Where are the men? SiilStrategies to involve men ifill iin ... · Where are the men? SiilStrategies...
59
Where are the men? S i i l S trateg i es to i nvo l ve i f il l i men i n f am il yp l ann i n g Grace Shih, MD MAS University of California‐ San Francisco Sarah Miller MD MPH Sarah Miller , MD MPH Institute for Family Health/AECOM‐ New York City
Transcript of Where are the men? SiilStrategies to involve men ifill iin ... · Where are the men? SiilStrategies...
Where are the men? S i i lStrategies to involve
i f il l imen in family planningGrace Shih, MD MASUniversity of California‐ San FranciscoSarah Miller MD MPHSarah Miller, MD MPHInstitute for Family Health/AECOM‐ New York City
DisclosuresDisclosures• We have no relationships to discloseWe have no relationships to disclose
• We are both vasectomy providers and trainerstrainers
ObjectivesObjectives• Discuss contraceptives currently availableDiscuss contraceptives currently available to men
• List and address barriers to men seeking• List and address barriers to men seeking reproductive care
Di k i i f• Discuss marketing strategies for men
• Describe strategies for counseling men and couples about family planning

BackgroundBackground• Traditional model –> family planningTraditional model > family planning focused on women• 2002 NSFG only 48% of men received• 2002 NSFG, only 48% of men received sexual/repro health services in past year
• <20% of males 15 19y counseled about• <20% of males 15‐19y counseled about birth control or STIs
Kalmuss, Perspect Sex Reprod Health 2007MacKellar, J Acquir Immune Defic Syndr 2005

BackgroundBackground• What happens if men are included in familyWhat happens if men are included in family planning?• Improved contraceptive practice• Improved contraceptive practice
• Reduced pregnancy ratesd lf d l• Decreased self‐reported sexual pressure
• Support for partner in contraceptive decisions
Danielson, Fam Plann Perspect 1990; Wang, Am J Public Health 1998; Becker, Contraception 2008
What contraceptive options areWhat contraceptive options are currently available for men?
• Vasectomy
C d• Condoms
• Abstinence• Withdrawal
• Natural family planningNatural family planning
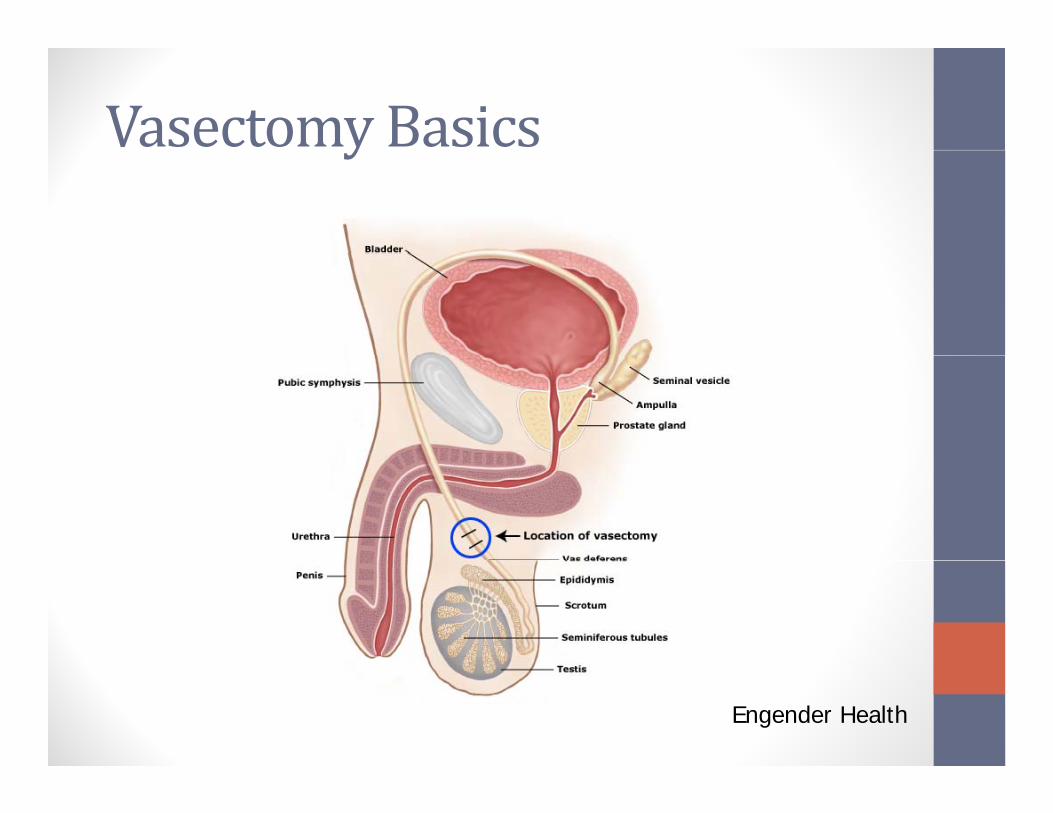
Vasectomy Basics y
Engender Health
Basic Vasectomy StepsBasic Vasectomy Steps
• Isolate the vas• Isolate the vas•Access the vas
• “No scalpel” vs. Incisional
•Disrupt the vas

