What works: a realist evaluation case study of intermediaries in infection control practice
12
ORIGINAL RESEARCH What works: a realist evaluation case study of intermediaries in infection control practice Lynne Williams, Christopher Burton & Jo Rycroft-Malone Accepted for publication 2 June 2012 Correspondence to L. Williams: e-mail: [email protected] Lynne Williams MSc RN Lecturer in Adult Nursing Centre for Health Related Research, School of Healthcare Sciences, Bangor University, UK Christopher Burton BN RGN DPhil Senior Research Fellow in Evidence Based Practice School of Healthcare Sciences, Bangor University, UK Jo Rycroft-Malone MSc PhD Professor of Health Services and Implementation Research University Director of Research, School of Healthcare Sciences, Bangor University, UK WILLIAMS L., BURTON C. & RYCROFT-MALONE J. (2012) What works: a realist evaluation case study of intermediaries in infection control practice. Journal of Advanced Nursing 00(0), 000–000. doi: 10.1111/j.1365-2648.2012. 06084.x. Abstract Aim. To report a study of an intermediary programme in infection control practice in one hospital in the UK. Background. Promoting best evidence in everyday practice is a constant problem in infection control. Intermediaries can influence the transfer and use of evidence in health care, but there remains a lack of evidence and theory about the specific actions and change processes, which can be successful in improving infection control practices. Design. An in-depth mixed methods case study. Methods. The study was undertaken in 2011. Participants were recruited through purposive sampling and included frontline staff, managers and nurses in intermediary roles in infection control. Results. For frontline staff, intermediary presence triggered a modification in behaviour. Different reactions were noted from the intermediaries’ high level of physical presence in clinical areas, the facilitative approaches they used to give feedback and the specific teaching strategies they employed to meet frontline staff needs. The specific intermediary actions uncovered in this study were contingent on the prevailing systems for performance management, organisational commitment and efforts in clinical areas to foster a collegiate environment. Conclusions. The study provides theoretical threads of how intermediaries can be successful in promoting evidence use under certain contextual conditions. Further testing of the specific intermediary mechanisms uncovered in this study will contribute to understanding different approaches that work in infection control in embedding evidence in practice. Keywords: case study, evidence-based practice, infection control, intermediary, nursing, realist evaluation © 2012 Blackwell Publishing Ltd 1 JAN JOURNAL OF ADVANCED NURSING
-
Upload
lynne-williams -
Category
Documents
-
view
215 -
download
0
Transcript of What works: a realist evaluation case study of intermediaries in infection control practice

ORIGINAL RESEARCH
What works: a realist evaluation case study of intermediaries
in infection control practice
Lynne Williams, Christopher Burton & Jo Rycroft-Malone
Accepted for publication 2 June 2012
Correspondence to L. Williams:
e-mail: [email protected]
Lynne Williams MSc RN
Lecturer in Adult Nursing
Centre for Health Related Research, School
of Healthcare Sciences, Bangor University,
UK
Christopher Burton BN RGN DPhil
Senior Research Fellow in Evidence Based
Practice
School of Healthcare Sciences, Bangor
University, UK
Jo Rycroft-Malone MSc PhD
Professor of Health Services and
Implementation Research
University Director of Research, School of
Healthcare Sciences, Bangor University, UK
WILL IAMS L . , BURTON C . & RYCROFT -MALONE J . ( 2 0 1 2 ) What works:
a realist evaluation case study of intermediaries in infection control practice.
Journal of Advanced Nursing 00(0), 000–000. doi: 10.1111/j.1365-2648.2012.
06084.x.
AbstractAim. To report a study of an intermediary programme in infection control
practice in one hospital in the UK.
Background. Promoting best evidence in everyday practice is a constant problem
in infection control. Intermediaries can influence the transfer and use of evidence
in health care, but there remains a lack of evidence and theory about the specific
actions and change processes, which can be successful in improving infection
control practices.
Design. An in-depth mixed methods case study.
Methods. The study was undertaken in 2011. Participants were recruited through
purposive sampling and included frontline staff, managers and nurses in
intermediary roles in infection control.
Results. For frontline staff, intermediary presence triggered a modification in
behaviour. Different reactions were noted from the intermediaries’ high level of
physical presence in clinical areas, the facilitative approaches they used to give
feedback and the specific teaching strategies they employed to meet frontline staff
needs. The specific intermediary actions uncovered in this study were contingent
on the prevailing systems for performance management, organisational
commitment and efforts in clinical areas to foster a collegiate environment.
Conclusions. The study provides theoretical threads of how intermediaries can be
successful in promoting evidence use under certain contextual conditions. Further
testing of the specific intermediary mechanisms uncovered in this study will
contribute to understanding different approaches that work in infection control in
embedding evidence in practice.
Keywords: case study, evidence-based practice, infection control, intermediary,
nursing, realist evaluation
© 2012 Blackwell Publishing Ltd 1
JAN JOURNAL OF ADVANCED NURSING

Introduction
Across the globe, priority is given to reducing rates of
healthcare-associated infections (HCAIs), ‘the most frequent
harmful event in health-care delivery’ (World Health Orga-
nization 2011a). Although policy directives and innovative
ways of working have led to improvements in recent years,
infection rates are still unacceptable. According to the
World Health Organization (2011b:22), ‘of every 100 hos-
pitalized patients at any given time, 7 and 10 of them will
acquire a HCAI in developed and developing countries,
respectively’. The implications for patients, both physical
and psychological, can be severe and the problems they
present greatly influence the public’s perception of the qual-
ity of healthcare services.
Policy intentions are clear: governments promote a zero
tolerance approach to HCAIs (Welsh Government 2011)
and the duty of all healthcare providers is to protect
patients from their risks (Infection Control Nurses Associ-
ation 2004). Current UK policy directs individuals to
assume responsibility and contribute towards prevention of
HCAIs (Welsh Assembly Government 2004). However,
despite important investment in infection control policy
and education programmes, understanding how this invest-
ment has influenced individual clinician behaviour change
in infection control practice is a complex phenomenon
(Wilcox 2009).
