What is trauma? · TRAUMA PATIENT CONFERENCE Management of Patients with Penetrating Trauma OLIVER...
19
6/4/2013 1 7 TH ANNUAL TREATMENT AND REHABILITATION OF THE PEDIATRIC TRAUMA PATIENT CONFERENCE Management of Patients with Penetrating Trauma OLIVER LAO, MD, MPH Presenter Disclosures Consultant/ Speakers bureaus No Disclosures. Research funding No Disclosures. Stock ownership/Corporate boards-employment No Disclosures. Off-label uses No Disclosures. What is trauma? Trauma Epidemiology 38,000 Deaths in US annually due to shootings. Mechanisms of penetrating trauma Knives, Arrows, Nails, etc Penetrating Trauma Years of Potential Life Lost 18.00% 16.40% 24.80% 40.80% Injury Cancer Heart Disease All Other Diseases MMWR 1982;31,599.
Transcript of What is trauma? · TRAUMA PATIENT CONFERENCE Management of Patients with Penetrating Trauma OLIVER...
6/4/2013
1
7 TH ANNUAL TREATMENT AND REHABILITATION OF THE PEDIATRIC
TRAUMA PATIENT CONFERENCE
Management of Patients with Penetrating Trauma
OLIVER LAO, MD, MPH
Presenter Disclosures
Consultant/
Speakers bureaus
No Disclosures.
Research funding No Disclosures.
Stock
ownership/Corporate boards-employment
No Disclosures.
Off-label uses No Disclosures.
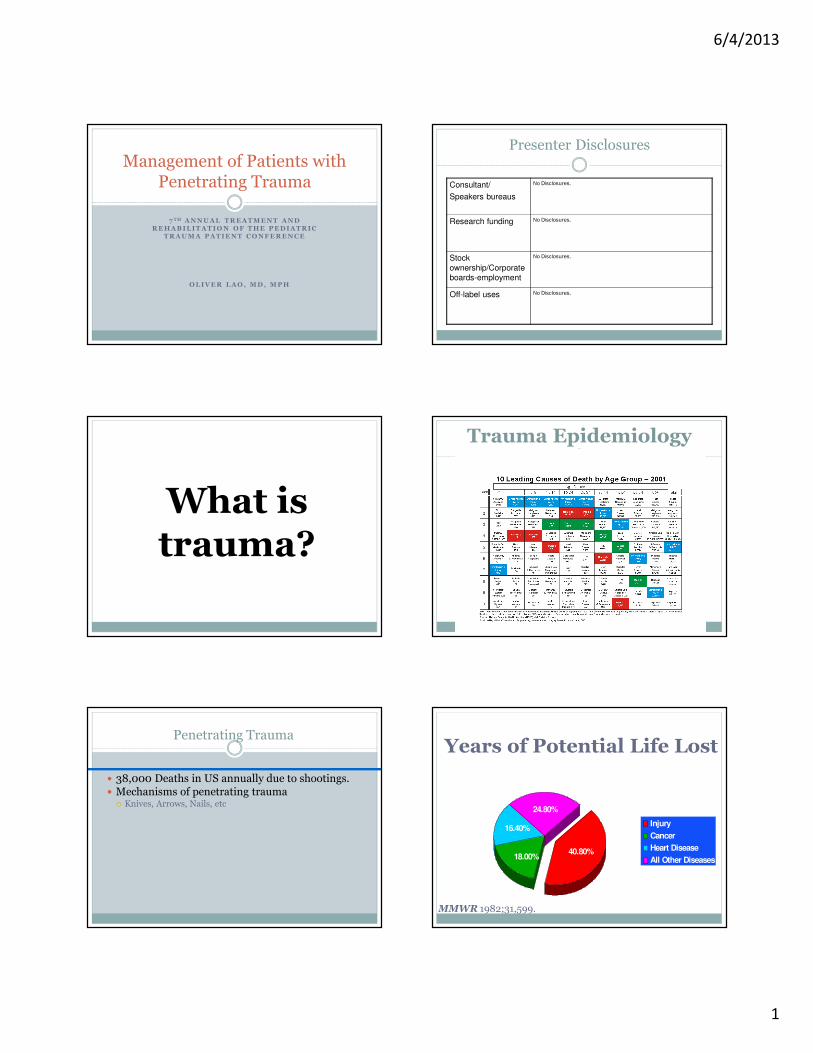
What is trauma?
Trauma Epidemiology
� 38,000 Deaths in US annually due to shootings.� Mechanisms of penetrating trauma
� Knives, Arrows, Nails, etc
Penetrating TraumaYears of Potential Life Lost
18.00%
16.40%
24.80%
40.80%
Injury
Cancer
Heart Disease
All Other Diseases
MMWR 1982;31,599.

