
WHO Humanitarian Response 2013
52
Department for Emergency Risk Management and Humanitarian Response (ERM) 2013 WHO Humanitarian Compendium of health priorities and WHO projects in consolidated appeals and response plans Response
Transcript of WHO Humanitarian Response 2013

Department forEmergency Risk Management andHumanitarian Response (ERM)
2013 WHO Humanitarian
Compendium of health priorities and WHO projects in consolidated appeals and response plans
Response

© World Health Organization, 2013
All rights reserved. Publications of the World Health Organization are available on the WHO web site (www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]).Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press through the WHO web site (http://www.who.int/about/licensing/copyright_form/en/index.html).The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
Cover photograph: WHO/Marko Kokic
WHO/ERM/BRO/2013.2

iii
Wor
ld H
ealth
Org
aniz
atio
n h
uman
itaria
n re
spon
se in
20
13 Content0
Foreword 1
Afghanistan 2
Burkina Faso 4
Central African Republic 6
Chad 8
The Democratic Republic of the Congo 10
Djibouti 13
Haiti 15
Kenya 18
Mali 20
Mauritania 23
The Niger 25
The occupied Palestinian territory 27
The Philippines (Mindanao) 30
The Republic of South Sudan 32
Somalia 34
The Sudan 36
The Syrian Arab Republic 38
Yemen 41
Zimbabwe 43
List of Acronyms 45
References 46
2013

iv
World Health Organization humanitarian response in 2013
2012 DonorsThe World Health Organization would like to thank all of the donors that provided funding for WHO’s work in emergencies and humanitarian response in 2012. We look forward to strengthening our collaboration in order to meet the needs of vulnerable populations affected by humanitarian emergencies.The African Development Bank, Australia, Brazil, Canada, Denmark, Finland, France, Georgia, Germany, Ireland, Italy, Japan, the League of Arab States, Norway, Programme d’Investissement et de Développement rural des Régions du Nord Mali (PIDRN), Programme intégré de Développement rural de la Région de Kidal (PIDRK), the Republic of Korea, the Russian Federation, Saudi Arabia, Spain, SIMFER S.A., Switzerland, the Office of the United Nations Special Coordinator for the Middle East Peace Process, the United Kingdom, the United States of America, the Central Emergency Response Fund, the Common Humanitarian Fund, the European Commission Humanitarian Aid Office (ECHO), the International Fund for Agricultural Development, the OCHA Emergency Response Fund, United Nations Development Programme, the UN Assistance Mission for Iraq (UNAMI) and the UN Trust Fund for Human Security.

1
This compendium provides an overview of health priorities and WHO projects in the 19 consolidat-ed appeals and response plans that have been developed to meet humanitarian needs in protracted emergencies in Afghanistan, Burkina Faso, the Central African Republic, Chad, the Democratic Republic of the Congo, Djibouti, Haiti, Kenya, Mali, Mauritania, the Niger, the occupied Palestinian territory, the Philippines, the Republic of South Sudan, Somalia, the Sudan, the Syrian Arab Republic, Yemen and Zimbabwe in 2013.It is expected that, in addition to protracted emergencies with a consolidated or similar appeal in place, WHO will have to respond to numerous natural disasters and sudden onset emergencies throughout 2013. In 2012, WHO and partners carried out humanitarian response operations in 43 countries.One of the main concerns for WHO and its health partners is the downward trend of humanitarian funding for health. Despite the fact that the demand for health assistance during humanitarian crises throughout the world is increasing, funding for the health sector in 2012 significantly decreased com-pared to the previous year, both in percentage as well in nominal terms. While in 2011, the OCHA Financial Tracking Service (FTS) reported that 64% of the humanitarian health needs were met globally, 2012 only saw just above 50% of health needs covered. Health components of over one third of the consolidated appeals were funded below 30%. Humanitarian funding is crucial to support key health priorities in countries in crisis. There are some success stories: in the Democratic Republic of the Congo, funds raised through the consolidated ap-peals process contributed to the reduction of morbidity and mortality caused by easily treated diseases such as measles and cholera. Donor funding made possible a measles vaccination campaign that reached about 6.4 million children; 135 cholera kits providing medicines and supplies to treat diarrhoeal dis-eases for approximately 40 000 people were purchased and prepositioned in vulnerable areas. Another example is in the occupied Palestinian territory, where health partners were able to provide essential health and nutrition services to 95% of the target group (1.7 million people in the West Bank and Gaza). However, there are still many emergencies for which sufficient funding could not be secured. For exam-ple, in the Sahel region, despite the close linkage between malnutrition and health, health requirements were covered at only 27%, while nutrition was funded at 71% and food security at 77%. In the Syrian Arab Republic, hospitals and health facilities are reporting shortages of vaccines and life-saving medi-cines and supplies. Funding received in 2012 was far from sufficient to cover the gap. In Pakistan, with overall health funding requirements covered at only 13% in 2012, many health partners did not receive any funding at all. Shortages in funding affect the most vulnerable. The consequence of low health funding levels is that dozens of life-saving projects could not be implemented in 2012 and thousands of people in need of care could not be reached, particularly those who are most vulnerable, like pregnant and lactating women and children. The long list of countries with underfunded projects that were planned to ben-efit women and children includes Afghanistan, Burkina Faso, the Central African Republic, Chad, Côte d’Ivoire, Djibouti, Liberia, Mali, Mauritania, the Niger, Somalia and Lesotho.Staff qualified to respond to health emergencies are crucial for a meaningful humanitarian intervention. In some countries there is no funding available to cover the costs of core functions such as cluster co-ordination and management of emergency health information.2013 is a key year for the humanitarian community. The roll-out of the Inter-Agency Standing Committee Transformative Agenda is expected to be completed in 2013 and an extra effort is needed to ensure that the policies, guidelines and management structures that have been designed throughout 2012 are in place to ensure a swift, effective and coordinated response to emergencies.The donor community needs to assume its responsibilities too. Without donor support humanitarian agencies are helpless. Health strategies, programmes and projects are futile without reasonable fund-ing to support them. The importance of health actors receiving timely and predictable funds cannot be emphasized enough. The earlier in the programme cycle funding is received, the more strategic planning can be, the sooner health programmes can start, the more lives can be saved, and the better people whose lives have been devastated by disasters can be helped. And this is our mission: save lives and al-leviate suffering. We can only achieve this with sufficient donor support.
Foreword1
2
World Health Organization humanitarian response in 2013
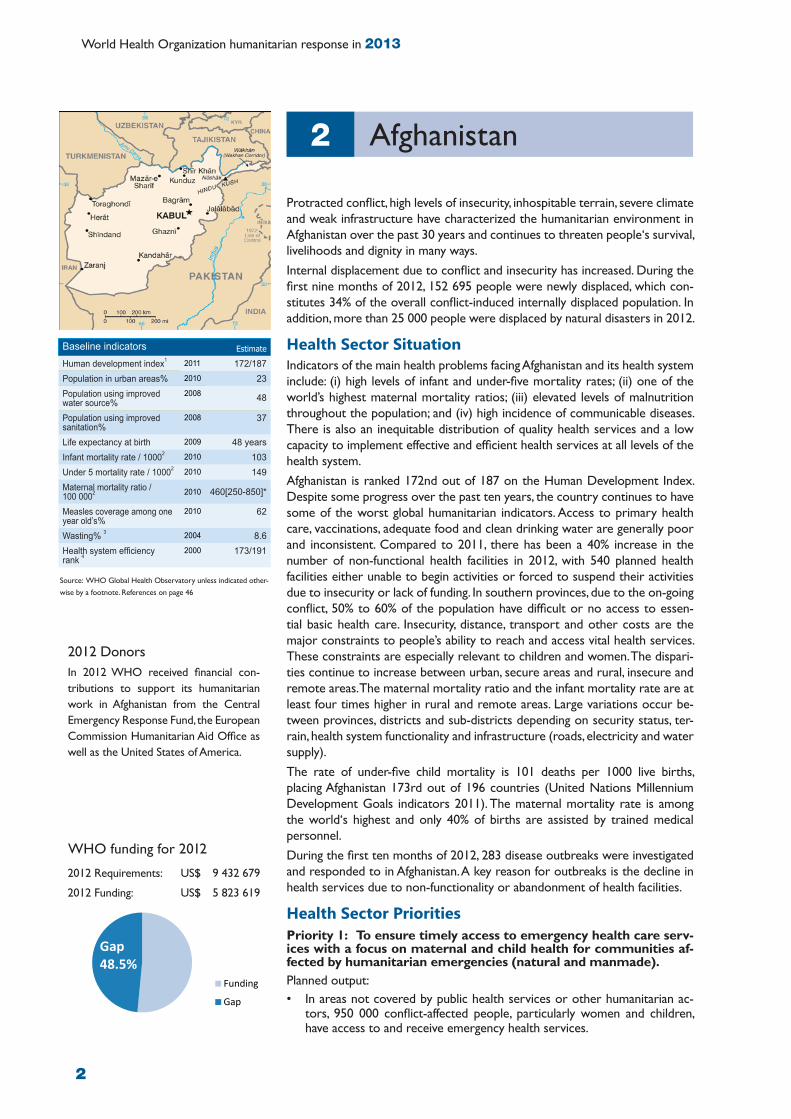
Protracted conflict, high levels of insecurity, inhospitable terrain, severe climate and weak infrastructure have characterized the humanitarian environment in Afghanistan over the past 30 years and continues to threaten people‘s survival, livelihoods and dignity in many ways.Internal displacement due to conflict and insecurity has increased. During the first nine months of 2012, 152 695 people were newly displaced, which con-stitutes 34% of the overall conflict-induced internally displaced population. In addition, more than 25 000 people were displaced by natural disasters in 2012.
Health Sector SituationIndicators of the main health problems facing Afghanistan and its health system include: (i) high levels of infant and under-five mortality rates; (ii) one of the world’s highest maternal mortality ratios; (iii) elevated levels of malnutrition throughout the population; and (iv) high incidence of communicable diseases. There is also an inequitable distribution of quality health services and a low capacity to implement effective and efficient health services at all levels of the health system. Afghanistan is ranked 172nd out of 187 on the Human Development Index. Despite some progress over the past ten years, the country continues to have some of the worst global humanitarian indicators. Access to primary health care, vaccinations, adequate food and clean drinking water are generally poor and inconsistent. Compared to 2011, there has been a 40% increase in the number of non-functional health facilities in 2012, with 540 planned health facilities either unable to begin activities or forced to suspend their activities due to insecurity or lack of funding. In southern provinces, due to the on-going conflict, 50% to 60% of the population have difficult or no access to essen-tial basic health care. Insecurity, distance, transport and other costs are the major constraints to people’s ability to reach and access vital health services. These constraints are especially relevant to children and women. The dispari-ties continue to increase between urban, secure areas and rural, insecure and remote areas. The maternal mortality ratio and the infant mortality rate are at least four times higher in rural and remote areas. Large variations occur be-tween provinces, districts and sub-districts depending on security status, ter-rain, health system functionality and infrastructure (roads, electricity and water supply). The rate of under-five child mortality is 101 deaths per 1000 live births, placing Afghanistan 173rd out of 196 countries (United Nations Millennium Development Goals indicators 2011). The maternal mortality rate is among the world‘s highest and only 40% of births are assisted by trained medical personnel. During the first ten months of 2012, 283 disease outbreaks were investigated and responded to in Afghanistan. A key reason for outbreaks is the decline in health services due to non-functionality or abandonment of health facilities.
Health Sector Priorities Priority 1: To ensure timely access to emergency health care serv-ices with a focus on maternal and child health for communities af-fected by humanitarian emergencies (natural and manmade).Planned output: • In areas not covered by public health services or other humanitarian ac-
tors, 950 000 conflict-affected people, particularly women and children, have access to and receive emergency health services.
Afghanistan2
WHO funding for 2012
Funding
Gap
Gap48.5%
2012 Requirements: US$ 9 432 679
2012 Funding: US$ 5 823 619
Baseline indicators Estimate
Human development index1 2011 172/187Population in urban areas% 2010 23Population using improved water source%
2008 48
Population using improved sanitation%
2008 37
Life expectancy at birth 2009 48 yearsInfant mortality rate / 10002 2010 103Under 5 mortality rate / 10002 2010 149Maternal mortality ratio / 100 0002 2010 460[250-850]*
Measles coverage among one year old’s%
2010 62
Wasting% 3 2004 8.6Health system efficiency rank 4
2000 173/191
2012 Donors In 2012 WHO received financial con-tributions to support its humanitarian work in Afghanistan from the Central Emergency Response Fund, the European Commission Humanitarian Aid Office as well as the United States of America.
Source: WHO Global Health Observatory unless indicated other-wise by a footnote. References on page 46

3
Priority 2: To strengthen the disease early warning mechanism and respond promptly to outbreaks that surpass the local response capacity across the country.Planned outputs:• A community-based disease early warning mechanism is established in 70 very high and high risk districts, and the
disease early warning system (DEWS) is strengthened.• Health Cluster partners are able to respond to more than 90% of outbreaks in a timely and efficient way.
Priority 3: To address the health needs of especially vulnerable groups requiring humanitarian aid (internally displaced persons (IDPs), refugees/returnees, persons in informal settlements and host communities)Planned outputs:• 50 000 IDPs in camps/camp-like settlements obtain access to emergency health services.• 50 000 IDPs living in host communities obtain access to emergency health.
Beneficiaries targeted by health partners in 2013Total: 1 608 000 (787 920 women and 820 080 men)
Geographical areas targeted by health partners in 2013Province: Districts:Nuristan Du Ab, Nurgaram, Mandol, Wama, Waygal, KamdeshHilmand Nad Ali, Dishu, Baghran, Nahri Saraj, Garmser, WasherKandahar Shah Wali Kot, Shorabank, Ghorak, Khakrez, Panjwayi, MaywandDaykundi Ishtarlay, Sangi Takht, Shahristan, GizabKunar Marawara, Dara I Oach, Shaygal Wa Shilitun, Chapa Dar, SarganiBadakhshan Kuf Ab, Kuran Wa Murjan, Khwahan, Kohistan, Raghistan, DarayimPaktika Waza Khawa, Wor Mayi, Gayan, BarmalFarah Bakwa, Khaki SafedLogar Azra, KharwarKabul District 5, 6, 8,9 (informal settlements)Khost Mando Zai, SpiraGhor Pasaband, Tulak, Lal Wa, SarjangalGhazni Bagrami Shahid, Andar, Zana Khan, NawaPaktya Jani Khail, Ali KhailHirat Adrashkan, Injil Badghis MugurUruzgan Shahidi Hassas, Khas Uruzgan Faryab Kohistan, Pashtun Kot
Health sector funding requirements for 2013 Health partners are appealing for US$ 16 913 808 for 2013Health partners appealing for funding in the 2013 appeal are: International Medical Corps, Humanitarian Assistance and Development Association for Afghanistan, Afghan Red Cross Society, United Nations Children’s Fund, Emergency, Bangladesh Rural Advancement Committee, Mercy Corps, Afghan Health and Development Services, Première Urgence Aide Médicale Internationale, Move Welfare Organization, United Nations Population Fund, Aga Khan Health Services, Medical Emergency Relief International, Care of Afghan Families, Coordination of Humanitarian Aid, Medical Services Corporation International, Serve Health Relief and Development Organization, German Agroaction, Terre Des Hommes, Healthnet International and Transcultural Psychosocial Organization, Agency for Assistance and Development of Afghanistan, Afghanistan Center for Training and Development, Sanayee Development Organization, Bakhtar Development Network, Emergency, Shuhada Organization, LEProsy COntrol, Swedish Committee for Afghanistan, Rural Rehabilitation Association for Afghanistan, Ibne Sina, Afghan Institute of Learning, International Assistance Mission, Afghan Transitional Authority, Securing Afghanistan’s Future and the World Health Organization.
WHO funding requirements for 2013WHO is requesting a total of US$ 9 000 000 for 2013

4
World Health Organization humanitarian response in 2013
In 2012, Burkina Faso, one of the world’s poorest countries, was severely af-fected by a food and nutrition crisis that had an adverse impact on the lives of an estimated 2.8 million people. While there have been regular rainfalls since, food security remains fragile as Burkina Faso’s population and agricultural pro-duction are highly vulnerable to weather-related incidents and the food assets of communities are exhausted. The conflict in northern Mali in early 2012 has further exacerbated the crisis as it led to an influx of refugees into Burkina Faso. In late 2012, about 36 000 Malian refugees were registered in Burkina Faso.
Health Sector SituationBurkina Faso has chronically high levels of food insecurity and malnutrition which were aggravated by the food and nutrition crisis in 2012 and thus wors-ened the already high global acute malnutrition (GAM) prevalence. The in-flux of Malian refugees further increased the pressure on Burkina Faso’s weak health system. Six out of ten children under the age of five die of pneumonia, malaria or di-arrhoea. Another 16% of mortality in this age group is due to birth-related conditions such as sepsis or prematurity. Measles outbreaks are recurrent. In recent years, epidemic diseases such as meningitis, cholera and measles have caused high levels of morbidity and mortality across all age groups. In 2012, the country simultaneously had to cope with a meningitis outbreak with 5300 suspected cases and 553 deaths (case fatality rate of 10%) and a measles out-break with 7607 suspected cases and 30 deaths (case fatality rate of 0.39%).
Health Sector Priorities Priority 1: To strengthen early warning and response systems for disease outbreaks throughout Burkina Faso and decrease the preva-lence of vaccine-preventable diseases.Planned output: • Improved prevention measures, earlier detection of disease outbreaks and
more rapid and efficient response to disease outbreaks such as meningitis, measles and cholera through the reinforcement of disease surveillance, out-break investigation, vaccination, training as well as the provision of the nec-essary medicines and equipment for case confirmation and management.
Priority 2: To decrease the risk and prevalence of diseases within the Malian refugee and host community populations.Planned outputs: • Children under two years of age and pregnant women among the Malian
refugee populations have access to routine vaccinations;• Refugees and host communities receive support in rapid HIV testing and
preventing mother-to-child transmission of HIV;• Support is extended for the prevention and treatment of malaria in refugee
camps and host communities, including through the distribution of insecti-cide-treated nets.
Priority 3: To reduce morbidity and mortality related to the food crisis Planned outputs: • Common paediatric diseases aggravated by malnutrition are treated and,
whenever possible, prevented.
Burkina Faso3
WHO funding for 20122012 Requirements: US$ 2 376 621
2012 Funding: US$ 787 977
FundingGap
Gap 66.8%
Baseline indicators Estimate
Human development index1 2011 172/187Population in urban areas% 2010 26Population using improved water source%
2008 76
Population using improved sanitation%
2008 11
Life expectancy at birth 2009 52 yearsInfant mortality rate / 10002 2010 93Under 5 mortality rate / 10002 2010 176Maternal mortality ratio / 100 0002 2010 300[190-520]*
Measles coverage among one year old’s%
2010 94
Wasting% 3 2009 11.3Health system efficiency rank 4
2000 132/191
2012 Donors In 2012 WHO received financial con-tributions to support its humanitarian work in Burkina Faso from the Central Emergency Response Fund and the European Commission Humanitarian Aid Office.
Source: WHO Global Health Observatory unless indicated other-wise by a footnote. References on page 46

5
• Integrated Management of Childhood Illness (IMCI) and nutritional care is improved through the promotion of case management skills of health care staff and improved family and community health practices.
• Medicines and consumables for anaemia prevention and blood for anaemia management are available.
Priority 4: To provide access to reproductive health/sexual and gender-based violence (SGBV)/HIV serv-ices in the regions that are most affected by drought and food insecurity.Planned outputs: • Assistance is provided to build the capacity of health service providers in the areas of reproductive health, SGBV
and HIV/AIDS, including through the support of formative supervision of health centres.• Quality, lifesaving reproductive health supplies and medical equipment are procured and available in sufficient
quantities.• The conduct of community mobilization and sensitization activities allows for increased access to reproductive
health services and care seeking.
Beneficiaries targeted by health partners in 2013Total: 7 405 530Most vulnerable women and young people (host community and refugees): 715 584
Geographical areas targeted by health partners in 2013Boucle du Mouhoun, Cascades, Centre, Centre Est, Centre Nord, Centre Ouest, Centre Sud, Est, Hauts Bassins, Nord, Plateau Central, Sahel and Sud Ouest.
Health sector funding requirements for 2013 Health partners are appealing for a total of US$ 7 116 962 Health partners appealing for funding in the 2013 appeal are: Médecins du Monde, United Nations Population Fund, United Nations Children’s Fund and the World Health Organization.
WHO funding requirements for 2013WHO is requesting a total of US$ 2 243 204 for the following projects:
Project titles Requested funds*
Response to the possible cholera outbreak in Burkina Faso BFA-13/H/55697
107 696
Reinforcement of management of anemia among pregnant and lactating women in 31 health dis-tricts affected by the 2012 food crisisBFA-13/H/55705
901 640
Reduction of morbidity and mortality related to the meningitis outbreakBFA-13/H/55708
446 102
Reinforcement of Integrated Management of Childhood Illness (IMCI) in areas affected by the food crisisBFA-13/H/55713
787 766
* Amounts given in US dollars.

