
Which Blunt Trauma Patients Should Be Studied by...
32
MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology & Maryland Shock-Trauma University of Maryland School of Medicine Which Blunt Trauma Patients Should Which Blunt Trauma Patients Should Be Studied by Abdominal CT? Hemodynamic stability maintained Unreliable clinical assessment Positive abdominal exam without overt signs (rebound, rigidity) Positive DPL or sonogram (FAST) Suspect retroperitoneal injury Unknown source of blood loss
-
Upload
duongduong -
Category
Documents
-
view
216 -
download
0
Transcript of Which Blunt Trauma Patients Should Be Studied by...

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
MDCT of Bowel and Mesenteric Injury: How Findings Influence Management
MDCT of Bowel and Mesenteric Injury: How Findings Influence Management
4th Nordic Trauma Radiology Course 20064th Nordic Trauma Radiology Course 2006
Stuart E. Mirvis, M.D., FACR
Department of Radiology & Maryland Shock-Trauma
University of Maryland School of Medicine
Which Blunt Trauma Patients Should Be Studied by Abdominal CT?
Which Blunt Trauma Patients Should Be Studied by Abdominal CT?
Hemodynamic stability maintainedUnreliable clinical assessmentPositive abdominal exam without overt signs (rebound, rigidity)Positive DPL or sonogram (FAST)Suspect retroperitoneal injuryUnknown source of blood loss

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
OverviewOverviewBMI < 0.5% admissions to traumaBMI 3-5% of patients having laparotomy for blunt traumaClinical signs present < 50% initiallyDPL variable results for BMI (sensitivity 69%)Sonography - 52% sensitiveNon-operative management of solid organ injuries requires high accuracy for BMI
Role of CT Is ControversialRole of CT Is Controversial
Many literature studies, mainly surgical,cite low sensitivity and high reader dependence (mainly ’80’s, early ’90s)More recent studies using helical and MDCT indicate consistently higher CT accuracy75% of respondents to AAST survey use CT most or all of the time for possible BMIStill actively debated (EAST) 13% perforated SB injuries missed by CT#
#Fakhry SM, Watts DD, Luchette FA. J Trauma 2003;54:295-306

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Sharma et al. The role of computed tomography in diagnosis of blunt intestinal and mesenteric trauma (BIMT). J Emerg Med. 2004
Jul;27(1):55-67.
CT of bowel and mesenteric injury
1995 to 2002: 36 cases of BM injury16 isolated and 20 non-isolated injuries Initial CT scan was abnormal in 74% (17 out of 23), and 83% on retrospect (2 additional cases) CT scans were abnormal (initial and repeat) in 96% (22 out of 23). Free fluid (78%), mesenteric stranding or edema (39%), bowel wall hematoma, or edema (30%). Free air 31%, oral contrast extravasation 15%
Allen TL, et al. Computed tomographic scanning without oral contrast solution for blunt bowel and mesenteric injuries in abdominal trauma.
J Trauma. 2004 Feb;56(2):314-22.
Oral vs. no oral contrast
N= 20 patients (500 blunt trauma reviewed)Sensitivity and specificity of CT imaging for the detection of BBMIs were 95.0% and 99.6% CT imaging of the abdomen without oral contrast for detection of BBMIs compares favorably with CT imaging using oral contrast.? Confidence level