6/4/2013
2
Mechanisms of Injury: Penetrating Trauma
� Gun shot wounds
� Stab wounds
� Impalement
Gun Shot Wounds: Mechanism
� Energy transfer� Shape/size of bullet� Distance to target
� Velocity (most important)� Kinetic energy = (Mass × Velocity2 )/2
� Surface area distributed� Tumble and yaw� Fragmentation
� Anatomy� Viscoelasticity
�Muscle� organs
Stab wounds
� Mechanism
� Blunt: Crush injury
� Sharp:Tissue disruption
� Extent of Injury
� Weapon size, length, sharpness, penetration
� Severe injury
� Chest and abdomen
� 4+ wounds
� Understanding principles of energy exchange increase the Index of Suspicion associated with
the MOI
Introduction to Penetrating Trauma
� Kinetic Energy Equation
� Greater the mass the greater the energy
� Double mass = double KE
� Greater the speed the greater the energy
� Double speed = 4x increase KE
Physics of Penetrating Trauma
2
)()(2
speedVelocityweightMassKE
×=
Physics of Penetrating Trauma
� Small & Fast bullet can cause greater damage than large and slow.� Different bullets of different weights traveling at different
speeds cause
� Low Energy/Low Velocity
� Knives and arrows
�Medium Energy/Medium Velocity Weapons
� Handguns, shotguns, low-powered rifles
� 250-400 mps
�High Energy/High Velocity
� Assault Rifles
� 600-1,000 mps

6/4/2013
3
Physics of Penetrating Trauma
� Bullet spins as it travels down barrel
� Rifling in barrel
� Allows bullet to travel straight with slight yaw
� Bullet departs barrel, spinning with a slight
wobble or yaw
�Weapon forced backward and absorbs
energy
� Recoil
Physics of Penetrating Trauma
� Remainder of energy propels bullet forward
at a high rate of speed.
� Trajectory is curved due to gravity
� As bullet strikes object, it slows and energy
is transferred to object.
� Law of Conservation of Energy
Ballistics
� Study of the characteristics of projectiles in
motion and effects upon objects impacted
� Factors affecting energy exchange between a
projectile and body tissue� Velocity
� Profile
� Stability
� Expansion & Fragmentation
� Secondary Impacts
� Shape
Energy Dissipation
� Drag:� wind resistance
� Cavitation:� formation of a partial vacuum and cavity within a semi-fluid medium
� Profile:� Size and shape of a projectile as it contacts a target
� Larger the profile=greater energy exchange
� Expansion and fragmentation results in damage
� Stability� Allows for straighter trajectory
� Decreases after striking object results in tumbling