6
World Health Organization humanitarian response in 2013
The Central African Republic has been in a state of crisis for many years. Underlying factors include extreme poverty as well as country-wide insecurity and violence due to unpredictable armed-group activities, crimes by armed bandits, and tensions between migrating and local farmers. State presence is weak outside the capital and its capacity to protect civilians is limited. Due to the conflict, more than 23 500 Central Africans were newly displaced in 2011 and 27 800 in 2012. The total number of displaced people is estimated to be 98 900.
Health Sector SituationAccording to WHO data, the Central African Republic has the world’s fifth highest death rate from infectious and parasitic diseases and is one of the countries with the shortest life expectancy (48 years) and the worst mortal-ity indicators:• Infant mortality rate of 106 per 1000 live births • Under-five mortality rate of 159 per 1000 live births with malaria being the
leading cause of mortality (28%), followed by pneumonia (17%) and diar-rhoea (14%).
• Maternal mortality ratio of 890 for 100 000 live births The health structure in the Central African Republic is extremely weak, sub-stantial gaps in the response to the population’s most basic health needs re-main when it comes to access to immediate life-saving health care, including access to emergency obstetric care and treatment of injuries resulting from conflict, as well as care for the treatment of endemic diseases, epidemics and immunization. The risk of malaria, cholera and diarrhoeal diseases is prevalent all year, but reaches a peak during the rainy season in July and August. The routine Expanded Programme on Immunization (EPI) coverage is poor, provoking high rates of vaccine-preventable diseases endemic to the Central African Republic, including measles, meningitis, neonatal tetanus, pertussis, yellow fever and polio. According to WHO global statistics, only 62% of one-year-olds in the Central African Republic were immunized against measles in 2010, which is 22.5% be-low the regional average. Reasons for poor vaccination coverage often include missed campaigns due to surges in violence, people living long distances away from vaccination sessions, unavailability of services and lack of knowledge due to poor health education.
Health Sector Priorities Priority 1: To improve access to emergency health services, includ-ing access to emergency basic and secondary health care for both the vulnerable and host populations of crisis-affected health districts and decrease the rate of vaccine preventable diseases. This includes strengthening/implementing Integrated Management of Childhood Illness (IMCI) and the Minimum Initial Service Package for repro-ductive health (MISP).
Planned outputs:• Crisis affected populations have access to free or subsidized emergen-
cy care in public health facilities that are supported by NGOs and UN agencies.
• Qualified health staff is available through the support of regional health sub-clusters.
The Central African Republic4
WHO funding for 20122012 Requirements: US$ 3 736 861
2012 Funding: US$ 1 537 642
FundingGap
Gap 58.9%
Baseline indicators Estimate
Human development index1 2011 179/187Population in urban areas% 2010 39Population using improved water source%
2008 67
Population using improved sanitation%
2008 34
Life expectancy at birth 2009 48 yearsInfant mortality rate / 10002 2010 106Under 5 mortality rate / 10002 2010 159Maternal mortality ratio / 100 0002 2010 890 [530-
1700]*Measles coverage among one year old’s%
2010 62
Wasting% 3 2006 12.2%Health system efficiency rank 4
2000 189/191
2012 Donors In 2012 WHO received financial con-tributions to support its humanitarian work in the Central African Republic from the Central Emergency Response Fund, the Russian Federation and Spain.
Source: WHO Global Health Observatory unless indicated other-wise by a footnote. References on page 46

7
• Health facilities have affordable emergency medicines and equipment available, including emergency medical, surgi-cal and obstetric kits. Targeted health facilities are able to cope with the clinical management of rape survivors and have emergency contraception and post-exposure prophylaxis kits available.
• Immunization coverage for vaccine preventable diseases such as measles is increased (to at least 95% of the target population in the case of measles).
Priority 2: To strengthen the capacity of local community and health districts authorities to prevent, prepare for and respond to disaster and health crisesPlanned outputs:• Existing institutional/community mechanisms to track public health events, prevent, prepare for and respond to dis-
asters and humanitarian crises are strengthened with a focus on the northern Central African Republic (meningitis belt) and the southern Central African Republic (health prefectures at risk of cholera).
• Health stakeholders are strengthening early warning of public health event and disease surveillance activities through decentralized health sub-clusters involving community-based committees in disaster management.
• The local and regional health sub-cluster mechanism for information sharing, public health event tracking and prompt response to crises is reinforced.
Beneficiaries targeted by health partners in 2013Total: 601 510Women: 246 377 (residents), 138 812 (HIV/AIDS affected), 306 (gender-based violence survivors)
Geographical areas targeted by health partners in 2013Vulnerable people in five heath regions and 14 districts:• Health region 2: Mambéré-Kadéï, Sangha-Mbaéré and Nana-Mambéré• Health region 3: Ouham and Ouham-Pendé• Health region 4: Ouaka, Kémo and Nana-Gribizi• Health region 5: Vakaga, Haute-Kotto and Bamingui-Bangoran• Health region 6: Base-Kotto, Mbomou and Haut-Mbomou.
Health sector funding requirements for 2013 Health partners are appealing for a total of US$ 12 913 936 Health partners appealing for funding in the 2013 appeal are: International Medical Corps United Kingdom, Première Urgence-Aide Médicale Internationale (First Emergency- International Medical Aid), United Nations Population Fund, Initiative pour le Développement de Centrafrique (Central Africa Development Initiative), United Nations Children’s Fund, Medical Emergency Relief International, Micronutritient Initiative and the World Health Organization.
WHO funding requirements for 2013WHO is requesting a total of US$ 2 472 933 for the following projects:
Project titles Requested funds*Strengthening a prompt and coordinated health cluster response to disaster and health crises in post-conflict affected health districts of the Central African Republic CAF-13/H/55854/122
1 294 700
Promoting Integrated Management of Childhood Illness (IMCI) and strengthening routine im-munization in northern and southern regions of the Central African RepublicCAF-13/H/56251/122
1 178 233
* Amounts given in US dollars.

8
World Health Organization humanitarian response in 2013
Food insecurity, floods and population displacements characterized 2012 in Chad. An estimated 1.8 million people in Chad were affected by food insecu-rity in 2012. Floods affected over half a million people and led to the displace-ment of thousands. The Libyan crisis has forced more than 90 000 Chadian workers to return, often to areas with high food insecurity and that lack basic services. This has further strained the livelihoods of the disaster-affected popu-lation. An estimated 290 000 Sudanese refugees remain in eastern Chad and about 60 000 Central African refugees in the south of the country. In addition, about 90 000 Chadians are still internally displaced in a country that is suffer-ing from chronic poverty and institutional weaknesses.
Health Sector SituationThe maternal mortality rate in Chad is the highest worldwide with 1100 per 100 000 live births. Most deaths of children under the age of five (76%) can be attributed to diarrhoea, malaria, pneumonia or birth-related factors (i.e. as-phyxia, premature birth, neonatal sepsis and congenital abnormalities). Every year, Chad faces a meningitis and measles epidemic in the southern and western part of the country. Furthermore, chronic malnutrition is a serious public health problem with the prevalence of global acute malnutrition (GAM) being as high as 18.1% in Chad’s Sahel region. According to standard WHO classification, the nutritional situation in Chad’s Sahel region is “critical”.The floods that ravaged many parts of Chad (east, south, south-west and cen-tre) in 2012 caused extensive material damage and loss of life, and significantly increased people’s vulnerability. Following the floods, the risk of faecal-oral di-arrhoeal diseases, especially cholera, remains high in the affected areas. Given the recurring nature of epidemics such as cholera, prevention and prepared-ness for diseases with epidemic potential are priorities. In 2011, about 17 000 cholera cases including 455 deaths were reported. The floods also damaged health-centre infrastructure and disrupted health services in affected regionsDamaged roads and swollen rivers made it difficult to access affected areas and limited the continuity of ongoing health programmes. The floods accentuated the poor hygiene and sanitation in affected regions, which increased the inci-dence of acute watery diarrhoea and malaria cases.
Health Sector Priorities Priority 1: To increase general access to and use of primary health services with an emphasis on providing immunization along with HIV/AIDS, sexual and gender-based violence and reproductive health services.Planned outputs: • At least 75% of the target population receives medical treatment as well as
immunization.• At least 80% of the target health facilities have essential drugs and other
medical consumables available without stock-outs. This includes emergency health kits, reproductive health kits as well as laboratory supplies for emer-gency health care response to crisis.
• Mass immunization campaigns of populations at risk of measles and menin-gitis are conducted and at least 85% of children under five years of age in target areas are immunized against measles and other illnesses covered by the Penta 3 vaccine.
• At least 50% of the target health facilities have prevention of mother to child transmission (PMTCT) of HIV and voluntary counseling and testing (VCT) services available.
Chad5
WHO funding for 20122012 Requirements: US$ 13 971 067
2012 Funding: US$ 1 377 066
FundingGap
Gap 90.1%
Baseline indicators Estimate
Human development index1 2011 179/187Population in urban areas% 2010 28Population using improved water source%
2008 50
Population using improved sanitation%
2008 9
Life expectancy at birth 2009 48 yearsInfant mortality rate / 10002 2010 99Under 5 mortality rate / 10002 2010 173Maternal mortality ratio / 100 0002 2010 1100 [640-
2000]*Measles coverage among one year old’s%
2010 46
Wasting% 3 2004 16.1Health system efficiency rank 4
2000 178/191
2012 Donors In 2012 WHO received financial contri-butions to support its humanitarian work in Chad from the Central Emergency Response Fund and Spain.
Source: WHO Global Health Observatory unless indicated other-wise by a footnote. References on page 46
9
• Gender-based violence cases referred to health facilities are correctly managed and receive the appropriate medical treatment.
• At least 30% of deliveries are assisted by trained staff in target health facilities.• At least 50% of women between 15 and 45 years of age in target areas have two ante-natal consultations.• At least 10% of women between 15 and 45 years of age in target areas utilize family planning services.
Priority 2: To rapidly detect and prevent disease outbreaks, as well as to ensure rapid medical care to populations affected by epidemics and/or malnutritionPlanned outputs: • Weekly disease surveillance reports are submitted in a timely manner to the National Surveillance Service, and
rapid investigation of suspected and rumoured cases is supported. • At least 50% of health facilities in target regions have staff trained on early warning systems. • Contingency stocks of essential medicines, laboratory reagents and medical consumables are available in target ar-
eas to control case fatality rates in the case of cholera, meningitis and measles outbreaks. • Health worker refresher training courses for epidemic response and control are conducted.• Mobile clinics are set up to provide outreach for referral of severe acute malnutrition with medical complications
in nomadic populations and remote areas, and therapeutic nutrition centres are provided with emergency pae-diatric medicines and laboratory supplies for proper management of the medical complications of severe acute malnutrition.
Priority 3: To strengthen the capacity of the health system and communities to recover after epidemics and natural disastersPlanned outputs:• After a crisis at least 50% of health facilities in affected regions have a community health committee for population
mobilization and management of health facilities in place.
Beneficiaries targeted by health partners in 2013Total: 1 795 751 (970 435 women and 825 316 men)
Geographical areas targeted by health partners in 2013Areas targeted by partners are defined according to the prevalence of disease. The population most affected by cholera outbreaks is mainly located in the regions bordering Lake Chad as well as Logone and Chari rivers. The west and south east are most at risk of meningitis and measles outbreaks. Refugees are located in eastern and southern Chad, while nutrition medical response will target the Sahel belt.
Health sector funding requirements for 2013 Health partners are appealing for a total of US$ 28 681 269 in 2013 Health partners appealing for funding in the 2013 appeal are: Cooperazione Internazionale (International Cooperation), Première Urgence Aide Médicale Internationale, United Nations Children’s Fund, International Organization for Migration, United Nations Population Fund, United Nations Joint Programme on HIV/AIDS and the World Health Organization.
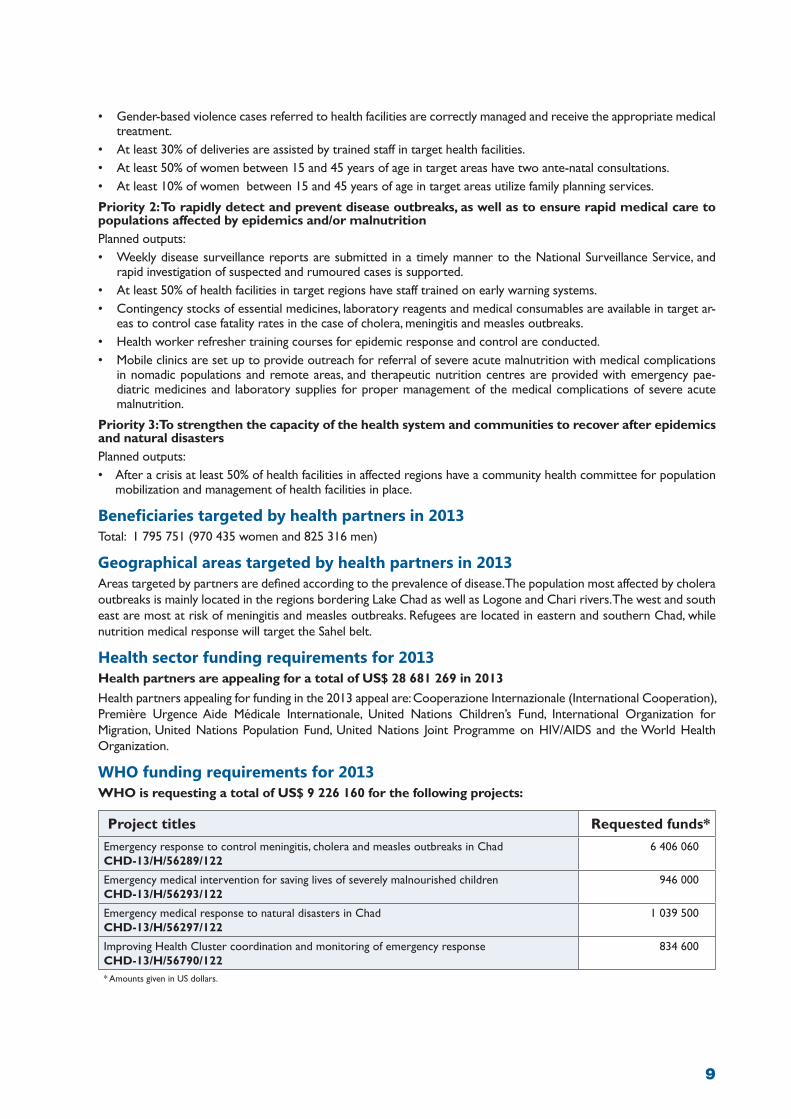
WHO funding requirements for 2013WHO is requesting a total of US$ 9 226 160 for the following projects:
Project titles Requested funds*Emergency response to control meningitis, cholera and measles outbreaks in Chad CHD-13/H/56289/122
6 406 060
Emergency medical intervention for saving lives of severely malnourished children CHD-13/H/56293/122
946 000
Emergency medical response to natural disasters in Chad CHD-13/H/56297/122
1 039 500
Improving Health Cluster coordination and monitoring of emergency response CHD-13/H/56790/122
834 600
* Amounts given in US dollars.

