Who are children with ADHD?
50
3/28/2019 1 Attention Deficit Hyperactivity Disorder (ADHD) Who are children with ADHD? https:// www.youtube.com/watch?v=w4t4JFKDD6s&feature=youtu.be Children and adolescents with Attention and / or Hyperactivity Deficits (DDAI Italian acronym) ADHD (English acronym Attention Deficit Hyperactivity Disorder) according to the DSM-5 ICD-10 Activity and attention disorder F90.0 Attention deficit disorder with predominant inattention F98.8
Transcript of Who are children with ADHD?

3/28/2019
1
Attention Deficit HyperactivityDisorder (ADHD)
Who are children with ADHD?
https://www.youtube.com/watch?v=w4t4JFKDD6s&feature=youtu.be
Children and adolescents with Attention and / or Hyperactivity Deficits
(DDAI Italian acronym)
ADHD (English acronym Attention Deficit Hyperactivity Disorder) according to the DSM-5
ICD-10
Activity and attention disorder F90.0
Attention deficit disorder with predominant inattention F98.8

3/28/2019
2
https://www.youtube.com/watch?v=w4t4JFKDD6s&t=8s
What is ADHD?
A neurodevelopmental disorder of self-regulation of behavior that manifests itself above all with difficulty in maintaining attention, (management of cognitive effort in general), motor control and impulsive responses. In most cases it is associated with other disorders, it is disabling for the subject and creates significant social difficulties

3/28/2019
3
Brief hystory of ADHD
Still (1902): "deficit in moral control and excessivevivacity and destructiveness ..."
Levin ('30): Minimum Brain Damage
Various authors ('40): Minimal Cerebral Dysfunction
DSM-II (1968): Child's Hyperkinetic Reaction
DSM-III (1980): ADD, with or without hyperactivity
DSM-III-R (1987): ADHD (14 symptoms)
DSM-IV (1994): ADHD (18 symptoms, 3 subtypes)
DSM-5 (2013): ADHD (age onset within 12 years, adult-specific)
3 core deficits of ADHD
Inattention
Hyperactivity
Impulsiveness
Learning difficulties
Interpersonalproblem
Regulation of emotion difficulties

3/28/2019
4
ADHD Symptoms
Inattention (adult specifications):
Pay attention to details (work is inaccurate ...)
Keep the attention for a prolonged period
Avoid distractions in uninspiring tasks
Organize your activities
Coping with long tasks (revisions of documents ...)
Hyperactivity
Move excessively, even in inappropriate contexts
Often under pressure (moved by a scooter)
Continuously switching from one activity to another ....
Impulsivity
"Shoot" the answers before the question has been completed
Difficulty waiting for your turn
Stop or be intrusive towards others
Type combined ADHD-C:
inattention + hyperactivity
Prevalent inattentive ADHD-I: inattention
Prevalent hyperactiveADHD-HI: hyperactive
Subtypes of ADHD