6/4/2013
4
Aspects of Ballistics
� Velocity� Causes Trajectory
� Faster = straighter trajectory
� Slower = more curved due to gravity
Aspects of Ballistics
� Profile
� Portion of bullet you see as it travels towards you
� Larger profile = greater energy exchange
� Caliber
� Diameter of a bullet (ID of gun)
� 0.22 caliber = 0.22 inches
� Bullets become unstable as they pass from one medium
to another.
Aspects of Ballistics
� Stability
� Bullet length increases bullet tumbling
� Can reduce the accuracy of the shot
� Reduced by Rifling in barrel (spinning)
� Yaw
� Gyroscopic effect on the center axis of the bullet that
reduces tumbling
� Tumbling of bullet once it strikes object
� Reduces kinetic energy
� Greater tissue damage
Bullet Gyroscopic Effect
Aspects of Ballistics
� Expansion & Fragmentation
� Results in increased profile
� Mushrooming
� Initial impact forces may result in fragmenting
� Greater tissue damage
Aspects of Ballistics
� Secondary Impacts� Bullet striking other objects can cause yaw and tumble
� Body Armor (Kevlar)
� Transmits energy throughout entire vest resulting in blunt trauma
� Myocardial Contusion
� Pulmonary Contusion
� Rib Fractures
� Shape� Handgun Ammunition = Blunt = Tumble
� Rifle Ammunition = Pointed = Piercing
6/4/2013
5
� Handguns� Small caliber, short barrel, medium-velocity
� Effective at close range
� Severity of injury based upon organs damaged
� Rifle� High-velocity, longer barrel, large caliber
� Increased accuracy at far distances
� Assault Rifles� Large magazine, semi- or full-automatic
� Similar injury to hunting rifles
� Multiple wounds
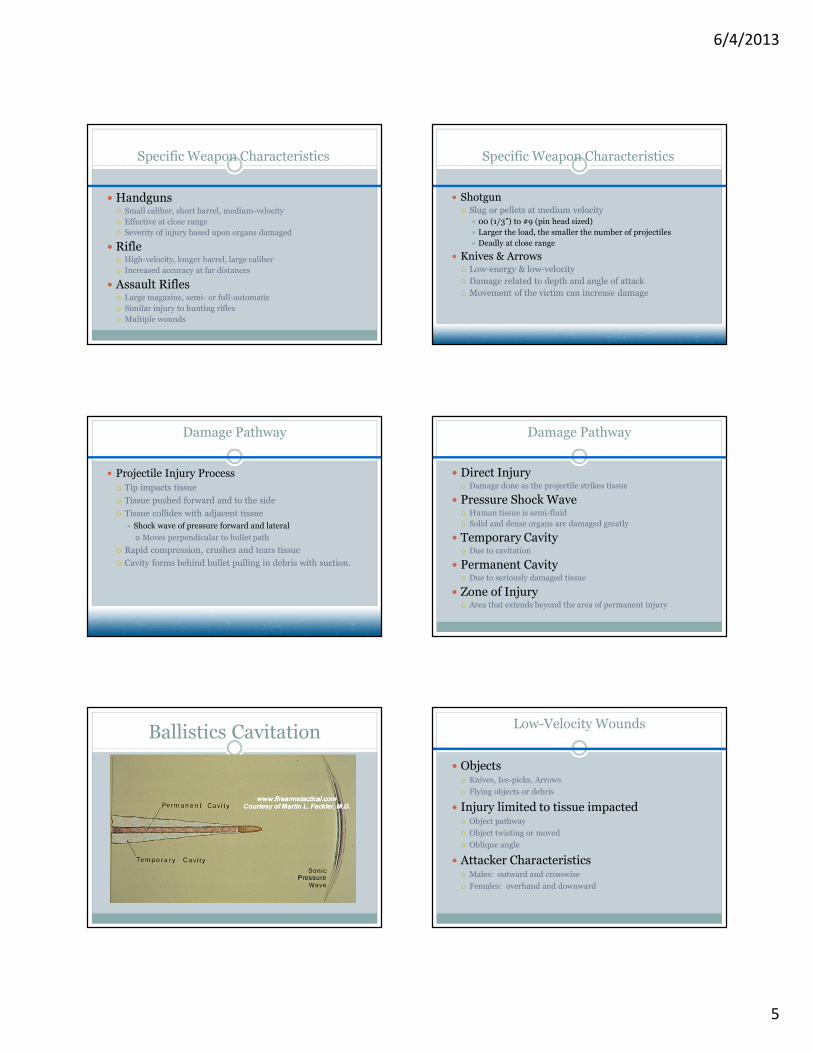
Specific Weapon Characteristics
� Shotgun� Slug or pellets at medium velocity
� 00 (1/3”) to #9 (pin head sized)
� Larger the load, the smaller the number of projectiles
� Deadly at close range
� Knives & Arrows� Low-energy & low-velocity
� Damage related to depth and angle of attack
� Movement of the victim can increase damage
Specific Weapon Characteristics
Damage Pathway
� Projectile Injury Process
� Tip impacts tissue
� Tissue pushed forward and to the side
� Tissue collides with adjacent tissue
� Shock wave of pressure forward and lateral
� Moves perpendicular to bullet path
� Rapid compression, crushes and tears tissue
� Cavity forms behind bullet pulling in debris with suction.
Damage Pathway
� Direct Injury� Damage done as the projectile strikes tissue
� Pressure Shock Wave� Human tissue is semi-fluid
� Solid and dense organs are damaged greatly
� Temporary Cavity� Due to cavitation
� Permanent Cavity� Due to seriously damaged tissue
� Zone of Injury� Area that extends beyond the area of permanent injury
Ballistics CavitationLow-Velocity Wounds
� Objects� Knives, Ice-picks, Arrows
� Flying objects or debris
� Injury limited to tissue impacted� Object pathway
� Object twisting or moved
� Oblique angle
� Attacker Characteristics� Males: outward and crosswise
� Females: overhand and downward