10
World Health Organization humanitarian response in 2013
The Democratic Republic of the Congo has been facing a complex humanitar-ian crisis for more than ten years. The main drivers of the crisis include:• Conflict and armed violence: this is particularly prevalent in the east of
the country and includes murder, inhuman treatment, abduction, forced re-cruitments and looting of villages.
• High numbers of displaced persons and refugees: there are an estimated 2.4 million people displaced inside the Democratic Republic of the Congo (as of early October 2012). South Kivu, North Kivu as well as Province Orientale and Katanga are the most affected provinces.
• An alarming sanitary, health and nutritional situation: maternal and child mortality levels are high, disease outbreaks are frequent and access to basic health care is weak.
• Local political instability as well as a general context of poverty and insecu-rity: 70% of the population is living below the poverty line.
Health Sector SituationProlonged instability and chronic emergencies in eastern Democratic Republic of the Congo have had a significant impact on the health of displaced and vul-nerable populations throughout the country. The affected population is having difficulties in accessing water, health care and basic services, which puts thou-sands of people at risk of disease outbreaks. There has been a major increase in epidemics across the whole country in 2012, including measles, cholera and viral haemorrhagic fevers among others.• While cholera cases have decreased in the western provinces, eastern
provinces are experiencing a resurgence of cholera cases since July 2012. In North Kivu, cholera is on the rise again, especially in Masisi and Kirotshe health zones, where fighting continues. In Karisimbi health zone, where Kanyaruchinya refugee camp has been established, there has been a worry-ing increase in cholera cases. Triggering factors include the lack of latrines and clean water sources and renewed violence.
• From January to November 2012, 54 909 cases of measles with 1509 deaths (case fatality rate of 2.7%) in 102 health zones were reported.
• Viral haemorrhagic fevers: there has been an outbreak of yellow fever in Equateur province. There hasn’t been a vaccination campaign for yellow fever in this area for the past 10 years. As of 6 November 2012, 77 cases (36 laboratory confirmed, 17 probable, and 25 suspected) of Ebola haem-orrhagic fever have been reported in Orientale Province. Of these, 36 have been fatal (12 confirmed and 13 probable).
The amelioration of obstetric care in the Democratic Republic of the Congo is a main priority, with a maternal mortality ratio of 540 per 100 000 live births and the death of one in four children under five being attributed to birth relat-ed causes such as prematurity, sepsis or asphyxia. Health partners are report-ing an increase in obstetrical emergencies.It is estimated that more than 17.3 million people are in an acute food crisis, of whom more than 315 000 are facing a humanitarian emergency. The causes of the food crisis include factors such as population displacement, insecurity, lack of access to food, and loss of livelihood.Health partners are facing major challenges in terms of security, access, com-munication and logistics. Communication challenges affect surveillance and early warning in remote areas of this vast country.
The Democratic Republic of the Congo6
2012 Requirements: US$ 38 400 000
2012 Funding: US$ 11 437 589
Baseline indicators Estimate
Human development index1 2011 187/187Population in urban areas% 2010 35Population using improved water source%
2008 -
Population using improved sanitation%
2008 -
Life expectancy at birth 2009 49 yearsInfant mortality rate / 10002 2010 112Under 5 mortality rate / 10002 2010 170Maternal mortality ratio / 100 0002 2010 540 [300-
1100]*Measles coverage among one year old’s%
2010 68
Wasting% 3 2006 14.0Health system efficiency rank 4
2000 188/191
2012 Donors In 2012 WHO received financial contri-butions to support its humanitarian work in the Democratic Republic of the Congo from Finland, Italy, the Russian Federation, the Central Emergency Response Fund and the Common Humanitarian Fund.
FundingGap
Gap 67%
WHO funding for 2012
Source: WHO Global Health Observatory unless indicated other-wise by a footnote. References on page 46

11
Health Sector Priorities The health priorities for the country must consider the differing needs of the health zones in the east and west of the country. The western provinces have a persistently weak health system which increases the risk of disease outbreaks. The conflicts in the eastern provinces are causing an alarming humanitarian situation.Planning figures for North Kivu indicate 250 000 people in need of urgent health assistance. There is a need for medi-cal supplies for emergency health services including surgery (e.g. trauma kits and transfusion kits), basic health services with preventive care and response to disease outbreaks.The main health priorities are to:• Increase access to a minimum package of health services including required life-saving interventions such as basic
health care, surgical services and emergency obstetric care to reduce maternal and child mortality.• Promote access to water and sanitation in areas at high risk for the spread of epidemics.• Strengthen technical and institutional capacities in the surveillance and response to diseases with epidemic potential.• Strengthen coordination of health partners to improve contingency plans and adapt responses to emerging
situations.• Strengthen capacities of communities, women and men, girls and boys, to reduce the risk of communicable diseases
and to mitigate the impact of recurrent epidemics.
Beneficiaries targeted by health partners in 2013• 3 396 700 displaced people and host families• 9 250 000 people affected by disease outbreaks• 1 911 800 women, pregnant women, girls and boys under five, persons living with HIV/AIDS and other vulnerable
persons• 1500 health staff
Geographical areas targeted by health partners in 2013• Provinces with weak health systems (mainly western provinces): Katanga (except Tanganyika), Kasaï Oriental, Kasaï
Occidental, Bandundu, Bas Congo, Equateur, and Tshopo District in Province Orientale.• Provinces with a tense humanitarian situation related to conflict (mainly eastern provinces): North Kivu, South Kivu,
Tanganyika District in Katanga Province, Maniema and Hubu Province (Bas-Uele, Haut-Uele) and Ituri in Province Orientale.
Health sector funding requirements for 2013 Health partners are appealing for a total of US$ 79 506 600 in 2013. Health partners appealing for funding in the 2013 appeal are: World Health Organization, United Nations Childen’s Fund, United Nations Population Fund, United Nations High Commissioner for Refugees, United Nations Development Programme/Global Fund, United Methodist Committee on Relief, Adventist Development and Relief Agency, The Alliance of International Medical Action, Care International, Médecins d’Afrique, Heal Africa, Medair, International Medical Corps, International Rescue Committee, Johanniter, Vétérinaires Sans Frontières Suisse, World Vision, Union Nationale des Femmes, Solidarité Pour la Promotion Sociale et la Paix, Save the Children, Medicos En Catastrophe, International Emergency and Development Aid Relief, Hope in Action, Heal Africa, Handicap International Belgique, Communication Information Formation – Santé, CACDFE, Action Humanitaire Pour la Santé et le Développement Communautaire, Doctors on Call for Service, Agir Ensemble, ALAD, Netrese, Universud, Red Cross DRC, Association Internationale de Cancer de Sein International, Caritas, Caritas Dungu, Caritas Bunia, Bureau Diocésain des Œuvres Médicales (BDOM), BDOM Bukavu, BDOM Boma, BDOM Matadi, Helpage International, IDESAFARP CACDEF, IRS, Lutte contre la délin-quance et l’exode rural, ANAM, Promotion et Complémentarité des Cultures pour le Développement, Green Bay Congo, Merlin, Première Urgences - Aide Médicale Internationale, Catholic Relief Services, Malteser International, People in Need, Associazione Volontari per il Servizio Internazionale, Médecins d’Afrique, Association de Santé Familiale/PSI, Louvain Développement, Cap Anamur, PMU inter life, Ruban Blanc, Médecins du Monde Belgique, Médecins du Monde France, Cooperazione e Sviluppo, Cooperazione Internazionale, Magna, Action Santé Femme, Action Contre la Faim/USA, UBS, Amis des Personnes en Détresse, Eglise du Christ au Congo, Aide et Action pour la Paix, Centre Régional d’Appui et de Formation pour le Développement, Conseil National des ONG de Santé en RDC, ECOS, CAPSA, Solidarité des Femmes pour le Développement Integral, ADES, PIAD, Eglise du Christ au Congo – Ministère de l’Eglise pour les Réfugiés et les Urgence, Projet Panzi Hospital Bukavu, 8e Communauté des Eglises de Pentecôte en Afrique Centrale, Communauté des Eglises Libres de Pentecôte en Afrique, Fédération des Droits de l’Homme, Management Sciences for Health/Strengthening Pharmaceutical Systems (SPS) Program, Development Alternatives Inc./USAID,

12
World Health Organization humanitarian response in 2013
Orebo, Assicas RD Congo, Eglise du Christ au Congo – IMA World Health, Cadimek, Action Nourriture Pour Tous, AHUDASEC, CREP/GL, Association D’encadrement des Personnes Infectées Par l’Hépatite/SOS Hépatites, Helen Keller International, Promotion et Complémentarité des Cultures pour le Développement, Save the Children United Kingdom, Universud, European Commission Humanitarian Aid Office, Association Régionale d’Approvisionnement enMédicaments Essentiels, MAS, Hope In Action, Programme National des Urgences et Action Humanitaire (PNUAH) of the Ministry of Public Health (MoPH), MoPH Directorates 4 and 9, Provinical Health Inspectorats, Bureaux des zones de Santé, Département Provincial de la Santé.Observers : International Committee of the Red Cross, Médecins Sans Frontières Netherlands, Médecins Sans Frontières France, Médecins Sans Frontières Suisse, Médecins Sans Frontières Espagne, International Organization for Migration.
WHO funding requirements for 2013WHO requires US$ 47 700 000 to carry out the priority health interventions below:
Project titles Requested funds*Response to the cholera outbreak in 165 health zones 12 000 000
Response to measles outbreaks (immunization and case management) 16 000 000
Minimum health care package (mainly in eastern provinces) 11 000 000
Support to coordination 500 000* Amounts given in US dollars.
project code DRC-13/H/56800/5826

13
Djibouti7
Baseline indicators Estimate
Human development index1 2011 165/187Population in urban areas% 2010 76Population using improved water source%
2008 92
Population using improved sanitation%
2008 56
Life expectancy at birth 2009 60 yearsInfant mortality rate / 10002 2010 73Under 5 mortality rate / 10002 2010 91Maternal mortality ratio / 100 0002 2010 200 [100-
410]*Measles coverage among one year old’s%
2010 85
Wasting% 3 2006 26.0Health system efficiency rank 4
2000 157/191
Recurrent drought, compounded by the increasing prices of basic commodi-ties and a general context of poverty, is affecting more than 210 000 persons in Djibouti and has had adverse effects on food security and livelihoods. There are also 26 000 refugees in the country, mainly from Somalia, as well as about 65 000 migrants on their way to Yemen and the Arab peninsula. Direct assist-ance is needed for refugees, migrants and host communities alike.
Health Sector SituationThe Djiboutian health system underperforms in its capacity to prevent, rapidly detect and respond to communicable diseases and epidemics. The most com-mon diseases, especially among children, are diarrhoeal and respiratory dis-eases including tuberculosis.The risks associated with such communicable diseases are compounded by the following factors:• The difficulty of positioning and stockpiling vaccines and medicines at
health centres and low immunization coverage; • Long lags in response time, due to understaffing and underfinancingThere is a general funding gap for prevention and awareness raising activities for diseases such as HIV/AIDS and tuberculosis. Screening tests, monitoring and patient support activities had to be discontinued in several instances.An additional health concern is the fact that the Djiboutian health system has great difficulty addressing the health needs of households affected by drought, People in rural areas who do not have sufficient means to cover health service costs are of particular concern,
Health Sector Priorities Priority 1: Reducing mortality and morbidity related to malnutri-tion and epidemics by at least 50% in the target Djiboutian popula-tion, particularly among children. Assisting migrants and their host communities in accessing health services.Planned outputs:• 50% of the target population in rural areas with no access to a health cen-
tre is covered by a monthly visit of a mobile health team or nurse.• 80% of the 30 target health posts are equipped to adequately stock vac-
cines and medicines. The cold chain can be maintained in all target health centres.
• The number of health centres and health posts that experience stock outs of essential medicines is reduced by 30%.
Priority 2: Strengthen the disease early warning system and surveil-lance capacities, particularly for diseases such as diarrhoea, measles, tuberculosis and HIV/AIDS and step up prevention and response.Planned outputs:• 25 out of 30 target health posts and five out of five target health cen-
tres have the necessary equipment to detect potentially epidemic diseases and respond appropriately via either treatment or referral (particularly for pregnant women).
• Suspected cases of epidemic-prone diseases in rural areas are detected within 72 hours and a response plan is established promptly.
• 75% of the population affected by acute diarrhoea is detected and treated within 72 hours.
• 80% of the target rural population is vaccinated against measles.
WHO funding for 20122012 Requirements: US$ 2 729 910
2012 Funding: US$ 400 582
FundingGap
Gap 85.3%
2012 Donors In 2012 WHO received financial contri-butions to support its humanitarian work in Djibouti from the Central Emergency Response Fund.
Source: WHO Global Health Observatory unless indicated other-wise by a footnote. References on page 46

14
World Health Organization humanitarian response in 2013
• Health information is collected from health structures (and mobile staff in rural areas), on a weekly basis and ana-lysed monthly.
• Vulnerable target populations are more aware of the risks, recognize the symptoms and react more appropriately to signs of potentially epidemic diseases and malnutrition. To that effect, posters will be printed and distributed to health facilities as well as youth and women’s associations.
Priority 3: Strengthen synergies between the health sector, social networks and communities.Planned outputs:• Data collected through studies on food security, nutrition and health are linked, analyzed, conclusions drawn and
brought forward through discussion in “focus groups”.• 20 pairs of trainers (four in each region) are trained on the prevention of communicable diseases and malnutrition
in drought-affected areas.• 40 awareness-raising sessions for drought-affected populations are conducted through the above-mentioned pairs
of trainers.
Priority 4: Develop the capacity of health authorities to strengthen health aspects in policies relating to disaster risk management and response.Planned outputs:• Health sector vulnerability study conducted.• Discussions held with Ministries and other authorities to improve understanding on health promotion, disaster risk
management, preparedness and response matters, both at national and regional level.• Capacity of authorities in emergency response strengthened through the establishment of regional response plans.
Beneficiaries targeted by health partners in 2013• Total: 217 000 people (101 000 women and 116 000 men)• Population with drought-related health problems: 152 000• Population at risk of epidemic diseases: 40 000• Migrants: 25 000 (refugees are targeted under a multi-sector response)
Geographical areas targeted by health partners in 2013Region: Coverage:Ali Sabieh MoH, WHO, UNFP and UNAIDSArta MoH, WHO, UNFP and UNAIDSDikhil MoH, WHO, IOM, UNFPA and UNAIDSObock MoH, WHO, IOM, UNFPA and UNAIDSTadjourah MoH, WHO, IOM, UNFPA and UNAIDSDjibouti-ville MoH, WHO, UNFPA and UNAIDSNational MoH and WHO
Health sector funding requirements for 2013 Health partners are appealing for a total of US$ 2 469 301 Partners appealing for funding within the health sector in the 2013 appeal are the World Health Organization and the Joint United Nations Programme on HIV/AIDS (note: agencies are also appealing for funding within the multi-sector response).
WHO funding requirements for 2013WHO is appealing for a total of US$ 2 542 086 (within the framework of both the health sector and the multi- sector response) for the following projects:
WHO Proposed Projects
Project titles Requested funds*Strengthening the synergy between health and social networks and community activities DJI-13/H/57064/122
172 785
Reduction and mitigation of the consequences of drought on the affected population DJI-13/H/57066/122
1 604 251
Epidemic response managementDJI-13/H/57069/122
765 050
* Amounts given in US dollars.

15
Three years have passed since the devastating earthquake that struck Haiti in January 2010 and caused more than 217 000 deaths, destroyed the homes of more than two million people and displaced more than 1.5 million people. The Government and humanitarian actors were able to help return or relocate almost 80% of these people out of camps. However, despite some improve-ments in the lives of the disaster-affected population, significant humanitarian needs remain. Even though the overall number of cholera cases following the 2011 outbreak has decreased, localized outbreaks in remote areas are on the rise while response capacities have diminished due to lack of available funding. Another concern is the food security situation which is deteriorating and now affecting over two million people. The 2012 tropical storms Isaac and Sandy have re-emphasized the fragility of both the population and the national disas-ter response capacity.
Health Sector SituationCholera continues to be an important public health concern. As of 27 November 2012, the Ministry of Public Health and Population reported 621 660 cases of cholera and 7759 deaths since the onset of the cholera epi-demic in October 2010. While the epidemic saw a steady decline in new in-fections and case fatality rates in 2012, Haiti is presently facing an increase in the frequency and number of cases of cholera in several departments identi-fied as the most vulnerable: the West (including Port-au-Prince), Artibonite, the Centre, the South, the South-east, Jeremie, Cap Haitien and Port de Paix.This increase is mainly due to: 1) the rainy season; 2) the cyclone season and in particular the passage of tropical storms Isaac and Sandy in 2012; and 3) the subsequent flooding which affected large parts of the country.Considering the current trends of morbidity, an estimated 118 000 people could fall victim to the epidemic during 2013. With the scaling down of hu-manitarian funding and the resulting decline in the number of international non-governmental organizations operating in the country, providing an ade-quate response to outbreaks has become increasingly difficult. The Ministry of Health is facing serious financial challenges and is unable to guarantee the continuation and functioning of cholera facilities.The precarious situation with regard to water supply systems and poor access to sanitation facilities throughout the country is the key determinant of the evolution of the disease. This is especially true in isolated rural communities where cholera persists even outside the rainy season and from where the dis-ease then spreads to other areas during the rainy season. General access to medical facilities is a challenge and access to clean water in medical facilities is often not possible, particularly in the South, South-east and Grande Anse Departments. The epidemiological surveillance system established by the Ministry of Health does not provide comprehensive, reliable data. A strengthening of the system is urgently needed, particularly at the commune level.
Health Sector Priorities Priority 1: To prevent the spread of cholera and other infectious diseases.Planned outputs: • Improved access to water in 69 health facilities providing treatment for
acute diarrhoea through the evaluation of water supplies and regular
Haiti8
WHO funding for 20122012 Requirements: US$ 4 317 421
2012 Funding: US$ 1 700 075
FundingGap
Gap 60.6%
Baseline indicators Estimate
Human development index1 2011 158/187Population in urban areas% 2010 52Population using improved water source%
2008 63
Population using improved sanitation%
2008 17
Life expectancy at birth 2009 62 yearsInfant mortality rate / 10002 2010 70Under 5 mortality rate / 10002 2010 165Maternal mortality ratio / 100 0002 2010 350[210-610]*
Measles coverage among one year old’s%
2010 59
Wasting% 3 2006 10.3%Health system efficiency rank 4
2000 138/191
2012 Donors In 2012 WHO received financial con-tributions to support its humanitarian work in Haiti from Canada, Finland, the Central Emergency Response Fund and the OCHA Emergency Response Fund.
Source: WHO Global Health Observatory unless indicated other-wise by a footnote. References on page 46

16
World Health Organization humanitarian response in 2013
water tests, maintenance and rehabilitation works of water supply systems, as well as integrating the monitoring and evaluation systems of health centres into the national surveillance systems for water quality.
• Improved sanitation facilities, hygiene promotion and infection control measures in 69 health facilities providing treatment for acute diarrhoea, through the evaluation of sanitation facilities and implementation of the necessary follow-up measures, training of health workers as well as improved disinfection and waste-disposal mechanisms.
• Improved general awareness and knowledge of cholera prevention, among populations in remote or isolated areas at risk of cholera, through the training and mobilization of community workers as well as communication campaigns.
Priority 2: To provide swift and adequate medical care to victims of the cholera outbreak by supporting health authorities in their efforts to strengthen medical response capacities at the decentralized levelPlanned outputs:• Cholera victims receive adequate treatment within 48 hours following an alert by rapid response teams following
the creation and training of rapid response teams as well as the pre-positioning of medical kits and material in all target areas.
• The Ministry of Health’s capacity to provide adequate treatment to victims of cholera is strengthened through train-ing hospital staff on the application of cholera treatment protocols and providing essential medicines and supplies to 69 cholera treatment facilities.
• The epidemiological surveillance system is strengthened, including at the community level, to detect new outbreaks early and ensure their close monitoring. Key measures in this area include the analysis of data and the production of regular epidemiological surveillance reports at the department level.
Priority 3: To reinforce the national public health emergency preparedness and response capacitiesPlanned outputs:• Coordination mechanisms are established at the national and departmental level, including all departments of the
Ministry of Health and the Direction de la Protection Civile (DPC), in collaboration with community focal points, referral hospitals and the ambulance system.
• Medical emergency response capacities of ten departments are reinforced through the pre-positioning of medi-cal emergency kits in each of the departments to cover the health needs of one percent of the population for one week, in accordance with the plan of the DPC.
Beneficiaries targeted by health partners in 2013• An estimated 118 000 new cholera cases• Staff and patients of 69 cholera treatment facilities in target areas• 1.5 to 2 million people are sensitized and receive information regarding prevention and treatment of cholera
Geographical areas targeted by health partners in 2013Target areas include the western part of Haiti (including Port-au-Prince), Artibonite, the Centre, South, South-East, Jeremie, Cap Haitien and Port de Paix.
Health sector funding requirements for 2013 Health partners are appealing for a total of US$ 29 000 000 in 2013
Health partners in 2013 are: Ministère de la Santé Publique et de la Population (Ministry of Public Health and Population), National Department of Potable Water and Sanitation, Direction de la Protection Civile (Civil Protection Agency), Action Contre la Faim (Action Against Hunger), Agence d’Aide à la Coopération Technique et au Développement (Agency for Technical Cooperation and Development), Adventist Development and Relief Agency, ARCA, AmeriCares Foundation, Aide Médicale Internationale, Ame-Sada, American Refugee Committee, Association of Volunteers in International Service, Bureau Anglican de l’Éducation en Haïti, Brigade Médicale Cubaine, Brigade for the Protection of Minors,CARE, Caritas Haiti, communiquer avec les populations affectées par un désastre (communicating with disaster-affected populations), (US) Center for Disease Control and Prevention, Centre d’Etude et de Coopération Internationale, Centre d’Education et d’Intervention Sociale, Cooperatzione e Sviluppo, Caribbean Fellowship Ministries, Christianville, Children’s Nutrition Programme of Haïti, Concern Worldwide, Cooperazione Internazionale, Catholic Relief Services, Direction Administration Pénitentiaire, Département Sanitaire du Nord, Entraide Protestante Suisse, Feed the Children, Fondation pour le Développement et l’Encadrement de la Famille Haïtienne, Fraternité Notre Dame, Global Assistance Partners, Groupe Haïtien d’Etude du Sarcome de Kaposi et des Infections Opportunistes, GOAL, GrassRoots United, Groupe de Recherche et d’Echanges Technologiques, Gruppo di Volontariato Civile (GVC), Handicap international, Healing Arts Mission, Heart to Heart International, Help for Orphans International, Haitian Health Foundation, Humedica, IBESR (Institut Bien Etre Social et de la Recherche), International Committee of the Red Cross, IEDA Relief, International Federation of the Red Cross, International Medical Corps, Institut Haitien de

