WHO_Economic Impact of Foodborne Illness

of 12
Transcript of WHO_Economic Impact of Foodborne Illness
-
8/8/2019 WHO_Economic Impact of Foodborne Illness
1/12
Foodborne illness
Economic impact of foodborne illnessWhat is damaging and distressing at thelevel of the individual also has seriousimplications on a far larger scale. In de-veloped countries efforts to quantify theeconomic impact of foodborne illness arecomparatively recent, but it is clear fromthese that foodborne illness is a majorburden on the economy. Costs arise froma number of different sources and areincurred both by the individual and by
KEY POINTS
lFood is essential for health and well-being.
l Food may also be a cause of illness.
l Foods may be intrinsically toxic or may be contaminated with toxicchemicals or pathogenic organisms.
l Foodborne illness is extensively under-reported.
l Microorganisms (bacteria, viruses, moulds and parasites) are themost important cause of foodborne illness.
l Bacteria are generally most important.
l Most foodborne illness is associated with gastrointestinalsymptoms of nausea, vomiting, stomach pains and diarrhoea.
l Foodborne illness is caused by two mechanisms: infection andintoxication.
l The infectious dose varies between organisms and between individuals.
l Foodborne illness can have seriously damaging effects onindividuals, particularly young children, and on society as a whole.
society at large. These costs include lossof income by the affected individual,cost of health care, loss of productivitydue to absenteeism, costs of investiga-
tion of an outbreak, loss of income dueto closure of businesses and loss of saleswhen consumers avoid particular prod-ucts. In 1989 it was estimated that thetotal cost of bacterial foodborne illnessto the United States economy was US$6,777,000,000. In developing countries,where the problem of diarrhoeal diseaseis far greater, the effect on economic ac-tivity and development can only be farmore severe.
-
8/8/2019 WHO_Economic Impact of Foodborne Illness
2/12
Basic Food S afety for H ealth W orkers
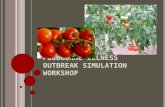
Figure 1.3 The malnutrition and diarrhoea cycle
t
t t
tDiarrhoea Death MalnutritionFood Contamination
Source : Mata, LJ Nutrition and infection. Protein Advisory Group bulletin (1971)
0 3 6 9 12 15 18 21 24 27 30 33 36
15
14
13
12
11
10
9
8
76
5
4
3
2
B o
d y w e
i g h t i n K G
Age in months
BC - BronchitisBN - BronchopneumoniaCEL - CellulitisCONJ - ConjuncivitisD - DiarrhoeaFUO - Fever of unknown originI - ImpetigoM - MeaslesS - StomatitisURI - Upper respiratory illness
Normal growth curve
Childs growth curve
CONJI
IURI
D
D
URICEL
DURI DMD D D
BC DD
D BCURI
FUO
DBC D
BC
D DURI
URID
URI
DURI D
URI
DURI
DDS
BN
Figure 1.4 Growth pattern of a child with frequent episodes of diarrhoea and other infections (The horizontal bars indicate the duration of the infectious disease)
-
8/8/2019 WHO_Economic Impact of Foodborne Illness
3/12
-
8/8/2019 WHO_Economic Impact of Foodborne Illness
4/12
Basic Food S afety for H ealth W orkers
differ appreciably. Shigella an denterotoxigenic E . coli (ETEC) are oth-erwise very similar organisms but esti-mates of their respective infective doses
are markedly different, reflecting differ-ences in their virulence.
Susceptibility to infection can vary witha range of factors such as age, generalhealth, nutrition, immune status andwhether a person is undergoing medicaltreatment. Listeriosis can be mild or evenasymptomatic in some individuals butcan be severe and often life-threateningin the unborn child. In people with low
gastric acidity, increased survival of ingested pathogens can reduce therequired infective dose, therebyincreasing the risk of infection. This isoften found in the elderly and may helpexplain their increased susceptibility tofoodborne infections. The food that is thevehicle of infection may also help reducethe infectious dose by protecting thepathogen from the lethal effect of thestomachs acidity. This has been noted
particularly with fatty foods such as sa-lami, cheese, chocolate and ice creamwhere low numbers of salmonella havebeen implicated in foodborne diseaseoutbreaks (Table 1.6).
Where the infectious dose is high, thefood vehicle can play a very specific rolein the illness. Depending on the foodscomposition and conditions of storage,a pathogen present at low and possibly
harmless levels may grow to numberssufficient to produce illness. The speedwith which bacteria can grow is describedin more detail in Chapter 2.