Background
Drawing on social influence theory, behaviour change is con-
sidered to be more likely to occur when individuals are influ-
enced by others, either individuals or groups (Rashotte
2007). This has led to an exploration of the potential impact
of ‘intermediaries’ (Ferguson et al. 2004, Thompson et al.
2006), a range of individuals who influence the transfer and
use of evidence (Milner et al. 2006). In the literature, certain
individuals are classed as intermediaries through their work
as linking agents, facilitators, change agents, champions and
opinion leaders (Ferguson et al. 2004, Thompson et al.
2006). The champion, for example, is perceived as an indi-
vidual having specialist knowledge, recognizing a need for
change, promoting a new idea with enthusiasm and determi-
nation and demonstrating passion for a project (Thompson
et al. 2006). However, although the evidence-based move-
ment has embraced the promise of different intermediaries
with their potential to promote knowledge transfer at the
edge of practice (Hoong Sin 2008), not enough is known
about what they do and how their skills may be used most
effectively.
In infection control, better understanding of how inter-
mediaries operate and what their unique contribution may
be to eradicating HCAIs is required (Gardam et al. 2009).
To date, few studies have explored the potential impact of
intermediaries. Lewis and Edwards (2008) reported on one
initiative in a UK healthcare organization. Clinical manag-
ers were identified as ‘champions’ during a period when
local levels of MRSA bacteriaemia were found to be unusu-
ally high. The initiative was found to contribute to a reduc-
tion in infection rates, improved staff confidence in their
own practice and anecdotal feedback found that patients
felt reassured in the presence of clinical champions. How-
ever, the champions were chosen on the basis of their
seniority, contrasting with opinions that determining who
champions are should be guided by their personal traits
rather than their position (Northway & Mawdsley 2007).
Moreover, the subsequent evaluation focused on the cham-
pions’ views of the initiative, rather than exploring the par-
ticular actions they used in their role, how these actions
impacted on the people around them in terms of evidence
use and the potential of the actions to be transferable else-
where.
In the USA, a recent study explored data on types and
numbers of champions operating in infection control in
hospitals (Damschroder et al. 2009). Despite recognition
that contextual factors affected successful implementation
practices to reduce the rates of infections, there was agree-
ment that champions were able to overcome contextual
barriers and enable them to promote evidence-based care.
Although the study offered some guidance, additional
insight into how intermediary actions can influence the pro-
motion of evidence-informed practice would have been
informative. However, the study did highlight how pre-
existing relationships in healthcare systems can affect the
degree of intermediary impact, of significance when efforts
are focused on tailoring intermediary interventions to
particular settings (Damschroder et al. 2009).
To date, few studies have examined the constituents of
successful intermediary actions, or identified their actual
impact in promoting evidence-informed practice. Although
evolving intermediary roles are considered important for
infection control (Dawson 2003, Barry & Carter 2010), lit-
tle guidance is available as to what they do and how they
could operate most effectively.
This present study is an in-depth exploration of an
intermediary programme in a specific setting. The inten-
tion was to generate theoretical explanations about how
specific change processes by both intermediaries and the
programme more generally were used and to highlight
how these could be transferred to other locations to
2 © 2012 Blackwell Publishing Ltd
L. Williams et al.

improve the promotion of evidence-informed infection
control practice.
Methodology
To enable an in-depth exploration of the intermediary pro-
gramme, realist evaluation was chosen as the overarching
framework, now an established approach to health services
research (Sullivan et al. 2002, Byng et al. 2005, Tolson
et al. 2007, Rycroft-Malone et al. 2008, 2010, Greenhalgh
et al. 2009). The growing popularity of realist evaluation is
in its potential to tease out transferable lessons from inter-
ventions (i.e. intermediary programmes operating in infec-
tion control) embedded in social systems (i.e. clinical areas/
wards). Tilley (2000) explains that the purpose of realist
evaluations is to give ‘context-mechanism-outcome configu-
rations’ (CMOCs), which will explain what works for
whom and in which circumstances (Pawson 2006), so that
the framework is explanatory in nature.
Teasing out the ‘mechanisms’ in any evaluation process is
not easy. For this study, mechanisms are considered to be
the cognitive and behavioural impacts of resources embed-
ded in the intermediary programme and are described as
the ‘causal pathway’ through which the impacts of pro-
grammes are realized (Marchal et al. 2010). Mechanisms
are not interventions or activities, they are what make an
intervention or activity work, its underlying mechanism of
action. Context may be interpreted as any space or place
where human interaction takes place, described as ‘appro-
priate social and cultural conditions’ (Pawson & Tilley
1997:57). Stakeholder involvement took place from the
early stages of the study to guide literature reviewing and
early hypotheses development.
Theoretical framework
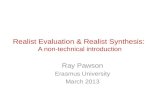
A framework was drawn up for the case study driven by
the realist methodology (Figure 1). Key concepts were
defined through an earlier scoping of the literature and
stakeholder discussions. As a focus of the research was the
programme’s ability to ensure the use of evidence in infec-
tion-control practice, the context section of the framework
was guided by the work of Greenhalgh et al. (2004) which
was useful for its interpretations of context for diffusion,
dissemination and sustainability of innovations in health-
care. The theoretical framework was intentionally broad so
that it provided enough guidance to shape the data collec-
tion methods and analysis, but flexible enough to ensure
that new ideas could emerge and refinement of the frame-
work to be undertaken.
The study
Aims
The aim of the study was to explore and explain how an
intermediary programme in infection control practice
worked in one hospital in the UK.
