
What to Know About the House GOP’s Repeal and Replace Plan€¦ · House GOP’s Repeal and...
32
research technology consulting What to Know About the House GOP’s Repeal and Replace Plan Health Care Advisory Board
Transcript of What to Know About the House GOP’s Repeal and Replace Plan€¦ · House GOP’s Repeal and...

research technology consulting
What to Know About the
House GOP’s Repeal and
Replace Plan
Health Care
Advisory Board

©2017 Advisory Board • All Rights Reserved • advisory.com
6 6
Today’s Panel
Eric Cragun
Senior Director,
Health Policy
Russell Davis
Executive Director,
Research
Rob Lazerow
Managing Director,
Health Care Advisory Board

7
2
3
1
Road Map
©2017 Advisory Board • All Rights Reserved • advisory.com • 33602A
GOP Moving Toward ACA “Repeal and Replace”
Key Details of American Health Care Act
Next Steps for Providers

©2017 Advisory Board • All Rights Reserved • advisory.com
8 8
Has It Really Only Been Two Months?
Source: Health Care Advisory Board analysis.
1) Ways and Means.
2) Energy and Commerce.
Timeline of ACA- and AHCA-Related Developments
January 12-13, 2017
Senate and House voted
to begin budget
reconciliation process
January 20, 2017
President Trump signed
executive order directing
agencies to review ACA
January 27, 2017
Non-binding deadline for
congressional committees
to develop proposals
February 10, 2017
Senate confirms
Tom Price as HHS
Secretary
March 6, 2017
GOP introduced
American Health
Care Act (AHCA)
February 15, 2017
HHS releases market
stabilization proposed
rule
March 9, 2017
House W&M1 and
E&C2 Committees
approve AHCA

©2017 Advisory Board • All Rights Reserved • advisory.com
9 9
Introducing the American Health Care Act (AHCA)
With Proposed Reconciliation Bill, GOP One Step Closer to ACA Repeal
Source: House Ways and Means Committee, available at: https://waysandmeans.house.gov/american-health-care-act/; House
Energy and Commerce Committee, available at: https://energycommerce.house.gov/news-center/press-releases/energy-and-
commerce-republicans-release-legislation-repeal-and-replace; Health Care Advisory Board interviews and analysis.
1) Restores funding in 2018 in non-expansion states and 2020 in expansion states.
Key Elements of the American Health Care Act
Repeals ACA Taxes Reforms Individual Market Reforms Medicaid Financing
• Retains expansion for
individuals who are enrolled by
the end of 2019
• Reverses DSH cuts1, provides
additional funding for FQHCs,
safety net providers
• Adopts per capita caps on
federal funding starting in 2020
• Eliminates individual mandate
retroactive to Dec. 31, 2015
• Requires insurers to penalize
individuals who do not
maintain continuous coverage
• In 2020, replaces subsidies
with refundable tax credits
adjusted for age and income
• Beginning in 2018, eliminates
ACA taxes on health insurers,
medications, HSAs, medical
device manufacturers, tanning
services, investment
income, etc.
• Delays implementation of
the Cadillac Tax until 2025
American Health Care Act
• Proposed reconciliation bill released by House Republicans on March 6, 2017
• Would repeal, replace, or adjust some components of the ACA, while leaving many others intact
©2017 Advisory Board • All Rights Reserved • advisory.com
10 10
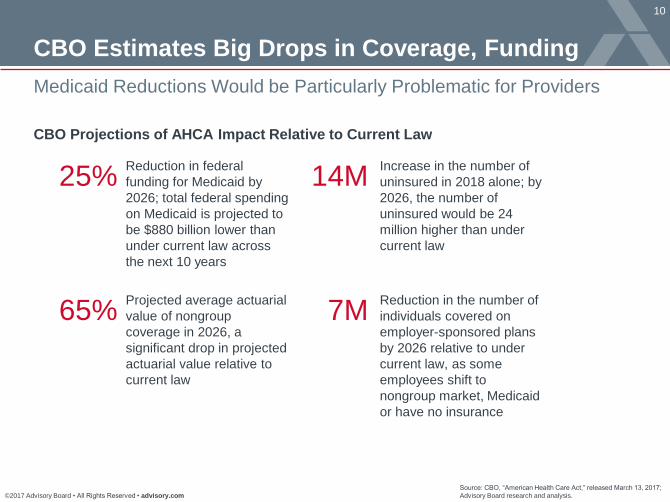
CBO Estimates Big Drops in Coverage, Funding
Medicaid Reductions Would be Particularly Problematic for Providers
Source: CBO, “American Health Care Act,” released March 13, 2017;
Advisory Board research and analysis.
25% Reduction in federal
funding for Medicaid by
2026; total federal spending
on Medicaid is projected to
be $880 billion lower than
under current law across
the next 10 years
14M Increase in the number of
uninsured in 2018 alone; by
2026, the number of
uninsured would be 24
million higher than under
current law
65% Projected average actuarial
value of nongroup
coverage in 2026, a
significant drop in projected
actuarial value relative to
current law
7M Reduction in the number of
individuals covered on
employer-sponsored plans
by 2026 relative to under
current law, as some
employees shift to
nongroup market, Medicaid
or have no insurance
CBO Projections of AHCA Impact Relative to Current Law