H ealth consequencesof foodborne illnessFor most adults in the industrialized
world, incidents of foodborne illness areunpleasant but are generally mild and self-
limiting indispositions that are restrictedto gastroenteritis and are not usually life-threatening. Exceptions occur with par-ticularly susceptible individuals such
as the very old or very young, pregnantwomen or those who are already very sick or weak for some other reason. Thesevulnerable groups constitute quite a largeproportion of the population and formany of them diarrhoeal disease can befatal.
A number of foodborne pathogens suchas Clostridium botulinumare also associatedwith acute extraintestinal (systemic)
disease. C. botulinum causes a severeneuroparalytic syndrome which is oftenfatal. The mortality rate in outbreaks inthe United States between 1976 and 1984was 7.5% but it can be substantiallyhigher (3). Survival in cases of botulismis critically dependent on early diagnosisand treatment.
Sometimes extra-intestinal diseasetransmitted by food is particularlyassociated with certain susceptible indi-viduals. For example, infection by L iste-ria monocytogenescan vary from a mild, flu-like illness to meningitis andmeningoencephalitis. It is particularlyserious in pregnant women; the mothermay experience relatively mild symptomsbut infection of the fetus can result inabortion, stillbirth or premature labour.Listeriosis is also more than 300 timesmore common in AIDS patients than in
the general population. Cancer patientsand other immunocompromisedindividuals are subject to bacteraemiacaused by foodborne bacteria. Verotoxin-producing E . coli generally results in abloody diarrhoea but can cause thehaemolytic uraemic syndrome,characterized by thrombocytopaenia,haemolytic anaemia and acute kidneyfailure, particularly in children.
Some chronic diseases, particularly ar-thritic conditions, can be triggered by
-
8/8/2019 WHO_Economic Impact of Foodborne Illness
5/12
Foodborne illness
Since the toxin is ingested with the foodthere is no direct person-to-person spread,as can occur with some enteric infec-tions, and the incubation period (the time
between consumption of the food andthe appearance of symptoms) tends tobe shorter, generally of the order of oneor two hours or even less in some cases.This is because the toxin begins to act assoon as it reaches the site of action,whereas with infections the microorgan-isms need time to multiply in the body.
There are some similarities here with otherbiotoxins such as mycotoxins and algal
toxins, though algae differ from toxigenicbacteria and moulds in that they do notmultiply in the food. Also, the health ef-fects of mycotoxins tend to be long-termrather than acute (see Chapter 2).
Infectious doseInfective pathogens can be introducedinto the body from a variety of sources.In the past, it was thought thatcontaminated water was the main sourceof the pathogens that cause diarrhoea.
This is probably still true in many cases,but it has been shown more recently thatfood may also be the vehicle of contamination in up to 70% of cases.
To cause illness, a sufficient number of cells must be consumed. This is knownas the infectious dose. The infectiousdose varies from one organism to anotherand from person to person. ForCampylobacter jejunithe infectious dose isthought to be quite low, while relativelyhigh numbers of non-typhoid Salmonellaare normally required to produce illness.Experiments have been conducted where
volunteers have consumed different lev-els of pathogens in order to determinethe infectious dose. These results and datafrom the investigation of actualoutbreaks give some indication of thenumbers of bacteria required to produceillness, but they should be regarded onlyas a rough guide (Table 1.6).
Successful infection is the result of theinteraction of two variable factors: thevirulence of the pathogen (its ability tocause illness) and the susceptibility of theindividual. The virulence of differentSalmonella serotypes, for example, can
Table 1.6 Estimated infectious doses
Escherichia colienteropathogenic 10 6 10 10
enterotoxigenic 10 6 10 8enteroinvasive 10 8
enterohaemorrhagic 10 1 10 3
Shigella 101 10 2
SalmonellaTyphi
-
8/8/2019 WHO_Economic Impact of Foodborne Illness
6/12
Basic Food S afety for H ealth W orkers
the normal functions of the gut are up-set in some way.
The gastrointestinal tract or gut is not aninternal organ of the body but a tube run-ning through it where foods are digestedand absorbed, and unwanted waste prod-ucts are expelled. In addition to absorp-tion of nutrients from foods, absorptionand secretion of water are important gutfunctions. Water absorption normallyexceeds secretion. Each day, a typicaladult will ingest about two litres of wa-ter. To this must be added saliva and se-cretions from the stomach, pancreas and
liver which altogether make a total of 8-10 litres entering the small intestine daily.About 90% of this fluid is absorbed be-fore it enters the large intestine where 80-90% of the remainder is absorbed.Changes in the small intestine that eitherdecrease absorption or increase secretionwill reduce overall absorption and resultin a larger fluid flow into the large intes-tine. If this exceeds the relatively limitedabsorptive capacity of the large intestine
then diarrhoea occurs.Bacteria cause foodborne illness by twomechanisms: infection and intoxication.The latter can also be caused by chemi-cal contaminants and naturally occurringtoxins.