6/4/2013
6
� Density of tissue affects the efficiency of energy transmission� Resiliency
� Strength and elasticity of an object
� Connective Tissue� Absorbs energy and limits tissue damage
� Organs� Solid Organs
� Dense and low resilience
� Hollow Organs� Fluid filled: transmit energy = increased damage
� Air filled: absorbs energy = less damage
Specific Tissue & Organ Injuries
� Lungs
� Air in lung absorbs energy
� Parenchyma is compressed and rebounds
� Pneumothorax or hemothorax can result
� Bone
� Resists displacement until it shatters
� Alters projectile path
Specific Tissue & Organ Injuries
General Body Regions
� Extremities� Injury limited to resiliency of tissue
� 60-80% of injuries with <10% mortality
� Abdomen (Includes Pelvis)� Highly susceptible to injury and hemorrhage
� Bowel perforation: 12-24 hrs peritoneal irritation
� Thorax� Rib impact results in explosive energy
� Heart & great vessels have extensive damage due to lack of fluid compression
� Any large chest wound compromises breathing
General Body Regions
� Neck
� Damages Trachea and Blood Vessels
� Neurological problems
� Sucking neck wound
� Head
� Cavitational energy trapped inside skull
� Serious bleeding and lethal
Wound Characteristics
� Entrance Wounds� Size of bullet profile for non-deforming bullets
� Deforming projectiles may cause large wounds
� Close Range
� Powder Burns (Tattooing of powder)
� 1-2 mm circle of discoloration
� Localized subcutaneous emphysema
� Exit Wounds� Appears to be “Blown” outward
� Pressure wave
� Scene Size-Up� Law-Enforcement
� DO NOT ENTER UNTIL SCENE IS SAFE!
� Weapons: Victim or Assailant
� Assailants
� IF A CRIME SCENE
� DOCUMENT
� DO NOT DISTURB EVIDENCE
� RETAIN CLOTHING, ETC
� LIMIT PERSONNEL INVOLVEMENT
Special Concerns with Penetrating Trauma