Design
The investigation was a single mixed methods case study
of an infection control intermediary programme operating
in one healthcare organization in the UK. Case study
research is recognized as being particularly useful when
the focus is on seeking answers to ‘why’ and ‘how’ ques-
tions (Yin 1994) and is compatible with realist evaluation
which seeks theoretical propositions about what works, for
whom and in what contexts. Case study has been used
successfully in healthcare studies driven by the principles
of realist evaluation (Marchal et al. 2010, Rycroft-Malone
et al. 2010), both design and methodology are linked by a
recognition of the importance of context (Rycroft-Malone
et al. 2010).
Sample/participants
The site was selected for its specific infection control inter-
mediary programme which included designated intermedi-
ary posts to address challenges in infection control
practice. In addition to intermediaries, purposive sampling
was used to identify others in the organization with profes-
sional or organizational responsibilities in infection control
(Procter et al. 2010). The inclusion criteria were partici-
pants who were employees of the chosen NHS Trust who
would consent to take part in the study, participants with
infection control responsibilities and adults over 18 years
with the capacity to consent. Individuals were recruited
through the local collaborator for the study. Participants
were contacted by invitation letter that included an infor-
mation sheet.
Data collection
Data were collected in 2011 through observation and
focused interviews, using an interview guide based on the
content of the theoretical framework. Unstructured observa-
tions were guided by an observation schedule, underpinned
by Gold’s typology (1969). Spradley’s (1980) dimensions of
observation was useful in guiding the observer as partici-
pant approach, where the focus is mainly on behaviour and
© 2012 Blackwell Publishing Ltd 3
JAN: ORIGINAL RESEARCH Realist evaluation intermediaries infection control

events, but where there is some level of interaction with
participants (Watson et al. 2010). For example, the obser-
vation guide was used to record settings, people, emotions
and accomplishments. Observation periods were planned
around the participants’ work and were all followed up by
individual audio-taped interviews. Observations took
place during participants’ clinical shifts, lasted on average
3–4 hours, with different clinical areas being visited during
each observation period. The observations were useful in
setting the scene for being able to describe the participants’
working environments and patterns. Documentation relat-
ing to the organization and the geographical setting also
provided contextual information and included audit reports,
annual reports, policies, job descriptions, newsletters and
other resources.
Ethical considerations
Research Ethics Committee approval was sought and
granted by the University Research Ethics Committee, NHS
Research Ethics Committee and access to site granted by
the local R&D Committee.
Data analysis
The approach to analysis was informed by the study’s theo-
retical framework and the analysis approach proposed by
Miles and Huberman (1994). An initial list of codes was
drawn up based on the theoretical framework. Codes were
assigned to the interview and observation data as individual
units and then compared and merged across the case. A
Context
+
Mechanisms
OUTCOMES
Intermediary
Actions
Activities
Behaviors
Outer SocialPerceptions
Attitudes
Behaviors
Environmental Political Drivers
Media
Inner
Organization Control
Strategic Direction
Management Systems
Leadership
Resource Allocation
Infrastructure
Degree of change Empowerment Levels of knowledge Patient safety
Figure 1 Theoretical framework (guided by Greenhalgh et al. 2004).
4 © 2012 Blackwell Publishing Ltd
L. Williams et al.

revised set of codes was formed through familiarizing with
the data and patterns of categories were derived. The codes
were mapped to the main categories and were then analysed
in more depth to formulate a set of sub-categories (Miles &
Huberman 1994). Although some initial codes were impor-
tant, the revised coding framework included those which
were emerging through scrutinizing the data sets. From this,
patterns could be located to match to the descriptive frame-
work. Patterns of themes were derived, based on the main
categories of context, mechanisms and outcomes. The cate-
gories were then fed into a thematic clustered matrix. This
approach is useful when analysis is attempting to shift away
from roles (i.e. what people are called or do) as was the case
in this study, which was more concerned with the mecha-
nisms of action of intermediaries (Miles & Huberman
1994). This was followed by an iterative process of identify-
ing potential mechanisms, contextual factors and outcomes
between LW, JRM, CB (Miles & Huberman 1994). The
process then moved to clarifying links between different
context, mechanisms and outcome threads and refining this
process repeatedly, to form a final range of inferred (or con-
jectured) context-mechanism-outcome configurations.
Rigour
The quality of the case study was attended to, through con-
sideration to four tests (Yin 1994). To address construct
validity, multiple data collection methods were used and the
case site report was sent back to the site to ensure accuracy.
The data analysis process was overseen by two experienced
researchers to ensure internal validity. External validity was
attended to through applying the study results to broader the-
ory. Reliability was addressed through the use of a research
protocol and keeping an audit trail throughout the process.
Results
The findings are reported as conjectured context, mecha-
nisms and outcomes configurations (Table 2) and are sup-
ported by verbatim quotations from interviews. The aim is to
give an overall initial description of what worked, for whom
and how, commencing with a description of the study site.
The site
The case study site was one Hospital in the UK belonging to
a group of Hospitals forming an NHS Foundation Trust.
Trust objectives were driven through having the status of a
public benefit corporation. The Trust’s vision and key priori-
ties indicated its commitment to reducing the risk of HCAIs,
visible through different strategies to promote patient safety,
such as walkabouts by Board Directors and collaboration
with patient groups, governors and members of the Founda-
tion Trust. Monitoring systems for governance requirements
and feedback reporting mechanisms through the independent
regulator of health and social care services for England
were noted. The Trust had also invested in an intermediary
programme to promote evidence-based infection control
Table 1 Participant recruitment and data
collection methods.Manager
(n = 1)
Matron
(n = 1)
Clinical nurse
specialist (n = 1)
Intermediary
(n = 4)
Healthcare
support
worker
(n = 1)
Staff nurse
(n = 1)
Interview
(approx
1 hour)
Interview
(approx
1 hour)
Interview
(approx
1 hour)
Observations
(3–4 hours)
Interviews
(approx
1 hour)
Interview
(approx
1 hour)
Interview
(approx
1 hour)
Documentation review: Audit reports, Annual reports, Policies, Job descriptions, News-
letters and other resources.