17
Sante Communautaire, International Lifeline, Internews, International Organization for Migration, International Rescue Committee, International Relief and Development, Israid, J/P Haitian Relief Organization, Konbit Santé, Malteser, Management Sciences for Health, MAST (Ministère des Affaires Sociales et du Travail), MCFDF (Ministère de la Condition Féminine et des Droits de la Femme), Médecins du Monde, Medical Teams International, Medic Haiti, Medishare, Mercy Corps, Merlin, Médecins sans Frontières, Norwegian Church Aid, Nacion En Transformacion, Opportunities Industrialization Centres International, Open Hands, Outreach International, Oxfam, Pharmacie et Aide Humanitaire, Panamerican Health Organization/World Health Organization, Petits Frères et Soeurs, Plan International, Pompiers sans Frontières, Première Urgence, Samaritan’s Purse, Réseau Haïtien pour la Sante et le Développement, Save the Children, Société d’Offres et de Demandes d’Emploi et de Consultations, Soeurs Ste. Therese, Solidarité Haitienne pour le Développement National, Sustainable Organic Integrated Livehood, Solidarités International, Sustainable Aid Supporting Haiti (SASH), Tearfund, Terres des hommes, Union des Jeunes pour le Développement Humain Réel et Durable (UJDHRD), United Nations Population Fund, United Nations Children’s Fund, United Nations Office for Project Services, World Hope International, World Water Relief, World Vision International, World Water Relief, and Zanmi Lasante.
WHO funding requirements for 2013WHO is appealing for a total of US$ 12 000 000 to help prevent the spread of cholera and other infectious diseases, support the provision of medical care and promote efforts to strengthen response capacities.

18
World Health Organization humanitarian response in 2013
In recent years, Kenya had to face recurrent humanitarian emergencies related to drought, floods, ethno-political conflicts and disease outbreaks. In addition, the situation in Somalia and the Republic of South Sudan contin-ues to influence the refugee dynamics across the borders into Kenya where 673 788 refugees are hosted in the Dadaab and Kakuma refugee camps and in Nairobi. The Kenya military offensive into Somalia has caused insecurity in north-eastern Kenya and has also hampered humanitarian access. In 2012, more than 80 000 people were displaced due to inter-communal vio-lence and as the March 2013 elections are approaching, there is a risk of in-creased tensions between communities.
Health Sector SituationThe current health situation in Kenya is characterized by a persisting risk of disease outbreaks including measles, cholera, hepatitis E, polio, malaria, dengue fever and rift valley fever. Further risk factors that may adversely affect the health situation in 2013 include inter-communal conflicts and potential vio-lence related to the elections in March 2013.Up to 450 000 people displaced due to conflict and insecurity, as well as their host communities, will require the provision of health services, particularly women and children. The current water and sanitation conditions in refugee camps and host communities are conducive to the spread of diseases. As Kenya is currently recovering from the effects of drought, existing malnutri-tion levels are expected to improve progressively if there are no new food-se-curity shocks in 2013. However, the nutritional situation requires surveillance.Kenya’s healthcare delivery system is still weak and the system in place is not likely to be able to respond to any large-scale disaster or disease outbreaks without humanitarian support from health partners. In addition, the devolution of decision-making power to the county levels in 2013 will require a substantial amount of technical and structural support from partners over an extended period of time.
Health Sector Priorities Priority 1: To ensure that critical life-saving services, resources and supplies are available and accessible to vulnerable population groups, particularly women and children, at key strategic locations in arid and semi-arid regions.Planned outputs: • Coordination of health sector partners at national, county and district level
takes place through health partner mapping, the establishment of coordina-tion forums, the development of joint sector response plans as well as the conduct of joint rapid health and nutrition assessments.
• Key partners for the provision of logistics support and the provision of life-saving health care services to special vulnerable groups will be identi-fied. Partners will be mapped, a system developed for tracking HIV/AIDS and tuberculosis cases and providing home-based treatments, a system established for community-based service provision and referral of preg-nant women and children as well as survivors of gender-based violence. Furthermore, at least 400 000 children at risk in arid and semi-arid regions are planned to be vaccinated against measles and polio. The capacities of district and provincial partners and hospitals to manage severe and compli-cated malnutrition cases will be enhanced.
Kenya9
WHO funding for 20122012 Requirements: US$ 2 493 100
2012 Funding: US$ 1 062 417
FundingGap
Gap 57.4%
Baseline indicators Estimate
Human development index1 2011 143/187Population in urban areas% 2010 22Population using improved water source%
2008 59
Population using improved sanitation%
2008 31
Life expectancy at birth 2009 60 yearsInfant mortality rate / 10002 2010 55Under 5 mortality rate / 10002 2010 85Maternal mortality ratio / 100 0002 2010 360[230-590]*
Measles coverage among one year old’s%
2010 86
Wasting% 3 2009 7.0Health system efficiency rank 4
2000 140/191
2012 Donors In 2012 WHO received financial contri-butions to support its humanitarian work in Kenya from Finland and the UN Trust Fund.
Source: WHO Global Health Observatory unless indicated other-wise by a footnote. References on page 46
19
• Essential medicines, laboratory reagents and basic equipment are prepositioned in target locations to prevent the spread of epidemic-prone diseases.
• Particular attention is given to the needs of pregnant women and children. Medical supplies, consumables, and re-productive health kits will be prepositioned in targeted locations.
• Early warning and alert networks are strengthened in at least 20 of the 47 counties through the dissemination of respective guidelines and tools, the provision of orientation training for district health teams and partners, as well as the provision of logistics support for timely investigation and reporting.
Priority 2: To promote health and nutrition awareness among communities and increase the utilization of essential health and nutrition services.Planned outputs: • District health teams receive support in reaching out to communities, including through the dissemination of tech-
nical guidelines and health education material as well as through training.• Vulnerable groups at community level receive special attention, including women and children, survivors of gender-
based violence and elderly people. Target groups will be identified, health promotion material made available and training conducted.
Priority 3: To support county level health sector governance structures in their commitment to disaster risk reduction and disaster preparedness.Planned outputs: • Forums for county capacity building and for early warning will be established. • Disaster risk reduction and management plans will be developed.
Beneficiaries targeted by health partners in 2013Total: 2 882 000Women: 1 731 500 (including 280 000 particularly vulnerable persons)Men: 1 150 500 (including 200 000 particularly vulnerable persons)
Geographical areas targeted by health partners in 2013Target areas include Nairobi, Eldoret, Nakuru, Garissa, Mombasa, Isiolo, Marsabit, Turkana and Kisumu.
Health sector funding requirements for 2013 Health partners are appealing for a total of US$ 15 625 091 in 2013Health partners appealing for funding in 2013 include: Cooperazione Internationale (International Cooperation), International Organization for Migration, Terre des Hommes, United Nations Children’s Programme, United Nations High Commissioner for Refugees, World Food Programme, and the World Health Organization.
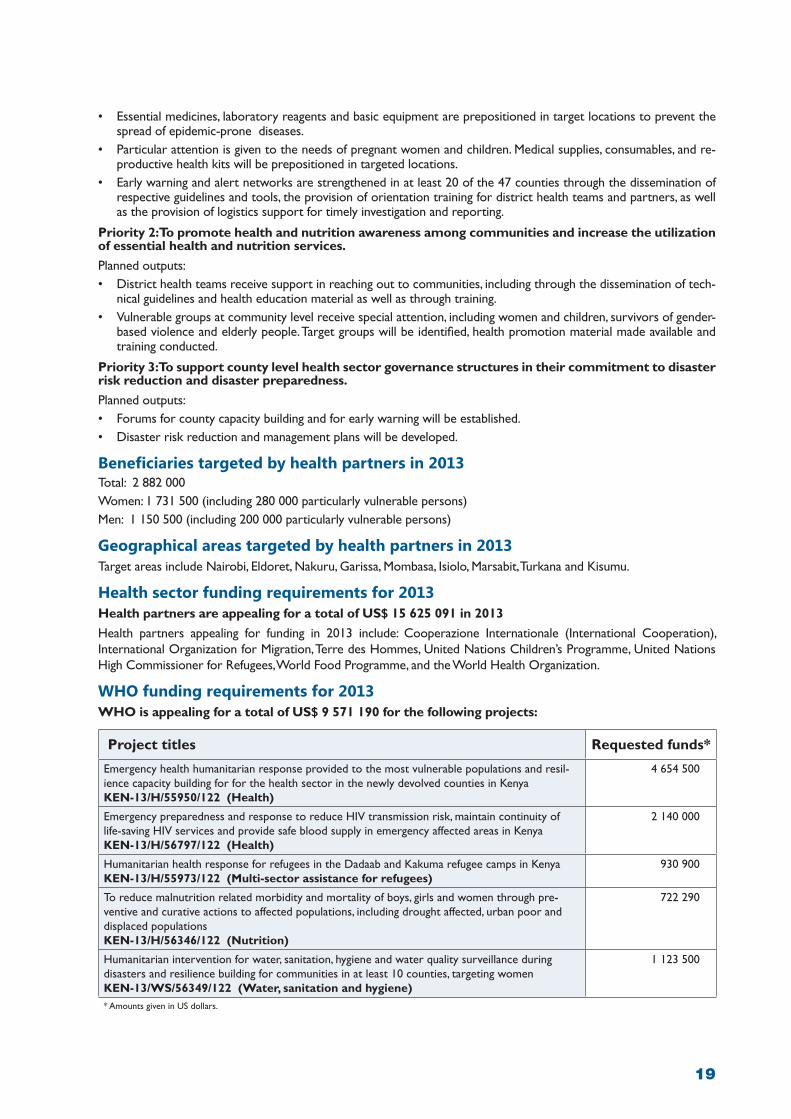
WHO funding requirements for 2013WHO is appealing for a total of US$ 9 571 190 for the following projects:
Project titles Requested funds*
Emergency health humanitarian response provided to the most vulnerable populations and resil-ience capacity building for for the health sector in the newly devolved counties in KenyaKEN-13/H/55950/122 (Health)
4 654 500
Emergency preparedness and response to reduce HIV transmission risk, maintain continuity oflife-saving HIV services and provide safe blood supply in emergency affected areas in KenyaKEN-13/H/56797/122 (Health)
2 140 000
Humanitarian health response for refugees in the Dadaab and Kakuma refugee camps in KenyaKEN-13/H/55973/122 (Multi-sector assistance for refugees)
930 900
To reduce malnutrition related morbidity and mortality of boys, girls and women through pre-ventive and curative actions to affected populations, including drought affected, urban poor and displaced populationsKEN-13/H/56346/122 (Nutrition)
722 290
Humanitarian intervention for water, sanitation, hygiene and water quality surveillance during disasters and resilience building for communities in at least 10 counties, targeting women KEN-13/WS/56349/122 (Water, sanitation and hygiene)
1 123 500
* Amounts given in US dollars.

20
World Health Organization humanitarian response in 2013
Mali is affected by an unprecedented humanitarian crisis. The political situa-tion is worsening and tensions and violence are increasing. The north is under the control of Islamist armed groups and the south controlled by the Malian government. As of January 2013, more than 2.5 million people in are affected by the conflict, thus limiting their access to basic social and health servic-es including the water infrastructure. Hundreds of thousands have been dis-placed by the conflict, of which about 227 000 are internally displaced and over 144 000 sought refuge in Burkina Faso, the Niger and Mauritania. In addition to the socio-political crisis, Mali is facing a nutritional crisis. At the end of 2012, the World Food Programme projected that 4.6 million people across Mali were at risk of food insecurity.
Health Sector SituationA major challenge facing the Malian health system is the disruption of the health and sanitation structure in the north of the country as a consequence of the armed conflict. A joint assessment of health actors concluded that only 10% of the health structures in the north of the country are functional. Several of them were looted and most of the qualified health workers have left their workplace. Functioning health structures, both in the northern and southern parts of the country are overwhelmed with the increasing health needs of lo-cal and displaced populations. The disease surveillance system is reported to be disrupted. In a context of limited access to water and sanitation, about 1.5 million people are at risk of contracting diseases such as cholera. While treatment of conflict-related conditions are a priority, health care serv-ices for chronic diseases, both transmissible and non-transmissible, will need to be sustained in the current complex environment. Sexual and gender-based violence is of serious concern and both medical assistance and psycho-social support for victims are priorities.In addition to conflict-related health challenges, malnutrition figures are alarm-ing. It is estimated that in 2013, 660 000 children under the age of five will suffer from acute malnutrition, of which 210 000 are expected to be suffering from severe acute malnutrition.
Health Sector Priorities Priority 1: Improve access to quality basic health services and refer-ral services, including reproductive health care and HIV/AIDS treat-ment, for crisis-affected target populations.Planned outputs: • 90% of functional health structures in crisis-affected zones will offer basic
health care services. Obstetrical and neonatal care services will be rein-forced in health structures.
• Vaccination coverage will be reinforced: more than 95% of children aged between six months and 15 years are planned to be immunized against measles.
• At least 70% of the population has access to health services.• 80% of people with HIV/AIDS and tuberculosis in target areas will have ac-
cess to adequate treatment
Mali10
WHO funding for 20122012 Requirements: US$ 8 207 492
2012 Funding: US$ 1 007 292
Funding
Gap
Gap 87.7%
Baseline indicators Estimate
Human development index1 2011 175/187Population in urban areas% 2010 36Population using improved water source%
2008 56
Population using improved sanitation%
2008 36
Life expectancy at birth 2009 53 yearsInfant mortality rate / 10002 2010 99Under 5 mortality rate / 10002 2010 178Maternal mortality ratio / 100 0002 2010 540[390-930]*
Measles coverage among one year old’s%
2010 63
Wasting% 3 2006 15.3%Health system efficiency rank 4
2000 163/191
2012 Donors In 2012 WHO received financial contri-butions to support its humanitarian work in Mali from the Central Emergency Response Fund and the International Fund for Agricultural Development.
Source: WHO Global Health Observatory unless indicated other-wise by a footnote. References on page 46