3/28/2019
5
Entity of the ADHD problemSymptoms SDQ 6-11 years (N = 2286) Partly True
Distracted, unable to concentrate 30% 13%
He does not carry out his duties 36% 10%
Restless, hyperactive 19,5% 10%
Constantly moving 17,5% 8%
He is not able to stop and think 51% 11%
Symptoms SDQ 12-19 years (N = 991) Partly True
Distracted, unable to concentrate 33% 11,5%
He does not carry out his duties 42% 7,5%
Restless, hyperactive 18% 6%
Constantly moving 15,5% 6%
He is not able to stop and think 45% 6%
Beyond main symptoms
Poor academic performance especially in subjects requiring organization and effort (production and comprehension of texts, study, mathematics)
Difficulty in social relationships both with adults and with peers
Poor self-regulation of emotions and impulses for which they often react inadequately or commit dangerous actions
Low motivation for performing activities that require cognitive effort
3/28/2019
6
Impulsive and inattentive: difficulty or disorder?
Normality Difficulty Disorder
Difficulties are linked to adverse episodic situations or to temperamental characteristics
Behavioral signs are mainly caused by environmental factors
The difficulties are constant and interfere with the activities
Comorbidity
Children and adolescents with ADHD may also experience other psychological and psychiatric disorders at the same time (comorbidity).In 70% of cases ADHD is associated with other disorders.Comorbidity can have a more complex impact on the prognosis and management of the ADHD boy.
Oppositional Defiant Disorder and Conduct Disorder 25%
Learning Disorder 30%
Anxiety Disorder 15%
Depression 15%
3/28/2019
7
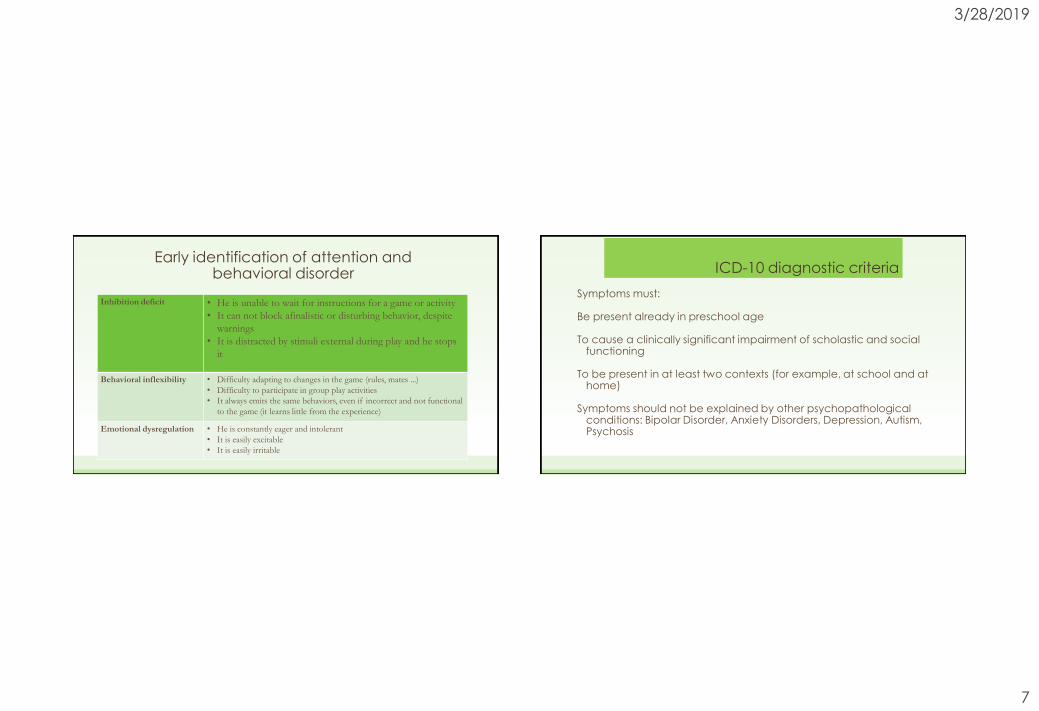
Early identification of attention and behavioral disorder
Inhibition deficit • He is unable to wait for instructions for a game or activity
• It can not block afinalistic or disturbing behavior, despite
warnings
• It is distracted by stimuli external during play and he stops
it
Behavioral inflexibility • Difficulty adapting to changes in the game (rules, mates ...)
• Difficulty to participate in group play activities
• It always emits the same behaviors, even if incorrect and not functional
to the game (it learns little from the experience)
Emotional dysregulation • He is constantly eager and intolerant
• It is easily excitable
• It is easily irritable
ICD-10 diagnostic criteria
Symptoms must:
Be present already in preschool age
To cause a clinically significant impairment of scholastic and social functioning
To be present in at least two contexts (for example, at school and at home)
Symptoms should not be explained by other psychopathological conditions: Bipolar Disorder, Anxiety Disorders, Depression, Autism, Psychosis
3/28/2019
8
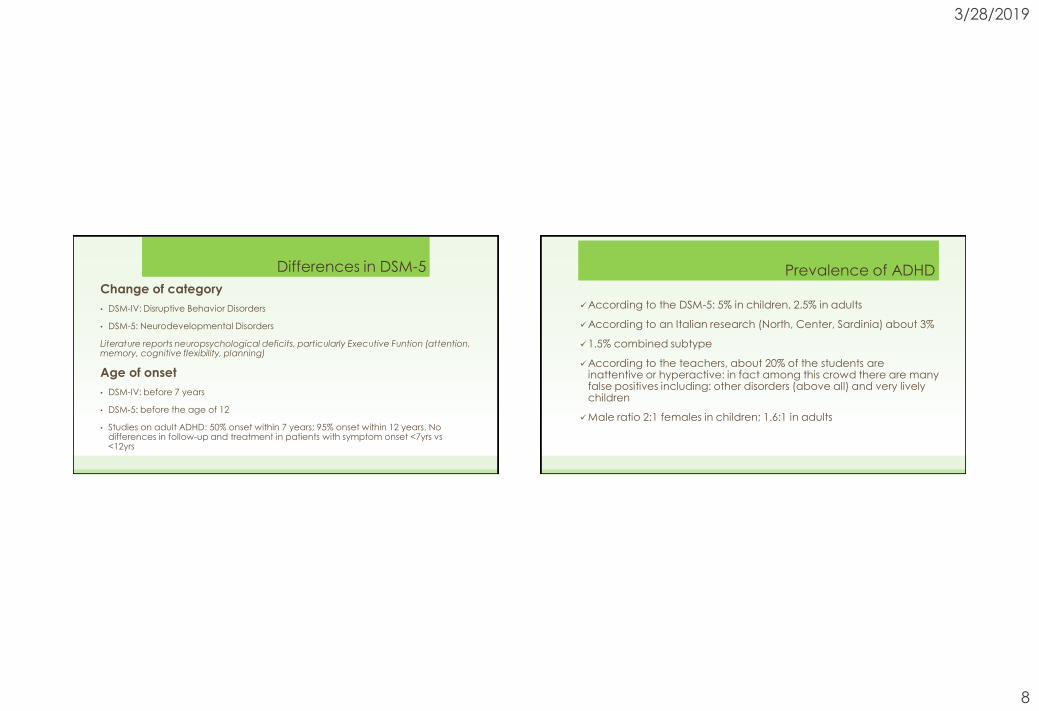
Differences in DSM-5
Change of category
• DSM-IV: Disruptive Behavior Disorders
• DSM-5: Neurodevelopmental Disorders
Literature reports neuropsychological deficits, particularly Executive Funtion (attention, memory, cognitive flexibility, planning)
Age of onset
• DSM-IV: before 7 years
• DSM-5: before the age of 12
• Studies on adult ADHD: 50% onset within 7 years; 95% onset within 12 years. No differences in follow-up and treatment in patients with symptom onset <7yrs vs <12yrs
Prevalence of ADHD
According to the DSM-5: 5% in children, 2.5% in adults
According to an Italian research (North, Center, Sardinia) about 3%
1.5% combined subtype
According to the teachers, about 20% of the students are inattentive or hyperactive: in fact among this crowd there are many false positives including: other disorders (above all) and very lively children
Male ratio 2:1 females in children; 1.6:1 in adults

3/28/2019
9
Epidemiology of ADHDDevelopment of ADHD
In preschool, hyperactivity is more evident (difficult to distinguish from liveliness)
Most of the first assessment requests occur when children are 8 - 10 years old
In the preadolescence the clinical presentation changes according to the factors of improvement or aggravation
In adolescence and adulthood
30% - 40% good remission of symptoms
60% - 70% remains the disorder
About half of them have co-morbidities with Externalized (Conduct) or Internalized disorders (Anxiety or Depression)

3/28/2019
10
Causes or expression of symptoms
Distinguish the causes (determinants of the disease) from the expression of symptoms (severity and duration)
The causes of ADHD are biological (genetic or not genetic)
The expression of symptoms also depends on parental education (more or less regulated), the family environment (more or less structured and predictable), the school environment (more or less supportive)
Brain structures involved in ADHD