Infection
Infection occurs when living bacteria areingested with food in numbers sufficientfor some to survive the acidity of thestomach, one of the bodys principal pro-tective barriers. These survivors then passinto the small intestine where they mul-tiply and produce symptoms.
Infections can be invasive or non-inva-sive. In non-invasive infections, the or-ganism attaches itself to the gut surfaceor epithelium to prevent itself from beingwashed out by the rapid flow of material
through the gut. It then multiplies, colo-nizing the surface. In some cases, suchas infection with enteropathogenic E s-cherichia coli, this produces changes in the
gut epithelium which reduce its absorp-tive capacity or cause fluid secretion.Colonizing bacteria can also produceenterotoxins; toxins that alter the functionof the cells lining the gut and cause themto secrete water and electrolytes into theintestine to produce a profuse waterydiarrhoea. A notable example of this ischolera, but a similar sequence of eventsoccurs with enterotoxigenic E . coliinfections.Invasive pathogens are not confined tothe intestinal lumen but can penetrate thecells lining the gut. In some cases theirpenetration is limited to the immediatevicinity of the gut, as with the non-ty-phoid salmonellas. Some pathogens in-vade the mucosa of the large intestinerather than the small intestine, producinginflammation, superficial abscesses andulcers, and the passage of dysenteric
stools containing blood, pus and largeamounts of mucus. In other cases,microbial invasion is not restricted to theguts immediate locality and the organ-ism spreads further through the body,producing symptoms other than diarrhoeaat sites remote from the gut itself, as forexample in brucellosis, listeriosis, typhoidand paratyphoid fevers.Illnesses caused by foodborne virusesand parasites are also broadly similar inthat viable organisms gain access to theirsite of action in the body via thegastrointestinal tract.
Intoxication
With foodborne intoxications, the bac-teria grow in the food producing a toxin.When the food is eaten, it is the toxin,rather than the microorganisms, thatcauses symptoms.
-
8/8/2019 WHO_Economic Impact of Foodborne Illness
7/12
Foodborne illness
figures are collected, but it is thought toreflect an underlying increase in thenumber of cases as well.
A number of factors have contributed tothis trend. Their relative importance var-ies between countries and between patho-gens but some of the most significant areas follows:
n Increasing industrialization and urbanliving has meant that the food chainhas become longer and more complex,increasing opportunities for contami-nation. It also means that more peo-ple are likely to be affected by a sin-
gle breakdown in food hygiene.n In poorer countries increased urbani-
zation and rapid population growthhave not been matched by develop-ment of the health-related infrastruc-ture, including basic sanitation, andthis has led to increased risk of con-tamination of the food and water sup-ply.
n Increasing affluence in other areas hasled to greater consumption of foodsof animal origin such as meat, milk,poultry and eggs. These foods are rec-ognized as more common vehicles of foodborne pathogens and this situa-tion can be exacerbated by the meth-ods of intensive production requiredto supply a larger market.
n There is greater international move-ment of both foods and people. Ex-
otic Salmonella serotypes have beenintroduced into Europe and theUnited States as a result of the im-portation of animal feeds. A numberof outbreaks of illness associated withimported foods have also been re-corded. Tourism is one of the worldsmajor growth industries and every yearmore and more people travel abroadwhere they are exposed to increasedrisk of contracting foodborne illness.
n Changing lifestyles also means thatfood preparation may be in the handsof the relatively inexperienced asmore mothers go out to work and
more people eat pre-prepared foods,meals from catering establishments orfood from street vendors.
n An increasing proportion of the popu-lation is more susceptible tofoodborne illness. This includes themalnourished, the elderly, those whohave some underlying condition suchas liver disease and those who areimmunocompromised as a result of
infections such as HIV and immuno-suppressive medical treatment.
Foodborne illness:its definition and natureThe term food poisoning has often been
used in some countries, but it is an ex-pression that can sometimes be restric-tive or misleading. Foodborne illness or foodborne diseaseare now the generally pre-ferred terms. Foodborne disease can bedefined as:
any disease of an infectious or toxicnature caused by or thought to becaused by the consumption of foodor water.