21
Priority 2: Strengthen early warning and surveillance systems, ensure adequate preparedness and re-sponse to diseases with epidemic potential and other disasters.Planned outputs: • A contingency plan for major health risks is established and stocks of medicines and medical equipment pre-positioned.• Epidemics are detected in a timely manner, and 95% of epidemics and disasters are responded to appropriately in
less than 15 days.• 80% of the health personnel in zones at risk receive training on epidemic response.• Social mobilization is reinforced
Priority 3: Contribute to the rehabilitation of health facilities.Planned outputs: • 25% of crisis-affected referral health facilities are rehabilitated and equipped by the end of 2013.• Health facilities in buffer zones in Mopti, Ségou and Koulikoro are strengthened
Priority 4: Strengthen coordination of emergency health interventions within the framework of the sec-toral responsibility approach in 2013.Planned output: • Close collaboration among all health cluster partners is established and coordination of activities improved at na-
tional and regional level.
Beneficiaries targeted by health partners in 2013Total: 2.5 million (estimated number of people throughout the country requiring health services in 2013) including:Children under age five: 500 000 Women: 1 040 000 Men: 960 000.
Geographical areas targeted by health partners in 2013• Food/nutritional crisis: Kayes, Koulikoro, Tombouctou, Gao, and Mopti (87% of acute malnutrition cases are re-
ported from the southern part of Mali). • Armed conflict: Gao, Kidal, Tombouctou, Mopti (Douentza, Tenenkou, Youwarou, Koro) and Ségou (Niono and
Macina).
Health sector funding requirements for 2013 Health partners are appealing for a total of US$ 28 885 768 in 2013Health partners appealing for funding in 2013 include: Agronomes et Vétérinaires Sans Frontières, Médecins du Monde Belgique, Médecins du Monde France, Santé Diabète, Santé et Développement, Save the Children, United Nations Children’s Fund, United Nations Population Fund and the World Health Organization.
WHO funding requirements for 2013WHO is appealing for a total of US$ 19 938 962 for the following projects:
WHO Proposed Projects
Project titles Requested funds*Strengthening the capacity of health centres to manage the health issues of young people and ado-lescents in the regions of Mopti, Ségou, Sikasso, Koulikoro, Kayes and Bamako district MLI-13/H/53407/122
3 330 000
Humanitarian assistance to victims of gender-based violence (displaced persons from northern Mali)MLI-13/H/53562/122
74 179
Support for rehabilitation and recommissioning of looted or destroyed health facilities in the re-gions of Gao, Kidal and Tombouctou (11 community health centres and four referral centres) MLI-13/H/53647/122
759 700
Strengthening of epidemiological surveillance and epidemic control in MaliMLI-13/H/53744/12
1 500 000
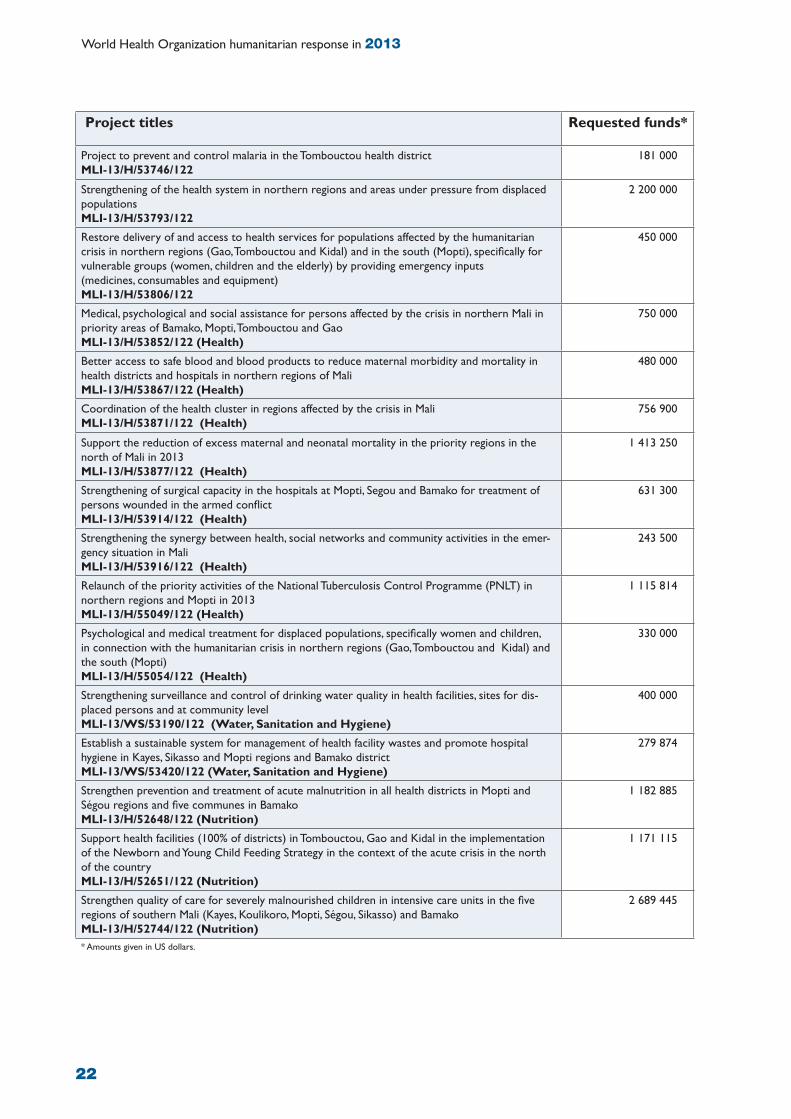
22
World Health Organization humanitarian response in 2013
Project titles Requested funds*
Project to prevent and control malaria in the Tombouctou health districtMLI-13/H/53746/122
181 000
Strengthening of the health system in northern regions and areas under pressure from displaced populationsMLI-13/H/53793/122
2 200 000
Restore delivery of and access to health services for populations affected by the humanitarian crisis in northern regions (Gao, Tombouctou and Kidal) and in the south (Mopti), specifically for vulnerable groups (women, children and the elderly) by providing emergency inputs (medicines, consumables and equipment)MLI-13/H/53806/122
450 000
Medical, psychological and social assistance for persons affected by the crisis in northern Mali in priority areas of Bamako, Mopti, Tombouctou and GaoMLI-13/H/53852/122 (Health)
750 000
Better access to safe blood and blood products to reduce maternal morbidity and mortality in health districts and hospitals in northern regions of MaliMLI-13/H/53867/122 (Health)
480 000
Coordination of the health cluster in regions affected by the crisis in Mali MLI-13/H/53871/122 (Health)
756 900
Support the reduction of excess maternal and neonatal mortality in the priority regions in the north of Mali in 2013 MLI-13/H/53877/122 (Health)
1 413 250
Strengthening of surgical capacity in the hospitals at Mopti, Segou and Bamako for treatment of persons wounded in the armed conflict MLI-13/H/53914/122 (Health)
631 300
Strengthening the synergy between health, social networks and community activities in the emer-gency situation in Mali MLI-13/H/53916/122 (Health)
243 500
Relaunch of the priority activities of the National Tuberculosis Control Programme (PNLT) in northern regions and Mopti in 2013 MLI-13/H/55049/122 (Health)
1 115 814
Psychological and medical treatment for displaced populations, specifically women and children, in connection with the humanitarian crisis in northern regions (Gao, Tombouctou and Kidal) and the south (Mopti) MLI-13/H/55054/122 (Health)
330 000
Strengthening surveillance and control of drinking water quality in health facilities, sites for dis-placed persons and at community level MLI-13/WS/53190/122 (Water, Sanitation and Hygiene)
400 000
Establish a sustainable system for management of health facility wastes and promote hospital hygiene in Kayes, Sikasso and Mopti regions and Bamako district MLI-13/WS/53420/122 (Water, Sanitation and Hygiene)
279 874
Strengthen prevention and treatment of acute malnutrition in all health districts in Mopti and Ségou regions and five communes in Bamako MLI-13/H/52648/122 (Nutrition)
1 182 885
Support health facilities (100% of districts) in Tombouctou, Gao and Kidal in the implementation of the Newborn and Young Child Feeding Strategy in the context of the acute crisis in the north of the countryMLI-13/H/52651/122 (Nutrition)
1 171 115
Strengthen quality of care for severely malnourished children in intensive care units in the five regions of southern Mali (Kayes, Koulikoro, Mopti, Ségou, Sikasso) and Bamako MLI-13/H/52744/122 (Nutrition)
2 689 445
* Amounts given in US dollars.

23
The food and nutrition crisis continues to affect a large part of Mauritania’s population. It is estimated that more than a million people, of whom 800 000 are in rural areas and 200 000 in urban areas require urgent food and nutri-tion assistance, with the south-eastern areas of Mauritania remaining the most affected by the crisis. In addition, more than 100 000 Malians fleeing hostilities have arrived in Mauritania since January 2012. This puts additional strain on a population which already had poor access to social and health services. The 2012 rainy season caused flooding in Mauritania which led to considerable damages.
Health Sector SituationThe availability of essential health services, for prevention, promotion and cure, throughout Mauritania remains insufficient. There is a lack of qualified health staff and medical equipment. Stock-outs of essential medicines and vaccines are frequent, and pre-positioning of emergency stocks almost nonexistent. The epidemiological situation in Mauritania is of concern. Limited access to clean water as well as a fragile sanitary and hygienic environment in both ur-ban and rural areas are conducive to the spread of diseases, particularly during and after flooding. As of October 2012, 34 cases of Rift Valley fever including 17 deaths were reported, 40 cases of meningitis including six deaths, as well as 34 measles cases. The possible emergence of cholera is being monitored. The food and nutritional crisis along with large population movements origi-nating from Mali have further increased the vulnerability of populations to communicable diseases. The early warning and response capacities of the health system are not adequate to prevent the eventual spread of epidemics. Detection and notification is often late, and analysis capacities at regional and district level is weak. Delays between case detection and confirmation vary between five and 28 days.
Health Sector Priorities Priority 1: Strengthen the capacity of health facilities/therapeu-tic feeding centres to treat medical complications of severe acute malnutrition.Planned outputs:• Persons admitted to health facilities/therapeutic feeding centres suffering
from medical complications of severe acute malnutrition receive adequate treatment, particularly children.
• Water quality control systems are established in all therapeutic feeding centres.
Priority 2: Strengthen preparedness to, detection of and response to epidemics.Planned outputs:• Detect diseases with epidemic potential within 48 hours.• Prompt, adequate treatment of epidemic prone diseases with mortality
rates remaining below 1% for cholera, below 50% for Rift Valley fever and below 10% for meningitis.
Priority 3: Strengthen essential health care services, particularly in the area of reproductive and child healthPlanned outputs: • Essential medicines and medical equipment is procured and delivered to
health facilities. Reproductive health kits are provided to health structures.
Mauritania11
WHO funding for 20122012 Requirements: US$ 2 018 300
2012 Funding: US$ 192 611
FundingGap
Gap 90.5%
Baseline indicators Estimate
Human development index1 2011 159/187Population in urban areas% 2010 41Population using improved water source%
2008 49
Population using improved sanitation%
2008 26
Life expectancy at birth 2009 58 yearsInfant mortality rate / 10002 2010 75Under 5 mortality rate / 10002 2010 111Maternal mortality ratio / 100 0002 2010 510[280-990]*
Measles coverage among one year old’s%
2010 67
Wasting% 3 2008 8.1Health system efficiency rank 4
2000 162/191
2012 Donors In 2012 WHO received financial con-tributions to support its humanitarian work in Mauritania from the Central Emergency Response Fund.
Source: WHO Global Health Observatory unless indicated other-wise by a footnote. References on page 46
24
World Health Organization humanitarian response in 2013
• Patients admitted to health facilities receive adequate treatment.• 80% of children below one year old are vaccinated against diphtheria, tetanus and pertussis.• 70% of children under five years of age are vaccinated against measles.• 70% of pregnant women have at least two prenatal consultations during their pregnancy • 60% of women giving birth are assisted by health staff.
Beneficiaries targeted by health partners in 2013Total: 18 006 (8643 women and 9363 men)
Geographical areas targeted by health partners in 2013Hodh El Chargui, Hodh El Gharbi, Assaba, Guidimakha, Gorgol and Tagant.
Health sector funding requirements for 2013 Health partners are appealing for a total of US$ 4 282 090 Health partners appealing for funding in the 2013 appeal are the United Nations Children’s Fund, the United Nations Population Fund and the World Health Organization.
WHO funding requirements for 2013WHO is appealing for a total of US$ 3 102 000 to implement the following health and multi-sector response projects:
Project titles Requested funds*Support for strengthening delivery of health services and the response capacity of village health committees in crisis settings MRT-13/H/54551/122
715 000
Strengthening delivery of health care to vulnerable populations affected by the food and nutrition crisis and host communities affected by the crisis in Mali MRT-13/H/54563/122
1 835 000
Project to strengthen management of acute malnutrition in nutrition rehabilitation centres for inpatient care (CRENI) and nutrition rehabilitation centres for outpatient care (CRENAS) MRT-13/H/54183/122
470 000
Support for emergency response preparedness through quality control of water in districts af-fected by the crisis MRT-13/WS/54562/122
82 000
* Amounts given in US dollars.

25
Chronic food insecurity, the absence of economic possibilities and an influx of refugees and returnees from conflict-affected neighbouring countries charac-terize the current humanitarian situation in the Niger. Each year, between 15 and 20% of the population (2 to 3 million people) are affected by food insecu-rity. Armed conflicts in Libya and Côte d’Ivoire in 2011 have led to 260 000 migrants returning to the Niger. Furthermore, the conflicts in Mali and Nigeria have prompted 50 000 Malian refugees, thousands of Nigerian returnees and persons expelled from Nigeria to seek refuge in the Niger. The population in-flux is expected to continue.
Health Sector SituationMalaria is the prime cause of morbidity and mortality in the Niger, particularly among children under five and pregnant women. In 2012, 2 630 075 malaria cases including 3049 deaths were recorded by the end of September. In 2013, 3.5 million cases are expected, half of which will be among children under five.Cholera is currently one of the main public health concerns. In 2012, the Niger reported the highest number of cases of cholera (4799 cases including 98 deaths) since the disease first occurred in the country in 1971. The epidemic affected the regions of Tillabéri (91% of the cases) and Tahoua (9% of the cas-es). There are 27 health districts at risk from the epidemic. The fact that 82% of the population of the Niger does not use toilet facilities increases the risk of cholera. Like other countries in the “African meningitis belt”, the Niger experiences re-current epidemics of meningitis. It is expected that there will be 2300 cases in 2013, of which 1600 will be in children under five years of age. Since 2011, the Niger has experienced a resurgence in outbreaks of measles. In 2012 the country reported a total of 1535 cases and six deaths.Regarding poliomyelitis, the Niger is at risk of recontamination as states in the north of neighbouring Nigeria are currently experiencing a poliomyelitis epi-demic with 97 confirmed cases.Although the prevalence of HIV/AIDS in the general population is below 1%, it is high among risk groups such as sex workers (35.6%), prison populations (2.7%), long-distance truck drivers (1.8%) and pregnant women (1.7%). The new infection rate has also increased.Food insecurity continues to affect the health status of the population. In chil-dren aged six to 23 months, at least one out of five children is affected by acute malnutrition. The health system is heavily burdened through supporting, year after year, the high number of cases of acute malnutrition requiring treatment.
Health Sector Priorities Priority 1: Improve access to and quality of primary and referral health care, particularly for reproductive health and HIV/AIDS serv-ices, for populations affected by health emergencies.Planned outputs:• Health facilities are adequately equipped with essential medicines and med-
ical equipment, including for reproductive health and HIV/AIDS treatment.• Vulnerable populations, including refugees and victims of flooding, benefit
from free primary health care services.• Mobile health clinics are available for geographic zones that are difficult to
access.
The Niger12
WHO funding for 20122012 Requirements: US$ 6 164 010
2012 Funding: US$ 1 982 154
Funding
Gap
Gap 67.8%
Baseline indicators Estimate
Human development index1 2011 186/187Population in urban areas% 2010 17Population using improved water source%
2008 48
Population using improved sanitation%
2008 9
Life expectancy at birth 2009 57 yearsInfant mortality rate / 10002 2010 73Under 5 mortality rate / 10002 2010 143Maternal mortality ratio / 100 0002 2010 590[360-
1100]*Measles coverage among one year old’s%
2010 71
Wasting% 3 2006 12.4Health system efficiency rank 4
2000 170/191
2012 Donors In 2012 WHO received financial contri-butions to support its humanitarian work in the Niger from the Central Emergency Response Fund.
Source: WHO Global Health Observatory unless indicated other-wise by a footnote. References on page 46

26
World Health Organization humanitarian response in 2013
Priority 2: Prevent, prepare for and respond appropriately to diseases with epidemic potential and oth-er disasters and health emergencies.Planned outputs:• Production and dissemination of at least 40 morbidity and mortality bulletins per year.• The mortality rate related to meningitis is below 10%.• A cholera response plan for 2013 is developed and the mortality rate related to cholera is below 1%.• The vaccine coverage for measles is above 90%.• Potential epidemics are investigated within 72 hours.• 50% of confirmed malaria cases are treated with artemisinin.
Priority 3: Reinforce the capacity of the health system and communities to withstand the impact of hu-manitarian crises.Planned outputs:• Major public health risks are covered by a contingency plan which is regularly updated.• Emergency health interventions are mapped and coordinated on a regular basis.• Synergies with the water and sanitation sector are reinforced.
Beneficiaries targeted by health partners in 2013Total: 1 717 800 (909 950 women and 807 850 men)
Geographical areas targeted by health partners in 2013Region: Coverage:Agadez UNFPA, UNICEF, UNAIDS, WHOTillabery UNFPA, UNICEF, UNAIDS, WHOMaradi UNFPA, UNICEF, UNAIDS, WHOZinder UNFPA, UNICEF, UNAIDS, WHONiamey UNFPA, UNICEF, UNAIDS, WHOTahoua UNFPA, UNICEF, UNAIDS, WHO, Organisation Nigerienne Pour le Developpement a la Base du
Potentiel Humain, CONCERN, Medecins du MondeDiffa UNFPA, UNICEF, UNAIDS, Save the Children, WHO
Health sector funding requirements for 2013 Health partners are appealing for a total of US$ 15 307 695 Agencies appealing for health sector funding in 2013 are: Comitato Internazionale per lo Sviluppo dei Popoli (International Committee for the Development of Peoples), Save the Children, World Vision International, Concern Worldwide, Arbeiter-Samariter-Bund, Vétérinaires Sans Frontières Belgique, CARE International, Sossin, Agency for Technical Cooperation and Development, Food and Agriculture Organization, Action Contre la Faim (Action Against Hunger) Spain, Lutheran World Relief, World Food Programme and World Health Organization.
WHO funding requirements for 2013WHO is appealing for a total of US$ 9 993 258 to implement the following projects:
WHO Proposed Projects
Project titles Requested funds*Measles and poliomyelitis epidemic response in areas affected by humanitarian crises NIG-13/H/54824/122
3 391 078
Emergency response to the health needs of populations in health districts hosting Malian refugees in the Tillabéri and Tahoua regions of the Niger NIG-13/H/54827/122
1 331 780
Prevention and emergency health response to epidemics and floods in the Niger NIG-13/H/54834/122
3 858 000
Emergency nutrition intervention for saving lives of severely malnourished children in the Niger NIG-13/H/54589/122
1 412 400
* Amounts given in US dollars.