©2017 Advisory Board • All Rights Reserved • advisory.com
11 11
Assessing the AHCA’s Likely Challenges for Providers
Source: Health Care Advisory Board interviews and analysis.
Not Worse Case… …But Impact Likely Significantly Negative
Does not impact Medicare payment
reforms or disrupt Medicare coverage
through transition to premium support
Bolsters safety net through restoration
of DSH payments, new funding for
FQHCs and safety net hospitals
Seeks to maintain some coverage
expansion gains in individual
market and Medicaid
Caps on Medicaid spending will
grow at CPI-M, as opposed to a more
aggressive target like CPI-U
Reimbursement Cuts Remain, Likely to Intensify
1
• Except for DSH cuts, proposal does not reverse
ACA’s payment cuts
• Reductions in Medicaid funding likely to cause
states to reduce provider reimbursement
Potential Reductions to Coverage Still Loom
2
• Medicaid per-enrollee spending growth already low,
states may be forced to cut eligibility and benefits
• Proposed tax credits less generous than ACA
subsidies for vast majority, could lead to attrition
from individual market

©2017 Advisory Board • All Rights Reserved • advisory.com
12 12
Far From a Done Deal
GOP Leadership Will Need to Solidify Support from Key GOP Factions
Source: New York Times, “House Republicans Unveil Plan to Replace Health Law,” March 6, 2017; RSC Policy Memo,
available at: http://www.politico.com/f/?id=0000015a-a684-d464-adfe-f69721ce0002, March 6, 2017; Letter to Honorable
Mitch McConnell, available at: http://www.portman.senate.gov/public/index.cfm?p=press-releases&id=c6d96a68-a891-
4ba1-8ad2-1ce166e0f8eb, March 6, 2017; Health Care Advisory Board interviews and analysis .
But Republican Rank and File Raising Concerns
“This is a Republican welfare entitlement.
Writing checks to individuals to purchase
insurance is, in principle, Obamacare.”
Republican Study Committee
White House Support Lends Weight to Repeal Effort
“Today, [March 6th], marks an important step toward restoring health care choices and
affordability back to the American people. President Trump looks forward to working with
both Chambers of Congress to repeal and replace Obamacare."
Sean Spicer, White House Press Secretary
“…We will not support a plan that does
not include stability for Medicaid expansion
populations or flexibility for states.”
Senators Portman (R-OH), Capito (R-WV),
Gardner (R-CO) and Murkowski (R-AK)