6/4/2013
7
� Penetrating Wound Assessment
� Internal Organ Injury Potential
� Entrance & Exit Wounds
Special Concerns with Penetrating Trauma
PROVIDE RAPID
TRANSPORT FOR ANY
GSW TO HEAD, CHEST,
OR ABDOMEN. TREAT
AGGRESIVELY FOR
SHOCK!!
Trauma is notbrain surgery!
• Air goes in & out
• Oxygen is good
• Blood goes round & round
• Stop bleeding
• Put things back where and how they belong
A-B-C-D-E
Initial Assessment: Primary Survey
•A = Airway
•B = Breathing
•C = Circulation
•D = Disability
•E = Exposure
• Clear & establish a good airway–Consider intubation for coma, shock, and neck/thoracic injuries
• C-spine stabilization
Initial Assessment: Airway
6/4/2013
8
• Clear & establish a good airway–Consider intubation for coma, shock, and neck/thoracic injuries
• C-spine stabilization
Initial Assessment: Airway
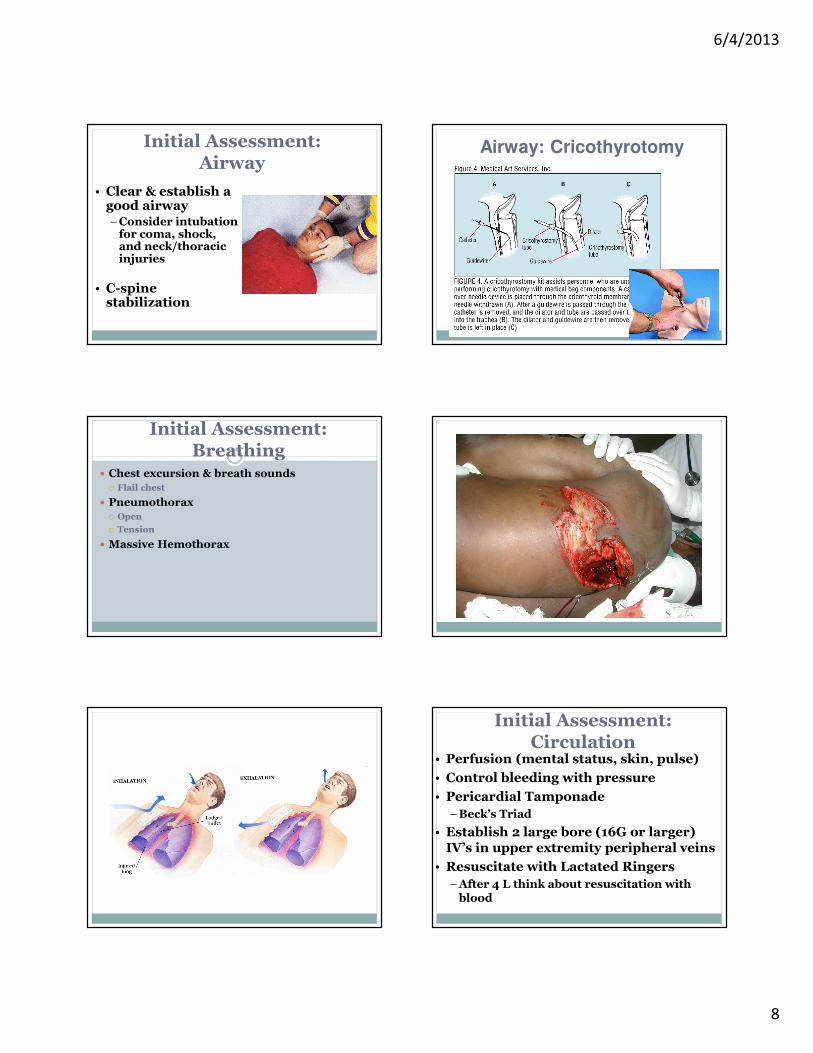
Airway: Cricothyrotomy
Initial Assessment: Breathing
� Chest excursion & breath sounds
� Flail chest
� Pneumothorax
� Open
� Tension
� Massive Hemothorax
Initial Assessment: Circulation
• Perfusion (mental status, skin, pulse)
• Control bleeding with pressure
• Pericardial Tamponade
–Beck’s Triad
• Establish 2 large bore (16G or larger) IV’s in upper extremity peripheral veins
• Resuscitate with Lactated Ringers
–After 4 L think about resuscitation with blood