3/28/2019
11
3 circuits of ADHD (Sonuga-Barke et al, 2010) A TRIPLE PATHWAYHYPOTHESIS
CORTICO-DORSAL
STRIATAL
LOOP
DISTURBANCE
INHIBITORY
DEFICITS
EXECUTIVE
DEFICITS
CORTICO-VENTRAL
STRIATAL
LOOP
DISTURBANCE
IMPAIRED
SIGNAL DELAYED
REWARD
DELAY AVERSION
ADHD
CORTICO-
CEREBELLAR
LOOP
DISTURBANCE
TEMPORO-
SENSORY-MOTOR
INTEGRATI’N
DEFICITS
MOTOR
ASYNCHRONY
SIMPLIFIED FUNCTIONAL
NEUROANATOMY
DLPFC
DORSAL
STRIATUM
Caudate
Nucleus
THALAMUS
MOTOR
CORTICES
NEO
CEREBELLUM
VENTRAL
STRIATUM
Nucleus
Accumbens
OFC
AMYGDALA
ANTERIOR
CINGULATE
3/28/2019
12
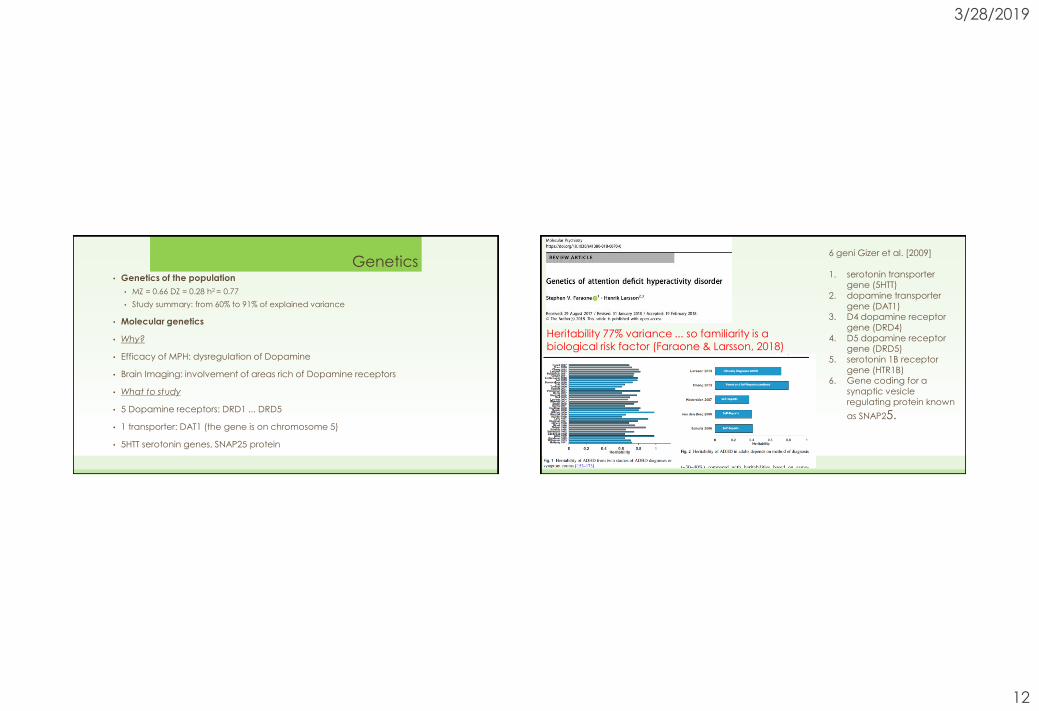
Genetics• Genetics of the population
• MZ = 0.66 DZ = 0.28 h2 = 0.77
• Study summary: from 60% to 91% of explained variance
• Molecular genetics
• Why?
• Efficacy of MPH: dysregulation of Dopamine
• Brain Imaging: involvement of areas rich of Dopamine receptors
• What to study
• 5 Dopamine receptors: DRD1 ... DRD5
• 1 transporter: DAT1 (the gene is on chromosome 5)
• 5HTT serotonin genes, SNAP25 protein
Heritability 77% variance ... so familiarity is a biological risk factor (Faraone & Larsson, 2018)
6 geni Gizer et al. [2009]
1. serotonin transportergene (5HTT)
2. dopamine transportergene (DAT1)
3. D4 dopamine receptorgene (DRD4)
4. D5 dopamine receptorgene (DRD5)
5. serotonin 1B receptorgene (HTR1B)
6. Gene coding for a
synaptic vesicleregulating protein known
as SNAP25.

3/28/2019
13
• 12 independent genome-wide significant loci associated with ADHD in a GWAS meta-analysis of 55,374 individuals
• FOXP2 and other biologically informative genes…..
• The results also highlight strong overlap with the
genetics of ADHD-related traits and health risk behaviors in the population, encouraging a dimensional view of ADHD as the extreme end of a continuum of symptoms
Risk factors of ADHD
biological
environment
Individual traits
Parent traits: education, imitation, genetics

3/28/2019
14
Mercury,
Manganese
• Maternal smoking OR =
1.60 Smoking mothers 60% more likely to have ADHD
child
• 75% if they smoke more than 10 cigarettes
• 54% with less than 10
cigarettes• Interactive effect with
socio-environmental
variables or parents' personalities?

3/28/2019
15
American Journal of Psychiatry,
2003
Consumption of alcohol during pregnancy
• Variability of results: 0.88 <OR> 2.5
• Some studies do not distinguish the amount of alcohol taken
• Consumption of alcohol is associated with family psychopathology (deviance, depression) and disadvantaged socio-economic status
• The direct effect between alcohol consumption and ADHD is weak
• Contradictory results, more research is needed
Interaction gene x environment: COMT x Anxiety mother
• Maternal anxiety predicts ADHD from 4 to 15 years (9% variance explained)
• The child's genotype and maternal anxiety interact to decrease WM performance and increase
ADHD symptoms

3/28/2019
16
• The Apgar index <9 is predictive of ADHD (22% of ADHD have this risk factor)
• Birth after term is the second perinatal risk factor for predicting ADHD
From pregnancy to 18 months
• Initial sample of over 100,000 pregnant mothers
• Interviewees at 6 and 18 months of age of the child (66% of the initial sample completed the study) on child development (language, cognition, motor skills), breastfeeding, sleep, crying, temperament, sleep
• 2034 children with ADHD selected from national registers (8-12 years)
• Retrospective analysis of interviews with mothers when their children were 6 and 18 months old to reconstruct the early risk factors of ADHD