Table 2 Conjectured context-mechanism-outcome configurations.
CCMO 1 In clinical areas, high levels of intermediary presence
and being alert to what is happening (surveillance)
leads to monitoring of infection control practice
CCMO 2 In clinical areas, high levels of intermediary presence
and increased attention to intermediary presence leads
to modification of behaviour
CCMO 3 Performance management and tailoring ways of
facilitating feedback lead to people being prompted
to change their practice
CCMO 4 Organizational commitment and increased attention to
intermediary presence enhances the availability of
support for staff
CCMO 5 Organizational commitment and increased attention to
intermediary presence trigger recognition by patients
CCMO 6 A practice-based approach to teaching and making
teaching relevant to local context leads to more
meaningful learning for staff
CCMO 7 Collegiate approaches in clinical areas and building
rapport into relationships enhances the availability of
support for staff
© 2012 Blackwell Publishing Ltd 5
JAN: ORIGINAL RESEARCH Realist evaluation intermediaries infection control

practice. There was evidence of recognition of the investment
that the Trust had made in terms of staffing. In the clinical
area, matrons were observed to be responsible for groups of
wards, beds, waiting lists and capacity with infection control
specified in their job descriptions with ward audits conducted
on a regular basis. The intermediaries were qualified nurses
operating under the direction of the Consultant Nurse for
Infection Control, collaborating with clinical leads and the
infection control team to contribute to the prevention and
control of healthcare-associated infections in one NHS Trust.
The intermediaries had clinical responsibilities, for example,
working alongside staff in clinical areas, maintaining infec-
tion control audits and policy implementation. Other respon-
sibilities included the provision of educational programmes
for staff, liaising and giving advice and administration.
In this case study, the main focus of the analysis centred
on uncovering what the mechanisms were and for whom
were they important. Mechanisms revolved around the
presence of and surveillance by the intermediaries in clinical
areas, ways of giving feedback, increased attention to their
being seen in practice, bringing education into the work-
place and building trust into relationships.
Watching practice
The clinical remit of the intermediaries had led to a high
level of presence in clinical areas:
And because they see us all the time on the ward they sort of just
get used to us being there and it then becomes a lot easier when
challenges need to happen because they don’t feel threatened and
you’re almost part of the team anyway (I4)
In turn, this allowed them to be alert to what was hap-
pening in practice, described by one participant as being
the ‘eyes and the ears’ for infection control and interpreted
here as a mechanism of seeing practice, incorporating the
surveillance of practice:
When we go on, so if we feel that something’s not being done
properly we’ll say to them Well actually if you don’t do this poten-
tially this patient could develop an infection (I4)
Intermediaries were observed seeing practice, enabling
the monitoring of evidence-based infection control practice
in day to day ward routines:
we just want to see…as well how nursing staff are doing things.
For example, we go round and we’ll wash a patient, but the staff
are ‘Oh great, she’s washing the patient’, but we’re seeing how they
dispose of that…bowl of water…are they tipping it down the hand
wash sink (I1)
Attention to infection control (frontline staff)
The clinical remit of the intermediary in clinical areas and
high levels of presence led to increased attention by front-
line staff:
People see you as like a police…policeman or policewoman…They
see you as…here comes infection control and that’s why I actually
said to you this morning, no doubt, somebody’s probably (whis-
pers) Infection control (I1)
In turn, intermediary presence and increased attention to
being seen in practice were observed to trigger modifica-
tions of behaviour by the frontline staff:
because we’re always there to see these things, we’re always there
to see if doctors are coming on, if they’re using the hand gel, if
they are bare below the elbows and nurses, if they’re wearing wrist
watches, they’ve got jewellery on and …so we’re sort of the eyes
and ears on the wards really (I4)
Thoughtful feedback
Organizational systems and processes where performances
in infection control were managed included feedback for
frontline staff. Approaches used by the intermediaries to
give feedback were very carefully chosen to encourage
frontline staff motivation and to promote best practice:
They also have the skills and…and the people skills that they need
to deal with… because they can’t keep coming down heavy
handed, I actually don’t think you get the best from people like
that (M1)
In their interactions with frontline staff, intermediaries
were observed to use facilitative approaches to give feedback:
It’s like I said on the wards before, if you go in guns blazing it gets
their backs up straight away and you won’t get anywhere with
them because they’ll class you as somebody coming in and having
a go at them (I2)
Through observations of intermediary actions, feedback
was observed to be given discreetly and in context:
And to be honest I don’t think anybody likes being challenged. So,
as you saw, I went up and I just whispered to him ‘You need to
take your watch off’, to which he took his watch off straight away.
I think if I’d have said ‘What are you doing with your watch on?’
and I’d had a bit of attitude towards it he’d have automatically put
a barrier up (I4)
In turn, this prompted individuals to consider their prac-
tice and, if required, modify their behaviour:
6 © 2012 Blackwell Publishing Ltd
L. Williams et al.

And if you speak to the doctors they will do it and they’ll say…if
they forget to take to their watch off they’ll say ‘Ever so sorry, I
forgot to take it off’ and they’ll take it straight off and there’s not
a problem (I2)
Availability of support
The organization’s commitment and subsequent high levels
of presence in clinical areas led to availability of support
for frontline staff, especially access to advice about infec-
tion control issues:
It’s not the same as an e-mail and then you have to wait a week, or
until you’re next back on shift or…and then that’s the whole time
then…it could be your next audit due then and nothing’s change and
nothing’s gone further, but to be visibly present there (SN1)
Individual frontline staff decisions to access the interme-
diaries for infection control issues were also noted from a
manager’s perspective:
But I think the…more junior staff in the ward tend to go to (the
intermediary) first, simply because she’s around and they…like I
say, they’ve developed that relationship with her now, where
they’re not…they don’t feel intimidated (M1)
High level of presence and specific approaches chosen by
the intermediaries resulted in observations of frontline staff
valuing a supportive resource:
I find that they’re my…they’re my support network and then they’ll
come and spend time with me and explain anything to me (SN1)
Attention to infection control – patients
Organizational commitment (also reflected in feedback
from patients on infection control procedures and cleanli-
ness) and attention to intermediary presence led to an
enhanced sense of recognition for patients. Intermediaries
were recognized by individual patients through their work
with them:
Now, if you’ve noted we’ve gone onto areas and a few patients
have recognized me and they recognize the other (intermediaries)
that go out (I1)
Being able to identify staff with specific infection control
responsibilities was noted to be important for relatives as well:
if they can see a name badge, whoever they’re talking to, if you
greet them through the door or if you’re sitting at the desk, they’ll
always look at your name badge to know who you are and it’s nice
just to hear them, when they talk to you they say ‘Oh you’re the
… you’re the link nurse that we saw on the ward. Can I just ask
you why my Dad’s got this card? (SN1)
Practice-based teaching
The intermediaries tailored education for frontline staff
through practice-based approaches to teaching. Although
formal teaching through staff mandatory induction or
updating was observed, there was also an effort to bring
education into the workplace through a focus on the rele-
vance to practice and local context:
it’s not always a formal based thing because somebody could ask
you a question and you could quite happily go off on a tangent
from what you’ve gone on there to do and go and…end up doing
something totally different that you hadn’t planned (I3)
Intermediaries were observed to adapt their teaching
strategies to suit frontline staff needs and they recognized
the challenges of addressing education in busy clinical envi-
ronments:
We do educational packages, on the job and…we do…instead of
doing big ‘come and sit down’ packages, as in sort of a proper…
educational session, we do little snapshots on the areas. So we do
teaching packages there. We try and teach things like aseptic tech-
nique (I4)
Bringing education into the workplace resulted in more
meaningful and real learning for frontline staff:
She can show somebody a hundred times how to do and MRSA
swab in the lab with a dummy, but if you…want to show them on
a real life patient, it’s so much easier if you’re there working with
that nurse (M1)
Building rapport
Intermediary actions to build relationships with frontline
staff were facilitated by general efforts to foster a collegiate
environment in clinical areas and were observed to be
focused on building rapport and trust:
you’ve got to build a relationship. It’s no good going into the areas
and being aggressive, being nasty, because you only then build up
this wall. You’ve got to go in and have a rapport with the staff (I1)
Intermediary efforts were focused on being accessible for
frontline staff:
if I’ve got any worries or anything I’ve always got in touch with
(the intermediary) like, you know…I’ve got her page number to
page her if I’ve got a problem (SW1)
© 2012 Blackwell Publishing Ltd 7
JAN: ORIGINAL RESEARCH Realist evaluation intermediaries infection control

Intermediary actions to promote effective relationships
with frontline staff, through building trust and engaging
with them, were noted:
because I was impressed with how she engages with the staff and
how actually…she really feels for them when things go wrong and
really tries hard to put it right and get in there and…you know,
‘Come on, I’ll show you how we do this’ and has really, really…
really got them all working together (M1)
Discussion
The principal aim of the case study was to uncover interme-
diary mechanisms of action to explain what worked to pro-
mote best practice in infection control. Realist evaluation
facilitated the generation of a group of theoretical supposi-
tions of what was working in certain contexts (Table 2).
Visibility
By virtue of intermediary frequency of presence in clinical
areas, visibility triggered a range of reactions from different
individuals. For frontline staff, seeing the intermediaries in
practice had a cognitive impact, reminding them of practic-
ing according to the evidence. However, despite being seen
as an important strategy for infection control teams (Gardam
et al. 2009), little evidence exists as to the impact of the
theory of visibility on quality and effectiveness in infection
control. Findings from this study show that the matron’s
responsibilities for infection control were supported by the
intermediaries. In this case, organizational commitment led
to enhanced visibility, a policy remit of the modern matron
role (Department of Health 2001, Dealey et al. 2007).
Although in the literature the focus is centred on the visibility
of leaders and managers in clinical areas for the promotion
of effective infection control practice (Healthcare Commis-
sion 2007), this study has highlighted the visibility of other
people (in a non-managerial role, with ascribed responsibility
for specific clinical issues) as being important.
Intermediary visibility resulting in recognition for patients
and reassurance for frontline staff reflects the relationship
found elsewhere in other public services, for example, the
significance of the relationship between police visibility and
public reassurance (HM Inspectorate of Constabulary
2002).The findings of this study raise important questions
about how visibility is operationalized in other contexts/
areas of health care, where responsibility for infection con-
trol lies with different structures to those described here.
Conversely, in this study, visibility of practice allowed the
intermediaries to monitor and intervene where required so
that infection control risks were minimized. Surveillance
has long been used as a powerful tool to protect social val-
ues (Dawson et al. 2005). Although behavioural surveil-
lance theory is a concept more likely to be applied in public
health (McQueen 1999), the impact of human surveillance
on behaviours in infection control practice requires further
unpacking.
Practice-based teaching
The frequency of presence of this group of intermediaries
enabled swift identification of frontline staff educational
needs and their skills and abilities to give adaptable models
of education facilitated this approach. Although infection
control education and training for frontline staff were fully
supported by the organization, it emerged that adapting
flexible strategies/approaches were crucial to ensure staff
needs were met and improving their understanding of infec-
tion control issues. Therefore, in addition to mandatory
training programmes and formal means of teaching, clini-
cally based teaching was employed, based in wards and
often focused on the problem frontline staff were concerned
with at the time. Intermediaries were instrumental in facili-
tating this approach and staff preferences for these interac-
tive approaches reflect findings of previous studies
(Wisniewski et al. 2007). These findings reflect the prob-
lem-based focus of andragogy in adult learning theories
(Gilmore 2011). Understanding the impact of different
learning styles for frontline staff in infection control is
important and requires further exploration.