Di tiDisruptingthe Vas
Ligation +/- Excision Ligation and Fascial Int
t e Vas
Ligation +/- Excision Ligation and Fascial Int
Open test end
Testicular end
C t d E i iCautery and Excision
Cautery and Fascial InterpostionAAFP 2006
DemoDemo• No Needle, No Scalpel, Open Ended Vasectomy
Vasectomy Effects (T/F)Vasectomy Effects (T/F) • Vasectomy decreases sexual experienceVasectomy decreases sexual experience
• Vasectomy increases risk of prostate cancercancer
• Sperm buildup can cause testicular rupture
• A man can have sex days after his vasectomy
Myth: Vasectomy decreases y ysexual experience• Men maintain erections and produce semen
• No perceptible difference in ejaculate (semen)No perceptible difference in ejaculate (semen)
• Sperm accounts for 2‐5% ejaculate
T l l h d• Testosterone levels unchanged
• Same sensations and function
Richards, Urology 1981; McDonald, Clin Anat 1996
Myth: Vasectomy decreases y ysexual experience• No change in interest in sex• No difference in ability to reach orgasmNo difference in ability to reach orgasm
• No (new) problems with erection
N h i l l• No change in sexual pleasure
Smith, J Sex Med 2010; Hofmeyr, J Sex Marital Ther 2002

Myth: Vasectomy causes y yprostate cancer
• “Vasectomy increases risk of prostate cancer and the apparent lack ofcancer and…the apparent lack of confounding or bias…suggest that the association may be causal ”association may be causal.
Giovannucci E. JAMA 1993
Myth: Vasectomy causes y yprostate cancerT k iti• Two keys critiques‐ Reliance on self or spousal report for predictor and outcome
‐ Detection bias
‐ Similar frequency of digital rectal exams in vasectomized and non‐exams in vasectomized and nonvasectomized men
Myth: Vasectomy causes y yprostate cancer
• “No change in current practice of vasectomy nor should vasectomy reversalvasectomy nor should vasectomy reversal be done as a prostate cancer prevention measure ”measure.
National Institute of Health 1993National Institute of Health 1993
Myth: Sperm buildup and y p ptesticular rupture• Sperm production continues
• Sperm is reabsorbedSperm is reabsorbed
• Can cause sperm granuloma
2 3 k• 2‐3 weeks post‐vasectomy
• Up to 60% men; symptomatic in 3‐5%• Treatment ‐ NSAIDs
Schwingl, Fertil Steril 2000

Potential methodsPotential methods• RISUG (Vasalgel)RISUG (Vasalgel)
• Ultrasoundh l ill• Nonhormonal pill
• Heat‐based methods
Male Contraceptive Information Project; Tsuruta, Repro Bio Endo 2012
Male involvement in family l i iplanning services
A “man” is‐ Strong
A man is…g
‐ Powerful‐ Dominant‐ Can Take it‐ Tough‐ Protective‐ In Control‐ Proud
In Their Own Right, The Alan Guttmacher Institute 2002
Messages sent tomen• Be self‐reliant
Messages sent to men…
• Conceal weakness
• Health is not a big issue
• Men are invincible• Men are invincible
• Ignorance is bliss
• Virility = manliness
In Their Own Right, The Alan Guttmacher Institute 2002.