3/28/2019
17
Risk factors in ADHD childrenRetrospective analysis at 6-18 months
0
0,5
1
1,5
2
2,5
3
3,5
30min pianto giorno allattamento seno 6
mesi
ritardo linguaggio seduta a 8 mesi cammino a 11 mesi no afferrare oggetti su
richiesta
iperattivo ipoattivo bambino difficile
6 mesi 18 mesi
From risk factors, to neuropsychology and finally to symptoms
• Comparison between 251 ADHD vs 213 non-ADHD (multi-step clinical diagnosis)
• Relationship between risk factors, neuropsychological processes, ADHD symptoms
• Risk factors: pre-natal exposure, health in pregnancy, peri-natal problems
• Neuropsychological processes: Inhibition, Active working memory, Memory span, Processing speed, Response variability, Arousal, Time processing
• Analysis of the direct influence of risk factors on ADHD symptoms
• Analysis of the indirect influence of risk factors on neuropsychological processes and in turn on ADHD symptoms

3/28/2019
18
Prenatal exposure-NPS-ADHD

3/28/2019
19
Pregnancy – NPS –ADHD
Inattention Hyperactivity
Perinatal – NPS - ADHD

3/28/2019
20
Mediation model for explaining ADHD
• Partialling out age, gender, ethnicity, family income, psychopathology of parents: pre-natal exposure does not directly predict ADHD
• Exposure to substances in pre-natal times influences memory span and temporal processing, which indirectly influence inattentiveness
• The health of the pregnant mother directly influences the ADHD symptoms, even after covariates
• Difficulties in the peri-natal phase affect the neuropsychological processes of response variability and temporal processing and indirectly ADHD symptoms

3/28/2019
21
Temperament, Executive Function, ADHD
2) Response set – Nepsy-2
Touch the yellow if you hear red
Touch red if you hear yellow
Touch blue if you hear blue
Executive Function (6 years)
1) Working Memory – WISC-IV
Temperament
Questionnaire (3-4 years)
Children Behavior
Questionnaire (parents)
94 questions on 3
macrodimensions:
1. Positive affectivity
2. Negative affectivity
3. Self-regulation
Temperament Assessment
Battery (Teachers)
29 questions on 4
dimensions
1. Inhibition
2. Activity level
3. Negative emotion
4. Persistence on the task
7 years: syntoms of ADHD usingK-SADS interview to parents
Attention: visual search
Interaction Temperament and Executive Function
Working memory is a more effective mediator than inhibition and flexibility processes
Managing
frustration and anger at 3-4 years
Executive Functions 6-year
ADHD symptoms at 7 years

3/28/2019
22
Delay aversion
M & Ms under the cup
Record every 5 '' if the
child resists the
temptation to take
candy (max 45 '')
Inhibiton Attention
K-CPT: length 7.5’, press a key
every 1-3sec, all blue
balls(10% of stimuli)
• Omissions
• Commissions
• RT

3/28/2019
23
ADHD risk factors and mediation models
• To define a model of pre-school Executive Function
• To identify the relationship between biological and environmental risk factors, related to the individual characteristics of the child and parents and the preschool ADHD traits
• To study the role of mediation of executive function between risk factors and preschool ADHD symptoms
With Nicoletta Scionti, Ylenia De Palma, Sara Bossi, Giulia LuziParticipants
• 5 Kindergartens in the Province of Milan, about 250 children with typical development
• 72% acceptance: 179 children balanced by gender and age rated by their parents and teachers

