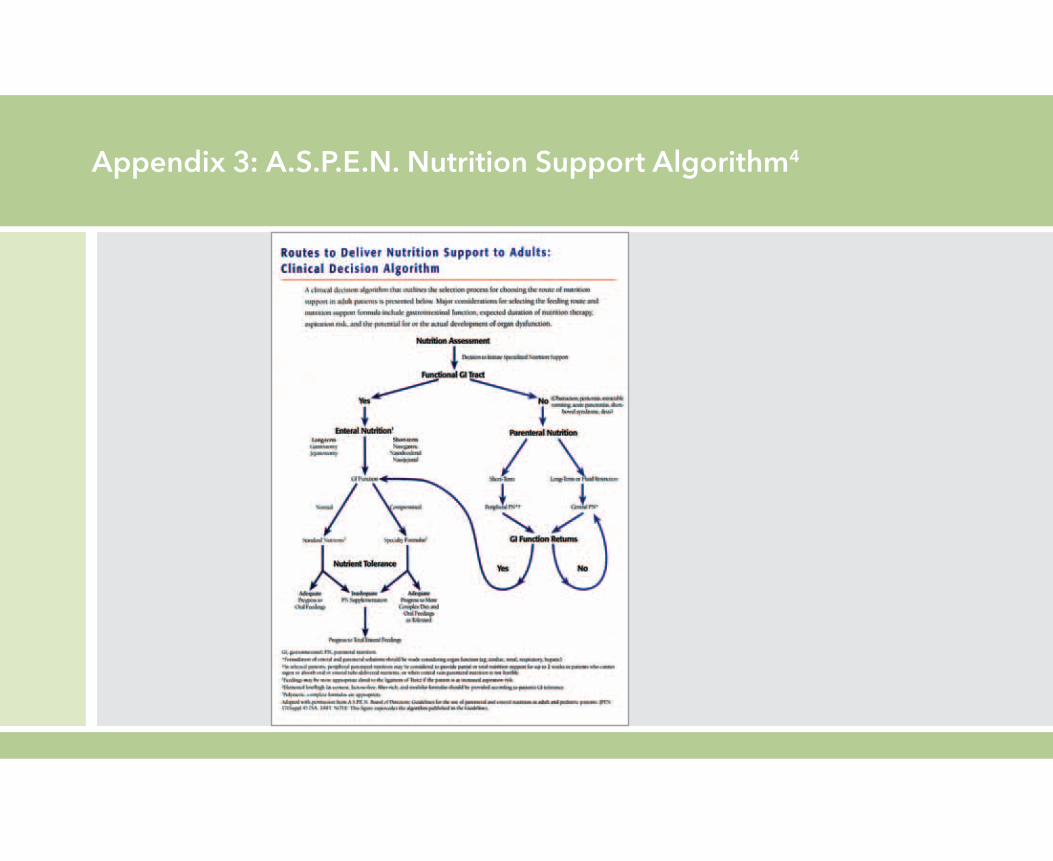
Appendix 3: A.S.P.E.N. Nutrition Support Algorithm4
References
1.HsuCW,SunSF,LinSL,etal.Duodenalversusgastricfeedinginmedicalintensivecareunitpatients: aprospective,randomized,clinicalstudy.Crit Care Med.2009:37(6);1866-1872.
2.BankheadR,BoullataJ,BrantleyS,etal.Enteralnutritionpracticerecommendations.JPEN J Parenter Enteral Nutr. 2009;33(2):122-167.
3.RussellMK,AndrewsMR,BrewerCK,etal.Standardsforspecializednutritionsupport:adulthospitalizedpatients. Nutr Clin Pract. 2002.;17(6):384-391.
4.ReprintedfromJ Parenter Enteral Nutr17(suppl4),A.S.P.E.N.Board:guidelinesfortheuseofparenteralandenteral nutritioninadultandpediatricpatients,7SA,copyright©1993,withpermissionfromSAGEPublications.
©COOK2012 CC-BOUSM-T2IFB-EN-201201
![DOSAGE FORMS AND STRENGTHS ......anticoagulated or to be anticoagulated for thromboprophylaxis. [See Warnings and Precautions (5.5) and Drug Interactions (7).] -----RECENT MAJOR CHANGES-----Boxed](https://static.fdocuments.in/doc/165x107/5f5fbaada8151e268829a33f/dosage-forms-and-strengths-anticoagulated-or-to-be-anticoagulated-for-thromboprophylaxis.jpg)