Though there are a number of importantexceptions that will be described later,in most cases and in most peoples minds,the illnesses caused by foodborne micro-organisms, principally bacteria, are asso-ciated with gastrointestinal symptoms of nausea, vomiting, stomach pains and di-arrhoea. Since diarrhoea is a commonclinical symptom in foodborne diseases,many of these diseases are referred to asdiarrhoeal diseases. These occur when
-
8/8/2019 WHO_Economic Impact of Foodborne Illness
8/12
Basic Food S afety for H ealth W orkers
foodborne in origin or may not be re-ported to the relevant authority for re-cording. Estimates vary but it is gener-ally believed that in developed countries
less than 10%, or even only 1%, of casesof foodborne illnesses ever reach officialstatistics. In countries with fewer re-sources, under-reporting must be evengreater, with probably less than 1% of
N o t
i f i c a
t i o n s
90000
80000
70000
60000
50000
40000
30000
1989 1990 1991 1992 1993 1994 1995 1996Year
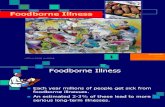
Figure 1.2a Foodborne illness : annual notifications, England and Wales
cases being reported. Studies in somecountries point to an under-reportingfactor of up to 350 in some cases.
Statistics from both developed and de-veloping countries show an increasingtrend in foodborne illness over recentyears (Figure 1.2). In part, this is prob-ably due to improvements in the way the
180
140
120
100
80
60
40
20
01976 1978 1980 1982 1984 1986 1988 1990 1992 1994
C a s e s p e r
1 0 0
, 0 0 0 p o p u
l a t i o n
Figure 1.2b Incidence of foodborne disease in Venezuela
Year
-
8/8/2019 WHO_Economic Impact of Foodborne Illness
9/12
Foodborne illness
Data collected by the Food Contamina-tion Monitoring and Assessment Pro-gramme (GEMS/ Food) indicate that inmany countries the trend in chemicalcontaminant levels is generally down-wards. This is most apparent in developedcountries where exposure to thesecontaminants is often much lower than
in developing countries (Figure 1.1).Factors contributing to this disparity arediscussed in Chapter 2. The general over-all improvement is due to increased re-striction of the use of toxic chemicalsand pesticides that persist in the environ-ment, and improved control of environ-mental pollution. Available data onfoodborne illness of biological origin pro-vide a strong contrast to this reduction
in chemical contamination.Several different types of organism cancause foodborne illness. Bacteria, single-celled organisms with typical dimensionsof around 1 m (10 -6m), are the most im-portant and well studied foodbornepathogens. A key factor is their ability tomultiply in food, thus increasing the haz-ard they pose. This is discussed in Chap-ter 2. Filamentous fungi (moulds) can alsogrow in foods and some produce toxicsubstances called mycotoxins.
A number of human viruses can be trans-mitted by food and human diseasescaused by protozoa, helminths and nema-todes that are animal parasites are prob-lems of emerging importance in anumber of countries. These differ frommost bacterial foodborne illnesses in thatthe causative organism does not multi-
ply in the food itself. A brief descriptionof the major foodborne pathogens andsome of their key features is presentedas Appendix 1. Most of the following isconcerned primarily with bacterial patho-gens, though specific aspects of otherpathogens are mentioned where appro-priate.
Extent of foodborneillnessMany developed countries have sophis-ticated systems for collecting data on theincidence and causes of foodborne illness.Yet it is known that these data representonly a fraction of the number of casesthat occur. Infected individuals may notseek medical advice, and if they do theirillness may not be recognized as
Figure 1.1Dietary intake of DDT by infants from human milk
DDT complex (DDT and its degradationproducts) contaminates food mainly as a resultof its earlier use in agriculture and public health.While DDT is now banned in most countriesfor agricultural uses, the persistence and fatsolubility of DDT have resulted in widespreadcontamination of the food chain. Levels of DDTin breast milk reflect the exposure of the mother to DDT and is a good indicator of the levels of DDT in the food supply. Breast milk is also thesole food for the first few months of life anddietary intake of DDT complex by infants insome countries approaches or exceeds theWHO recommended provisional tolerableintake of 20 g DDT/kg body weight/day.
Source: GEMS/Food WHO document (WHO/FSF/FOS/97.9)
-
8/8/2019 WHO_Economic Impact of Foodborne Illness
10/12
Basic Food S afety for H ealth W orkers
In most cases foods are not contaminatedintentionally but rather from carelessnessor insufficient education or training in foodsafety. In some cases, contamination may
be deliberate as, for example, in the mis-use of food additives such as prohibitedcolouring. In one serious case in Spain, con-taminated industrial rapeseed oil was soldfor human consumption, killing more than500 people and crippling more than 20,000(1).
How the relative importance of these haz-ards is perceived depends on who you ask.Surveys indicate that, as far as the general
public is concerned, hazards associated
with pesticide residues, environmentalchemical contaminants and the use of foodadditives cause most concern. Yet experi-ence shows that most outbreaks of
foodborne disease are associated withmicrobiological contamination.