3/28/2019
24
Procedure
• Children were presented with a battery for the
assessment of cognitive functioning
• Parents and teachers filled a questionnaire on
developmental steps and behavior at present
MaterialBattery to assess Cognitive Function
• The game of color and form (FE-PS)
• Day / Night (FE-PS)
• Continuous Performance Test (Corkum et al., 1995; Mahone et al., 2001)
• Truck Loading (Carlson et al., 2004)
• Statue (NEPSY-II)
• Digit span (WISC-IV)
• Progressive Colored Matrices by Raven (Giofré & Belacchi, 2015)
• The gift (Sonuga-Barke et al., 1992; 2003)
3/28/2019
25
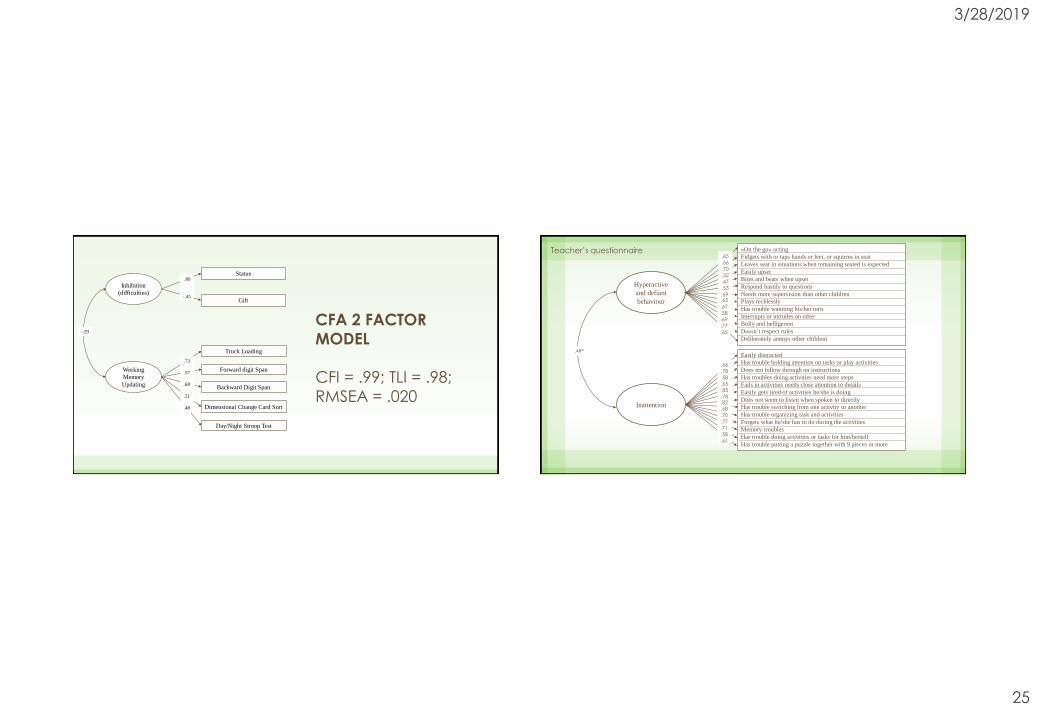
Statue
Dimensional Change Card Sort
Gift
Truck Loading
Day/Night Stroop Test
Forward digit Span
Backward Digit Span
Inhibition
(difficulties)
Working
Memory
Updating
.80
-.45
.73
.57
.68
.51
.48
-.29
CFA 2 FACTOR
MODEL
CFI = .99; TLI = .98;
RMSEA = .020
Hyperactive
and defiant
behaviour
Inattention
«On the go» acting
Fidgets with or taps hands or feet, or squirms in seat
Leaves seat in situations when remaining seated is expected
Easily upset
Bites and beats when upset
Respond hastily to questions
Needs more supervision than other children
Plays recklessly
Has trouble wainting his/her turn
Interrupts or intrudes on other
Bully and belligerent
Doesn’t respect rules
Deliberately annoys other children
Easily distracted
Has trouble holding attention on tasks or play activities
Does not follow through on instructions
Has troubles doing activities need more steps
Fails in activities needs close attention to details
Easily gets tired of activities he/she is doing
Does not seem to listen when spoken to directly
Has trouble switching from one activity to another
Has trouble organizing task and activities
Forgets what he/she has to do during the activities
Memory troubles
Has trouble doing activities or tasks for him/herself
Has trouble putting a puzzle together with 9 pieces or more
.65
.66
.70
.32
.47
.53
.66
.78
.58
.65
.85
.78
.82
.68
.70
.77
.71
.58
.61
.69.65
.67
.58
.69
.77
.65
.48*
Teacher’s questionnaire
3/28/2019
26
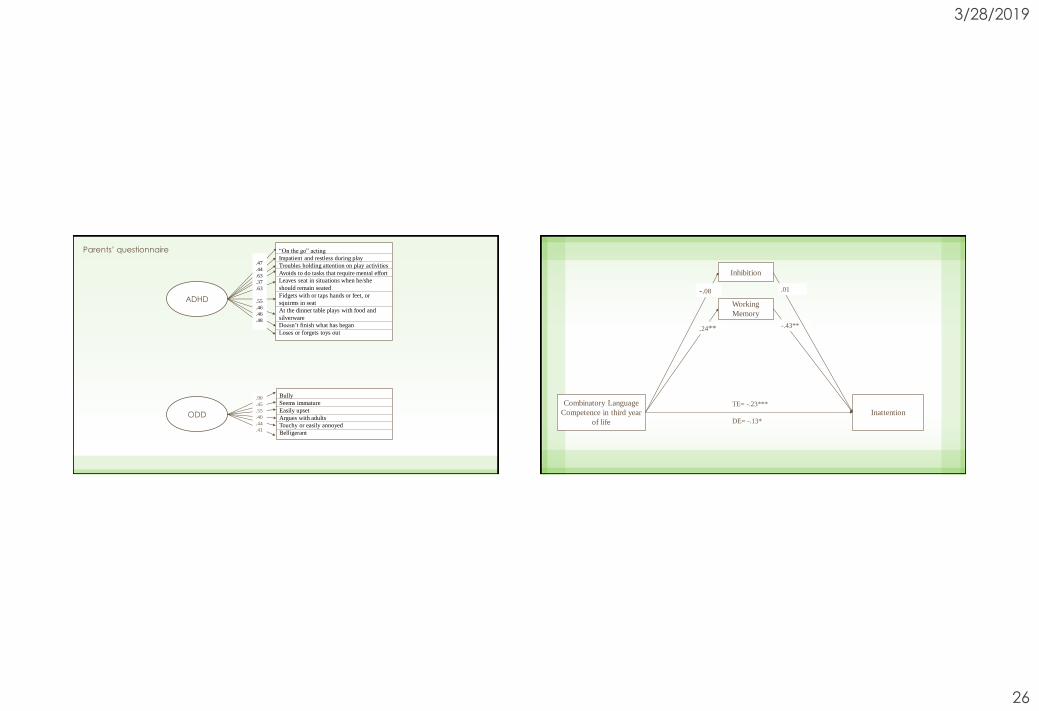
ADHD
ODD
.90
.45
.55
.40
.44
.41
“On the go” acting
Impatient and restless during play
Troubles holding attention on play activities
Avoids to do tasks that require mental effort
Leaves seat in situations when he/she
should remain seated
Fidgets with or taps hands or feet, or
squirms in seat
At the dinner table plays with food and
silverware
Doesn’t finish what has began
Loses or forgets toys out
Bully
Seems immature
Easily upset
Argues with adults
Touchy or easily annoyed
Belligerant
.47
.44
.63
.37
.63
.55
.46
.46
.48
Parents’ questionnaire
Combinatory Language
Competence in third year
of life
Inattention
Inhibition
TE= -.23***
DE= -.13*
-.43**
-.08
.24**
.01
Working
Memory

3/28/2019
27
Combinatory Language
Competence in third year
of life
Hyperactivity
Defiance
Inhibition
Working
Memory
TE= -.19**
DE= -.11
.24** -.25**
-.08 .13
Gross-motor skills
competence in the first
year of life
Hyperactivity and
Defiance
Inhibition
TE = -.15*
DE= -.09
Working
Memory
-.16*
.14
-.27**
.12