Performance management and feedback
The call to consider the impact of organizational context on
quality of care is not new (Burton et al. 2009). However,
implementation research seeks further exploration of specific
contextual factors which contribute to making evidence use
part of day-to-day practice (Stetler et al. 2009). In this
study, performance management and ways of providing
feedback were found to be instrumental in motivating peo-
ple to change. In contrast to a general learning climate as
part of the context for evidence implementation, high level
of feedback for individuals, teams and systems has already
been recognized as an important element for successful
implementation of evidence-based practice (Rycroft-Malone
2004). Greenhalgh et al. (2004) found that in complex
service innovations, providing feedback as an active imple-
mentation strategy increased the likelihood of success in
establishing evidence use. Using performance feedback in
infection control reflects the findings of Grol and Grimshaw
8 © 2012 Blackwell Publishing Ltd
L. Williams et al.

(2003) who stress that regularity is the key, with withdrawal
of feedback affecting the impact on practice. However, in
this study, it was the manner of performance feedback, facil-
itated by the intermediaries, which appeared to be most
important, warranting additional exploration.
Facilitation
The ‘facilitative’ approach uncovered here reflects, to a
degree, the findings of Harvey et al. (2002:585) who
conclude that a facilitator who ‘provides face to face com-
munication and uses a range of enabling techniques has
some impact on changing clinical and organizational prac-
tice’. The concepts of building trusting relationships and
working in partnership with staff, support the enabling
attributes required of different intermediaries facilitating
evidence in organizations (Milner et al. 2005, Stetler et al.
2006). Furthermore, the potential contribution of the
intermediary in supporting frontline staff promotes effec-
tive team working (Firth-Cozens 2004), a key characteris-
tic of quality care for the infection control arena (Griffiths
et al. 2008).
Context
Organizational commitment for the intermediary pro-
gramme was instrumental in triggering the availability of
support for frontline staff. One organizational feature
recognized for its success in standardizing care based on
the best evidence is the micro system (Ferlie & Shortell
2001), based on the ethos of a core team caring for a
defined population and possessing the right resources to
support frontline staff and patients (Nelson et al.1998).
While, in terms of organizational culture, the use of micro
systems appears to be beneficial in supporting services,
their ability to branch out in different areas of health care
is highly dependent on investment and resources available.
Additional evaluation of how other areas of health care
promote the uptake of evidence in infection control would
enhance understanding of different enabling systems in
play.
Limitations
Although the case study generated a small sample of
respondents, it addressed the principal intention which was
to explore in depth what was working in terms of a partic-
ular infection control intermediary programme. Although it
is not possible to draw generalizations from one case study,
the findings give some insight into certain contextual condi-
tions which can trigger successful mechanisms of actions
and potential for theoretical transferability. Furthermore,
influence of other contextual factors requires further explo-
ration as to how they impact on important mechanisms. In
line with the principles of realist evaluation, further work
will be conducted to test these findings and generate better
understanding of the relationships between the contexts,
mechanisms and outcomes configurations uncovered here,
to develop clearer theory about what works in complex
programmes.
What is already known about this topic
● Across the globe, the provision, uptake and implemen-
tation of available evidence that promotes best prac-
tice in infection control and reduces the risks to
patients is a key priority.
● Understanding how to get what is already known to
work into everyday practice firstly requires the
unpacking of contextual factors that influence individ-
ual and organizational behaviour.
● In healthcare, a range of individuals, collectively
known as intermediaries, are recognized as having the
potential to influence the transfer and use of evidence
in practice.
What this paper adds
● High levels of visibility of people in intermediary roles
in clinical areas trigger a range of reactions from
frontline staff and patients.
● Specific ways intermediaries give feedback on perfor-
mance and develop relationships in clinical areas can
impact on individuals’ behaviour.
● A practice-based approach to teaching and making it
relevant to local context leads to more meaningful
learning for staff.
Implications for practice and/or policy
● Intermediary programmes in infection control can
influence behaviour, but their success will be contin-
gent on organizational commitment, including invest-
ment.
● For the infection control arena, a clearer understand-
ing of the impact of intermediary presence and visibil-
ity in clinical areas is required.
● Intervention planning in infection control requires
early consideration of contextual conditions which are
likely to influence its success or failure.
© 2012 Blackwell Publishing Ltd 9
JAN: ORIGINAL RESEARCH Realist evaluation intermediaries infection control

Conclusion
In this study, specific actions employed by infection con-
trol intermediaries have emerged as having the potential to
trigger change, providing theoretical suppositions of how
intermediaries can be successful in promoting appropriate
infection control practice in certain contextual conditions.
Through the use of realist evaluation as a framework,
important elements have emerged about visibility, facilita-
tion, performance feedback and ways of providing educa-
tion. To increase the potential for change, managers and
policy makers need to be made aware of the ways inter-
mediary programmes can influence behaviours and build
these into initiatives. For the infection control arena, a
clearer understanding of the impact of intermediary
presence and visibility in clinical areas is required. Inter-
vention planning in infection control requires early consid-
eration of contextual conditions, which are likely to
influence its success or failure, which includes organiza-
tional commitment and investment. Further testing of the
specific intermediary mechanisms of action uncovered in
this study will contribute to understanding different
approaches that work in infection control in embedding
evidence in practice.
Funding
This research was conducted as part of a PhD Fellowship
awarded to Lynne Williams by the research capacity build-
ing collaboration (rcbcwales) in January 2010.
Conflict of interest
No conflict of interest has been declared by the authors.
Author contributions
All authors meet at least one of the following criteria (rec-
ommended by the ICMJE: http://www.icmje.org/ethi-
cal_1author.html) and have agreed on the final version:
● substantial contributions to conception and design, acqui-
sition of data, or analysis and interpretation of data;
● drafting the article or revising it critically for important
intellectual content.
References
Barry D. & Carter Y. (2010) Developing Satellite Roles in
Infection Prevention Teams to Fulfil Responsibilities. Retrieved
from http://www.nursingtimes.net on 13 September.