©2017 Advisory Board • All Rights Reserved • advisory.com
13 13
GOP Must Still Reckon with Reconciliation in Senate
Even if House Passes Bill, Parliamentarian’s Ruling Could Alter Provisions
Source: Peterson K, “Chief Senate Parliamentarian Will Play Crucial
Role in Health Care Legislation,” 16 Jan 2017, available at:
www.wsj.com; Advisory Board research and analysis.
The Basics of Budget Reconciliation
May only be used for provisions that impact
spending, revenues, or the federal debt limit
Senate debate is limited to 20 hours
Because of the limits set on debate time, no
Senate filibuster is permitted
Bills may pass in the Senate with a simple
majority of 51 votes
20 Bills passed through
reconciliation that
became law since 1980
Meet the Senate Parliamentarian
• Currently Elizabeth
MacDonough, a lawyer
who has been in the
role since 2012
• She is the sixth person
to hold the role since it
was established in 1935
• The Parliamentarian
helps Senate leaders
determine process
based on historical
precedent
• In budget reconciliation,
the Parliamentarian
determines which
provisions meet rules of
reconciliation Im
age:
ww
w.s
enate
.gov

©2017 Advisory Board • All Rights Reserved • advisory.com
14 14
AHCA Only the First Step in Republicans’ Plan
GOP Laying Out Three Phases to Health Care Reform
Source: The White House, “Three-Pronged Approach to Repeal and Replace
Obamacare,” March 13, 2017; Health Care Advisory Board interviews and analysis.
Administrative
Action
Additional
Legislation
Budget
Reconciliation 1
A Three-Pronged Approach to Repeal and Replace the ACA
2 3
Proposed Target Areas:
• Repeal ACA taxes, employer
and individual mandates
• Replace insurance subsidies
with refundable tax credits
• Reform Medicaid financing
• Increase contribution limit of
health savings accounts
• Allocate funds for state
innovations
• Require continuous coverage
insurance incentive
Process: Requires simple
majority in House and Senate
Likely Target Areas:
• Shorten individual market
enrollment period and limit
special enrollment
• Loosen restrictions on actuarial
value of individual market plans
• Enable state flexibility through
waiver process
• Approve state Medicaid
eligibility changes (e.g. work
requirements, premiums)
Process: Federal agencies issue
regulation through rulemaking
Process: Requires simple majority
in House, super-majority in Senate
Likely Target Areas:
• Allow insurance to be sold
across state lines
• Expand use of HSAs
• Allow formation of Association
Health Plans
• Remove “essential benefits”
requirements
• Reform malpractice regulation
• Streamline FDA processes
• Expand flexibility of state use
of federal dollars
15
2
3
1
Road Map
©2017 Advisory Board • All Rights Reserved • advisory.com • 33602A
GOP Moving Toward ACA “Repeal and Replace”
Key Details of American Health Care Act
Next Steps for Providers

©2017 Advisory Board • All Rights Reserved • advisory.com
16 16
Individual Market Topping Reform Agenda
Mechanics Fundamentally Changed in GOP Replacement
Private Insurance Changes
Source: Health Care Advisory Board interviews and analysis.
“Patient and State Stability” Fund
Grants flexible federal funding for
states to support insurance markets
(e.g. by creating high-risk pool or
assisting with out-of-pocket costs)
Expansion of Health Savings
Accounts
Increase in the breadth of services
that may be paid for using HSAs
and the total amount of money that
can be contributed to them
Updated Age-Rating Ratio
Allows age-based premium
differential for individual plans
to change from 3:1 to 5:1
Individual, Refundable Tax Credits
Provides tax credits for individual
insurance purchase to those not
offered employer-sponsored plans;
credits are based on age and income
and tied to CPI-U growth
Repeals Alters Establishes
Continuous Coverage Incentive
Requires insurers to penalize
individuals who have had a two-
month coverage gap in previous 12
months with a 30% surcharge
Individual and Employer
Mandate
Eliminates the penalty on
individuals and employers for not
gaining or not offering insurance
coverage
ACA Insurance Premium and
Cost-Sharing Subsidies
Removes ACA tax credits based on
income and tied to the growth of the
regional silver plan premiums, as
well as cost-sharing subsidies
Actuarial Value Standards
Eliminates the requirement that
plans meet actuarial value
minimums standardized by metal
tier (Bronze, Silver, etc.)