Barrier: Lack of effective male contraceptives
• Myth: male reproductive biology is harder• Myth: male reproductive biology is harder to study/control
L k f l i d l• Lack of male contraceptive development‐Socio‐culturalE i‐Economic‐Commercial constraints N bi l i l l i‐Not biological complexity
NICHD 2000

Use of Vasectomy Worldwidey
Female
Male
Vasectomy > Tubal LigationNew Zealand (23%) UK (18%) Bhutan DenmarkNew Zealand (23%), UK (18%), Bhutan, Denmark, Netherlands
Engender Health, 2003
Lowuse of vasectomy in USLow use of vasectomy in US• 2006‐2008 NSFG2006 2008 NSFG
• Overall 23% rely on sterilization• Female:male 3:1Female:male 3:1
• Homogenous group
Barone, Perspect Sex Reprod Health 2004
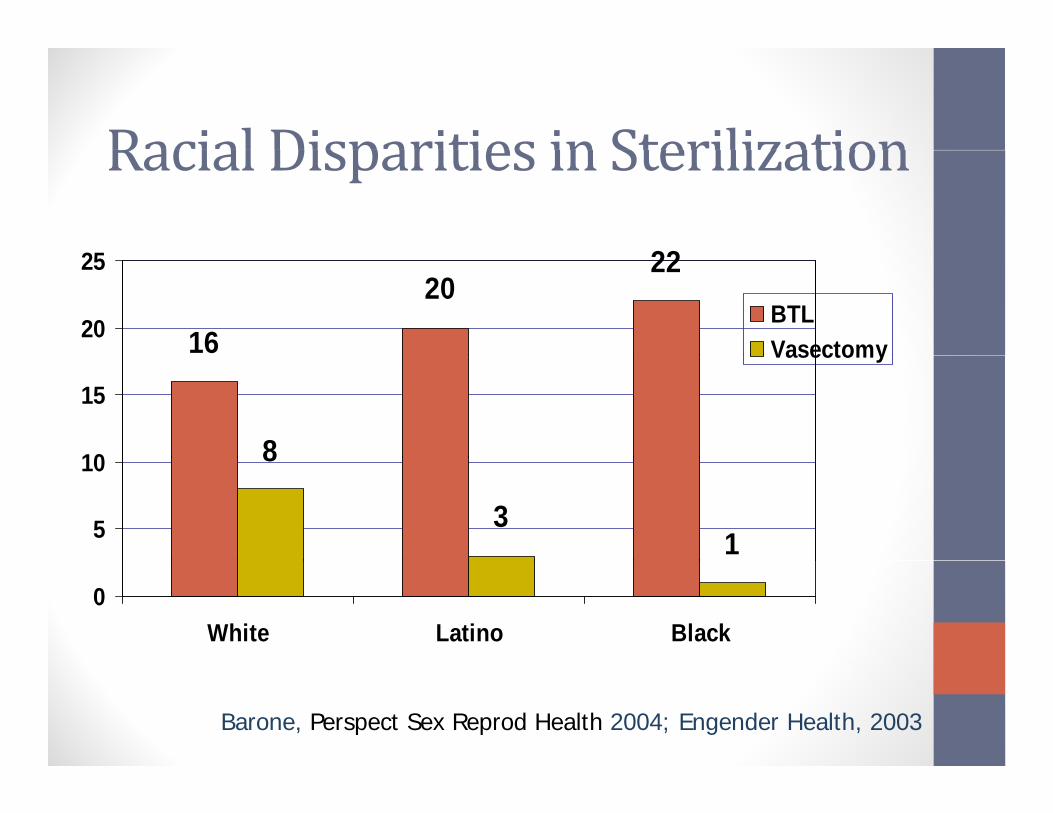
Racial Disparities in SterilizationRacial Disparities in Sterilization2225
16
2220
20
25
BTLVasectomy
810
15
Vasectomy
13
8
5
10
0White Latino Black
Barone, Perspect Sex Reprod Health 2004; Engender Health, 2003
Brainstorm: Barriers to male involvement
•Cultural•SystemicSystemic
•Individual
Barriers: SystemicBarriers: Systemic• Clinic EnvironmentClinic Environment
• Images with women‐focused posters, magazine tv programs handoutsmagazine, tv programs, handouts
• Lack of marketing to men
L k f l f d h lth d ti• Lack of male‐focused health education
• Staff and provider resistance• Lack of knowledge/training
• Access to healthcare in generalg
Barriers: IndividualBarriers: Individual• FearFear
• Of healthcare, in generalOf d ti l l t• Of procedures, particularly vasectomy
• Of public perception/judgment
• Comfort with provider
• Knowledge g• Pregnancy risks and outcomes
Brainstorm: Add i B iAddressing Barriers
Adapt the clinic environmentAdapt the clinic environment• Make men feel more welcome in your clinicy
• Visual Messaging‐ include “male identity”
• Literature men’s magazines• Literature – men’s magazines
• Staff– receptionists, clinicians…