Burton C., Green T. & Fisher A. (2009) The organizational
context of nursing care in stroke units: a case study approach.
International Journal of Nursing Studies 46(1), 85–94.
Byng R., Norman I. & Redfern S. (2005) Using realistic evaluation
to evaluate a practice-level intervention to improve primary
health care for patients with long-term mental illness. Evaluation
11(1), 69–93.
Damschroder L.J., Banaszak-Holl J., Kowalski C.P., Forman J.,
Saint S. & Krein S.L. (2009) The role of the ‘champion’ in
infection prevention: results from a multisite qualitative study.
Quality Safety Health Care 18(6), 434–440.
Dawson S.J. (2003) The role of the infection control link nurse.
Journal of Hospital Infection 54(4), 251–257.
Dawson S., Burnett B. & McArdle F.. (2005) Watching learning
from behind closed doors: the impact of surveillance on student
online behaviourIn Proceedings: E Learn 2005: World
Conference on E-learning in Corporate, Government, Healthcare
and Higher Education, Vancouver, Canada.
Dealey C., Moss H., Marshall J. & Elcoat C. (2007) Auditing the
impact of implementing the Modern Matron role in an acute
teaching trust. Journal of Nursing Management 15(1), 22–33.
Department of Health (2001) Implementing the NHS Plan: Modern
Matrons: Strengthening the Role of Ward Sisters and Introducing
Senior SistersHSC 2001/010, The Stationery Office, London.
Ferguson L., Milner M. & Snelgrove-Clarke E. (2004) The role of
intermediaries: getting evidence into practice. Journal of Wound,
Ostomy & Continence Nursing 31(6), 325–327.
Ferlie E.B. & Shortell S.M. (2001) Improving the quality of health
care in the United Kingdom and the United States: a framework
for change. The Millbank Quarterly 79(2), 281–315.
Firth-Cozens J. (2004) Organisational trust: the keystone to patient
safety. Quality Safety Health Care 13(1), 56–61.
Gardam M.A., Lemieux C., Reason P., van Dijk M. & Goel V.
(2009) Healthcare-associated infections as patient safety
indicators. Healthcare Papers 9(3), 8–24.
Gilmore G. (2011) Educating the infection prevention and control
educators –musings from the IFIC education chair (Editorial
Commentary). International Journal of Infection Control 7(2),
1–3.
Gold R. (1969) Roles in sociological field observation. In Issues in
Participant Observation: a Text and Reader (McCall G. &
Simmons J., eds), Addison Wesley, London, pp. 30–39.
Greenhalgh T., Robert G. & Bate P. (2004) How to Spread Good
Ideas – A Systematic Review off the Literature on Diffusion,
Dissemination and Sustainability of Innovations in Health
Service Delivery and Organisation. National Co-ordinating
Centre for NHS Service Delivery and Organisation R&D
(NCCSDO), London.
Greenhalgh T., Humphrey C., Hughes J., McFarlane F., Butler C.
& Pawson R. (2009) How do you modernize a health service? A
realist evaluation of whole-scale transformation in London.
Milbank Quarterly 87(2), 391–416.
Griffiths P., Renz A. & Rafferty A. (2008) The Impact of
Organisation and Management Factors on Infection Control in
Hospitals: A Scoping Review. RCN, London.
Grol R. & Grimshaw J. (2003) ‘From best evidence to best
practice: effective implementation of change in patients’ care’.
The Lancet 362(9391), 1225–1230.
10 © 2012 Blackwell Publishing Ltd
L. Williams et al.

Harvey G., Loftus-Hills A., Rycroft-Malone J., Titchen A., Kitson
A., McCormack B. & Seers K. (2002) Getting evidence into
practice: the role and function of facilitation. Journal of
Advanced Nursing 37(6), 577–588.
Healthcare Commission (2007) Healthcare Associated Infection:
What Else can the NHS do?. Retrieved from http://www.
healthcarecommission.org.uk on 7 November 2011.
HM Inspectorate of Constabulary (2002) Narrowing the Gap –
Police Visibility and Public Reassurance-Managing Public
Expectation and Demand. The Stationery Office, Edinburgh.
Hoong Sin C. (2008) The role of intermediaries in getting evidence
into policy and practice: some useful lessons from examining
consultancy-client relationships. Evidence and Policy 4(1), 85–
103.
Infection Control Nurses Association (2004) Core Competencies
for Practitioners in Infection Control Prevention and Control,
2nd edn. Retrieved from http://www.icna.co.uk on 7 November
2011.
Lewis T. & Edwards C. (2008) How clinical champions can
improve quality. Nursing Management 14(10), 24–27.
Marchal B., Dedzo M. & Kegels G. (2010) A realistic evaluation of
the management of a well performing regional hospital in Ghana.
BMC Health Services Research 10(24) , Retrieved from http://
www.biomedcentral.com/1472-6963/10/24 on 7 November 2011.
McQueen D.V. (1999) A world behaving badly: the global
challenge for behavioural surveillance. American Journal of
Public Health 89(9), 1312–1314.
Miles M.B. & Huberman A.M. (1994) Qualitative Data Analysis
(2nd edn). Sage Publications, Thousand Oaks, CA.
Milner M., Estabrooks C.A. & Humphrey C. (2005) Clinical nurse
educators as agents for change: increasing research utilisation in
nursing practice. International Journal of Nursing Studies 42(8),
899–914.
Milner M., Estabrooks C.A. & Myrick F. (2006) Research
utilisation and clinical nurse educators: a systematic review.
Journal of Evaluation in Clinical Practice 12(6), 639–655.
Nelson E.C., Batalden P.B. & Mohr J.J. (1998) Building a quality
future. Frontiers of Health Services Management 15(1), 3–32.
Northway T. & Mawdsley C. (2007) The Canadian ICU
Collaborative: on being a nurse champion. Influencing support
and change. Canadian Association of Critical Care Nurses 18(3),
25–27.