©2017 Advisory Board • All Rights Reserved • advisory.com
17 17
Subsidies Would Drop for Low-Income Individuals
Impact Would be Particularly Dramatic for Older, Low-Income Individuals
Source: Kaiser Family Foundation, “How Affordable Care Act Repeal and Replace Plans
Might Shift Health Insurance Tax Credits,” available at: kff.org; Advisory Board analysis.
Projected Premium Tax Credit Available in Individual Market in 2020
Individual with $20,000 in Income (160% FPL)
$0 $0 $0
$2,000 $2,000 $2,000
Reno, NV US Average Mobile, AL
$2,899 $3,225
$4,522
$2,000 $2,000 $2,000
Reno, NV US Average Mobile, AL
$9,030 $9,874
$13,235
$4,000 $4,000 $4,000
Reno, NV US Average Mobile, AL
ACA AHCA
$0 $0 $0
$4,000 $4,000 $4,000
Reno, NV US Average Mobile, AL
ACA AHCA
Individual with $75,000 in Income (600% FPL)
27-y
ear
old
60-y
ear
old
©2017 Advisory Board • All Rights Reserved • advisory.com
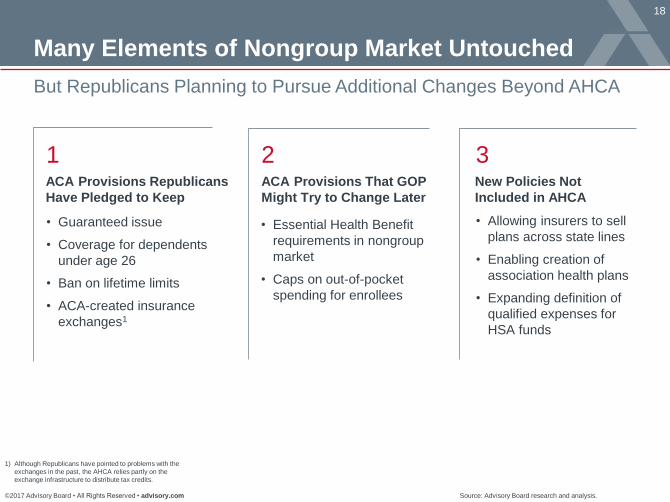
18 18
Many Elements of Nongroup Market Untouched
But Republicans Planning to Pursue Additional Changes Beyond AHCA
Source: Advisory Board research and analysis.
1) Although Republicans have pointed to problems with the
exchanges in the past, the AHCA relies partly on the
exchange infrastructure to distribute tax credits.
ACA Provisions Republicans
Have Pledged to Keep
ACA Provisions That GOP
Might Try to Change Later
New Policies Not
Included in AHCA
1 2 3
• Guaranteed issue
• Coverage for dependents
under age 26
• Ban on lifetime limits
• ACA-created insurance
exchanges1
• Essential Health Benefit
requirements in nongroup
market
• Caps on out-of-pocket
spending for enrollees
• Allowing insurers to sell
plans across state lines
• Enabling creation of
association health plans
• Expanding definition of
qualified expenses for
HSA funds