6/4/2013
9
Initial Assessment: Disability
• Neurologic status
–Glasgow Coma Scale
• Eye
•Motor-best predictor of long term outcome
• Verbal
–Spinal Cord Injury
Initial Assessment: Exposure
• Remove clothes
• Temperature
–warm blankets
• Finger and tube in every orifice
• Maintain full spine precautions
–Log Roll
Initial Assessment:Exposure
• Stabilize Fractures
• Relocate dislocated joints
• Reassess pulses
Secondary Survey• Patient history
• Head to toe physical exam
• Radiography
–Lateral C-spine, C-xray, pelvis
–One cavity above/below entrance/exit wounds
–FAST
• Urinary bladder drainage
• NGT
• Blood sampling/monitoring
� Penetrating Wound Care� Facial Wounds
� Difficult intubations
� Depress chest
� Pass ET through bubbling tissue
� Consider LMA and Combitube
� Consider Cricothyreotomy & Cricothyreostomy
� Chest Wounds� Pneumothorax
� 2/3” the diameter of the trachea or larger to entrain air
� 3-sided occlusive dressing
� Needle Decompress
� Pericardial Tamponade
Special Concerns with Penetrating Trauma

6/4/2013
10
� Impaled Objects
� Low-energy
� Dangerous to remove
� DO NOT REMOVE
� UNLESS
� In Cheek
� Interferes with CPR: ASSESS!!!
Special Concerns with Penetrating Trauma Neck
• Air goes in & out
• Oxygen is good
• Blood goes round & round
• Stop bleeding
• Put things back where and how they belong
A-B-C-D-E
Initial Assessment: Primary Survey
•A = Airway
•B = Breathing
•C = Circulation
•D = Disability
•E = Exposure
ETIOLOGY
� Stab wounds (SW) vs gunshot wounds (GSW)
� In the civilian sector, SWs account for 55-70% of the injuries.
� GSWs carry a higher morbidity and mortality.
� The morbidity and mortality of GSWs depend on the characteristics and velocity of the missile.

6/4/2013
11
Penetrating Neck
Among all penetrating neck wounds, the following occur:
�Major vascular injury: 15–25% Internal Jugular vein injured most
commonly
�Laryngotracheal injury: 10-15%
�Pharyngeal or esophageal injury:
7%
�Spinal cord injury: 10-15% of GSW, rare in SW
Anatomy� III – Base of skull to Angle of Mandible: distal internal carotid and vertebral vessels, cranial nerves, parotid gland, nasopharynx
� II - Angle of mandible to cricoid cartilage: carotid and vertebral vessels, larynx, trachea, esophagus, vagus and recurrent laryngeal nerves, spinal cord
� I - Cricoid cartilage to clavicles: great vessels of upper chest, upper lung, esophagus, trachea, thoracic duct, cervical nervous system
In stable patients, management varies based on Zone of injury.
Stable or Unstable?
� Airway, Breathing, Circulation
� BP < 90 which poorly responds to volume = Unstable patient
-CXR to help determine trajectory/op approach
-To the OR
ZONE II INJURY – STABLE PATIENT
Physical exam – the most essential portion of the evaluation
“Hard” clinical signs:-Active bleeding-large, pulsatile, &/or expanding hematoma-cervical bruit or thrill-central neurologic deficit
These “hard” clinical signs strongly predict presence of major vascular injury and generally mandate operative or other therapeutic intervention.
ZONE II INJURY – STABLE PATIENT
� If no “hard” clinical signs of vascular injury are present, a growing body of evidence supports simple
observation of these patients.
� Simple observation of stable Zone II patients without “hard” clinical signs has a missed injury rate of 0.6%. (8 studies, 1216 total pts, 837 observed)