Pawson R. (2006) Evidence-Based Policy – A Realist Perspective.
Sage, London.
Pawson R. & Tilley N. (1997) Realistic Evaluation. Sage, London.
Procter S., Allan T. & Lacey A. (2010) Sampling Ch12. In The
Research Process in Nursing, 6th edn (Gerrish K. & Lacey A.,
eds), Wiley-Blackwell, Oxford, pp. 142–152.
Rashotte L. (2007) Social influence In Blackwell Encyclopedia of
Sociology (Ritzer G., ed.), John Wiley & Sons, Oxford, pp. 4426–
4429.
Rycroft-Malone J. (2004) The PARIHS framework – a framework
for guiding the implementation of evidence-based practice.
Journal of Nursing Care Quality 19(4), 297–304.
Rycroft-Malone J., Fontenla M., Bick D. & Seers K. (2008)
Protocol-based care: impact on roles and service delivery. Journal
of Evaluation in Clinical Practice 14(5), 867–873.
Rycroft-Malone J., Fontenla M., Bick D. & Seers K. (2010) A
realistic evaluation: the case of protocol-based care.
Implementation Science 5(38), Retrieved from http://www.
implementationscience.com/content/5/1/38 on 7 November 2011.
Spradley J.P. (1980) Participant Observation, Harcourt Brace
Jovanovich College Publishers, Orlando, FL.
Stetler C.B., Legro M.W., Rycroft-Malone J., Bowman C., Curran
G., Guihan M., Hagedorn H., Pineros S. & Wallace C. (2006)
Role of ‘external facilitation’ in implementation of research
findings: a qualitative evaluation of facilitation experiences in the
Veterans Health Administration. Implementation Science 1(23),
Retrieved from http://www.implementationscience.com/content/1/
1/23 on 14 November 2011.
Stetler C.B., Ritchie J., Rycroft-Malone J., Schultz A. & Charns M.
P. (2009) Institutionalising evidence-based practice: an
organisational case study using a model of strategic change.
Implementation Science 4(78), Retrieved from http://www.
implementationscience.com/content/4/1/78 on 8 July 2011.
Sullivan H., Barnes M. & Matka E. (2002) Building collaborative
capacity through ‘theories of change’ Early lessons from the
evaluation of health action zones in England. Evaluation 8(2),
205–226.
Thompson G.N., Estabrooks C.A. & Degner L.F. (2006) Clarifying
the concepts in knowledge transfer: a literature review. Journal
of Advanced Nursing 53(6), 691–701.
Tilley N. (2000) Realistic Evaluation: An Overview. The Founding
Conference of the Danish Evaluation Society, Nottingham Trent
University.
Tolson D., McIntosh J., Loftus L. & Cormie P. (2007) Developing
a managed clinical network in palliative care: a realistic
evaluation. International Journal of Nursing Studies 44(2), 183–
195.
Watson H., Booth J. & Whyte R. (2010) Observation Ch 31. In
The Research Process in Nursing (Gerrish K. & Lacey A., eds),
6th edn, Wiley-Blackwell Oxford, pp. 382–394.
Welsh Assembly Government (2004) Healthcare Associated
Infections – A Strategy for Hospitals in Wales. Retrieved from
http://nww.nphs.wales.nhs.uk on 8 July 2011.
Welsh Government (2011) Together for Health–A Five Year Vision
for the NHS in Wales. Retrieved from http://www.cymru.gov.uk
on 11 November 2011.
Wilcox M. (2009) Infection Control – A Psychological Approach
to Changing Practice. Radcliffe Publishing, Oxford.
Wisniewski M.F., Kim S., Trick W.E. , Welbel S.F. & Weinstein R.
A. (2007) Chicago Antimicrobial Resistance Project Effect of
education on hand hygiene beliefs and practices: a 5-year
program. Infection Control and Hospital Epidemiology 28(1),
88–91.
World Health Organization (2011a) Clean Care is Safer Care.
Retrieved from http://www.who.int/topics/infection_control/en/
on 5 October 2011.
World Health Organization (2011b) Report on the Burden of
Endemic Health-Care Associated Infection Worldwide – A
Systematic Review of the Literature. World Health Organisation,
Geneva.
Yin R.K. (1994) Case Study Research: Design and Methods, 2nd
edn, Sage Publications, London.
© 2012 Blackwell Publishing Ltd 11
JAN: ORIGINAL RESEARCH Realist evaluation intermediaries infection control

The Journal of Advanced Nursing (JAN) is an international, peer-reviewed, scientific journal. JAN contributes to the advancement of
evidence-based nursing, midwifery and health care by disseminating high quality research and scholarship of contemporary relevance
and with potential to advance knowledge for practice, education, management or policy. JAN publishes research reviews, original
research reports and methodological and theoretical papers.
For further information, please visit JAN on the Wiley Online Library website: www.wileyonlinelibrary.com/journal/jan
Reasons to publish your work in JAN:
• High-impact forum: the world’s most cited nursing journal and with an Impact Factor of 1·540 – ranked 9th of 85 in the 2010
Thomson Reuters Journal Citation Report (Social Science – Nursing). JAN has been in the top ten every year for a decade.
• Most read nursing journal in the world: over 3 million articles downloaded online per year and accessible in over 10,000 libraries
worldwide (including over 3,500 in developing countries with free or low cost access).
• Fast and easy online submission: online submission at http://mc.manuscriptcentral.com/jan.
• Positive publishing experience: rapid double-blind peer review with constructive feedback.
• Rapid online publication in five weeks: average time from final manuscript arriving in production to online publication.
• Online Open: the option to pay to make your article freely and openly accessible to non-subscribers upon publication on Wiley
Online Library, as well as the option to deposit the article in your own or your funding agency’s preferred archive (e.g. PubMed).
12 © 2012 Blackwell Publishing Ltd
L. Williams et al.