©2017 Advisory Board • All Rights Reserved • advisory.com
19 19
CBO Expects Stable Market, But
Demographics May Shift
Number with Private Insurance Likely to be Lower
Premiums May Be Higher in the Short-Term, but Lower Long-Term
Source: CBO, “American Health Care Act,” released March 13, 2017;
Advisory Board research and analysis.
-10
-8
-6
-4
-2
0
2017 2020 2023 2026
Nongroup Employment-based
CBO Projected Change in Individuals Covered
By Source of Insurance;
Relative to Current Law Baseline
Mill
ion
s
2 million
fewer
nongroup
enrollees
7 million
fewer
employer-
sponsored
enrollees
“In CBO and JCT’s assessment, … the
nongroup market would probably be
stable in most areas under either current
law or the legislation.”
“In 2018 and 2019 … average premiums
… would be 15 to 20 percent higher
than under current law, mainly because
… fewer comparatively healthy people
[would] sign up.”
“By 2026, average premiums … would
be roughly 10 percent lower than
under current law” due to stabilization
funds, elimination of actuarial value
requirements, and “a younger mix of
enrollees.”
©2017 Advisory Board • All Rights Reserved • advisory.com
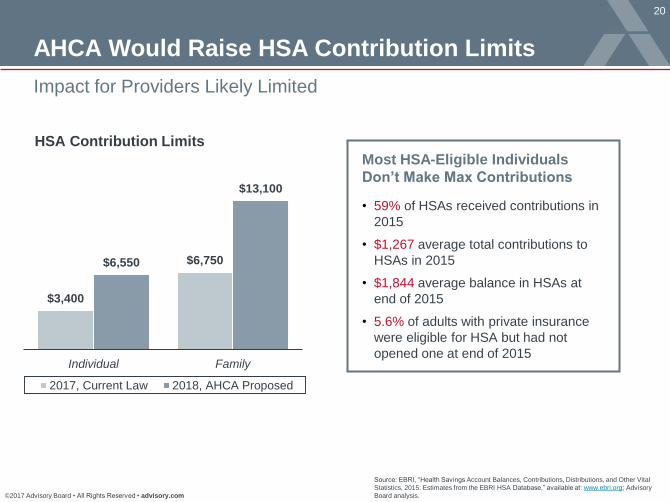
20 20
AHCA Would Raise HSA Contribution Limits
Impact for Providers Likely Limited
Source: EBRI, “Health Savings Account Balances, Contributions, Distributions, and Other Vital
Statistics, 2015: Estimates from the EBRI HSA Database,” available at: www.ebri.org; Advisory
Board analysis.
$3,400
$6,750 $6,550
$13,100
Individual Family
2017, Current Law 2018, AHCA Proposed
HSA Contribution Limits
Most HSA-Eligible Individuals
Don’t Make Max Contributions
• 59% of HSAs received contributions in
2015
• $1,267 average total contributions to
HSAs in 2015
• $1,844 average balance in HSAs at
end of 2015
• 5.6% of adults with private insurance
were eligible for HSA but had not
opened one at end of 2015
©2017 Advisory Board • All Rights Reserved • advisory.com
21 21
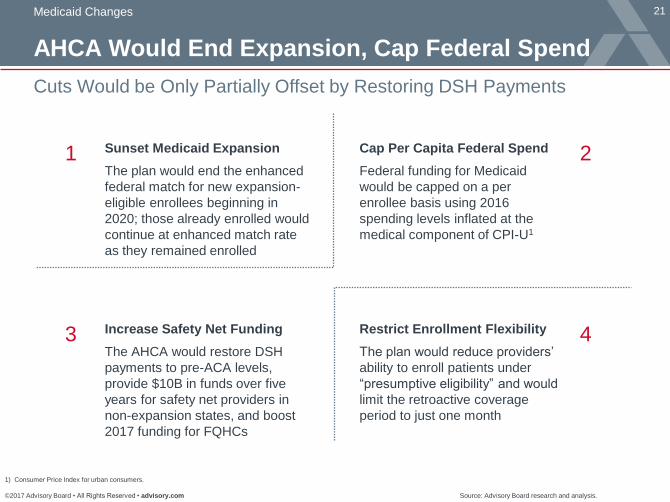
AHCA Would End Expansion, Cap Federal Spend
Cuts Would be Only Partially Offset by Restoring DSH Payments
Medicaid Changes
Source: Advisory Board research and analysis.
1) Consumer Price Index for urban consumers.
Sunset Medicaid Expansion
The plan would end the enhanced
federal match for new expansion-
eligible enrollees beginning in
2020; those already enrolled would
continue at enhanced match rate
as they remained enrolled
Cap Per Capita Federal Spend
Federal funding for Medicaid
would be capped on a per
enrollee basis using 2016
spending levels inflated at the
medical component of CPI-U1
Increase Safety Net Funding
The AHCA would restore DSH
payments to pre-ACA levels,
provide $10B in funds over five
years for safety net providers in
non-expansion states, and boost
2017 funding for FQHCs
Restrict Enrollment Flexibility
The plan would reduce providers’
ability to enroll patients under
“presumptive eligibility” and would
limit the retroactive coverage
period to just one month
1 2
3 4