6/4/2013
12
ZONES I AND III INJURY – STABLE PATIENT
� Physical exam is less reliable in Zones I and III
� Routine arteriography for both diagnosis, localization, and possible (Zone III) treatment
� Routine esophagography or esophagoscopy in Zone I injury
OR
� Zone I injury, site unclear:
median sternotomy is the most versatile incision. May extend incision up the neck or out laterally
infraclavicularly
� Zone II injury:
Standard anterior neck incision
� Zone III injury
Standard anterior neck incision
in the OR, ZII or III
� Pt supine, neck extended, rotated away from injured side
� Surgically prepare and drape to include a potential
median sternotomy incision
� Incision made anterior to the sternocleidomastoid
muscle
� Expose carotid arteries, internal jugular vein to elucidate source of hemorrhage
Chest
• Air goes in & out
• Oxygen is good
• Blood goes round & round
• Stop bleeding
• Put things back where and how they belong
A-B-C-D-E

6/4/2013
13
Initial Assessment: Primary Survey
•A = Airway
•B = Breathing
•C = Circulation
•D = Disability
•E = Exposure
Spaces
Cardiac Box
� Superior: clavicles
� Inferior: costal margins
� Lateral: midclavicular line
Penetrating Cardiac Injuries
� More proximal coronary artery lacerations require coronary bypass. Rarely, the interventricular
septum, a valve, papillary muscle, or chordaetendineae is lacerated, producing an acute shunt or valvular insufficiency. These lesions are poorly tolerated and can quickly produce massive
pulmonary edema and cardiogenic shock
Penetrating Cardiac Injuries Prognosis
� Several factors adversely affect survival. These include GSW mechanisms and wounds that involve the left ventricle, multiple cardiac chambers, intrapericardial great vessels, or one or more coronary arteries. Factors favorable to survival include stab wound mechanisms with minor perforations, isolated right ventricular wounds, a systolic blood pressure greater than 50 mm Hg on arrival at the ED, and the presence of cardiac tamponade.
6/4/2013
14
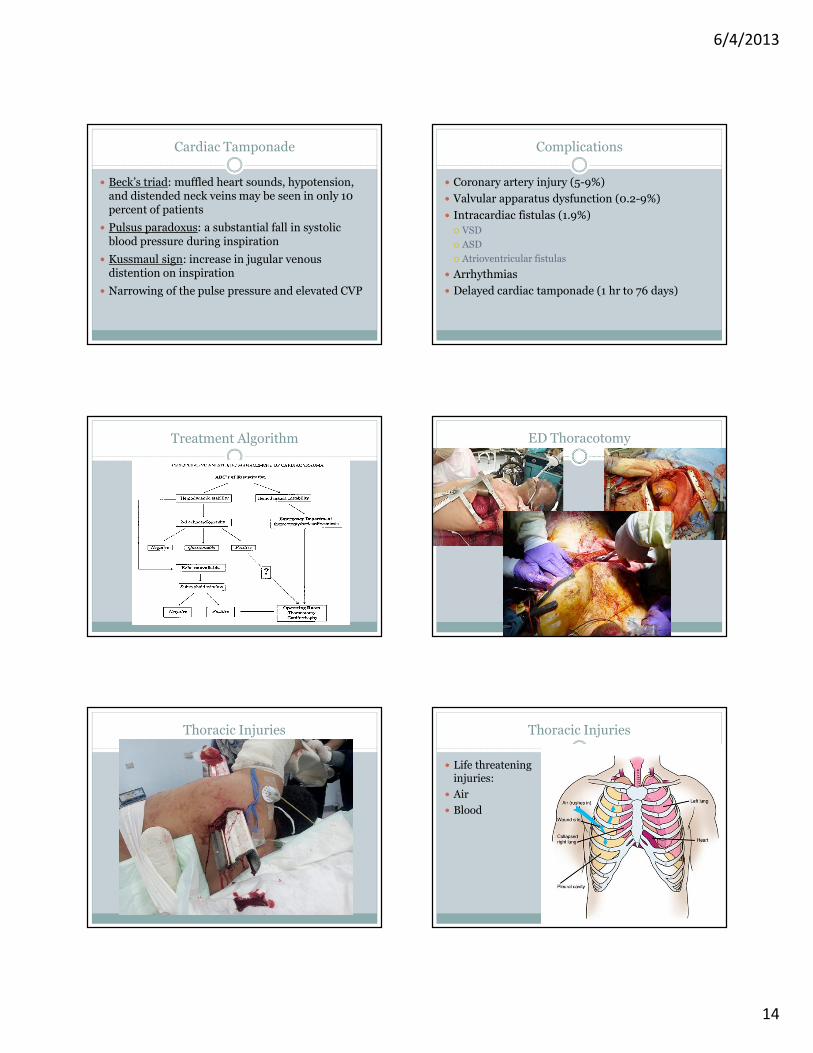
Cardiac Tamponade
� Beck’s triad: muffled heart sounds, hypotension, and distended neck veins may be seen in only 10 percent of patients
� Pulsus paradoxus: a substantial fall in systolic blood pressure during inspiration
� Kussmaul sign: increase in jugular venous distention on inspiration
� Narrowing of the pulse pressure and elevated CVP
Complications
� Coronary artery injury (5-9%)
� Valvular apparatus dysfunction (0.2-9%)
� Intracardiac fistulas (1.9%)
� VSD
� ASD
� Atrioventricular fistulas
� Arrhythmias
� Delayed cardiac tamponade (1 hr to 76 days)
Treatment Algorithm ED Thoracotomy
Thoracic Injuries Thoracic Injuries
� Life threatening injuries:
� Air
� Blood

