What to do if the spine x-ray shows a ---? – Part 2
44
Scoliosis Classification: Idiopathic: 80% Infantile <3; Juvenile 4-10; Adolescent: 10-18 Or: Early onset <5; Late onset >5 Congenital: Osteogenic: hemivertebra, fused vertebra Neurogenic: tethered cord, syringomyelia, Chiari Developmental: Achondroplasia NF OI Neuromuscular: Cerebral palsy Tumour: Osteoid osteoma BPNST
-
Upload
spineplus -
Category
Health & Medicine
-
view
792 -
download
0
Transcript of What to do if the spine x-ray shows a ---? – Part 2

Scoliosis Classification:
Idiopathic: 80% Infantile <3; Juvenile 4-10; Adolescent: 10-18
Or: Early onset <5; Late onset >5
Congenital: Osteogenic: hemivertebra, fused vertebra
Neurogenic: tethered cord, syringomyelia, Chiari
Developmental: Achondroplasia
NF OI
Neuromuscular: Cerebral palsy
Tumour: Osteoid osteoma
BPNST

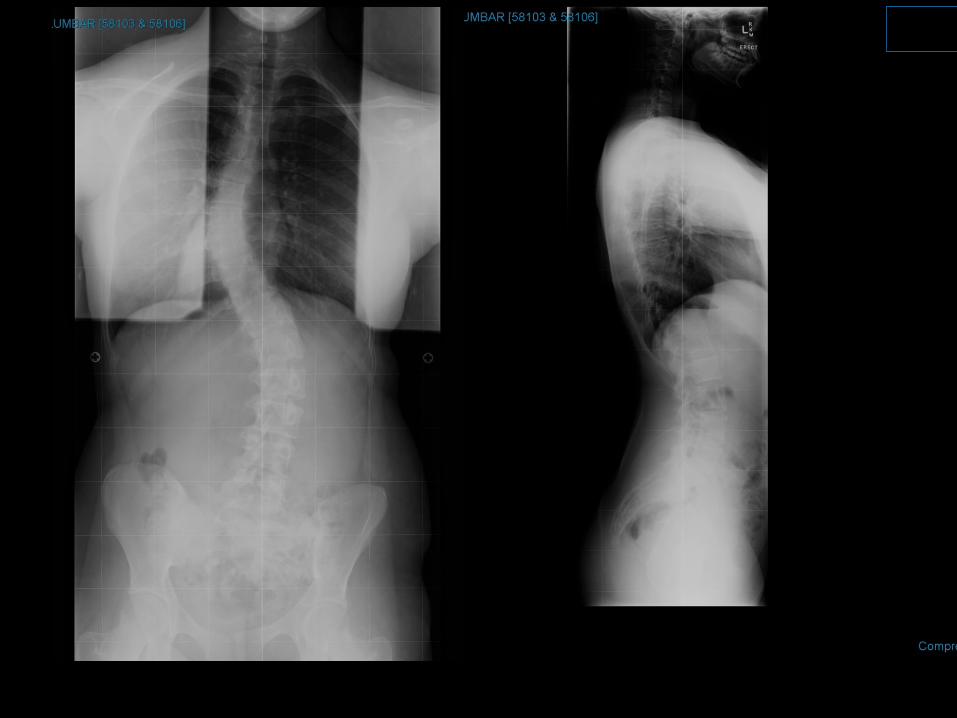
Xray report- there is a mild thoracic scoliosis convex to the left centered at T10.



Adolescent gymnast



16 F
Fit & well
Curve noticed 12 yrs of age
Left thoracic and right T/L curve
O/E Absent abdominal reflex ,
Brisk lower limb reflexes,? Up going plantars


Scheuermann's Disease
Thoracic pain
Kyphosis of greater than 40 degrees
Vertebral end plate abnormality
Variable wedging of at least 3 consecutive thoracic vertebra

16 yr M
Chronic cough
No pain
CXR report- Scheuermann's disease of the thoracic spine is noted.


22 yr M
Chronic Thoracic Pain
Increasing kyphosis



Nomenclature of disc herniations and spinal stenosis
Consistent
Reflect common usage where appropriate
Surgically relevant
‘Able to visualize over the phone’
2 morphological characteristics: Nature of disc pathology Location
Able to add further descriptors Neural structures Clinical context
www.asnr.org/spine_nomenclature/reporting
Disc Degeneration Annular Tear/Fissure
Disc Bulge
Disc Herniation – Protrusion
-- Extrusion
Disc Sequestration

Annular tear/ fissure
‘Tear’ and ‘fissure’ interchangeable
‘Tear’ more common usage Does not imply trauma