©2017 Advisory Board • All Rights Reserved • advisory.com
22 22
Significant Changes to Medicaid Funding Model
AHCA Intended to Limit Spending, HHS May Give States Flexibility
Source: Health Care Advisory Board interviews and analysis
Per Capita Allotment
• Cap on amount of federal
contribution to each state per
enrollee category
• States spending over the cap
would see reduced payment
for the subsequent year
• Spending targets would be
based on 2016 spending and
trended forwarded using CPI-M
growth rate
The [Trump] Administration will act
to…maximize flexibility for States in
administering Medicaid, to enable
States to experiment with innovative
methods to deliver healthcare to our
low-income citizens
Presidential Transition Health Policy Outline
AHCA’s Proposals to Reform Medicaid Financing

©2017 Advisory Board • All Rights Reserved • advisory.com
23
Impact Hinges on Growth Rate of Spending Target
AHCA Strikes Middle Ground in Proposed Growth Rate of CPI-M
Source: CMS, National Health Expenditures Fact Sheet, available at: www.cms.gov/research-statistics-data-
and-systems/statistics-trends-and-reports/nationalhealthexpenddata/nhe-fact-sheet.html; CMS, National Health
Expenditures Projections 2016-2025, available at: https://www.cms.gov/research-statistics-data-and-
systems/statistics-trends-and-reports/nationalhealthexpenddata/nationalhealthaccountsprojected.html; CMS,
2016 Actuarial Report on the Financial Outlook for Medicaid, available at: https://www.cms.gov/Research-
Statistics-Data-and-Systems/Research/ActuarialStudies/Downloads/MedicaidReport2016.pdf; Health Care
Advisory Board interviews and analysis.
1) From CMS 2016 Medicaid Actuarial Report and CMS
NHE Projects, 2015-2025.
Growth Factor Actual Average Annual
Growth Rate 2000-2011
Projected Average Annual
Growth Rate 2017-20251
Urban Consumer Price
Index (CPI-U) 2.45% 2.6%
CPI-U +
population growth 3.4% 3.5%
Medical Care Inflation
(CPI-M) 3.9% 4.2%
Gross Domestic Product
(GDP) 3.8% 5.0%
CPI-M + 1 percentage point 4.9% 5.2%
National Per Capita Health
Expenditures 6.3% 4.8%
Average National Medicaid
Spending Growth Per-
Enrollee
3.8% 4.3%
Proposed
in AHCA

©2017 Advisory Board • All Rights Reserved • advisory.com
24 24
Impact of Medicaid Reform Would Vary by State
Source: Kaiser Family Foundation, “Data Note: Variation in Per Enrollee Medicaid
Spending Across States,” Feb. 2017; Health Care Advisory Board interviews and analysis.
5.1%
2.8% 1.7%
6.6%
3.2%
1.2%
4.0%
5.6%
DE: 3.7%
DC: 5.0%
MD: 5.9%
3.4%
5.7%
1.2%
3.2%
RI: 4.9%
CT: -0.5%
4.8%
6.6%
MA: 5.8%
NJ: 2.9%
VT: 6.9%
National Average:
3.8%
2.8%
2.9%
7.1% 5.5%
6.6%
5.0% 4.8%
4.3%
4.2%
3.3%
1.5%
4.0%
1.0%
2.1%
3.2%
2.6% 4.3%
0.9%
4.0%
3.7%
1.8%
6.5%
2.5%
2.1% 3.5%
NH: 1.8%
2.1%
8.1%
3.1%
Average Annual Growth in Medicaid Spending Per-Enrollee
Fiscal Year 2000-2011 Spending Growth
Fell Above CPI-M
Spending Growth
Fell Below CPI-M