Providing services tomenProviding services to men
• Make it clear that you are providing careMake it clear that you are providing care for him, not just seeing him as a partner to a female patienta female patient.

TrainingTrainingFor staffFor staff
• Training, educationC “ ”• Create “team”
• Involve other team members in counseling
For healthcare providers
• Didactics modeling practice• Didactics, modeling, practice

Communication and CultureWhen choosing a health care provider,
Communication and Cultureg p
men value expertise and communication style over gender.

Marketing family planningMarketing family planning tomento men

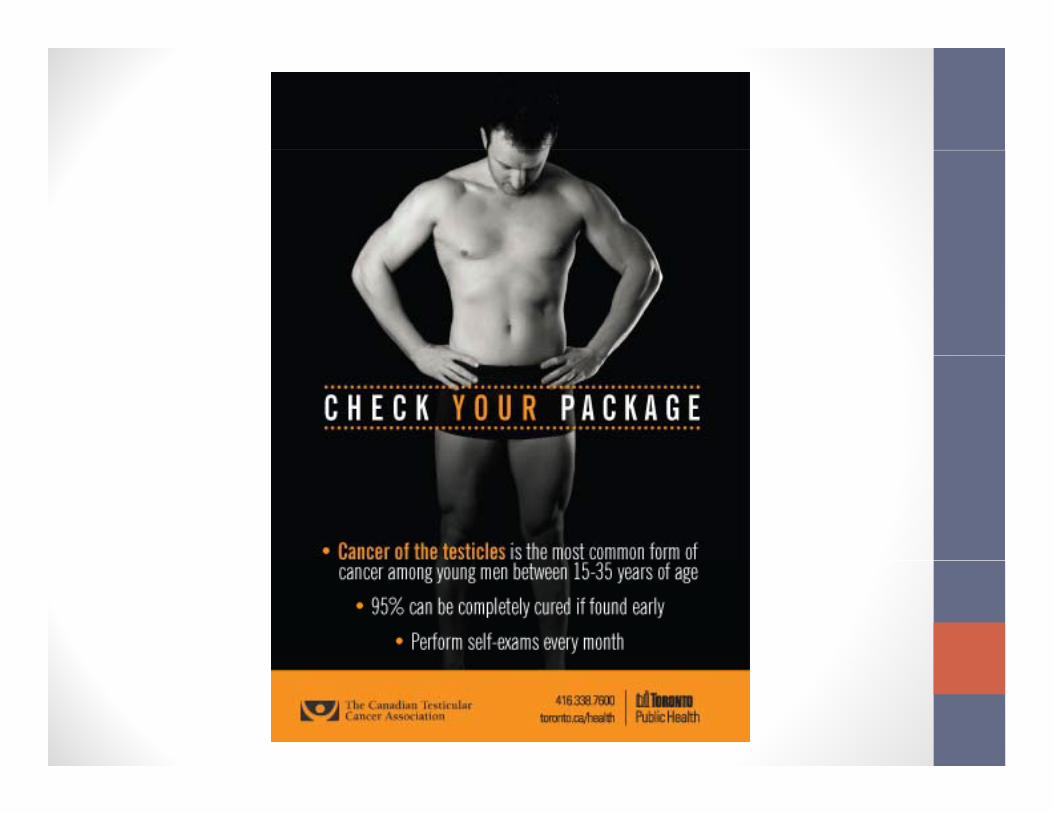

Marketing TipsMarketing Tips• Give positive images of menGive positive images of men
• Emphasize “action”
l i l• Focus on one clear, simple message
• Use humor
• Privacy is important

Counseling men
Women are the Gatekeepers to Men’s Health• Use all opportunities to discuss men’s health P t l i t• Promote male services to women• “Attention Ladies: Medical Services now available for men”available for men
• “Get your man tested…his health is your health”your health
Don’tmiss opportunitiesDon t miss opportunities
•One Key Questions initiative•One Key Questions initiative• TALK to your patients (MALE and female) about their reproductive plans

Why counselmen?Why counsel men?
Of 6 illi i llOf >6 million pregnancies annually
Unintended

CounselingMenCounseling Men• Model‐ Disease preventionModel Disease prevention
Women and Men: Similarity yand Differences
Common experienceCommon experienceFemaleexperience
Maleexperience

“Sexperts”Sexperts
• Social expectation is for men to “knowSocial expectation is for men to know everything” about sex
• Not knowing may cause anxiety• Not knowing may cause anxiety
• May be reluctant to ask questions
CounselingMenCounseling Men• What do you do in your practice?y y p

Sample questionsSample questions• What do you or your partner(s) do for y y p ( )birth control?