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
MDCT Technique (16-slice)MDCT Technique (16-slice)0.75 or 1.5mm X 16mm slice thicknessPitch 1.25Oral contrast (add rectal for penetrating injury)IV contrast 120-150ml (350 mg/ml)Intravenous contrast @ 6 ml/sec X 15 sec., then 4/sec. X 15 sec. (skull base to pubis)3-5 mm reconstructions for PACSUse 1mm reconstructed images for reference and MPR, 3D, volumetric studies
Diagnostic (operative) CT Signs of Full-thickness Bowel Injury
Bowel contrast extravasationPneumoperitoneum, intramural, intramesenteric air without known or alternative source (20% sensitive)Direct visualization of tear in wall (rare)
MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
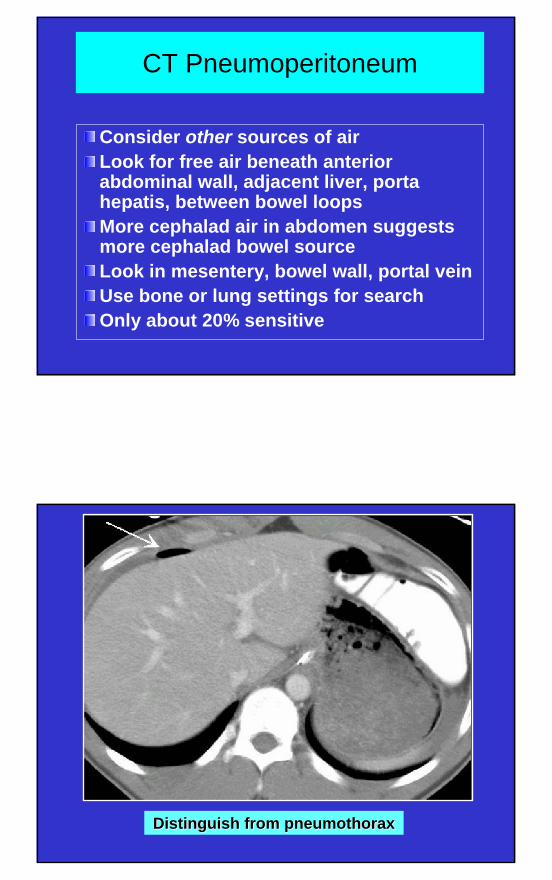
CT Pneumoperitoneum
Consider other sources of airLook for free air beneath anterior abdominal wall, adjacent liver, portahepatis, between bowel loopsMore cephalad air in abdomen suggests more cephalad bowel sourceLook in mesentery, bowel wall, portal veinUse bone or lung settings for searchOnly about 20% sensitive
Distinguish fromDistinguish from pneumothoraxpneumothorax

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Pneumoperitoneum: windows & levels for bone or lung
Pneumoperitoneum: windows & levels for bone or lung
Jenunal Perforation
Blunt TraumaJenunal Perforation
Blunt Trauma

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Was DPL performed?Was DPL performed?Was DPL performed?
Jejunum: Blunt full-thickness injury
Jejunum: Blunt full-thickness injury

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Subtle free air: Colon rupture
Subtle free air: Colon rupture
Duodenal ruptureDuodenal ruptureDuodenal rupture

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Direct rupture of duodenum; free air
& hematoma
Direct rupture of duodenum; free air
& hematoma
Colon rupture: Intramural air, free air
Colon rupture: Intramural Colon rupture: Intramural air, free airair, free air

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Intramural duodenal air delayed duodenal
hematoma – 4d
Intramural duodenal air delayed duodenal
hematoma – 4d
Oral contrast leakOral contrast leak
Requires oral contrastSpills into low resistance peritoneal spaceActive bleeding usually dissects into mesentery and has surrounding hematomaExtravasated urine from intraperitoneal bladder rupture can confuse diagnosis (delayed imaging)

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Oral contrast spillage:
OR jejunal perforationOral contrast spillage:
OR jejunal perforation
Fecal spillage right colon &
Lumbar Hernia

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Indirect Signs of Bowel Injury: Indirect Signs of Bowel Injury:
Bowel wall thickening (subjective)Adjacent mesenteric infiltration or hematoma Dilated, fluid-filled loops - atonicIncreased wall contrast enhancementFree fluid of ? source
Bowel Wall Thickening
Normal bowel 1-2 mm partially distended; 3-4 mm when collapsed Seen in proximal small bowel most commonly5-6 mm mild thickening, 7-8mm moderate, >8 mm markedContusion localized thickening involving adjacent loops (prox. jejunum)No other findings equals contusionBowel wall hematoma can co-exist

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Bowel contusion & free fluid:
Full-thickness bowel injury
Bowel contusion & free fluid:
Full-thickness bowel injury

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Bowel Contusion
Jejunal perforation at OR

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Horse kicks broom into abdomen !
Duodenal transection –direct diagnosis
Delayed colonic hematoma;
Pt. on anticoagulants
Delayed colonic hematoma;
Pt. on anticoagulants

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Bowel Wall EnhancementBowel Wall Enhancement
Patchy increased density in bowel with thickened wallOften seen with mesenteric edemaMechanism: slowed perfusion, leaky capillaries, re-perfusion phenomenonMandates careful follow-up
Thick-walled enhancing bowel
Thick-walled enhancing bowel

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Enhancing small bowel wall
Enhancing small bowel wall
Intraperitoneal FluidIntraperitoneal Fluid
Always measure fluid densityTrace amount occasionally seen in cul-de-sac of women of child-bearing yearsMay be the only sign of injury to bowel/mesentery or solid organ (20%+)Larger amounts of fluid in more locations increases chance of injuryMesenteric triangles (bowel – mesenteric origin likely)

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Pelvic Fluid: MalePelvic Fluid: MalePelvic Fluid: Male
CT of Mesenteric InjuryCT of Mesenteric Injury
Active bleedingHematoma Infiltration (misty, hazy)Triangle sign of intramesenteric fluidFascial thickeningDifficult to distinguish operative from non-operative lesions