©2017 Advisory Board • All Rights Reserved • advisory.com
25 25
CBO Projects Medicaid Funding
Would be Dramatically Lower
Federal Medicaid Spend Projected to be 25% Lower
Reduction Result of Funding Caps, Eligibility Cuts, and End of Mandate
Source: CBO, “American Health Care Act,” released March 13, 2017;
Advisory Board research and analysis.
-16
-14
-12
-10
-8
-6
-4
-2
0
2017 2020 2023 2026
CBO Projected Change in Medicaid Enrollment
Relative to Current Law Baseline
Mill
ion
s
14 million
fewer
Medicaid
enrollees
“CBO estimates that several major
provisions affecting Medicaid would
decrease direct spending by $880
billion over the 2017-2026 period.”
“By 2026, Medicaid spending would be
about 25 percent less than what CBO
projects under current law.”
“On the basis of historical data…, CBO
projects that fewer than one-third of
those enrolled [in Medicaid] as of
December 31, 2019, would have
maintained continuous eligibility two
years later.”

©2017 Advisory Board • All Rights Reserved • advisory.com
26 26
Not a Rosy Picture for Providers
Regardless of State Response, Spending Cuts Would Impact Hospitals
Source: Health Care Advisory Board interviews and analysis.
ACA Boost to Medicaid Funding
Positively Impacted Hospital
Finances
Medicaid admissions increased
21% for investor-owned hospitals
in expansion states
Self-pay admissions decreased
by 47% for investor-owned
hospitals in expansion states
Uncompensated care costs
reduced by $5 billion in expansion
states in 2014
Potential State Options
Pull back on
eligibility
Move to
Medicaid
managed care
Keep existing
fee-for-service
payment model
Spike in uninsured rate
Lower rates through
health plan contracting
Lower payment rates
Options Potential Impact

©2017 Advisory Board • All Rights Reserved • advisory.com
27 27
• Medicare surtax
• Capital gains surtax
• Increased tax on non-
qualified HSA distributions
AHCA Repeals Almost All ACA-Imposed Taxes
Potential Benefits for Pharma, Payers, and Device Manufacturers
Tax Changes
Source: Advisory Board research and analysis.
ACA Taxes Repealed Under the AHCA
Taxes on High Earners
Individuals Industry Taxes
• Tax on medical devices
• Tax on over-the-counter
medications
• Tax on prescription medications
• Tax on health insurers
• Excise tax on high-cost health
insurance (“Cadillac Tax”)
delayed to 2025

©2017 Advisory Board • All Rights Reserved • advisory.com
28 28
AHCA Would Retain Medicare IPPS Cuts
No Intent to Begin Raising Provider Payments Anytime Soon
What Didn’t Change?
Source: CBO, “Letter to the Honorable John Boehner Providing an Estimate for H.R. 6079, The Repeal of Obamacare Act,”
July 24, 2012; CBO, “Cost Estimate and Supplemental Analyses for H.R. 2, the Medicare Access and CHIP Reauthorization
Act of 2015; The Daily Briefing, “How to Understand Last Week’s Big Budget Deal,” November 2, 2015; Budget of the United
States Government (Proposed) FY 2016; Health Care Advisory Board interviews and analysis.
1) Inpatient Prospective Payment System.
2) Disproportionate Share Hospital.
3) Medicare Access and CHIP Reauthorization Act.
“Productivity” Adjustments and Other Cuts
2013 2014 2015 2016 2017 2018 2019 2020 2021 2022
($4B)
($14B)
($24B) ($29B)
($38B)
($54B)
($67B)
($76B)
($86B) ($94B)
ACA IPPS1 Update
Adjustments
ACA DSH2 Payment Cuts
MACRA3 IPPS Update
Adjustments

©2017 Advisory Board • All Rights Reserved • advisory.com
29 29
A More Limited Scope Than Previous Proposals
Notable Components of Past Proposals Left Out of Current Bill
Source: Health Care Advisory Board interviews and analysis.
Noteworthy Absences from AHCA
Proposed Bill Does Not Target:
Insurance Market
Protections
Payment
Reform
Center for Medicare
& Medicaid
Innovation (i.e. no
impact to funding)
Medicare Shared
Savings Program
MACRA
Medicare payment
(i.e. no repeal of
ACA payment cuts)
Medicare coverage
(i.e. no shift to
premium support)
Tax exclusions
for employer-
sponsored
insurance
Medicare Part D
(i.e. no move to
Medicare bidding
system)
Restrictions on
drug importation
Medicare Employer
Health Benefits
Drug
Spending
Guaranteed
issue
Dependent
eligibility until 26
Essential health
benefits in
individual market