3/28/2019
28
How to carry out an assessment for ADHD
The diagnosis of ADHD is clinical: the clinician decides whether or not the child has the disorder on the basis of the data collected
At least 7-10 hours of assessment is needed to outline a complete picture including:
Free or structured interviews with parents and teachers
questionnaires for parents and teachers
cognitive tests to the child (Cognitive Level, Learning, Attention, Executive Functions)
observations (during task when the child applies strategies)
interview with the child (to observe the behavior, the attitude and the awareness of the problem)
Questionnaires
• CBCL – Child Behavior Checklist (Achenbach, 2001)
• Conners Rating Scale: Parents, Teachers, Child (Short – Long) (Conners, 2007)
• Brown ADD Scale: 3-7 years for parents and teachers, 8-12 years for parents, teachers and self-report, adolescents

3/28/2019
29

3/28/2019
30
https://www.youtube.com/watch?v=-eGpC8VuwII
Treatments for ADHD
Patient
Parents
Teachers
Cognitive-behavioral therapyDrug therapyCounseling
CounselingBehavioral interventions
Parent training
Counseling
Psycho-educational training

3/28/2019
31
Goal of psychological treatments
Parent training
• reduction of behavioral and emotional problems at home
• improvement of the parent-child relationship
• Behavior modification in the classroom
• reduction of behavioral and emotional problems at school
• improvement of teacher-child relationship
• Cognitive-behavioral therapy (CBT) with the child
• reduction of behavioral and emotional problems
• improvement of social and academic skills
Multimodal Treatment for ADHD - MTA
• Pharmacological therapy (Med)
• Psycho-educational therapy: Parent Training, TeacherTraining, Cognitive-behavioral therapy for children(Beh)
• Combined therapy: drug + psycho-educational therapy (Comb)
• Community therapy: Basic pediatrician (CC)

3/28/2019
32
Composite measure(Conners et al.(2001), JAACAP, 40, 159-167)
Combined Therapy is more efficacious
Normalization rates for different types of therapy
25
34
56
68
0
10
20
30
40
50
60
70
80
Percentuale
Pediatrician
(63% drug)Drug CombinedBehavioral
Therapy

3/28/2019
33
It is important to know that
• Children of the combined therapy received 20% less drug
• 63% of children of the control group were treated using drugs
• Parents in the drug therapy group received unstructured training (booklets)
• Combined therapy and psychological therapy produce the same results for: social skills, parent-child relationships, relationships with peers. For these aspects, the effectiveness was due to psychological therapy, not to medication.
3/28/2019
34
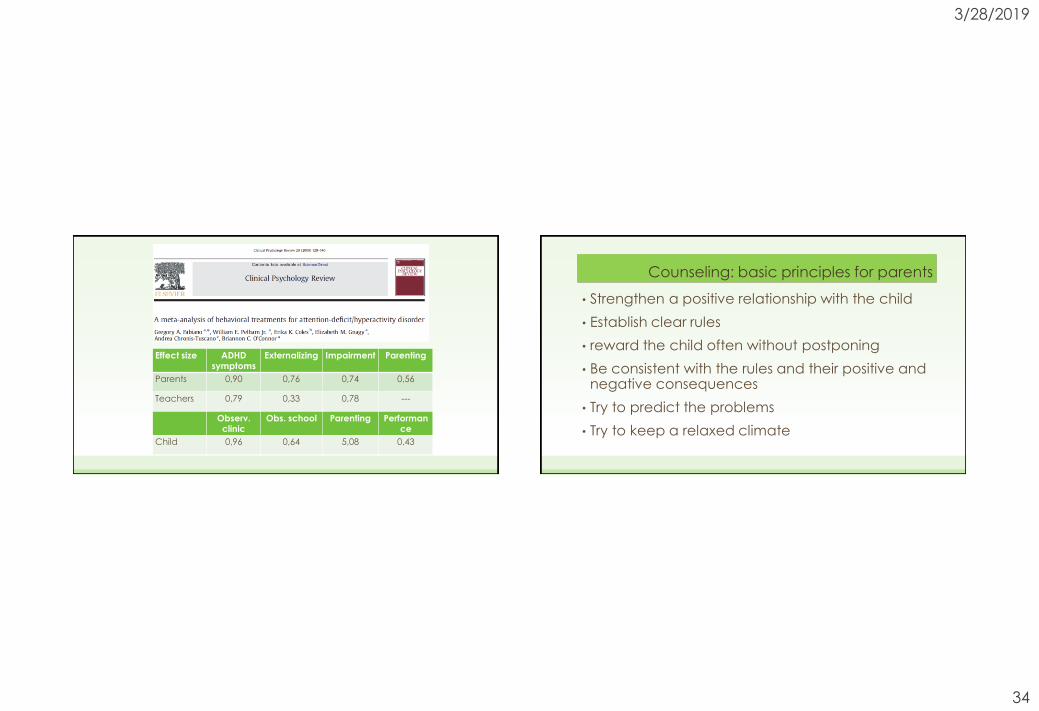
Effect size ADHD symptoms
Externalizing Impairment Parenting
Parents 0,90 0,76 0,74 0,56
Teachers 0,79 0,33 0,78 ---
Observ.clinic
Obs. school Parenting Performance
Child 0,96 0,64 5,08 0,43
Counseling: basic principles for parents
• Strengthen a positive relationship with the child
• Establish clear rules
• reward the child often without postponing
• Be consistent with the rules and their positive and negative consequences
• Try to predict the problems
• Try to keep a relaxed climate

3/28/2019
35
PARENT TRAINING is the most effective non-pharmacological intervention for
self-regulation disordersTraining for parents aiming to help them to understandwhat is happening in their family, facilitating realisticattributions about their behavior and about their child,increasing their skills in the management of dysfunctionalbehaviors
Parent training
3/28/2019
36
The first one is informative on the characteristics ofthe ADHD child on the basis of information obtainedfrom the literature
The second one is the analysis of negative andpositive thoughts about him/herself as parent andabout their child
The third one is an application of behavioralstrategies to solve problem at home
Three main ingredients Parent training - method
• Semi-structured training 8-10 sessions lasting for 90-120 minutes every 2 weeks
• Small group of parents (8-12 parents in couple)
• Discussion about important facts of the last 2 weeks
• Presentation of a strategy
• Analysis of thoughts and beliefs, observation, reward, response cost, time-out, fading, prompting, planning and routines, prolem solving
• Discussion about the possible application at home
• Homework
• Problem solving at home