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Mild mesenteric contusion (misty- hazy)
Mild mesenteric contusion Mild mesenteric contusion (misty(misty-- hazy)hazy)
Mesenteric hematoma:
renal infarctMesenteric Mesenteric hematomahematoma::
renal infarctrenal infarct

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Colonic contusion with mesenteric tear -hematomaColonic contusion with mesenteric tear -hematoma
Active mesenteric bleed-delayed diffusion
Active mesenteric bleed-delayed diffusion
MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
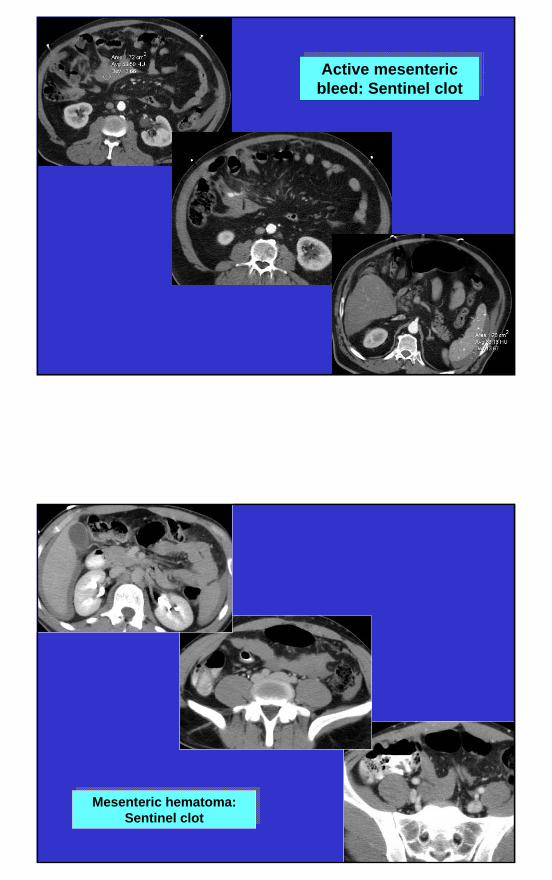
Active mesenteric bleed: Sentinel clotActive mesenteric
bleed: Sentinel clot
Mesenteric hematoma: Sentinel clot
Mesenteric hematoma: Sentinel clot

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Active Mesenteric Bleed
Delayed
Active bleeding mesenteric hematoma;
Tear at root of mesentery
Active bleeding mesenteric hematoma;
Tear at root of mesentery

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Active mesenteric bleed
Enveloping Mesenteric Hematoma
Enveloping Mesenteric Hematoma

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Intramural gastric hematoma
Management for Indirect CT Findings
Serial physical examination* F/U CT 6-8 hoursFollow-up sonography (same examiner)Diagnostic peritoneal lavage (WBC, bile)Exploration

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
MVC: Abdominal Pain- initial CT
Follow-up CT – 10 hr.
Jejunal rupture in OR

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Mimics & Masks of Bowel InjuryMimics & Masks of Bowel Injury
Shock bowel: follows prolonged hypotension or cardiac arrests
Diffuse bowel wall thickeningPatchy increased enhancementDilated, fluid-filled bowelSmall bowel mainly involvedMesenteric edema commonUsually flat IVC, renal veinsMay see increased renal and adrenal enhancement, decreased spleen density

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Shock BowelShock Bowel
Shock BowelShock Bowel

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Shock Bowel: Small bowel & colonShock Bowel: Small bowel & colonShock Bowel: Small bowel & colon
Shock bowelShock bowelShock bowel

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Shock BowelShock Bowel
Mimics & Masks of Bowel InjuryMimics & Masks of Bowel Injury
Increased venous return pressureOver resuscitation, cardiac tamponade, tension pneumothorax, hematoma compressing IVCDistended IVC and renal veinsDiffuse edematous small bowel and mesenteryOften retroperitoneal, pericholecysticedema and peritoneal fluidRarely involves colon

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Pericardial
TamponadePericardial
Tamponade
Increased CVP
Periportallymphedema
Increased CVP
Periportallymphedema

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Increased CVP
Small bowel edema
Increased CVP
Small bowel edema
Summary
• What are the CT findings of bowel and mesenteric injury?
• Which of those findings indicates need for surgical intervention? observation? anxiety?
• What are the major concurrent trauma findings that mimic or mask signs of bowel and mesenteric injury?

MDCT Bowel & Mesenteric Injury
SE Mirvis, MD: ASER 2005
Thank You


