30
2
3
1
Road Map
©2017 Advisory Board • All Rights Reserved • advisory.com • 33602A
GOP Moving Toward ACA “Repeal and Replace”
Key Details of American Health Care Act
Next Steps for Providers

©2017 Advisory Board • All Rights Reserved • advisory.com
31 31
Use free-markets to promote private
sector competition in payer, provider
markets
Focus more aggressively on
reducing federal health care
spending
Mandate greater consumer choice
and shopping at the point-of-care and
point-of-coverage through improved
transparency
Reduce federal role in health
care; provide states more
autonomy to make decisions, cut
spending
The Next Era of Health Care Reform
Four Key Principles Guiding GOP Reform Efforts
Reduce Federal
Entitlement Spending
Embrace Free Markets and
Consumer Choice
Promote Transparency of Cost
and Quality
Devolve Health Policy
Control to States 1 2
3 4
Source: Health Care Advisory Board interviews and analysis.

©2017 Advisory Board • All Rights Reserved • advisory.com
32 32
Path Forward Not Dependent on Politics
No-Regrets Priorities for Next Era of Health Care Reform
• Multi-channel navigation
platform, including search,
price estimation, and
triage/scheduling helps
streamline transactions
• Development of diverse
network of access points
(e.g. urgent care, retail,
enhanced access to
specialty care, primary
care) to meet varied
consumer access demands
Accessibility
• Organization-wide
commitment and investment
in service delivery and quality
improvement drives broad
engagement in delivering
superior outcomes
• High-reliability approach to
both service delivery and
clinical quality ensures
baseline of performance
Reliability
• Willingness to partner
with lower-cost
providers offers patients
affordable options, helps
prevent markets from
becoming overbuilt
• When markets are
already overbuilt,
commitment to scale
back excess capacity
ensures affordability in
the long-term
Affordability
Source: Health Care Advisory Board interviews and analysis.

©2017 Advisory Board • All Rights Reserved • advisory.com
33 33
Adapting Provider Strategy to New Market Realities
Four Key Steps to Succeed In the Next Era of Health Care Reform
Source: Health Care Advisory Board interviews and analysis.
Radically Reduce
Cost Structure
Establish a Sustainable
Medicare Risk Strategy
Build a Consumer
Loyalty Platform
Elevate Physician
Network Performance
1 2
3 4
Reduce cost structure to enable
pricing flexibility
Prioritize consumer loyalty
strategy to build durable patient
relationships
Carefully pace transition to
Medicare risk to capture returns
from care management
Restructure physician network to
meet twin mandates of population
health and consumerism
2016-2017 Health Care Advisory Board National Meeting
To learn more, attend the 2016-2017 Health Care Advisory Board National
Meeting; members can register here or at https://www.advisory.com/research

©2017 Advisory Board • All Rights Reserved • advisory.com
34 34
Managing your GoTo panel
How to Ask a Question
To ask the presenter, please type your question
into the “Questions” box on your GoTo panel and
press send.
Minimizing and maximizing
your screen
Use the orange and white arrow to
minimize and maximize your GoTo
panel.
Use the blue and white square to
maximize the presentation area.

©2017 Advisory Board • All Rights Reserved • advisory.com
35 35
Webconference Survey
Please note that the survey does not apply to webconferences viewed on demand.
Please take a minute to provide your
thoughts on today’s presentation.
Thank You!

2445 M Street NW, Washington DC 20037
P 202.266.5600 │ F 202.266.5700 │ advisory.com


















![PART I - utamaduniwetu.files.wordpress.com€¦ · An Act to repeal and replace the Newspaper Ordinance and to amend the Penal Code [] ENACTED by the Parliament of the United Republic](https://static.fdocuments.in/doc/165x107/6059f83a31bb1420ef2ade14/part-i-an-act-to-repeal-and-replace-the-newspaper-ordinance-and-to-amend-the-penal.jpg)