3/28/2019
37
What should I think…
• Many of his disturbing behaviors are not intentional
• it does not matter to find the responsibilities, the solutions are more important
• it's not just my fault that he behaves like that
• I can not let him do what he wants
• I have to start teaching him how to behave, taking into account that it will take more time, patience ... and a counseling
Some positive behaviors• The commands must be short, simple and specific
• you need to pay close attention to positive behaviors
• gratification must be given in a broad way and immediately after the child's action
• we must ignore the slightly negative behaviors
• we must not lose control of the boy
• it is necessary to be a model and a support to solve problems
• one must be consistent in gratifications and behavioral contracts
• it is important to establish and enforce the rules of behavior: few, understandable and accepted

3/28/2019
38
Strengths and Difficulties• Strengths
• he's good at sports
• is ready in speed games
• It is intuitive
• he is sociable
• he is affectionate
• cares for family members
• participate in group activities
• it is generous
• he invented
• Difficulties
• he is distracted
• interrupts others
• it is disobedient
• it is never "never" calm
• it's hurried
• it is disorganized
• disturbs the companions
• does not respect the rules
• does not perform the tasks
• it is inconstant
Routines at home• Timetable and sleep rhythm
• Feeding hours
• Care of your person
• Homework
• Own material management
• Return times
• Behavior in public
• Table behavior
3/28/2019
39
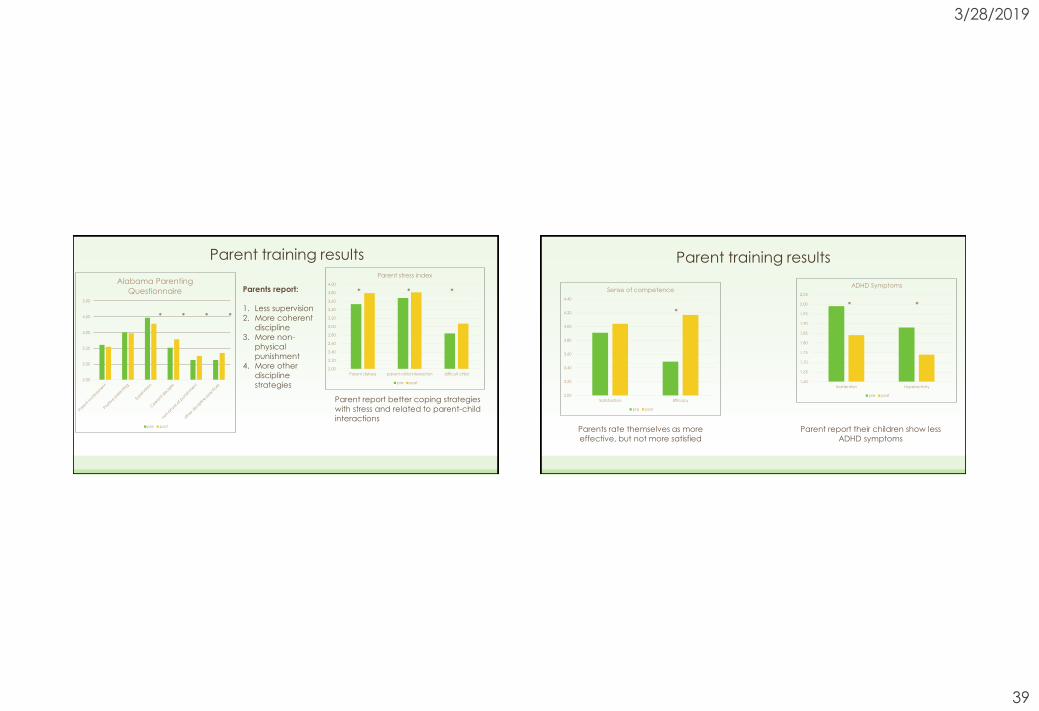
Parent training results
2,50
3,00
3,50
4,00
4,50
5,00
Alabama Parenting
Questionnaire
pre post
* * * *
Parent report better coping strategies
with stress and related to parent-child
interactions
2,00
2,20
2,40
2,60
2,80
3,00
3,20
3,40
3,60
3,80
4,00
Parent distress parent-child interaction difficult child
Parent stress index
pre post
* * *Parents report:
1. Less supervision
2. More coherent
discipline
3. More non-
physical
punishment
4. More other
discipline
strategies
Parent training results
3,00
3,20
3,40
3,60
3,80
4,00
4,20
4,40
Satisfaction Efficacy
Sense of competence
pre post
*
Parents rate themselves as more
effective, but not more satisfied
1,60
1,65
1,70
1,75
1,80
1,85
1,90
1,95
2,00
2,05
Inattention Hyperactivity
ADHD Symptoms
pre post
* *
Parent report their children show less
ADHD symptoms

3/28/2019
40
Mediation of the Parent training effectSonuga-Barke et al 2002
• Maternal ADHD reduces the positive effect of PT
• The major severity ADHD symptoms is a negative predictive index
• The coexistence of other problems (CBCL) is a positive predictive index
• Prevent the development of secondary problems
• Reduce parental stress
• Preventing some negative development trajectories
Why a PT for preschoolers?

3/28/2019
41
Efficacy of PT for preschoolers
Mean Effect Size of ADHD
symptoms reduction is 0,61
(medium effect)
• The Parent Training and the related material must bemediated by words and concrete examples drawnfrom the stories of the parents themselves
• the parents should be helped to analyze theproblems of the child and to seek the solution
• it is necessary to favor mutual help between parents,so that a problem solved in a positive way canexercise in others the curiosity and the research of thereasons that have pushed towards the solution
Some important notes…
3/28/2019
42
TEACHER TRAINING
It is necessary to take into account:
The teacher's interpretations on problematic behaviors
The school needs (quantity of students, diversity and problems, teachers available)
The pupil's needs (cognitive profile, specific behavioral difficulties, family or social problems)
The systematic consultancy is structured in 3 phases:
1. Observation
2. Reflections on space, time and attention
3. Behavioral strategies
A starting point…
• some hyperactive students in the classroom ... .climate of poor behavioral control
• «Infect» other students ... a sense of impotence in teachers
• students who are not content "pull more and more the rope" to look for limits, boundaries, motivations to behave better
• juxtaposition of dissatisfied: students who provoke without goals, teachers who can not manage them ...
• Stress, a sense of powerlessness, lack of shared objectives ...