This is reflected in the available statisticson the etiology of foodborne illness.(Table 1.5). One study estimated thatpeople are 100,000 times more likely tobecome ill as a result of microorganismsin food than as a result of pesticideresidues ( 2).
Table 1.4 Mean daily intakes (mg) of natural food toxicants
Class of compound (food source) PopulationTotal Vegetarian
Glucosinolates (brassicas) 50 110Glycoalkaloids (potatoes) 13 70 - 90Saponins (legumes) 15 100 (*220)Isoflavones (soya)
-
8/8/2019 WHO_Economic Impact of Foodborne Illness
11/12
Foodborne illness
and established processing and handlingprocedures are followed, the majority donot cause serious problems. Natural foodtoxins are described in more detail inChapter 2 but a few examples are givenin Table 1.3 and estimates for some meandaily intakes in the United Kingdom arepresented in Table 1.4.
Table 1.2 Examples of vitamin and mineral deficiency syndromes
Micronutrient Deficiency syndromeA Night blindness, xeropthalmiaThiamine Beriberi, Wernickes encephalopathy; Korsakoffs psychosisNiacin PellagraRiboflavin Mucosal lesionsPyridoxine Glossitis, neuropathyFolate Megaloblastosis, villus atrophyB12 Pernicious anaemia, megaloblastosis, neuropathyC ScurvyD Rickets, osteomalociaK HypoprothrombinaemiaIodine Goitre, cretinismIron Anaemia
Other foodborne hazards can be describedas extrinsic, indicating that their presenceis a result of contamination of the food.This includes contamination with indus-trial chemicals or pesticide residues, rightthrough to the presence of pathogenic bac-teria or parasites. The range of possibili-ties is summarized in Table 1.3.
Table 1.3 Causes of foodborne illness Examples
INTRINSIC HAZARDS(Natural Toxins or Antinutritional Factors) oxalic acid (rhubarb, spinach)
alkaloidssolanine (potatoes)dioscorine (yams)
cyanide (cassava, lima beans)haemagglutinin (red kidney beans)protease inhibitors (legumes)phytic acid (bran)amatoxin, psilocybin and others(toxic mushroom)
EXTRINSIC HAZARDSChemical Contamination dioxins, PCBs
heavy metalscadmiummercurylead
pesticide residuesBiological Contamination Bacteria
causing infection e.g. Salmonellacausing intoxication e.g. C. botulinum
Parasiteshelminths e.g. roundwormsprotozoa e.g. Giardia lamblia
Viruses e.g. Hepatitis A, Small Round-StructuredViruses (SRSVs)
Fungi/mycotoxins e.g. aflatoxinAlgae (e.g.dinoflagellates leading to paralytic
shellfish poisoning)
-
8/8/2019 WHO_Economic Impact of Foodborne Illness
12/12
Basic Food S afety for H ealth W orkers
Food is essential both for growth and forthe maintenance of life. It supplies theenergy and materials required to buildand replace tissues, to carry out work andto maintain the bodys defences againstdisease.
Food can also be responsible for ill-health.Failure to consume enough of the right kindof food will impede growth and impairhealth. For example, protein-energymalnutrition can lead to a range of clinicalmanifestations. These vary from marasmus,where consumption of protein, dietaryenergy and other nutrients are chronicallyreduced, to kwashiorkor (sometimesthought to be associated with an over-reliance on low protein staples) whichresults in a quantitative and qualitative
deficiency of protein (Table 1.1).
Food in health and
disease
C h a p t e r 1Foodborneillness
Even when a diet provides enough pro-tein and energy, it may not supply suffi-cient essential minerals or vitamins andmay thus give rise to characteristic defi-ciency disorders (Table 1.2).
Illness can also result from what a foodcontains rather than from what it lacks.
Some hazards of this kind are describedas being intrinsic to the food in the sensethat they are normal and natural constitu-ents of the food. Many common foodplants, for instance, contain toxic com-pounds designed to deter predators orinvading microorganisms. Their intake isinevitably higher in those people with alargely vegetarian diet.
However, in most cases where the food
supply is generally varied and plentiful,
Table 1.1 Classification of severe protein-energy malnutrition in children
Weight for age* With oedema Without oedema60 80% Kwashiorkor UndernutritionLess than 60% Marasmic kashiorkor Marasmus
* As % of standard (National Centre for Health Statistics) weightSource: Tomkins, AM Nutrition in clinical medicine. In: Textbook of Medicine. RL Souhami and J Maxham (eds) 2nd edn.Churchill Livingstone, Edinburgh, 1994: p.106.