Disc bulge
Generalised extension of disc tissue beyond intervertebral disc space
‘Generalised’ = >50% circumference (>1800)
Relatively short distance, <3mm
Disc Protrusion
Involves less than 180% of the disc
The base of the herniation is wider than the height.
<180 but >90% - broad based
<90% - focal
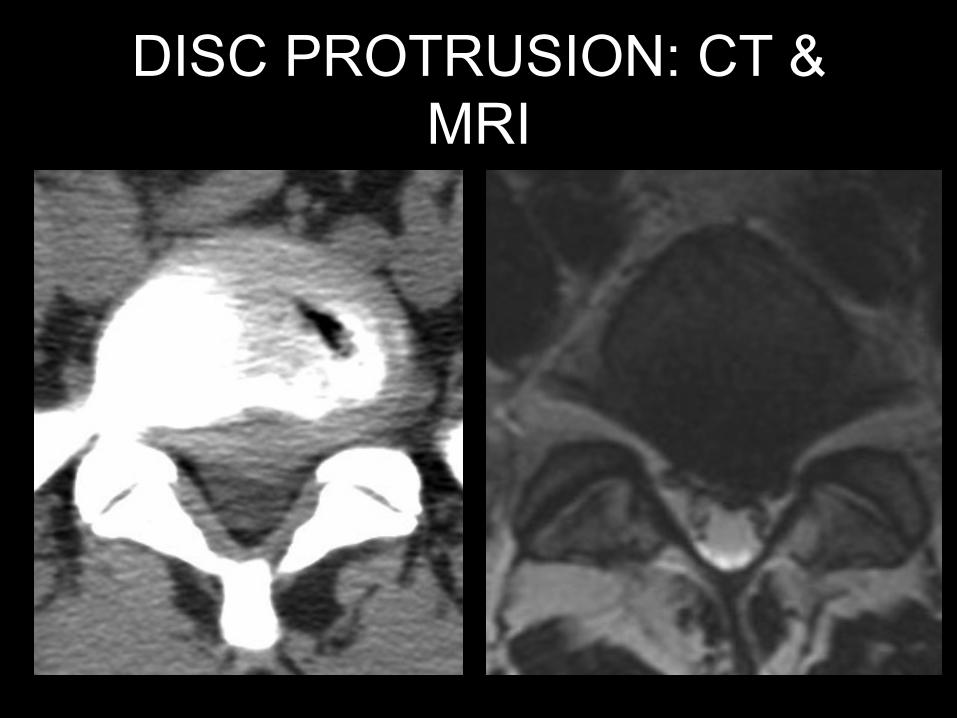
DISC PROTRUSION: CT & MRI

Extruded disc Greatest distance in any plane between
edges > base
T1

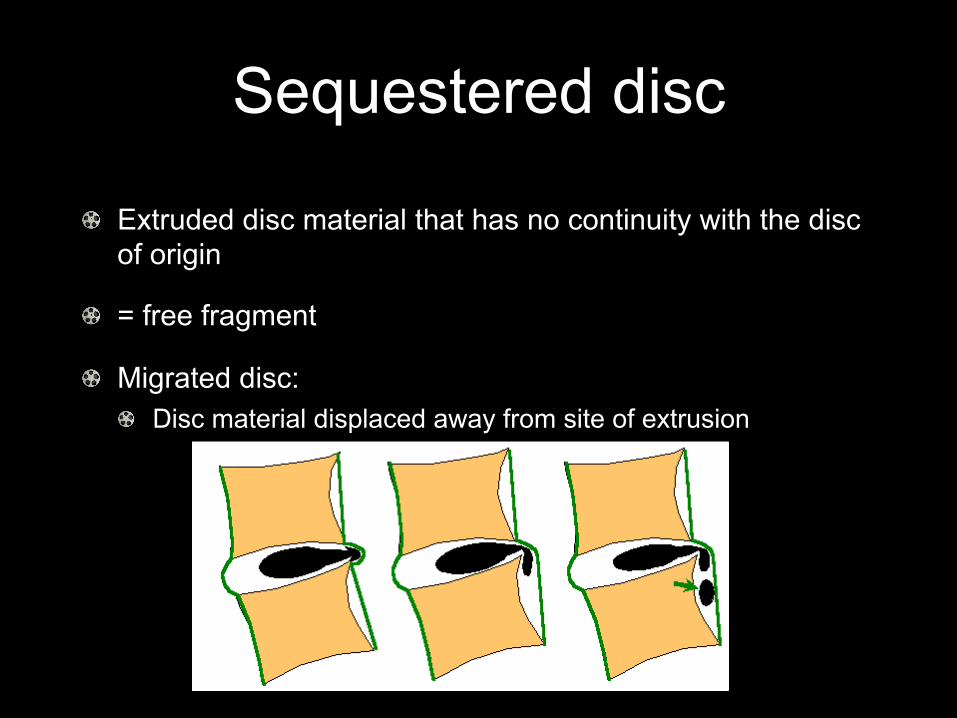
Sequestered disc
Extruded disc material that has no continuity with the disc of origin
= free fragment
Migrated disc: Disc material displaced away from site of extrusion

T2 T2
T1

Image interpretation A few cases

68M
Sudden onset bilateral leg pain and weakness
Urinary retention




Dx: Cauda equina syndrome
Cause: massive sequestration
Other causes: Tumour
Primary of lower cord: ependymoma Primary of nerve: BPNST Primary of dura: meningioma Primary of vertebral body: chordoma, giant cell tumour Secondary
Trauma

Clinical details: 54M. Left leg pain, paresthesia and weakness.



MR LUMBAR SPINE Clinical details: 54M. Left leg pain, paresthesia and weakness. Sequences: T1, T2 transverse and sagittal Findings:
Conclusion: Multilevel disc degeneration. Spondylolisthesis at L5/S1 with associated degenerative changes. The most significant lesion is a broad based left central disc extrusion at L4/5 compressing the left side of thecal sac displacing the left L5 and S1 nerve roots.

CT LUMBAR SPINE Clinical Details: 57 M. Episodes of feeling both lower limbs being weak and giving way.


CT LUMBAR SPINE Clinical Details: 57 M. Episodes of feeling both lower limbs being weak and giving way. Findings:
Conclusion: Severe facet joint degeneration and disc degeneration at the L4/5 level resulting in moderately severe central canal stenosis and bilateral subarticular stenosis, more marked on the left.

CT LUMBAR SPINE Clinical Details: 57M. Moderately severe back pain for one year.


CT LUMBAR SPINE Clinical Details: 57M. Moderately severe back pain for one year. Findings:
Conclusion: Bilateral L5 pars defects and L5/S1 spondylolisthesis with secondary degenerative changes as described.