27
The most salient features of the longstanding occupation, including conflict, ac-cess restrictions and financial constraints, remain largely unchanged. As a result, the nature and the scope of humanitarian needs have not decreased. The fragil-ity of the political situation was underlined in November 2012 when the esca-lation in violence in Gaza caused some 12 000 Palestinians to be temporarily displaced. The escalation exacerbated an already fragile humanitarian situation.
Health Sector SituationAccess to essential health and nutrition services remains limited for the pop-ulations in Gaza, East Jerusalem and its peripheries, Area C, closed military areas (or Seam Zone), and some localities in Area B. There are many factors hampering access to quality essential health and nutrition services for vulner-able Palestinian communities including: continued restrictions on importation of medical supplies, equipment and spare parts; limitations on movement of patients, health staff and medical students; deterioration in essential medicine stocks due to the Palestinian Authority (PA) fiscal crisis; widespread insecurity in the West Bank and Gaza; and restrictive planning and zoning policies in the West Bank. Access to East Jerusalem tertiary hospitals is of particular concern. There are 542 obstacles to Palestinian movement in the West Bank, including 61 staffed checkpoints, which considerably limit access to health and nutrition services. In addition, approximately 11 300 Palestinians reside in the closed area between the Barrier and the Green Line or in enclaves. Residents have to pass through checkpoints to reach hospitals and health centres, schools and workplaces. The impact on the residents’ access to health care is a particular source of concern, especially access to emergency health services after the checkpoint closures.The requirement for ‘visitor permits’ to enter the Seam Zone generally pre-vents doctors from providing house calls, ambulances from collecting patients and mobile teams from providing health services. As a precautionary measure, pregnant women often leave their community one month before delivery to avoid complications in accessing health care services at the time of delivery.The Palestinian Ministry of Health has been facing a severe financial crisis since April 2012, with debts for medicines and referral abroad amounting to ap-proximately US$ 175 million. As a result, referrals abroad have been limited. Furthermore, the Ministry of Health was unable to pay its suppliers, thus af-fecting the supply of medicines and medical items to health facilities. In early June 2012, 149 essential medicines were reported at zero stock in the West Bank (28% of the total essential medicines list for the occupied Palestinian territory).In Gaza, the Israeli blockade and internal Palestinian divide have led to a gradual erosion of the public health system. Shortages of fuel, medical supplies, equip-ment, inadequate health infrastructure and a flagging medical training pro-gramme have led to a situation where the health care network performs at a fraction of its capacity. Essential medicines and other medical supplies have deteriorated due to budg-etary restrictions faced by the PA as well as the political split between the PA in Ramallah and the local authorities in Gaza. Commodities for family plan-ning are entirely donor-funded in the absence of a dedicated PA or de facto budget line.
The occupied Palestinian territory13
WHO funding for 20122012 Requirements: US$ 1 020 600
2012 Funding: US$ 1 005 099
FundingGap
Gap 1.5%
Baseline indicators Estimate
Human development index1 2011 114/187Population in urban areas% 2010 -Population using improved water source%
2008 -
Population using improved sanitation%
2008 -
Life expectancy at birth 2009 -Infant mortality rate / 10002 2010 -Under 5 mortality rate / 10002 2010 -Maternal mortality ratio / 100 0002 2010 -
Measles coverage among one year old’s%
2010 -
Wasting% 3 2004 -Health system efficiency rank 4
2000 -
2012 Donors In 2012 WHO received financial con-tributions to support its humanitarian work in the occupied Palestinian terri-tory from Norway, Switzerland and the Office of the United Nations Special Coordinator for the Middle East Peace Process.
Source: WHO Global Health Observatory unless indicated other-wise by a footnote. References on page 46
28
World Health Organization humanitarian response in 2013
Adequate maintenance of medical equipment is still challenged by restrictions on the entry of technicians and manufac-turers, as well as on the ability to send equipment for servicing outside Gaza. Currently around 23% of medical equip-ment in Gaza used in the public health system is not functional. Specialized medical knowledge requires months and years of training in medical units that are only available in the West Bank, particularly in East Jerusalem. However, travel restrictions make access to such training impossible for most medi-cal staff. Significant capacity shortages exist in the area of cardiovascular diseases, oncology, ophthalmology, orthopaed-ics and neurosurgery, which account for the majority of referrals abroad.
Health and Nutrition Sector Priorities Priority 1: Ensure access of the vulnerable populations in the West Bank and Gaza to essential health and nutrition services.Planned outputs:• People in vulnerable communities receive access to integrated primary health care services• People in vulnerable communities receive mental health and psycho-social support services• People in vulnerable communities receive nutrition services • People in vulnerable communities receive reproductive health services
Priority 1: Facilitate access of the vulnerable populations in the West Bank and Gaza to remedies and recovery through the provision of services, monitoring, reporting and advocacy.Planned outputs:• Health services are provided to communities defined as vulnerable to displacement• Victims of violence are referred to the organizations with the protection mandate• Monitoring of access to services in East Jerusalem is maintained• Monitoring of access to services in Gaza is maintained• Publications with information about access to health services and incidence of violence and human rights violations
are developed
Priority 3: Build emergency preparedness of the vulnerable communities in the West Bank and Gaza to mitigate the impact of the current and potential new emergencies.Planned outputs:• Community members are trained in topics relevant to emergency preparedness• Health providers are trained in topics relevant to emergency preparedness• Health staff is trained in first aid (including psychological first aid and primary trauma care)• Community members are trained in first aid (including psychological first aid and primary trauma care)
Beneficiaries targeted by health partners in 2013Total: 1 678 935 (1 183 820 women and 495 115 men)Women, pregnant women, men, children under five, newborns, children with cerebral palsy/multiple disabilities, older people, people with non-communicable diseases, patients from the West Bank, Gaza and East Jerusalem who are socially and economically disadvantaged and needing specialized health care, people with disabilities, health professionals and community-based first responders, and Palestinian refugees.
Geographical areas targeted by health partners in 2013All of the Gaza Strip, Area C, Seam Zone and East Jerusalem
Health sector funding requirements for 2013 Health partners are appealing for a total of US$ 22 536 007 in 2013Health partners appealing for funding in 2013 are: CARE International, HelpAge International, United Nations Relief and Works Agency for Palestine Refugees in the Near East, Medico International, Union of Health Work Committees, United Nations Population Fund, Medical Aid for Palestinians, St. John Eye Hospital, Handicap International, Save the Children, Danish Church Aid, and the United Nations Children’s Programme.

29
WHO funding requirements for 2013WHO is appealing for a total of US$ 6 002 700 for the following projects:
Project titles Requested funds*Strengthening health coordination and health rights advocacy in the occupied Palestinian terri-tory OPT-13/H/52117/122
823 900
Procurement of pharmaceuticals for the Palestinian MoH OPT-13/H/57530/R/122
5 178 800
* Amounts given in US dollars.

30
World Health Organization humanitarian response in 2013
After four decades of conflict in Mindanao, a Framework Agreement has been signed between the Government of the Republic of the Philippines and the Moro Islamic Liberation Front (MILF). While foundations for lasting peace are being laid, the Government still confronts a significant challenge in responding to the needs of people affected by repeated cycles of violent conflict and natu-ral disasters. The Philippines is the third most disaster-prone country in the world, frequently hit by flooding, landslides, earthquakes and tsunamis.
Health Sector SituationCommunities in areas of Mindanao often lack the basics in health care. Close to a third of the barangays assessed in 2012 had no barangay health station (BHS). A barangay is the smallest administrative division in the Philippines. In some areas, a weekly mobile clinic is the only provider of health care available to an entire community, and in the more remote areas there is virtually no health care provision whatsoever. Residents in areas with no access to basic health services have to seek health services from the nearest barangay with a health facility or the main health facility in the poblacion (central barangay), which is often far away.In barangays with health stations, facilities are often in a poor state of repair without any functional source of water that would be needed to wash hands and instruments. Several BHS have been damaged by the floods or during the conflict in 2008-2009 and have not been repaired since. Nongovernmental or-ganization partners reported that in one of the sites assessed in August 2012, the BHS was being used as a residence by the son of the village chief while an-other was converted into a warehouse for farm materials. Such scenes are not uncommon in other remote areas. There is also a widespread lack of medicines and qualified staff. This is particu-larly pronounced in isolated, rural communities which are insecure and difficult to access. Communities assessed in 2012 primarily had access to visits from a rural health midwife, but for 35% of these communities such visits occur no more than twice a month. Geographic distance, difficult terrain and security concerns are reasons cited for the infrequent visits. Significant gaps in disease surveillance continue to be a problem. Disease sur-veillance is an essential aspect of humanitarian response in Mindanao, given the lack of health services for responding to disease outbreaks and the underlying vulnerability of people living in abject poverty.Almost a third of areas assessed lack prenatal and postnatal services. Of about 800 reported births in the areas assessed in January 2012, only 28% (220) were delivered inside a health facility. Of the 72% (540) of births delivered outside a health facility, only 40% were assisted by skilled birth attendants, while the rest were attended to by traditional birth attendants (TBA). Over half (53%) of women with pregnancy-related problems were brought to the rural health unit (RHU) while 14% were still referred to unskilled TBAs who are more readily accessible in the remote barangays. In half of the communities, there were reports of one or more deaths within six weeks of giving birth. The lack of access to family planning services, due in large part to low awareness about family planning, myths and misconceptions and shortage of family planning ma-terials contributes to an increase in unwanted and unplanned pregnancies. Additionally, the lack of youth-focused health programmes contributes to the rise in of early marriages and teen pregnancies. This results in young, pregnant women at high risk of mortality and morbidity as they are not physically de-veloped nor psychologically prepared for motherhood. The lack of awareness
The Philippines (Mindanao)14
WHO funding for 20122012 Requirements: US$ 1 941 839
2012 Funding: US$ 376 799
FundingGap
Gap 80.6%
Baseline indicators Estimate
Human development index1 2011 112/187Population in urban areas% 2010 49Population using improved water source%
2008 91
Population using improved sanitation%
2008 76
Life expectancy at birth 2009 70 yearsInfant mortality rate / 10002 2010 23Under 5 mortality rate / 10002 2010 29Maternal mortality ratio / 100 0002 2010 99[66-140]*
Measles coverage among one year old’s%
2010 88
Wasting% 3 2008 6.9Health system efficiency rank 4
2000 60/191
2012 Donors In 2012 WHO received financial contri-butions to support its humanitarian work in the Philipplines from Australia and the Central Emergency Response Fund.
Source: WHO Global Health Observatory unless indicated other-wise by a footnote. References on page 46

31
about the benefits of reproductive health among the affected population leads to poor health-seeking behaviour.In the changing context of Mindanao, there is also a strong recognition that health interventions could significantly con-tribute as an entry point and an instrument to peace initiatives. Therefore, there is a strong need to mobilize commu-nity level groups (such as community health teams and Muslim religious leaders) to encourage enhanced community participation as well as to empower women, men, and adolescents to demand appropriate and quality health informa-tion and services
Health Sector Priorities • Provide support for affected populations, especially the vulnerable groups, to access essential preventive, promotive
and curative health services (including mental health and psychosocial services, adult and adolescent reproductive health). Provide mobile health services to communities without existing health facilities. Continue to rehabilitate barangay health stations and preposition emergency medicines and supplies.
• Strengthen the emergency disease surveillance system and improve information management. Build local capacity through training, investigate outbreaks within 48 hours of detection and initiate response within 24 hours after con-firmation. Furthermore, establish a database of pregnant and lactating women.
• Reinforce health education, promotion and advocacy through the organization of Community Health Teams, con-ducting health information sessions and the provision of health information material to households.
Beneficiaries targeted by health partners in 2013The Health Cluster will target 529 599 people, including 317 735 females and 211 824 males in 40 municipalities. The majority (18) of these targeted municipalities are among the 33 identified for assistance. Given that the needs of af-fected populations do not vary widely among the prioritised municipalities, the selection of how many affected people to include and which areas to target were based on the current Health Cluster capacity to respond.
Geographical areas targeted by health partners in 2013Region Province Municipality:Armm Lanao del sur Bubong, Butig, Ditsaan-Ramain Maguindanao Buluan, Datu Blah T. sinuat, Datu Odin sinsuat (Dinaig), Datu Paglas, Datu Piang,
Datu Saudi Amaptuan, Gen, S.K. Pendatun, Guindulungan, Kabuntalan (Tumbao), Mamasapano, Rjah buayan, shariff Aguak(Maganoy), south Upi, sultan Kudarat (Nuling), Sultan Sa Barongis (Lambayong), Talayan
IX Zamboanga Sibugay PayaoXII North Cotabao Aleosan, Arakan, Carmen, Kabacan, Magpet, Midsayap, M’lang, Pigkawayan, Pikit,
President Roxas, tulunan Sarangani Maitum, Malapatan, Malungon South Cotabato Polomolok, T’boli Sultan Kudarat Bagumbayan, Lambayong (mariano Marcos), Lebak, Palimgang
Health sector funding requirements for 2013 Health partners are appealing for a total of US$ 5 210 057 in 2013Health partners appealing for funding in 2013 include: Plan, United Nations Children’s Programme, Action Contre le Faim (Action Against Hunger) Spain, World Food Programme, Health Organization for Mindanao, United Youth of the Philippines-Women, Central Mindanao Integrated Livelihood Assistance for Rural Development Foundation, Mindanao Human Rights Action Center, Young Advocates for Peace and Development Network, Child Alert Mindanao, United Nations High Commissioner for Refugees, Nonviolent Peaceforce, United Nations Population Fund, Magungaya Mindanao Incorporated.
WHO funding requirements for 2013WHO is appealing for a total of US$ 1 610 470 to implement the following projects:
Project titles Requested funds*Access to preventive and curative health services for populations in conflict-affected and natural hazard prone areas PHI-13/H/56270/122
260 470
Typhoon Bopha: Ensuring access to health services for affected populations PHI-13/H/57141/R/122
600 000
Typhoon Bopha: Health Response to the Typhoon Bopha crisis in Mindanao PHI-13/H/57393/R/122
750 000
* Amounts given in US dollars.

32
World Health Organization humanitarian response in 2013
Political tensions over unresolved Comprehensive Peace Agreement issues between the Republic of South Sudan and the Sudan characterized the new state’s first year of independence, including border demarcation, oil transit fees and the fate of the contested Abyei area. The shutdown of oil production at the start of the year had serious economic implications as it led to the an-nouncement of an austerity budget in July 2012. Insecurity continued to cause displacement related to inter-communal violence, attacks by non-state armed actors, and cross-border hostilities with the Sudan. In addition, more than 175 000 Sudanese refugees fleeing fighting in the Sudan and more than 130 000 returnees arrived in the Republic of South Sudan during 2012. The number of food insecure people rose sharply in 2012. Flooding was reported in all 10 states, with the heaviest hit being Jonglei, Lakes, Northern Bahr el Ghazal, Unity and Warrap.
Health Sector SituationHealth care coverage across the Republic of South Sudan is poor, only one out of five people uses a healthcare facility at least once a year and only 40% of people are able to access health care within in a five kilometer radius. The catchment population of existing health facilities varies throughout the country, ranging from 4000 people per facility in Western Bahr el Ghazal to 34 800 in Eastern Equatoria. Of the 1200 functional healthcare facilities in the country, it is estimated that 800 are supported by humanitarian partners. Health Cluster partners provide at least 60% of countrywide services and consultations. Infant and under-five mortality rates are high, at an estimated 75 and 105 per 1000 live births. On average, only 6.3% of children under two years of age are fully immunized. In cases where mothers are not educated, the rate is as low as 4.5%. Less than 20% of children complete the three basic immunizations and routine measles immunization is thought to be lower. Maternal mortality is very high with an estimated 1000 per 100 000 live births. On average, a woman gives birth to 6.7 children, thus about one in fifteen women will die during childbirth. Communicable disease outbreaks in the Republic of South Sudan are common in all states. Twenty-five measles outbreaks occurred in 2012 as of August, re-sulting in 1862 cases and 59 deaths (compared to 25 outbreaks, 1,027 cases and 39 deaths in all 2011). Outbreaks manifested despite nationwide cam-paigns, reflecting poor access to and coverage of basic healthcare and rou-tine immunizations. Between January 2011 and August 2012, over 8123 cases of kala azar were diagnosed and treated with 90% of cases in Jonglei State’s Fangak County. Conflict-related displacement caused the disease to spread to non-endemic areas in Koch and Mayendit counties in Unity State. In 2012, there were also continued cases of anthrax in Western Bahr el Ghazal, hepa-titis E in refugee communities in Upper Nile and Unity States, and a rubella outbreak in the Equatorias. Weak logistic systems, poor infrastructure and environmental access con-straints often rupture the distribution of medicines. An upsurge in malaria cases and improved case reporting demonstrated that there were insufficient stocks of anti-malarials in-country and that emergency procurement of sup-plies was necessary. Health partners are often called upon to assist in procure-ment, transport and distribution.
The Republic of South Sudan15
WHO funding for 20122012 Requirements: US$ 20 543 572
2012 Funding: US$ 10 291 074
FundingGap
Gap 49.9%
Baseline indicators* Estimate
Human development index1 000/000Population in urban areas 2011 00%Population using improved water source
2010 00%
Population using improved sanitation
2008 00%
Life expectancy at birth 2009 0 yearsInfant mortality rate / 10002 2010 00Under 5 mortality rate / 10002 2010 00Maternal mortality ratio / 100 0002 2010 000[000-000]*
Measles coverage among one year old’s%
2010 00
Wasting 3 2006 00.0%Health system efficiency rank 4
2000 000/000
* Baseline health indicators are currently not available for the Republic of South Sudan. They are included in the baseline health indicators for the Sudan (page 35)
Source: WHO Global Health Observatory unless indicated other-wise by a footnote. References on page 46
2012 Donors In 2012 WHO received financial contri-butions to support its humanitarian work in the Republic of South Sudan from the United States of America, Central Emergency Response Fund, European Commission Humanitarian Aid Office and the Common Humanitarian Fund.

33
Health Sector Priorities The key priorities of the health cluster in 2013 are to: • Maintain the existing safety net by providing basic health packages and emergency referral services, especially in ar-
eas of instability, underserved areas and among vulnerable groups.• Strengthen emergency preparedness, including surgical interventions. The main focus will be placed on training and
building skills for epidemic preparedness, surveillance of disease outbreaks, case management of epidemic-prone diseases, and key emergency surgical and obstetric interventions. Prepositioning of essential medicines, vaccines and equipment (including diarrhoea, trauma and reproductive health kits) will help in having adequate supplies available in an emergency.
• Respond to health-related emergencies, including controlling the spread of communicable diseases. The Health Cluster will support health partners to respond to emergencies and cover critical gaps to ensure complete service delivery, including primary healthcare, health education, surgical interventions and referral and reproductive health-care in line with the Minimum Initial Service Package.
Beneficiaries targeted by health partners in 2013Total: the Health Cluster aims to assist up to 2.9 million individuals with medical consultations and healthcare services in 2013.The Health Cluster estimates that the majority of the Republic of South Sudan’s 4.6 million people in need, including returnees, refugees and displaced people, will require some form of healthcare support. The Health Cluster plans to provide 2.1 million medical consultation to host communities (a minimum of 0.4 consultation per person per year), as well as one consultation per person to 785 000 emergency-affected people.
Geographical areas targeted by health partners in 2013Health Cluster partners will be continue to operate in all ten of the Republic of South Sudan’s states.
Health sector funding requirements for 2013 Health partners are appealing for a total of US$ 88 400 471 in 2013 Health partners appealing for funding in the 2013 appeal are: Cooperative for Assistance and Relief Everywhere, Comitato Collaborazione Medica (Medical Collaboration Committee), Catholic Agency for Overseas Development, International Rescue Committee, Medical Environmental Development with Air Assistance, Medical Emergency Relief International, Nile Hope Development Forum, Relief International, United Nations Population Fund, United Nations Children’s Fund, United Nations Industrial and Development Organization, Collegio Universitario Aspirante E Medici Missionnari, International Medical Corps United Kingdom, International Organization for Migration, Malteser International, The Health Support Organization, Upper Nile Kala-azar Eradication Association, American Refugee Committee, Catholic Diocese of Torit, Christian Mission Aid, Comitato di Coordinamento delle Organizzazioni per il Servizio Volontario (Coordinating Committee for International Voluntary Service), Oxford Committee for Famine Relief-Great Britain, Samaritan’s Purse, Save the Children, Solidarités, United Nations High Commissioner for Refugees, Agency for Technical Cooperation and Development, Danish Refugee Council, Handicap International, Lutheran World Federation, and the World Health Organization.
WHO funding requirements for 2013WHO is appealing for a total of US$ 10 604 040 to implement the following projects:
Project titles Requested funds*Responding to health-related emergencies in populations of humanitarian concern in the Republic of South Sudan SSD-13/H/55471/122
10 604 040
* Amounts given in US dollars.