6/4/2013
15
Thoracic Injuries: Air Thoracic Injuries: Needle Decompression
Thoracic Injuries: Blood Thoracic Injuries: Sucking Chest Wound
Abdomen
• Air goes in & out
• Oxygen is good
• Blood goes round & round
• Stop bleeding
• Put things back where and how they belong

6/4/2013
16
A-B-C-D-E
Initial Assessment: Primary Survey
•A = Airway
•B = Breathing
•C = Circulation
•D = Disability
•E = Exposure
Penetrating Abdominal Trauma
GSW KSW
OR HD Unstable HD Stable/No peritonitis
OR Peritoneal Penetration
Positive Negative
OR Observation
Penetrating Abdominal Trauma
Abdominal Trauma
Abdominal Trauma Abdominal Trauma

6/4/2013
17
Abdominal Cavity Abdominal Trauma?
Pelvic Injury
�Introduction
� significant blood loss if bilateral
�may settle in retroperitoneal space
�3% of all fractures
�mortality 8 - 50%
�2ndmost common cause of traumatic death
Pelvic Fracture
� Signs & Symptoms
� pelvic instability
� pain (suprapubic also)
� crepitus
� bloody meatus
� neurovascular deficits
• Air goes in & out
• Oxygen is good
• Blood goes round & round
• Stop bleeding
• Put things back where and how they belong

6/4/2013
18
A-B-C-D-E
Initial Assessment: Primary Survey
•A = Airway
•B = Breathing
•C = Circulation
•D = Disability
•E = Exposure
Pelvic Injury: MAST Pelvic Injury: Sheet
Pelvis
�Interventions�Stable patient
�analgesia
�Repair vs mobilization
�Unstable patient�Immobilize
�Ex-fix
�Angiography�embolization
Extremity/Vascular Injury

6/4/2013
19
Extremity/Vascular
• Air goes in & out
• Oxygen is good
• Blood goes round & round
• Stop bleeding
• Put things back where and how they belong
A-B-C-D-E
Initial Assessment: Primary Survey
•A = Airway
•B = Breathing
•C = Circulation
•D = Disability
•E = Exposure
Extremity/Vascular: Tourniquet Extremity/Vascular: BP Cuff