3/28/2019
43
A breaking point
• Isolate and define specific behaviors that create chaos and tension in the classroom (occasional observations are needed)
• Link provocative behaviors and advantages for pupils, links that are invisible to teachers (functional ABC observations are needed)
• Define simple, clear and shared rules (contrary to negative behaviors and which become common objectives)
• Agree a goal and explain how to achieve it ... respecting the rules and positive behaviors
Looking for a meaning
• Why should hyperactive pupils respect the rules?
• What are the motivations of the pupils to improve their behavior? ... .. is it more fun to provoke and break the rules?
• We need more motivation and find meaning in positive behavior
• Almost everyone must be convinced of the advantage and the consequences of compliance with the rules
• A collective award, pleasant to make everyone feel more competent is already a good reason!

3/28/2019
44
Steps of the project
1. Observation in the classroom
2. Occasional, Functional, Systematic
3. Sharing with teachers of classroom observations and definition of behavioral goals
4. Panel realization: rules, contract, points system, puzzle with final prize
5. Talking with students to share rules, positive behaviors and create a mutual respect
I keep silence during the lesson During the lesson I am sitting still

3/28/2019
45
To intervene I raise my hand
Contract and the tokens

3/28/2019
46
Teacher gives tokens for the final prize
Don’t raise hand– Don’t wait
0
10
20
30
40
50
60
70
80
90
Baseline Token 1 Token 2 Token 3 Token 4 Token 5 Token 6 Token 7 Token 8
Non alzare la mano Alzare la mano ma non aspettare
3/28/2019
47
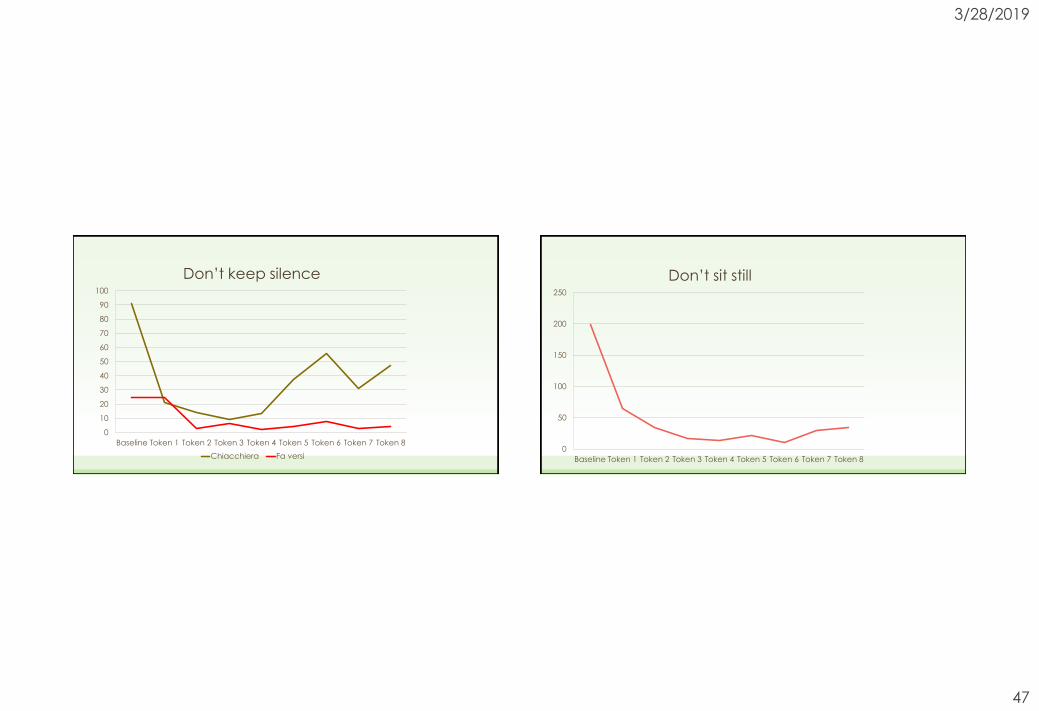
Don’t keep silence
0
10
20
30
40
50
60
70
80
90
100
Baseline Token 1 Token 2 Token 3 Token 4 Token 5 Token 6 Token 7 Token 8
Chiacchiera Fa versi
Don’t sit still
0
50
100
150
200
250
Baseline Token 1 Token 2 Token 3 Token 4 Token 5 Token 6 Token 7 Token 8

3/28/2019
48
Raise hand
0
20
40
60
80
100
120
140
160
Positive behavior
Intervention at school for disruptive behavior
• The intervention does not focus on a single child (with ADHD or ODD) but
• It involves all pupils of the classroom
• A baseline observation is necessary: to understand the classroom, the start a project in collaboration with the children, to assess possiblechanges
• Positive behaviors could be augmented and the climate of the classroom could improve
• The final goal is to set an higher well-being at school
• For disruptive children in this context it is easier to respect the rules

3/28/2019
49
The work with the child
• It can be useful to work with the child on attention
• Need to get used to working in an organized, reflective, continuous, systematic way
• It should be gratified, supported to generalize the reflective and careful style
• He needs to improve awareness before and after the performance of activities and exercises
The work with the child
• The problem of generalization of results
• adults must be supportive models and educators
• The child and the adolescent fear judgment and deny the difficulties
• Denial of problems is contrary to emotional awareness
• Two ingredients: exercises on attention and functions + metacognition to generalize the results
• We can discuss training for children during Executive Function section

3/28/2019
50
Which therapy?
Drug therapy can be useful:
• in children with severe ADHD symptoms
• if there are no educational resources (family and school) to apply a psychological therapy
• if a crystallized situation needs to be unlocked
Psychological therapy is necessary if:
• there are social / relational problems
• it is noted that educators are motivated to "change"
• there is a long-term intervention