34
World Health Organization humanitarian response in 2013
With a gross domestic product per capita amounting to US$ 284, the fourth lowest worldwide, Somalia is one of the poorest countries in the world. Conflict and instability over the last two decades have caused massive dis-placement, destroyed local social mechanisms, and prevented institutional in-vestment critical to ensure services and livelihoods. Furthermore, the 2011 famine in Somalia led to the loss of livestock which are the prime family asset for Somali rural populations. It also created displacement as households went off in search of food and other resources. The quality of health, nutrition, edu-cation and water and sanitation services across the country remains extremely poor due to weak governance, lack of access, insufficient numbers of skilled staff, as well as low and irregular salaries.
Health Sector SituationChild and maternal mortality rates continue to be among the highest in the world: one out of ten Somali children dies before seeing their first birthday. Almost a third of all deaths under the age of five are birth-related, another quarter can be attributed to pneumonia and 16% caused by diarrhoea. One out of twelve women dies due to pregnancy-related causes. The lack of ade-quate pre-natal and maternal care, coupled with a high fertility rate (6.3), puts women at elevated and recurrent risk. Maternal and child malnutrition is the cause of more than one-third of all deaths of children under five. Throughout the country, an estimated 236 000 children are acutely malnourished and in need of specialized nutrition treat-ment services. Health service provision is weak with one physician per about 25 000 and a nurse/midwife per 9000 people, respectively. An estimated 71% of the Somali population does not have reliable access to safe water throughout the year, and 77% of the population does not have access to adequate sanitation facilities.
Health Sector Priorities The Health Cluster will focus on ‘building back better’ by:• Establishing an appropriate, sustainable humanitarian health system in the
north; • Building preparedness systems and capacities to deal with any future crisis
in the south;• Instigating vulnerability reduction measures throughout the country. The Health Cluster will predominantly address life-saving humanitarian issues with linkages to resilience-building efforts. Health interventions will be modu-lated over three years, with more life-saving in year one, then increasing access to basic health services, and moving to more resilience-building activities by year three on tailor-made area-based approaches. Health Cluster action will evolve around the following priorities: • Prevent and control epidemic-prone and other communicable diseas-
es through expansion of surveillance, disaster risk reduction, emergen-cy preparedness and life-saving humanitarian health services for various Somali zones and target populations (e.g. internally displaced persons, re-turnees and vulnerable groups) in line with the national Health Strategic Frameworks.
• Increase access to high-impact emergency obstetric and routine repro-ductive, maternal and newborn and child health services as per national priority packages (e.g. Minimum Initial Service Package) to harness sta-bility, resilience and facilitate progress towards health-related Millennium Development Goals.
Somalia16
WHO funding for 20122012 Requirements: US$ 10 572 141
2012 Funding: US$ 4 406 961
FundingGap
Gap 58.3%
Baseline indicators Estimate
Human development index1 2011 -Population in urban areas% 2010 37Population using improved water source%
2008 30
Population using improved sanitation%
2008 23
Life expectancy at birth 2009 51 yearsInfant mortality rate / 10002 2010 108Under 5 mortality rate / 10002 2010 180Maternal mortality ratio / 100 0002 2010 1000[460-
2400]*Measles coverage among one year old’s%
2010 46
Wasting% 3 2004 13.2Health system efficiency rank 4
2000 179/191
2012 Donors In 2012 WHO received financial contri-butions to support its humanitarian work in Somalia from the United States of America and the Common Humanitarian Fund.
Source: WHO Global Health Observatory unless indicated other-wise by a footnote. References on page 46

35
• Facilitate early recovery and transition of health systems through enhanced coordination with humanitarian and development partners and the provision of technical support and capacity-building of partners outlined in the hu-manitarian partnership principles.
Beneficiaries targeted by health partners in 2013Total: 3 549 955 (1 829 447 women and 1 365 508 men)
Geographical areas targeted by health partners in 2013Priority locations include regions that are currently not covered by existing health sector plans (except emergency pre-paredness plans for emergencies in hot-spot areas) in South and Central Somalia, Somaliland and Puntland.
Health sector funding requirements for 2013 Health partners are appealing for a total of US$ 90 219 661 Health partners appealing for funding in the 2013 appeal are: Action Africa Help International, Action Contre la Faim, American Refugee Committee, Aamin Voluntary and Relief Organization, INTERSOS, Komitee Cap Anamur, Cooperazione e Sviluppo (Cooperation and Development), Comitato Internazionale per lo Sviluppo dei Popoli (International Committee for the Development of People), Cooperazione Internazionale (International Cooperation), Comitato di Coordinamento delle Organizzazioni per il Servizio Volontario (Coordinating Committee for International Voluntary Service), Gruppo per le Relazioni Transculturali (Group for Transcultural Relations), Humanitarian Initiative Just Relief Aid Organization, International Medical Corps, International Organization for Migration, Islamic Relief Worldwide, International Resuce Committee, Médecins du Monde France, Medical Emergency Relief International, Mulrani International, Relief International, Family Empowerment and Relief Organization, Salama Medical Agency, Save the Children, Somali Young Doctors Association, Switzerland-Somalia ‘Kalmo’ (peace and affinity) , United Nations Children’s Fund, Women and Health Alliance, WARDI Relief and Development Initiatives, Zamzam Foundation, Intersos, Kissito Healthcare International, Medical Environmental Development with Air Assistance, Mercy-USA for Aid and Development, United Nations Population Fund, Muslim AID and the World Health Organization.
WHO funding requirements for 2013WHO is appealing for a total of US$ 18 811 556 for the following projects:
Project titles Requested funds*Promotion of mental health and prevention, treatment and rehabilitation of MNS disorders, with respect for human rights and social protection, for people affected by conflicts and crisis in Somalia SOM-13/H/56500/122
562 438
Extension of access to emergency health care and life-saving services, including emergency surgi-cal procedures and Comprehensive Emergency Obstetric Care through direct service delivery, strengthening the referral networks, scaling up health facilities, and training of health workers to be able to facilitate and provide the servicesSOM-13/H/56710/122
4 500 000
Provision of life-saving child health services to vulnerable and newly accessible populations in Somalia, through Child Health Days, focusing on South and Central SomaliaSOM-13/H/56712/122
3 648 423
Provision of Maternal and Newborn Health Services Within the Continuum of CareSOM-13/H/56712/122
706 200
Promotion of health services for the prevention and control of Neglected Tropical DiseasesSOM-13/H/56713/122
500 000
Provision of basic essential health services to children in underserved areasSOM-13/H/56714/122
1 846 000
Provision of a coordinated response for the delivery of essential health services to the most vulnerable population in order to reduce morbidity and mortality in SomaliaSOM-13/H/56715/122
1 622 495
Strengthening laboratory and blood safety servicesSOM-13/H/56716/122
821 420
Enhancing blood safety, general lab capacity, and other interventions to address HIV/AIDS and other disease prevention and treatment, in the humanitarian response in SomaliaSOM-13/H/56719/122
1 391 000
* Amounts given in US dollars.
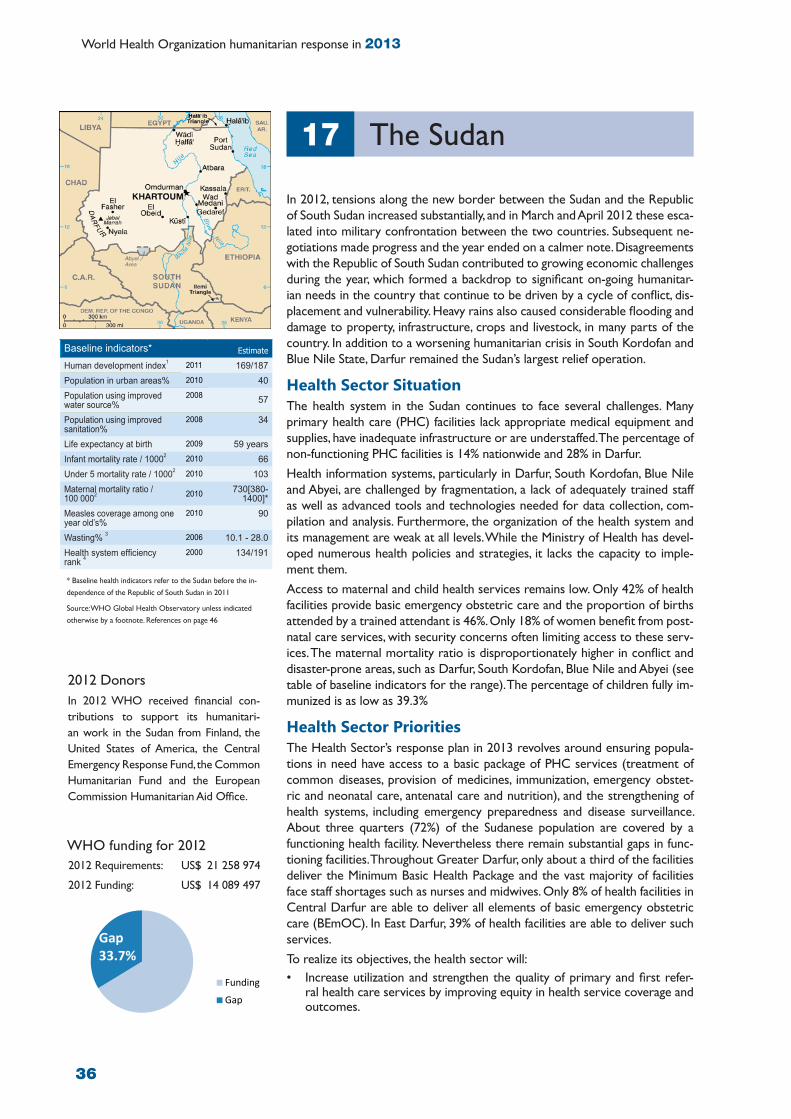
36
World Health Organization humanitarian response in 2013
In 2012, tensions along the new border between the Sudan and the Republic of South Sudan increased substantially, and in March and April 2012 these esca-lated into military confrontation between the two countries. Subsequent ne-gotiations made progress and the year ended on a calmer note. Disagreements with the Republic of South Sudan contributed to growing economic challenges during the year, which formed a backdrop to significant on-going humanitar-ian needs in the country that continue to be driven by a cycle of conflict, dis-placement and vulnerability. Heavy rains also caused considerable flooding and damage to property, infrastructure, crops and livestock, in many parts of the country. In addition to a worsening humanitarian crisis in South Kordofan and Blue Nile State, Darfur remained the Sudan’s largest relief operation.
Health Sector SituationThe health system in the Sudan continues to face several challenges. Many primary health care (PHC) facilities lack appropriate medical equipment and supplies, have inadequate infrastructure or are understaffed. The percentage of non-functioning PHC facilities is 14% nationwide and 28% in Darfur. Health information systems, particularly in Darfur, South Kordofan, Blue Nile and Abyei, are challenged by fragmentation, a lack of adequately trained staff as well as advanced tools and technologies needed for data collection, com-pilation and analysis. Furthermore, the organization of the health system and its management are weak at all levels. While the Ministry of Health has devel-oped numerous health policies and strategies, it lacks the capacity to imple-ment them.Access to maternal and child health services remains low. Only 42% of health facilities provide basic emergency obstetric care and the proportion of births attended by a trained attendant is 46%. Only 18% of women benefit from post-natal care services, with security concerns often limiting access to these serv-ices. The maternal mortality ratio is disproportionately higher in conflict and disaster-prone areas, such as Darfur, South Kordofan, Blue Nile and Abyei (see table of baseline indicators for the range). The percentage of children fully im-munized is as low as 39.3%
Health Sector Priorities The Health Sector’s response plan in 2013 revolves around ensuring popula-tions in need have access to a basic package of PHC services (treatment of common diseases, provision of medicines, immunization, emergency obstet-ric and neonatal care, antenatal care and nutrition), and the strengthening of health systems, including emergency preparedness and disease surveillance. About three quarters (72%) of the Sudanese population are covered by a functioning health facility. Nevertheless there remain substantial gaps in func-tioning facilities. Throughout Greater Darfur, only about a third of the facilities deliver the Minimum Basic Health Package and the vast majority of facilities face staff shortages such as nurses and midwives. Only 8% of health facilities in Central Darfur are able to deliver all elements of basic emergency obstetric care (BEmOC). In East Darfur, 39% of health facilities are able to deliver such services. To realize its objectives, the health sector will:• Increase utilization and strengthen the quality of primary and first refer-
ral health care services by improving equity in health service coverage and outcomes.
The Sudan17
WHO funding for 20122012 Requirements: US$ 21 258 974
2012 Funding: US$ 14 089 497
Funding
Gap
Gap 33.7%
Baseline indicators* Estimate
Human development index1 2011 169/187Population in urban areas% 2010 40Population using improved water source%
2008 57
Population using improved sanitation%
2008 34
Life expectancy at birth 2009 59 yearsInfant mortality rate / 10002 2010 66Under 5 mortality rate / 10002 2010 103Maternal mortality ratio / 100 0002 2010 730[380-
1400]*Measles coverage among one year old’s%
2010 90
Wasting% 3 2006 10.1 - 28.0Health system efficiency rank 4
2000 134/191
* Baseline health indicators refer to the Sudan before the in-dependence of the Republic of South Sudan in 2011
Source: WHO Global Health Observatory unless indicated otherwise by a footnote. References on page 46
2012 Donors In 2012 WHO received financial con-tributions to support its humanitari-an work in the Sudan from Finland, the United States of America, the Central Emergency Response Fund, the Common Humanitarian Fund and the European Commission Humanitarian Aid Office.

37
• Improve emergency preparedness, risk reduction, disease surveillance, and the prevention and control of epidemic-prone and communicable diseases.
• Build the capacity of the health workforce to achieve sufficient numbers of trained personnel with the right mix of skills to respond to the health needs of vulnerable populations.
• Mainstream cross-cutting themes such as gender, environment, early recovery and HIV/AIDS into all health programmes.
• Differentiate between the needs of women, girls, men and boys
Beneficiaries targeted by health partners in 2013Total target population: 3 937 322 (1 956 734 women and 1 980 588 men). Target beneficiaries are internally displaced persons and returnees (a total of 2.56 million persons) and affected host populations (a total of 1.37 million persons).
Geographical areas targeted by health partners in 2013In 2013, Darfur, South Kordofan, Abyei, Blue Nile State and East Sudan, remain the priority areas for humanitarian health interventions.
Health sector funding requirements for 2013 Health partners are appealing for a total of US$ 75 383 641 in 2013Health partners appealing for funding in the 2013 appeal are: Almassar Charity Organization for Nomads, American Refugee Committee, CARE International Switzerland in Sudan, Comitato di Coordinamento delle Organizzazione per il Servizio Volontario, Concern Worldwide, EMERGENCY, GOAL, HelpAge International, Human Relief Foundation UK, Humanitarian Aid and Development Organization, International Medical Corps UK, Islamic Relief Worldwirde, Johanniter, Kuwaiti Patients Helping Fund, Medical Emergency Relief Internationa, Mercy Malaysia, Mubadiroon Organization, Muslim Aid, Norwegian Church Aid, Om Al Momineen Charity Organization for Development, Panhealth Care Organization, Partner Aid International, Relief International, Rufaida Health Foundation, Save the Children, Sudanese Development Call Organization, Sudanese Red Crescent, Talawiet Organization for Development, United Nations Children’s Fund, United Nations Population Fund, World Health Organization, World Relief, and World Vision Sudan.
WHO funding requirements for 2013WHO is appealing for a total of US$ 17 546 407 for the following projects:
Project titles Requested funds*Support access to quality health services including communicable disease control and prevention SUD-13/H/54396/122
14 235 400
Nutrition support for Blue Nile, White Nile and Sinnar StatesSUD-13/H/54952/122
1 310 107
Support to emergency and recovery WASH interventions in Darfur, East and transitional areas SUD-13/WS/54913/122
2 000 900
* Amounts given in US dollars.

38
World Health Organization humanitarian response in 2013
The Syrian Arab Republic18
WHO funding for 20122012 Requirements: US$ 31 145 000
2012 Funding: US$ $ 8 556 692
FundingGap
Gap 72.5%
Baseline indicators* Estimate
Human development index1 2011 119/187Population in urban areas% 2010 56Population using improved water source%
2008 89
Population using improved sanitation%
2008 96
Life expectancy at birth 2009 74 yearsInfant mortality rate / 10002 2010 14Under 5 mortality rate / 10002 2010 16Maternal mortality ratio / 100 0002 2010 70[41-110]*
Measles coverage among one year old’s%
2010 82
Wasting% 3 2006 11.5Health system efficiency rank 4
2000 108/191
2012 Donors In 2012 WHO received financial contri-butions to support its humanitarian work in the Syrian Arab Republic from Finland, Ireland, Italy, the League of Arab States, Norway, the United States of America, the Central Emergency Response Fund and the OCHA Emergency Response Fund.
The events in the Syrian Arab Republic since March 2011 have resulted in significant humanitarian needs of directly affected populations which include those injured during the events, families who lost their breadwinners or left their home areas as well as the relatives, friends and communities hosting them. The consequences of the events are manifold and mainly include.• The aggravation of poverty• Damage to housing and infrastructure including water and power utilities,
schools, medical and other social service facilities, industrial and agricultural infrastructure;
• Fuel shortages • Disruptions to telecommunications; • A rapid shrinkage of the private sector and the informal sector, leading to
livelihood losses and rising unemployment; • Unsafe movement on major routes in the country and across bordersFurthermore, the effect of economic sanctions is also aggravating the situa-tion, as international transactions are becoming more difficult for both the public and the private sectors. Sanctions also significantly affected the import of fuel derivatives, which created shortages in the local market and resulted in the increase of prices of diesel and heating oil, as well as overall living costs for families.
Health Sector SituationThe current events in the Syrian Arab Republic have caused a serious disrup-tion of the health system through adverse effects on the health care infrastruc-ture, lack of access to health facilities, the decreasing availability of the health workforce, and the lack of essential medicines and supplies. According to Government statistics, as of January 2013, almost 55% of public hospitals, approximately 10% of health centres and 58% of ambulances have been damaged or destroyed. The functioning hospitals are often overwhelmed with patients. There are reports of hospitals being targeted and destroyed in contested areas.The worsening security situation is preventing many health care workers from reporting to duty, contributing to severe staffing shortages in hospitals and other health facilities. Many doctors have left the country. For example, over 50% of the medical doctors have left Homs. In Damascus, Aleppo and Homs at least 70% of the health providers live in rural areas and therefore frequent-ly cannot reach their work place due to irregular public transportation, and blocked and unsafe roads. Prior to the current situation, over 51% of health expenditure was out-of-pocket, mainly to cover the costs of medicines and hospitalization in the pri-vate sector. In the current situation of socio-economic deterioration and the consequent reduction in the number of operational public health facilities, the private sector is being used by the minority that can afford it, while most peo-ple are relying on the remaining under-resourced public health services.Before the current events started in March 2011, more than 90% of medi-cines in Syria were locally produced. The combined effects of economic sanc-tions, currency fluctuations unavailability of hard currency, fuel shortages and increases in operational costs have adversely affected the production of medi-cines and pharmaceutical products. In affected areas there is a critical short-age of life-saving medicines, for example, insulin is not available in a number of areas. Even where limited medicines and supplies are available, their equitable distribution is difficult due to the current situation.
Source: WHO Global Health Observatory unless indicated other-wise by a footnote. References on page 46