• How do you protect yourself from STDs d ?and HIV?
• How are you about using condoms?h k h d b h h• Who makes the decision about whether to
use a condom?• What questions do you have about your• What questions do you have about your own health?
Communication and Culture
‐ Create a confidential space
‐ Protect their “shame”
‐ Allow them to lead‐ Allow them to lead
‐ Provide “action” oriented lplans
‐Talk about physical feelings or thoughts before emotions
Communication and Culture
‐ Wait. Let them talk, address other ,concerns first
‐ Wait for the right time When theWait for the right time. When the opportunity arises to discuss reproductive health take ithealth, take it.
Normalize and ValidateNormalize and Validate
“A lot of guys ask that same question….”
“It’s often difficult for people, especially men to talk about such personal issuesmen, to talk about such personal issues when they first come to the clinic.”

CounselingMenCounseling Men

CounselingMenCounseling Men• Don’t make assumptionsDon t make assumptions
k d d i• Ask open‐ended questions
• Tailor sessions to address patient’s concerns
• Provide easy access to information
CounselingMenCounseling Men• Use common comfortable languageUse common, comfortable language
lk l• Talk less
• Take a neutral stance
• Accept your limited role
Closing thoughts
I t ti ’ ibilit ?
Closing thoughts
• Is contraception a woman’s responsibility?
• Does society encourage female over male sterilization?
• Does there have to be a “reason” for a couple to choose male over female sterilization?
• What is our job?
What you can doWhat you can do• Advocate for male servicesd ocate o a e se ces
• Change cultural norms ‐ familyChange cultural norms family planning = women AND men
• We as providers need to change if we want better outcomes for our patients

Special ThanksSpecial Thanks• Marsha Gelt, MPH – Cardea ServicesMarsha Gelt, MPH Cardea Services