39
Accessing reproductive health care services poses a challenge in crisis areas. An increasing number of pregnant women are requesting an elective C-section as they are worried that they will not be able to reach clinics and hospitals in time for delivery.Similarly, the current situation has created challenges in implementing the national immunization programme. The ship-ment of vaccines has been complicated and there are difficulties in maintaining the cold chain, which has resulted in a number of unusable vaccines. The national vaccination coverage for the first quarter of 2012 dropped from 95% to an estimated 80%.The prolonged crisis has resulted in growing unavailability of food and fuel for transport and heating. Living conditions are unhygienic, health care services are inaccessible or limited and immunization coverage for children under five re-duced. These combined factors may have serious implications on the nutritional status of children under five and preg-nant and lactating women. There are reports of growing mental health needs. Mobile clinics report an increasing number of people seeking psy-chosocial assistance for affected family members.
Health Sector Priorities Health sector objectives include:• To support effective and efficient delivery of life-saving emergency health care (medical, surgical, maternal, child
health, etc.) at all levels of health facilities in directly and indirectly affected areas.• To facilitate the population’s access to essential primary and secondary health care (both preventive and curative)
including support for chronic diseases, reproductive health, infant and child health, nutrition, and mental health services.
The strategy to reach these objectives includes the following priority actions: • Coordinate the Health Sector response by working with the Ministry of Health, the Ministry of Higher Education,
non-governmental organizations and community based organizations. • Implement interventions to fill the gaps in health service delivery through local non-governmental organizations and
in close cooperation with the Ministry of Health. • Distribute essential medicines and supplies to health facilities and to implementing partners with access to conflict
areas.• Deliver a standardized package of essential of quality health care services (preventive and curative) through imple-
menting partners.• Support the regular supply of essential medicines and supplies through a functioning supply chain with emergency
medical stockpiles at the regional level. • Update information on health needs and service availability through on-going integrated assessment missions with
relevant UN partners (WHO, UNICEF, UNFPA, WFP and UNHCR) and in close cooperation with the Ministry of Health.
• Monitor service delivery and remote activities using participating non-governmental organizations and community-based organizations.
• Standardize systems for reporting with implementing partners.• Strengthen the health response capacity of the Ministry of Health and implementing partners. • Conduct advocacy activities with international and national stakeholders to raise awareness for the respect and sup-
port of health-humanitarian principles.• Mobilize resources for health.
Beneficiaries targeted by health partners in 2013The overall target population includes 4 million conflict-affected persons.• 430 000 diabetic patient out of which 40 000 are insulin-dependent children• 5000 haemodialysis patients• 3572 tuberculosis patients• 56 000 cardiovascular patients• 42 000 chronic respiratory patients• 400 000 for trauma-related injuries• 50 000 surgical assistance; (men, women, children)• Supplies for 20 000 post-operative hospital care patients• About 1 million women, men, girls and boys in need of psychosocial assistance• About 1.2 million persons affected by, or at risk of, malnutrition

40
World Health Organization humanitarian response in 2013
Geographical areas targeted by health partners in 2013Based on locations served in 2012, the target areas in 2013 are planned to include: Damascus, Rural Damascus, Aleppo, Rural Aleppo, Homs, Hama, Idleb, Dara’a, Albou Kamal, Deir el-Zour, and MouadamiehRoughly half of those in need are located in the three most affected governorates: Aleppo (19.8%); Homs (14.8%); and Rural Damascus (14.8%).
Health sector funding requirements for 2013 Health partners are appealing for a total of US$ 81 905 133 Health partners appealing for funding in the 2013 appeal are: United Nations Population Fund, United Nations Development Programme, United Nations Relief and Works Agency, United Nations High Commissioner for Refugees, and the World Health Organization.
WHO funding requirements for 2013WHO is appealing for a total of US$ 48 465 000 for the following projects:
Project titles Requested funds*Support health information management and coordination SYR-13/CSS/57248/122
2 600 000
Expand nutritional support servicesSYR-13/H/57242/122
1 850 000
Rehabilitation and restoration of damaged/non-functional health facilities in affected areasSYR-13/H/57243/122
5 480 000
Strengthen the capacity for health responseSYR-13/H/57244/122
5 100 000
Strengthen trauma and referral managementSYR-13/H/57245/122
9 335 000
Support delivery of primary health careSYR-13/H/57246/122
7 950 000
Support delivery of secondary and tertiary health careSYR-13/H/57247/122
9 950 000
Support mental health services (WHO) and psychosocial services (UNDP) SYR-13/H/57249/122
3 100 000
Safety and security for humanitarian assistanceSYR-13/S/57240/122
1 000 000
Restoration of water supply, sanitation, solid waste, hygiene and drainage services in healthcare facilities and hospitalsSYR-13/WS/57241/122
2 100 000
* Amounts given in US dollars.

41
Conflict, extreme poverty, volatile food and commodity prices, increasing cost of living and unemployment constitute the main drivers of the crisis that Yemen is currently facing. The Government’s capacity to provide social serv-ices remains low in many parts of the country. New localized conflicts, particu-larly in the north and the south, are expected to continue in 2013, exacerbated by weak rule of law and security systems.
Health Sector SituationThe year 2012 has witnessed repeated disease outbreaks such as measles, den-gue, chikungunya and even cases of polio. Epidemiological data suggests that the key causes of morbidity in communities are diarrhoea, acute respiratory tract infections (ARI) and malaria. According to WHO data, children under five years of age account for nearly 50% of diarrhoea and ARI cases.On-going conflict and socio-economic disruption in Yemen have reduced the capacity of health care services to address the health needs of the popula-tion. In July 2012, WHO assessed 49 health facilities in Abyan, 44 (90%) of which lacked the essential medicines required for a minimum package of health care services. The same assessment found that out of 49 health facilities, 18 (37%) were partially or fully damaged and nine (18%) were looted. Only 6% of the health facilities in Abyan were conducting immunization on a daily basis. Furthermore, substantial gaps remain in the area of reproductive health and family planning.
Health Sector Priorities Priority 1: Ensure effective intra- and inter-cluster coordination, pri-marily between the Health, Nutrition and WASH Clusters. Focus on joint needs assessment, programming, monitoring and evaluation, in order to ensure a more effective and efficient response to the humanitarian health needs of crisis-affected and other vulnerable populations, especially women and children.Planned outputs: Enhanced intra- and inter-cluster coordination mechanisms and processes will be implemented through updating and sharing a standard re-porting format on a monthly basis, conducting joint assessments, and planning and implementing joint health, nutrition and water and sanitation programmes.
Priority 2: Improve access to quality primary and secondary (hos-pital) health-care services, including basic health and emergency referral services for vulnerable populations, through a focused ap-proach on health system strengtheningPlanned outputs: Vulnerable populations will have improved access to a stand-ardized package of quality life-saving, essential health care services. This package should encompass Integrated Management of Childhood Illness, the Minimum Initial Service Package for reproductive health (including the clinical manage-ment of victims of sexual violence), clinical management of severely malnour-ished children with health complications and treatment of patients suffering from chronic diseases and mental health conditions.
Priority 3: Strengthen local capacity in priority districts to detect, prepare for, respond to, mitigate and manage health risks with a fo-cus on communicable diseases and seasonal emergencies Planned output: Emerging health threats and outbreaks are prevented through fast, timely, effective and coordinated joint health interventions. A weekly sur-veillance report will be disseminated among partners.
Yemen19
WHO funding for 20122012 Requirements: US$ 42 213 597
2012 Funding: US$ 8 319 490
Funding
Gap
Gap 80.3%
Baseline indicators Estimate
Human development index1 2011 154/187Population in urban areas% 2010 32Population using improved water source%
2008 62
Population using improved sanitation%
2008 52
Life expectancy at birth 2009 65 yearsInfant mortality rate / 10002 2010 57Under 5 mortality rate / 10002 2010 77Maternal mortality ratio / 100 0002 2010 200[110-370]*
Measles coverage among one year old’s%
2010 73
Wasting 3 2003 15.2%Health system efficiency rank 4
2000 120/191
2012 Donors In 2012 WHO received financial con-tributions to support its humanitarian work in Yemen from Japan, the League of Arab States, Spain, the United States of America, the Central Emergency Response Fund, and the OCHA Emergency Response Fund.
Source: WHO Global Health Observatory unless indicated other-wise by a footnote. References on page 46

42
World Health Organization humanitarian response in 2013
Priority 4: Prevent excess maternal and child morbidity and mortality within priority districts, focusing on safe motherhood and child survival interventionsPlanned output: Health services and standards for mothers and neonates are improved, and avoidable morbidity and mortality among pregnant women, neonates and young children lowered, particularly through the implementation of vaccination campaigns in camps, urban and rural settings.
Beneficiaries targeted by health partners in 2013Total: 4 195 690 beneficiaries, including 2 139 802 women.
Geographical areas targeted by health partners in 2013Health action will be concentrated in 59 districts that are identified through geographical prioritization and needs as-sessment criteria, including the total affected population, internally displaced populations, availability of basic health care services and coverage of measles vaccination. The priority is on the following locations: Taizz, Aden, Lahj, Abyan, Amran, Ibb, Al-Dhali, Hodieda, Sa’ada, Sana’a, Al-Baydah and Hajjah Governorates.
Health sector funding requirements for 2013 Health partners are appealing for a total of US$ 58 652 315 Health partners appealing for funding in the 2013 appeal are: Relief International, United Nations Population Fund, Save the Children, Médecins du Monde France, Adventist Development and Relief Agency, International Rescue Committee, Yemen Family Care Association, Medical Emergency Relief International, International Medical Corps, International Organization for Migration, United Nations Children’s Programme, Joint United Nations Programme on HIV/AIDS, and the World Health Organization.
WHO funding requirements for 2013WHO is appealing for a total of US$ 33 430 350 for the following projects:
Project titles Requested funds*Delivery of an essential package of life saving health care services and revitalization of health services for IDPs, host and other affected communities including nutritional surveillance and mass casualty management during potential violence YEM-13/H/53769/122
24 460 200
Surveillance and response to epidemics and other public health events of national concern; pre-vention, control and treatment of vaccine-preventable and endemic diseases in the affected areas of Yemen YEM-13/H/53787/122
4 916 650
Health cluster coordination at central and field levels for effective humanitarian action YEM-13/H/53885/122
588 500
Supporting of nutrition services and malnutrition case management through the establishment of stabilization centres YEM-13/H/53699/122
1 465 000
Provision of WASH services for health facilities in conflict affected areas YEM-13/WS/53697/122
2 000 000
* Amounts given in US dollars.

43
While the overall humanitarian situation has continued to improve and re-mained largely stable in 2012, a significant number of highly vulnerable groups, including displaced and migration-affected populations, still require humani-tarian aid. Vulnerabilities include drought-related food insecurity which is ex-pected to increase in 2013, as well as outbreaks of epidemic-prone diarrhoeal diseases.
Health Sector SituationThe overall impact of Zimbabwe’s decade-long economic decline and cuts in public health expenditure have resulted in the deterioration of health care fa-cility infrastructures at all levels. Access to basic health care has been greatly reduced. In addition, key activities such as outreach services, referral of patients, drug distribution, surveillance, as well as monitoring and evaluation of local health centres are hampered by the lack of transport possibilities and poor road networks. The lack of hu-man resources has further compounded the decline in critical public health programmes and the quality and coverage of services in areas such as ca-pacity building for emergency preparedness and response as well as disease surveillance.Epidemiological reports by the Ministry of Health and Child Welfare (MoHCW) as well as outbreak response reports by WHO and partners indicate that Zimbabwe continues to be vulnerable to outbreaks of epidemic-prone diar-rhoeal diseases such as cholera, typhoid fever, rotavirus and dysentery. The decline in access to clean water and sanitation facilities has further complicat-ed the situation. In 2011, ten out of the country’s 62 districts (Bikita, Buhera, Chimanimani, Chegutu, Chipinge, Chiredzi, Kadoma, Murehwa, Mutare and Mutasa) reported 1140 cases of cholera and 45 deaths, giving a crude case fa-tality rate of 4.0%. As of 21 October 2012, typhoid fever outbreaks in Harare, Chitungwiza, Bindura and Zvimba had reached a cumulative figure of 4940 cas-es and three deaths. From 2 May to 19 June 2012, Chiredzi district reported 22 cases and one death from cholera. Zimbabwe continues to have a high prevalence of HIV infection which presents a high economic burden on an already stretched health system and increases the vulnerability of populations to the effects of disease outbreaks.
Health Sector PrioritiesThe Health Cluster will continue to foster close coordination with the MoHCW to ensure that cluster priorities are aligned with those of the MoHCW. Planned interventions will support the restoration of basic and life-saving services by strengthening existing MoHCW systems and structures and filling gaps in the health care delivery system. The focus will be on the most vulnerable rural and peri-urban districts.
Priority 1: Strengthen country-wide disease surveillance and emer-gency preparednessActivities under this priority will focus on strengthening preparedness and rapid response mechanisms in areas vulnerable to epidemic-prone diseases and natural disasters through:• Training key cadres of the National Health System, including clinical and
health information personnel, community health workers and members of the health executive teams on case management, integrated disease sur-veillance and response, as well as information management.
Zimbabwe20
WHO funding for 20122012 Requirements: US$ 1 700 000
2012 Funding: US$ 707 210
Baseline indicators Estimate
Human development index1 2011 173/187Population in urban areas% 2010 38Population using improved water source%
2008 82
Population using improved sanitation%
2008 44
Life expectancy at birth 2009 49 yearsInfant mortality rate / 10002 2010 51Under 5 mortality rate / 10002 2010 80Maternal mortality ratio / 100 0002 2010 570[320-920]*
Measles coverage among one year old’s %
2010 84
Wasting% 3 2011 3.1Health system efficiency rank 4
2000 155/191
2012 Donors In 2012 WHO received financial con-tributions to support its humanitarian work in Zimbabwe from the European Commission Humanitarian Aid Office.
Funding
Gap
Gap 58.4%
Source: WHO Global Health Observatory unless indicated other-wise by a footnote. References on page 46

44
World Health Organization humanitarian response in 2013
• Providing direct technical support for outreach activities in emergency affected and vulnerable areas for information dissemination, immunization campaigns, primary health care service delivery and psycho-social interventions.
• Revitalizing information sharing and coordination mechanisms, including at the community, district and provincial levels, for disaster risk reduction and response planning.
• Supporting the provision and pre-positioning of medical supplies, communication materials and offering logistics support
Priority 2: Reduce morbidity and mortality due to diarrhoeal disease outbreaks in Chipinge, Chimanimani and Chiredzi districtsActivities will be concentrated on three of the most vulnerable districts, namely Chipinge, Chimanimani and Chiredzi. They will include:• Training rapid response teams and health staff on case management as well as integrated disease surveillance and
response.• Conducting social mobilization sessions in communities.• Increasing coordination with the district health teams and joint supervision in the field.• Procuring emergency supplies, including laboratory supplies.
Beneficiaries targeted by health partners in 2013Total: 692 422 (360 059 women and 332 363 men)
Geographical areas targeted by health partners in 2013The geographical areas targeted will include 29 districts in Zimbabwe, with a particular focus on Chipinge, Chimanimani and Chiredzi districts.
Health sector funding requirements for 2013 Health partners are appealing for a total of US$ 4 990 000 Health partners appealing for funding in the 2013 appeal are the International Organization for Migration and the World Health Organization.
WHO funding requirements for 2013WHO is appealing for a total of US$ 3 000 000 for the following projects:
Project titles Requested funds*Strengthening capacity for early warning and early action in response to public health emergenciesZIM-13/H/54465/122
2 000 000
Diarrhoeal disease outbreak preparedness and response in Chimanimani, Chipinge and Chiredzi DistrictsZIM-13/H/54467/122
1 000 000
* Amounts given in US dollars.

45
List of acronyms21
ARI Acute respiratory tract infectionBHS Barangay health stationCAP Consolidated Appeal ProcessCERF Central Emergency Response FundDEWS Disease Early Warning SystemDPC Direction de la Protection CivileECHO Humanitarian Aid Office of the European CommissionEPI Expanded Programme on Immunization FMoH Federal Ministry of HealthGAM Global acute malnutritionHIV Human Immune-Deficiency VirusHIV/AIDS Human Immune Deficiency Virus/Acquired Immuno-Deficiency SyndromeIDPs Internally displaced personsIMCI Integrated Management of Childhood IllnessIOM International Organization for MigrationMISP Minimum Initial Service PackageMoH Ministry of HealthMoHCW Ministry of Health and Child WelfareMoPH Ministry of Public Health and PopulationNGO Nongovernmental organizationOCHA United Nations Office for the Coordination of Humanitarian AffairsPHC Primary health carePMTCT Prevention of mother to child transmissionSGBV Sexual and gender-based violenceSRH Sexual and reproductive healthSTI Sexually Transmissible InfectionsTBA Traditional birth attendantsUN United NationsUNAIDS UN Joint Programme on HIV/AIDSUNCT UN Country TeamUNFPA UN Population FundUNHCR UN High Commissioner for RefugeesUNICEF UN Children’s FundUNRWA UN Relief and Works Agency for Palestine Refugees in the Near EastVCT Voluntary counselling and testingWASH Water, sanitation and hygieneWFP World Food ProgrammeWHO World Health OrganizationWHO/PEC World Health Organization/Polio,Emergencies and Country Cooperation

46
World Health Organization humanitarian response in 2013
Source: WHO Global Health Observatory1 Source: UNDP2 live births3 Weight-for-Height <-2 z-scores of WHO Growth Standards, among children 0-59 months.
Source: WHO Global Database on Child Growth and Malnutrition4 Source: WHO Measuring overall health system performance
* 95% confidence interval
Baseline indicators* Estimate
Human development index1 2011 000/000Population in urban areas% 2010 00Population using improved water source%
2008 00
Population using improved sanitation%
2008 00
Life expectancy at birth 2009 0 yearsInfant mortality rate / 10002 2010 00Under 5 mortality rate / 10002 2010 00Maternal mortality ratio / 100 0002 2010 000[000-000]*
Measles coverage among one year old’s%
2010 00
Wasting% 3 2006 00.0Health system efficiency rank 4
2000 000/000
References22
47
World Health Organization20 Avenue Appia1211 Geneva 27SwitzerlandTelephone: + 41 22 791 21 11Facsimile: + 41 22 791 31 11E-mail: [email protected] www.who.int/disasters
Regional Office for AfricaEmergency and Humanitarian ActionBP 06 Cité du Djoué Brazzaville Republique du CongoTelephone: + 47 241 39100 / + 242 770 02 02Facsimile /Registry): + 47 241 39503E-mail: [email protected] http://www.afro.who.int/
Regional Office for the AmericasEmergency Preparedness and Disaster Relief525, 23rd Street, N.W.Washington, DC 20037United States of AmericaTelephone: +1 202 974 3000Facsimile: +1 202 974 3663E-mail: [email protected] http://www.paho.org/disasters/
Regional Office for the Eastern MediterraneanEmergency Preparedness and Humanitarian ActionMonazamet El Seha El Alamia StreetExtension of Abdul Razzak Al SanhouriP.O. Box 7608,Nasr City, Cairo 11371 EgyptTelephone: + 202 2276 50 00 Facsimile: + 202 2 2670 24 92 E-mail: [email protected]://www.emro.who.int/eha
Regional Office for EuropeDisaster Preparedness and Response8, ScherfigsvejDK-2100 Copenhagen ØDenmarkTelephone: + 45 39 171 717Facsimile: + 45 39 171 818E-mail: [email protected] http://www.euro.who.int/
Regional Office for South-East AsiaEmergency and Humanitarian ActionWorld Health HouseIndraprastha EstateMahatama Gandhi MargNew Delhi 110 002IndiaTelephone: + 91-11-2337 0804Facsimile: + 91-11-2337 9507E-mail: [email protected] http://www.searo.who.int/
Regional Office for the Western PacificP.O. Box 29321000 ManilaThe PhilippinesTelephone: + 63 2 528 8001Facsimile: + 63 2 521 1036/526 0279E-mail: [email protected] http://www.wpro.who.int/sites/eha/
Contacts

Department for Emergency Risk Management and Humanitarian Response (ERM)
www.who.int/disasters


















